
Intergenerational Influence of Gender and the DM1 Phenotype of the Transmitting Parent in Korean Myotonic Dystrophy Type 1


Abstract
:1. Introduction
2. Intergenerational Data Collection and Analysis
3. Intergenerational Influences in Korean DM1
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aslanidis, C.; Jansen, G.; Amemiya, C.; Shutler, G.; Mahadevan, M.; Tsilfidis, C.; Chen, C.; Alleman, J.; Wormskamp, N.G.; Vooijs, M.; et al. Cloning of the essential myotonic dystrophy region and mapping of the putative defect. Nature 1992, 355, 548–551. [Google Scholar] [CrossRef] [PubMed]
- Brook, J.D.; McCurrach, M.E.; Harley, H.G.; Buckler, A.J.; Church, D.; Aburatani, H.; Hunter, K.; Stanton, V.P.; Thirion, J.P.; Hudson, T.; et al. Molecular basis of myotonic dystrophy: Expansion of a trinucleotide (CTG) repeat at the 3’ end of a transcript encoding a protein kinase family member. Cell 1992, 68, 799–808. [Google Scholar] [CrossRef]
- Harley, H.G.; Brook, J.D.; Rundle, S.A.; Crow, S.; Reardon, W.; Buckler, A.J.; Harper, P.S.; Housman, D.E.; Shaw, D.J. Expansion of an unstable DNA region and phenotypic variation in myotonic dystrophy. Nature 1992, 355, 545–546. [Google Scholar] [CrossRef] [PubMed]
- Cumming, S.A.; Jimenez-Moreno, C.; Okkersen, K.; Wenninger, S.; Daidj, F.; Hogarth, F.; Littleford, R.; Gorman, G.; Bassez, G.; Schoser, B.; et al. Genetic determinants of disease severity in the myotonic dystrophy type 1 OPTIMISTIC cohort. Neurology 2019, 93, e995–e1009. [Google Scholar] [CrossRef]
- Hogrel, J.Y.; Ollivier, G.; Ledoux, I.; Hébert, L.J.; Eymard, B.; Puymirat, J.; Bassez, G. Relationships between grip strength, myotonia, and CTG expansion in myotonic dystrophy type 1. Ann. Clin. Transl. Neurol. 2017, 4, 921–925. [Google Scholar] [CrossRef]
- André, L.M.; Ausems, C.R.M.; Wansink, D.G.; Wieringa, B. Abnormalities in Skeletal Muscle Myogenesis, Growth, and Regeneration in Myotonic Dystrophy. Front. Neurol. 2018, 9, 368. [Google Scholar] [CrossRef]
- Rakocevic-Stojanovic, V.; Savic, D.; Pavlovic, S.; Lavrnic, D.; Stevic, Z.; Basta, I.; Romac, S.; Apostolski, S. Intergenerational changes of CTG repeat depending on the sex of the transmitting parent in myotonic dystrophy type 1. Eur. J. Neurol. 2005, 12, 236–237. [Google Scholar] [CrossRef]
