Statistical Modelling of Temperature-Attributable Deaths in Portuguese Metropolitan Areas under Climate Change: Who Is at Risk?



Abstract
:1. Introduction
2. Data and Methods
2.1. Mortality Data
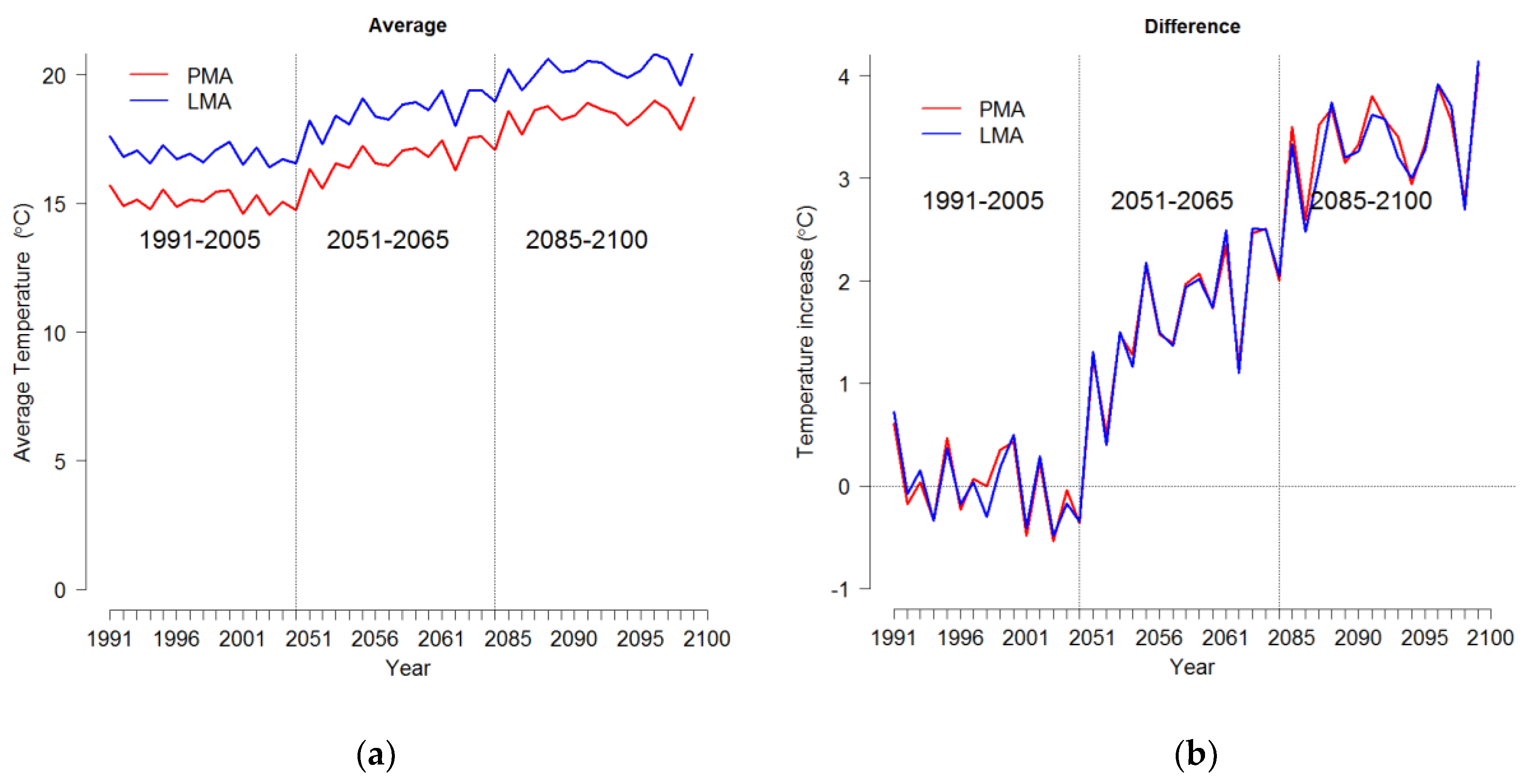
2.2. Temperature Projections
2.3. Statistical Approach
2.3.1. Estimation of Temperature-Mortality Association
2.3.2. Attributable Risk from DLNMs
2.3.3. Projection of Temperature-Mortality Association
2.4. Model Assessment and Sensitivity Analysis
3. Results
3.1. Descriptive Statistics
3.2. Temperature-Mortality Association
3.3. Projected Exposure and Health Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rodrigues, M.; Santana, P.; Rocha, A. Effects of extreme temperatures on cerebrovascular mortality in Lisbon: A distributed lag non-linear model. Int. J. Biometerol. 2019, 63, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Guo, Y.; Sera, F.; Vicedo-Cabrera, A.M.; Huber, V.; Tong, S.; Coelho, M.S.Z.S.; Saldiva, P.H.N.; Lavigne, E.; Correa, P.M.; et al. Projections of temperature-related excess mortality under climate change scenarios. Lancet Planet Health 2017, 19, e360–e367. [Google Scholar] [CrossRef]
- Petkova, E.; Horton, R.; Bader, D.; Kinney, P. Projected Heat-Related Mortality in the U.S. Urban Northeast. Int. J. Environ. Res. Public Health 2013, 10, 6734–6747. [Google Scholar] [CrossRef] [PubMed]
- Achebak, H.; Devolder, D.; Ballester, J. Trends in temperature-related age-specific and sex-specific mortality from cardiovascular diseases in Spain: A national time-series analysis. Lancet Planet. Health 2019, 3, e297–e306. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.; Ren, Z.; Zhang, Y.; Feng, B.; Lin, H.; Xiao, J.; Zeng, W.; Li, X.; Li, Z.; Rutherford, S.; et al. Modification Effects of Population Expansion, Ageing, and Adaptation on Heat-Related Mortality Risks Under Different Climate Change Scenarios in Guangzhou, China. Int. J. Environ. Res. Public Health 2019, 16, 376. [Google Scholar] [CrossRef] [Green Version]
- Qiu, H.; Tian, L.; Ho, K.F.; Yu, I.T.; Thach, T.Q.; Wong, C.M. Who is more vulnerable to death from extremely cold temperatures? A case-only approach in Hong Kong with a temperate climate. Int. J. Biometeorol. 2016, 60, 711–717. [Google Scholar]
- Li, T.T.; Horton, R.M.; Kinney, P.L. Projections of seasonal patterns in temperature-related deaths for Manhattan, New York. Nat. Clim. Chang. 2013, 3, 717–721. [Google Scholar] [CrossRef] [Green Version]
- Green, H.K.; Andrews, N.; Armstrong, B.; Bickler, G.; Pebody, R. Mortality during the 2013 heatwave in England–How did it compare to previous heatwaves? A retrospective observational study. Environ. Res. 2016, 147, 343–349. [Google Scholar] [CrossRef]
- Rodrigues, M.; Santana, P.; Rocha, A. Bootstrap approach to validate the performance of models for predicting mortality risk temperature in Portuguese metropolitan areas. Environ. Health 2019, 18, 25. [Google Scholar] [CrossRef] [Green Version]
- Benmarhnia, T.; Deguen, S.; Kaufman, J.S.; Smargiassi, A. Vulnerability to heat-related mortality: A systematic review, meta-analysis, and meta-regression analysis. Epidemiology 2015, 26, 781–793. [Google Scholar] [CrossRef]
