
Efficient Lung Cancer Molecular Diagnostics by Combining Next Generation Sequencing with Reflex Idylla Genefusion Assay Testing

Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Specimens
2.2. Sample Collection for Idylla Gene Fusion Assay Validation
2.3. Validation of the Idylla Gene Fusion Assay
2.4. Performance Comparisons with Reference Methods
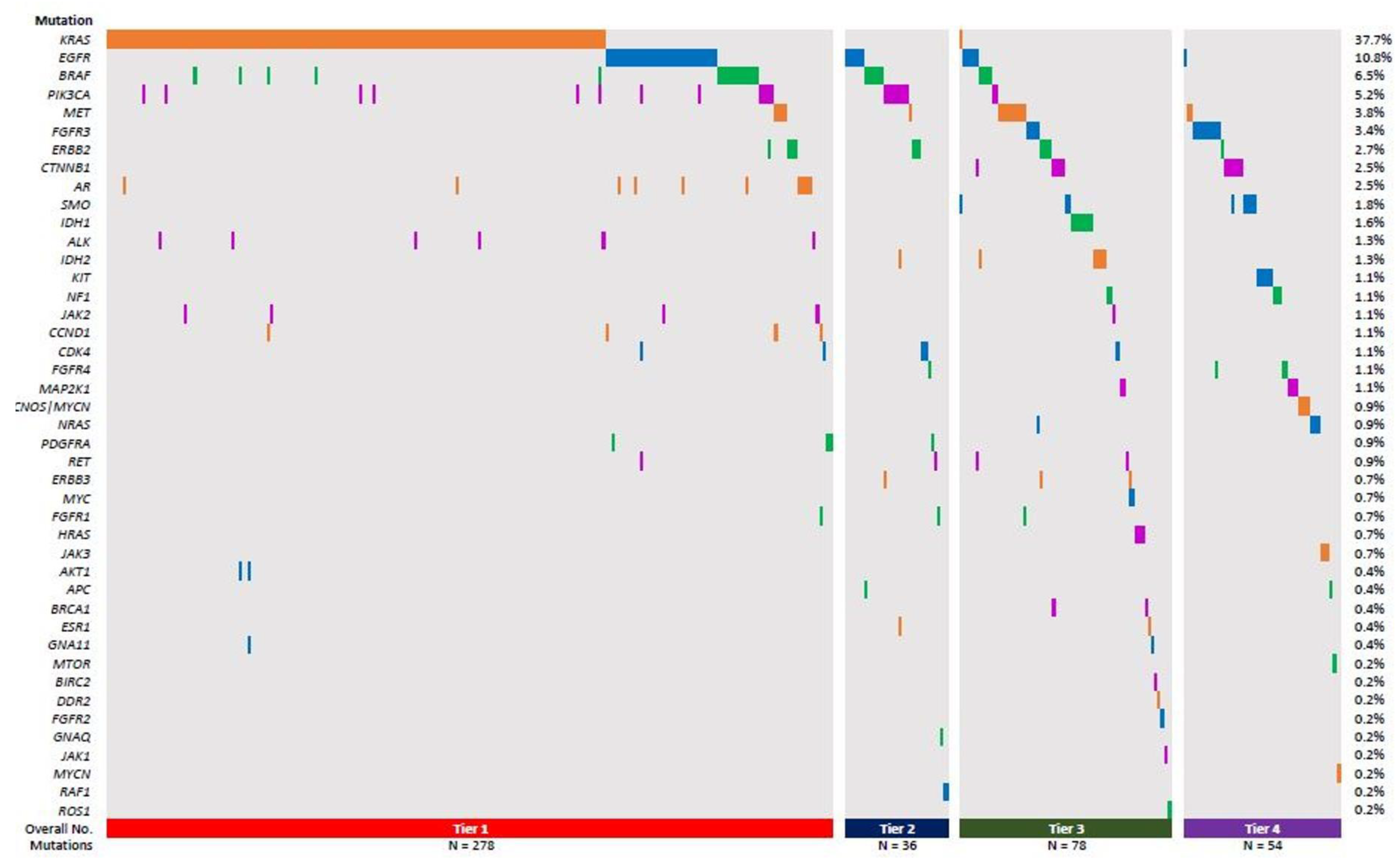
2.5. Classification of Mutations
2.6. Statistical Analysis
3. Results
3.1. ALK or ROS1 Fusion-Bearing Lung Cancer Cases Are Rare and Do Not Bear Additional SNV, or Small Indel Variants as Determined by the OFA NGS Test
3.2. Validating the Idylla Gene Fusion Assay
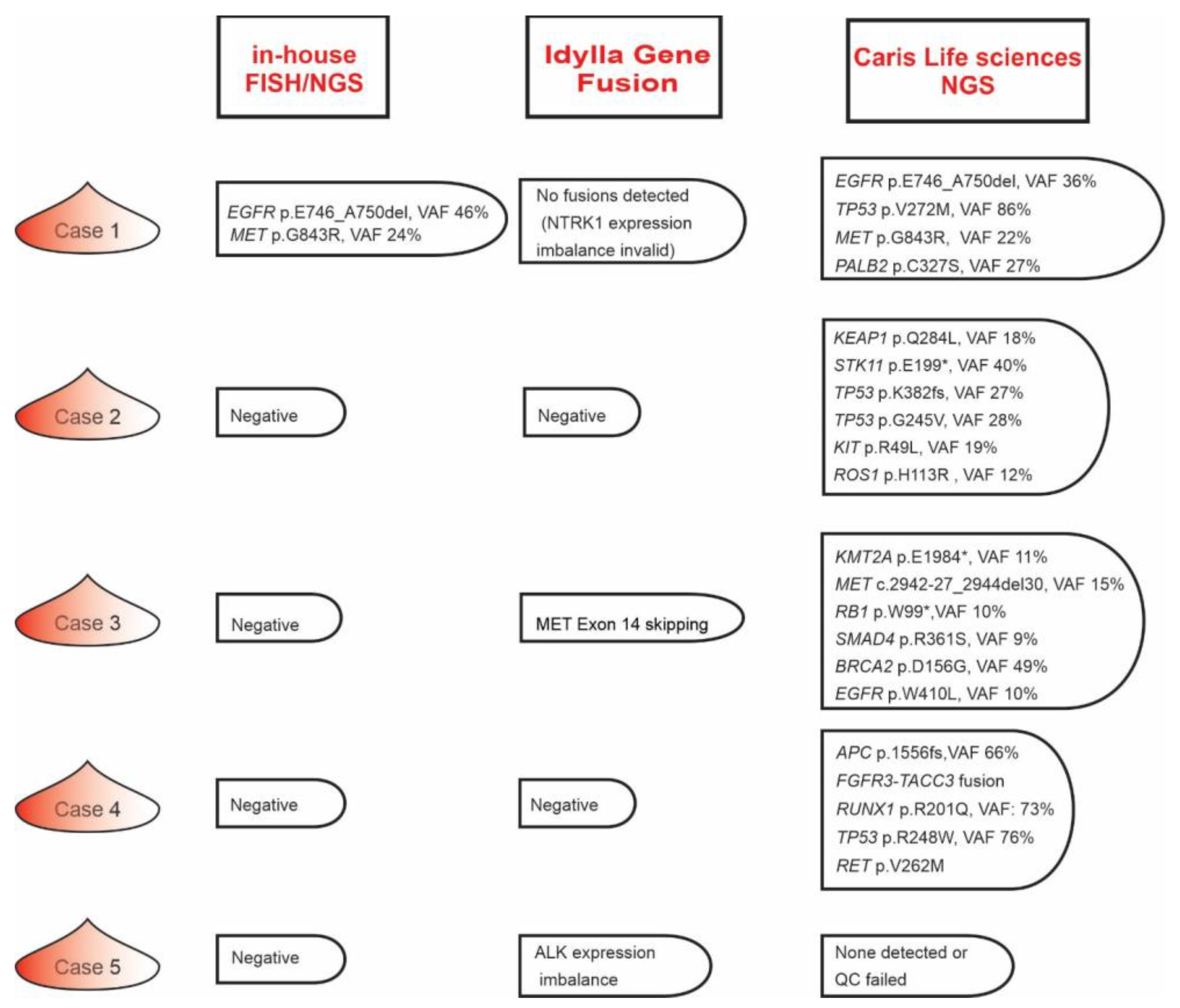
3.3. Testing the Diagnostic Utility of Idylla Genefusion Assay
3.4. Fine Tuning the Lung Cancer Molecular Testing Blueprint
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsao, A.S.; Scagliotti, G.V.; Bunn, P.A.; Carbone, D.P.; Warren, G.W.; Bai, C.; de Koning, H.J.; Yousaf-Khan, A.U.; McWilliams, A.; Tsao, M.S.; et al. Scientific Advances in Lung Cancer 2015. J. Thorac. Oncol. 2016, 11, 613–638. [Google Scholar] [CrossRef]
- Cheng, Y.; Zhang, T.; Xu, Q. Therapeutic advances in non-small cell lung cancer: Focus on clinical development of targeted therapy and immunotherapy. MedComm 2021, 2, 692–729. [Google Scholar] [CrossRef] [PubMed]
- El-Deiry, W.S.; Goldberg, R.M.; Lenz, H.J.; Shields, A.F.; Gibney, G.T.; Tan, A.R.; Brown, J.; Eisenberg, B.; Heath, E.I.; Phuphanich, S.; et al. The current state of molecular testing in the treatment of patients with solid tumors, 2019. CA Cancer J. Clin. 2019, 69, 305–343. [Google Scholar] [CrossRef] [PubMed]
- Chevallier, M.; Borgeaud, M.; Addeo, A.; Friedlaender, A. Oncogenic driver mutations in non-small cell lung cancer: Past, present and future. World J. Clin. Oncol. 2021, 12, 217–237. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.; Faivre-Finn, C.; Mok, T.; Reck, M.; Van Schil, P.; Hellmann, M. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv192–iv237. [Google Scholar] [PubMed]