- Martorell, L.; Cobo, A.M.; Baiget, M.; Naudo, M.; Poza, J.J.; Parra, J. Prenatal diagnosis in myotonic dystrophy type 1. Thirteen years of experience: Implications for reproductive counselling in DM1 families. Prenat. Diagn. 2007, 27, 68–72. [Google Scholar] [CrossRef]
- Lavedan, C.; Hofmann-Radvanyi, H.; Shelbourne, P.; Rabes, J.P.; Duros, C.; Savoy, D.; Dehaupas, I.; Luce, S.; Johnson, K.; Junien, C. Myotonic dystrophy: Size- and sex-dependent dynamics of CTG meiotic instability, and somatic mosaicism. Am. J. Hum. Genet. 1993, 52, 875–883. [Google Scholar]
- Redman, J.B.; Fenwick, R.G., Jr.; Fu, Y.H.; Pizzuti, A.; Caskey, C.T. Relationship between parental trinucleotide GCT repeat length and severity of myotonic dystrophy in offspring. JAMA 1993, 269, 1960–1965. [Google Scholar] [CrossRef]
- Tsilfidis, C.; MacKenzie, A.E.; Mettler, G.; Barcelo, J.; Korneluk, R.G. Correlation between CTG trinucleotide repeat length and frequency of severe congenital myotonic dystrophy. Nat. Genet. 1992, 1, 192–195. [Google Scholar] [CrossRef]
- Pratte, A.; Prevost, C.; Puymirat, J.; Mathieu, J. Anticipation in myotonic dystrophy type 1 parents with small CTG expansions. Am. J. Med. Genet. Part A 2015, 167, 708–714. [Google Scholar] [CrossRef]
- Dean, N.L.; Loredo-Osti, J.C.; Fujiwara, T.M.; Morgan, K.; Tan, S.L.; Naumova, A.K.; Ao, A. Transmission ratio distortion in the myotonic dystrophy locus in human preimplantation embryos. Eur. J. Hum. Genet. 2006, 14, 299–306. [Google Scholar] [CrossRef]
- Dogan, C.; De Antonio, M.; Hamroun, D.; Varet, H.; Fabbro, M.; Rougier, F.; Amarof, K.; Bes, M.C.A.; Bedat-Millet, A.L.; Behin, A.; et al. Gender as a Modifying Factor Influencing Myotonic Dystrophy Type 1 Phenotype Severity and Mortality: A Nationwide Multiple Databases Cross-Sectional Observational Study. PLoS ONE 2016, 11, e0148264. [Google Scholar] [CrossRef]
- Perna, A.; Maccora, D.; Rossi, S.; Nicoletti, T.F.; Zocco, M.A.; Riso, V.; Modoni, A.; Petrucci, A.; Valenza, V.; Grieco, A.; et al. High Prevalence and Gender-Related Differences of Gastrointestinal Manifestations in a Cohort of DM1 Patients: A Perspective, Cross-Sectional Study. Front. Neurol. 2020, 11, 394. [Google Scholar] [CrossRef]
