
Impact of COVID-19 Lock-Downs on Nature Connection in Southern and Eastern Africa

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Procedure
2.2. Survey Method and Statistical Analysis
3. Results
3.1. Comparative Changes in Perception and Behavior
3.2. Confirmatory Factor Analysis
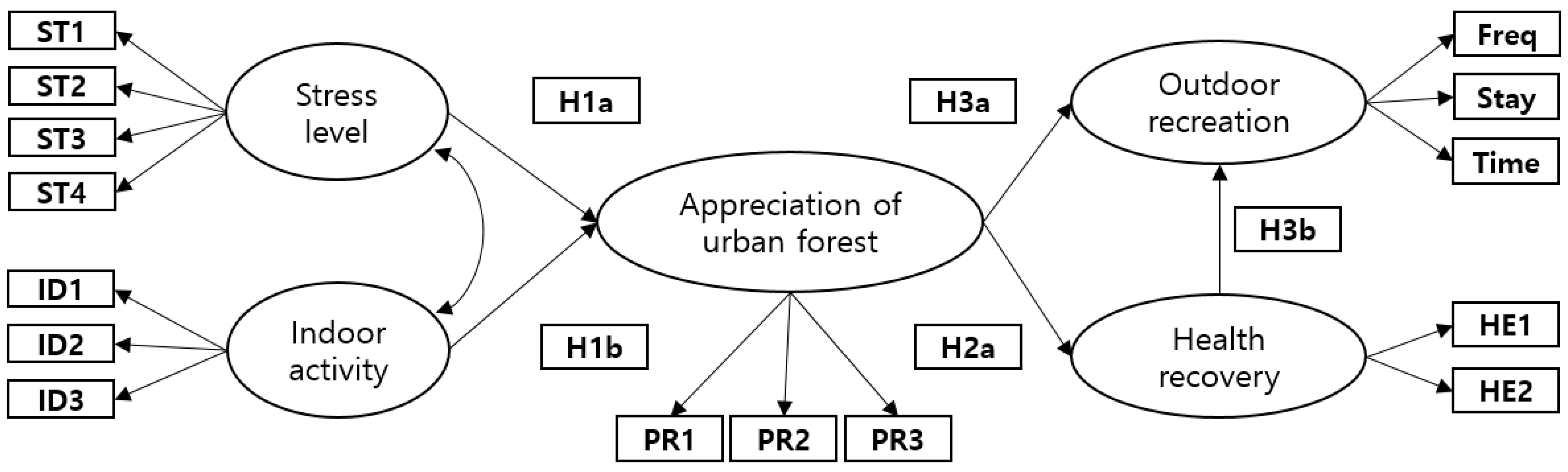
3.3. Structural Equation Modeling for the Research Hypotheses
4. Discussion
4.1. Distancing from Nature during Lock-Down Measures
4.2. Perception of Recovery in Human Health in Nature during the COVID-19 Pandemic
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Hypothesis: Direction | Malawi | Rwanda | South Africa | Tanzania | Zambia | ||
|---|---|---|---|---|---|---|---|
| H1a: Stress level → | Appreciation of urban forest | Estimate | 0.106 | 0.419 | 0.363 | 0.027 | 0.375 |
| S.E. | 0.118 | 0.136 | 0.152 | 0.174 | 0.114 | ||
| CR | 0.898 | 3.081 | 3.175 | 0.002 | 3.281 | ||
| p | 0.497 | 0.002 | 0.001 | 0.998 | 0.001 | ||
| Result | Reject | Accept | Accept | Reject | Accept | ||
| H1b: Indoor activity → | Appreciation of urban forest | Estimate | 0.091 | 0.447 | 0.114 | 0.314 | 0.285 |
| S.E. | 0.134 | 0.160 | 0.167 | 0.215 | 0.142 | ||
| CR | 0.679 | 2.787 | 0.680 | 1.463 | 2.006 | ||
| p | 0.497 | 0.005 | 0.496 | 0.143 | 0.045 | ||
| Result | Reject | Accept | Reject | Reject | Accept | ||
| H2: Appreciation of urban forest → | Perception of health recovery | Estimate | 0.454 | 0.571 | 0.563 | 0.067 | 0.402 |
| S.E. | 0.172 | 0.155 | 0.177 | 0.082 | 0.097 | ||
| CR | 2.647 | 3.695 | 3.175 | 0.812 | 4.123 | ||
| p | 0.008 | 0.000 | 0.001 | 0.417 | 0.000 | ||
| Result | Accept | Accept | Accept | Reject | Accept | ||
| Model fit test | Chi2 | 119.963 | 64.672 | 130.390 | 151.270 | 140.689 | |
| p-value | 0.000 | 0.079 | 0.000 | 0.000 | 0.000 | ||
| GFI | 0.838 | 0.859 | 0.838 | 0.769 | 0.812 | ||
| AGFI | 0.747 | 0.781 | 0.747 | 0.639 | 0.707 | ||
| NFI | 0.780 | 0.848 | 0.774 | 0.722 | 0.810 | ||
| IFI | 0.859 | 0.961 | 0.847 | 0.795 | 0.869 | ||
| TLI | 0.807 | 0.946 | 0.792 | 0.720 | 0.822 | ||
| CFI | 0.854 | 0.959 | 0.843 | 0.788 | 0.865 | ||
| RMSEA | 0.122 | 0.048 | 0.052 | 0.167 | 0.057 | ||
References
- Wadvalla, B.A. How Africa has tackled COVID-19. BMJ 2020, 370, m2830. [Google Scholar] [CrossRef] [PubMed]
- Berhan, Y. Will Africa be devastated by COVID-19 as many predicted? Perspective and Prospective. Ethiop. J. Health Sci. 2020, 30, 459. [Google Scholar] [CrossRef] [PubMed]
- Massinga Loembé, M.; Tshangela, A.; Salyer, S.J.; Varma, J.K.; Ouma, A.E.O.; Nkengasong, J.N. COVID-19 in Africa: The spread and response. Nat. Med. 2020, 26, 999–1003. [Google Scholar] [CrossRef] [PubMed]
- Divala, T.; Burke, R.M.; Ndeketa, L.; Corbett, E.L.; MacPherson, P. Africa faces difficult choices in responding to COVID-19. Lancet 2020, 395, 1611. [Google Scholar] [CrossRef]
- Musanabaganwa, C.; Cubaka, V.; Mpabuka, E.; Semakula, M.; Nahayo, E.; Hedt-Gauthier, B.L.; NG, K.C.S.; Murray, M.B.; Kateera, F.; Mutesa, L.; et al. One hundred thirty-three observed COVID-19 deaths in 10 months: Unpacking lower than predicted mortality in Rwanda. BMJ Glob. Health 2021, 6, e004547. [Google Scholar] [CrossRef] [PubMed]
