
Assessment of Bidirectional Relationships between Leisure Sedentary Behaviors and Neuropsychiatric Disorders: A Two-Sample Mendelian Randomization Study

 , , and
, , and
Abstract
:1. Introduction
2. Methods and Materials
2.1. Data Sources and Instruments
2.1.1. Leisure Sedentary Behaviors
2.1.2. AD
2.1.3. SCZ
2.1.4. MDD
2.2. Linkage Disequilibrium Score Regression (LDSC) of Genetic Correlation
2.3. Instrument Variable Selection
2.4. Statistical Analyses
2.5. Pleiotropy in MR Analyses
2.6. Weak Instrumental Bias in MR Analyses
3. Results
3.1. Genetic Correlation between Sedentary Behaviors and NPDs
3.2. MR Analyses
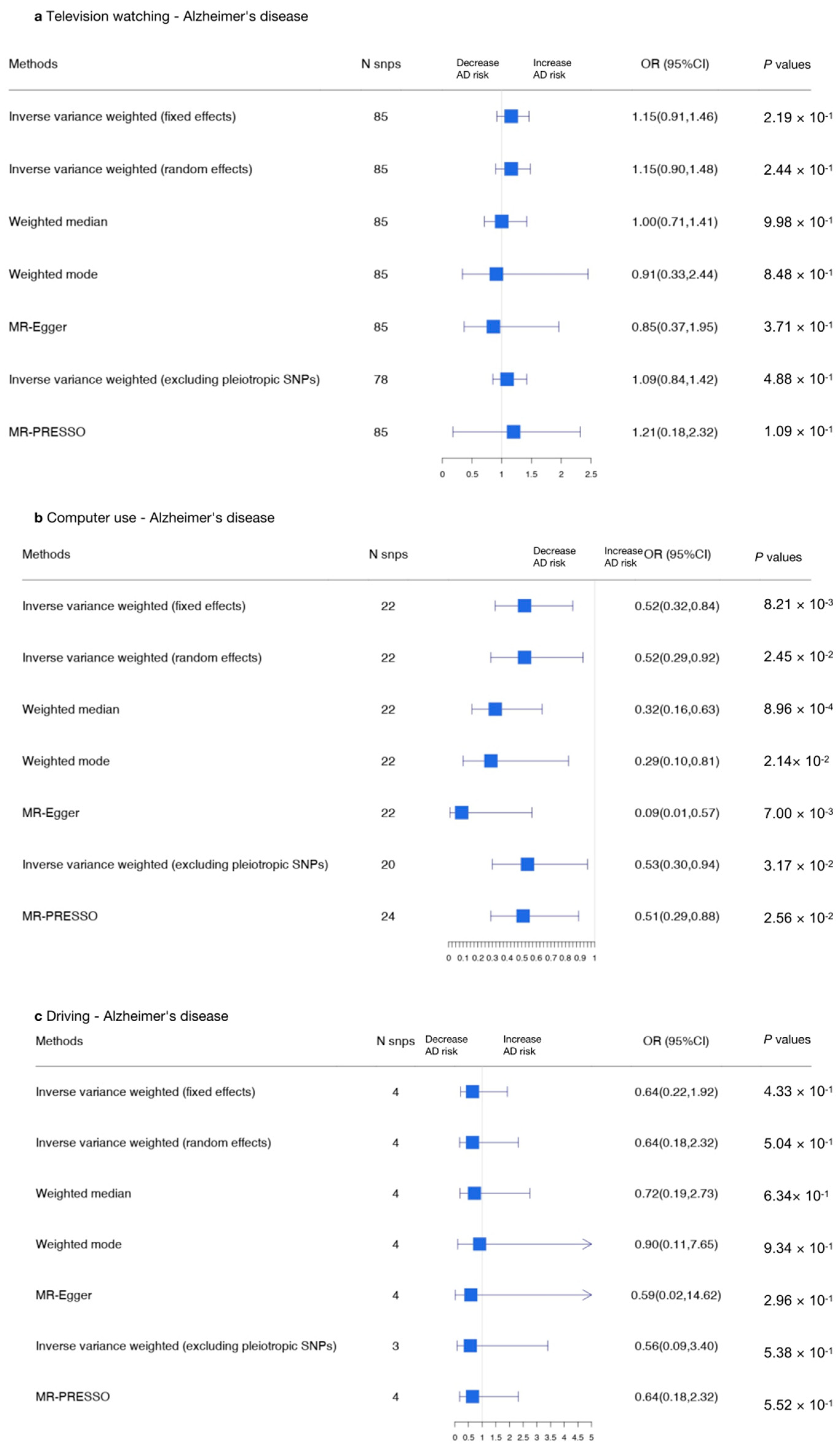
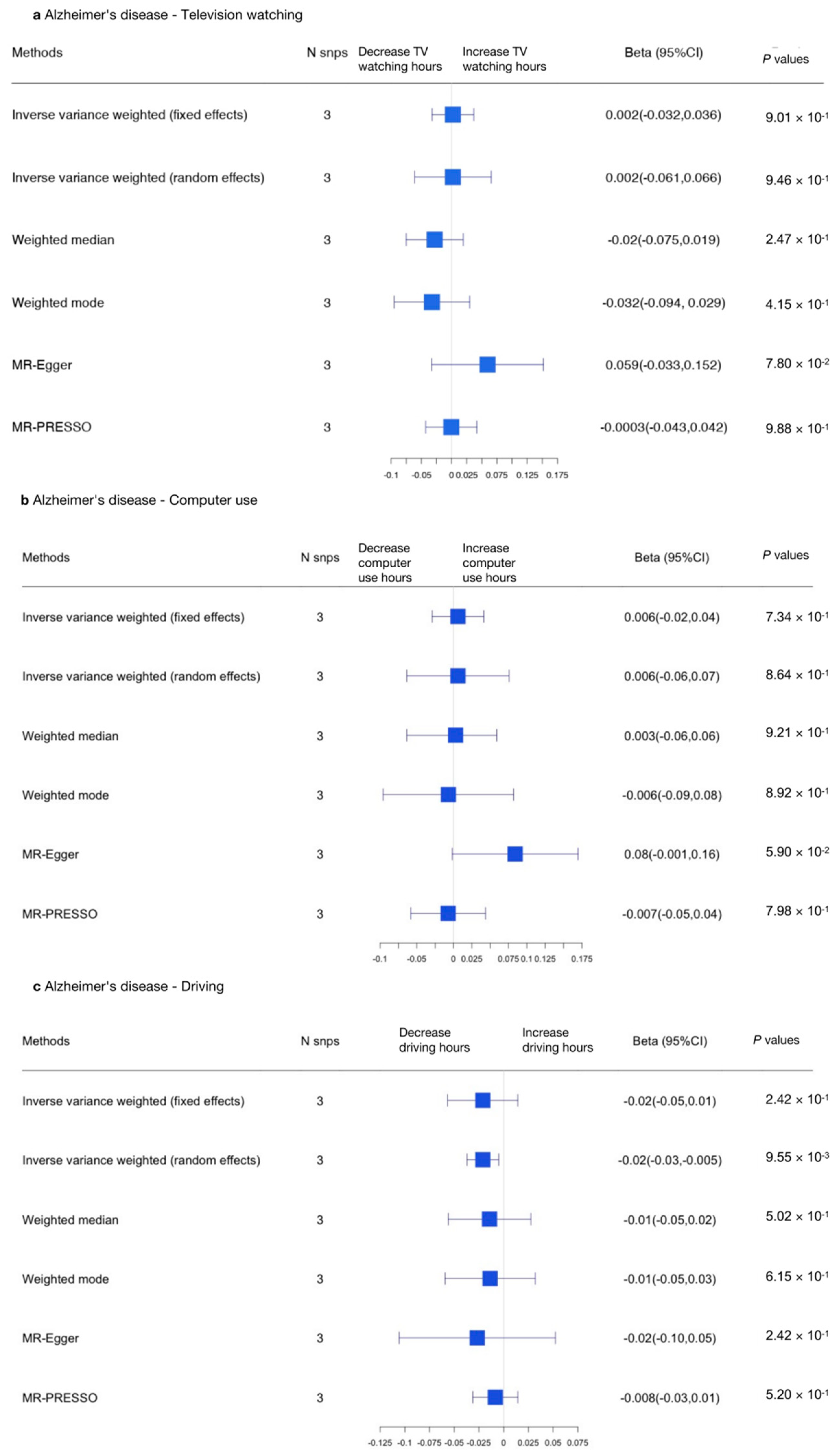
3.2.1. Sedentary Behaviors and AD
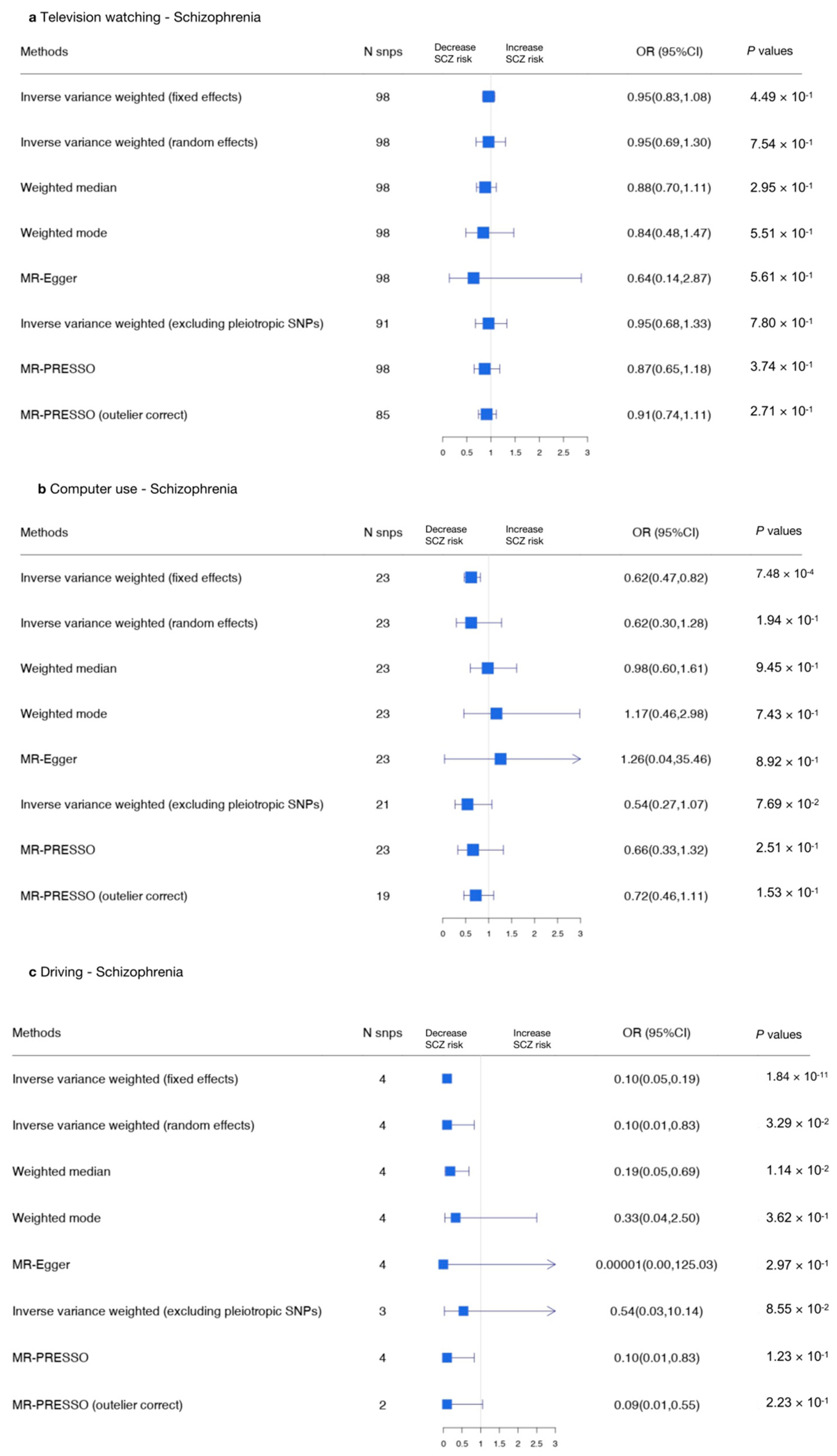
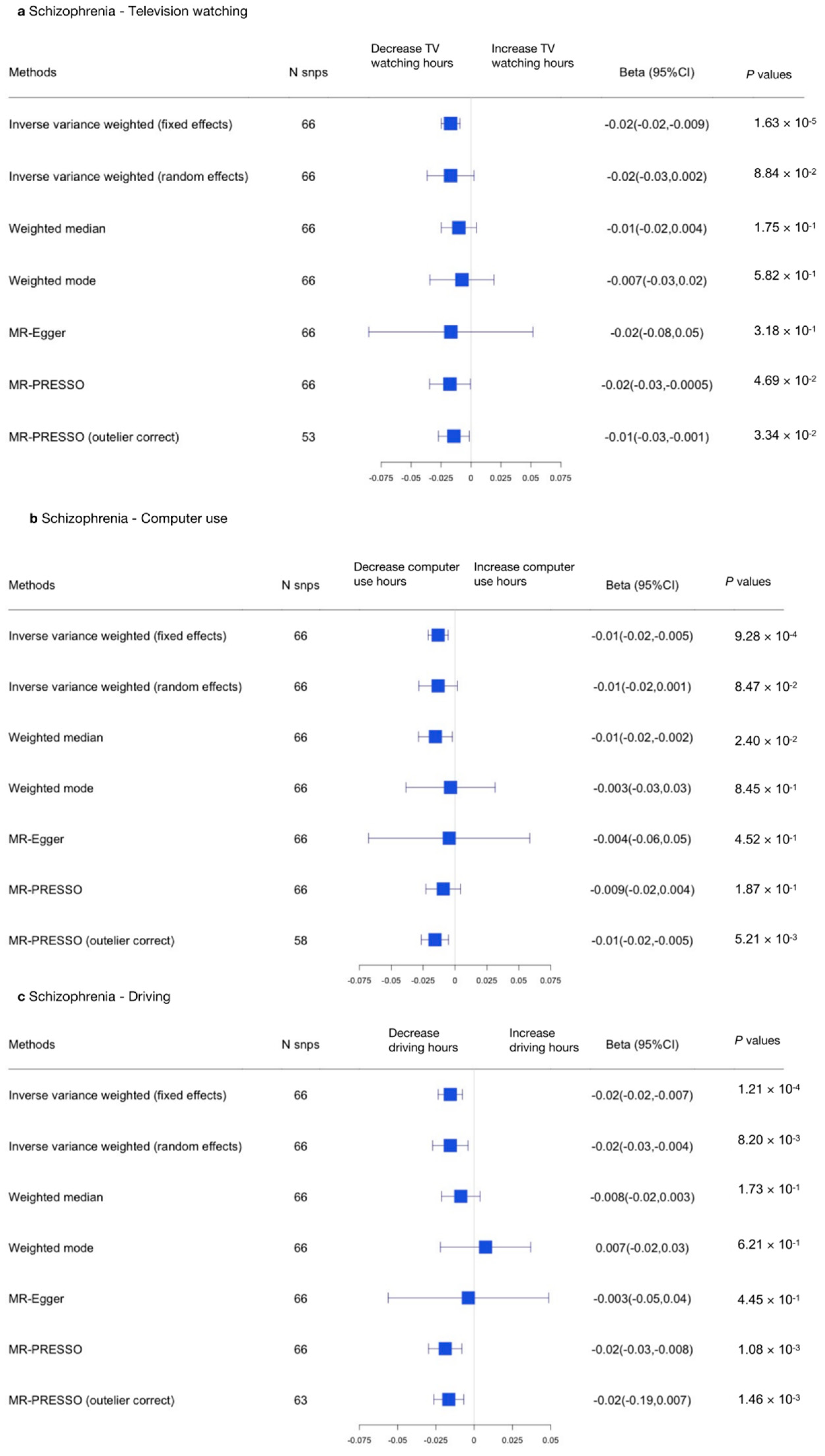
3.2.2. Sedentary Behaviors and SCZ
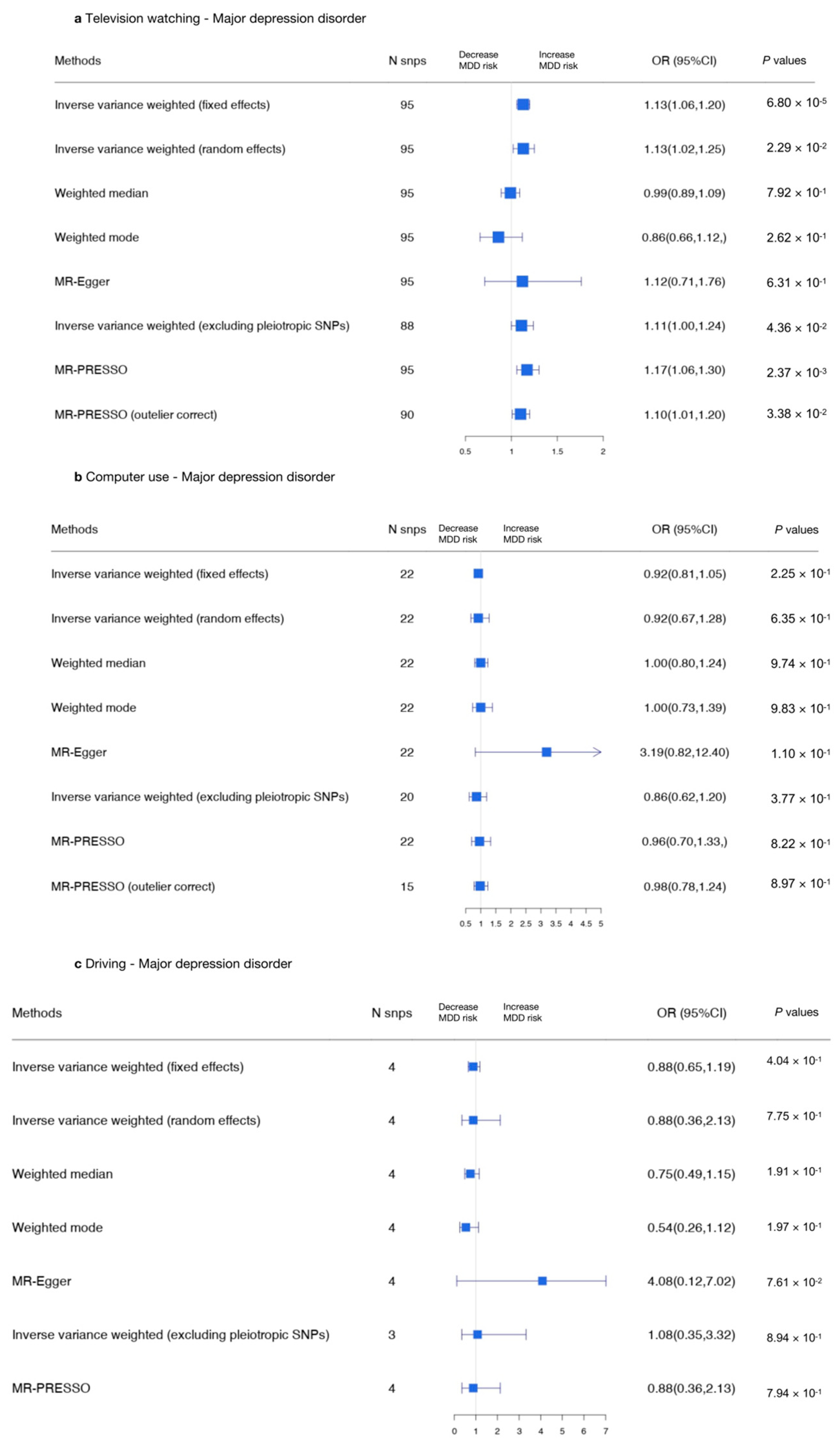
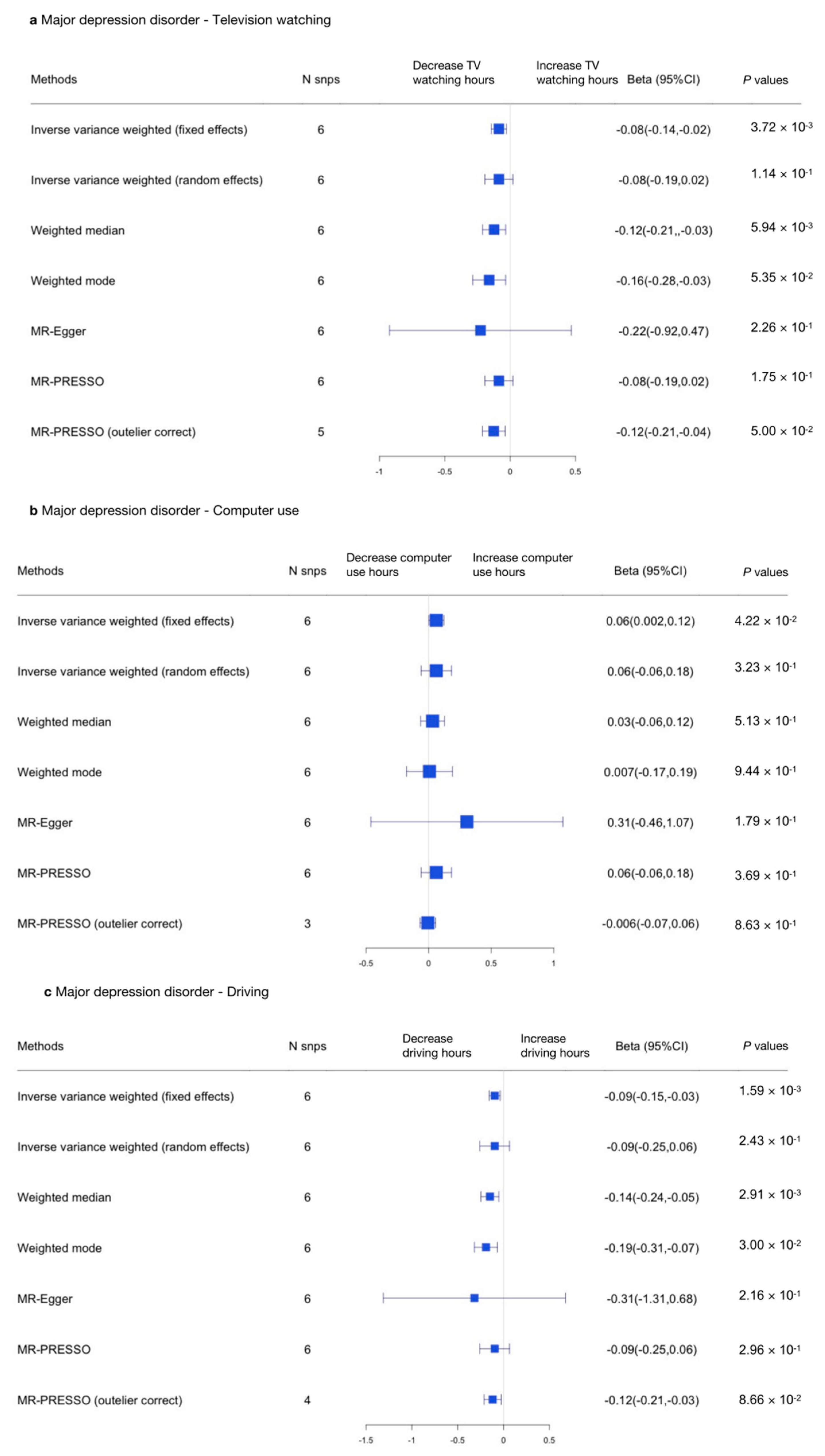
3.2.3. Sedentary Behaviors and MDD
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stein, D.J.; Phillips, K.A.; Bolton, D.; Fulford, K.W.M.; Sadler, J.Z.; Kendler, K.S. What is a mental/psychiatric disorder? From DSM-IV to DSM-V. Psychol. Med. 2010, 40, 1759–1765. [Google Scholar] [CrossRef] [Green Version]
