
Immunogenetic Aspects of Sarcopenic Obesity

Abstract
:1. Introduction
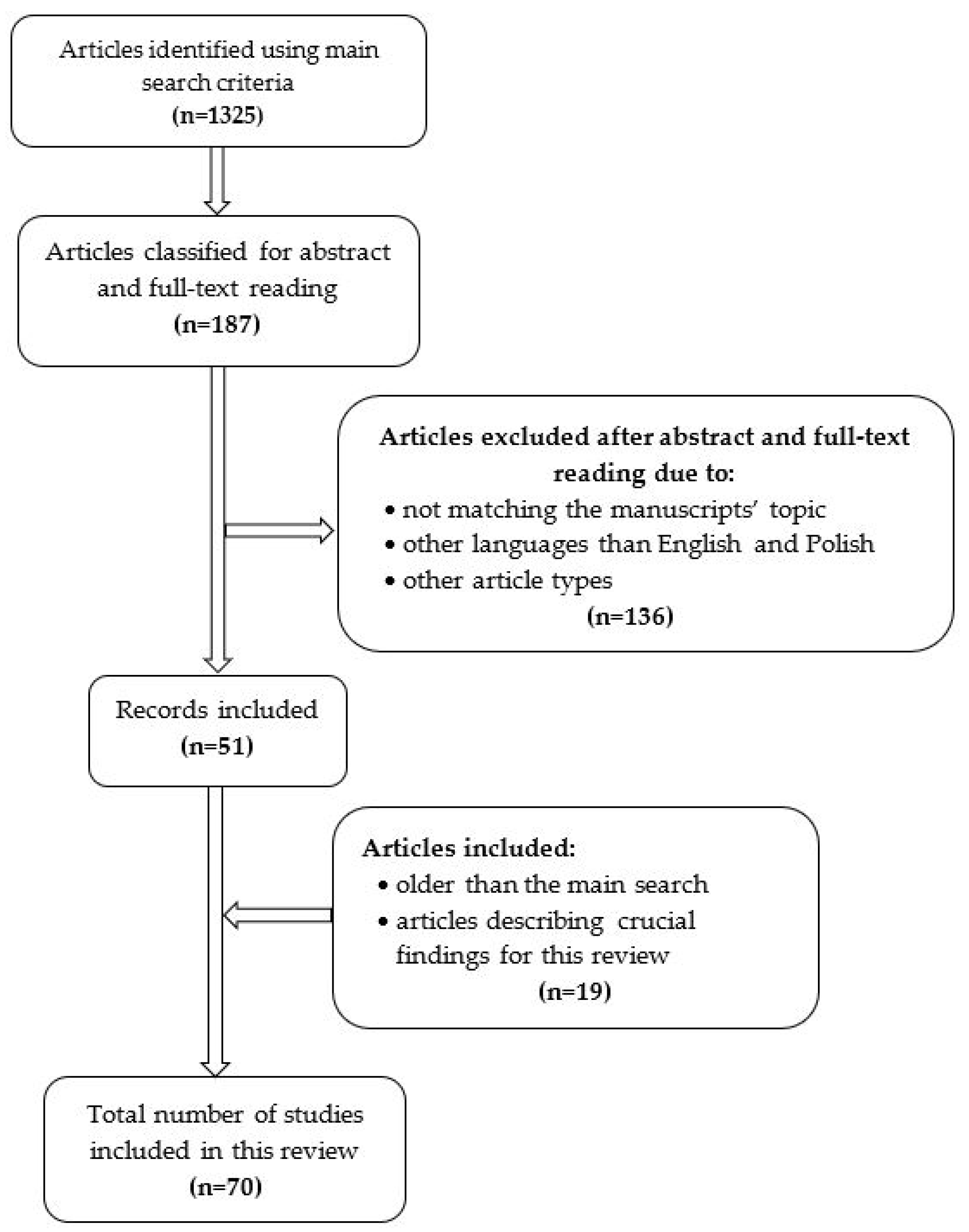
2. Materials and Methods
3. Obesity and Sarcopenia—What Came First: The Egg or the Chicken?

{kind=link}
{kind=link}
{kind=link}
| Muscle Mass Estimation and Cut-Off Points in Sarcopenic Patients | ||
|---|---|---|
| Method | Criteria | Reference |
| Anthropometric | Reference population: Rosetta study [18]—a population-based survey of 883 elderly Hispanic and non-Hispanic white men and women living in New Mexico ALM/ht2
| [18,19] |
| Dual X-ray absorptiometry—DXA | reference population: Rosetta study [18] Sarcopenia Index ALM/ht2
| [33,34,35] |
| STUDY: Health ABC—the Health Aging and Body Composition Sarcopenia index: ALM/ht2
| [36] | |
| DXA—less than the twentieth percentile of healthy adults Sarcopenia index: ALM/ht2
| [17] | |
| Bioelectrical impedance—BIA | STUDY: NHANES III—the Third National Health and Nutrition Examination Survey Sarcopenia definition: ratio of muscle mass/total body mass
| [37] |
| Study population: subjects who attended a 1988–1992 Rancho Bernardo Study clinic Sarcopenia definition: the value of FFM of > or =2.0 standard deviations below the gender-specific mean of a young reference population (Mean FFM was 43.5 kg for women and 61.7 kg for men.) Sarcopenia index—Total lean mass/ht2 M ≤ 8.50 kg/m2 F ≤ 5.75 kg/m2 | [38] | |
| STUDY: NHANES III—the Third National Health and Nutrition Examination Survey Sarcopenia definition: total muscle mass/ht2:
| [39] | |
| STUDY: Cardiovascular Health Study Sarcopenia definition: fat-free mass:
| [40] | |
| Estimation of cut-off points for SO | ||
| dual X-ray absorptiometry—DXA | Analysis of two definitions of SO: New Mexico Elder Health Survey
Health ABC study
| [36] |
New Mexico Elder Health Survey:
| [41] | |
Nutrition as a Determinant of Successful Aging study
| [42] | |
4. Immune Involvement in Sarcopenic Obesity
4.1. Pro-Inflammatory Cytokine Synthesis and Their Relation to Sarcopenic Obesity
4.2. Hormonal Factors Related to Immune Response and Genetic Background
4.3. Infections during Childhood and the Risk of Obesity
4.4. The Role of Maternal HLA in Sarcopenic Obesity
4.5. The Link between Genetic Background and Inflammation in Sarcopenic Obesity
5. Genetic Aspects of Sarcopenic Obesity
5.1. Genetic Susceptibility to Sarcopenic Obesity
5.2. Epigenetic Factors in Sarcopenic Obesity
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Donini, L.M.; Busetto, L.; Bischoff, S.C.; Cederholm, T.; Ballesteros-Pomar, M.D.; Batsis, J.A.; Bauer, J.M.; Boirie, Y.; Cruz-Jentoft, A.J.; Dicker, D.; et al. Definition and Diagnostic Criteria for Sarcopenic Obesity: ESPEN and EASO Consensus Statement. Obes. Facts 2022, 15, 321–335. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Wong, P.Y.; Chung, Y.L.; Chow, S.K.-H.; Cheung, W.H.; Law, S.W.; Chan, J.C.N.; Wong, R.M.Y. Deciphering the “Obesity Paradox” in the Elderly: A Systematic Review and Meta-Analysis of Sarcopenic Obesity. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2023, 24, e13534. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.; Mei, F.; Shang, Y.; Hu, K.; Chen, F.; Zhao, L.; Ma, B. Global Prevalence of Sarcopenic Obesity in Older Adults: A Systematic Review and Meta-Analysis. Clin. Nutr. 2021, 40, 4633–4641. [Google Scholar] [CrossRef] [PubMed]
- Donini, L.M.; Busetto, L.; Bauer, J.M.; Bischoff, S.; Boirie, Y.; Cederholm, T.; Cruz-Jentoft, A.J.; Dicker, D.; Frühbeck, G.; Giustina, A.; et al. Critical Appraisal of Definitions and Diagnostic Criteria for Sarcopenic Obesity Based on a Systematic Review. Clin. Nutr. 2020, 39, 2368–2388. [Google Scholar] [CrossRef] [PubMed]
- Wagenaar, C.A.; Dekker, L.H.; Navis, G.J. Prevalence of Sarcopenic Obesity and Sarcopenic Overweight in the General Population: The Lifelines Cohort Study. Clin. Nutr. 2021, 40, 4422–4429. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.; Nguyen, T.T.; Zhang, Y.; Ryu, D.; Gariani, K. Sarcopenic Obesity: Epidemiology, Pathophysiology, Cardiovascular Disease, Mortality, and Management. Front. Endocrinol. 2023, 14, 1185221. [Google Scholar] [CrossRef] [PubMed]
- Von Berens, Å.; Obling, S.R.; Nydahl, M.; Koochek, A.; Lissner, L.; Skoog, I.; Frändin, K.; Skoglund, E.; Rothenberg, E.; Cederholm, T. Sarcopenic Obesity and Associations with Mortality in Older Women and Men—A Prospective Observational Study. BMC Geriatr. 2020, 20, 199. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Tan, Y.; Shi, Y.; Wang, X.; Liao, Z.; Wei, P. Diabetes and Sarcopenic Obesity: Pathogenesis, Diagnosis, and Treatments. Front. Endocrinol. 2020, 11, 568. [Google Scholar] [CrossRef]
- Guo, A.; Li, K.; Xiao, Q. Sarcopenic Obesity: Myokines as Potential Diagnostic Biomarkers and Therapeutic Targets? Exp. Gerontol. 2020, 139, 111022. [Google Scholar] [CrossRef]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation. World Health; WHO Technical Report Series 894; World Health Organization: Geneva, Switzerland, 2000; pp. i–xii, 1–253. [Google Scholar]
- World Health Organization Regional Office for the Western. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000; ISBN 978-0-9577082-1-1. [Google Scholar]
- Cruz-Jentoft, A.J.; Landi, F.; Topinková, E.; Michel, J.-P. Understanding Sarcopenia as a Geriatric Syndrome. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 1–7. [Google Scholar] [CrossRef]
- Makizako, H. Frailty and Sarcopenia as a Geriatric Syndrome in Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2019, 16, 4013. [Google Scholar] [CrossRef]
