
When Mast Cells Run Amok: A Comprehensive Review and Case Study on Severe Neonatal Diffuse Cutaneous Mastocytosis

 ,
,
Abstract
:1. Introduction
2. Case Report
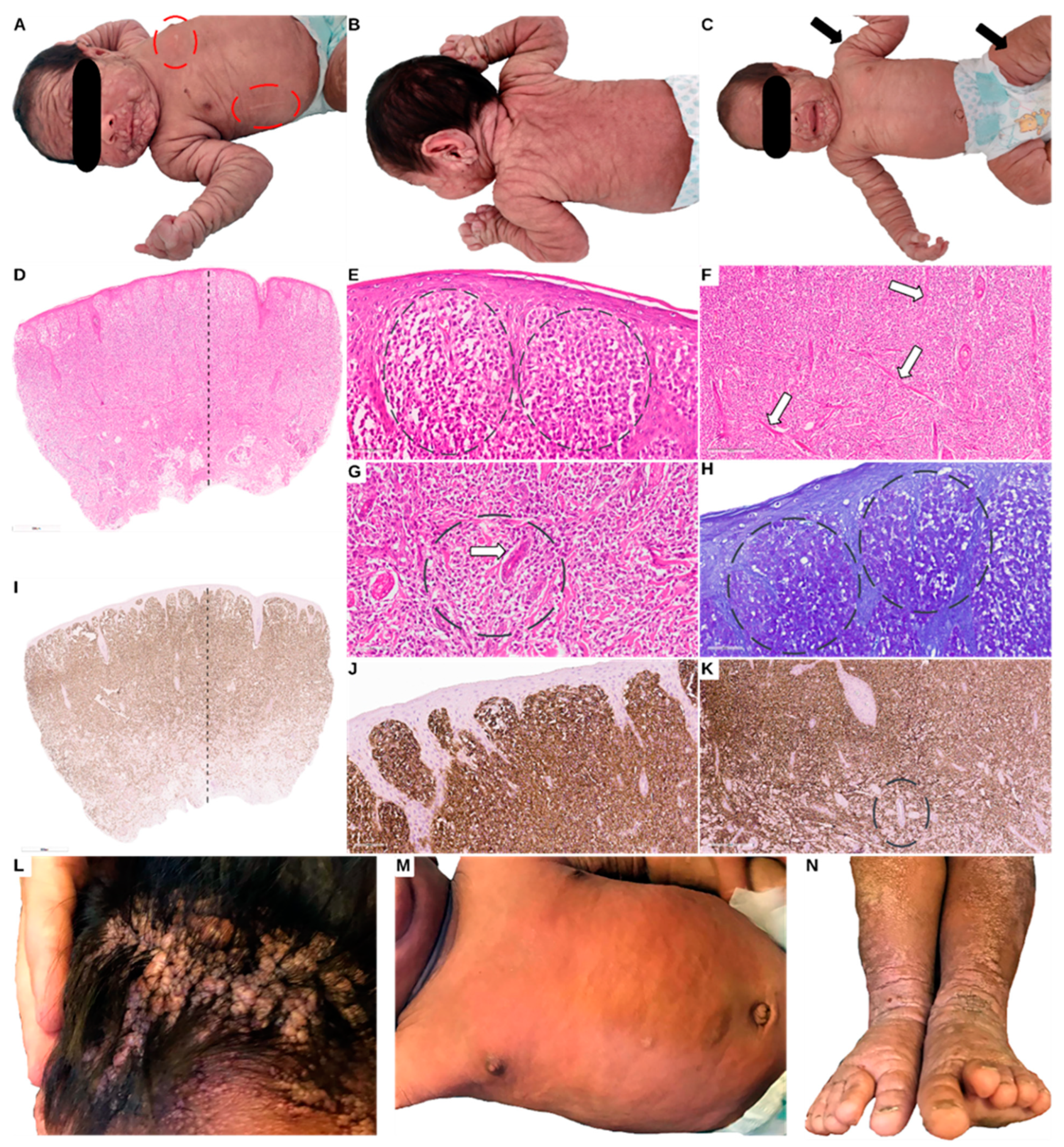
2.1. At Birth
2.2. At 2 Months of Age
2.3. At Age 4 Months
2.4. At Age 1 Year and 2 Months
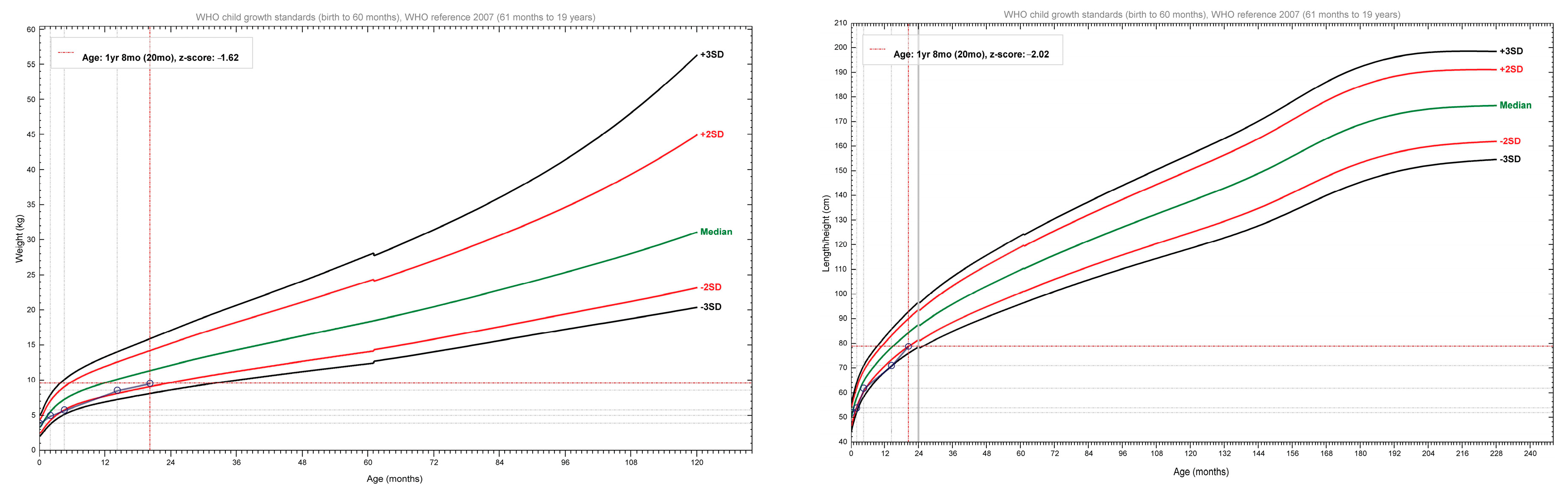
2.5. At Age 1 Year and 8 Months
2.6. At Age 2 Years
3. Literature Review
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bibi, S.; Langenfeld, F.; Jeanningros, S.; Brenet, F.; Soucie, E.; Hermine, O.; Damaj, G.; Dubreuil, P.; Arock, M. Molecular defects in mastocytosis: KIT and beyond KIT. Immunol. Allergy Clin. N. Am. 2014, 34, 239–262. [Google Scholar] [CrossRef]
- Chatterjee, A.; Ghosh, J.; Kapur, R. Mastocytosis: A mutated KIT receptor induced myeloproliferative disorder. Oncotarget 2015, 6, 18250–18264. [Google Scholar] [CrossRef]
- Frieri, M.; Quershi, M. Pediatric Mastocytosis: A Review of the Literature. Pediatr. Allergy Immunol. Pulmonol. 2013, 26, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.Y.; Sharma, V.; Worobec, A.S.; Metcalfe, D.D.; Zwick, D.C. Congenital bullous mastocytosis with myeloproliferative disorder and c-kit mutation. J. Am. Acad. Dermatol. 1998, 39, 119–121. [Google Scholar] [CrossRef] [PubMed]
- Heide, R.; Zuidema, E.; Beishuizen, A.; Hollander, J.C.D.; Van Gysel, D.; Seyger, M.M.; Pasmans, S.G.; Kakourou, T.; Oranje, A.P. Clinical Aspects of Diffuse Cutaneous Mastocytosis in Children: Two Variants. Dermatology 2009, 219, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, N.; Shapiro, N.; Bhutada, A.; Rastogi, S. c-KIT-Positive Fatal Diffuse Cutaneous Mastocytosis with Systemic Manifestations in a Neonate. J. Pediatr. Hematol. 2019, 41, e338–e340. [Google Scholar] [CrossRef]
- Jenkinson, H.A.; Lundgren, A.D.; Carter, M.C.; Diaz, L.Z.; Levy, M.L. Management of a neonate with diffuse cutaneous mastocytosis: Case report and literature review. Pediatr. Dermatol. 2019, 36, 486–489. [Google Scholar] [CrossRef]
