
A Systematic Review of the Heterogenous Gene Expression Patterns Associated with Multidrug Chemoresistance in Conventional Osteosarcoma
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Study Selection
2.5. Data Extraction
2.6. Quality Assessment of Individual Studies
2.7. Data Synthesis
3. Results
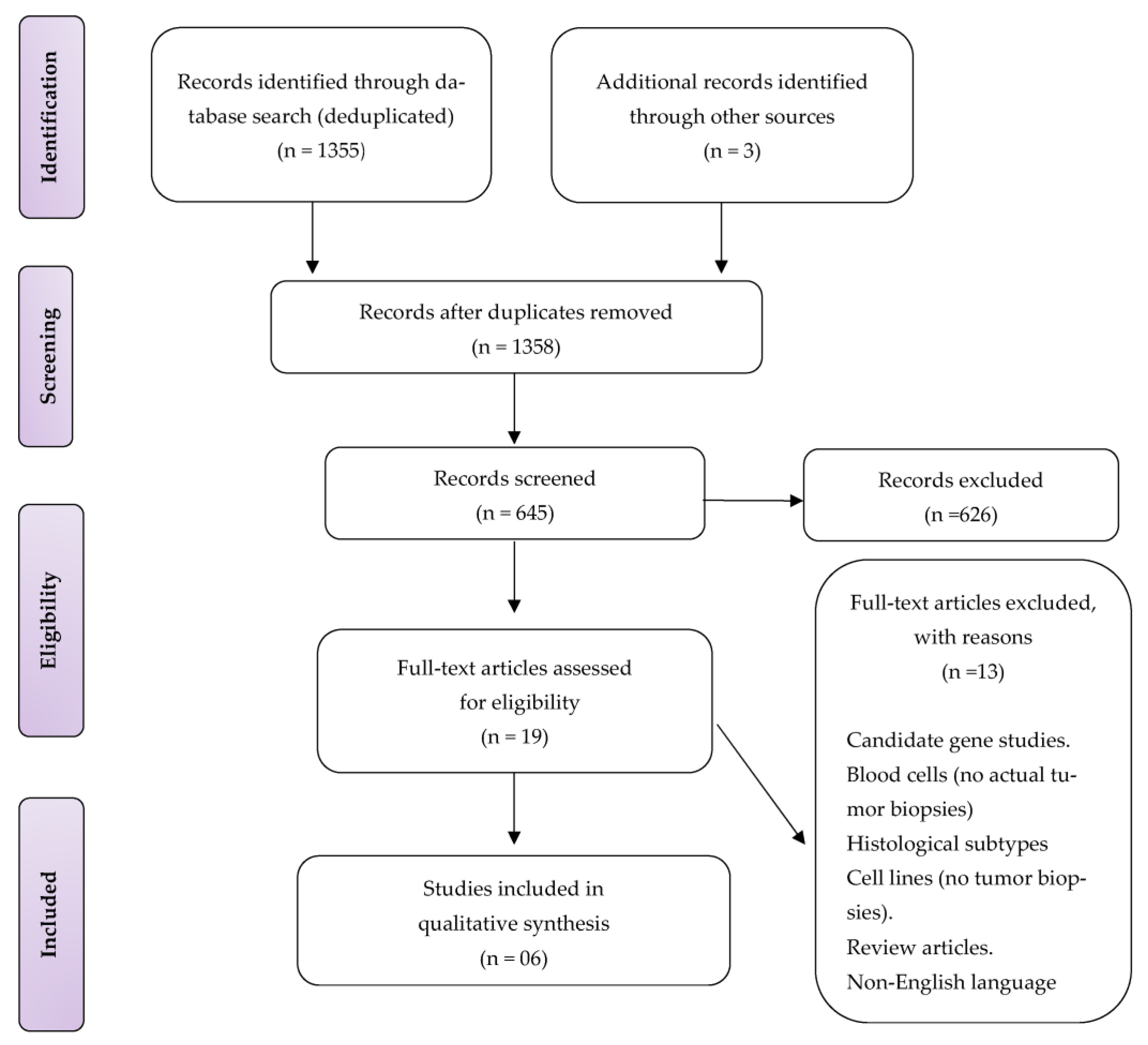
3.1. Study Selection
3.2. Study Characteristics and Interventions
3.3. Study Designs and Outcome Measures
3.4. Relationship of the Gene Expressions with Chemoresistance and Their Biological Mechanisms
3.5. Genetic Alterations in Non-Responders and Biological Mechanisms
4. Discussion
4.1. Drug Sensitivity Chemoresistance Genes
4.2. Extracellular Bone Matrix Chemoresistance Genes
4.3. Signal Transduction Pathway Chemoresistance Genes
4.4. Strengths and Limitations
4.5. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AKR1C4 | Aldo-Keto Reductase Family 1 Member C3 |
| ALDH1L2 | Aldehyde Dehydrogenase 1 Family Member L2 |
| AMPD2 | Adenosine Monophosphate Deaminase 2 |
| BCLAF1 | BCL2 Associated Transcription Factor 1 |
| CFL1 | Cofilin 1 |
| CLCN1 | Chloride Voltage-Gated Channel 1 |
| CLDN5 | Claudin 5 |
| COG3 | Component Of Oligomeric Golgi Complex 3 |
| CTSB | Cathepsin B |
| DIS3 | DIS3 Homolog, Exosome Endoribonuclease And 3′-5′ Exoribonuclease |
| DSP | Desmoplakin |
| EFNB2 | Ephrin B2 |
| ERBB4(HER4) | Erb-B2 Receptor Tyrosine Kinase 4 |
| ERK1 | Mitogen-Activated Protein Kinase 3 |
| F13A1 | Coagulation Factor XIII A Chain |
| FGF2 | Fibroblast Growth Factor 2 |
| FTH1 | Ferritin Heavy Chain 1 |
| GAPD | Glyceraldehyde-3-Phosphate Dehydrogenase |
| GPX1 | Glutathione Peroxidase 1 |
| GSTO1 | Glutathione S-Transferase Omega 1 |
| HLA-A | Major Histocompatibility Complex, Class I, A |
| HLA-B | Major Histocompatibility Complex, Class I, B |
| IFI30 | IFI30 Lysosomal Thiol Reductase |
| IL17RC | Interleukin 17 Receptor C |
| KARS | Lysyl-TRNA Synthetase 1 |
| KRT19 | Keratin 19 |
| OR52N1 | Olfactory Receptor Family 52 Subfamily N Member |
| OXCT | 3-Oxoacide CoA Transferase 1 |
| PDCD5 | Programmed Cell Death 5 |
| PDE6C | Phosphodiesterase 6C) |
| PDHX | Pyruvate Dehydrogenase Complex Component X |
| PLA2G2A | Phospholipase A2 Group IIA |
| RAB4B | RAB4B, Member RAS Oncogene Family |
| RPS 29 | Ribosomal Protein S29 |
| RPS19 | Ribosomal Protein S19 |
| RPS2 | Ribosomal Protein S2 |
| RPS20 | Ribosomal Protein S20 |
| SCN8A | Sodium Voltage-Gated Channel Alpha Subunit 8. |
| SCYA14 | Small inducible cytokine subfamily A (Cys–Cys)14 |
| SP140L | SP140 Nuclear Body Protein Like |
| SPARCL | SPARC Like 1 |
| SPP1 | Secreted Phosphoprotein. |
| STAT3 | Signal Transducer and Activator of Transcription 3 |
| STC2 | Stanniocalcin 2 |
| STK11 | Serine/Threonine Kinase 11 |
| THBS1 | Thrombospondin 1 |
| THBS4 | Thrombospondin 4 |
| TMPO | Thymopoietin |
| TMSB10 | Thymosin Beta 10 |