- Dennison, E.M.; Sayer, A.A.; Cooper, C. Epidemiology of Sarcopenia and Insight into Possible Therapeutic Targets. Nat. Rev. Rheumatol. 2017, 13, 340–347. [Google Scholar] [CrossRef]
- Papadopoulou, S.K.; Tsintavis, P.; Potsaki, P.; Papandreou, D. Differences in the Prevalence of Sarcopenia in Community-Dwelling, Nursing Home and Hospitalized Individuals. A Systematic Review and Meta-Analysis. J. Nutr. Health Aging 2020, 24, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; Abellan van Kan, G.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An Undiagnosed Condition in Older Adults. Current Consensus Definition: Prevalence, Etiology, and Consequences. International Working Group on Sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, D.; Visser, M.; De Meersman, R.E.; Sepúlveda, D.; Baumgartner, R.N.; Pierson, R.N.; Harris, T.; Heymsfield, S.B. Appendicular Skeletal Muscle Mass: Effects of Age, Gender, and Ethnicity. J. Appl. Physiol. 1997, 83, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of Sarcopenia among the Elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M.; et al. The FNIH Sarcopenia Project: Rationale, Study Description, Conference Recommendations, and Final Estimates. J. Gerontol. A Biomed. Sci. Med. Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef]
- Zanker, J.; Sim, M.; Anderson, K.; Balogun, S.; Brennan-Olsen, S.L.; Dent, E.; Duque, G.; Girgis, C.M.; Grossmann, M.; Hayes, A.; et al. Consensus Guidelines for Sarcopenia Prevention, Diagnosis and Management in Australia and New Zealand. J. Cachexia Sarcopenia Muscle 2023, 14, 142–156. [Google Scholar] [CrossRef]
- Sayer, A.A.; Syddall, H.; Martin, H.; Patel, H.; Baylis, D.; Cooper, C. The Developmental Origins of Sarcopenia. J. Nutr. Health Aging 2008, 12, 427–432. [Google Scholar] [CrossRef]
- Jung, H.N.; Jung, C.H.; Hwang, Y.-C. Sarcopenia in Youth. Metabolism 2023, 144, 155557. [Google Scholar] [CrossRef]
- Schaap, L.A.; van Schoor, N.M.; Lips, P.; Visser, M. Associations of Sarcopenia Definitions, and Their Components, with the Incidence of Recurrent Falling and Fractures: The Longitudinal Aging Study Amsterdam. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1199–1204. [Google Scholar] [CrossRef]
- Masanés, F.; Rojano I Luque, X.; Salvà, A.; Serra-Rexach, J.A.; Artaza, I.; Formiga, F.; Cuesta, F.; López Soto, A.; Ruiz, D.; Cruz-Jentoft, A.J. Cut-off Points for Muscle Mass—Not Grip Strength or Gait Speed—Determine Variations in Sarcopenia Prevalence. J. Nutr. Health Aging 2017, 21, 825–829. [Google Scholar] [CrossRef]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the Measurement of Muscle Mass: A Need for a Reference Standard. J. Cachexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef]
- Treviño-Aguirre, E.; López-Teros, T.; Gutiérrez-Robledo, L.; Vandewoude, M.; Pérez-Zepeda, M. Availability and Use of Dual Energy X-ray Absorptiometry (DXA) and Bio-Impedance Analysis (BIA) for the Evaluation of Sarcopenia by Belgian and Latin American Geriatricians. J. Cachexia Sarcopenia Muscle 2014, 5, 79–81. [Google Scholar] [CrossRef]
- McGregor, R.A.; Cameron-Smith, D.; Poppitt, S.D. It Is Not Just Muscle Mass: A Review of Muscle Quality, Composition and Metabolism during Ageing as Determinants of Muscle Function and Mobility in Later Life. Longev. Healthspan 2014, 3, 9. [Google Scholar] [CrossRef]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic Value of Grip Strength: Findings from the Prospective Urban Rural Epidemiology (PURE) Study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- Pagotto, V.; Silveira, E.A. Applicability and Agreement of Different Diagnostic Criteria for Sarcopenia Estimation in the Elderly. Arch. Gerontol. Geriatr. 2014, 59, 288–294. [Google Scholar] [CrossRef]
- Dam, T.-T.; Peters, K.W.; Fragala, M.; Cawthon, P.M.; Harris, T.B.; McLean, R.; Shardell, M.; Alley, D.E.; Kenny, A.; Ferrucci, L.; et al. An Evidence-Based Comparison of Operational Criteria for the Presence of Sarcopenia. J. Gerontol. A Biomed. Sci. Med. Sci. 2014, 69, 584–590. [Google Scholar] [CrossRef] [PubMed]
- Sui, S.X.; Holloway-Kew, K.L.; Hyde, N.K.; Williams, L.J.; Tembo, M.C.; Leach, S.; Pasco, J.A. Definition-Specific Prevalence Estimates for Sarcopenia in an Australian Population: The Geelong Osteoporosis Study. JCSM Clin. Rep. 2020, 5, 89–98. [Google Scholar] [CrossRef]
- Melton, L.J.; Khosla, S.; Crowson, C.S.; O’Connor, M.K.; O’Fallon, W.M.; Riggs, B.L. Epidemiology of Sarcopenia. J. Am. Geriatr. Soc. 2000, 48, 625–630. [Google Scholar] [CrossRef]
- Morley, J.E.; Baumgartner, R.N.; Roubenoff, R.; Mayer, J.; Nair, K.S. Sarcopenia. J. Lab. Clin. Med. 2001, 137, 231–243. [Google Scholar] [CrossRef]
- Iannuzzi-Sucich, M.; Prestwood, K.M.; Kenny, A.M. Prevalence of Sarcopenia and Predictors of Skeletal Muscle Mass in Healthy, Older Men and Women. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M772–M777. [Google Scholar] [CrossRef]
- Newman, A.B.; Kupelian, V.; Visser, M.; Simonsick, E.; Goodpaster, B.; Nevitt, M.; Kritchevsky, S.B.; Tylavsky, F.A.; Rubin, S.M.; Harris, T.B.; et al. Sarcopenia: Alternative Definitions and Associations with Lower Extremity Function. J. Am. Geriatr. Soc. 2003, 51, 1602–1609. [Google Scholar] [CrossRef]
