
Association of Surfactant Protein D Single Nucleotide Polymorphisms rs721917, rs2243639, rs3088308 with Recurrent Aphthous Stomatitis in Pakistani Population

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Sample Collection
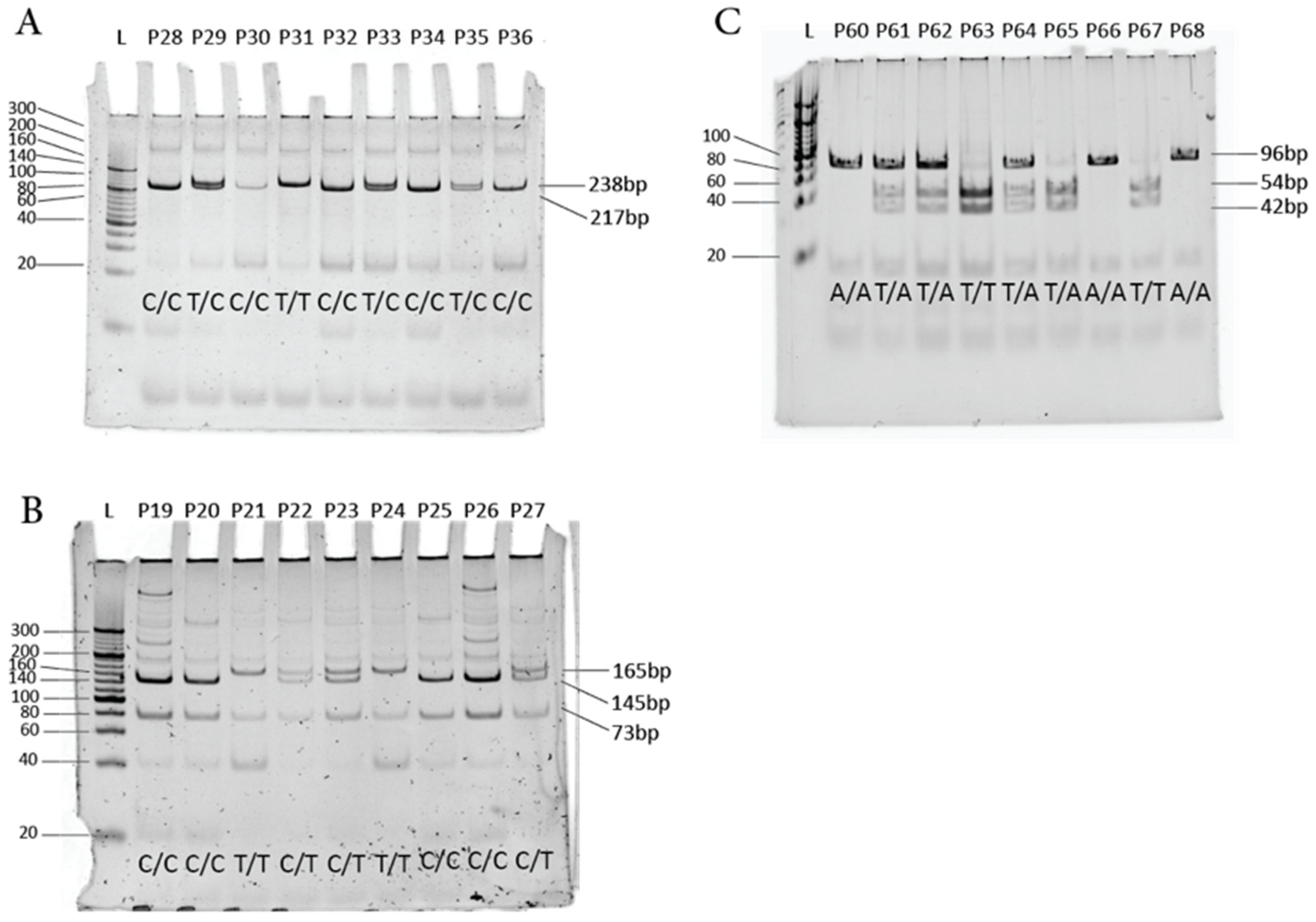
2.3. SP-D SNP Genotyping by Restriction Fragment Length Polymorphism (RFLP)
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics and RAS Establishment
3.2. Association Analysis of SP-D SNPs
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mortazavi, H.; Safi, Y.; Baharvand, M.; Rahmani, S. Diagnostic features of common oral ulcerative lesions: An updated decision tree. Int. J. Dent. 2016, 2016, e7278925. [Google Scholar] [CrossRef] [PubMed]
- Krisdapong, S.; Sheiham, A.; Tsakos, G. Impacts of recurrent aphthous stomatitis on quality of life of 12-and 15-year-old Thai children. Qual. Life Res. 2012, 21, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Montgomery-Cranny, J.A.; Wallace, A.; Rogers, H.J.; Hughes, S.C.; Hegarty, A.M.; Zaitoun, H. Management of recurrent aphthous stomatitis in children. Dent. Update 2015, 42, 564–572. [Google Scholar] [CrossRef]
- Edgar, N.R.; Saleh, D.; Miller, R.A. Recurrent aphthous stomatitis: A review. J. Clin. Aesthet. Dermatol. 2017, 10, 26–36. [Google Scholar] [PubMed]
- Goel, R.M.; Ormond, M.; Nayee, S.; Hullah, E.A.; Sanderson, J.D.; Escudier, M. A guide to oral ulceration for the medical physician. Br. J. Hosp. Med. 2015, 76, 337–342. [Google Scholar] [CrossRef]
- Liang, M.W.; Neoh, C.Y. Oral aphthosis: Management gaps and recent advances. Ann. Acad. Med. Singap. 2012, 41, 463–470. [Google Scholar] [CrossRef]
- Rivera, C. Essentials of recurrent aphthous stomatitis. Biomed. Rep. 2019, 11, 47–50. [Google Scholar] [CrossRef]
- Shi, L.; Wan, K.; Tan, M.; Yin, G.; Ge, M.; Rao, X.; He, L.; Jin, Y.; Yao, Y. Risk factors of recurrent aphthous ulceration among university students. Int. J. Clin. Exp. Med. 2015, 8, 6218–6223. [Google Scholar]
- Swain, S.K.; Gupta, S.; Sahu, M.C. Recurrent aphthous ulcers—Still a challenging clinical entity. Apollo Med. 2017, 14, 202–206. [Google Scholar]
- Zain, R.B. Oral recurrent aphthous ulcers/stomatitis: Prevalence in Malaysia and an epidemiological update. J. Oral Sci. 2000, 42, 15–19. [Google Scholar] [CrossRef]
- Stanley, H.R. Aphthous lesions. Oral Surg. Oral Med. Oral Path. 1972, 33, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Preeti, L.; Magesh, K.; Rajkumar, K.; Karthik, R. Recurrent aphthous stomatitis. J. Oral Maxillofac. Path. 2011, 15, 252. [Google Scholar] [CrossRef] [PubMed]
- Akintoye, S.O.; Greenberg, M.S. Recurrent aphthous stomatitis. Dent. Clin. 2014, 58, 281–297. [Google Scholar] [CrossRef]
- Ślebioda, Z.; Szponar, E.; Kowalska, A. Etiopathogenesis of recurrent aphthous stomatitis and the role of immunologic aspects: Literature review. Arch. Immunol. Ther. Exp. 2014, 62, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Field, E.; Allan, R. Oral ulceration–aetiopathogenesis, clinical diagnosis and management in the gastrointestinal clinic. Aliment. Pharmacol. Ther. 2003, 18, 949–962. [Google Scholar] [CrossRef]
- Khan, N.F.; Ghafoor, F.; Khan, A.A. Pathogenesis of recurrent aphthous stomatitis: A review of literature. Proc. Shaikh Zayed Postgrad. Med. Inst. 2006, 20, 113–118. [Google Scholar]
- Hamedi, S.; Sadeghpour, O.; Shamsardekani, M.R.; Amin, G.; Hajighasemali, D.; Feyzabadi, Z. The most common herbs to cure the most common oral disease: Stomatitis recurrent aphthous ulcer (RAU). Iran. Red Crescent Med. J. 2016, 18, e21694. [Google Scholar] [CrossRef]
- Bilodeau, E.A.; Lalla, R.V. Recurrent oral ulceration: Etiology, classification, management, and diagnostic algorithm. Periodontology 2000 2019, 80, 49–60. [Google Scholar] [CrossRef]
- Patil, S.; Doni, B.; Maheshwari, S. Prevalence and distribution of oral mucosal lesions in a geriatric Indian population. Can. Geriatr. J. 2015, 18, 11–14. [Google Scholar] [CrossRef]
- Feng, J.; Zhou, Z.; Shen, X.; Wang, Y.; Shi, L.; Wang, Y.; Hu, Y.; Sun, H.; Liu, W. Prevalence and distribution of oral mucosal lesions: A cross-sectional study in Shanghai, China. J. Oral Pathol. Med. 2015, 44, 490–494. [Google Scholar] [CrossRef]
- Safadi, R.A. Prevalence of recurrent aphthous ulceration in Jordanian dental patients. BMC Oral Health 2009, 9, 31. [Google Scholar] [CrossRef]