- International Organization for Migration. Regional Strategic Preparedness and Response Plan COVID-19. IOM East and Horn of Africa. April–December 2020. Available online: https://www.iom.int/news/iom-regional-office-launches-covid-19-strategic-preparedness-and-response-plan-east-and-horn-africa (accessed on 7 May 2022).
- El-Sadr, W.M.; Justman, J. Africa in the path of COVID-19. N. Engl. J. Med. 2020, 383, e11. [Google Scholar] [CrossRef]
- Tembo, J.; Maluzi, K.; Egbe, F.; Bates, M. COVID-19 in Africa. BMJ 2021, 372, n457. [Google Scholar] [CrossRef]
- Saleh, M. Impact of COVID-19 on Tanzania political economy. Int. J. Adv. Stud. Soc. Sci. Innov. 2020, 4, 24–36. [Google Scholar] [CrossRef]
- Mbow, M.; Lell, B.; Jochems, S.P.; Cisse, B.; Mboup, S.; Dewals, B.G.; Jaye, A.; Dieye, A.; Yazdanbakhsh, M. COVID-19 in Africa: Dampening the storm? Science 2020, 369, 624–626. [Google Scholar] [CrossRef]
- Ogbolosingha, A.J.; Singh, A. COVID-19 pandemic: Review of impediments to public health measures in Sub-Saharan Africa. Am. J. Prev. Med. 2020, 6, 68–75. [Google Scholar] [CrossRef]
- Mwisongo, A.; Nabyonga-Orem, J. Global health initiatives in Africa–governance, priorities, harmonisation and alignment. BMC Health Serv. Res. 2016, 16, 245–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Africa CDC. COVID-19 Africa Hotspot Dashboard. Available online: https://africacdccovid.org/ (accessed on 27 April 2022).
- Bammel, G.; Burrus-Bammel, L.L. Leisure and Human Behaviour; Wm. C. Brown Company Publishers: Dubuque, IA, USA, 1982; 361p. [Google Scholar]
- Landry, C.E.; Bergstrom, J.; Salazar, J.; Turner, D. How Has the COVID-19 Pandemic Affected Outdoor Recreation in the US? A Revealed Preference Approach. Appl. Econ. Perspect. Policy 2021, 43, 443–457. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Liu, S.; Lithopoulos, A.; Zhang, C.Q.; Garcia-Barrera, M.A. Correlates of perceived physical activity transitions during the COVID-19 pandemic among Canadian adults. Appl. Psychol. Health Well-Being 2020, 12, 1157–1182. [Google Scholar] [CrossRef]
- Morse, J.W.; Gladkikh, T.M.; Hackenburg, D.M.; Gould, R.K. COVID-19 and human-nature relationships: Vermonters’ activities in nature and associated nonmaterial values during the pandemic. PLoS ONE 2020, 15, e0243697. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Li, F. Physical activity during the coronavirus disease-2019 global pandemic. J. Sport Health Sci. 2020, 9, 291. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, S.J. Nature experience influences nature aversion: Comparison of South Korea and Germany. Soc. Behav. Personal. 2018, 46, 161–176. [Google Scholar] [CrossRef]
- Lee, J.H.; Cheng, M.; Syamsi, M.N.; Lee, K.H.; Aung, T.R.; Burns, R.C. Accelerating the Nature Deficit or Enhancing the Nature-Based Human Health during the Pandemic Era: An International Study in Cambodia, Indonesia, Japan, South Korea, and Myanmar, following the Start of the COVID-19 Pandemic. Forests 2022, 13, 57. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic: WHO Characterizes COVID-19 as a Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 27 April 2022).
