
Sex Differences in the Efficacy of Mediterranean Diet Treatment: A Nutrigenomics Pilot Study
 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Dietary Assessment and Mediterranean Diet Treatment
2.3. Evaluation of Body Composition
2.4. Blood Analyses and Indexes
2.5. RNA Extraction and RT-PCR
2.6. Statistical Analyses
3. Results
3.1. Basic Characteristics among Females and Males
3.2. Effect of Intervention on Body Composition and Clinical Parameters in Females and Males
3.3. Effect of Intervention on Biochemical Parameters in Females and Males
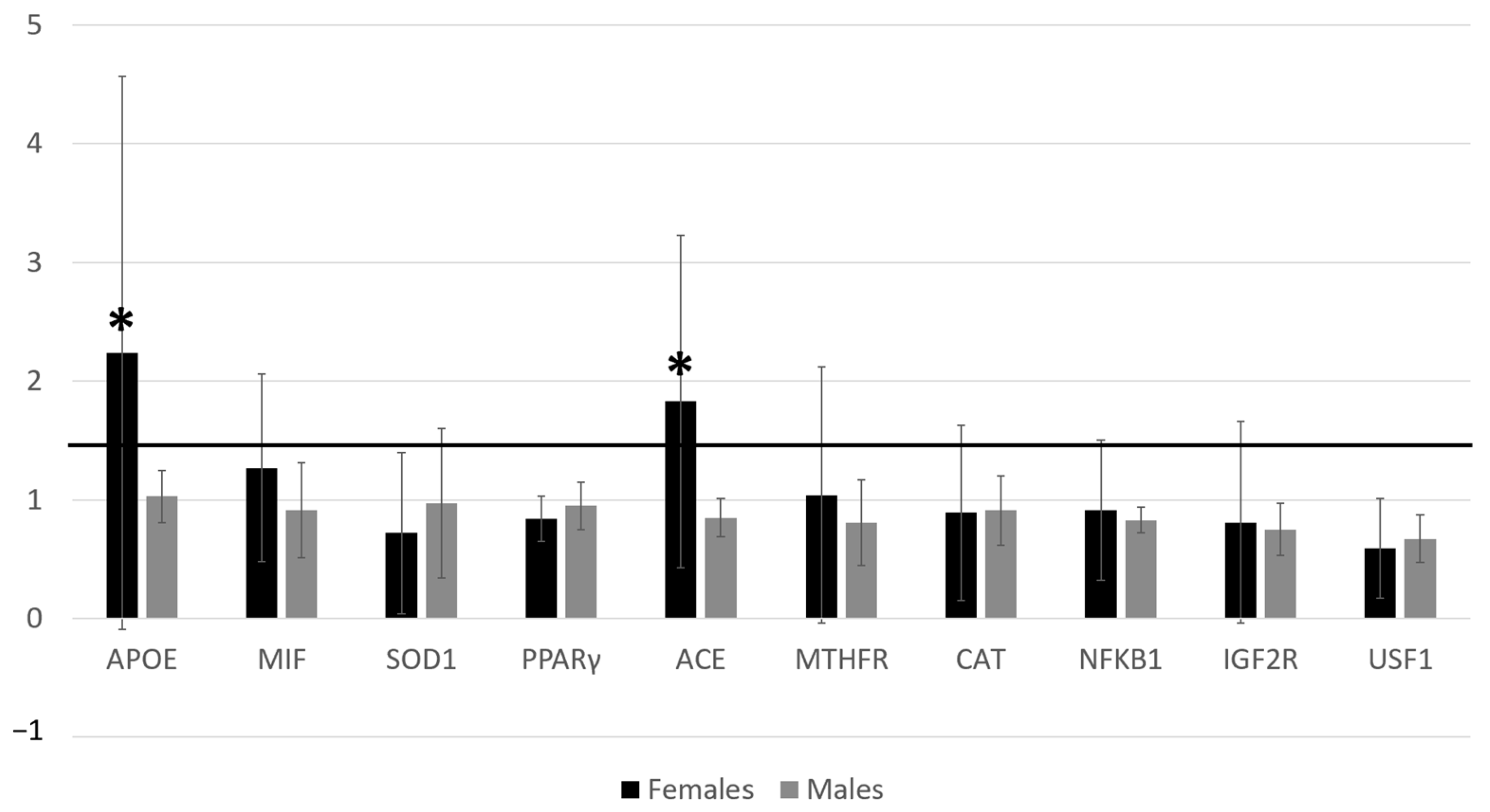
3.4. Effect of Intervention on Gene Expression in Females and Males
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Forman, H.J.; Zhang, H. Targeting Oxidative Stress in Disease: Promise and Limitations of Antioxidant Therapy. Nat. Rev. Drug Discov. 2021, 20, 689–709. [Google Scholar] [CrossRef] [PubMed]
- Hybertson, B.M.; Gao, B.; Bose, S.K.; McCord, J.M. Oxidative Stress in Health and Disease: The Therapeutic Potential of Nrf2 Activation. Mol. Asp. Med. 2011, 32, 234–246. [Google Scholar] [CrossRef] [PubMed]
- Gualtieri, P.; Marchetti, M.; Frank, G.; Smeriglio, A.; Trombetta, D.; Colica, C.; Cianci, R.; De Lorenzo, A.; Di Renzo, L. Antioxidant-Enriched Diet on Oxidative Stress and Inflammation Gene Expression: A Randomized Controlled Trial. Genes 2023, 14, 206. [Google Scholar] [CrossRef] [PubMed]
- Nani, A.; Murtaza, B.; Sayed Khan, A.; Khan, N.A.; Hichami, A. Antioxidant and Anti-Inflammatory Potential of Polyphenols Contained in Mediterranean Diet in Obesity: Molecular Mechanisms. Molecules 2021, 26, 985. [Google Scholar] [CrossRef] [PubMed]
- Perrone, M.A.; Gualtieri, P.; Gratteri, S.; Ali, W.; Sergi, D.; Muscoli, S.; Cammarano, A.; Bernardini, S.; Di Renzo, L.; Romeo, F. Effects of Postprandial Hydroxytyrosol and Derivates on Oxidation of LDL, Cardiometabolic State and Gene Expression: A Nutrigenomic Approach for Cardiovascular Prevention. J. Cardiovasc. Med. 2019, 20, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Merra, G.; Botta, R.; Gualtieri, P.; Manzo, A.; Perrone, M.A.; Mazza, M.; Cascapera, S.; De Lorenzo, A. Post-Prandial Effects of Hazelnut-Enriched High Fat Meal on LDL Oxidative Status, Oxidative and Inflammatory Gene Expression of Healthy Subjects: A Randomized Trial. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 1610–1626. [Google Scholar] [PubMed]
- Bjune, J.-I.; Strømland, P.P.; Jersin, R.Å.; Mellgren, G.; Dankel, S.N. Metabolic and Epigenetic Regulation by Estrogen in Adipocytes. Front. Endocrinol. 2022, 13, 828780. [Google Scholar] [CrossRef]
- Renzo, L.D.; Carraro, A.; Minella, D.; Botta, R.; Contessa, C.; Sartor, C.; Iacopino, A.M.; Lorenzo, A.D. Nutrient Analysis Critical Control Point (NACCP): Hazelnut as a Prototype of Nutrigenomic Study. FNS 2014, 5, 79–88. [Google Scholar] [CrossRef]
- Buscemi, S.; Rosafio, G.; Vasto, S.; Massenti, F.M.; Grosso, G.; Galvano, F.; Rini, N.; Barile, A.M.; Maniaci, V.; Cosentino, L.; et al. Validation of a Food Frequency Questionnaire for Use in Italian Adults Living in Sicily. Int. J. Food Sci. Nutr. 2015, 66, 426–438. [Google Scholar] [CrossRef]