- Davatchi, F.; Tehrani-Banihashemi, A.; Jamshidi, A.R.; Chams-Davatchi, C.; Gholami, J.; Moradi, M.; Akhlaghi, M.; Foroozanfar, M.H.; Barghamdi, M.; Noorolahzadeh, E.; et al. The prevalence of oral aphthosis in a normal population in Iran: A WHO-ILAR COPCORD study. Arch. Iran Med. 2008, 11, 207–209. [Google Scholar]
- Souza, P.R.M.d.; Duquia, R.P.; Breunig, J.d.A.; Almeida, H.L.d. Recurrent aphthous stomatitis in 18-year-old adolescents-Prevalence and associated factors: A population-based study. An. Bras. Dermatol. 2017, 92, 626–629. [Google Scholar] [CrossRef] [PubMed]
- Shulman, J.D. An exploration of point, annual, and lifetime prevalence in characterizing recurrent aphthous stomatitis in USA children and youths. J. Oral Path. Med. 2004, 33, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, M.J. Prevalence of recurrent aphthous ulceration experience in patients attending Piramird dental speciality in Sulaimani City. J. Clin. Exp. Dent. 2013, 5, e89–e94. [Google Scholar] [CrossRef]
- Lakdawala, Y.A.; Masood, S.; Gulzar, I.; Batool, F.; Arshad, R. Frequency Of Apthous Ulcers—A Study. Pak. Oral Dent. J. 2017, 37, 419–421. [Google Scholar]
- Bankvall, M.; Östman, S.; Jontell, M.; Naluai, Å.S. A family-based genome-wide association study of recurrent aphthous stomatitis. Oral Dis. 2020, 26, 1696–1705. [Google Scholar] [CrossRef] [PubMed]
- Girardelli, M.; Valencic, E.; Moressa, V.; Margagliotta, R.; Tesser, A.; Pastore, S.; Spadola, O.; Athanasakis, E.; Severini, G.M.; Taddio, A. Genetic and immunologic findings in children with recurrent aphthous stomatitis with systemic inflammation. Pediatr. Rheumatol. 2021, 19, 70. [Google Scholar] [CrossRef]
- Najafi, S.; Moqadam, I.F.; Mohammadzadeh, M.; Bidoki, A.Z.; Yousefi, H.; Farhadi, E.; Tonekaboni, A.; Meighani, G.; Amirzargar, A.A.; Rezaei, N. Interleukin-10 gene polymorphisms in recurrent aphthous stomatitis. Immunol. Investig. 2014, 43, 405–409. [Google Scholar] [CrossRef]
- Guimarães, A.L.S.; Correia-Silva, J.d.F.; de Sá, A.R.; Victória, J.M.N.; Diniz, M.G.; Costa, F.d.O.; Gomez, R.S. Investigation of functional gene polymorphisms IL-1β, IL-6, IL-10 and TNF-α in individuals with recurrent aphthous stomatitis. Arch. Oral Biol. 2007, 52, 268–272. [Google Scholar] [CrossRef]
- Karakus, N.; Yigit, S.; Rustemoglu, A.; Kalkan, G.; Bozkurt, N. Effects of interleukin (IL)-6 gene polymorphisms on recurrent aphthous stomatitis. Arch. Dermatol. Res. 2014, 306, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Karasneh, J.; Bani-Hani, M.; Alkhateeb, A.; Hassan, A.; Thornhill, M. Association of MMP but not TIMP-1 gene polymorphisms with recurrent aphthous stomatitis. Oral Dis. 2014, 20, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Glas, J.; Beynon, V.; Bachstein, B.; Steckenbiller, J.; Manolis, V.; Euba, A.; Müller-Myhsok, B.; Folwaczny, M. Increased plasma concentration of surfactant protein D in chronic periodontitis independent of SFTPD genotype: Potential role as a biomarker. Tissue Antigens 2008, 72, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Stoeckelhuber, M.; Feuerhake, F.; Schmitz, C.; Wolff, K.-D.; Kesting, M.R. Immunolocalization of surfactant proteins SP-A, SP-B, SP-C, and SP-D in infantile labial glands and mucosa. J. Histochem. Cytochem. 2018, 66, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Christmann, U.; Buechner-Maxwell, V.; Witonsky, S.; Hite, R. Role of lung surfactant in respiratory disease: Current knowledge in large animal medicine. J. Vet. Intern. Med. 2009, 23, 227–242. [Google Scholar] [CrossRef] [PubMed]
- Nayak, A.; Dodagatta-Marri, E.; Tsolaki, A.G.; Kishore, U. An insight into the diverse roles of surfactant proteins, SP-A and SP-D in innate and adaptive immunity. Front. Immunol. 2012, 7, 131. [Google Scholar] [CrossRef] [PubMed]
- Madsen, J.; Kliem, A.; Tornøe, I.; Skjødt, K.; Koch, C.; Holmskov, U. Localization of lung surfactant protein D on mucosal surfaces in human tissues. J. Immunol. 2000, 164, 5866–5870. [Google Scholar] [CrossRef]
- Bräuer, L.; Möschter, S.; Beileke, S.; Jäger, K.; Garreis, F.; Paulsen, F.P. Human parotid and submandibular glands express and secrete surfactant proteins A, B, C and D. Histochem. Cell Biol. 2009, 132, 331–338. [Google Scholar] [CrossRef]
