
Association between Aldosterone Synthase (CYP11B2) Gene Polymorphism and Hypertension in Pashtun Ethnic Population of Khyber Pakhtunkwha, Pakistan

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Material and Methods
2.1. Subjects Characteristics
2.2. Blood Sample Collection
2.3. DNA Extraction
2.4. Whole Exome Sequencing
2.5. WES Analysis
2.6. Genotyping of CYP11B2
2.7. Statistical Analysis
3. Results
3.1. Subject Characteristics
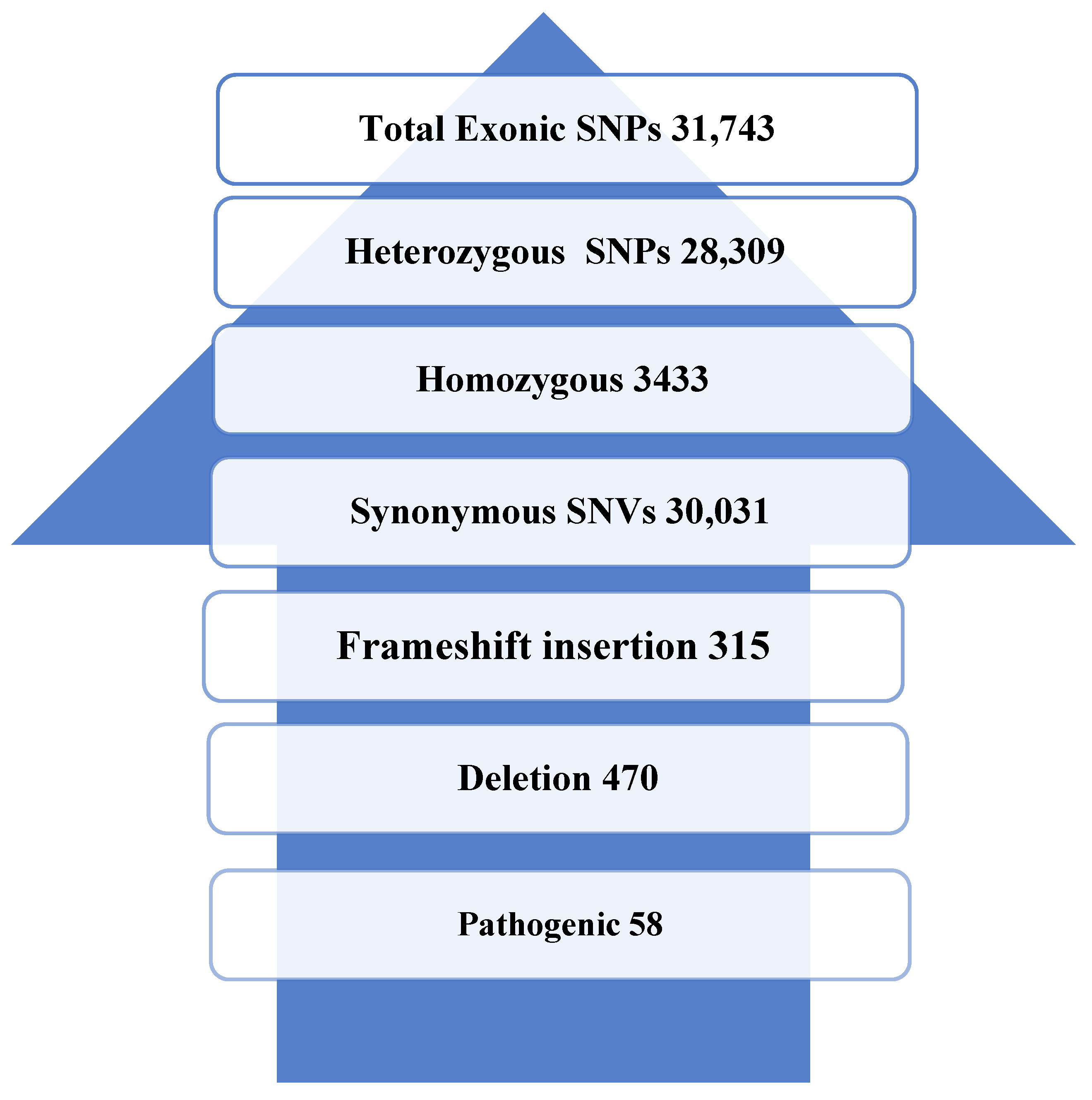
3.2. WES Results
3.3. Minor Allele Frequency Analysis (MAF)
3.4. Association between SNP and HTN
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shafi, S.T.; Shafi, T. A survey of hypertension prevalence, awareness, treatment, and control in health screening camps of rural central Punjab, Pakistan. J. Epidemiol. Glob. Health 2017, 7, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Lifton, R.P.; Gharavi, A.G.; Geller, D.S. Molecular mechanisms of human hypertension. Cell 2001, 104, 545–556. [Google Scholar] [CrossRef] [PubMed]
- Kearney, P.M.; Whelton, M.; Reynolds, K.; Muntner, P.; Whelton, P.K.; He, J. Global burden of hypertension: Analysis of worldwide data. Lancet 2005, 365, 217–223. [Google Scholar] [CrossRef]
- Chalmers, J.; MacMahon, S.; Mancia, G.; Whitworth, J.; Beilin, L.; Hansson, L.; Neal, B.; Rodgers, A.; Ni Mhurchu, C.; Clark, T. 1999 World Health Organization-International Society of Hypertension Guidelines for the Management of Hypertension. Clin. Exp. Hypertens. 1999, 21, 1009–1060. [Google Scholar] [PubMed]
- Lewington, S.; Lacey, B.; Clarke, R.; Guo, Y.; Kong, X.L.; Yang, L.; Chen, Y.; Bian, Z.; Chen, J.; Meng, J.; et al. The Burden of Hypertension and Associated Risk for Cardiovascular Mortality in China. JAMA Intern. Med. 2016, 176, 524–532. [Google Scholar] [CrossRef]
- Shah, N.; Shah, Q.; Shah, A.J. The burden and high prevalence of hypertension in Pakistani adolescents: A meta-analysis of the published studies. Arch. Public Health 2018, 76, 265–275. [Google Scholar] [CrossRef]
- D’Agostino, R.B.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel., W.B. General cardiovascular risk profile for use in primary care: The Framingham heart study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef]
- World Health Report. Reducing Risks, Promoting Healthy Life; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Yang, G.; Kong, L.; Zhao, W.; Wan, X.; Zahi, Y.; Chin, L.C.; Koplan, J.P. Emergence of chronic non-communicable diseases in China. Lancet 2008, 372, 1697–1705. [Google Scholar] [CrossRef]
- Ezzati, M.; Lopez, A.D.; Rodgers, A.; Haroon, S.V.; Murray, C.J. Selected major risk factors and global and regional burden of disease. Lancet 2002, 360, 1347–1360. [Google Scholar] [CrossRef]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R.; Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar]