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low Relative Skeletal Muscle Mass (Sarcopenia) in Older Persons Is Associated with Functional Impairment and Physical Disability. J. Am. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Castillo, E.M.; Goodman-Gruen, D.; Kritz-Silverstein, D.; Morton, D.J.; Wingard, D.L.; Barrett-Connor, E. Sarcopenia in Elderly Men and Women: The Rancho Bernardo Study. Am. J. Prev. Med. 2003, 25, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Baumgartner, R.N.; Ross, R.; Rosenberg, I.H.; Roubenoff, R. Skeletal Muscle Cutpoints Associated with Elevated Physical Disability Risk in Older Men and Women. Am. J. Epidemiol. 2004, 159, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I. Influence of Sarcopenia on the Development of Physical Disability: The Cardiovascular Health Study. J. Am. Geriatr. Soc. 2006, 54, 56–62. [Google Scholar] [CrossRef]
- Baumgartner, R.N.; Wayne, S.J.; Waters, D.L.; Janssen, I.; Gallagher, D.; Morley, J.E. Sarcopenic Obesity Predicts Instrumental Activities of Daily Living Disability in the Elderly. Obes. Res. 2004, 12, 1995–2004. [Google Scholar] [CrossRef]
- Bouchard, D.R.; Dionne, I.J.; Brochu, M. Sarcopenic/Obesity and Physical Capacity in Older Men and Women: Data from the Nutrition as a Determinant of Successful Aging (NuAge)-the Quebec Longitudinal Study. Obesity 2009, 17, 2082–2088. [Google Scholar] [CrossRef]
- Barazzoni, R.; Bischoff, S.; Boirie, Y.; Busetto, L.; Cederholm, T.; Dicker, D.; Toplak, H.; Van Gossum, A.; Yumuk, V.; Vettor, R. Sarcopenic Obesity: Time to Meet the Challenge. Obes. Facts 2018, 11, 294–305. [Google Scholar] [CrossRef]
- Roubenoff, R. Sarcopenic Obesity: The Confluence of Two Epidemics. Obes. Res. 2004, 12, 887–888. [Google Scholar] [CrossRef]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Benzeval, M.; Deary, I.J.; Dennison, E.M.; Der, G.; Gale, C.R.; Inskip, H.M.; Jagger, C.; et al. Grip Strength across the Life Course: Normative Data from Twelve British Studies. PLoS ONE 2014, 9, e113637. [Google Scholar] [CrossRef]
- Sayer, A.A.; Syddall, H.E.; Gilbody, H.J.; Dennison, E.M.; Cooper, C. Does Sarcopenia Originate in Early Life? Findings from the Hertfordshire Cohort Study. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, M930–M934. [Google Scholar] [CrossRef]
- Gonzalez, A.; Simon, F.; Achiardi, O.; Vilos, C.; Cabrera, D.; Cabello-Verrugio, C. The Critical Role of Oxidative Stress in Sarcopenic Obesity. Oxidative Med. Cell. Longev. 2021, 2021, 4493817. [Google Scholar] [CrossRef]
- Lynch, G.M.; Murphy, C.H.; Castro, E.d.M.; Roche, H.M. Inflammation and Metabolism: The Role of Adiposity in Sarcopenic Obesity. Proc. Nutr. Soc. 2020, 79, 435–447. [Google Scholar] [CrossRef]
- Schrager, M.A.; Metter, E.J.; Simonsick, E.; Ble, A.; Bandinelli, S.; Lauretani, F.; Ferrucci, L. Sarcopenic Obesity and Inflammation in the InCHIANTI Study. J. Appl. Physiol. 2007, 102, 919–925. [Google Scholar] [CrossRef]
- Ahmed, B.; Sultana, R.; Greene, M.W. Adipose Tissue and Insulin Resistance in Obese. Biomed. Pharmacother. 2021, 137, 111315. [Google Scholar] [CrossRef]
- Panee, J. Monocyte Chemoattractant Protein 1 (MCP-1) in Obesity and Diabetes. Cytokine 2012, 60, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Huber, J.; Kiefer, F.W.; Zeyda, M.; Ludvik, B.; Silberhumer, G.R.; Prager, G.; Zlabinger, G.J.; Stulnig, T.M. CC Chemokine and CC Chemokine Receptor Profiles in Visceral and Subcutaneous Adipose Tissue Are Altered in Human Obesity. J. Clin. Endocrinol. Metab. 2008, 93, 3215–3221. [Google Scholar] [CrossRef] [PubMed]
- Lauterbach, M.A.R.; Wunderlich, F.T. Macrophage Function in Obesity-Induced Inflammation and Insulin Resistance. Pflug. Arch. 2017, 469, 385–396. [Google Scholar] [CrossRef]
- Chylikova, J.; Dvorackova, J.; Tauber, Z.; Kamarad, V. M1/M2 Macrophage Polarization in Human Obese Adipose Tissue. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czechoslov. 2018, 162, 79–82. [Google Scholar] [CrossRef]
- Hong, S.-H.; Choi, K.M. Sarcopenic Obesity, Insulin Resistance, and Their Implications in Cardiovascular and Metabolic Consequences. Int. J. Mol. Sci. 2020, 21, 494. [Google Scholar] [CrossRef]
- Alizadeh Pahlavani, H. Exercise Therapy for People with Sarcopenic Obesity: Myokines and Adipokines as Effective Actors. Front. Endocrinol. 2022, 13, 811751. [Google Scholar] [CrossRef]
- Hu, M.; Yu, Z.; Luo, D.; Zhang, H.; Li, J.; Liang, F.; Chen, R. Association between -174G>C Polymorphism in the IL-6 Promoter Region and the Risk of Obesity: A Meta-Analysis. Medicine 2018, 97, e11773. [Google Scholar] [CrossRef] [PubMed]
- Koc, G.; Doran, T.; Uygur, M.M.; Kirac, D. Obesity Is Associated with IL-6 Gene Polymorphisms Rs1800795 and Rs1800796 but Not SOCS3 Rs4969170. Mol. Biol. Rep. 2023, 50, 2041–2048. [Google Scholar] [CrossRef]
- Luotola, K. IL-1 Receptor Antagonist (IL-1Ra) Levels and Management of Metabolic Disorders. Nutrients 2022, 14, 3422. [Google Scholar] [CrossRef]
- Gangemi, S.; Basile, G.; Monti, D.; Alba Merendino, R.; Di Pasquale, G.; Bisignano, U.; Nicita-Mauro, V.; Franceschi, C. Age-Related Modifications in Circulating IL-15 Levels in Humans. Mediat. Inflamm. 2005, 2005, 245–247. [Google Scholar] [CrossRef] [PubMed]
- Quinn, L.S.; Anderson, B.G.; Conner, J.D.; Wolden-Hanson, T.; Marcell, T.J. IL-15 Is Required for Postexercise Induction of the pro-Oxidative Mediators PPARδ and SIRT1 in Male Mice. Endocrinology 2014, 155, 143–155. [Google Scholar] [CrossRef]
- Tilg, H.; Moschen, A.R. Adipocytokines: Mediators Linking Adipose Tissue, Inflammation and Immunity. Nat. Rev. Immunol. 2006, 6, 772–783. [Google Scholar] [CrossRef] [PubMed]