- Shakoori, T.A.; Sin, D.D.; Bokhari, S.; Ghafoor, F.; Shakoori, A. SP-D polymorphisms and the risk of COPD. Dis. Markers 2012, 33, 91–100. [Google Scholar] [CrossRef]
- Vieira, F.; Kung, J.W.; Bhatti, F. Structure, genetics and function of the pulmonary associated surfactant proteins A and D: The extra-pulmonary role of these C type lectins. Ann. Anat. 2017, 211, 184–201. [Google Scholar] [CrossRef]
- Sorensen, G.L. Surfactant protein D in respiratory and non-respiratory diseases. Front.Med. 2018, 5, 18. [Google Scholar] [CrossRef] [PubMed]
- Heidinger, K.; König, I.R.; Bohnert, A.; Kleinsteiber, A.; Hilgendorff, A.; Gortner, L.; Ziegler, A.; Chakraborty, T.; Bein, G. Polymorphisms in the human surfactant protein-D (SFTPD) gene: Strong evidence that serum levels of surfactant protein-D (SP-D) are genetically influenced. Immunogenetics 2005, 57, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Leth-Larsen, R.; Garred, P.; Jensenius, H.; Meschi, J.; Hartshorn, K.; Madsen, J.; Tornoe, I.; Madsen, H.O.; Sorensen, G.; Crouch, E.; et al. A common polymorphism in the SFTPD gene influences assembly, function, and concentration of surfactant protein D. J. Immunol. 2005, 174, 1532–1538. [Google Scholar] [CrossRef]
- Sørensen, G.L.; Hjelmborg, J.v.B.; Kyvik, K.O.; Fenger, M.; Høj, A.; Bendixen, C.; Sørensen, T.I.; Holmskov, U. Genetic and environmental influences of surfactant protein D serum levels. Am. J. Physiol. Lung Cell. Mol. Physiol. 2006, 290, L1010–L1017. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Kuan, P.J.; Xing, C.; Cronkhite, J.T.; Torres, F.; Rosenblatt, R.L.; DiMaio, J.M.; Kinch, L.N.; Grishin, N.V.; Garcia, C.K. Genetic defects in surfactant protein A2 are associated with pulmonary fibrosis and lung cancer. Am. J. Hum. Genet. 2009, 84, 52–59. [Google Scholar] [CrossRef]
- Skinner, M.L.; Schlosser, R.J.; Lathers, D.; Neal, J.G.; Woodworth, B.A.; Hall, J.; Newton, D.A.; Baatz, J.E. Innate and adaptive mediators in cystic fibrosis and allergic fungal rhinosinusitis. Am. J. Rhinol. 2007, 21, 538–541. [Google Scholar] [CrossRef]
- Todd, D.A.; Marsh, M.J.; George, A.; Henderson, N.G.; Barr, H.; Sebastian, S.; Clark, G.T.; Koster, G.; Clark, H.W.; Postle, A.D. Surfactant phospholipids, surfactant proteins, and inflammatory markers during acute lung injury in children. Pediatr. Crit. Care Med. 2010, 11, 82–91. [Google Scholar] [CrossRef]
- Hallman, M.; Haataja, R. Surfactant protein polymorphisms and neonatal lung disease. Semin. Perinatol. 2006, 30, 350–361. [Google Scholar] [CrossRef]
- Thomas, N.J.; Fan, R.; DiAngelo, S.; Hess, J.C.; Floros, J. Haplotypes of the surfactant protein genes A and D as susceptibility factors for the development of respiratory distress syndrome. Acta Paediatr. 2007, 96, 985–989. [Google Scholar] [CrossRef]
- Ohlmeier, S.; Vuolanto, M.; Toljamo, T.; Vuopala, K.; Salmenkivi, K.; Myllärniemi, M.; Kinnula, V.L. Proteomics of human lung tissue identifies surfactant protein A as a marker of chronic obstructive pulmonary disease. J. Proteome Res. 2008, 7, 5125–5132. [Google Scholar] [CrossRef]
- Puthothu, B.; Forster, J.; Heinze, J.; Heinzmann, A.; Krueger, M. Surfactant protein B polymorphisms are associated with severe respiratory syncytial virus infection, but not with asthma. BMC Pulm. Med. 2007, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Chroneos, Z.; Sever-Chroneos, Z.; Shepherd, V. Pulmonary surfactant: An immunological perspective. Cell. Physiol. Biochem. 2010, 25, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, G.L.; Bladbjerg, E.M.; Steffensen, R.; Tan, Q.; Madsen, J.; Drivsholm, T.; Holmskov, U. Association between surfactant protein D (SFTPD) gene and subclinical carotid artery atherosclerosis. Atherosclerosis 2016, 246, 7–12. [Google Scholar] [CrossRef]
- Xu, J.; Chen, Y.; Tang, L.; Teng, X.; Feng, L.; Jin, L.; Wang, G.; Wang, L. Association of surfactant protein D gene polymorphism with susceptibility to gestational diabetes mellitus: A case–control study. BMC Pregnancy Childbirth 2022, 22, 231. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Zhou, C.; Huang, F.; Duan, N.; Wang, Y.; Zheng, L.; Wang, X.; Wang, W. Relationship between dietary factors and recurrent aphthous stomatitis in China: A cross-sectional study. J. Int. Med. Res. 2021, 49, 3000605211017724. [Google Scholar] [CrossRef]