- Vaske, J.J. Survey Research and Analysis: Applications in Parks, Recreation and Human Dimensions; Venture Publishing: State College, PA, USA, 2008; 635p. [Google Scholar]
- World Health Organization. A Systematic Approach to Monitoring and Analysing Public Health and Social Measures (PHSM) in the Context of the COVID-19 Pandemic: Underlying Methodology and Application of the PHSM Database and PHSM Severity Index (No. WHO/EURO: 2020-1610-41361-56329); World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2020; 45p. [Google Scholar]
- Marsh, H.W.; Dowson, M.; Pietsch, J.; Walker, R. Why multicollinearity matters: A reexamination of relations between self-efficacy, self-concept, and achievement. J. Educ. Psychol. 2004, 96, 518. [Google Scholar] [CrossRef]
- Chen, F.F. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct. Equ. Modeling A Multidiscip. J. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Hair, J.F.; Ringle, C.M.; Sarstedt, M. PLS-SEM: Indeed a silver bullet. J. Mark. Theory Pract. 2011, 19, 139–152. [Google Scholar] [CrossRef]
- Mulaik, S.A.; James, L.R.; Van Alstine, J.; Bennett, N.; Lind, S.; Stilwell, C.D. Evaluation of goodness-of-fit indices for structural equation models. Psychol. Bull. 1989, 105, 430–445. [Google Scholar] [CrossRef]
- Kim, H.; Ku, B.; Kim, J.Y.; Park, Y.J.; Park, Y.B. Confirmatory and exploratory factor analysis for validating the phlegm pattern questionnaire for healthy subjects. Evid-Based Complementary Altern. Med. 2016, 2016, 2696019. [Google Scholar] [CrossRef] [PubMed]
- Shadfar, S.; Malekmohammadi, I. Application of Structural Equation Modeling (SEM) in restructuring state intervention strategies toward paddy production development. Int. J. Acad. Res. Bus. Soc. Sci. 2013, 3, 576. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Marsh, H.W.; Balla, J.R.; McDonald, R.P. Goodness-of-fit indexes in confirmatory factor analysis: The effect of sample size. Psychol. Bull. 1988, 103, 391. [Google Scholar] [CrossRef]
- Marsh, H.W.; Balla, J.R.; Hau, K.T. An evaluation of incremental fit indices: A clarification of mathematical and empirical properties. In Advanced Structural Equation Modeling Techniques; Marcoulides, G.A., Schumacker, R.E., Eds.; Psychology Press: Mahwah, NJ, USA, 1996; pp. 315–353. [Google Scholar]
- Cangur, S.; Ercan, I. Comparison of model fit indices used in structural equation modeling under multivariate normality. J. Mod. Appl. Stat. Methods 2015, 14, 14. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Steiger, J.H. Understanding the limitations of global fit assessment in structural equation modeling. Personal. Individ. Differ. 2007, 42, 893–898. [Google Scholar] [CrossRef]
- Fabrigar, L.R.; MacCallum, R.C.; Wegener, D.T.; Strahan, E.J. Evaluating the use of exploratory factor analysis in psychological research. Psychol. Methods 1999, 4, 272–299. [Google Scholar] [CrossRef]
- Abu-Bader, S.; Jones, T.V. Statistical mediation analysis using the sobel test and hayes SPSS process macro. Int. J. Quant. Qual. Res. Methods 2021, 9, 42–61. [Google Scholar]
- Sobel, M.E. Asymptotic intervals for indirect effects in structural equations models. In Sociological Methodology; Leinhart, S., Ed.; Jossey-Bass: San Francisco, CA, USA, 1982; pp. 290–312. [Google Scholar]
- Arndt, C.; Davies, R.; Gabriel, S.; Harris, L.; Makrelov, K.; Robinson, S.; Levy, S.; Simbanegavi, W.; van Seventer, D.; Anderson, L. COVID-19 lockdowns, income distribution, and food security: An analysis for South Africa. Glob. Food Secur. 2020, 26, 100410. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.; Lin, W.; Li, N.; Wen, Y.; Wang, Y.; Jiang, W.; Zhang, J.; Zhong, H.; Chen, X.; Luo, W.; et al. Electroencephalography (EEG)-Based Neural Emotional Response to the Vegetation Density and Integrated Sound Environment in a Green Space. Forests 2021, 12, 1380. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, M. Electroencephalogram Application for the Analysis of Stress Relief in the Seasonal Landscape. Int. J. Environ. Res. Public Health 2021, 18, 8522. [Google Scholar] [CrossRef] [PubMed]