| TNFRSF1B | TNF Receptor Superfamily Member 1B |
| TPSAB1 | Tryptase Alpha/Beta 1 |
| TWIST1 | Twist Family BHLH Transcription Factor 1 |
| TYROBP | Transmembrane Immune Signalling Adaptor TYROBP |
| UBE2A | Ubiquitin Conjugating Enzyme E2 A |
| UBE4A | Ubiquitination Factor E4A |
| VWF | Von Willebrand Factor |
| ZNF12 | Zinc Finger Protein 12 |
References
- Fletcher, C.D.M.; Unni, K.K.; Mertens, F. (Eds.) World Health Organization Classification of Tumours: Pathology and Genetics of Tumours of Soft Tissue and Bone; IARC Press: Lyon, France, 2002; pp. 1–36. [Google Scholar]
- Klein, M.J.; Siegal, G.P. Osteosarcoma: Anatomic and histologic variants. Am. J. Clin. Pathol. 2006, 125, 555–581. [Google Scholar] [CrossRef] [PubMed]
- Bacci, G.; Balladelli, A.; Palmerini, E.; Alberghini, M.; Pollastri, P.; Galletti, S.; Mercuri, M.; Picci, P. Neoadjuvant chemotherapy for osteosarcoma of the extremities in preadolescent patients: The Rizzoli Institute experience. J. Pediatr. Haematol./Oncol. 2008, 30, 908–912. [Google Scholar] [CrossRef] [PubMed]
- Huvos, A.G.; Rosen, G.; Marcove, R.C. Primary osteogenic sarcoma: Pathologic aspects in 20 patients after treatment with chemotherapy en bloc resection, and prosthetic bone replacement. Arch. Pathol. Lab. Med. 1977, 101, 14–18. [Google Scholar] [PubMed]
- Smeland, S.; Bielack, S.S.; Whelan, J.; Bernstein, M.; Hogendoorn, P.; Krailo, M.D.; Gorlick, R.; Janeway, K.A.; Ingleby, F.C.; Anninga, J.; et al. survival and prognosis with osteosarcoma: Outcomes in more than 2000 patients in the EURAMOS-1 (European and American Osteosarcoma Study) cohort. Eur. J. Cancer 2019, 109, 36–50. [Google Scholar] [CrossRef] [Green Version]
- Marina, N.M.; Smeland, S.; Bielack, S.S.; Bernstein, M.; Jovic, G.; Krailo, M.D.; Hook, J.M.; Arndt, C.; van den Berg, H.; Brennan, B.; et al. Comparison of MAPIE versus MAP in patients with a poor response to preoperative chemotherapy for newly diagnosed high-grade osteosarcoma (EURAMOS-1): An open-label, international randomised controlled trial. Lancet Oncol. 2016, 17, 1396–1408. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; He, Z.; Duan, Y.; Wang, C.; Kamar, S.; Shi, X.; Yang, J.; Yang, J.; Zhao, N.; Han, L.; et al. Does intensified chemotherapy increase survival outcomes of osteosarcoma patients? A meta-analysis. J. Bone Oncol. 2018, 12, 54–60. [Google Scholar] [CrossRef]
- Mintz, M.B.; Sowers, R.; Brown, K.M.; Hilmer, S.C.; Mazza, B.; Huvos, A.G.; Meyers, P.A.; LaFleur, B.; McDonough, W.S.; Henry, M.M.; et al. An expression signature classifies chemotherapy-resistant pediatric osteosarcoma. Cancer Res. 2005, 65, 1748–1754. [Google Scholar] [CrossRef] [Green Version]