- Wöhrl, S.; Moritz, K.B.; Bracher, A.; Fischer, G.; Stingl, G.; Loewe, R. A c-kit Mutation in Exon 18 in Familial Mastocytosis. J. Investig. Dermatol. 2013, 133, 839–841. [Google Scholar] [CrossRef]
- Andrews, S. FastQC: A Quality Control Tool for High Throughput Sequence Data. 2010. Available online: https://www.bioinformatics.babraham.ac.uk/projects/fastqc/ (accessed on 5 May 2020).
- Bolger, A.M.; Lohse, M.; Usadel, B. Trimmomatic: A flexible trimmer for Illumina sequence data. Bioinformatics 2014, 30, 2114–2120. [Google Scholar] [CrossRef]
- Smith, T.; Heger, A.; Sudbery, I. UMI-tools: Modeling sequencing errors in Unique Molecular Identifiers to improve quantification accuracy. Genome Res. 2017, 27, 491–499. [Google Scholar] [CrossRef]
- Freed, D.; Aldana, R.; Weber, J.A.; Edwards, J.S. The Sentieon Genomics Tools–A fast and accurate solution to variant calling from next-generation sequence data. bioRxiv 2017. [Google Scholar] [CrossRef]
- McLaren, W.; Gil, L.; Hunt, S.E.; Riat, H.S.; Ritchie, G.R.S.; Thormann, A.; Flicek, P.; Cunningham, F. The Ensembl Variant Effect Predictor. Genome Biol. 2016, 17, 122. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus rec-ommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Ge-Netics Med. 2015, 17, 405–423. [Google Scholar] [CrossRef]
- Willemze, R.; Ruiter, D.J.; Scheffer, E.; VAN Vloten, W.A. Diffuse cutaneous mastocytosis with multiple cutaneous mastocytomas: Report of a case with clinical, histopathological and ultrastructural aspects. Br. J. Dermatol. 1980, 102, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Oku, T.; Hashizume, H.; Yokote, R.; Sano, T.; Yamada, M. The Familial Occurrence of Bullous Mastocytosis (Diffuse Cutaneous Mastocytosis). Arch. Dermatol. 1990, 126, 1478–1484. [Google Scholar] [CrossRef] [PubMed]
- Sethuraman, G.; Handa, S.; Radotra, B.; Kumar, B. Diffuse cutaneous mastocytosis with bullae or bullous mastocytosis: A question of semantics. Pediatr. Dermatol. 1999, 16, 409–411. [Google Scholar] [CrossRef]