- Shah, S.; Luby, S.; Rahbar, M.; Khan, A.; McCormick, J. Hypertension and its determinants among adults in high mountain villages of the Northern Areas of Pakistan. J. Hum. Hypertens. 2001, 15, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Saleem, F.; Hassali, A.A.; Shafie, A.A. Hypertension in Pakistan: Time to take some serious action. Br. J. Gen. Pract. 2010, 60, 449–450. [Google Scholar] [CrossRef] [PubMed]
- Gradman, A.H.; Alfayoumi, F. From left ventricular hypertrophy to congestive heart failure: Management of hypertensive heart disease. Prog. Cardiovasc. Dis. 2006, 48, 326–341. [Google Scholar] [CrossRef] [PubMed]
- Ishaq, M.; Memon, F.; Beaney, T.; Xia, X.; Kobeissi, E.; Poulter, N.R. May Measurement Month 2017: An analysis of the blood pressure screening campaign results in Pakistan South Asia. Eur. Heart J. 2019, 21, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Ishtiaq, S.; Ilyas, U.; Naz, S.; Altaf, R.; Afzaal, H.; Muhammad, S.A.; Zaman, S.U.; Imran, M.; Ali, F.; Sohail, F.; et al. Assessment of the risk factors of hypertension among adult and elderly group in twin cities of Pakistan. J. Pak. Med. Assoc. 2017, 67, 1664–1669. [Google Scholar]
- Kubatova, A.P.; Zotova, T.Y.; Azova, M.M.; Aissa, A.A. The ACE gene polymorism influence on the course of hypertension in the Caucasians as part of the metabolic syndrome. Vestn. Novykh Meditsinskikh Tekhnologii 2016, 23, 66–70. [Google Scholar]
- Eleni, S.; Dimitrios, K.; Vaya, P.; Areti, M.; Norma, V.; Magdalini, G. Angiotensin-I converting enzyme gene and I/D polymorphism distribution in the Greek population and a comparison with other European populations. J. Genet. 2008, 87, 91–93. [Google Scholar] [CrossRef]
- Tchelougou, D.; Kologo, J.K.; Karou, S.D.; Yaméogo, V.N.; Bisseye, C.; Djigma, F.W.; Ouermi, D.; Compaoré, T.R.; Assih, M.; Pietra, V.; et al. Renin-angiotensin system genes polymorphisms and essential hypertension in Burkina Faso, West Africa. Int. J. Hypertens. 2015, 2015, 979631. [Google Scholar] [CrossRef]
- Ismail, M.; Akhter, N.; Nasir, M.; Firesat, S.; Yub, Q.; Khaliq, S. Association between the angiotensin converting enzyme gene insertion/deletion polymorphism and essential hypertension in young Pakistan patients. J. Biochem. Mol. Bio. 2004, 35, 252–255. [Google Scholar]
- Randhawa, N.K.; Kumar, A.; Matharaoo, K.; Bhanwer, A.J.S. Association studies of angiotensin converting enzyme gene insertion/deletion polymorphism with hypertension in Punjabi population. Int. J. Hum. J. Genet. 2006, 6, 317–321. [Google Scholar] [CrossRef]
- Das, M.; Pal, S.; Ghosh, A. Angiotensin converting enzyme gene polymorphism (insertion/deletion) and hypertension in adult Asian Indians: A population-based study from Calcutta, India. Hum. Biol. 2008, 80, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Agrawal, B.K.; Goel, R.K.; Sehajpal, P.K. Angiotensin-converting enzyme gene polymorphism in hypertensive rural population of Haryana, India. J. Emerg. Trauma Shock 2009, 2, 150–154. [Google Scholar] [PubMed]