- Man, T.-K.; Chintagumpala, M.; Visvanathan, J.; Shen, J.; Perlaky, L.; Hicks, J.; Johnson, M.; Davino, N.; Murray, J.; Helman, L.; et al. Expression profiles of osteosarcoma that can predict response to chemotherapy. Cancer Res. 2005, 65, 8142–8150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ochi, K.; Daigo, Y.; Katagiri, T.; Nagayama, S.; Tsunoda, T.; Myoui, A.; Naka, N.; Araki, N.; Kudawara, I.; Ieguchi, M.; et al. Prediction of response to neoadjuvant chemotherapy for osteosarcoma by gene-expression profiles. Int. J. Oncol. 2004, 24, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Sun, W.; Wang, H.; Zuo, D.; Hua, Y.; Cai, Z. Research progress on the multidrug resistance mechanisms of osteosarcoma chemotherapy and reversal. Tumour Biol. 2015, 36, 1329–1338. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2000. [Google Scholar]
- Chiappetta, C.; Mancini, M.; Lessi, F.; Aretini, P.; De Gregorio, V.; Puggioni, C.; Carletti, R.; Petrozza, V.; Civita, P.; Franceschi, S.; et al. Whole-exome analysis in osteosarcoma to identify a personalized therapy. Oncotarget 2017, 8, 80416–80428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Endo-Munoz, L.; Cumming, A.; Sommerville, S.; Dickinson, I.; Saunders, N.A. Osteosarcoma characterised by reduced expression of markers of osteoclastogenesis and antigen presentation compared with normal bone. Br. J. Cancer 2010, 103, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Salas, S.; Jiguet-Jiglaire, C.; Campion, L.; Bartoli, C.; Frassineti, F.; Deville, J.-L.; Maues De Paula, A.; Forest, F.; Jézéquel, P.; Gentet, J.C.; et al. Correlation between ERK1 and STAT3 expression and chemoresistance in patients with conventional osteosarcoma. BMC Cancer 2014, 14, 606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, D. Gene expression studies using microarrays: Principles, problems, and prospects. Adv. Physiol. Educ. 2002, 26, 256–270. [Google Scholar] [CrossRef] [Green Version]
- Shyr, D.; Liu, Q. Next generation sequencing in cancer research and clinical application. Biol. Proced. Online 2013, 15, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghorbel, M.T.; Murphy, D. Suppression subtractive hybridization. Methods Mol. Biol. 2011, 789, 237–259. [Google Scholar]
- Wunder, J.S.; Bell, R.S.; Wold, L.; Andrulis, I.L. Expression of the multidrug resistance gene in osteosarcoma: A pilot study. J. Orthop. Res. 1993, 11, 396–403. [Google Scholar] [CrossRef]
- Baldini, N.; Scotlandi, K.; Barbanti-Bròdano, G.; Manara, M.C.; Maurici, D.; Bacci, G.; Bertoni, F.; Picci, P.; Sottili, S.; Campanacci, M.; et al. Expression of P-glycoprotein in high-grade osteosarcomas in relation to clinical outcome. N. Engl. J. Med. 1995, 333, 1380–1385. [Google Scholar] [CrossRef]
- Baldini, N.; Scotlandi, K.; Serra, M.; Picci, P.; Bacci, G.; Sottili, S.; Campanacci, M. P-glycoprotein expression in osteosarcoma: A basis for risk-adapted adjuvant chemotherapy. J. Orthop. Res. 1999, 17, 629–632. [Google Scholar] [CrossRef]