- Waters, W.J.; Lacson, P.S. Mast Cell Leukemia Presenting as Urticaria Pigmentosa: Report of a case. Pediatrics 1957, 19, 1033–1042. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T.; Kukita, A. A fatal case of purely cutaneous form of diffuse mastocytosis. Proc. XII Int. Cong Dermatol. 1962, 2, 1558–1561. [Google Scholar]
- Allison, J. Skin Mastocytosis Presenting as a Neonatal Bullous Eruption. Australas. J. Dermatol. 1967, 9, 83–85. [Google Scholar] [CrossRef]
- Burgoon, C.F.; Graham, J.H.; McCaffree, D.L. Mast Cell Disease: A cutaneous variant with multisystem involvement. Arch. Dermatol. 1968, 98, 590–605. [Google Scholar] [CrossRef] [PubMed]
- Klaber, M. Diffuse cutaneous mastocytosis in mother and daughter. Proc. R. Soc. Med. 1976, 69, 16–18. [Google Scholar] [CrossRef] [PubMed]
- Harrison, P.; Cook, L.; Lake, H.; Shuster, S. Diffuse cutaneous mastocytosis: A report of neonatal onset. Acta Derm.-Venereol. 1979, 59, 541–543. [Google Scholar] [CrossRef] [PubMed]
- Enomoto, U.; Kusakabe, H.; Matsumura, T.; Kuno, T.; Tamai, H.; Kiyokane, K. Diffuse cutaneous mastocytosis responding to cyproheptadine. Clin. Exp. Dermatol. 1999, 24, 16–18. [Google Scholar] [CrossRef] [PubMed]
- Hannaford, R.; Rogers, M. Presentation of cutaneous mastocytosis in 173 children. Australas. J. Dermatol. 2001, 42, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, E.I.; Faria, B.C.; Cartell, A.; Santos, B.A.; Cestari, T.F. Systemic mastocytosis in childhood: Report of 3 cases. J. Pediatr. 2002, 78, 176–180. [Google Scholar] [CrossRef]
- Mann, C.; Sepp, N.; Simma, B. Congenital cutaneous mastocytosis. J. Pediatr. 2004, 145, 134. [Google Scholar] [CrossRef]
- Walker, T.; von Komorowski, G.; Scheurlen, W.; Dorn-Beineke, A.; Back, W.; Bayerl, C. Neonatal Mastocytosis with Pachydermic Bullous Skin without c-Kit 816 Mutation. Dermatology 2005, 212, 70–72. [Google Scholar] [CrossRef]
- Duckworth, A.K.; Bhatti, A.; Barnes, C. Diffuse cutaneous mastocytosis in fraternal twins. Int. J. Dermatol. 2009, 48, 170–172. [Google Scholar] [CrossRef] [PubMed]