- Behravan, J.; Naghibi, M.; Mazloomi, M.A. Polymorphism of angiotensin II type 1receptor gene in Essential Hypertension in Iranian population. DARU J. Pharm. Sci. 2006, 14, 82–86. [Google Scholar]
- Tareen, M.; Shafique, K.; Mirza, S.; Arain, Z.I.; Ahmad, I.; Vart, P. Location of residence or social class, which is the stronger determinant associated with cardiovascular risk factors among Pakistani population? A cross sectional study. Rural Remote Health 2011, 11, 1700–1709. [Google Scholar] [CrossRef] [PubMed]
- Sever, P.S.; Poulter, N.R. A hypothesis for the pathogenesis of essential hypertension: The initiating factors. J. Hypertens. 1989, 7, S9–S12. [Google Scholar] [CrossRef]
- Hyder, A.A.; Morrow, R.H. Applying burden of disease methods in developing countries: A case study from Pakistan. Am. J. Public Health 2000, 909, 1235–1240. [Google Scholar]
- Hottenga, J.J.; Boomsma, D.I.; Kupper, N.; Posthuma, D.; Snieder, H.; Willemsen, G.; de Geus, E.J. Heritability and stability of resting blood pressure. Twin. Res. Hum. Genet. 2005, 8, 499–508. [Google Scholar] [CrossRef]
- Miall, W.E.; Oldham, P. The hereditary factor in arterial blood-pressure. Br. Med. J. 1963, 1, 75–80. [Google Scholar] [CrossRef]
- Brown, M.J. The causes of essential hypertension. Br. J. Clin. Pharmacol. 1996, 42, 21–27. [Google Scholar] [CrossRef]
- Williams, R.R.; Hunt, S.C.; Hopkins, P.N.; Wu, L.L.; Hasstedt, S.J.; Berry, T.D.; Barlow, G.K.; Stults, B.M.; Schumacher, M.C.; Ludwig, E.H.; et al. Genetic basis of familial dyslipidemia and hypertension. Am. J. Hypertens. 1993, 6, 319–327. [Google Scholar]
- Miyaki, K.; Htun, N.C.; Song, Y.; Ikeda, S.; Muramatsu, M.; Shimbo, T. The combined impact of 12 common variants on hypertension in Japanese men, considering GWAS results. J. Hum. Hypertens. 2012, 26, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Padmanabhan, S.; Caulfield, M.; Dominiczak, A.F. Genetic and Molecular Aspects of Hypertension. Circ. Res. 2015, 116, 937–959. [Google Scholar] [CrossRef] [PubMed]
- Pi, Y.; Zhang, L.L.; Chang, K.; Guo, L.; Liu, Y.; Li, B.H.; Cao, X.J.; Liao, S.Q.; Gao, C.Y.; Li, J.C. Lack of an association between CYP11B2 C-344T gene polymorphism and ischemic stroke: A meta-analysis of 7710 subjects. PLoS ONE 2013, 8, e68842. [Google Scholar] [CrossRef]
- Munroe, P.B.; Barnes, M.R.; Caulfield, M.J. Advances in blood pressure genomics. Circ. Res. 2013, 112, 1365–1379. [Google Scholar] [CrossRef]
- Cooper-DeHoff, R.M.; Johnson, J.A. Hypertension pharmacogenomics: In search of personalized treatment approaches. Nat. Rev. Nephrol. 2016, 12, 110–122. [Google Scholar] [CrossRef]
- Wise, I.A.; Charchar, F.J. Epigenetic modifications in essential hypertension. Int. J. Mol. Sci. 2016, 17, 451. [Google Scholar] [CrossRef]