- Kob, R.; Bollheimer, L.C.; Bertsch, T.; Fellner, C.; Djukic, M.; Sieber, C.C.; Fischer, B.E. Sarcopenic Obesity: Molecular Clues to a Better Understanding of Its Pathogenesis? Biogerontology 2015, 16, 15–29. [Google Scholar] [CrossRef]
- Morley, J.E. Hormones and Sarcopenia. Curr. Pharm. Des. 2017, 23, 4484–4492. [Google Scholar] [CrossRef]
- Roh, E.; Choi, K.M. Health Consequences of Sarcopenic Obesity: A Narrative Review. Front. Endocrinol. 2020, 11, 332. [Google Scholar] [CrossRef]
- Park, S. Association between Polygenetic Risk Scores Related to Sarcopenia Risk and Their Interactions with Regular Exercise in a Large Cohort of Korean Adults. Clin. Nutr. 2021, 40, 5355–5364. [Google Scholar] [CrossRef]
- Semenova, E.A.; Pranckevičienė, E.; Bondareva, E.A.; Gabdrakhmanova, L.J.; Ahmetov, I.I. Identification and Characterization of Genomic Predictors of Sarcopenia and Sarcopenic Obesity Using UK Biobank Data. Nutrients 2023, 15, 758. [Google Scholar] [CrossRef]
- Evans, K.; Abdelhafiz, D.; Abdelhafiz, A.H. Sarcopenic Obesity as a Determinant of Cardiovascular Disease Risk in Older People: A Systematic Review. Postgrad. Med. 2021, 133, 831–842. [Google Scholar] [CrossRef]
- Pradhan, G.; Samson, S.L.; Sun, Y. Ghrelin: Much More than a Hunger Hormone. Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 619–624. [Google Scholar] [CrossRef]
- Esposito, P.; Picciotto, D.; Battaglia, Y.; Costigliolo, F.; Viazzi, F.; Verzola, D. Myostatin: Basic Biology to Clinical Application. Adv. Clin. Chem. 2022, 106, 181–234. [Google Scholar] [CrossRef]
- Aghaali, M.; Hashemi-Nazari, S.S. Association between Early Antibiotic Exposure and Risk of Childhood Weight Gain and Obesity: A Systematic Review and Meta-Analysis. J. Pediatr. Endocrinol. Metab. JPEM 2019, 32, 439–445. [Google Scholar] [CrossRef]
- Bassetti, S.; Tschudin-Sutter, S.; Egli, A.; Osthoff, M. Optimizing Antibiotic Therapies to Reduce the Risk of Bacterial Resistance. Eur. J. Intern. Med. 2022, 99, 7–12. [Google Scholar] [CrossRef]
- Rasmussen, S.H.; Shrestha, S.; Bjerregaard, L.G.; Ängquist, L.H.; Baker, J.L.; Jess, T.; Allin, K.H. Antibiotic Exposure in Early Life and Childhood Overweight and Obesity: A Systematic Review and Meta-Analysis. Diabetes Obes. Metab. 2018, 20, 1508–1514. [Google Scholar] [CrossRef]
- Cho, I.; Yamanishi, S.; Cox, L.; Methé, B.A.; Zavadil, J.; Li, K.; Gao, Z.; Mahana, D.; Raju, K.; Teitler, I.; et al. Antibiotics in Early Life Alter the Murine Colonic Microbiome and Adiposity. Nature 2012, 488, 621–626. [Google Scholar] [CrossRef]
- Wilkins, A.T.; Reimer, R.A. Obesity, Early Life Gut Microbiota, and Antibiotics. Microorganisms 2021, 9, 413. [Google Scholar] [CrossRef]
- Bach, D.; Pich, S.; Soriano, F.X.; Vega, N.; Baumgartner, B.; Oriola, J.; Daugaard, J.R.; Lloberas, J.; Camps, M.; Zierath, J.R.; et al. Mitofusin-2 Determines Mitochondrial Network Architecture and Mitochondrial Metabolism. A Novel Regulatory Mechanism Altered in Obesity. J. Biol. Chem. 2003, 278, 17190–17197. [Google Scholar] [CrossRef]
- Dutra, M.T.; Avelar, B.P.; Souza, V.C.; Bottaro, M.; Oliveira, R.J.; Nóbrega, O.T.; Moreno Lima, R. Relationship between Sarcopenic Obesity-Related Phenotypes and Inflammatory Markers in Postmenopausal Women. Clin. Physiol. Funct. Imaging 2017, 37, 205–210. [Google Scholar] [CrossRef]
- Sakuma, K.; Yamaguchi, A. Sarcopenic Obesity and Endocrinal Adaptation with Age. Int. J. Endocrinol. 2013, 2013, 204164. [Google Scholar] [CrossRef]
- Mazurkiewicz, M.; Lizurej, W.; Mazurkiewicz, L.; Majewski, A.; Tobis, S.; Cymerys, M. C-Reactive Protein and Albumin Levels as Useful Tools for Predicting In-Hospital Outcomes in Polish Nonagenarians. Clin. Interv. Aging 2023, 18, 1547–1554. [Google Scholar] [CrossRef]
- Ohler, A.M.; Braddock, A. Infections and Antibiotic Use in Early Life, and Obesity in Early Childhood: A Mediation Analysis. Int. J. Obes. 2005 2022, 46, 1608–1614. [Google Scholar] [CrossRef]
- Voss, J.D.; Atkinson, R.L.; Dhurandhar, N.V. Role of Adenoviruses in Obesity. Rev. Med. Virol. 2015, 25, 379–387. [Google Scholar] [CrossRef]
- Voss, J.D.; Dhurandhar, N.V. Viral Infections and Obesity. Curr. Obes. Rep. 2017, 6, 28–37. [Google Scholar] [CrossRef]
- Pasarica, M.; Mashtalir, N.; McAllister, E.J.; Kilroy, G.E.; Koska, J.; Permana, P.; de Courten, B.; Yu, M.; Ravussin, E.; Gimble, J.M.; et al. Adipogenic Human Adenovirus Ad-36 Induces Commitment, Differentiation, and Lipid Accumulation in Human Adipose-Derived Stem Cells. Stem Cells 2008, 26, 969–978. [Google Scholar] [CrossRef]
- Jones, G.; Pilling, L.C.; Kuo, C.-L.; Kuchel, G.; Ferrucci, L.; Melzer, D. Sarcopenia and Variation in the Human Leukocyte Antigen Complex. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 301–308. [Google Scholar] [CrossRef]
- Jones, G.; Trajanoska, K.; Santanasto, A.J.; Stringa, N.; Kuo, C.-L.; Atkins, J.L.; Lewis, J.R.; Duong, T.; Hong, S.; Biggs, M.L.; et al. Genome-Wide Meta-Analysis of Muscle Weakness Identifies 15 Susceptibility Loci in Older Men and Women. Nat. Commun. 2021, 12, 654. [Google Scholar] [CrossRef]
- Singh, A.N.; Gasman, B. Disentangling the Genetics of Sarcopenia: Prioritization of NUDT3 and KLF5 as Genes for Lean Mass & HLA-DQB1-AS1 for Hand Grip Strength with the Associated Enhancing SNPs & a Scoring System. BMC Med. Genet. 2020, 21, 40. [Google Scholar] [CrossRef]
- Sica, A.; Erreni, M.; Allavena, P.; Porta, C. Macrophage Polarization in Pathology. Cell. Mol. Life Sci. 2015, 72, 4111–4126. [Google Scholar] [CrossRef]