- Marí-Dell’Olmo, M.; Tobías, A.; Gómez-Gutiérrez, A.; Rodríguez-Sanz, M.; de Olalla, P.G.; Camprubí, E.; Gasparrini, A.; Borrell, C. Social inequalities in the association between temperature and mortality in a South European context. Int. J. Public Health 2019, 64, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Almeida, S.P.; Casimiro, E.; Calheiros, J. Effects of apparent temperature on daily mortality in Lisbon and Oporto, Portugal. Environ. Health 2010, 9, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunes, A.R. General and specified vulnerability to extreme temperatures among older adults. Int. J. Environ. Health Res. 2019, 5, 1–18. [Google Scholar] [CrossRef] [PubMed]
- McKee, C. Deaths in Winter: Can Britain Learn: Can Britain learn from Europe? Eur. J. Epidemiol. 1989, 5, 178–182. [Google Scholar] [CrossRef]
- Healy, J.D. Excess winter mortality in Europe: A cross country analysis identifying key risk factors. J. Epidemiol. Community Health 2003, 57, 784–789. [Google Scholar] [CrossRef] [Green Version]
- Fowler, T.; Southgate, R.J.; Waite, T.; Harrell, R.; Kovats, S.; Bone, A.; Doyle, Y.; Murray, V. Excess winter deaths in Europe: A multi-country descriptive analysis. Eur. J. Pub. Health 2015, 25, 339–345. [Google Scholar] [CrossRef] [Green Version]
- Liddell, C.; Morris, C.; Thomson, H.; Guiney, C. Excess winter deaths in 30 European countries 1980–2013: A critical review of methods. J. Public Health 2016, 38, 806–814. [Google Scholar] [CrossRef] [Green Version]
- Paget, J.; Spreeuwenberg, P.; Charu, V. Global mortality associated with seasonal influenza epidemics: New burden estimates and predictors from the GLaMOR Project. J. Glob. Health 2019, 9, 020421. [Google Scholar] [CrossRef]
- Almendra, R.; Santana, P.; Freire, E.; Vasconcelos, J. Seasonal mortality patterns and regional contrasts in Portugal. Bull. Geogr. Socio-econ Ser. 2016, 32, 7–18. [Google Scholar] [CrossRef] [Green Version]
- Antunes, L.; Silva, S.; Marques, J. The effect of extreme cold temperatures on the risk of death in the two major Portuguese cities. Int. J. Biometeorol. 2017, 61, 127–135. [Google Scholar] [CrossRef]
- Intergovernmental Panel on Climate Change (IPCC). Climate Change 2013: The Physical Science Basis. Contribution of Working Group I to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Cambridge University Press: Cambridge, UK, 2013. [Google Scholar]
- World Health Organization—WHO. Quantitative Risk Assessment of the Effects of Climate Change on Selected Causes of Death, 2030s and 2050s; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Woodward, A.; Smith, K.; Campbell-Lendrum, D.; Chadee, D.; Honda, Y.; Liu, Q. Climate change and health: On the latest IPCC report. Lancet 2014, 383, 1185–1189. [Google Scholar] [CrossRef]
- Rosenthal, J.K.; Kinney, P.L.; Metzger, K.B. Intra-urban vulnerability to heat-related mortality in New York City, 1997–2006. Health Place 2014, 30, 45–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, J.G.; Cavan, G.; Connelly, A.; Guy, S.; Handley, J.; Kazmierczak, A. Climate change and the city: Building capacity for urban adaptation. Prog. Plan. 2015, 95, 1–66. [Google Scholar] [CrossRef]
- Balbus, J.M.; Malina, C. Identifying vulnerable subpopulations for climate change health effects in the United States. J. Occup. Environ. Med. 2009, 51, 33–37. [Google Scholar] [CrossRef]
- Wilhelmi, O.V.; Hayden, M.H. Connecting people and place: A new framework for reducing urban vulnerability to extreme heat. Environ. Res. Lett. 2010, 5, 014021. [Google Scholar] [CrossRef]