- Lifton, R.P.; Dluhy, R.G.; Powers, M.; Rich, G.M.; Cook, S.; Ulick, S.; Lalouel, J.-M. A chimaeric llβ-hydroxylase/aldosterone synthase gene causes glucocorticoid-remediable aldosteronism and human hypertension. Nature 1992, 355, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Ehret, G.B.; Caulfield, M.J. Genes for blood pressure: An opportunity to understand hypertension. Eur. Heart J. 2013, 34, 951–961. [Google Scholar] [CrossRef]
- Jan, A.; Saeed, M.; Afridi, M.H.; Khuda, F.; Shabbir, M.; Khan, H.; Ali, S.; Hassan, M.; Samiullah, U.; Akbar, R.; et al. Association of HLA-B Gene Polymorphisms with Type 2 Diabetes in Pashtun Ethnic Population of Khyber Pakhtunkhwa, Pakistan. J. Diabetes Res. 2021, 2021, 6669731. [Google Scholar] [CrossRef]
- Rahman, N.; Zakiullah; Jan, A.; Saeed, M.; Khan, M.A.; Parveen, Z.; Iqbal, J.; Ali, S.; Shah, W.A.; Akbar, R.; et al. Association of APOE (rs429358 and rs7412) and PON1 (Q192R and L55M) Variants with Myocardial Infarction in the Pashtun Ethnic Population of Khyber Pakhtunkhwa, Pakistan. Genes 2023, 14, 687. [Google Scholar] [CrossRef]
- Jan, A.; Zakiullah; Ali, S.; Muhammad, B.; Arshad, A.; Shah, Y.; Bahadur, H.; Khan, H.; Khuda, F.; Akbar, R.; et al. Decoding type 2 diabetes mellitus genetic risk variants in Pakistani Pashtun ethnic population using the nascent whole exome sequencing and MassARRAY genotyping: A case-control association study. PLoS ONE 2023, 18, e0281070. [Google Scholar] [CrossRef] [PubMed]
- Jan, A.; Saeed, M.; Zakiullah; Akbar, R.; Khan, H. Evaluation of Type 2 Diabetes Risk Variants (Alleles) in the Pashtun Ethnic Population of Pakistan. J. ASEAN Fed. Endocr. Soc. 2023, 38, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Sham, P.; Bader, J.S.; Craig, I.; O’Donovan, M.; Owen, M. DNA pooling: A tool for large-scale association studies. Nat. Rev. Genet. 2002, 3, 862–871. [Google Scholar] [CrossRef]
- Druley, T.E.; Vallania, F.L.; Wegner, D.J.; Varley, K.E.; Knowles, O.L.; Bonds, J.A.; Robison, S.W.; Doniger, S.W.; Hamvas, A.; Cole, F.S.; et al. Quantification of rare allelic variants from pooled genomic DNA. Nat. Methods 2009, 6, 263–265. [Google Scholar] [CrossRef] [PubMed]
- Bolger, A.M.; Lohse, M.; Usadel, B. Trimmomatic: A flexible trimmer for Illumina sequence data. Bioinformatics 2014, 30, 2114–2120. [Google Scholar] [CrossRef]
- Sabiha, B.; Ali, J.; Yousafzai, Y.M.; Haider, S.A. Novel deleterious mutation in MYO7A, TH and EVC2 in two Pakistani brothers with familial deafness. Pak. J. Med. Sci. 2019, 35, 17–22. [Google Scholar] [CrossRef]
- Wang, K.; Li, M.; Hakonarson, H. ANNOVAR: Functional annotation of genetic variants from high-throughput sequencing data. Nucleic Acids Res. 2010, 38, e164. [Google Scholar] [CrossRef]