- Gu, X.; Zhang, Y.; Li, D.; Cai, H.; Cai, L.; Xu, Q. N6-Methyladenosine Demethylase FTO Promotes M1 and M2 Macrophage Activation. Cell. Signal. 2020, 69, 109553. [Google Scholar] [CrossRef]
- McFadden, M.J.; Sacco, M.T.; Murphy, K.A.; Park, M.; Gokhale, N.S.; Somfleth, K.Y.; Horner, S.M. FTO Suppresses STAT3 Activation and Modulates Proinflammatory Interferon-Stimulated Gene Expression. J. Mol. Biol. 2022, 434, 167247. [Google Scholar] [CrossRef]
- Carpenter, R.L.; Lo, H.-W. STAT3 Target Genes Relevant to Human Cancers. Cancers 2014, 6, 897–925. [Google Scholar] [CrossRef]
- Dubey, P.K.; Patil, M.; Singh, S.; Dubey, S.; Ahuja, P.; Verma, S.K.; Krishnamurthy, P. Increased m6A-RNA Methylation and FTO Suppression Is Associated with Myocardial Inflammation and Dysfunction during Endotoxemia in Mice. Mol. Cell. Biochem. 2022, 477, 129–141. [Google Scholar] [CrossRef]
- Hernandez-Quiles, M.; Broekema, M.F.; Kalkhoven, E. PPARgamma in Metabolism, Immunity, and Cancer: Unified and Diverse Mechanisms of Action. Front. Endocrinol. 2021, 12, 624112. [Google Scholar] [CrossRef]
- Parisi, L.; Gini, E.; Baci, D.; Tremolati, M.; Fanuli, M.; Bassani, B.; Farronato, G.; Bruno, A.; Mortara, L. Macrophage Polarization in Chronic Inflammatory Diseases: Killers or Builders? J. Immunol. Res. 2018, 2018, 8917804. [Google Scholar] [CrossRef]
- Araki, A.; Hosoi, T.; Orimo, H.; Ito, H. Association of Plasma Homocysteine with Serum Interleukin-6 and C-Peptide Levels in Patients with Type 2 Diabetes. Metabolism 2005, 54, 809–814. [Google Scholar] [CrossRef]
- Lisboa, J.V.d.C.; Ribeiro, M.R.; Luna, R.C.P.; Lima, R.P.A.; do Nascimento, R.A.F.; Monteiro, M.G.C.A.; Lima, K.Q.d.F.; Fechine, C.P.N.d.S.; de Oliveira, N.F.P.; Persuhn, D.C.; et al. Food Intervention with Folate Reduces TNF-α and Interleukin Levels in Overweight and Obese Women with the MTHFR C677T Polymorphism: A Randomized Trial. Nutrients 2020, 12, 361. [Google Scholar] [CrossRef]
- Gholami, M.; Sharifi, F.; Shahriari, S.; Khoshnevisan, K.; Larijani, B.; Amoli, M.M. Association of Interleukin-6 Polymorphisms with Obesity: A Systematic Review and Meta-Analysis. Cytokine 2019, 123, 154769. [Google Scholar] [CrossRef]
- Melo, A.P.C.; Teixeira, H.M.P.; Coelho, R.S.; De Jesus, T.D.S.; Queiroz, G.A.; Silva, H.D.S.; De Almeida, Y.C.F.; Alcantara-Neves, N.M.; De Matos, S.M.A.; D’innocenzo, S.; et al. Variants in Proinflammatory Genes IL1RL1, IL1B and IRF4 Are Associated with Overweight in a Pediatric Brazilian Population. Gene 2022, 828, 146478. [Google Scholar] [CrossRef]
- Maculewicz, E.; Antkowiak, B.; Antkowiak, O.; Borecka, A.; Mastalerz, A.; Leońska-Duniec, A.; Humińska-Lisowska, K.; Michałowska-Sawczyn, M.; Garbacz, A.; Lorenz, K.; et al. The Interactions between Interleukin-1 Family Genes: IL1A, IL1B, IL1RN, and Obesity Parameters. BMC Genom. 2022, 23, 112. [Google Scholar] [CrossRef]
- Hinney, A.; Körner, A.; Fischer-Posovszky, P. The Promise of New Anti-Obesity Therapies Arising from Knowledge of Genetic Obesity Traits. Nat. Rev. Endocrinol. 2022, 18, 623–637. [Google Scholar] [CrossRef]
- Mahmoud, R.; Kimonis, V.; Butler, M.G. Genetics of Obesity in Humans: A Clinical Review. Int. J. Mol. Sci. 2022, 23, 11005. [Google Scholar] [CrossRef]
- Sivaprakasam, S.; Sikder, M.O.F.; Ramalingam, L.; Kaur, G.; Dufour, J.M.; Moustaid-Moussa, N.; Wachtel, M.S.; Ganapathy, V. SLC6A14 Deficiency Is Linked to Obesity, Fatty Liver, and Metabolic Syndrome but Only under Conditions of a High-Fat Diet. Biochim. Biophys. Acta Mol. Basis Dis. 2021, 1867, 166087. [Google Scholar] [CrossRef]
- Męczekalski, B.; Czyżyk, A.; Warenik-Szymankiewicz, A. Rola Genów w Powstawaniu Otyłości. Współczesne Poglądy, Patogeneza, Aspekty Kliniczne. Endokrynol. Otyłość Zaburzenia Przemiany Mater. 2008, 4, 27–37. [Google Scholar]
- Shabana; Shahid, S.U.; Hasnain, S. Use of a Gene Score of Multiple Low-Modest Effect Size Variants Can Predict the Risk of Obesity Better than the Individual SNPs. Lipids Health Dis. 2018, 17, 155. [Google Scholar] [CrossRef]
- Tan, P.Y.; Mitra, S.R. The Combined Effect of Polygenic Risk from FTO and ADRB2 Gene Variants, Odds of Obesity, and Post-Hipcref Diet Differences. Lifestyle Genom. 2020, 13, 84–98. [Google Scholar] [CrossRef]
- Castro, G.V.; Latorre, A.F.S.; Korndorfer, F.P.; de Carlos Back, L.K.; Lofgren, S.E. The Impact of Variants in Four Genes: MC4R, FTO, PPARG and PPARGC1A in Overweight and Obesity in a Large Sample of the Brazilian Population. Biochem. Genet. 2021, 59, 1666–1679. [Google Scholar] [CrossRef]
- Frayling, T.M.; Timpson, N.J.; Weedon, M.N.; Zeggini, E.; Freathy, R.M.; Lindgren, C.M.; Perry, J.R.B.; Elliott, K.S.; Lango, H.; Rayner, N.W.; et al. A Common Variant in the FTO Gene Is Associated with Body Mass Index and Predisposes to Childhood and Adult Obesity. Science 2007, 316, 889–894. [Google Scholar] [CrossRef]
- Lan, N.; Lu, Y.; Zhang, Y.; Pu, S.; Xi, H.; Nie, X.; Liu, J.; Yuan, W. FTO—A Common Genetic Basis for Obesity and Cancer. Front. Genet. 2020, 11, 559138. [Google Scholar] [CrossRef]
- Park, H.-G.; Choi, J.-H. Genetic Variant Rs9939609 in FTO Is Associated with Body Composition and Obesity Risk in Korean Females. BMJ Open Diabetes Res. Care 2023, 11, e003649. [Google Scholar] [CrossRef]
- Ran, S.; Jiang, Z.-X.; He, X.; Liu, Y.; Zhang, Y.-X.; Zhang, L.; Pei, Y.-F.; Zhang, M.; Hai, R.; Gu, G.-S.; et al. Replication of FTO Gene Associated with Lean Mass in a Meta-Analysis of Genome-Wide Association Studies. Sci. Rep. 2020, 10, 5057. [Google Scholar] [CrossRef] [PubMed]