- Lindeman, N.I.; Cagle, P.T.; Aisner, D.L.; Arcila, M.E.; Beasley, M.B.; Bernicker, E.H.; Colasacco, C.; Dacic, S.; Hirsch, F.R.; Kerr, K.; et al. Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment With Targeted Tyrosine Kinase Inhibitors: Guideline From the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. Arch. Pathol. Lab. Med. 2018, 142, 321–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirsch, F.R.; Scagliotti, G.V.; Mulshine, J.L.; Kwon, R.; Curran, W.J.; Wu, Y.-L.; Paz-Ares, L. Lung cancer: Current therapies and new targeted treatments. Lancet 2017, 389, 299–311. [Google Scholar] [PubMed]
- Hirsch, F.R.; Suda, K.; Wiens, J.; Bunn, P.A. New and emerging targeted treatments in advanced non-small-cell lung cancer. Lancet 2016, 388, 1012–1024. [Google Scholar]
- Shi, J.; Hua, X.; Zhu, B.; Ravichandran, S.; Wang, M.; Nguyen, C.; Brodie, S.A.; Palleschi, A.; Alloisio, M.; Pariscenti, G. Somatic genomics and clinical features of lung adenocarcinoma: A retrospective study. PLoS Med. 2016, 13, e1002162. [Google Scholar] [CrossRef] [PubMed]
- Nkosi, D.; Miller, C.A.; Jajosky, A.N.; Oltvai, Z.N. Incidental discovery of acute myeloid leukemia during liquid biopsy of a lung cancer patient. Cold Spring Harb. Mol. Case Stud. 2022, 8, a006201. [Google Scholar] [CrossRef] [PubMed]
- Jordan, E.J.; Kim, H.R.; Arcila, M.E.; Barron, D.; Chakravarty, D.; Gao, J.; Chang, M.T.; Ni, A.; Kundra, R.; Jonsson, P.; et al. Prospective Comprehensive Molecular Characterization of Lung Adenocarcinomas for Efficient Patient Matching to Approved and Emerging Therapies. Cancer Discov. 2017, 7, 596–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, Y.-H.; Barbee, J.; Yang, S.-R.; Chang, J.C.; Liang, P.; Mullaney, K.; Chan, R.; Salazar, P.; Benayed, R.; Offin, M.; et al. Clinical Utility and Performance of an Ultrarapid Multiplex RNA-Based Assay for Detection of ALK, ROS1, RET, and NTRK1/2/3 Rearrangements and MET Exon 14 Skipping Alterations. J. Mol. Diagn. 2022, 24, 642–654. [Google Scholar] [CrossRef] [PubMed]