- De Lorenzo, A.; Di Renzo, L.; Morini, P.; De Miranda, R.C.; Romano, L.; Colica, C. New Equations to Estimate Resting Energy Expenditure in Obese Adults from Body Composition. Acta Diabetol. 2018, 55, 59–66. [Google Scholar] [CrossRef]
- Alberti-Fidanza, A.; Fidanza, F. Mediterranean Adequacy Index of Italian Diets. Public Health Nutr. 2004, 7, 937–941. [Google Scholar] [CrossRef] [PubMed]
- Merra, G.; Gualtieri, P.; Cioccoloni, G.; Falco, S.; Bigioni, G.; Tarsitano, M.G.; Capacci, A.; Piccioni, A.; Costacurta, M.; Franceschi, F.; et al. FTO Rs9939609 Influence on Adipose Tissue Localization in the Italian Population. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 3223–3235. [Google Scholar] [CrossRef] [PubMed]
- Pujia, R.; Tarsitano, M.G.; Arturi, F.; De Lorenzo, A.; Lenzi, A.; Pujia, A.; Montalcini, T. Advances in Phenotyping Obesity and in Its Dietary and Pharmacological Treatment: A Narrative Review. Front. Nutr. 2022, 9, 804719. [Google Scholar] [CrossRef] [PubMed]
- Haun, D.R.; Pitanga, F.J.G.; Lessa, I. Razão Cintura/Estatura Comparado a Outros Indicadores Antropométricos de Obesidade Como Preditor de Risco Coronariano Elevado. Rev. Assoc. Med. Bras. 2009, 55, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Marchetti, M.; Cioccoloni, G.; Gratteri, S.; Capria, G.; Romano, L.; Soldati, L.; Mele, M.C.; Merra, G.; Cintoni, M.; et al. Role of Phase Angle in the Evaluation of Effect of an Immuno-Enhanced Formula in Post-Surgical Cancer Patients: A Randomized Clinical Trial. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1322–1334. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, A.; Sasso, G.F.; Andreoli, A.; Sorge, R.; Candeloro, N.; Cairella, M. Improved Prediction Formula for Total Body Water Assessment in Obese Women. Int. J. Obes. Relat. Metab. Disord. 1995, 19, 535–538. [Google Scholar] [PubMed]
- Di Renzo, L.; Bertoli, A.; Bigioni, M.; Gobbo, V.; Premrov, M.; Calabrese, V.; Di Daniele, N.; De Lorenzo, A. Body Composition and -174G/C Interleukin-6 Promoter Gene Polymorphism: Association with Progression of Insulin Resistance in Normal Weight Obese Syndrome. CPD 2008, 14, 2699–2706. [Google Scholar] [CrossRef]
- Di Renzo, L.; Galvano, F.; Orlandi, C.; Bianchi, A.; Di Giacomo, C.; La Fauci, L.; Acquaviva, R.; De Lorenzo, A. Oxidative Stress in Normal-Weight Obese Syndrome. Obesity 2010, 18, 2125–2130. [Google Scholar] [CrossRef]
- Kaneva, A.M.; Bojko, E.R. Age-Adjusted Cut-off Values of Lipid Accumulation Product (LAP) for Predicting Hypertension. Sci. Rep. 2021, 11, 11095. [Google Scholar] [CrossRef]
- Ahn, N.; Baumeister, S.E.; Amann, U.; Rathmann, W.; Peters, A.; Huth, C.; Thorand, B.; Meisinger, C. Visceral Adiposity Index (VAI), Lipid Accumulation Product (LAP), and Product of Triglycerides and Glucose (TyG) to Discriminate Prediabetes and Diabetes. Sci. Rep. 2019, 9, 9693. [Google Scholar] [CrossRef]