- Shahzad, H.S.F.; Ahmad, S.; Imran, H.M.; Sarwar, M.; Wattoo, Y.; Rasul, F. Association of Body Mass Index with Lifestyle Behaviours among Students of Punjab University. Int. J. Med. Dent. Sci. 2020, 9, 1823–1829. [Google Scholar]
- Krueger, M.; Puthothu, B.; Gropp, E.; Heinze, J.; Braun, S.; Heinzmann, A. Amino acid variants in Surfactant protein D are not associated with bronchial asthma. Pediatr. Allergy Immunol. 2006, 17, 77–81. [Google Scholar] [CrossRef]
- Yilmaz, S.; Cimen, K.A. Familial Behçet’s disease. Rheumatol. Int. 2010, 30, 1107–1109. [Google Scholar] [CrossRef]
- Almoznino, G.; Zini, A.; Mizrahi, Y.; Aframian, D. Elevated serum IgE in recurrent aphthous stomatitis and associations with disease characteristics. Oral Dis. 2014, 20, 386–394. [Google Scholar] [CrossRef]
- Scully, C.; Bagan, J.-V. Adverse drug reactions in the orofacial region. Crit. Rev. Oral Biol. Med. 2004, 15, 221–239. [Google Scholar] [CrossRef]
- Khan, N.F.; Saeed, M.; Chaudhary, S.; Khan, N. Haematological parameters and recurrent aphthous stomatitis. J. Coll. Physicians Surg. Pak. 2013, 23, 124–127. [Google Scholar] [PubMed]
- Azfar, M.; Qureshi, S. Awareness Regarding Oral Aphthous Ulcers and its Risk Factors Among BDS and MBBS Students-A Cross-Sectional Survey. J. Pak. Dent. Assoc. 2021, 30, 215–218. [Google Scholar] [CrossRef]
- Ship, J.; Chavez, E.M.; Doerr, P.A.; Honson, B.S.; Sarmadi, M. Recurrent Aphthout Stomatitis. Quintessence Int. 2000, 31, 95–112. [Google Scholar]
- Rathod, U.; Kulkarni, S.; Agrawal, V. Prevalence of recurrent aphthous ulcers in dental student: A questionnaire based study. Stress 2017, 180, 80–83. [Google Scholar]
- Linhartova, P.B.; Janos, J.; Slezakova, S.; Bartova, J.; Petanova, J.; Kuklinek, P.; Fassmann, A.; Dusek, L.; Holla, L.I. Recurrent aphthous stomatitis and gene variability in selected interleukins: A case–control study. Eur. J. Oral Sci. 2018, 126, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Grimaux, X.; Leducq, S.; Goupille, P.; Aubourg, A.; Miquelestorena-Standley, E.; Samimi, M. Aphthous mouth ulcers as an initial manifestation of sécukinumab-induced inflammatory bowel disease. Ann. Dermatol. Venereol. 2018, 145, 676–682. [Google Scholar] [CrossRef]
- Brignardello-Petersen, R. Patients who seek professional treatment of recurrent aphthous stomatitis probably have an increased risk of having head and neck cancer and other types of cancers. J. Am. Dent. Assoc. 2019, 150, e24. [Google Scholar] [CrossRef]
- Masood, R.; Malik, H.; Gul, L.; Imtiaz, Z.; Sajjad, U.H. Incidence of Aphthous Ulcers in All Forms of Tobacco Users, Mixed Habits and Non-Users. J. Islam. Int. Med. Coll. 2020, 15, 116–121. [Google Scholar]
- Oyetola, E.; Mogaji, I.; Aghor, T.; Ayilara, O. Pattern of presentation of oral ulcerations in patients attending an oral medicine clinic in Nigeria. Ann. Ib. Postgrad. Med. 2018, 16, 9–11. [Google Scholar]
- Queiroz, S.I.M.L.; Silva, M.V.A.d.; Medeiros, A.M.C.d.; Oliveira, P.T.d.; Gurgel, B.C.d.V.; Silveira, É.J.D.d. Recurrent aphthous ulceration: An epidemiological study of etiological factors, treatment and differential diagnosis. An. Bras. Dermatol. 2018, 93, 341–346. [Google Scholar] [CrossRef]
- Sharma, R.; Sharma, A. Recurrent Aphthous Ulcers (RAS) and Its Prevalence among People of Punjab. Int. Health Res. J. 2019, 2, 309–312. [Google Scholar] [CrossRef]
- Healy, C.M.; Williams, D.M.; Thornhill, M.H. Haematinic deficiency in recurrent aphthous stomatitis: Its prevalence and response to treatment. Oral Biosci. Med. 2004, 1, 259–266. [Google Scholar]
- Porter, S.; Kingsmill, V.; Scully, C. Audit of diagnosis and investigations in patients with recurrent aphthous stomatitis. Oral Surg. Oral Med. Oral Path. 1993, 76, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Burgan, S.Z.; Sawair, F.A.; Amarin, Z.O. Hematologic status in patients with recurrent aphthous stomatitis in Jordan. Saudi Med. J. 2006, 27, 381–384. [Google Scholar] [PubMed]
- Aslam, A.; Hassan, S.H.; Khan, D.A.; Chaudhary, M.A.G. Psychological stress associated with aphthous ulcers and temporomandibular disorders. Pak. Armed Forces Med. J. 2017, 67, 453–457. [Google Scholar]
- Arora, P.N.; Dhillon, K.S.; Rajan, S.R.; Sayal, S.K.; Das, A.L. Serum zinc levels in cutaneous disorders. Med. J. Armed Forces India 2002, 58, 304–306. [Google Scholar] [CrossRef]