- Das-Munshi, J.; Ford, T.; Hotopf, M.; Prince, M.; Stewart, R. Practical Psychiatric Epidemiology; Oxford University Press: Oxford, UK, 2020. [Google Scholar] [CrossRef]
- Reichenberg, A.; Levine, S.Z. Primary challenges and practical solutions in preventive psychiatry. World Psychiatry 2021, 20, 228–230. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. On Behalf of SBRN Terminology Consensus Project Participants. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Vancampfort, D.; Firth, J.; Schuch, F.; Rosenbaum, S.; Mugisha, J.; Hallgren, M.; Probst, M.; Ward, P.; Gaughran, F.; De Hert, M.; et al. Sedentary behavior and physical activity levels in people with schizophrenia, bipolar disorder and major depressive disorder: A global systematic review and meta-analysis. World Psychiatry 2017, 16, 308–315. [Google Scholar] [CrossRef]
- Bort-Roig, J.; Briones-Buixassa, L.; Felez-Nobrega, M.; Guàrdia-Sancho, A.; Sitjà-Rabert, M.; Puig-Ribera, A. Sedentary behaviour associations with health outcomes in people with severe mental illness: A systematic review. Eur. J. Public Health 2019, 30, 150–157. [Google Scholar] [CrossRef]
- Huang, Y.; Li, L.; Gan, Y.; Wang, C.; Jiang, H.; Cao, S.; Lu, Z. Sedentary behaviors and risk of depression: A meta-analysis of prospective studies. Transl. Psychiatry 2020, 10, 26. [Google Scholar] [CrossRef] [Green Version]
- Falck, R.S.; Davis, J.C.; Liu-Ambrose, T. What is the association between sedentary behaviour and cognitive function? A systematic review. Br. J. Sports Med. 2016, 51, 800–811. [Google Scholar] [CrossRef] [Green Version]
- Carpenter, C.A.; Miller, M.C.; Sui, X.; West, D.S. Weight Status and Sedentary Behavior of Alzheimer’s Disease Caregivers. Am. J. Health Behav. 2020, 44, 3–12. [Google Scholar] [CrossRef]