- Nair, D.; Carrigan, T.P.; Curtin, R.J.; Popovic, Z.B.; Kuzmiak, S.; Schoenhagen, P.; Flamm, S.D.; Desai, M.Y. Association of Total Cholesterol/High-Density Lipoprotein Cholesterol Ratio With Proximal Coronary Atherosclerosis Detected by Multislice Computed Tomography. Prev. Cardiol. 2009, 12, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Hata, M.; Takayama, T.; Sezai, A.; Yoshitake, I.; Hirayama, A.; Minami, K. Efficacy of Aggressive Lipid Controlling Therapy for Preventing Saphenous Vein Graft Disease. Ann. Thorac. Surg. 2009, 88, 1440–1444. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Fan, Z.; Zhang, Y.; Li, T. Independent Association of Severity of Obstructive Sleep Apnea with Lipid Metabolism of Atherogenic Index of Plasma (AIP) and apoB/apoAI Ratio. Sleep Breath. 2020, 24, 1507–1513. [Google Scholar] [CrossRef] [PubMed]
- Bazzi, W.M.; Dejbakhsh, S.Z.; Bernstein, M.; Russo, P. Neutrophil-Lymphocyte Ratio in Small Renal Masses. ISRN Urol. 2014, 2014, 759253. [Google Scholar] [CrossRef]
- Erdal, E.; İnanir, M. Platelet-to-Lymphocyte Ratio (PLR) and Plateletcrit (PCT) in Young Patients with Morbid Obesity. Rev. Assoc. Med. Bras. 2019, 65, 1182–1187. [Google Scholar] [CrossRef] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of Relative Gene Expression Data Using Real-Time Quantitative PCR and the 2−ΔΔCT Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]
- D’Innocenzo, S.; Biagi, C.; Lanari, M. Obesity and the Mediterranean Diet: A Review of Evidence of the Role and Sustainability of the Mediterranean Diet. Nutrients 2019, 11, 1306. [Google Scholar] [CrossRef]
- Bredella, M.A. Sex Differences in Body Composition. Adv. Exp. Med. Biol. 2017, 1043, 9–27. [Google Scholar] [CrossRef]
- Schorr, M.; Dichtel, L.E.; Gerweck, A.V.; Valera, R.D.; Torriani, M.; Miller, K.K.; Bredella, M.A. Sex Differences in Body Composition and Association with Cardiometabolic Risk. Biol. Sex. Differ. 2018, 9, 28. [Google Scholar] [CrossRef]
- Chang, E.; Varghese, M.; Singer, K. Gender and Sex Differences in Adipose Tissue. Curr. Diab Rep. 2018, 18, 69. [Google Scholar] [CrossRef]
- Giagulli, V.A.; Castellana, M.; Pelusi, C.; Triggiani, V. Androgens, Body Composition, and Their Metabolism Based on Sex. In Frontiers of Hormone Research; Pasquali, R., Pignatelli, D., Eds.; S. Karger AG: Basel, Switzerland, 2019; Volume 53, pp. 18–32. ISBN 978-3-318-06470-4. [Google Scholar]
- Álvarez-Fernández, C.; Romero-Saldaña, M.; Álvarez-López, Á.; Molina-Luque, R.; Molina-Recio, G.; Vaquero-Abellán, M. Adherence to the Mediterranean Diet According to Occupation-Based Social Classifications and Gender. Arch. Environ. Occup. Health 2021, 76, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Bédard, A.; Hudon, A.-M.; Drapeau, V.; Corneau, L.; Dodin, S.; Lemieux, S. Gender Differences in the Appetite Response to a Satiating Diet. J. Obes. 2015, 2015, 140139. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Cinelli, G.; Dri, M.; Gualtieri, P.; Attinà, A.; Leggeri, C.; Cenname, G.; Esposito, E.; Pujia, A.; Chiricolo, G.; et al. Mediterranean Personalized Diet Combined with Physical Activity Therapy for the Prevention of Cardiovascular Diseases in Italian Women. Nutrients 2020, 12, 3456. [Google Scholar] [CrossRef] [PubMed]