- Erel, A.; Özsoy, E.; Biberoğlu, G.; Bilgihan, A.; Hasanoğlu, A.; Yis, M.; Atahan, C.; Oruk, S. Serum levels of vitamins A, C, and E, β-carotene, selenium, and zinc in patients with Behçet’s disease. Biol. Trace Elem. Res. 2003, 95, 97–106. [Google Scholar] [CrossRef]
- Khademi, H.; Shaikhiany, J. Comparisson of Serum zing level in recurrent patients and normal individuals. Dent. Res. J. 2008, 2, 2. [Google Scholar]
- Ozturk, P.; Kurutas, E.B.; Ataseven, A. Copper/zinc and copper/selenium ratios, and oxidative stress as biochemical markers in recurrent aphthous stomatitis. J. Trace Elem. Med. Biol. 2013, 27, 312–316. [Google Scholar] [CrossRef]
- Seyedmajidi, S.A.; Seyedmajidi, M.; Moghadamnia, A.; Khani, Z.; Zahedpasha, S.; Jenabian, N.; Jorsaraei, G.; Halalkhor, S.; Motallebnejad, M. Effect of zinc-deficient diet on oral tissues and periodontal indices in rats. Int. J. Mol. Cell. Med. 2014, 3, 81–87. [Google Scholar]
- Ślebioda, Z.; Krawiecka, E.; Szponar, E.; Dorocka-Bobkowska, B. Evaluation of serum zinc levels in patients with recurrent aphthous stomatitis (RAS). BMC Oral Health 2017, 17, 158. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.; Haley, J. Effect of bioactive B12 in adhering discs on aphthous ulcers. Inside Dent. 2008, 4, 60–64. [Google Scholar]
- Volkov, I.; Rudoy, I.; Freud, T.; Sardal, G.; Naimer, S.; Peleg, R.; Press, Y. Effectiveness of vitamin B12 in treating recurrent aphthous stomatitis: A randomized, double-blind, placebo-controlled trial. J. Am. Board Fam. Med. 2009, 22, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Nur’aeny, N.; Gurnida, D.A.; Suwarsa, O.; Sufiawati, I. The Impact of DNA Methylation on IL6 mRNA Levels in Hematinic Deficiency and Atopy-Associated Recurrent Aphthous Stomatitis Patients. Int. J. Dent. 2021, 2021, e5560695. [Google Scholar] [CrossRef] [PubMed]
- Sun, A.; Chen, H.M.; Cheng, S.J.; Wang, Y.P.; Chang, J.Y.F.; Wu, Y.C.; Chiang, C.P. Significant association of deficiencies of hemoglobin, iron, vitamin B12, and folic acid and high homocysteine level with recurrent aphthous stomatitis. J. Oral Path. Med. 2015, 44, 300–305. [Google Scholar] [CrossRef]
- Basirat, M.; Rabiei, M.; Ashouri, A.; Rostami, M.A. Association of lifestyle and aphthous stomatitis among dentistry students. Casp. J. Health Res. 2018, 3, 86–90. [Google Scholar] [CrossRef]
- Du, Q.; Ni, S.; Fu, Y.; Liu, S. Analysis of dietary related factors of recurrent aphthous stomatitis among college students. Evid. Based Complement. Alternat. Med. 2018, 2018, e2907812. [Google Scholar] [CrossRef]
- Baccaglini, L.; Shuster, J.J.; Theriaque, D.W.; Naveed, Z. Elevated serum insulin-like growth factor 1 in recurrent aphthous stomatitis. Clin. Exp. Dent. Res. 2019, 5, 269–275. [Google Scholar] [CrossRef]
- Darjani, A.; Joukar, F.; Naghipour, M.; Asgharnezhad, M.; Mansour-Ghanaei, F. Lifetime prevalence of recurrent aphthous stomatitis and its related factors in Northern Iranian population: The PERSIAN Guilan Cohort Study. Clin. Oral Investig. 2021, 25, 711–718. [Google Scholar] [CrossRef]
- Xiang, H.; Cheng, D.; Guo, H.; Wang, Y.; Jia, Z.; Gao, Q. Relationships of interleukin-17 polymorphisms with recurrent aphthous ulcer risk in a Han Chinese population. J. Int. Med. Res. 2020, 48, 300060520976833. [Google Scholar] [CrossRef]
- Chiang, C.-P.; Chang, J.Y.-F.; Wang, Y.-P.; Wu, Y.-H.; Wu, Y.-C.; Sun, A. Recurrent aphthous stomatitis–Etiology, serum autoantibodies, anemia, hematinic deficiencies, and management. J. Formos. Med. Assoc. 2019, 118, 1279–1289. [Google Scholar] [CrossRef] [PubMed]
- Najafi, S.; Yousefi, H.; Mohammadzadeh, M.; Bidoki, A.; Moqadam, I.F.; Farhadi, E.; Amirzargar, A.; Rezaei, N. Association study of interleukin-1 family and interleukin-6 gene single nucleotide polymorphisms in recurrent aphthous stomatitis. Int. J. Immunogenet. 2015, 42, 428–431. [Google Scholar] [CrossRef] [PubMed]
- Sun, A.; Hsieh, R.; Liu, B.; Wang, J.; Leu, J.; Wu, Y.; Chiang, C. Strong association of antiepithelial cell antibodies with HLA-DR3 or DR7 phenotype in patients with recurrent oral ulcers. J. Formos. Med. Assoc. 2000, 99, 290–294. [Google Scholar] [PubMed]
- Haagsman, H.P.; Diemel, R.V. Surfactant-associated proteins: Functions and structural variation. Comp. Biochem. Physiol. A Mol. Integr. Physiol. 2001, 129, 91–108. [Google Scholar] [CrossRef]