- Zanobetti, A.; O’Neill, M.S.; Gronlund, C.J.; Schwartz, J.D. Susceptibility to mortality in weather extremes: Effect modification by personal and small-area characteristics. Epidemiology 2013, 24, 809–819. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.; Lin, H.; Liu, Y. Individual-level and community level effect modifiers of the temperature-mortality relationship in 66 Chinese communities. BMJ Open 2015, 5, e009172. [Google Scholar] [CrossRef] [Green Version]
- Kamal-Chaoui, L.; Robert, A. Competitive Cities and Climate Change; OECD Regional Development: Paris, France, 2009. [Google Scholar]
- Rafael, S.; Martins, H.; Marta-Almeida, M.; Sá, E.; Coelho, S.; Rocha, A. Quantification and mapping of urban fluxes under climate change: Application of WRF-SUEWS model to Greater Porto area (Portugal). Environ. Res. 2017, 155, 321–344. [Google Scholar] [CrossRef]
- Intergovernmental Panel on Climate Change (IPCC). Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects; Cambridge University Press: Cambridge, UK, 2014; pp. 1–32. [Google Scholar]
- Marengo, J.A.; Rusticucci, M.; Penalba, O.; Renom, M. An intercomparison of observed and simulated extreme rainfall and temperature events during the last half of the twentieth century: Part 2: Historical trends. Clim. Chang. 2010, 98, 509–529. [Google Scholar] [CrossRef] [Green Version]
- Meehl, G.A.; Karl, T.; Easterling, D.R.; Changnon, S.; Pielke, R., Jr.; Changnon, D.; Evans, J.; Groisman, P.Y.; Knutson, T.R.; Kunkel, K.E.; et al. An Introduction to Trends in Extreme Weather and Climate Events: Observations, Socioeconomic Impacts, Terrestrial Ecological Impacts, and Model Projections. Bull. Am. Meteorol. Soc. 2000, 81, 413–416. [Google Scholar] [CrossRef] [Green Version]
- Easterling, D.R.; Meehl, G.A.; Parmesan, C.; Changnon, S.A.; Karl, T.R.; Mearns, L.O. Climate Extremes: Observations, Modeling, and Impacts. Science 2000, 289, 2068–2074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moberg, A.; Jones, P.D. Regional climate model simulations of daily maximum and minimum near-surface temperatures across Europe compared with observed station data 1961–1990. Clim. Dyn. 2004, 23, 695–715. [Google Scholar] [CrossRef]
- Alexander, L.V.; Zhang, X.; Peterson, T.C.; Caesar, J.; Gleason, B.; Tank, A.M.G.K.; Haylock, M.; Collins, D.; Trewin, B.; Rahimzadeh, F.; et al. Global observed changes in daily climate extremes of temperature and precipitation. J. Geophys. Res. 2006, 111, D05109. [Google Scholar] [CrossRef] [Green Version]
- Sillmann, J.; Kharin, V.V.; Zwiers, F.W.; Zhang, X.; Bronaugh, D. Climate extremes indices in the CMIP5 multimodel ensemble: Part 2. Future climate projections. J. Geophys. Res. Atmos. 2013, 118, 2473–2493. [Google Scholar] [CrossRef]
- Beniston, M.; Stephenson, D.B.; Christensen, O.B.; Ferro, C.A.T.; Frei, C.; Goyette, S.; Halsnaes, K.; Holt, T.; Jylhä, K.; Ko, B.; et al. Future extreme events in European climate: An exploration of regional model projections. Clim. Chang. 2007, 81, 71–95. [Google Scholar] [CrossRef] [Green Version]
- Tank, A.M.G.K.; Können, G.P. Trends in Indices of Daily Temperature and Precipitation Extremes in Europe, 1946–1999. J. Clim. 2003, 16, 3665–3680. [Google Scholar] [CrossRef]
- Sánchez, E.; Gallardo, C.; Gaertner, M.A.; Arribas, A.; Castro, M. Future climate extreme events in the Mediterranean simulated by a regional climate model: A first approach. Glob. Planet. Chang. 2004, 44, 163–180. [Google Scholar] [CrossRef]
- Goubanova, K.; Li, L. Extremes in temperature and precipitation around the Mediterranean basin in an ensemble of future climate scenario simulations. Glob. Planet. Chang. 2007, 57, 27–42. [Google Scholar] [CrossRef]