- Khanal, P.; He, L.; Stebbings, G.; Onambele-Pearson, G.L.; Degens, H.; Williams, A.; Thomis, M.; Morse, C.I. Prevalence and Association of Single Nucleotide Polymorphisms with Sarcopenia in Older Women Depends on Definition. Sci. Rep. 2020, 10, 2913. [Google Scholar] [CrossRef] [PubMed]
- Clément, K.; Biebermann, H.; Farooqi, I.S.; Van der Ploeg, L.; Wolters, B.; Poitou, C.; Puder, L.; Fiedorek, F.; Gottesdiener, K.; Kleinau, G.; et al. MC4R Agonism Promotes Durable Weight Loss in Patients with Leptin Receptor Deficiency. Nat. Med. 2018, 24, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Collet, T.-H.; Dubern, B.; Mokrosinski, J.; Connors, H.; Keogh, J.M.; Mendes de Oliveira, E.; Henning, E.; Poitou-Bernert, C.; Oppert, J.-M.; Tounian, P.; et al. Evaluation of a Melanocortin-4 Receptor (MC4R) Agonist (Setmelanotide) in MC4R Deficiency. Mol. Metab. 2017, 6, 1321–1329. [Google Scholar] [CrossRef] [PubMed]
- Brodowski, J.; Szkup, M.; Jurczak, A.; Wieder-Huszla, S.; Brodowska, A.; Laszczyńska, M.; Karakiewicz, B.; Kęcka, K.; Grochans, E. Searching for the Relationship between the Parameters of Metabolic Syndrome and the Rs17782313 (T>C) Polymorphism of the MC4R Gene in Postmenopausal Women. Clin. Interv. Aging 2017, 12, 549–555. [Google Scholar] [CrossRef]
- Yang, J.; Gao, Q.; Gao, X.; Tao, X.; Cai, H.; Fan, Y.; Zhang, N.; Zhang, Y.; Li, L.; Li, H. Melanocortin-4 Receptor Rs17782313 Polymorphisms Are Associated with Serum Triglycerides in Older Chinese Women. Asia Pac. J. Clin. Nutr. 2016, 25, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Lima, R.P.A.; Ribeiro, M.R.; de Farias Lima, K.Q.; de Sena, E.A.; de Oliveira Costa, D.; Luna, R.C.P.; do Nascimento, R.A.F.; da Conceição Rodrigues Gonçalves, M.; de Toledo Vianna, R.P.; de Moraes, R.M.; et al. Methylation Profile of the ADRB3 Gene and Its Association with Lipid Profile and Nutritional Status in Adults. Biol. Res. 2019, 52, 21. [Google Scholar] [CrossRef] [PubMed]
- Luo, Z.; Zhang, T.; Wang, S.; He, Y.; Ye, Q.; Cao, W. The Trp64Arg Polymorphism in Β3 Adrenergic Receptor (ADRB3) Gene Is Associated with Adipokines and Plasma Lipids: A Systematic Review, Meta-Analysis, and Meta-Regression. Lipids Health Dis. 2020, 19, 99. [Google Scholar] [CrossRef] [PubMed]
- De Jesus, Í.C.; Alle, L.F.; Munhoz, E.C.; da Silva, L.R.; Lopes, W.A.; Tureck, L.V.; Purim, K.S.M.; Titski, A.C.K.; Leite, N. Trp64Arg Polymorphism of the ADRB3 Gene Associated with Maximal Fat Oxidation and LDL-C Levels in Non-Obese Adolescents. J. Pediatr. 2018, 94, 425–431. [Google Scholar] [CrossRef] [PubMed]
- González-Hedström, D.; Priego, T.; Amor, S.; de la Fuente-Fernández, M.; Martín, A.I.; López-Calderón, A.; Inarejos-García, A.M.; García-Villalón, Á.L.; Granado, M. Olive Leaf Extract Supplementation to Old Wistar Rats Attenuates Aging-Induced Sarcopenia and Increases Insulin Sensitivity in Adipose Tissue and Skeletal Muscle. Antioxidants 2021, 10, 737. [Google Scholar] [CrossRef] [PubMed]
- McKean-Cowdin, R.; Li, X.; Bernstein, L.; McTiernan, A.; Ballard-Barbash, R.; Gauderman, W.J.; Gilliland, F. The ADRB3 Trp64Arg Variant and Obesity in African-American Breast Cancer Cases. Int. J. Obes. 2005 2007, 31, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Grygiel-Górniak, B.; Kaczmarek, E.; Mosor, M.; Przysławski, J.; Nowak, J. Gene-Diet-Related Factors of Hyperglycaemia in Postmenopausal Women. J. Appl. Genet. 2018, 59, 169–177. [Google Scholar] [CrossRef]
- Grygiel-Górniak, B.; Kaczmarek, E.; Mosor, M.; Przysławski, J.; Nowak, J. The Gene-Diet Associations in Postmenopausal Women with Newly Diagnosed Dyslipidemia. J. Nutr. Health Aging 2017, 21, 1031–1037. [Google Scholar] [CrossRef]
- de Luis, D.A.; Aller, R.; Izaola, O.; Gonzalez-Sagrado, M.; Conde, R. Relation of Trp64Arg Polymorphism of β3-Adrenoreceptor Gene with Cardiovascular Risk Factors in Presurgical Morbidly Obese Patients. Arch. Med. Res. 2008, 39, 791–795. [Google Scholar] [CrossRef]
- Clément, K.; Vaisse, C.; Manning, B.S.; Basdevant, A.; Guy-Grand, B.; Ruiz, J.; Silver, K.D.; Shuldiner, A.R.; Froguel, P.; Strosberg, A.D. Genetic Variation in the β3-Adrenergic Receptor and an Increased Capacity to Gain Weight in Patients with Morbid Obesity. N. Engl. J. Med. 1995, 333, 352–354. [Google Scholar] [CrossRef]
- Kurokawa, N.; Young, E.H.; Oka, Y.; Satoh, H.; Wareham, N.J.; Sandhu, M.S.; Loos, R.J.F. The ADRB3 Trp64Arg Variant and BMI: A Meta-Analysis of 44 833 Individuals. Int. J. Obes. 2005 2008, 32, 1240–1249. [Google Scholar] [CrossRef]
- Bhutia, Y.D.; Mathew, M.; Sivaprakasam, S.; Ramachandran, S.; Ganapathy, V. Unconventional Functions of Amino Acid Transporters: Role in Macropinocytosis (SLC38A5/SLC38A3) and Diet-Induced Obesity/Metabolic Syndrome (SLC6A19/SLC6A14/SLC6A6). Biomolecules 2022, 12, 235. [Google Scholar] [CrossRef]
- Suviolahti, E.; Oksanen, L.J.; Öhman, M.; Cantor, R.M.; Ridderstråle, M.; Tuomi, T.; Kaprio, J.; Rissanen, A.; Mustajoki, P.; Jousilahti, P.; et al. The SLC6A14 Gene Shows Evidence of Association with Obesity. J. Clin. Investig. 2003, 112, 1762–1772. [Google Scholar] [CrossRef]
- Durand, E.; Boutin, P.; Meyre, D.; Charles, M.A.; Clement, K.; Dina, C.; Froguel, P. Polymorphisms in the Amino Acid Transporter Solute Carrier Family 6 (Neurotransmitter Transporter) Member 14 Gene Contribute to Polygenic Obesity in French Caucasians. Diabetes 2004, 53, 2483–2486. [Google Scholar] [CrossRef]