- Sorber, L.; Van Dorst, B.; Bellon, E.; Zwaenepoel, K.; Lambin, S.; De Winne, K.; Lardon, F.; Pauwels, P.; Siozopoulou, V. NTRK Gene Fusion Detection in a Pan-Cancer Setting Using the Idylla GeneFusion Assay. J. Mol. Diagn. 2022, 24, 750–759. [Google Scholar] [CrossRef] [PubMed]
- Depoilly, T.; Garinet, S.; van Kempen, L.C.; Schuuring, E.; Clavé, S.; Bellosillo, B.; Ercolani, C.; Buglioni, S.; Siemanowski, J.; Merkelbach-Bruse, S.; et al. Multicenter Evaluation of the Idylla GeneFusion in Non–Small-Cell Lung Cancer. J. Mol. Diagn. 2022, 24, 1021–1030. [Google Scholar] [CrossRef]
- Wang, R.; Wang, L.; Li, Y.; Hu, H.; Shen, L.; Shen, X.; Pan, Y.; Ye, T.; Zhang, Y.; Luo, X.; et al. FGFR1/3 tyrosine kinase fusions define a unique molecular subtype of non-small cell lung cancer. Clin. Cancer Res. 2014, 20, 4107–4114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pham, C.; Lang, D.; Iams, W.T. Successful Treatment and Retreatment With Erdafitinib for a Patient With FGFR3-TACC3 Fusion Squamous NSCLC: A Case Report. JTO Clin. Res. Rep. 2023, 4, 100511. [Google Scholar] [CrossRef] [PubMed]
- Matthieu, G.; Charline, C.; Pascale, M.; Jean-Philippe, M.; David, C.; Arnaud, U. Performances of the Idylla GeneFusion Assay: Contribution to a rapid diagnosis of targetable gene fusions in tumour samples. J. Clin. Pathol. 2023, jcp-2023-208798. [Google Scholar] [CrossRef]
- Leone, A.; Muscarella, L.A.; Graziano, P.; Tornese, A.; Grillo, L.R.; Di Lorenzo, A.; Bronzini, M.; Scarpino, S.; Sparaneo, A.; Rossi, G. Robust Performance of the Novel Research-Use-Only Idylla GeneFusion Assay Using a Diverse Set of Pathological Samples with a Proposed 1-Day Workflow for Advanced NSCLC Evaluation. Cancers 2023, 15, 292. [Google Scholar] [CrossRef] [PubMed]