- Giorgi, F.; Lionello, P. Climate change projections for the Mediterranean region. Glob. Planet Chang. 2008, 63, 90–104. [Google Scholar] [CrossRef]
- Fonseca, D.; Carvalho, M.J.; Marta-Almeida, M.; Melo-Gonçalves, P.; Rocha, A. Recent trends of extreme temperature indices for the Iberian Peninsula. Phys. Chem. Earth 2016, 94, 66–76. [Google Scholar] [CrossRef]
- Gasparrini, A.; Armstrong, B. The impact of heat waves on mortality. Epidemiology 2012, 22, 68–73. [Google Scholar] [CrossRef] [Green Version]
- D’Ippoliti, D.; Michelozzi, P.; Marino, C.; de’Donato, F.; Menne, B.; Katsouyanni, K.; Kirchmayer, U.; Analitis, A.; Medina-Ramón, M.; Paldy, A.; et al. The impact of heat waves on mortality in 9 European cities: Results from the EuroHEAT project. Environ. Heal. 2010, 9, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russo, S.; Dosio, A.; Graversen, R.G.; Sillmann, J.; Carrao, H.; Dunbar, M.B.; Singleton, A.; Montagna, P.; Barbola, P.; Vogt, J.V. Magnitude of extreme heat waves in present climate and their projection in a warming world. J. Geophys. Res. Atmos. 2014, 119, 12500–12512. [Google Scholar] [CrossRef] [Green Version]
- Meehl, G.A.; Tebaldi, C. More intense, more frequent, and longer lasting heatwaves in the 21st Century. Science 2004, 305, 994–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, T.C.; Heim, R.R.; Hirsch, R.; Kaiser, D.P.; Brooks, H.; Di enbaugh, N.S.; Dole, R.M.; Giovannettone, J.P.; Guirguis, K.; Karl, T.R.; et al. Monitoring and understanding changes in heat waves, cold waves, floods, and droughts in the United States: State of knowledge. Bull. Am. Meteorol. Soc. 2013, 94, 821–834. [Google Scholar] [CrossRef] [Green Version]
- Schoetter, R.; Cattiaux, J.; Douville, H. Changes of western European heat wave characteristics projected by the CMIP5 ensemble. Clim. Dyn. 2015, 45, 1601–1616. [Google Scholar] [CrossRef]
- Bador, M.; Terray, L.; Boé, J.; Somot, S.; Alias, A.; Gibelin, A.-L.; Dubuisson, B. Future summer mega-heatwave and record-breaking temperatures in a warmer France climate. Environ. Res. Lett. 2017, 12, 074025. [Google Scholar] [CrossRef] [Green Version]
- Ouzeau, G.; Soubeyroux, J.-M.; Schneider, M.; Vautard, R.; Planton, S. Heat waves analysis over France in present and future climate: Application of a new method on the EURO-CORDEX ensemble. Clim. Serv. 2016, 4, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Lhotka, O.; Kyselý, J.; Plavcová, E. Evaluation of major heat waves’ mechanisms in EURO-CORDEX RCMs over Central Europe. Clim. Dyn. 2018, 50, 4249–4262. [Google Scholar] [CrossRef]
- Morabito, M.; Crisci, A.; Messeri, A.; Messeri, G.; Betti, G.; Orlandini, S.; Raschi, A.; Maracchi, G. Increasing Heatwave Hazards in the Southeastern European Union Capitals. Atmosphere 2017, 8, 115. [Google Scholar] [CrossRef] [Green Version]
- Pereira, S.C.; Marta-Almeida, M.; Carvalho, A.C.; Rocha, A. Heat wave and cold spell changes in Iberia for a future climate scenario. Int. J. Clim. 2017, 37, 5192–5205. [Google Scholar] [CrossRef] [Green Version]
- Viceto, C.; Cardoso Pereira, S.; Rocha, A. Climate Change Projections of Extreme Temperatures for the Iberian Peninsula. Atmosphere 2019, 10, 229. [Google Scholar] [CrossRef] [Green Version]
- Skamarock, W.C.; Klemp, J.B.; Dudhia, J.; Gill, D.O.; Barker, D.; Wang, W. A Description of the Advanced Research WRF Version 3. Available online: http://opensky.ucar.edu/islandora/object/technotes:500 (accessed on 28 June 2018).