- Koga, H.; Kokubo, T.; Akaishi, M.; Iida, K.; Korematsu, S. Neonatal Onset Diffuse Cutaneous Mastocytosis: A Case Report and Review of the Literature. Pediatr. Dermatol. 2010, 28, 542–546. [Google Scholar] [CrossRef]
- Lange, M.; Niedoszytko, M.; Nedoszytko, B.; Łata, J.; Trzeciak, M.; Biernat, W. Diffuse cutaneous mastocytosis: Analysis of 10 cases and a brief review of the literature. J. Eur. Acad. Dermatol. Venereol. 2011, 26, 1565–1571. [Google Scholar] [CrossRef]
- Ghiasi, M.; Ghanadan, A.; Jesri, S.B.; Sotudeh, S.; Ramyar, A. Diffuse cutaneous mastocytosis: Report of a severe case with fatal outcome. Dermatol. Online J. 2011, 17, 7. [Google Scholar] [CrossRef] [PubMed]
- Park, M.-N.; Kim, G.-A.; Chey, M.J.; Shim, G.H. A Case of Diffuse Cutaneous Mastocytosis in a Newborn. Korean J. Perinatol. 2014, 25, 105–109. [Google Scholar] [CrossRef]
- Folch, B.S.; Almaraz, R.L.; González, R.S.; Heras, B.M.d.L. Diffuse cutaneous mastocytosis. Presentation of 3 cases and therapeutic management review. An. Pediatr. A (Engl. Ed.) 2016, 5, 286–288. [Google Scholar] [CrossRef]
- Turnbull, L.; Calhoun, D.A.; Agarwal, V.; Drehner, D.; Chua, C. Congenital Mastocytosis: Case Report and Review of the Literature. Cureus 2020, 12, 12. [Google Scholar] [CrossRef] [PubMed]
- Trevisan, G.; Pauluzzi, P.; Gatti, A.; Semeraro, A. Familial mastocytosis associated with neurosensory deafness. J. Eur. Acad. Dermatol. Venereol. 2000, 14, 119–122. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Present Case | Case Aggregation of DCM from the Literature | |
|---|---|---|
| Number of cases | 1 | 31 |
| Sex (Male/Female) | M | 19 M, 11 F, 1 NA |
| Darier sign (positive, negative or no information) | Positive | 20 positive, 1 negative, 10 and NA |
| Systemic involvement (SI) | Yes | 9 had SI, 13 without SI, and 9 NA |
| Positive (elevated) blood and/or urine markers | Yes, elevated serum tryptase | 15 had elevated markers, 7 had normal markers, and 9 NA |
| Bone-marrow biopsy (BMB) | Yes—no involvement | 7 had BMB, 13 without BMB, and 11 NA |