- He, C.; Sun, Z.; Hoffman, R.M.; Yang, Z.; Jiang, Y.; Wang, L.; Hao, Y. P-glycoprotein overexpression is associated with cisplatin resistance in human osteosarcoma. Anticancer Res. 2019, 39, 1711–1718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaseta, M.K.; Khaldi, L.; Gomatos, I.P.; Tzagarakis, G.P.; Alevizos, L.; Leandros, E.; Papagelopoulos, P.J.; Soucacos, P.N. Prognostic value of bax, bcl-2, and p53 staining in primary osteosarcoma. J. Surg. Oncol. 2008, 97, 259–266. [Google Scholar] [CrossRef]
- Wu, P.; Wu, D.; Zhao, L.; Huang, L.; Shen, G.; Huang, J.; Chai, Y. Prognostic role of STAT3 in solid tumors: A systematic review and meta-analysis. Oncotarget 2016, 7, 19863–19883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Z.; Wang, S.-L.; Chen, H.; Shen, R.-K.; Li, X.-D.; Huang, Q.-S.; Wu, C.Y.; Weng, D.F.; Lin, J.H. Clinicopathological and prognostic values of ErbB receptor family amplification in primary osteosarcoma. Scand. J. Clin. Lab. Investig. 2019, 79, 601–612. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Yang, Y.; Zhang, Y.; Liu, H.; Dou, Q. A meta-analysis on the role of pleiotrophin (PTN) as a prognostic factor in cancer. PLoS ONE 2018, 13, e0207473. [Google Scholar] [CrossRef]
- Sandberg, A.A.; Bridge, J.A. Updates on the cytogenetics and molecular genetics of bone and soft tissue tumors: Osteosarcoma and related tumors. Cancer Genet. Cytogenet. 2003, 145, 1–30. [Google Scholar] [CrossRef]
- Sadykova, L.R.; Ntekim, A.I.; Muyangwa-Semenova, M.; Rutland, C.S.; Jeyapalan, J.N.; Blatt, N.; Rizvanov, A.A. Epidemiology and Risk Factors of Osteosarcoma. Cancer Investig. 2020, 38, 259–269. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Country | Sample Size | Age (Range) | Patient Age | Sampling Strategy | Non-Conventional Osteosarcomas | Chemotherapy Drugs and Doses | Response to Chemotherapy | Genetic Analysis | Method | Newcastle-Ottawa Score |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Chiappetta et al. [14] | Italy | 8 | 11–35 | 2/8 | Primary tumour before chemotherapy | 0 | N/A | 38% | * WES + GEP | NGS (Exome probes) + Quantitative RT-PCR | 7 |
| Endo-Munoz et al. [15] | Australia | 22 | 7–67 | 16/22 | Primary tumour before chemotherapy | 0 | * Doxorubicin 25 mg m−2 andCisplatin 100 mg m−2 | 77% | * WGS + GEP | Oligonucleotide Microarray + RT-PCR | 9 |
| Man et al. [9] | USA | 20 | 11–21 | 19/20 | Primary tumour before and after chemotherapy | 0 | * High-dose methotrexate, doxorubicin, and cisplatin | 64% | * GEP | cDNA Microarray + Quantitative RT-PCR | 7 |
| Mintz et al. [8] | USA | 30 | - | - | Primary tumour before chemotherapy | 0 | * High-dose methotrexate, doxorubicin, and cisplatin | 50% | * GEP | Oligonucleotide Microarray + Quantitative RT-PCR | 9 |
| Ochi et al. [10] | Japan | 19 | 10–70 | 13/19 | Primary tumour before chemotherapy | 2 | * Doxorubicin 90 mg m−2,Cisplatin 120 mg m−2, ifosfamide 15 g m−2 | 54% | * GEP | cDNA Microarray + Semi-Quantitative RT-PCR | 7 |