- Giorgetta, M.; Jungclaus, J.; Reick, C.H.; Legutke, S.; Bader, J.; Bottinger, M.; Brovkin, V.; Crueger, T.; Esch, M.; Fieg, K. Climate and carbon cycle changes from 1850 to 2100 in MPI-ESM simulations for the Coupled Model Intercomparison Project phase 5. J. Adv. Model. Earth Syst. 2013, 5, 572–597. [Google Scholar] [CrossRef]
- Russo, S.; Sillmann, J.; Fischer, E.M. Top ten European heatwaves since 1950 and their occurrence in the coming decades Environ. Res. Lett. 2015, 10, 124003. [Google Scholar] [CrossRef]
- Moss, R.; Babiker, M.; Brinkman, S.; Calvo, E.; Carter, T.; Edmonds, J.; Elgizouli, I.; Emori, S.; Erda, L.; Hibbard, K.; et al. Towards New Scenarios for Analysis of Emissions, Climate Change, Impacts, and Response Strategies; Intergovernmental Panel on Climate Change (IPCC): Noordwijkerhout, The Netherlands, 2007. [Google Scholar]
- Van Vuuren, D.P.; Edmonds, J.; Kainuma, M.; Riahi, K.; Thomson, A.; Hibbard, K.; Hurtt, G.C.; Kram, T.; Krey, V.; Lamarque, J.F.; et al. The representative concentration pathways: An overview. Clim. Chang. 2011, 109, 5–31. [Google Scholar] [CrossRef]
- Wood, A.W.; Maurer, E.P.; Kumar, A.; Lettenmaier, D.P. Long-range experimental hydrologic forecasting for the eastern United States. J. Geophys. Res. 2002, 107, 4429. [Google Scholar] [CrossRef]
- Marta-Almeida, M.; Teixeira, J.C.; Carvalho, M.J.; Melo-Gonçalves, P.; Rocha, A.M. High resolution WRF climatic simulations for the Iberian Peninsula: Model validation. Phys. Chem. Earth 2016, 94, 94–105. [Google Scholar] [CrossRef]
- Saurral, R.; Montroull, N.; Camilloni, I. Development of statistically unbiased 21st century hydrology scenarios over La Plata Basin. Int. J. River Basin Manag. 2013, 11, 329–343. [Google Scholar] [CrossRef]
- Dosio, A.; Paruolo, P.; Rojas, R. Bias correction of the ENSEMBLES high resolution climate change projections for use by impact models: Analysis of the climate change signal. J. Geophys. Res. Atmos. 2012, 117, 17110. [Google Scholar] [CrossRef] [Green Version]
- Barredo, J.I.; Caudullo, G.; Dosio, A. Mediterranean habitat loss under future climate conditions: Assessing impacts on the Natura 2000 protected area network. Appl. Geogr. 2016, 75, 83–92. [Google Scholar] [CrossRef]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Distributed lag non-linear models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, M.; Santana, P.; Rocha, A. Projections of Temperature-Attributable Deaths in Portuguese Metropolitan Areas: A Time-Series Modelling Approach. Atmosphere 2019, 10, 735. [Google Scholar] [CrossRef] [Green Version]
- Casanueva, A.; Burgstall, A.; Kotlarski, S.; Messeri, A.; Morabito, M.; Flouris, A.D.; Nybo, L.; Spirig, C.; Schwierz, C. Overview of Existing Heat-Health Warning Systems in Europe. Int. J. Environ. Res. Public Health 2019, 16, 2657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravindra, K.; Rattan, P.; Mor, S.; Aggarwal, A. Generalized additive models: Building evidence of air pollution, climate change and human health. Environ. Int. 2019, 132, 104987. [Google Scholar] [CrossRef]
- Tobías, A.; Armstrong, B.; Gasparrini, A. Investigating uncertainty in the minimum mortality temperature. Epidemiology 2017, 28, 72–76. [Google Scholar] [CrossRef]