- Peric, S.; Pesovic, J.; Savic-Pavicevic, D.; Rakocevic Stojanovic, V.; Meola, G. Molecular and Clinical Implications of Variant Repeats in Myotonic Dystrophy Type 1. Int. J. Mol. Sci. 2021, 23, 354. [Google Scholar] [CrossRef]
- Nam, S.H.; Son, Y.B.; Lee, B.L.; Lee, J.; Ki, C.S.; Lee, M. Clinical characteristics of congenital myotonic dystrophy diagnosed by molecular genetic method. Korean J. Pediatr. 2007, 50, 868–874. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, J.Y.; Kim, G.P.; Sung, J.J.; Lim, K.S.; Lee, K.W.; Chae, J.H.; Hong, Y.H.; Seong, M.W.; Park, S.S. Molecular and clinical characteristics of myotonic dystrophy type 1 in koreans. Korean J. Lab. Med. 2008, 28, 483–492. [Google Scholar] [CrossRef]
- Oh, J.H.; Lee, J.Y.; Lee, J.S.; Choi, J.C.; Kang, J.H.; Kang, S.Y. Congenital Myotonic Dystrophy Diagnosed in an Adolescent Period. J. Korean Neurol. Assoc. 2008, 26, 383–386. [Google Scholar]
- Yim, S.Y.; Cho, K.H.; Kim, J.Y.; Hong, J.Y.; Lee, I.Y. A Floppy Baby with Congenital Myotonic Dystrophy Complicated with Huge Subgaleal Hematoma Occurring in Non-instrumental Vaginal Delivery. J. Genet. Med. 2009, 6, 166–169. [Google Scholar]
- Kim, H.S.; Chung, K.W.; Kang, S.H.; Choi, S.K.; Cho, S.Y.; Koo, H.; Kim, S.B.; Choi, B.O. Myotonic dystrophy type I combined with X-linked dominant Charcot-Marie-Tooth neuropathy. Neurogenetics 2010, 11, 425–433. [Google Scholar] [CrossRef]
- Kang, S.Y.; Kang, H.J.; Chung, P.W.; Kim, K.K.; Lee, S.; Choi, B.O. Congestive heart failure after physical exercise in a young patient with myotonic dystrophy type 1. Int. J. Neurosci. 2011, 121, 637–639. [Google Scholar] [CrossRef]
- Son, S.B.; Chun, J.M.; Kim, K.A.; Ko, S.Y.; Lee, Y.K.; Shin, S.M. A case report on 30-week premature twin babies with congenital myotonic dystrophy conceived by in vitro fertilization. J. Korean Med. Sci. 2012, 27, 1269–1272. [Google Scholar] [CrossRef]
- Son, H.K.; Cha, Y.S.; Suh, H.; Ki, C.S.; Shin, Y.B. Upper thoracic myelopathy caused by delayed neck extensor weakness in myotonic dystrophy. Ann. Rehabil. Med. 2012, 36, 569–572. [Google Scholar] [CrossRef]
- Kim, H.N.; Cho, Y.K.; Cho, J.H.; Yang, E.M.; Song, E.S.; Choi, Y.Y. Transient complete atrioventricular block in a preterm neonate with congenital myotonic dystrophy: Case report. J. Korean Med. Sci. 2014, 29, 879–883. [Google Scholar] [CrossRef]