- Bellili, N.M.; Foucan, L.; Fumeron, F.; Mohammedi, K.; Travert, F.; Roussel, R.; Balkau, B.; Tichet, J.; Marre, M. Associations of the −344 T>C and the 3097 G>A polymorphisms of CYP11B2 gene with hypertension, type 2 diabetes, and metabolic syndrome in a French population. Am. J. Hypertens. 2010, 23, 660–667. [Google Scholar] [CrossRef]
- Jan, A.; Zakiullah; Khuda, F.; Akbar, R. Validation of Genome-Wide Association Studies (GWAS)-Identified Type 2 Diabetes Mellitus Risk Variants in Pakistani Pashtun Population. J. ASEAN Fed. Endocr. Soc. 2023, 38, 55–61. [Google Scholar] [CrossRef]
- Ranade, K.; Wu, K.D.; Risch, N.; Olivier, M.; Pei, D.; Hsiao, C.-F.; Chuang, L.-M.; Ho, L.-T.; Jorgenson, E.; Pesich, R.; et al. Genetic variation in aldosterone synthase predicts plasma glucose levels. Proc. Natl. Acad. Sci. USA 2001, 98, 13219–13224. [Google Scholar] [CrossRef]
- Kupari, M.; Hautanen, A.; Lankinen, L.; Koskinen, P.; Virolainen, J.; Nikkila, H.; White, P.C. Associations between human aldosterone synthase (CYP11B2) gene polymorphisms and left ventricular size, mass, and function. Circulation 1998, 97, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Hautanen, A.; Toivanen, P.; Mänttäri, M.; Tenkanen, L.; Kupari, M.; Manninen, V.; Kayes, K.M.; Rosenfeld, S.; White, P.C. Joint effects of an aldosterone synthase (CYP11B2) gene polymorphism and classic risk factors on risk of myocardial infarction. Circulation 1999, 100, 2213–2218. [Google Scholar] [CrossRef] [PubMed]
- Sookoian, S.; Gianotti, T.F.; Pirola, C. Role of the C-344T aldosterone synthase gene variant in left ventricular mass and left ventricular structure-related phenotypes. Heart 2008, 94, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.-X.; Wang, B.-J.; Ouyang, J.-Z.; Deng, X.-Y.; Ma, X.; Li, H.-Z.; Wu, Z.; Liu, S.-L.; Xu, H.; Zhang, X. Polymorphisms in CYP11B2 and CYP11B1 genes associated with primary hyperaldosteronism. Hypertens. Res. 2010, 33, 478–484. [Google Scholar] [CrossRef]
- Pojoga, L.; Gautier, S.; Blanc, H.; Guyene, T.-T.; Poirier, O.; Cambien, F.; Benetos, A. Genetic determination of plasma aldosterone levels in essential hypertension. Am. J. Hypertens. 1998, 11, 856–860. [Google Scholar] [CrossRef]
- Tsukada, K.; Ishimitsu, T.; Teranishi, M.; Saitoh, M.; Yoshii, M.; Inada, H.; Ohta, S.; Akashi, M.; Minami, J.; Ono, H.; et al. Positive association of CYP11B2 gene polymorphism with genetic predisposition to essential hypertension. J. Hum. Hypertens. 2002, 16, 789–793. [Google Scholar] [CrossRef]
- Gu, D.; Ge, D.; He, J.; Li, B.; Chen, J.; Liu, D.; Chen, R. Haplotypic analyses of the aldosterone synthase gene CYP11B2 associated with stage-2 hypertension in northern Han Chinese. Clin. Genet. 2004, 66, 409–416. [Google Scholar] [CrossRef]
- Komiya, I.; Yamada, T.; Takara, M.; Asawa, T.; Shimabukuro, M.; Nishimori, T.; Takasu, N. Lys173Arg and− 344T/C variants of CYP11B2 in Japanese patients with low-renin hypertension. Hypertension 2000, 35, 699–703. [Google Scholar] [CrossRef]