- Vail, E.; Song, J.; Xu, J.; Frye, J.S.; Kim, J.T.; Pao, A.; Schreck, R.; Aguiluz, A.S.; Zhang, W.; Alkan, S.; et al. Comparison of Large, Medium, and Small Solid Tumor Gene Panels for Detection of Clinically Actionable Mutations in Cancer. Target. Oncol. 2020, 15, 523–530. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sample Type | |
|---|---|
| Surgical resection/biopsy | 24 |
| Cytology cell blocks | 10 |
| Primary Site | |
| Lung | 15 |
| Lymph node | 7 |
| Thyroid | 6 |
| Bone | 1 |
| Ovary | 1 |
| Brain | 1 |
| Pleural fluid | 1 |
| Diaphragmatic implant | 2 |
| Tumor Cellularity | |
| >70% | 16 |
| >50–70 | 8 |
| >40–50 | 3 |
| >30–40 | 1 |
| >20–30 | 1 |
| >10–20 | 4 |
| 0–10 | 1 |
| Kinase Gene | FISH/NGS Confirmed | Idylla | Overall Concordance | ||||
|---|---|---|---|---|---|---|---|
| Positive | Negative | Positive | Negative | FS | EI | ||
| ALK fusions | 13 | 8 | 12 | 9 | 12 | 9 | 92% (12/13) |
| RET fusions | 2 | 8 | 2 | 8 | 2 | 2 | 100% (2/2) |
| ROS1 fusions | 5 | 8 | 4 | 9 | 3 | 2 | 80% (4/5) |
| MET exon 14 skipping | 6 | 8 | 6 | 8 | 6 | N/A | 100% (6/6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nkosi, D.; George, G.V.; Liu, H.; Buldo, M.; Velez, M.J.; Oltvai, Z.N. Efficient Lung Cancer Molecular Diagnostics by Combining Next Generation Sequencing with Reflex Idylla Genefusion Assay Testing. Genes 2023, 14, 1551. https://doi.org/10.3390/genes14081551
Nkosi D, George GV, Liu H, Buldo M, Velez MJ, Oltvai ZN. Efficient Lung Cancer Molecular Diagnostics by Combining Next Generation Sequencing with Reflex Idylla Genefusion Assay Testing. Genes. 2023; 14(8):1551. https://doi.org/10.3390/genes14081551
Chicago/Turabian StyleNkosi, Dingani, Giby V. George, Huijie Liu, Meghan Buldo, Moises J. Velez, and Zoltán N. Oltvai. 2023. "Efficient Lung Cancer Molecular Diagnostics by Combining Next Generation Sequencing with Reflex Idylla Genefusion Assay Testing" Genes 14, no. 8: 1551. https://doi.org/10.3390/genes14081551