- Kim, H.J.; Oh, J.H.; Kang, S.Y. Bilateral Adduction Palsy in a Patient with Myotonic Dystrophy Type 1. Exp. Neurobiol. 2016, 25, 143–145. [Google Scholar] [CrossRef]
- Chung, B.; Wong, V.; Ip, P. Prevalence of neuromuscular diseases in Chinese children: A study in southern China. J. Child Neurol. 2003, 18, 217–219. [Google Scholar] [CrossRef]
- Hsiao, K.M.; Chen, S.S.; Li, S.Y.; Chiang, S.Y.; Lin, H.M.; Pan, H.; Huang, C.C.; Kuo, H.C.; Jou, S.B.; Su, C.C.; et al. Epidemiological and genetic studies of myotonic dystrophy type 1 in Taiwan. Neuroepidemiology 2003, 22, 283–289. [Google Scholar] [CrossRef]
- Lee, J.Y.; Jeong, H.N. Nationwide incidence of myotonic dystrophy type 1 and the status of multi-organ involvement. J. Neurol. 2022, 269, 2666–2672. [Google Scholar] [CrossRef]
- Sugimoto, M.; Kuru, S.; Takada, H.; Horie, R.; Yamauchi, K.; Kubota, T.; Matsumura, T.; Nakamura, H.; Kimura, E.; Takahashi, M.P. Characteristics of myotonic dystrophy patients in the national registry of Japan. J. Neurol. Sci. 2022, 432, 120080. [Google Scholar] [CrossRef]
- Medica, I.; Marković, D.; Peterlin, B. Genetic epidemiology of myotonic dystrophy in Istria, Croatia. Acta Neurol. Scand. 1997, 95, 164–166. [Google Scholar] [CrossRef] [PubMed]
- Siciliano, G.; Manca, M.; Gennarelli, M.; Angelini, C.; Rocchi, A.; Iudice, A.; Miorin, M.; Mostacciuolo, M. Epidemiology of myotonic dystrophy in Italy: Re-apprisal after genetic diagnosis. Clin. Genet. 2001, 59, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Segel, R.; Silverstein, S.; Lerer, I.; Kahana, E.; Meir, R.; Sagi, M.; Zilber, N.; Korczyn, A.D.; Shapira, Y.; Argov, Z.; et al. Prevalence of myotonic dystrophy in Israeli Jewish communities: Inter-community variation and founder premutations. Am. J. Med. Genet. Part A 2003, 119, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Mladenovic, J.; Pekmezovic, T.; Todorovic, S.; Rakocevic-Stojanovic, V.; Savic, D.; Romac, S.; Apostolski, S. Survival and mortality of myotonic dystrophy type 1 (Steinert’s disease) in the population of Belgrade. Eur. J. Neurol. 2006, 13, 451–454. [Google Scholar] [CrossRef]
- Norwood, F.L.; Harling, C.; Chinnery, P.F.; Eagle, M.; Bushby, K.; Straub, V. Prevalence of genetic muscle disease in Northern England: In-depth analysis of a muscle clinic population. Brain 2009, 132, 3175–3186. [Google Scholar] [CrossRef]