- Bröer, S. Epithelial Neutral Amino Acid Transporters: Lessons from Mouse Models. Curr. Opin. Nephrol. Hypertens. 2013, 22, 539–544. [Google Scholar] [CrossRef]
- Cheng, Q.; Shah, N.; Bröer, A.; Fairweather, S.; Jiang, Y.; Schmoll, D.; Corry, B.; Bröer, S. Identification of Novel Inhibitors of the Amino Acid Transporter B0 AT1 (SLC6A19), a Potential Target to Induce Protein Restriction and to Treat Type 2 Diabetes. Br. J. Pharmacol. 2017, 174, 468–482. [Google Scholar] [CrossRef] [PubMed]
- Javed, K.; Cheng, Q.; Carroll, A.J.; Truong, T.T.; Bröer, S. Development of Biomarkers for Inhibition of SLC6A19 (B0AT1)-A Potential Target to Treat Metabolic Disorders. Int. J. Mol. Sci. 2018, 19, 3597. [Google Scholar] [CrossRef] [PubMed]
- Corpeleijn, E.; Petersen, L.; Holst, C.; Saris, W.H.; Astrup, A.; Langin, D.; MacDonald, I.; Martinez, J.A.; Oppert, J.-M.; Polak, J.; et al. Obesity-Related Polymorphisms and Their Associations with the Ability to Regulate Fat Oxidation in Obese Europeans: The NUGENOB Study. Obesity 2010, 18, 1369–1377. [Google Scholar] [CrossRef] [PubMed]
- Auwerx, J. PPARgamma, the Ultimate Thrifty Gene. Diabetologia 1999, 42, 1033–1049. [Google Scholar] [CrossRef] [PubMed]
- Laganà, A.S.; Vitale, S.G.; Nigro, A.; Sofo, V.; Salmeri, F.M.; Rossetti, P.; Rapisarda, A.M.C.; La Vignera, S.; Condorelli, R.A.; Rizzo, G.; et al. Pleiotropic Actions of Peroxisome Proliferator-Activated Receptors (PPARs) in Dysregulated Metabolic Homeostasis, Inflammation and Cancer: Current Evidence and Future Perspectives. Int. J. Mol. Sci. 2016, 17, 999. [Google Scholar] [CrossRef]
- Wang, S.; Lin, Y.; Gao, L.; Yang, Z.; Lin, J.; Ren, S.; Li, F.; Chen, J.; Wang, Z.; Dong, Z.; et al. PPAR-γ Integrates Obesity and Adipocyte Clock through Epigenetic Regulation of Bmal1. Theranostics 2022, 12, 1589–1606. [Google Scholar] [CrossRef] [PubMed]
- Ren, D.; Collingwood, T.N.; Rebar, E.J.; Wolffe, A.P.; Camp, H.S. PPARgamma Knockdown by Engineered Transcription Factors: Exogenous PPARgamma2 but Not PPARgamma1 Reactivates Adipogenesis. Genes Dev. 2002, 16, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Deeb, S.S.; Fajas, L.; Nemoto, M.; Pihlajamäki, J.; Mykkänen, L.; Kuusisto, J.; Laakso, M.; Fujimoto, W.; Auwerx, J. A Pro12Ala Substitution in PPARgamma2 Associated with Decreased Receptor Activity, Lower Body Mass Index and Improved Insulin Sensitivity. Nat. Genet. 1998, 20, 284–287. [Google Scholar] [CrossRef] [PubMed]
- Muntean, C.; Sasaran, M.O.; Crisan, A.; Banescu, C. Effects of PPARG and PPARGC1A Gene Polymorphisms on Obesity Markers. Front. Public Health 2022, 10, 962852. [Google Scholar] [CrossRef] [PubMed]
- Franks, P.W.; Jablonski, K.A.; Delahanty, L.; Hanson, R.L.; Kahn, S.E.; Altshuler, D.; Knowler, W.C.; Florez, J.C.; Diabetes Prevention Program Research Group. The Pro12Ala Variant at the Peroxisome Proliferator-Activated Receptor γ Gene and Change in Obesity-Related Traits in the Diabetes Prevention Program. Diabetologia 2007, 50, 2451–2460. [Google Scholar] [CrossRef]
- Dedoussis, G.V.; Vidra, N.; Butler, J.; Papoutsakis, C.; Yannakoulia, M.; Hirschhorn, J.N.; Lyon, H.N. Peroxisome Proliferator-Activated Receptor-γ (PPARγ) Pro12Ala Polymorphism and Risk for Pediatric Obesity. Clin. Chem. Lab. Med. 2009, 47, 1047–1050. [Google Scholar] [CrossRef]
- Li, S.; He, C.; Nie, H.; Pang, Q.; Wang, R.; Zeng, Z.; Song, Y. G Allele of the Rs1801282 Polymorphism in PPARγ Gene Confers an Increased Risk of Obesity and Hypercholesterolemia, While T Allele of the Rs3856806 Polymorphism Displays a Protective Role Against Dyslipidemia: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2022, 13, 919087. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Lou, Y.; Jin, W.; Liu, Y.; Lu, L.; Lu, G. The Pro12Ala Polymorphism in the Peroxisome Proliferator-Activated Receptor Gamma-2 Gene (PPARγ2) Is Associated with Increased Risk of Coronary Artery Disease: A Meta-Analysis. PLoS ONE 2012, 7, e53105. [Google Scholar] [CrossRef]
- Chmielewska-Kassassir, M.; Woźniak, L.A.; Ogrodniczek, P.; Wójcik, M. The role of peroxisome proliferator-activated receptors γ (PPARγ) in obesity and insulin resistance. Postęp. Hig. Med. Dośw. 2013, 67, 1283–1299. [Google Scholar] [CrossRef]
- Ristow, M.; Müller-Wieland, D.; Pfeiffer, A.; Krone, W.; Kahn, C.R. Obesity Associated with a Mutation in a Genetic Regulator of Adipocyte Differentiation. N. Engl. J. Med. 1998, 339, 953–959. [Google Scholar] [CrossRef]
- Kurnaz-Gomleksiz, O.; Torun, B.C.; Isbir, T.; Bulut, T.; Sokucu, N.; Yilmaz-Aydogan, H.; Canbay, E. The Role of PPAR-Gamma C161T Polymorphism in Colorectal Cancer Susceptibility. In Vivo 2022, 36, 1911–1915. [Google Scholar] [CrossRef]
- Galbete, C.; Toledo, J.; Martínez-González, M.Á.; Martínez, J.A.; Guillén-Grima, F.; Marti, A. Lifestyle Factors Modify Obesity Risk Linked to PPARG2 and FTO Variants in an Elderly Population: A Cross-Sectional Analysis in the SUN Project. Genes Nutr. 2013, 8, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Maguolo, A.; Zusi, C.; Giontella, A.; Miraglia Del Giudice, E.; Tagetti, A.; Fava, C.; Morandi, A.; Maffeis, C. Influence of Genetic Variants in FADS2 and ELOVL2 Genes on BMI and PUFAs Homeostasis in Children and Adolescents with Obesity. Int. J. Obes. 2005 2021, 45, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Khamlaoui, W.; Mehri, S.; Hammami, S.; Hammouda, S.; Chraeif, I.; Elosua, R.; Hammami, M. Association Between Genetic Variants in FADS1-FADS2 and ELOVL2 and Obesity, Lipid Traits, and Fatty Acids in Tunisian Population. Clin. Appl. Thromb. Off. J. Int. Acad. Clin. Appl. Thromb. 2020, 26, 1076029620915286. [Google Scholar] [CrossRef] [PubMed]