- Lim, P.O.; Macdonald, T.M.; Holloway, C.; Friel, E.; Anderson, N.H.; Dow, E.; Jung, R.T.; Davies, E.; Fraser, R.; Connell, J.M. Variation at the aldosterone synthase (CYP11B2) locus contributes to hypertension in subjects with a raised aldosterone-to-renin ratio. J. Clin. Endocrinol. Metab. 2002, 87, 4398–4402. [Google Scholar] [CrossRef]
- Li, W.; Liu, C. The −344C/T polymorphism in the CYP11B2 gene is associated with essential hypertension in the Chinese. J. Renin-Angiotensin-Aldosterone Syst. 2014, 15, 150–155. [Google Scholar] [CrossRef]
- Chandra, S.; Saluja, D.; Narang, R.; Bhatia, J.; Srivastava, K. Atrial natriuretic peptide and aldosterone synthase gene in essential hypertension: A case–control study. Gene 2015, 567, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Stowasser, M. Update in primary aldosteronism. J. Clin. Endocrinol. Metab. 2015, 100, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, F.; Yamamoto, K.; Katsuya, T.; Sugiyama, T.; Nabika, T.; Ohnaka, K.; Yamaguchi, S.; Takayanagi, R.; Ogihara, T.; Kato, N. Reevaluation of the association of seven candidate genes with blood pressure and hypertension: A replication study and meta-analysis with a larger sample size. Hypertens. Res. 2012, 35, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.R.; Kim, S.H.; Kang, S.H.; Kim, H.J.; Kong, M.H.; Hong, S.-H. Association of the K173R variant and haplotypes in the aldosterone synthase gene with essential hypertension. Genes Genom. 2014, 36, 625–632. [Google Scholar] [CrossRef]
- Niu, S.; Zhang, B.; Zhang, K.; Zhu, P.; Li, J.; Sun, Y.; He, N.; Zhang, M.; Gao, Z.; Li, X.; et al. Synergistic effects of gene polymorphisms of the renin–angiotensin–aldosterone system on essential hypertension in Kazakhs in Xinjiang. Clin. Exp. Hypertens. 2016, 38, 63–70. [Google Scholar] [CrossRef]
- Russo, P.; Lauria, F.; Loguercio, M.; Barba, G.; Arnout, J.; Cappuccio, F.P.; De Lorgeril, M.; Donati, M.B.; Iacoviello, L.; Krogh, V. −344C/T Variant in the promoter of the aldosterone synthase gene (CYP11B2) is associated with metabolic syndrome in men. Am. J. Hypertens. 2007, 20, 218–222. [Google Scholar] [CrossRef]
- Byrd, J.B.; Auchus, R.J.; White, P.C. Aldosterone synthase promoter polymorphism and cardiovascular phenotypes in a large, multiethnic population-based study. J. Investig. Med. 2015, 63, 862–866. [Google Scholar] [CrossRef]
- Chen, J.F.; Jing, J.; Tan, H.; Song, M.B.; Yu, S.Y.; Huang, L. Lack of association of CYP11B2-344C/T polymorphism with essential hypertension: A meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 9162–9167. [Google Scholar]
- Li, X.; Xie, P.; He, J.; Cai, H.; Yang, R.; Zhang, Q.; Li, B.; Qi, W.; Ma, H. CYP11B2 gene polymorphism and essential hypertension among Tibetan, Dongxiang and Han populations from northwest of China. Clin. Exp. Hypertens. 2016, 38, 375–380. [Google Scholar] [CrossRef]