- Vanacore, N.; Rastelli, E.; Antonini, G.; Bianchi, M.L.; Botta, A.; Bucci, E.; Casali, C.; Costanzi-Porrini, S.; Giacanelli, M.; Gibellini, M.; et al. An Age-Standardized Prevalence Estimate and a Sex and Age Distribution of Myotonic Dystrophy Types 1 and 2 in the Rome Province, Italy. Neuroepidemiology 2016, 46, 191–197. [Google Scholar] [CrossRef]
- Lefter, S.; Hardiman, O.; Ryan, A.M. A population-based epidemiologic study of adult neuromuscular disease in the Republic of Ireland. Neurology 2017, 88, 304–313. [Google Scholar] [CrossRef]
- Lindberg, C.; Bjerkne, F. Prevalence of myotonic dystrophy type 1 in adults in western Sweden. Neuromuscul. Disord. 2017, 27, 159–162. [Google Scholar] [CrossRef]
- Pagola-Lorz, I.; Vicente, E.; Ibáñez, B.; Torné, L.; Elizalde-Beiras, I.; Garcia-Solaesa, V.; García, F.; Delfrade, J.; Jericó, I. Epidemiological study and genetic characterization of inherited muscle diseases in a northern Spanish region. Orphanet. J. Rare Dis. 2019, 14, 276. [Google Scholar] [CrossRef]
- Husebye, S.A.; Rebne, C.B.; Stokland, A.E.; Sanaker, P.S.; Bindoff, L.A. A hospital based epidemiological study of genetically determined muscle disease in south western Norway. Neuromuscul. Disord. 2020, 30, 181–185. [Google Scholar] [CrossRef]
- Hagerman, K.A.; Howe, S.J.; Heatwole, C.R. The myotonic dystrophy experience: A North American cross-sectional study. Muscle Nerve 2019, 59, 457–464. [Google Scholar] [CrossRef]
- Ford, C.; Kidd, A.; Hammond-Tooke, G. Myotonic dystrophy in Otago, New Zealand. New Zealand Med. J. 2006, 119, U2145. [Google Scholar]
- Fedorova, S.A.; Khusainova, R.I.; Kutuev, I.A.; Sukhomiatova, A.L.; Nikolaeva, I.A.; Kulichkin, S.S.; Akhmetova, V.L.; Salimova, A.Z.; Sviatova, G.S.; Berezina, G.M.; et al. Polymorphism of CTG-repeats in the DMPK gene in populations of Yakutia and central Asia. Mol. Biol. 2005, 39, 385–393. [Google Scholar] [CrossRef]
- Thornton, C.A. Myotonic dystrophy. Neurol. Clin. 2014, 32, 705–719. [Google Scholar] [CrossRef]
- Krause, A.; Seymour, H.; Ramsay, M. Common and Founder Mutations for Monogenic Traits in Sub-Saharan African Populations. Annu. Rev. Genom. Hum. Genet. 2018, 19, 149–175. [Google Scholar] [CrossRef]