- Gasparrini, A.; Leone, M. Attributable risk from distributed lag models. BMC Med. Res. Methodol. 2014, 14, 55. [Google Scholar] [CrossRef] [Green Version]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Zanobetti, A.; Schwartz, A.; Tobias, A.; Tong, S.; Rocklöv, J.; Forsberg, B. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Gasparrini, A. Distributed Lag Linear and Non-Linear Models in R: The Package dlnm. J. Stat. Softw. 2011, 43, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Basu, R. High ambient temperature and mortality: A review of epidemiologic studies from 2001 to 2008. Environ. Health 2009, 8, 40–52. [Google Scholar] [CrossRef] [Green Version]
- Cheng, H.; Wang, M.; Li, Q.; Yagouti, A.; Lavigne, F.; Forty, R. Assessment of the effect of cold and hot temperatures on mortality in Ontario, Canada: A population-based study. CMAJ Open 2016, 4, 48–58. [Google Scholar] [CrossRef] [Green Version]
- Keatinge, W.R.; Coleshaw, S.R.; Easton, J.C. Increased platelet and red cell counts, blood viscosity, and plasma cholesterol levels during heat stress, and mortality from coronary and cerebral thrombosis. Am. J. Med. 1986, 81, 795–800. [Google Scholar] [CrossRef]
- Woodhouse, P.R.; Khaw, K.T.; Plummer, M.; Meade, T.W.; Foley, A. Seasonal variations of plasma fibrinogen and factor VII activity in the elderly: Winter infections and death from cardiovascular disease. Lancet 1994, 343, 435–439. [Google Scholar] [CrossRef]
- Mercer, J.B. Cold—an underrated risk factor for health. Environ. Res. 2003, 92, 8–13. [Google Scholar] [CrossRef]
- Keatinge, W.R.; Coleshaw, S.R.; Cotter, F.; Mattock, M.; Murphy, M.; Chelliah, R. Increases in platelet and red cell counts, blood viscosity, and arterial pressure during mild surface cooling: Factors in mortality from coronary and cerebral thrombosis in winter. Br. Med. J. 1984, 289, 1405–1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keatinge, W.R. Winter mortality and its causes. Int. J. Circumpolar. Health 2002, 61, 292–299. [Google Scholar] [CrossRef]
- Neild, P.J. Cold-induced increases in erythrocyte count, plasma cholesterol and plasma fibrinogen of elderly people without a comparable rise in protein C or factor X. Clin. Sci. 1994, 86, 43–48. [Google Scholar] [CrossRef] [Green Version]
- Ryti, N.R.I.; Guo, Y.; Jaakkola, J.J.K. Global association of cold spells and adverse health effects: A systematic review and meta-analysis. Environ. Health Perspect. 2016, 124, 12–22. [Google Scholar] [CrossRef]
- Hajat, S.; Vardoulakis, S.; Heaviside, C.; Eggen, B. Climate change effects on human health: Projections of temperature-related mortality for the UK during the 2020s, 2050s, and 2080s. J. Epidemiol. Community Health 2014, 68, 641–648. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.S.; Campbell, M.; Li, Q.; Li, G.; Auld, H.; Day, N. Differential and combined impacts of extreme temperatures and air pollution on human mortality in south-central Canada. Part II: Future estimates. Air Qual. Atmos. Health 2009, 1, 223–235. [Google Scholar] [CrossRef] [Green Version]
- Baccini, M.; Kosatsky, T.; Analitis, A.; Anderson, R.; D’Ovidio, M.; Menne, B. Impact of heat on mortality in 15 European cities: Attributable deaths under different weather scenarios. J. Epidemiol. Community Health 2011, 65, 64–70. [Google Scholar] [CrossRef]