- Gong, H.T.; Ma, X.L.; Du, F.H.; Du, F.H. Association of polymorphism of angiotensin converting enzyme gene and aldosterone synthase gene with essential hypertension. Chin. Gen. Pract. 2011, 14, 2609–2611. [Google Scholar]
- Wang, J.-H.; Lin, C.-M.; Wang, L.-S.; Lai, N.-S.; Chen, D.-Y.; Cherng, J.-M. Association between molecular variants of the angiotensinogen gene and hypertension in Amis tribes of eastern Taiwan. J. Formos. Med Assoc. 2002, 101. [Google Scholar]


{kind=link}
| Disease | Frequency | |
|---|---|---|
| Cases | Control | |
| Hypercholesterolemia | 7.50% | 2.83% |
| DM | 28.5% | 15.0% |
| Retinopathy | 53.0% | 0.00% |
| IHD | 8.00% | 0.00% |
| HCV | 0.00% | 0.00% |
| HBV | 0.00% | 0.00% |
| Variables | Cases n (f) | Control n (f) | p Value |
|---|---|---|---|
| Gender | |||
| Male | 130 (65%) | 173 (86.5%) | 0.051 |
| Female | 70 (35%) | 27 (13.5%) | |
| Address | |||
| Peshawar | 35 (17.5%) | 16 (16%) | 0.318 |
| Charsadda | 26 (13%) | 13 (13%) | |
| Mardan | 31 (15.5%) | 13 (13%) | |
| Kohat | 18 (9.0%) | 11 (11%) | |
| Swabi | 19 (9.5%) | 4 (4%) | |
| Nowshera | 17 (8.5%) | 5 (5%) | |
| Bannu | 18 (9.0%) | 10 (%) | |
| karak | 5 (2.5%) | 2 (25%) | |
| Dir | 22 (11%) | 10 (2%) | |
| Swat | 15 (7.5%) | 10 (10%) | |
| Occupation | |||
| Business | 30 (15.0%) | 6 (6.0%) | 0.058 |
| Govt. servant | 37 (18.5%) | 27 (27.0%) | |
| Retired | 35 (17.5.0%) | 30 (30.0%) | |
| Farming | 25 (12.5%) | 10 (10.0%) | |
| House wife | 40 (20.0%) | 15 (15.0%) | |
| Labor | 33 (16.5%) | 12 (12.0%) | |
| Family history of HTN | |||
| Yes | 133 (66.5%) | 25 (25%) | 0.003 |
| No | 67 (33.5%) | 75 (63%) | |
| Exercise | |||
| Yes | 71 (35.5%) | 43 (34%) | 0.128 |
| No | 129 (64.5%) | 57 (57%) | |
| Smoking | |||
| Yes | 96 (48%) | 20 (20%) | 0.093 |
| No | 104 (52.0%) | 80 (80%) | |
| Naswar | |||
| Yes | 130 (65.0) | 53 (53%) | 0.081 |
| No | 70 (35.0% | 47 (47%) | |
| Diet and drug compliance | |||
| Yes | 127 (63.5.5%) | 42 (42%) | 0.212 |
| No | 73 (36.5) | 58 (58%) | |
| Socioeconomic factors | |||
| Good | 52 (26.0%) | 34 (34%) | 0.314 |
| Average | 102 (51.0%) | 53 (53%) | |
| Below | 46 (23%) | 13 (13%) |
| SNP ID | Gene | Variant | Chr Position | Sift Prediction | Polyphen Prediction | Minor Frequency (%) | Read Depth | ||
|---|---|---|---|---|---|---|---|---|---|
| Cases = 200 | Control = 200 | Cases | Control | ||||||
| rs4536 | CYP11B2 | C>T | 8:143995761 | Tol | Benign | 0.10 | 0.09 | 130 | 120 |
| rs4537 | CYP11B2 | T>C | 8:143995792 | Tol | Benign | 0.23 | 0.22 | 100 | 110 |
| rs4545 | CYP11B2 | C˃T | 8:143994041 | Tol | Benign | 0.08 | 0.06 | 76 | 70 |
| rs4543 | CYP11B2 | C˃T | 8:143995743 | Tol | Benign | 0.04 | 0.03 | 150 | 140 |
| rs1799998 | CYP11B2 | T˃C | 8:142918184 | Del | Prob Dam | 0.42 | 0.30 | 250 | 210 |