- Pan, H.; Lin, H.M.; Ku, W.Y.; Li, T.C.; Li, S.Y.; Lin, C.C.; Hsiao, K.M. Haplotype analysis of the myotonic dystrophy type 1 (DM1) locus in Taiwan: Implications for low prevalence and founder mutations of Taiwanese myotonic dystrophy type 1. Eur. J. Hum. Genet. 2001, 9, 638–641. [Google Scholar] [CrossRef]
- Lu, H.; Li, Y.; Sadowsky, M.; Da, Y. Clinical characteristics of 37 Chinese patients with myotonic dystrophy Type 1. Brain Circ. 2016, 2, 95–98. [Google Scholar] [CrossRef]
- Johnson, N.E.; Butterfield, R.J.; Mayne, K.; Newcomb, T.; Imburgia, C.; Dunn, D.; Duval, B.; Feldkamp, M.L.; Weiss, R.B. Population-Based Prevalence of Myotonic Dystrophy Type 1 Using Genetic Analysis of Statewide Blood Screening Program. Neurology 2021, 96, e1045–e1053. [Google Scholar] [CrossRef]
- Dean, N.L.; Tan, S.L.; Ao, A. Instability in the transmission of the myotonic dystrophy CTG repeat in human oocytes and preimplantation embryos. Fertil. Steril. 2006, 86, 98–105. [Google Scholar] [CrossRef]
- Welle, S.; Tawil, R.; Thornton, C.A. Sex-related differences in gene expression in human skeletal muscle. PLoS ONE 2008, 3, e1385. [Google Scholar] [CrossRef]
- Fialho, D.; Kullmann, D.M.; Hanna, M.G.; Schorge, S. Non-genomic effects of sex hormones on CLC-1 may contribute to gender differences in myotonia congenita. Neuromuscul. Disord. 2008, 18, 869–872. [Google Scholar] [CrossRef]
- Savić, D.; Keckarević, D.; Branković-Srećković, V.; Apostolski, S.; Todorović, S.; Romac, S. Clinical case report atypical myopathy in a young girl with 91 CTG repeats in DM1 locus and a positive DM1 family history. Int. J. Neurosci. 2006, 116, 1509–1518. [Google Scholar] [CrossRef]
- Joosten, I.B.T.; Hellebrekers, D.; de Greef, B.T.A.; Smeets, H.J.M.; de Die-Smulders, C.E.M.; Faber, C.G.; Gerrits, M.M. Parental repeat length instability in myotonic dystrophy type 1 pre- and protomutations. Eur. J. Hum. Genet. 2020, 28, 956–962. [Google Scholar] [CrossRef]
- Ashizawa, T.; Anvret, M.; Baiget, M.; Barceló, J.M.; Brunner, H.; Cobo, A.M.; Dallapiccola, B.; Fenwick, R.G., Jr.; Grandell, U.; Harley, H.; et al. Characteristics of intergenerational contractions of the CTG repeat in myotonic dystrophy. Am. J. Hum. Genet. 1994, 54, 414–423. [Google Scholar]