- Khodarahmi, M.; Javidzade, P.; Farhangi, M.A.; Hashemzehi, A.; Kahroba, H. Interplay between Fatty Acid Desaturase2 (FADS2) Rs174583 Genetic Variant and Dietary Antioxidant Capacity: Cardio-Metabolic Risk Factors in Obese Individuals. BMC Endocr. Disord. 2022, 22, 167. [Google Scholar] [CrossRef] [PubMed]
- Santana, J.d.M.; Pereira, M.; Carvalho, G.Q.; Gouveia Peluzio, M.d.C.; Drumond Louro, I.; Santos, D.B.d.; Oliveira, A.M. FADS1 and FADS2 Gene Polymorphisms Modulate the Relationship of Omega-3 and Omega-6 Fatty Acid Plasma Concentrations in Gestational Weight Gain: A NISAMI Cohort Study. Nutrients 2022, 14, 1056. [Google Scholar] [CrossRef]
- Lee, S. The Genetic and Epigenetic Association of LDL Receptor Related Protein 1B (LRP1B) Gene with Childhood Obesity. Sci. Rep. 2019, 9, 1815. [Google Scholar] [CrossRef]
- Khanal, P.; Williams, A.G.; He, L.; Stebbings, G.K.; Onambele-Pearson, G.L.; Thomis, M.; Degens, H.; Morse, C.I. Sarcopenia, Obesity, and Sarcopenic Obesity: Relationship with Skeletal Muscle Phenotypes and Single Nucleotide Polymorphisms. J. Clin. Med. 2021, 10, 4933. [Google Scholar] [CrossRef]
- Goddard, T.; Tsintzas, K.; Stephan, B.C.M.; Prado, C.M.; Mazidi, M.; Siervo, M. Sarcopenic Obesity Is Associated with Telomere Shortening: Findings from the NHANES 1999–2002. Int. J. Obes. 2005 2022, 46, 437–440. [Google Scholar] [CrossRef]
- Lu, L.; He, X.; Song, Y.; Zhuang, M.; Wu, X.; Chen, N. Prevalence and Risk Factors of Sarcopenia without Obesity and Sarcopenic Obesity among Chinese Community Older People in Suburban Area of Shanghai: A Cross-Sectional Study. Front. Aging Neurosci. 2022, 14, 1034542. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Pérez, D.; Arteaga-Pazmiño, C.; Maza-Moscoso, C.P.; Flores-Madrid, S.; Álvarez-Córdova, L. Food Insecurity as a Risk Factor of Sarcopenic Obesity in Older Adults. Front. Nutr. 2022, 9, 1040089. [Google Scholar] [CrossRef] [PubMed]



| Criteria of Sarcopenia | ||
|---|---|---|
| Organization | Criteria | Reference |
| The New Mexico Elder Health Survey, 1993–1995 (1997) (1998) | Reference population: Rosetta study (n = 883) [18] Sarcopenia definition: an appendicular skeletal muscle mass (kg)/height2 (m2) less than two standard deviations below the mean of a young reference group. | [18,19] |
| International working group on sarcopenia—consensus of geriatricians and scientists (2011) | Sarcopenia definition: the age-associated loss of skeletal muscle mass and function. Diagnosis of sarcopenia:
| [17] |
| The Foundation for the National Institutes of Health Biomarkers Consortium Sarcopenia Project, (2014) | 1. Weakness
3. ALM adjusted for BMI: M < 0.789 and F < 0.512 | [20] |
| The European Working Group on Sarcopenia in Older People 2 (EWGSOP2) (2019) | Criteria 1. Low muscle strength 2. Low muscle quantity or quality 3. Low physical performance Sarcopenia:
| [2] |
| Australia and New Zealand. The Australian and New Zealand Society for Sarcopenia and Frailty Research (ANZSSFR) Sarcopenia, (2023) | 1. Screening tools
3. sarcopenia conformation: DXA, BIA, CT, MRI | [21] |
| Disease and/or Its Definitions Used | Genetic Risk Factor | Studied Population; n | Definition Used/Conclusion | Citation |
|---|---|---|---|---|
| Obesity or impaired metabolic functions | FTO (rs9939609) | Korean adult women; n = 3335 |
| [108] |
| ADRB3 | adults; n = 265 |
| [115] | |
| schoolchildren; n = 72 | Trp64Arg and Arg64Arg allele carriers present with higher LDL-c levels and lover maximal fat oxidation rates | [117] | ||
| Obesity or impaired metabolic functions (BMI ≥ 30 kg/m2) | SLC6A14 | French-Caucasian adults; n = 1267, controls = 649 | 20649 C > T and 22510 C > G polymorphisms are associated with obesity | [127] |
| Finnish men; n = 117, controls = 182 | association of SLC6A14 polymorphisms with obesity | [126] | ||
| n = 722 Europeans | 22510 C > G allele reduces fasting fat oxidation | [131] | ||
| Sarcopenia | FTO | n = 2207 | ↓ LMI in 29 SNP of FTO | [109] |
| Sarcopenia %SMM sarcopenia definition used | FTO (rs9939609) | women > 60 years; n = 307 | ↑ sarcopenia risk | [110] |
| NOS3 (rs1799983) | ||||
| Sarcopenia | GDF5 (rs143384) | Europeans > 60 yeas; n = 256.523 | ↓ grip strength | [85] |
| Sarcopenia SMI < 29.0% in men and SMI < 22.8% in women | FADS2 (rs97384) | men and women > 50 years; n = 1599 controls = 23,391 |
| [66] |
| MYO10 (rs3157) | ||||
| KCNQ5 (rs6453647) | ||||
| DOCK5 (rs11135857) | ||||
| LRP1B (rs74659977) | ||||
| SO SMI < 6.76 kg/m2, HGS < 28.5 kg and BF% > 38% | ACTN3 (rs1815739) | older women in England; n = 307 | Sarcopenia in obese women | [151] |
| MTHFR (rs1801131) | ||||
| MTHFR (rs1537516) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazurkiewicz, Ł.; Czernikiewicz, K.; Grygiel-Górniak, B. Immunogenetic Aspects of Sarcopenic Obesity. Genes 2024, 15, 206. https://doi.org/10.3390/genes15020206
Mazurkiewicz Ł, Czernikiewicz K, Grygiel-Górniak B. Immunogenetic Aspects of Sarcopenic Obesity. Genes. 2024; 15(2):206. https://doi.org/10.3390/genes15020206
Chicago/Turabian StyleMazurkiewicz, Łukasz, Krystian Czernikiewicz, and Bogna Grygiel-Górniak. 2024. "Immunogenetic Aspects of Sarcopenic Obesity" Genes 15, no. 2: 206. https://doi.org/10.3390/genes15020206