- Olszewska-Guizzo, A.; Escoffier, N.; Chan, J.; Puay Yok, T. Window view and the brain: Effects of floor level and green cover on the alpha and beta rhythms in a passive exposure EEG experiment. Int. J. Environ. Res. Public Health 2018, 15, 2358. [Google Scholar] [CrossRef] [Green Version]
- Bae, Y.M.; Lee, Y.; Kim, S.M.; Piao, Y.H. A comparative study on the forest therapy policies of Japan and Korea. J. Korean Soc. For. Sci. 2014, 103, 299–306. [Google Scholar] [CrossRef] [Green Version]
- Chopdar, P.K.; Paul, J.; Prodanova, J. Mobile shoppers’ response to COVID-19 phobia, pessimism and smartphone addiction: Does social influence matter? Technol. Forecast. Soc. Change 2022, 174, 121249. [Google Scholar] [CrossRef]
- Elhai, J.D.; Yang, H.; McKay, D.; Asmundson, G.J. COVID-19 anxiety symptoms associated with problematic smartphone use severity in Chinese adults. J. Affect. Disord. 2020, 274, 576–582. [Google Scholar] [CrossRef]
- Limone, P.; Toto, G.A. Psychological and emotional effects of Digital Technology on Children in COVID-19 Pandemic. Brain Sci. 2021, 11, 1126. [Google Scholar] [CrossRef]
- Daglis, T. The Increase in Addiction during COVID-19. Encyclopedia 2021, 1, 1257–1266. [Google Scholar] [CrossRef]
- David, M.E.; Roberts, J.A. Smartphone Use during the COVID-19 Pandemic: Social Versus Physical Distancing. Int. J. Environ. Res. Public Health 2021, 18, 1034. [Google Scholar] [CrossRef]
- Nathan, A.; George, P.; Ng, M.; Wenden, E.; Bai, P.; Phiri, Z.; Christian, H. Impact of COVID-19 Restrictions on Western Australian Children’s Physical Activity and Screen Time. Int. J. Environ. Res. Public Health 2021, 18, 2583. [Google Scholar] [CrossRef] [PubMed]
- García-Tascón, M.; Sahelices-Pinto, C.; Mendaña-Cuervo, C.; Magaz-González, A.M. The impact of the COVID-19 confinement on the habits of PA practice according to gender (male/female): Spanish case. Int. J. Environ. Res. Public Health 2020, 17, 6961. [Google Scholar] [CrossRef] [PubMed]
- Rice, W.L.; Mateer, T.; Taff, B.D.; Lawhon, B.; Reigner, N.; Newman, P. Longitudinal Changes in the Outdoor Recreation Community’s Reaction to the COVID-19 Pandemic: Final Report on a Three-Phase National Survey of Outdoor Enthusiasts. SocArXiv Gnjcy Cent. Open Sci. 2020, 1–10. [Google Scholar] [CrossRef]
- Yamori, K.; Goltz, J.D. Disasters without Borders: The Coronavirus Pandemic, Global Climate Change and the Ascendancy of Gradual Onset Disasters. Int. J. Environ. Res. Public Health 2021, 18, 3299. [Google Scholar] [CrossRef]
- Venter, Z.S.; Barton, D.N.; Gundersen, V.; Figari, H.; Nowell, M. Urban nature in a time of crisis: Recreational use of green space increases during the COVID-19 outbreak in Oslo, Norway. Environ. Res. Lett. 2020, 15, 104075. [Google Scholar] [CrossRef]
- Newhouse, N. Implications of attitude and behavior research for environmental conservation. J. Environ. Educ. 1990, 22, 26–32. [Google Scholar] [CrossRef]
- Soga, M.; Gaston, K.J. Extinction of experience: The loss of human–nature interactions. Front. Ecol. Environ. 2016, 14, 94–101. [Google Scholar] [CrossRef] [Green Version]
- Wolsko, C.; Lindberg, K. Experiencing connection with nature: The matrix of psychological well-being, mindfulness, and outdoor recreation. Ecopsychology 2013, 5, 80–91. [Google Scholar] [CrossRef]
- Kim, D.; Avenzora, R.; Lee, J.H. Exploring the Outdoor Recreational Behavior and New Environmental Paradigm among Urban Forest Visitors in Korea, Taiwan, and Indonesia. Forests 2021, 12, 1651. [Google Scholar] [CrossRef]
- Lee, J.H.; Lee, D.J. Nature experience, recreation activity and health benefits of visitors in mountain and urban forests in Vienna, Zurich and Freiburg. J. Mt. Sci. 2015, 12, 1551–1561. [Google Scholar] [CrossRef]