- Haczku, A. Protective role of the lung collectins surfactant protein A and surfactant protein D in airway inflammation. J. Allergy Clin. Immunol. 2008, 122, 861–879. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.Q.; Tao, Z.Z.; Kong, Y.G.; Xiao, B.K.; Chen, S.M.; Xu, Y.; Wang, Y.; He, Q. Association between single nucleotide polymorphisms of surfactant protein D and allergic rhinitis in Chinese patients. Tissue Antigens 2009, 73, 546–552. [Google Scholar] [CrossRef]
- Berg, K.; Madsen, H.; Garred, P.; Wiseth, R.; Gunnes, S.; Videm, V. The additive contribution from inflammatory genetic markers on the severity of cardiovascular disease. Scand. J. Immunol. 2009, 69, 36–42. [Google Scholar] [CrossRef]
- Ishii, T.; Hagiwara, K.; Kamio, K.; Ikeda, S.; Arai, T.; Mieno, M.N.; Kumasaka, T.; Muramatsu, M.; Sawabe, M.; Gemma, A. Involvement of surfactant protein D in emphysema revealed by genetic association study. Eur. J. Hum. Genet. 2012, 20, 230–235. [Google Scholar] [CrossRef]
- Pueyo, N.; Ortega, F.J.; Mercader, J.M.; Moreno-Navarrete, J.M.; Sabater, M.; Bonas, S.; Botas, P.; Delgado, E.; Ricart, W.; Martinez-Larrad, M.T. Common genetic variants of surfactant protein-D (SP-D) are associated with type 2 diabetes. PLoS ONE 2013, 8, e60468. [Google Scholar] [CrossRef]
- Ishii, T.; Hagiwara, K.; Ikeda, S.; Arai, T.; Mieno, M.N.; Kumasaka, T.; Muramatsu, M.; Sawabe, M.; Gemma, A.; Kida, K. Association between genetic variations in surfactant protein d and emphysema, interstitial pneumonia, and lung cancer in a Japanese population. J. Chronic Obstr. Pulm. Dis. 2012, 9, 409–416. [Google Scholar] [CrossRef]
- Kristiansen, M.; Frisch, M.; Madsen, H.O.; Garred, P.; Jacobsen, S. Smoking and polymorphisms of genes encoding mannose-binding lectin and surfactant protein-D in patients with rheumatoid arthritis. Rheumatol. Int. 2014, 34, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Floros, J.; Lin, H.-M.; García, A.; Salazar, M.A.; Guo, X.; DiAngelo, S.; Montano, M.; Luo, J.; Pardo, A.; Selman, M. Surfactant protein genetic marker alleles identify a subgroup of tuberculosis in a Mexican population. J. Infect. Dis. 2000, 182, 1473–1478. [Google Scholar] [CrossRef] [PubMed]
- Soto-Cárdenas, M.J.; Gandía, M.; Brito-Zerón, P.; Arias, M.T.; Armiger, N.; Bové, A.; Bosch, X.; Retamozo, S.; Akasbi, M.; Pérez-De-Lis, M. Etiopathogenic role of surfactant protein D in the clinical and immunological expression of primary Sjögren syndrome. J. Rheumatol. 2015, 42, 111–118. [Google Scholar] [CrossRef] [PubMed]
- García-Laorden, M.; Castro, F.R.d.; Solé-Violán, J.; Rajas, O.; Blanquer, J.; Borderías, L.; Aspa, J.; Briones, M.L.; Saavedra, P.; Marcos-Ramos, J.A.; et al. Influence of genetic variability at the surfactant proteins A and D in community-acquired pneumonia: A prospective, observational, genetic study. Crit. Care. 2011, 15, R57. [Google Scholar] [CrossRef]
- Gandhi, C.K.; Thomas, N.J.; Meixia, Y.; Spear, D.; Fu, C.; Zhou, S.; Wu, R.; Keim, G.; Yehya, N.; Floros, J. SNP–SNP Interactions of Surfactant Protein Genes in Persistent Respiratory Morbidity Susceptibility in Previously Healthy Children. Front. Genet. 2022, 13, e815727. [Google Scholar] [CrossRef]
- Lin, Z.; John, G.; Hegarty, J.P.; Berg, A.; Yu, W.; Wang, Y.; Kelly, A.A.; Peterson, B.Z.; Poritz, L.S.; Floros, J. Genetic Variants and Monoallelic Expression of Surfactant Protein-D in Inflammatory Bowel Disease. Ann. Hum. Genet. 2011, 75, 559–568. [Google Scholar] [CrossRef]
- Tanaka, M.; Arimura, Y.; Goto, A.; Hosokawa, M.; Nagaishi, K.; Yamashita, K.; Yamamoto, H.; Sonoda, T.; Nomura, M.; Motoya, S. Genetic Variants inSurfactant, Pulmonary-associated Protein D (SFTPD) and Japanese Susceptibility to Ulcerative Colitis. Inflamm. Bowel Dis. 2009, 15, 918–925. [Google Scholar] [CrossRef]
- Liao, Y.; Huang, C.; Wang, J.; Fan, X. Association of surfactant-associated protein D gene polymorphisms with the risk of COPD: A meta-analysis. Clinics 2019, 74, e855. [Google Scholar] [CrossRef]
- Shakoori, T.A.; Sin, D.D. SNP rs3088308 is a risk factor for poor lung function in healthy smokers. J. Pak. Med. Assoc. 2016, 66, 1137–1141. [Google Scholar]


{kind=link}
| SNP ID | rs2243639 | rs721917 | rs3088308 |
|---|---|---|---|
| SNP type | Missense variant | Missense variant | Missense variant |