- Salehi, L.B.; Bonifazi, E.; Stasio, E.D.; Gennarelli, M.; Botta, A.; Vallo, L.; Iraci, R.; Massa, R.; Antonini, G.; Angelini, C.; et al. Risk prediction for clinical phenotype in myotonic dystrophy type 1: Data from 2,650 patients. Genet. Test. 2007, 11, 84–90. [Google Scholar] [CrossRef]
- De Temmerman, N.; Sermon, K.; Seneca, S.; De Rycke, M.; Hilven, P.; Lissens, W.; Van Steirteghem, A.; Liebaers, I. Intergenerational instability of the expanded CTG repeat in the DMPK gene: Studies in human gametes and preimplantation embryos. Am. J. Hum. Genet. 2004, 75, 325–329. [Google Scholar] [CrossRef]
- Barbé, L.; Lanni, S.; López-Castel, A.; Franck, S.; Spits, C.; Keymolen, K.; Seneca, S.; Tomé, S.; Miron, I.; Letourneau, J.; et al. CpG Methylation, a Parent-of-Origin Effect for Maternal-Biased Transmission of Congenital Myotonic Dystrophy. Am. J. Hum. Genet. 2017, 100, 488–505. [Google Scholar] [CrossRef]
- Yanovsky-Dagan, S.; Cohen, E.; Megalli, P.; Altarescu, G.; Schonberger, O.; Eldar-Geva, T.; Epsztejn-Litman, S.; Eiges, R. DMPK hypermethylation in sperm cells of myotonic dystrophy type 1 patients. Eur. J. Hum. Genet. 2022, 30, 980–983. [Google Scholar] [CrossRef]
- Tomé, S.; Dandelot, E.; Dogan, C.; Bertrand, A.; Geneviève, D.; Péréon, Y.; Simon, M.; Bonnefont, J.P.; Bassez, G.; Gourdon, G. Unusual association of a unique CAG interruption in 5’ of DM1 CTG repeats with intergenerational contractions and low somatic mosaicism. Hum. Mutat. 2018, 39, 970–982. [Google Scholar] [CrossRef]
- Pešović, J.; Perić, S.; Brkušanin, M.; Brajušković, G.; Rakočević-Stojanović, V.; Savić-Pavićević, D. Molecular genetic and clinical characterization of myotonic dystrophy type 1 patients carrying variant repeats within DMPK expansions. Neurogenetics 2017, 18, 207–218. [Google Scholar] [CrossRef]
- Cumming, S.A.; Hamilton, M.J.; Robb, Y.; Gregory, H.; McWilliam, C.; Cooper, A.; Adam, B.; McGhie, J.; Hamilton, G.; Herzyk, P.; et al. De novo repeat interruptions are associated with reduced somatic instability and mild or absent clinical features in myotonic dystrophy type 1. Eur. J. Hum. Genet. 2018, 26, 1635–1647. [Google Scholar] [CrossRef] [PubMed]