- Dernini, S.; Berry, E.; Serra-Majem, L.; La Vecchia, C.; Capone, R.; Medina, F.; Aranceta-Bartrina, J.; Belahsen, R.; Burlingame, B.; Calabrese, G.; et al. Med Diet 4.0: The Mediterranean Diet with Four Sustainable Benefits. Public Health Nutr. 2017, 20, 1322–1330. [Google Scholar] [CrossRef] [PubMed]
- Mascaró, C.M.; Bouzas, C.; Montemayor, S.; Casares, M.; Llompart, I.; Ugarriza, L.; Borràs, P.-A.; Martínez, J.A.; Tur, J.A. Effect of a Six-Month Lifestyle Intervention on the Physical Activity and Fitness Status of Adults with NAFLD and Metabolic Syndrome. Nutrients 2022, 14, 1813. [Google Scholar] [CrossRef] [PubMed]
- Schiaffino, S.; Reggiani, C. Fiber Types in Mammalian Skeletal Muscles. Physiol. Rev. 2011, 91, 1447–1531. [Google Scholar] [CrossRef]
- Ciciliot, S.; Rossi, A.C.; Dyar, K.A.; Blaauw, B.; Schiaffino, S. Muscle Type and Fiber Type Specificity in Muscle Wasting. Int. J. Biochem. Cell Biol. 2013, 45, 2191–2199. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Gualtieri, P.; Romano, L.; Marrone, G.; Noce, A.; Pujia, A.; Perrone, M.A.; Aiello, V.; Colica, C.; De Lorenzo, A. Role of Personalized Nutrition in Chronic-Degenerative Diseases. Nutrients 2019, 11, 1707. [Google Scholar] [CrossRef]
- Ji, H.; Kim, A.; Ebinger, J.E.; Niiranen, T.J.; Claggett, B.L.; Bairey Merz, C.N.; Cheng, S. Sex Differences in Blood Pressure Trajectories Over the Life Course. JAMA Cardiol. 2020, 5, 255. [Google Scholar] [CrossRef]
- Leblanc, V.; Bégin, C.; Hudon, A.-M.; Royer, M.-M.; Corneau, L.; Dodin, S.; Lemieux, S. Gender Differences in the Long-Term Effects of a Nutritional Intervention Program Promoting the Mediterranean Diet: Changes in Dietary Intakes, Eating Behaviors, Anthropometric and Metabolic Variables. Nutr. J. 2014, 13, 107. [Google Scholar] [CrossRef]
- Velázquez-López, L.; Muñoz-Torres, A.V.; García-Peña, C.; López-Alarcón, M.; Islas-Andrade, S.; Escobedo-de La Peña, J. Fiber in Diet Is Associated with Improvement of Glycated Hemoglobin and Lipid Profile in Mexican Patients with Type 2 Diabetes. J. Diabetes Res. 2016, 2016, 2980406. [Google Scholar] [CrossRef] [PubMed]
- Vellar, O.D. Changes in Hemoglobin Concentration and Hematocrit During the Menstrual Cycle: I. A Cross-sectional Study. Acta Obstet. Gynecol. Scand. 1974, 53, 243–246. [Google Scholar] [CrossRef]
- Parhizkar, S.; Holtzman, D.M. APOE Mediated Neuroinflammation and Neurodegeneration in Alzheimer’s Disease. Semin. Immunol. 2022, 59, 101594. [Google Scholar] [CrossRef] [PubMed]