| Exon involved | Fourth exon | First exon | Seventh exon |
| Position | Chr10: 79941966 (GRCh38.p13) | Chr10: 79946568 (GRCh38.p13) | Chr10: 79938112 (GRCh38.p13) |
| Cytogenetic location | 10q22.3 | 10q22.3 | 10q22.3 |
| Natural Variant # | VAR_020939 | VAR_020937 | VAR_020940 |
| Alleles | T > C/T > G forward strand | A > G forward strand | A > T forward strand |
| cDNA position | 581 | 135 | 911 |
| Protein position | 180 | 11 | 290 |
| Variation Type | Single nucleotide | Single nucleotide | Single nucleotide |
| Amino acid substitution | Thr180Ala | Met11Thr | Ser290Thr |
| SNP | Restriction Enzyme | Genotype | Product Size (bp) | Incubation Temperature/Time |
|---|---|---|---|---|
| rs2243639 | BstU1 | T/T (wild type) | 165, 73 | 60 °C/2 h |
| C/C | 145, 73 | |||
| T/C | 165, 145, 73 | |||
| rs721917 | Tail | T/T (wild type) | 238 | 37 °C/15 min |
| C/C | 217, 21 | |||
| T/C | 238, 217, 21 | |||
| rs3088308 | MnII | T/T (wild type) | 54, 42, 19 | 37 °C/15 min |
| A/A | 96, 19 | |||
| T/A | 96, 54, 42, 19 |
| SNP ID | Genotypes | Case n (%) | Control n (%) | OR | 95% (CI) | p-Value |
|---|---|---|---|---|---|---|
| rs2243639 | C/T | 36 (33.9) | 25 (23.6) | 1.67 | 0.91–3.04 | 0.09 |
| T/T | 9 (8.5) | 15 (14.2) | 0.56 | 0.23–1.34 | 0.19 | |
| C/C | 61 (57.5) | 66 (62.3) | 0.82 | 0.47–1.42 | 0.48 | |
| C allele | 158 (74.5) | 157 (74.1) | 1.02 | 0.66–1.5 | 0.91 | |
| T allele | 54 (25.5) | 55 (25.9) | 0.97 | 0.63–1.5 | 0.91 | |
| rs721917 | T/C | 50 (47.2) | 38 (35.8) | 1.5 | 0.92–2.77 | 0.09 |
| T/T | 10 (9.4) | 2 (1.8) | 5.4 | 1.15–25.35 | 0.03 | |
| C/C | 46 (43.4) | 66 (62.3) | 0.39 | 0.22–0.69 | 0.003 | |
| C allele | 142 (66.9) | 170 (80.2) | 0.50 | 0.32–0.78 | 0.002 | |
| T allele | 70 (33.0) | 42 (19.8) | 1.99 | 1.28–3.10 | 0.002 | |
| rs3088308 | T/A | 52 (49.1) | 27 (25.5) | 2.8 | 1.57–5.03 | 0.0005 |
| T/T | 35 (33.0) | 35 (33.0) | 1 | 0.56–1.77 | 1.0 | |
| A/A | 19 (17.9) | 44 (41.5) | 3.30 | 1.8–6.7 | 0.0002 | |
| T allele | 122 (57.5) | 97 (45.7) | 1.60 | 1.09–2.36 | 0.01 | |
| A allele | 90 (42.4) | 115 (54.3) | 1.62 | 1.42–3.91 | 0.01 |
| Study Parameters | T/A | T/T | A/A | A Allele | T Allele | |
|---|---|---|---|---|---|---|
| n (%) | ||||||
| Gender | Female | 36 (69.3) p = 0.001 Cl: 1.89–15.7 | 25 (71.4) p = 0.005 Cl: 1.52–11.9 | 12 (63.2) p = 0.1 Cl: 0.25–2.06 | 60 (66.7) p < 0.001 Cl: 1.65–7.58 | 86 (70.1) p < 0.001 Cl: 1.4–10.1 |
| Male | 16 (30.7) p = 0.001 Cl: 0.42–0.92 | 10 (28.8) p = 0.005 Cl: 0.34–0.87 | 7 (36.8) p = 0.1 Cl: 0.48–3.86 | 30 (33.3) p < 0.001 Cl: 0.66 –0.96 | 36 (29.5) p < 0.001 Cl: 0.26–0.93 | |
| Hb level | Low | 18 (34.6) p = 0.8 Cl: 0.47–2.36 | 11 (31.4) p = 0.3 Cl: 0.35–2.0 | 7 (36.8) p = 0.7 Cl: 0.41–3.27 | 32 (35.5) p = 0.6 Cl: 0.63–2.00 | 40 (32.8) p = 0.6 Cl: 0.49–1.56 |
| Normal | 34 (65.4) p = 0.8 Cl: 0.42–2.11 | 24 (68.6) p = 0.6 Cl: 0.49–2.8 | 12 (63.1) p = 0.7 Cl: 0.30–2.40 | 58 (64.4) p = 0.6 Cl: 0.49–1.56 | 82 (67.2) p = 0.6 Cl: 0.63–2.00 | |
| BMI | Underweight | 8 (15.4) p = 0.3 Cl: 0.46–5.04 | 3 (8.6) p = 0.5 Cl: 0.18–2.88 | 2 (10.5) p = 0.7 Cl: 0.14–3.64 | 12 (13.3) p = 0.6 Cl: 0.52–2.70 | 14 (11.4) p = 0.6 Cl: 0.36–1.92 |
| Normal | 24 (46.2) p = 0.9 Cl: 0.34–1.66 | 15 (42.8) p = 0.6 Cl: 0.52–3.01 | 10 (52.6) p = 0.5 Cl: 0.42–3.18 | 44 (48.9) p = 1.0 Cl: 0.69–2.08 | 54 (44.3) p = 0.7 Cl: 0.48–1.43 | |
| Obese | 20 (38.5) p = 0.8 Cl: 0.48–2.49 | 10 (28.6) p = 0.3 Cl: 0.36–2.24 | 7 (36.8) p = 0.8 Cl: 0.34–2.74 | 34 (37.8) p = 0.3 Cl: 0.43–1.33 | 54 (44.3) p = 0.7 Cl: 0.75–2.28 | |
| RAS types | Minor | 42 (80.7) p = 0.2 Cl: 0.71–4.36 | 25 (71.4) p = 0.9 Cl: 0.28–1.82 | 13 (68.4) p = 0.4 Cl: 0.21–1.92 | 68 (75.5) p = 0.9 Cl: 0.53–1.89 | 92 (75.4) p = 0.9 Cl: 0.52–1.86 |
| Major | - | 2 (5.7) p = 0.1 Cl: 0.49–228.5 | - | - | 4 (3.3) p = 0.1 Cl: 0.336–129.3 | |
| Herpetiform | 10 (19.3) p = 0.4 Cl: 0.27–1.70 | 8 (22.8) p = 0.8 Cl: 0.38–2.67 | 6 (31.6) p = 0.3 Cl: 0.59–5.30 | 22 (24.5) p = 0.5 Cl: 0.62–2.28 | 26 (31.3) p = 0.5 Cl: 0.43–1.59 | |
| Study Parameters | T/C | T/T | C/C | C Allele | T Allele | |
|---|---|---|---|---|---|---|
| n (%) | ||||||
| Gender | Female | 32 (64.0) p = 0.3 Cl: 0.28–1.48 | 8 (80.0) p = 0.4 Cl: 0.38–9.5 | 33 (71.8) p = 0.5 Cl: 0.54–2.93 | 98 (69.0) p = 0.9 Cl: 0.55–1.89 | 48 (68.6) p = 0.9 Cl: 0.52–1.81 |