- Kotera, Y.; Richardson, M.; Sheffield, D. Effects of Shinrin-Yoku (Forest Bathing) and Nature Therapy on Mental Health: A Systematic Review and Meta-analysis. Int. J. Ment. Health Addict. 2020, 20, 337–361. [Google Scholar] [CrossRef]
- Shin, W.S.; Yeoun, P.S.; Yoo, R.W.; Shin, C.S. Forest experience and psychological health benefits: The state of the art and future prospect in Korea. Environ. Health Prev. Med. 2010, 15, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, K.H.; Shin, W.S.; Khil, T.G.; Kim, D.J. Six-step model of nature-based therapy process. Int. J. Environ. Res. Public Health 2020, 17, 685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebenberger, M.; Arnberger, A. Exploring visual preferences for structural attributes of urban forest stands for restoration and heat relief. Urban For. Urban Green. 2019, 41, 272–282. [Google Scholar] [CrossRef]
- Nilsson, K.; Sangster, M.; Gallis, C.; Hartig, T.; De Vries, S.; Seeland, K.; Schipperijn, J. (Eds.) Forests, Trees and Human Health; Springer Science & Business Media: New York, NY, USA; Dordrecht, The Netherlands; Heidelberg, Germany; London, UK, 2010; 427p. [Google Scholar]
- Park, B.J.; Shin, C.S.; Shin, W.S.; Chung, C.Y.; Lee, S.H.; Kim, D.J.; Kim, Y.H.; Park, C.E. Effects of forest therapy on health promotion among middle-aged women: Focusing on physiological indicators. Int. J. Environ. Res. Public Health 2020, 17, 4348. [Google Scholar] [CrossRef]
- Arnberger, A.; Eder, R.; Allex, B.; Ebenberger, M.; Hutter, H.P.; Wallner, P.; Bauer, N.; Zaller, J.G.; Frank, T. Health-related effects of short stays at mountain meadows, a river and an urban site—Results from a field experiment. Int. J. Environ. Res. Public Health 2018, 15, 2647. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Park, D.B.; Seo, J.I. Exploring the Relationship between Forest Structure and Health. Forests 2020, 11, 1264. [Google Scholar] [CrossRef]
- Sacchelli, S.; Grilli, G.; Capecchi, I.; Bambi, L.; Barbierato, E.; Borghini, T. Neuroscience application for the analysis of cultural ecosystem services related to stress relief in forest. Forests 2020, 11, 190. [Google Scholar] [CrossRef] [Green Version]
- Ohe, Y.; Ikei, H.; Song, C.; Miyazaki, Y. Evaluating the relaxation effects of emerging forest-therapy tourism: A multidisciplinary approach. Tour. Manag. 2017, 62, 322–334. [Google Scholar] [CrossRef]
- Hong, J.Y.; Lee, J.H. Analysis of Electroencephalogram and Electrocardiogram Changes in Adults in National Healing Forests Environment. J. People Plants Environ. 2018, 21, 575–589. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.S.; Kim, J.; Khil, T.; Yi, J.; Kim, D.J. Effects of the Forest Healing Program on Depression, Cognition, and the Autonomic Nervous System in the Elderly with Cognitive Decline. J. People Plants Environ. 2021, 24, 107–117. [Google Scholar] [CrossRef]
- Yu, Y.M.; Lee, Y.J.; Kim, J.Y.; Yoon, S.B.; Shin, C.S. Effects of forest therapy camp on quality of life and stress in postmenopausal women. For. Sci. Technol. 2016, 12, 125–129. [Google Scholar] [CrossRef]
- Jung, W.H.; Woo, J.M.; Ryu, J.S. Effect of a forest therapy program and the forest environment on female workers’ stress. Urban For. Urban Green. 2015, 14, 274–281. [Google Scholar] [CrossRef]
- Lee, M.M.; Park, B.J. Effects of Forest Healing Program on Depression, Stress and Cortisol Changes of Cancer Patients. J. People Plants Environ. 2020, 23, 245–254. [Google Scholar] [CrossRef]
- Li, Q.; Kobayashi, M.; Kumeda, S.; Ochiai, T.; Miura, T.; Kagawa, T.; Imai, M.; Wang, Z.; Otsuka, T.; Kawada, T. Effects of forest bathing on cardiovascular and metabolic parameters in middle-aged males. Evid-Based Complementary Altern. Med. 2016, 2016, 2587381. [Google Scholar] [CrossRef] [PubMed]