- Carl-McGrath, S.; Gräntzdörffer, I.; Lendeckel, U.; Ebert, M.P.; Röcken, C. Angiotensin II-Generating Enzymes, Angiotensin-Converting Enzyme (ACE) and Mast Cell Chymase (CMA1), in Gastric Inflammation May Be Regulated by H. Pylori and Associated Cytokines. Pathology 2009, 41, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Lin, Q.; Fan, K.; Tang, M.; Zhang, W.; Yang, B.; Ou, Q. The Effects of Genetic Polymorphisms of APOE on Circulating Lipid Levels in Middle-Aged and Elderly Chinese Fujian Han Population: Toward Age- and Sex-Personalized Management. Lipids Health Dis. 2021, 20, 158. [Google Scholar] [CrossRef] [PubMed]
- Li, Y. Angiotensin-Converting Enzyme Gene Insertion/Deletion Polymorphism and Essential Hypertension in the Chinese Population: A Meta-Analysis Including 21,058 Participants. Intern. Med. J. 2012, 42, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, D.S.; Santos, R.S.; Jardim, P.C.B.V.; Silva, E.G.; Reis, A.A.S.; Pedrino, G.R.; Ulhoa, C.J. The Combination of ACE I/D and ACE2 G8790A Polymorphisms Revels Susceptibility to Hypertension: A Genetic Association Study in Brazilian Patients. PLoS ONE 2019, 14, e0221248. [Google Scholar] [CrossRef]


{kind=link}
| Index | Formula | Cut-Offs | Reference |
|---|---|---|---|
| Lipid Accumulation Product (LAP) for males | (WC [cm] − 65) × Tg concentration [mM] | 20.10 to 63.89 cm mmol/L | [19] |
| Lipid Accumulation Product (LAP) for females | (WC [cm] − 58) × Tg concentration [mM] | 25.16 to 31.59 cm mmol/L | [19] |
| Visceral Adiposity Index (VAI) for males | [WC/39.68 + (1.88 × BMI)] × [Tg/1.03] × 1.31/HDL-c] | 2.33 | [20] |
| Visceral Adiposity Index (VAI) for females | [WC/36.58 + (1.89 × BMI)] × [Tg/0.81] × [1.52/HDL-c] | 1.32 | [20] |
| Cardiovascular Risk Indexes | Total Cholesterol/HDL-c | ≤4 | [21] |
| LDL-c/HDL-c | <1.5 | [22] | |
| Atherogenic Index of Plasma (AIP) | Log (Tg/HDL-c) | <0.11 low risk. ≥0.11 and ≤0.21 moderate risk. >0.21 high risk | [23] |
| Neutrophil/lymphocyte Ratio (NLR) | Neutrophils/Lymphocyte | <1.6 low risk. ≥1.6 and ≤2.4 moderate risk. >2.4 high risk | [24] |
| Platelet-to-lymphocyte Ratio (PLR) | Platelet/Lymphocyte | <150 | [25] |
| Target Genes | Sequences |
|---|---|
| APO-E | 5′-GACCATGAAGGAGTTGAAGGCCTAC-3′ 3′-CTCGCGGGCCCCGGCCTGGTA-5′ |
| MIF | 5′-AGAACCGCTCCTACAGCAAGCT-3′ 3′-GGAGTTGTTCCAGCCCACATTG-5′ |
| NFκB | 5′-GAAATTCCTGATCCAGACAAAAAC-3′ 3′-ATCACTTCAATGGCCTCTGTGTAG-5′ |
| PPRγ | 5′-GGGATGTCTCATAATGCCATCA-3′ 3′-CGCCAACAGCTTCTCCTTCT-5′ |
| ACE | 5′-CTGGAGACCACTCCCATCCTTTCT-3′ 3′-GATGTGGCCATCACATTCGTCAGAT-5′ |
| MTHFR | 5′-TGTGGTCTCTTCATCCCTCGC-3′ 3′-CCTTTTGGTGATGCTTGTTGGC-5′ |
| CAT | 5′-GTGCGGAGATTCAACACTGCCA-3′ 3′-CGGCAATGTTCTCACACAGACG-5′ |
| SOD1 | 5′-CTCACTCTCAGGAGACCATTGC-3′ 3′-CCACAAGCCAAACGACTTCCAG-5′ |
| IGF2-R | 5′-TTGAGTGGCGAACGCAGTATGC-3′ 3′-CAGTGATGGCTTCCCAGTTGTC-5′ |
| USF1 | 5′-GCTCTATGGAGAGCACCAAGTC-3′ 3′-AGACAAGCGGTGGTTACTCTGC-5′ |
| Females | Males | |||||
|---|---|---|---|---|---|---|
| Before MedD | After MedD | p-Value | Before MedD | After MedD | p-Value | |
| Weight (kg) | 63.13 ± 9.65 | 62.99 ± 9.99 | 0.97 | 74.50 ± 7.02 | 74.12 ± 7.10 | a 0.71 |
| BMI (kg/m2) | 24.63 ± 3.87 | 24.57 ± 4.03 | 0.97 | 24.35 ± 1.87 | 24.35 ± 2.12 | 0.99 |
| WC (cm) | 74.23 ± 6.20 | 75.50 ± 5.26 | 0.62 | 83.10 ± 8.68 | 84.15 ± 9.91 | a 0.74 |