| Male | 18 (36.0) p = 0.3 Cl: 0.007–0.03 | 2 (20.0) p = 0.4 Cl: 0.10–2.61 | 13 (28.2) p = 0.6 Cl: 0.34–1.81 | 44 (31.0) p = 0.9 Cl: 0.52–1.81 | 22 (31.4) p = 0.9 Cl: 0.55–1.89 | |
| Hb level | Low | 15 (30.0) p = 0.4 Cl: 0.31–1.60 | 5 (50.0) p = 0.2 Cl: 0.56–7.78 | 16 (34.8) p = 0.8 Cl: 0.47–2.39 | 47 (33.0) p = 0.7 Cl: 0.48–1.62 | 25 (35.7) p = 0.7 Cl: 0.61–2.04 |
| Normal | 35 (70.0) p = 0.4 Cl: 0.62–3.12 | 5 (50.0) p = 0.2 Cl: 0.12–1.77 | 30 (65.2) p = 0.8 Cl: 0.41–2.10 | 95 (67.0) p = 0.7 Cl: 0.61–2.04 | 45 (64.3) p = 0.7 Cl: 0.48–1.62 | |
| BMI | Underweight | 6 (12.0) p = 0.07 Cl: 0.29–3.05 | - | 7 (15.2) p = 0.4 Cl: 0.50–5.18 | 20 (14.0) p = 0.1 Cl: 0.72–4.98 | 6 (8.6) p = 0.1 Cl: 0.20–1.37 |
| Normal | 28 (56.0) p = 0.05 Cl: 0.9–4.6 | 2 (20.0) p = 0.1 Cl: 0.05–1.29 | 19 (41.3) p = 0.2 Cl: 0.32–1.52 | 66 (46.5) p = 0.5 Cl: 0.66–2.12 | 32 (45.7) p = 0.5 Cl: 0.47–1.50 | |
| Obese | 16 (32.0) p = 0.06 Cl: 0.21–1.03 | 8 (80.0) p = 0.02 Cl: 1.3–33 | 20 (43.5) p = 0.7 Cl: 0.52–2.51 | 46 (32.5) p = 0.1 Cl: 0.35–1.14 | 32 (45.7) p = 0.1 Cl: 0.87–2.84 | |
| RAS types | Minor | 36 (72.0) p = 0.4 Cl: 0.28–1.70 | 7 (70.0) p = 0.6 Cl: 0.17–3.07 | 37 (80.4) p = 0.5 Cl: 0.64–4.07 | 110 (77.5) p = 0.3 Cl: 0.71–2.63 | 50 (71.4) p = 0.3 Cl: 0.37–1.39 |
| Major | 1(2.0) p = 0.9 Cl: 0.06–18.43 | 1 (10.0) p = 0.1 Cl: 0.60–3.37 | - | 1 (0.7) p = 0.1 Cl: 0.02–1.55 | 3 (4.3) p = 0.1 Cl: 0.64–1.82 | |
| Herpetiform | 13 (26.0) p = 0.4 Cl: 0.57–3.58 | 2 (20.0) p = 0.4 Cl: 0.16–4.25 | 9 (19.6) p = 0.8 Cl: 0.28–1.85 | 31 (31.8) p = 0.6 Cl: 0.44–1.71 | 17 (24.3) p = 0.6 Cl: 0.58–2.25 | |
| Study Parameters | C/T | T/T | C/C | C Allele | T Allele | |
|---|---|---|---|---|---|---|
| n (%) | ||||||
| Gender | Female | 25 (69.4) p = 0.9 Cl: 0.43–2.48 | 9 (100) p = 0.2 Cl: 0.55–174 | 39 (64.0) p = 0.2 Cl: 0.2–1.3 | 123 (77.8) p = 0.7 Cl: 0.41–1.92 | 43 (79.6) p = 0.7 Cl: 0.51–2.38 |
| Male | 11 (30.6) p = 0.9 Cl: 0.40–2.29 | - | 22 (34.0) p = 0.2 Cl: 0.24–1.35 | 35 (22.2) p = 0.7 Cl: 0.51–2.38 | 11 (20.4) p = 0.7 Cl: 0.41–1.92 | |
| Hb level | Low | 12 (33.3) p = 0.9 Cl: 0.40–2.24 | 20 (32.8) p = 0.7 Cl: 0.39–1.99 | 4 (44.4) p = 0.4 Cl: 0.40–6.46 | 52 (33.0) p = 0.5 Cl: 0.43–1.58 | 20 (37.0) p = 0.5 Cl: 0.62–2.28 |
| Normal | 24 (66.7) p = 0.9 Cl: 0.44–2.44 | 41 (67.2) p = 0.7 Cl: 0.50–2.54 | 5 (55.6) p = 0.4 Cl: 0.15–2.44 | 106 (67.0) p = 0.5 Cl: 0.62–2.28 | 34 (63.0) p = 0.5 Cl: 0.43–1.58 | |
| BMI | Underweight | 3 (8.3) p = 0.4 Cl: = 0.15–2.43 | 8 (13.1) p = 0.9 Cl: 0.43–5.49 | 1 (11.1) p = 0.9 Cl: 0.11–8.57 | 19 (12.0) p = 0.5 Cl: 0.47–3.78 | 5 (9.2) p = 0.5 Cl: 0.26–2.10 |
| Normal | 17 (47.2) p = 0.8 Cl: 0.42–2.11 | 30 (49.2) p = 0.7 Cl: 0.51–2.39 | 4 (44.4) p = 0.9 Cl: 0.27–4.30 | 77 (48.7) p = 0.7 Cl: 0.59–2.04 | 25 (46.3) p = 0.7 Cl: 0.48–1.68 | |
| Obese | 16 (44.5) p = 0.5 Cl: 0.56–2.87 | 23 (37.7) p = 0.4 Cl: 0.34–1.65 | 4 (44.4) p = 0.8 Cl: 0.24–3.91 | 62 (39.2) p = 0.5 Cl: 0.43–1.50 | 24 (44.5) p = 0.5 Cl: 0.66–2.31 | |
| RAS types | Minor | 25 (69.4) p = 0.3 Cl: 0.24–1.54 | 6 (66.7) p = 0.5 Cl: 0.15–2.79 | 49 (80.4) p = 0.1 Cl: 0.75–4.5 | 123 (77.8) p = 0.1 Cl: 0.81–3.20 | 37 (68.5) p = 0.1 Cl: 0.311–1.23 |
| Major | 1 (2.8) p = 0.6 Cl: 0.11–32.4 | - | 1 (1.6) p = 0.8 Cl: 0.04–12.04 | 3 (1.9) p = 0.9 Cl: 0.10–10.1 | 1 (1.8) p = 0.9 Cl: 0.09–9.5 | |
| Herpetiform | 10 (27.8) p = 0.3 Cl: 0.60–3.92 | 3 (33.3) p = 0.4 Cl: 0.41–7.8 | 11 (18.0) p = 0.1 Cl: 0.35–1.20 | 32 (20.3) p = 0.1 Cl: 0.30–1.22 | 16 (29.6) p = 0.1 Cl: 0.81–3.31 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizvi, Z.; Choudhry, N.; Gondal, A.J.; Yasmin, N. Association of Surfactant Protein D Single Nucleotide Polymorphisms rs721917, rs2243639, rs3088308 with Recurrent Aphthous Stomatitis in Pakistani Population. Genes 2023, 14, 1119. https://doi.org/10.3390/genes14051119
Rizvi Z, Choudhry N, Gondal AJ, Yasmin N. Association of Surfactant Protein D Single Nucleotide Polymorphisms rs721917, rs2243639, rs3088308 with Recurrent Aphthous Stomatitis in Pakistani Population. Genes. 2023; 14(5):1119. https://doi.org/10.3390/genes14051119
Chicago/Turabian StyleRizvi, Zainab, Nakhshab Choudhry, Aamir Jamal Gondal, and Nighat Yasmin. 2023. "Association of Surfactant Protein D Single Nucleotide Polymorphisms rs721917, rs2243639, rs3088308 with Recurrent Aphthous Stomatitis in Pakistani Population" Genes 14, no. 5: 1119. https://doi.org/10.3390/genes14051119