- Åström, C.; Åström, D.O.; Andersson, C.; Ebi, K.L.; Forsberg, B. Vulnerability reduction needed to maintain current burdens of heat-related mortality in a changing climate—magnitude and determinants. Int. J. Environ. Res. Public Health 2017, 14, 741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santamouris, M. Recent Progress on Urban Overheating and Heat Island Research. Integrated Assessment of the Energy, Environmental, Vulnerability and Health Impact Synergies with the Global Climate Change. Energy Build. 2019, 207, 109482. [Google Scholar] [CrossRef]
- Estrada, F.; Botzen, W.J.W.; Tol, R.S.J. A global economic assessment of city policies to reduce climate change impacts. Nat. Clim. Chang. 2017, 7, 403–406. [Google Scholar] [CrossRef] [Green Version]
- Pietrapertosa, F.; Salvia, M.; Hurtado, S.D.G.; d’Alonzo, V.; Church, J.M.; Geneletti, D.; Reckien, D. Urban climate change mitigation and adaptation planning: Are Italian cities ready? Cities 2019, 91, 93–105. [Google Scholar] [CrossRef]
- Kinney, P.L.; O’Neill, M.S.; Bell, M.L.; Schwartz, J. Approaches for estimating effects of climate change on heat-related deaths: Challenges and opportunities Environ. Sci. Policy 2008, 11, 87–96. [Google Scholar] [CrossRef]
- Knowlton, K.; Lynn, B.; Goldberg, R.A.; Rosenzweig, C.; Hogrefe, C.; Rosenthal, J.K.; Kinney, P.L. Projecting heat-related mortality impacts under a changing climate in the New York City region. Am. J. Public Health 2007, 97, 2028–2034. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metropolitan Area/Age | Season | Mean ± SD | Min. | Percentiles | Max. | ||
|---|---|---|---|---|---|---|---|
| P25 | P50 | P75 | |||||
| All ages | |||||||
| LMA | Total | 29.13 ± 8.54 | 8.0 | 23 | 28 | 34 | 88 |
| Summer | 24.36 ± 6.29 | 8.0 | 20 | 24 | 28 | 88 | |
| Winter | 35.32 ± 8.79 | 11 | 29 | 35 | 41 | 71 | |
| PMA | Total | 13.58 ± 4.75 | 3.0 | 10 | 13 | 16 | 36 |
| Summer | 11.41 ± 3.59 | 3.0 | 9.0 | 11 | 14 | 27 | |
| Winter | 16.57 ± 5.01 | 3.0 | 13 | 16 | 20 | 36 | |
| Age < 65 years | |||||||
| LMA | Total | 3.79 ± 2.11 | 0.0 | 2.0 | 4.0 | 5.0 | 14 |
| Summer | 3.43 ± 1.95 | 0.0 | 2.0 | 3.0 | 5.0 | 11 | |
| Winter | 4.34 ± 2.38 | 0.0 | 3.0 | 4.0 | 6.0 | 14 | |
| PMA | Total | 1.70 ± 1.41 | 0.0 | 1.0 | 1.0 | 3.0 | 10 |
| Summer | 1.51 ± 1.29 | 0.0 | 1.0 | 1.0 | 2.0 | 7 | |
| Winter | 1.98 ± 1.54 | 0.0 | 1.0 | 2.0 | 3.0 | 10 | |
| Age 65+ years | |||||||
| LMA | Total | 25.34 ± 7.84 | 7.0 | 20 | 24 | 30 | 78 |
| Summer | 20.96 ± 5.73 | 7.0 | 17 | 21 | 24 | 78 | |
| Winter | 31.70 ± 7.65 | 13 | 26 | 31 | 36 | 65 | |
| PMA | Total | 11.87 ± 4.35 | 1.0 | 9.0 | 11 | 14 | 33 |
| Summer | 9.90 ± 3.33 | 1.0 | 8.0 | 10 | 12 | 23 | |
| Winter | 14.62 ± 4.62 | 2.0 | 11 | 14 | 18 | 33 | |
| Metropolitan Area | Season | Mean | SD | Min. | Percentiles | Max. | |||
|---|---|---|---|---|---|---|---|---|---|
| P1 | P2.5 | P97.5 | P99 | ||||||
| LMA | Total | 16.90 | 4.80 | 3.20 | 10.80 | 13.30 | 26.51 | 28.20 | 34.00 |
| Summer | 21.81 | 2.86 | 16.10 | 18.50 | 19.60 | 28.60 | 29.77 | 34.00 | |
| Winter | 12.72 | 3.42 | 3.20 | 8.80 | 10.60 | 21.60 | 23.39 | 30.20 | |
| PMA | Total | 15.09 | 4.42 | 1.00 | 9.40 | 11.80 | 24.00 | 26.50 | 31.50 |
| Summer | 19.48 | 2.84 | 12.90 | 16.30 | 17.60 | 26.80 | 28.27 | 31.50 | |
| Winter | 11.10 | 2.64 | 1.00 | 7.60 | 9.20 | 15.80 | 16.60 | 18.40 | |
| MA/Ages | Summer Temperature (99%) | logRR | 95% CI | Winter Temperature (1%) | logRR | 95% CI | ||
| Low | High | Low | High | |||||
| All ages Lisbon | 29.77 | 0.09 | −0.02 | 0.19 | 5.80 | 0.64 | −0.23 | 1.52 |