| HC (cm) | 101.69 ± 8.29 | 100.86 ± 8.97 | 0.83 | 96.64 ± 3.81 | 97.18 ± 5.24 | a 1.0 |
| WHR | 0.72 ± 0.02 | 0.74 ± 0.02 | 0.11 | 0.85 ± 0.05 | 0.86 ± 0.05 | 0.81 |
| Bicipital Skinfold | 7.73 ± 1.98 | 7.06 ± 2.20 | 0.48 | 4.62 ± 2.19 | 4.18 ± 1.97 | a 0.79 |
| Triceps Skinfold | 20.59 ± 5.89 | 20.07 ± 6.59 | 0.85 | 12.10 ± 3.25 | 10.47 ± 5.87 | 0.53 |
| Subscapular Skinfold | 14.92 ± 4.23 | 14.38 ± 4.16 | 0.77 | 14.19 ± 5.81 | 13.61 ± 5.43 | a 0.65 |
| Suprailiac Skinfold | 15.16 ± 4.78 | 14.64 ± 4.33 | a 0.82 | 10.59 ± 5.08 | 9.98 ± 6.09 | a 0.52 |
| Handgrip Strength (kg) | 23.88 ± 5.36 | 24.23 ± 5.42 | 0.89 | 33.12 ± 12.93 | 34.48 ± 12.47 | 0.87 |
| RF (s) | 7.18 ± 3.71 | 6.84 ± 2.15 | 0.81 | 16.80 ± 6.91 | 5.36 ± 2.09 | 0.009 ** |
| SBP | 107.00 ± 9.48 | 113.11 ± 4.96 | 0.1 | 117.29 ± 10.87 | 111.43 ± 6.90 | 0.25 |
| DBP | 71.00 ± 3.94 | 72.11 ± 4.19 | a 0.46 | 76.00 ± 5.80 | 72.14 ± 6.98 | 0.28 |
| Before MedD | After MedD | |
|---|---|---|
| Weight (kg) | 0.018 * | 0.023 * |
| BMI (kg/m2) | 0.8 | 0.8 |
| WC (cm) | 0.026 * | 0.033 * |
| HC (cm) | 0.15 | 0.3 |
| WHR | 0.0001 *** | 0.0001 *** |
| Bicipital Skinfold | 0.008 ** | 0.015 * |
| Triceps Skinfold | 0.004 ** | 0.008 ** |
| Subscapular Skinfold | 0.7 | 0.7 |
| Suprailiac Skinfold | 0.07 | 0.08 |
| Handgrip Strength (kg) | 0.1 | 0.051 |
| RF (s) | 0.009 ** | 0.2 |
| SBP | 0.056 | 0.5 |
| DBP | a 0.04 * | 0.9 |
| Females | Males | |||||
|---|---|---|---|---|---|---|
| Before MedD | After MedD | p-Value | Before MedD | After MedD | p-Value | |
| Resistance (Ohm) | 559.80 ± 78.30 | 571.16 ± 72.33 | 0.74 | 452.86 ± 46.75 | 462.00 ± 49.40 | a 0.84 |
| Reactance (Ohm) | 53.20 ± 20.83 | 64.25 ± 9.19 | 0.14 | 51.57 ± 4.19 | 54.85 ± 9.22 | 0.4 |
| PhA (°) | 5.99 ± 0.88 | 6.52 ± 0.95 | 0.21 | 6.52 ± 0.49 | 6.77 ± 0.81 | 0.51 |
| FFM (kg) | 44.83 ± 5.41 | 44.88 ± 5.92 | 0.98 | 62.45 ± 7.27 | 61.90 ± 6.33 | 0.88 |
| FFM (%) | 71.58 ± 6.91 | 71.76 ± 6.98 | 0.95 | 83.84 ± 6.42 | 83.60 ± 6.10 | 0.94 |
| TBW (L) | 33.07 ± 3.70 | 33.09 ± 4.03 | 0.99 | 45.70 ± 5.31 | 45.31 ± 4.64 | 0.88 |
| TBW (%) | 52.80 ± 4.46 | 52.92 ± 4.33 | 0.95 | 61.37 ± 4.70 | 61.20 ± 4.48 | 0.94 |
| ECW (L) | 15.58 ± 2.49 | 14.42 ± 1.73 | 0.24 | 19.85 ± 2.29 | 19.34 ± 2.67 | 0.7 |
| ECW (%) | 46.00 ± 4.16 | 43.75 ± 4.19 | 0.24 | 43.47 ± 2.21 | 42.60 ± 3.28 | 0.57 |
| BCM (kg) | 24.65 ± 5.09 | 25.22 ± 4.57 | 0.79 | 35.10 ± 4.61 | 35.34 ± 3.88 | 0.91 |
| FM (kg) | 18.30 ± 6.59 | 18.11 ± 6.26 | 0.94 | 12.04 ± 4.89 | 12.22 ± 4.97 | 0.94 |
| FM (%) | 28.42 ± 6.91 | 28.24 ± 6.98 | 0.95 | 16.15 ± 6.42 | 16.40 ± 6.10 | 0.94 |
| Na/K | 1.00 ± 0.13 | 0.94 ± 0.11 | a 0.32 | 1.08 ± 0.12 | 1.04 ± 0.15 | 0.57 |
| ICW (%) | 54.00 ± 4.16 | 56.25 ± 4.19 | 0.24 | 56.52 ± 2.21 | 57.40 ± 3.28 | 0.57 |
| MM (kg) | 29.57 ± 4.59 | 30.34 ± 6.25 | 0.75 | 41.47 ± 6.32 | 43.07 ± 4.59 | 0.59 |
| MM (%) | 47.20 ± 5.94 | 49.22 ± 6.53 | 0.47 | 55.62 ± 6.26 | 59.64 ± 3.75 | 0.17 |
| BMR | 1447.02 ± 115.5 | 1481.09 ± 132.37 | 0.54 | 1768.31 ± 134.27 | 1774.98 ± 112.23 | 0.92 |