| Salas et al. [16] | France | 52 | 17.4 (mean) | - | Primary tumour before chemotherapy | 0 | * High-dose methotrexate, doxorubicin | 54% | * GEP | cDNA SSH + Quantitative RT-PCR | 7 |
| Study | Number of DEGs | DEGs Associated with Non-Response |
|---|---|---|
| Chiappetta et al., 2017 [14] | 15i | ALDHIL2, BCLAF1, CLCN1, COG3, DIS3, ERB4, KARS, OR52N1, PDE6C, PDHX, SCN8A, SP140L, THBS1, UBE4A, ZNF12 |
| Endo-Munoz et al., 2010 [15] | 123ii | TMSB10, SPP1, IFI30, RPS2, HLA-B, STK11, CTSB, IL17RC, FTH1, CFL1, HLA-A, TYROBP, RPS19, RPS20, RPS 29 |
| Man et al., 2005 [9] | 45iii | TWIST1, PDCD5, OXCT, TMPO, UBE2A, EFNB2, AMPD2 |
| Mintz et al., 2005 [8] | 104ii | KRT19, PLA2G2A, SPARCL1, DSP, TPS1, GAPD, RAB4B, CLDN5, THBS4, TNFRSF11, F13A1, STC2, SCYA14, FGF2, VWF |
| Ochi et al., 2004 [10] | 60iii | AKR1C4, GPX1, GSTTLp28, |
| Salas et al., 2014 [16] | 126iii | STAT3, ERK1 |
| Biological Function | Genes Symbol | Gene Name | References |
|---|---|---|---|
| Extracellular Matrix Bone Remodelling (Osteoid Formation and Resorption) | |||
| OPG TGF-ß1 PLA2G2A TREM2 DSP ANXA2 | Osteoprotegerin Transforming Growth Factor beta 1 Phospholipase A2 Group IIA Triggering receptor expressed on myeloid cell. Desmoplakin Annexin A2 | [8,15] [8,10,15] [8] [8] [8] [8,15] | |
| Signal transduction pathways and angiogenesis | |||
| ERBB4/HER2 STAT3 AKR1C4 TWIST1 TMPOMCM2 FGFR1 PTN | Erb-B2 Receptor Tyrosine Kinase 4 Signal Transducer and Activator of Transcription 3 Aldo-keto Reductase Family 1 Member C4 Twist Family BHLH Transcription Factor 1 ThymopoietinMinichromosome Maintenance Complex Component 2 Fibroblast Growth Factor Receptor 1 Pleiotrophin | [14] [16] [10] [9] [9] [9] [9] [8] | |
| Drug sensitivity | |||
| Anti-apoptotic | BCL-2 MT1G MT1L | BCL2 Apoptosis Regulator Metallothionein 1G Metallothionein 1L, pseudogene. | [14] [8,15] [8,15] |
| Detoxification in cell | CYP4X1 GSTP1 | Cytochrome P450 Family 4 Subfamily X Member 1 Glutathione S-transferase Pi 1 | [10,15] [10] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mthethwa, P.G.; Marais, L.C.; Ramsuran, V.; Aldous, C.M. A Systematic Review of the Heterogenous Gene Expression Patterns Associated with Multidrug Chemoresistance in Conventional Osteosarcoma. Genes 2023, 14, 832. https://doi.org/10.3390/genes14040832
Mthethwa PG, Marais LC, Ramsuran V, Aldous CM. A Systematic Review of the Heterogenous Gene Expression Patterns Associated with Multidrug Chemoresistance in Conventional Osteosarcoma. Genes. 2023; 14(4):832. https://doi.org/10.3390/genes14040832
Chicago/Turabian StyleMthethwa, Phakamani Goodman, Leonard Charles Marais, Veron Ramsuran, and Collen Michelle Aldous. 2023. "A Systematic Review of the Heterogenous Gene Expression Patterns Associated with Multidrug Chemoresistance in Conventional Osteosarcoma" Genes 14, no. 4: 832. https://doi.org/10.3390/genes14040832