- Mangin, A.; de Pontual, L.; Tsai, Y.C.; Monteil, L.; Nizon, M.; Boisseau, P.; Mercier, S.; Ziegle, J.; Harting, J.; Heiner, C.; et al. Robust Detection of Somatic Mosaicism and Repeat Interruptions by Long-Read Targeted Sequencing in Myotonic Dystrophy Type 1. Int. J. Mol. Sci. 2021, 22, 2616. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, M.L.; Leoncini, E.; Masciullo, M.; Modoni, A.; Gadalla, S.M.; Massa, R.; Rastelli, E.; Terracciano, C.; Antonini, G.; Bucci, E.; et al. Increased risk of tumor in DM1 is not related to exposure to common lifestyle risk factors. J. Neurol. 2016, 263, 492–498. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
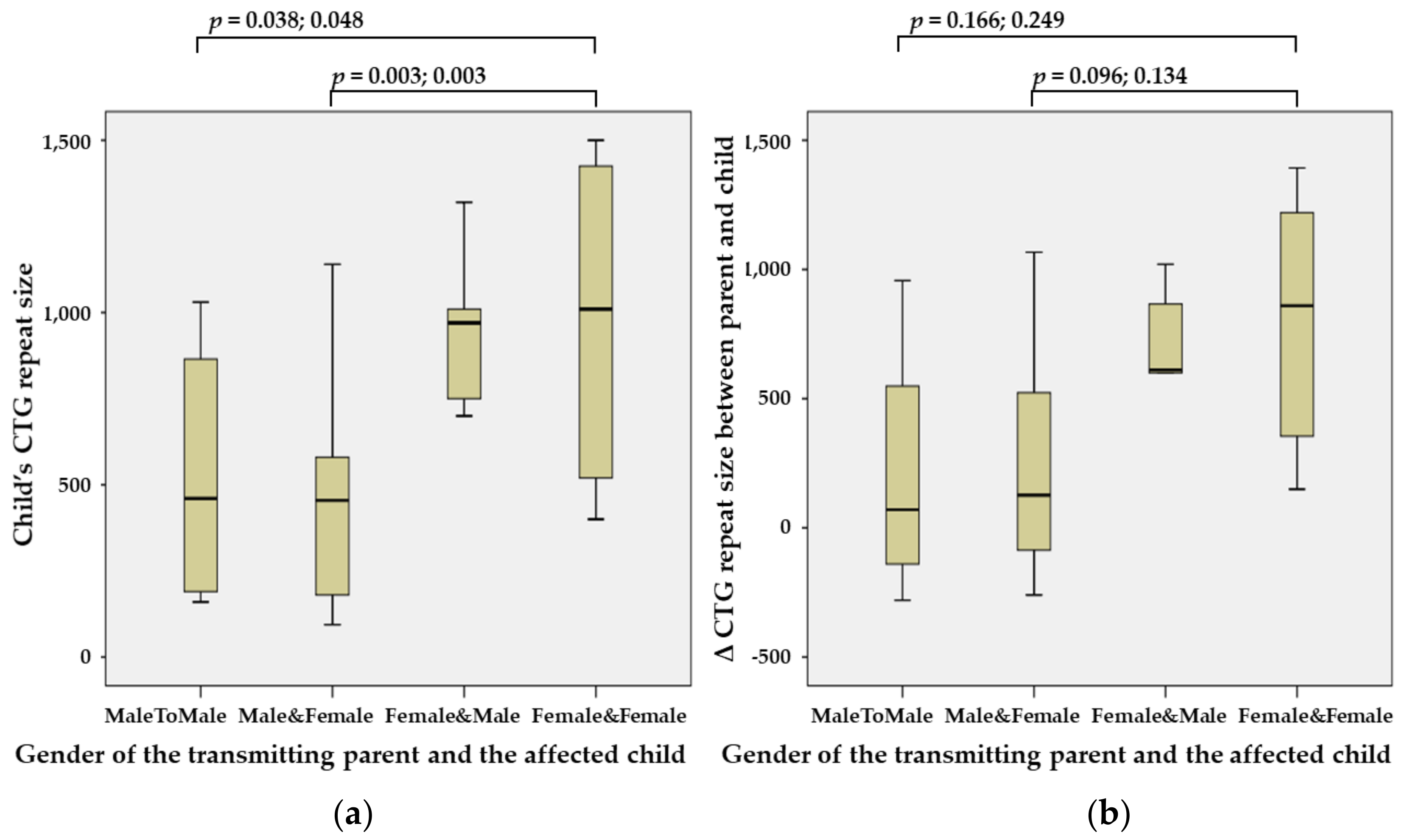
| Parent Gender | Child Gender | Child DM1 Phenotype | Child’s Repeat Size; Median (Range) | Δ Repeat Size; Median (Range) | ||
|---|---|---|---|---|---|---|
| Mild | Classic | Congenital | ||||
| Male | Male | 0 | 4 | 1 | 650 (160–1030) | 70 (−280–957) |
| Male | Female | 1 | 9 | 1 | 480 (94–1140) | 127 (−260–1067) |
| Female | Male | 0 | 8 | 6 | 970 (220–1667) | 611 (10–1020) |
| Female | Female | 0 | 4 | 10 | 1309 (400–2083) | 860 (150–1393) |
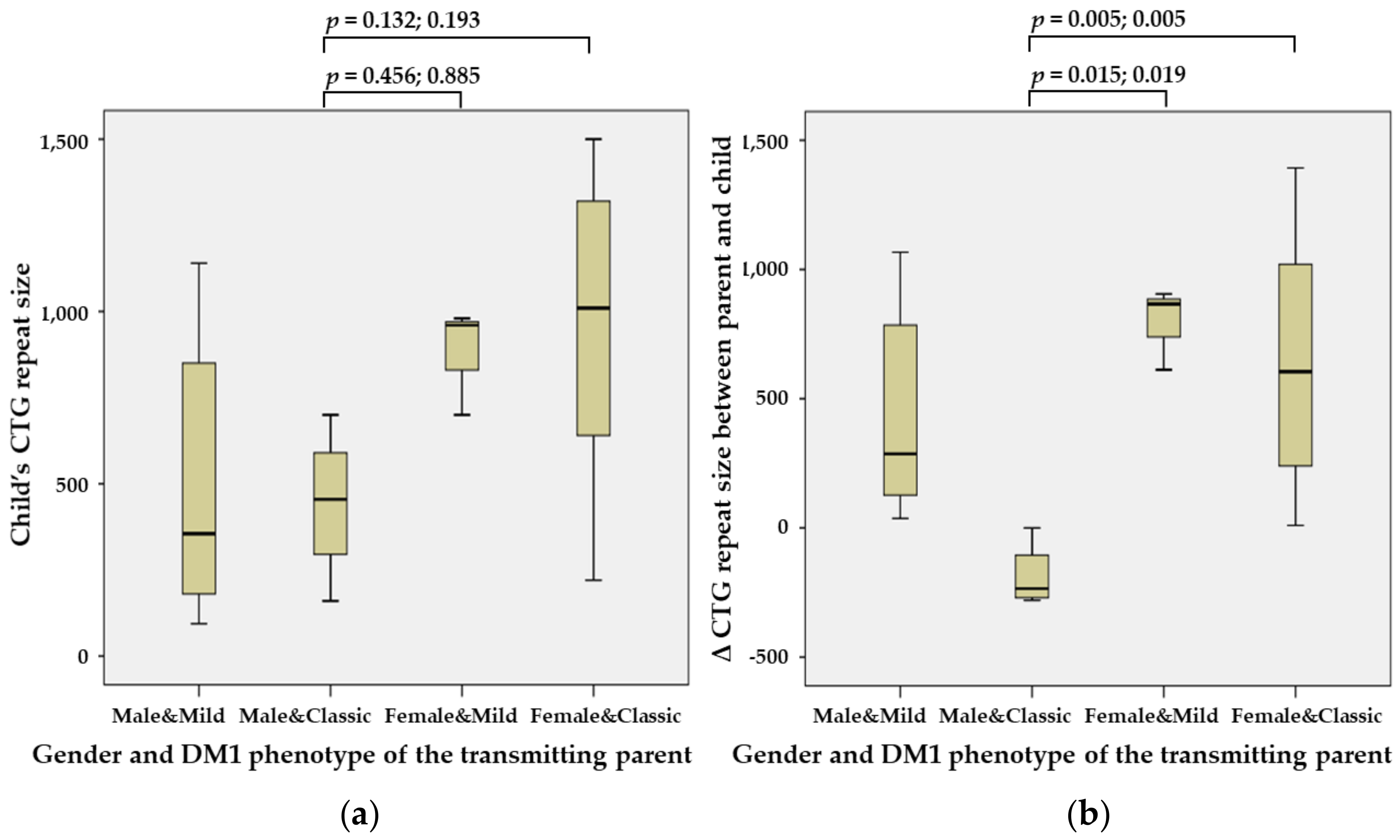
| Parent Gender | Parent Phenotype | Child DM1 Phenotype | Child’s Repeat Size; Median (Range) | Δ Repeat Size; Median (Range) | ||
|---|---|---|---|---|---|---|
| Mild | Classic | Congenital | ||||
| Male | Mild | 1 | 5 | 2 | 355 (94–1140) | 287 (37–1067) |
| Male | Classic | 0 | 4 | 0 | 455 (160–700) | −235 (−280–0) |
| Female | Mild | 0 | 3 | 0 | 960 (700–980) | 866 (612–905) |
| Female | Classic | 0 | 6 | 8 | 1010 (220–1500) | 605 (10–1393) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, J.Y.; Jang, W.; Park, J. Intergenerational Influence of Gender and the DM1 Phenotype of the Transmitting Parent in Korean Myotonic Dystrophy Type 1. Genes 2022, 13, 1465. https://doi.org/10.3390/genes13081465
Han JY, Jang W, Park J. Intergenerational Influence of Gender and the DM1 Phenotype of the Transmitting Parent in Korean Myotonic Dystrophy Type 1. Genes. 2022; 13(8):1465. https://doi.org/10.3390/genes13081465
Chicago/Turabian StyleHan, Ji Yoon, Woori Jang, and Joonhong Park. 2022. "Intergenerational Influence of Gender and the DM1 Phenotype of the Transmitting Parent in Korean Myotonic Dystrophy Type 1" Genes 13, no. 8: 1465. https://doi.org/10.3390/genes13081465