| rs4539 | CYP11B2 | T>C | 8:143996539 | Tol | benign | 0.34 | 0.35 | 50 | 40 |
| rs4546 | CYP11B2 | G>A | 8:143996553 | Tol | Benign | 0.25 | 0.23 | 40 | 38 |
| rs6418 | CYP11B2 | A>G | 8:143996363 | Tol | Benign | 0.06 | 0.05 | 30 | 25 |
| SNP | Chr (Gene) | Minor Allele | Minor Allele Frequency (%) | p Value | |
|---|---|---|---|---|---|
| Cases = 200 | Control = 200 | ||||
| rs4536 | 8 (CYP11B2) | T | 10 | 9.0 | 0.343 |
| rs4537 | 8 (CYP11B2) | C | 23 | 22 | 0.492 |
| rs4545 | 8 (CYP11B2) | T | 8.0 | 5.0 | 0.483 |
| rs4543 | 8 (CYP11B2) | T | 4.0 | 3.0 | 0.432 |
| rs1799998 | 8 (CYP11B2) | T | 42 | 30 | 0.001 |
| rs4539 | 8 (CYP11B2) | C | 34 | 35 | 0.879 |
| rs4546 | 8 (CYP11B2) | A | 25 | 23 | 0.042 |
| rs6418 | 8 (CYP11B2) | G | 6.0 | 5.0 | 0.462 |
| SNP | Chr (Gene) | Minor Allele | OR | CI (95%) | p Value |
|---|---|---|---|---|---|
| rs4536 | 8 (CYP11B2) | T | 0.124 | 1.15–1.27 | 0.321 |
| rs4537 | 8 (CYP11B2) | C | 0.246 | 1.54–1.75 | 0.451 |
| rs4545 | 8 (CYP11B2) | T | 0.076 | 1.12–1.42 | 0.354 |
| rs4543 | 8 (CYP11B2) | T | 0.045 | 1.53–1.78 | 0.352 |
| rs1799998 | 8 (CYP11B2) | T | 2.257 | 1.76–2.85 | 0.045 |
| rs4539 | 8 (CYP11B2) | C | 0.754 | 1.25–1.86 | 0.765 |
| rs4546 | 8 (CYP11B2) | C | 0.053 | 1.06–1.76 | 0.071 |
| rs6418 | 8 (CYP11B2) | G | 0.872 | 1.26–2.02 | 0.327 |
| When adjusted for age, gender, smoking and family history of hypertension | |||||
| rs4536 | 8 (CYP11B2) | T | 0.214 | 1.32–1.524 | 0.348 |
| rs4537 | 8 (CYP11B2) | C | 0.112 | 1.05–1.87 | 0.254 |
| rs4545 | 8 (CYP11B2) | T | 0.056 | 1.11–1.47 | 0.483 |
| rs4543 | 8 (CYP11B2) | T | 0.035 | 1.45–1.75 | 0.434 |
| rs1799998 | 8 (CYP11B2) | T | 2.275 | 1.75–2.96 | 0.001 |
| rs4539 | 8 (CYP11B2) | C | 0.675 | 1.15–1.75 | 0.879 |
| rs4546 | 8 (CYP11B2) | C | 0.043 | 1.05–1.78 | 0.042 |
| rs6418 | 8 (CYP11B2) | G | 0.765 | 1.15–2.01 | 0.315 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shah, W.A.; Jan, A.; Khan, M.A.; Saeed, M.; Rahman, N.; Zakiullah; Afridi, M.S.; Khuda, F.; Akbar, R. Association between Aldosterone Synthase (CYP11B2) Gene Polymorphism and Hypertension in Pashtun Ethnic Population of Khyber Pakhtunkwha, Pakistan. Genes 2023, 14, 1184. https://doi.org/10.3390/genes14061184
Shah WA, Jan A, Khan MA, Saeed M, Rahman N, Zakiullah, Afridi MS, Khuda F, Akbar R. Association between Aldosterone Synthase (CYP11B2) Gene Polymorphism and Hypertension in Pashtun Ethnic Population of Khyber Pakhtunkwha, Pakistan. Genes. 2023; 14(6):1184. https://doi.org/10.3390/genes14061184
Chicago/Turabian StyleShah, Waheed Ali, Asif Jan, Muhammad Asghar Khan, Muhammad Saeed, Naveed Rahman, Zakiullah, Muhammad Sajjad Afridi, Fazli Khuda, and Rani Akbar. 2023. "Association between Aldosterone Synthase (CYP11B2) Gene Polymorphism and Hypertension in Pashtun Ethnic Population of Khyber Pakhtunkwha, Pakistan" Genes 14, no. 6: 1184. https://doi.org/10.3390/genes14061184