| BCMI | 9.36 ± 1.46 | 9.82 ± 1.70 | 0.52 | 11.48 ± 1.14 | 11.64 ± 1.24 | 0.81 |
| Before MedD | After MedD | |
|---|---|---|
| Resistance (Ohm) | 0.006 ** | 0.004 ** |
| Reactance (Ohm) | 0.8 | 0.056 |
| PhA (°) | 0.1 | 0.5 |
| FFM (kg) | 0.0001 *** | 0.0001 *** |
| FFM (%) | 0.002 ** | 0.003 ** |
| TBW (L) | a 0.001 ** | 0.0001 *** |
| TBW (%) | 0.002 ** | 0.002 ** |
| ECW (L) | 0.003 ** | 0.0001 ** |
| ECW (%) | 0.1 | 0.5 |
| BCM (kg) | 0.001 ** | 0.0001 *** |
| FM (kg) | 0.051 | 0.057 |
| FM (%) | 0.002 ** | 0.003 ** |
| Na/K | 0.1 | a 0.1 |
| ICW (%) | 0.1 | 0.5 |
| MM (kg) | 0.0001 *** | 0.0001 *** |
| MM (%) | 0.013 ** | 0.002 ** |
| BMR | 0.0001 *** | 0.0001 *** |
| BCMI | 0.006 ** | 0.03 * |
| Females | Males | |||||
|---|---|---|---|---|---|---|
| Before MedD | After MedD | p-Value | Before MedD | After MedD | p-Value | |
| Glycemia (mg/dL) | 80.40 ± 7.58 | 76.20 ± 8.91 | 0.27 | 83.86 ± 8.72 | 79.71 ± 10.53 | 0.43 |
| Insulin (μU/mL) | 6.90 ± 3.06 | 6.93 ± 2.84 | 0.98 | 7.58 ± 6.07 | 7.20 ± 4.80 | 0.89 |
| Total Cholesterol (mg/dL) | 165.60 ± 17.04 | 174.50 ± 26.11 | 0.37 | 159.14 ± 18.56 | 163.43 ± 18.36 | 0.67 |
| HDL-c (mg/dL) | 65.00 ± 8.85 | 67.10 ± 8.31 | 0.59 | 58.14 ± 10.97 | 57.57 ± 5.85 | 0.9 |
| Tg (mg/dL) | 65.90 ± 31.01 | 62.40 ± 21.94 | 0.77 | 77.86 ± 60.34 | 72.43 ± 57.66 | 0.86 |
| LDL-c (mg/dL) | 90.70 ± 12.30 | 100.50 ± 16.57 | 0.15 | 93.14 ± 10.18 | 96.57 ± 16.04 | 0.64 |
| AST (U/L) | 19.40 ± 16.06 | 22.00 ± 18.73 | a 0.73 | 30.86 ± 25.19 | 17.86 ± 5.36 | a 0.56 |
| ALT (U/L) | 23.10 ± 7.21 | 25.30 ± 13.01 | a 0.82 | 28.86 ± 6.66 | 24.00 ± 5.91 | 0.17 |
| Basophils (cells/mL) | 0.02 ± 0.01 | 0.02 ± 0.01 | 0.65 | 0.02 ± 0.01 | 0.02 ± 0.01 | a 0.72 |
| Basophils (%) | 0.43 ± 0.33 | 0.30 ± 0.13 | a 0.42 | 0.45 ± 0.30 | 0.37 ± 0.12 | 0.5 |
| Eosinophils (cells/mL) | 0.10 ± 0.09 | 0.12 ± 0.09 | a 0.51 | 0.15 ± 0.11 | 0.15 ± 0.06 | 0.97 |
| Hematocrit (%) | 38.96 ± 2.58 | 39.94 ± 1.86 | 0.34 | 43.01 ± 2.87 | 42.87 ± 2.75 | 0.92 |
| Hb (g/dL) | 13.12 ± 0.96 | 13.40 ± 0.67 | a 0.04 * | 14.77 ± 1.37 | 14.61 ± 1.36 | a 0.69 |
| Lymphocytes (cells/mL) | 1.99 ± 0.49 | 2.06 ± 0.52 | a 0.88 | 2.01 ± 0.36 | 2.07 ± 0.24 | 0.72 |
| Lymphocytes (%) | 31.51 ± 6.58 | 28.37 ± 7.24 | 0.32 | 32.58 ± 4.67 | 35.00 ± 7.35 | 0.47 |
| MCH (pg) | 30.75 ± 1.76 | 30.64 ± 1.93 | 0.89 | 29.75 ± 3.13 | 29.48 ± 3.15 | 0.87 |
| MCHC (g/dL) | 33.66 ± 0.92 | 33.67 ± 0.97 | 0.98 | 34.28 ± 1.34 | 34.05 ± 1.30 | a 0.52 |
| MCV (Fl) | 91.38 ± 4.47 | 91.03 ± 4.50 | 0.86 | 86.64 ± 6.94 | 86.51 ± 7.05 | a 0.84 |
| Monocytes (cells/mL) | 0.41 ± 0.08 | 0.45 ± 0.11 | 0.39 | 0.43 ± 0.08 | 0.41 ± 0.13 | 0.66 |
| Monocytes (%) | 6.66 ± 1.46 | 6.26 ± 1.37 | 0.53 | 7.05 ± 1.21 | 6.58 ± 1.43 | 0.51 |
| Neutrophils (cells/mL) | 3.82 ± 0.97 | 4.82 ± 1.44 | 0.08 | 3.60 ± 0.85 | 3.61 ± 1.91 | a 0.09 |
| Neutrophils (%) | 59.63 ± 7.84 | 63.43 ± 7.63 | 0.28 | 57.54 ± 5.27 | 55.54 ± 8.25 | 0.59 |
| Platelets (cells/mL) | 270.90 ± 67.32 | 285.10 ± 65.81 | 0.63 | 210.43 ± 32.70 | 213.14 ± 32.59 | 0.87 |