| Porto | 28.27 | 0.14 | −0.77 | 1.05 | 5.20 | 1.51 | −1.10 | 4.13 |
| Age < 65 years | ||||||||
| Lisbon | 29.77 | 0.20 | 0.00 | 0.60 | 5.80 | 0.32 | −2.09 | 1.64 |
| Porto | 28.27 | 0.80 | 0.01 | 1.59 | 5.20 | 1.45 | −1.30 | 4.22 |
| Age 65+ years | ||||||||
| Lisbon | 29.77 | 0.05 | −0.04 | 0.15 | 5.80 | 0.72 | −0.21 | 1.64 |
| Porto | 28.27 | 0.14 | −0.84 | 1.12 | 5.20 | 2.17 | −1.29 | 5.65 |
| Summer Temperature (Maximum) | logRR | 95% CI | Winter Temperature (Minimum) | logRR | 95% CI | |||
| Low | High | Low | High | |||||
| All ages Lisbon | 34.00 | 2.03 | 0.15 | 3.93 | 3.20 | 5.34 | 1.96 | 8.92 |
| Porto | 31.50 | 1.06 | 0.42 | 2.14 | 1.00 | 1.65 | −0.70 | 4.01 |
| Age < 65 years | ||||||||
| Lisbon | 34.00 | 1.07 | −4.12 | 6.27 | 3.20 | 4.47 | 0.74 | 8.21 |
| Porto | 31.50 | 0.03 | −9.09 | 9.14 | 1.00 | 1.77 | −1.54 | 3.1 |
| Age 65+ years | ||||||||
| Lisbon | 34.00 | 2.18 | 0.19 | 4.17 | 3.20 | 7.14 | 4.06 | 18.42 |
| Porto | 31.50 | 1.02 | 0.04 | 1.34 | 1.00 | 4.37 | 1.52 | 16.22 |
| Metropolitan Area/Age | Period | Extreme Cold | Extreme Heat |
|---|---|---|---|
| LMA | |||
| All ages | |||
| All year | 2051–2065 | −0.55 ( −0.71 to −0.40) | 1.04 (0.55 to 1.47) |
| 2085–2099 | −0.45 (−0.57 to −0.33) | 0.44 (0.19 to 0.67) | |
| Summer 1 | 2051–2065 | 1.58 (0.75 to 1.90) | |
| 2085–2099 | 0.10 (0.04 to 0.14) | ||
| Winter 2 | 2051–2065 | −0.67 (−1.19 to 0.59) | |
| 2085–2099 | 0.79 (−1.39 to 0.69) | ||
| <65 years | |||
| Summer 1 | 2051–2065 | 0.08 (0.11 to 0.21) | |
| 2085–2099 | 1.38 (1.67 to 2.37) | ||
| Winter 2 | 2051–2065 | −1.15 (−3.11 to 49.01) | |
| 2085–2099 | −1.39 (−3.76 to 53.11) | ||
| 65+ years | |||
| Summer 1 | 2051–2065 | 0.10 (0.00 to 0.18) | |
| 2085–2099 | 2.22 (0.11 to 1.82) | ||
| Winter 2 | 2051–2065 | −1.41 (−2.53 to 1.50) | |
| 2085–2099 | −1.67 (−3.05 to 1.10) | ||
| PMA | |||
| All ages | |||
| All year | 2051–2065 | −0.49 (−1.00 to 0.05) | 0.39 (−0.14 to 0.88) |
| 2085–2099 | −0.31 (−0.57 to −0.01) | 0.14 (−0.10 to 0.37) | |
| Summer 1 | 2051–2065 | 0.08 (−0.24 to 0.21) | |
| 2085–2099 | 0.57 (−1.10 to 1.15) | ||
| Winter 2 | 2051–2065 | −1.13 (−1.47 to 3.49) | |
| 2085–2099 | −1.34 (−1.74 to 4.16) | ||
| <65 years | |||
| Summer 1 | 2051–2065 | 0.06 (−0.35 to 0.20) | |
| 2085–2099 | 0.39 (−2.01 to 1.12) | ||
| Winter 2 | 2051–2065 | −0.28 (−0.58 to 0.96) | |
| 2085–2099 | −0.32 (−0.68 to 0.85) | ||
| 65+ years | |||
| Summer 1 | 2051–2065 | 0.23 (0.05 to 0.28) | |
| 2085–2099 | 1.37 (0.41 to 1.52) | ||
| Winter2 | 2051–2065 | −1.35 (−1.51 to 17.84) | |
| 2085–2099 | −1.58 (−1.75 to 17.79) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, M.; Santana, P.; Rocha, A. Statistical Modelling of Temperature-Attributable Deaths in Portuguese Metropolitan Areas under Climate Change: Who Is at Risk? Atmosphere 2020, 11, 159. https://doi.org/10.3390/atmos11020159
Rodrigues M, Santana P, Rocha A. Statistical Modelling of Temperature-Attributable Deaths in Portuguese Metropolitan Areas under Climate Change: Who Is at Risk? Atmosphere. 2020; 11(2):159. https://doi.org/10.3390/atmos11020159
Chicago/Turabian StyleRodrigues, Mónica, Paula Santana, and Alfredo Rocha. 2020. "Statistical Modelling of Temperature-Attributable Deaths in Portuguese Metropolitan Areas under Climate Change: Who Is at Risk?" Atmosphere 11, no. 2: 159. https://doi.org/10.3390/atmos11020159