- Ideno, Y.; Hayashi, K.; Abe, Y.; Ueda, K.; Iso, H.; Noda, M.; Lee, J.S.; Suzuki, S. Blood pressure-lowering effect of Shinrin-yoku (Forest bathing): A systematic review and meta-analysis. BMC Complementary Altern. Med. 2017, 17, 409. [Google Scholar] [CrossRef]
- Baek, J.E.; Shin, H.J.; Kim, S.H.; Kim, J.Y.; Park, S.; Sung, S.Y.; Cho, H.-Y.; Hahm, S.C.; Lee, M.G. The Effects of Forest Healing Anti-aging Program on Physical Health of the Elderly: A Pilot Study. Korean Soc. Phys. Med. 2021, 16, 81–90. [Google Scholar] [CrossRef]
- Kim, T.; Song, B.; Cho, K.S.; Lee, I.S. Therapeutic potential of volatile terpenes and terpenoids from forests for inflammatory diseases. Int. J. Mol. Sci. 2020, 21, 2187. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Kim, S.; Kim, G.; Choi, Y.; Kim, E.; Paek, D. Evidence-Based Status of Forest Healing Program in South Korea. Int. J. Environ. Res. Public Health 2021, 18, 10368. [Google Scholar] [CrossRef]
- Dolling, A.; Nilsson, H.; Lundell, Y. Stress recovery in forest or handicraft environments–An intervention study. Urban For. Urban Green. 2017, 27, 162–172. [Google Scholar] [CrossRef]
- Kim, J.G.; Khil, T.G.; Lim, Y.; Park, K.; Shin, M.; Shin, W.S. The psychological effects of a campus forest therapy program. Int. J. Environ. Res. Public Health 2020, 17, 3409. [Google Scholar] [CrossRef] [PubMed]
- Bielinis, E.; Jaroszewska, A.; Łukowski, A.; Takayama, N. The effects of a forest therapy programme on mental hospital patients with affective and psychotic disorders. Int. J. Environ. Res. Public Health 2020, 17, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doimo, I.; Masiero, M.; Gatto, P. Forest and wellbeing: Bridging medical and forest research for effective forest-based initiatives. Forests 2020, 11, 791. [Google Scholar] [CrossRef]
- Naomi, A.S. Access to Nature Has Always Been Important; with COVID-19, it Is Essential. HERD Health Environ. Res. Des. J. 2020, 13, 242–244. [Google Scholar] [CrossRef]
- Tomita, A.; Vandormael, A.M.; Cuadros, D.; Di Minin, E.; Heikinheimo, V.; Tanser, F.; Slotow, R.; Burns, J.K. Green environment and incident depression in South Africa: A geospatial analysis and mental health implications in a resource-limited setting. Lancet Planet. Health 2017, 1, e152–e162. [Google Scholar] [CrossRef]
- Nawrath, M.; Guenat, S.; Elsey, H.; Dallimer, M. Exploring uncharted territory: Do urban greenspaces support mental health in low-and middle-income countries? Environ. Res. 2021, 194, 110625. [Google Scholar] [CrossRef]
- Brode, N. 15% of Americans Plan to Hike More than Usual Due to COVID-19. Civic Science. Available online: https://civicscience.com/how-americans-are-fighting-cabin-fever/ (accessed on 4 February 2022).
- Smith, T.D.; Yu, Z.; Le, A.B. An examination of work interference with family using data from a representative sample of workers participating in the general social survey and NIOSH quality of worklife module. J. Fam. Issues 2020, 41, 2356–2376. [Google Scholar] [CrossRef]
- Amichai-Hamburger, Y.; Hayat, Z. The impact of the Internet on the social lives of users: A representative sample from 13 countries. Comput. Hum. Behav. 2011, 27, 585–589. [Google Scholar] [CrossRef]
- Banerjee, S.; Galizzi, M.M.; Hortala-Vallve, R. Trusting the trust game: An external validity analysis with a UK representative sample. Games 2021, 12, 66. [Google Scholar] [CrossRef]
- Gamil, Y.; Alhagar, A. The impact of pandemic crisis on the survival of construction industry: A case of COVID-19. Mediterr. J. Soc. Sci. 2020, 11, 122. [Google Scholar] [CrossRef]
- Gursoy, D.; Chi, C.G. Effects of COVID-19 pandemic on hospitality industry: Review of the current situations and a research agenda. J. Hosp. Mark. Manag. 2020, 29, 527–529. [Google Scholar] [CrossRef]
- Laing, T. The economic impact of the Coronavirus 2019 (COVID-2019): Implications for the mining industry. Extr. Ind. Soc. 2020, 7, 580–582. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Abdelmaksoud, A.; Jafferany, M.; Lotti, T.; Sadoughifar, R.; Goldust, M. COVID-19 and economy. Dermatol. Ther. 2020, 33, e13329. [Google Scholar] [CrossRef] [PubMed]