| Out of the 7 that had BMB, 4 had BM involvement | ||
| Biopsy | Yes—skin | 27 had a biopsy performed (with skin being the most common), 2 without biopsy, 2 NA |
| Special stains | Toluidine Blue | 12 cases had special stains, (Toluidine Blue and Giemsa most used), 8 had no special stains, 11 NA |
| Ultrastructural analysis (UA) | No UA | 2 had UA, 26 without UA, and 3 NA |
| IHC | CD117 (c-kit)—diffuse positivity | 5 had IHC for CD117, 3 had IHC for Tryptase, 9 no IHC performed, and 14 NA |
| Variant testing | KIT—c.1504_1509dup p.(Ala502_Tyr503dup) | 3 cases with KIT p.(Asp8l6Val), KIT dup A502Y503 |
| Treatment | Cromoglycate | The main treatment was antihistamines and/or cromoglycate (23 cases) with systemic corticoids for systemic manifestations (8 cases), 1 case with Vitamin K and 1 case with iron preparation, and 6 cases with NA |
| Follow-up | 2 years | The longest follow-up was 27 years |
| Complications | Splenomegaly and cervical adenopathy | Complications were reported in 17 cases with the most common complication being spleen and/or hepatomegaly, 10 had none reported, 4 NA |
| Vital status at follow-up (alive or dead) | Alive | 24 were alive at follow-up, 6 were dead with 1 death of unknown cause |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olteanu, E.-G.; Bataneant, M.; Puiu, M.; Chirita-Emandi, A. When Mast Cells Run Amok: A Comprehensive Review and Case Study on Severe Neonatal Diffuse Cutaneous Mastocytosis. Genes 2023, 14, 2021. https://doi.org/10.3390/genes14112021
Olteanu E-G, Bataneant M, Puiu M, Chirita-Emandi A. When Mast Cells Run Amok: A Comprehensive Review and Case Study on Severe Neonatal Diffuse Cutaneous Mastocytosis. Genes. 2023; 14(11):2021. https://doi.org/10.3390/genes14112021
Chicago/Turabian StyleOlteanu, Emilian-Gheorghe, Mihaela Bataneant, Maria Puiu, and Adela Chirita-Emandi. 2023. "When Mast Cells Run Amok: A Comprehensive Review and Case Study on Severe Neonatal Diffuse Cutaneous Mastocytosis" Genes 14, no. 11: 2021. https://doi.org/10.3390/genes14112021