| Red Blood Cells (million/μL) | 4.27 ± 0.35 | 4.39 ± 0.28 | 0.4 | 4.97 ± 0.16 | 4.96 ± 0.20 | 0.94 |
| RDW-CV (%) | 13.04 ± 0.58 | 13.19 ± 0.66 | a 0.62 | 13.17 ± 0.70 | 13.10 ± 0.78 | 0.86 |
| White Blood Cells (cells/mL) | 6.36 ± 1.06 | 7.50 ± 1.70 | 0.09 | 6.24 ± 1.13 | 6.27 ± 2.11 | a 0.48 |
| Before MedD | After MedD | |
|---|---|---|
| Glycemia (mg/dL) | a 0.4 | a 0.4 |
| Insulin (μU/mL) | 0.7 | 0.8 |
| Total Cholesterol (mg/dL) | 0.4 | 0.3 |
| HDL-c (mg/dL) | 0.1 | 0.02 * |
| Tg (mg/dL) | a 0.9 | 0.6 |
| LDL-c (mg/dL) | 0.6 | 0.6 |
| AST (U/L) | 0.2 | a 0.7 |
| ALT (U/L) | 0.1 | a 0.6 |
| Basophils (cells/mL) | 0.8 | 0.8 |
| Basophils (%) | 0.8 | 0.2 |
| Eosinophils (cells/mL) | 0.3 | 0.4 |
| Hematocrit (%) | 0.008 ** | 0.01 * |
| Hb (g/dL) | 0.01 * | 0.03 * |
| Lymphocytes (cells/mL) | 0.9 | a 0.4 |
| Lymphocytes (%) | 0.7 | 0.08 |
| MCH (pg) | 0.4 | 0.3 |
| MCHC (g/dL) | 0.2 | 0.4 |
| MCV (Fl) | 0.1 | 0.1 |
| Monocytes (cells/mL) | a 0.8 | 0.4 |
| Monocytes (%) | 0.5 | 0.6 |
| Neutrophils (cells/mL) | 0.6 | 0.1 |
| Neutrophils (%) | 0.5 | 0.06 |
| Platelets (cells/mL) | 0.04 * | 0.01 * |
| Red Blood Cells (million/μL) | 0.0001 *** | 0.0001 *** |
| RDW-CV (%) | 0.6 | a 0.7 |
| White Blood Cells (cells/mL) | 0.8 | 0.2 |
| Females | Males | |||||
|---|---|---|---|---|---|---|
| Before MedD | After MedD | p-Value | Before MedD | After MedD | p-Value | |
| LAP | 10.64 ± 2.60 | 11.80 ± 4.22 | 0.47 | 19.32 ± 25.55 | 19.22 ± 26.49 | a 0.84 |
| VAI | 0.74 ± 0.37 | 0.70 ± 0.27 | a 0.94 | 0.80 ± 0.70 | 0.73 ± 0.65 | 0.84 |
| Total Cholesterol/HDL-c | 2.56 ± 0.23 | 2.60 ± 0.27 | 0.73 | 2.80 ± 0.51 | 2.87 ± 0.52 | a 0.84 |
| LDL-c/HDL-c | 1.40 ± 0.21 | 1.50 ± 0.24 | 0.34 | 1.66 ± 0.43 | 1.70 ± 0.39 | 0.86 |
| AIP | −0.026 ± 0.18 | −0.056 ± 0.18 | 0.71 | 0.047 ± 0.33 | 0.01 ± 0.31 | 0.83 |
| NLR | 2.01 ± 0.67 | 2.42 ± 0.84 | 0.24 | 1.81 ± 0.41 | 1.74 ± 0.87 | a 0.27 |
| PLR | 137.66 ± 25.84 | 141.28 ± 32.80 | 0.78 | 105.92 ± 16.76 | 103.71 ± 19.08 | 0.82 |
| Before MedD | After MedD | |
|---|---|---|
| LAP | a 0.8 | a 0.5 |
| VAI | a 0.3 | a 0.4 |
| Total Cholesterol/HDL-c | 0.2 | 0.1 |
| LDL-c/HDL-c | 0.1 | 0.2 |
| AIP | 0.5 | 0.5 |
| NLR | 0.4 | a 0.1 |
| PLR | 0.012 * | 0.016 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Renzo, L.; Gualtieri, P.; Frank, G.; De Santis, G.L.; Cianci, R.; Bigioni, G.; De Lorenzo, A. Sex Differences in the Efficacy of Mediterranean Diet Treatment: A Nutrigenomics Pilot Study. Genes 2023, 14, 1980. https://doi.org/10.3390/genes14111980
Di Renzo L, Gualtieri P, Frank G, De Santis GL, Cianci R, Bigioni G, De Lorenzo A. Sex Differences in the Efficacy of Mediterranean Diet Treatment: A Nutrigenomics Pilot Study. Genes. 2023; 14(11):1980. https://doi.org/10.3390/genes14111980
Chicago/Turabian StyleDi Renzo, Laura, Paola Gualtieri, Giulia Frank, Gemma Lou De Santis, Rossella Cianci, Giulia Bigioni, and Antonino De Lorenzo. 2023. "Sex Differences in the Efficacy of Mediterranean Diet Treatment: A Nutrigenomics Pilot Study" Genes 14, no. 11: 1980. https://doi.org/10.3390/genes14111980