- Shankar, K. The impact of COVID-19 on IT services industry-expected transformations. Br. J. Manag. 2020, 31, 450. [Google Scholar] [CrossRef]
- Bizoza, A.; Sibomana, S. Indicative socio-economic impacts of the novel coronavirus (COVID-19) outbreak in Eastern Africa: Case of Rwanda. SSRN 2020, 3586622, 1–23. [Google Scholar] [CrossRef]

| Country, Surveyed Area | Forested Area (% of Land Surface) | Population (×1000) | GDP Growth Rates | GDP/ People ($) | Survey Respondents | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total (Pers.) | Female (%) | Age (%) | ||||||||||
| ′19 | ′20 | ′21 | ~29 | ~39 | ~49 | 50~ | ||||||
| Malawi, Lilongwe | 22,417 sq.km (23.7%) | 19,129 | 5.5 | 0.9 | 2.2 | 636 | 95 | 46.3 | 29.5 | 43.2 | 25.3 | 2.1 |
| Rwanda, Kigali | 2760 sq.km (11.1%) | 12,952 | 10.1 | 3.5 | 6.7 | 797 | 65 | 47.6 | 73.8 | 16.9 | 3.1 | 5.2 |
| South Africa, Pretoria | 170,500 sq.km (14.0%) | 59,308 | 0.2 | −5.8 | 4.0 | 5655 | 94 | 42.5 | 39.4 | 26.6 | 26.6 | 7.4 |
| Tanzania, Dodoma | 457,450 sq.km (51.6%) | 59,734 | 6.3 | 2.0 | 4.6 | 1076 | 74 | 37.8 | 12.2 | 48.6 | 39.2 | 0.0 |
| Zambia, Lusaka | 448,140 sq.km (60.2%) | 18,383 | 1.5 | −3.5 | 2.3 | 985 | 102 | 51.9 | 8.8 | 39.2 | 48.0 | 3.9 |
| Category | Items (Since COVID-19, …) | Var. | Cronbach’s α | ||||
|---|---|---|---|---|---|---|---|
| MA | RW | SA | TA | ZA | |||
| Stress level | I am unsatisfied with the restricted daily life (activity, visitation, work, school). | ST1 | 0.826 | 0.860 | 0.831 | 0.801 | 0.878 |
| I am unsatisfied with limited communication opportunities with other people. | ST2 | ||||||
| It has decreased communication with other people (except family). | ST3 | ||||||
| It has increased the communication with my family. * | ST4 | ||||||
| Indoor activity | I don’t have enough leisure activities. | ID1 | 0.821 | 0.792 | 0.803 | 0.841 | 0.862 |
| The screen time for visiting websites and watching TV has increased. | ID2 | ||||||
| I prefer online activities to be offline (shopping, learning, communicating, etc.). | ID3 | ||||||
| Appreciation of urban forests | I get a positive feeling when I visit urban forests. * | PR1 | 0.793 | 0.774 | 0.836 | 0.810 | 0.775 |
| It became more challenging to go to the outdoor natural environment in urban forests. | PR2 | ||||||
| I love to experience the outdoor nature around me, particularly during the pandemic. * | PR3 | ||||||
| Perception of health recovery in nature | Through nature experience in the urban forest, I felt my mental recovery. * | HE1 | 0.786 | 0.797 | 0.775 | 0.852 | 0.784 |
| Through nature experience in the urban forest, I felt my body recover. * | HE2 | ||||||
| Country | Malawi | Rwanda | South Africa | Tanzania | Zambia |
|---|---|---|---|---|---|
| Month | January–June | January–June | January–June | January–June | January–June |
| School Workplace Public events Gathering Transport Stay at home Movement Travel abroad Mask |  |  |  |  |  |
 no data;
no data;  recommended;
recommended;  subnational only;
subnational only;  national.
national.| Visit Frequency | Staying Time | Transport Time | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Month | January | June | t-value | January | June | t-value | January | June | t-value |
| Malawi | 2.61 | 2.15 | 3.009 ** | 3.07 | 3.51 | −2.993 ** | 3.66 | 3.96 | −3.243 ** |
| Rwanda | 3.66 | 2.38 | 6.022 *** | 3.48 | 2.48 | 4.309 *** | 3.49 | 3.00 | 2.075 * |
| South Africa | 2.77 | 2.34 | 4.535 *** | 2.71 | 1.96 | 5.647 *** | 3.06 | 2.98 | 1.051 |
| Tanzania | 3.44 | 2.00 | 8.021 *** | 2.97 | 2.00 | 7.083 *** | 3.16 | 3.49 | −2.042 * |
| Zambia | 3.32 | 2.59 | 4.630 *** | 3.25 | 2.67 | 4.338 *** | 3.48 | 3.27 | 1.902 |
| Average | 3.11 | 2.30 | 11.110 *** | 3.08 | 2.55 | 7.214 *** | 3.37 | 3.35 | 0.350 |
| Stress Level | Indoor Activity | Appreciation of Urban Forests | Perception of Health Recovery | |
|---|---|---|---|---|
| Malawi | 3.74 ± 0.39 | 4.10 ± 0.28 a,b | 3.51 ± 0.36 | 3.81 ± 0.40 b |
| Rwanda | 3.70 ± 0.42 | 3.89 ± 0.46 b | 3.62 ± 0.45 | 3.80 ± 0.47 b |
| South Africa | 3.82 ± 0.48 | 3.80 ± 0.46 b | 3.74 ± 0.43 | 3.93 ± 0.42 a,b |
| Tanzania | 3.93 ± 0.38 | 3.99 ± 0.40 a,b | 3.61 ± 0.48 | 4.23 ± 0.40 a |
| Zambia | 3.57 ± 0.44 | 4.29 ± 0.39 a | 3.54 ± 0.48 | 4.05 ± 0.48 a,b |
| F-value | 2.042 | 4.895 | 0.968 | 3.450 |
| p-value | 0.088 | 0.001 | 0.425 | 0.009 |
| Category | Variables | Malawi | Rwanda | South Africa | Tanzania | Zambia | |
|---|---|---|---|---|---|---|---|
| Stress level | ß-coeff. | ST1 | 0.708 | 0.912 | 0.675 | 0.875 | 0.852 |
| ST2 | 0.695 | 0.704 | 0.762 | 0.958 | 0.967 | ||
| ST3 | 0.683 | 0.834 | 0.828 | 0.509 | 0.788 | ||
| ST4 | 0.890 | 0.716 | 0.718 | 0.486 | 0.616 | ||
| CR | 0.840 | 0.855 | 0.813 | 0.829 | 0.879 | ||
| AVE | 0.571 | 0.599 | 0.522 | 0.569 | 0.651 | ||
| Indoor activity | ß-coeff. | ID1 | 0.753 | 0.573 | 0.554 | 0.720 | 0.762 |
| ID2 | 0.787 | 0.716 | 0.913 | 0.993 | 0.884 | ||
| ID3 | 0.792 | 0.910 | 0.831 | 0.753 | 0.827 | ||
| CR | 0.890 | 0.735 | 0.797 | 0.879 | 0.879 | ||
| AVE | 0.729 | 0.509 | 0.577 | 0.713 | 0.709 | ||
| Appreciation of urban forests | ß-coeff. | PR1 | 0.631 | 0.628 | 0.864 | 0.674 | 0.756 |
| PR2 | 0.611 | 0.849 | 0.779 | 0.678 | 0.770 | ||
| PR3 | 0.998 | 0.735 | 0.757 | 0.976 | 0.673 | ||
| CR | 0.833 | 0.760 | 0.839 | 0.800 | 0.731 | ||
| AVE | 0.635 | 0.519 | 0.635 | 0.580 | 0.506 | ||
| Health recovery perception | ß-coeff. | HE1 | 0.729 | 0.894 | 0.772 | 0.942 | 0.742 |
| HE2 | 0.937 | 0.743 | 0.830 | 0.794 | 0.869 | ||
| CR | 0.843 | 0.787 | 0.732 | 0.890 | 0.851 | ||
| AVE | 0.732 | 0.651 | 0.578 | 0.803 | 0.742 | ||
| Model fit summary | Chi2 | 103.768 | 60.609 | 92.394 | 137.957 | 136.846 | |
| P-level | 0.000 | 0.105 | 0.000 | 0.000 | 0.000 | ||
| GFI | 0.860 | 0.865 | 0.877 | 0.791 | 0.822 | ||
| AGFI | 0.773 | 0.781 | 0.801 | 0.740 | 0.790 | ||
| NFI | 0.810 | 0.858 | 0.840 | 0.846 | 0.815 | ||
| IFI | 0.888 | 0.967 | 0.916 | 0.918 | 0.872 | ||
| TLI | 0.840 | 0.952 | 0.910 | 0.894 | 0.881 | ||
| CFI | 0.884 | 0.965 | 0.913 | 0.912 | 0.916 | ||
| RMSEA | 0.071 | 0.054 | 0.056 | 0.051 | 0.063 |
| Hypothesis: Direction | Malawi | Rwanda | South Africa | Tanzania | Zambia | |
|---|---|---|---|---|---|---|
| H1a: Stress level → | Appreciation of urban forests | Reject | Accept | Accept | Reject | Accept |
| H1b: Indoor activity → | Appreciation of urban forests | Reject | Accept | Reject | Reject | Accept |
| H2: Appreciation of urban forests → | Perception of health recovery | Accept | Accept | Accept | Reject | Accept |
| Indirect Effect | Malawi | Rwanda | South Africa | Tanzania | Zambia | |
|---|---|---|---|---|---|---|
| Stress level → Urban forest → Health | Z-value | 0.850 | 2.363 | 1.909 | 0.152 | 2.576 |
| p | 0.197 | 0.009 | 0.028 | 0.439 | 0.004 | |
| Indoor activity → Urban forest → Health | Z-value | 0.657 | 2.226 | 0.667 | 0.713 | 1.806 |
| p | 0.255 | 0.013 | 0.252 | 0.237 | 0.035 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-h.; Mkandawire, M.; Niyigena, P.; Xotyeni, A.; Itamba, E.; Siame, S. Impact of COVID-19 Lock-Downs on Nature Connection in Southern and Eastern Africa. Land 2022, 11, 872. https://doi.org/10.3390/land11060872
Lee J-h, Mkandawire M, Niyigena P, Xotyeni A, Itamba E, Siame S. Impact of COVID-19 Lock-Downs on Nature Connection in Southern and Eastern Africa. Land. 2022; 11(6):872. https://doi.org/10.3390/land11060872
Chicago/Turabian StyleLee, Ju-hyoung, Madalitso Mkandawire, Patrick Niyigena, Abonisiwe Xotyeni, Edwin Itamba, and Sylvester Siame. 2022. "Impact of COVID-19 Lock-Downs on Nature Connection in Southern and Eastern Africa" Land 11, no. 6: 872. https://doi.org/10.3390/land11060872