- Strassnig, M.T.; Harvey, P.D.; Miller, M.L.; Depp, C.A.; Granholm, E. Real world sedentary behavior and activity levels in patients with schizophrenia and controls: An ecological momentary assessment study. Ment. Health Phys. Act. 2020, 20, 100364. [Google Scholar] [CrossRef]
- Hallgren, M.; Dunstan, D.W.; Owen, N. Passive Versus Mentally Active Sedentary Behaviors and Depression. Exerc. Sport Sci. Rev. 2019, 48, 20–27. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.B.; Silva, E.S.; Hallgren, M.; De Leon, A.P.; Dunn, A.L.; Deslandes, A.C.; et al. Physical Activity and Incident Depression: A Meta-Analysis of Prospective Cohort Studies. Am. J. Psychiatry 2018, 175, 631–648. [Google Scholar] [CrossRef]
- Vancampfort, D.; Stubbs, B.; Firth, J.; Hallgren, M.; Schuch, F.; Lahti, J.; Rosenbaum, S.; Ward, P.B.; Mugisha, J.; Carvalho, A.F.; et al. Physical activity correlates among 24,230 people with depression across 46 low- and middle-income countries. J. Affect. Disord. 2017, 221, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Zschucke, E.; Gaudlitz, K.; Ströhle, A. Exercise and Physical Activity in Mental Disorders: Clinical and Experimental Evidence. J. Prev. Med. Public Health 2013, 46, S12–S21. [Google Scholar] [CrossRef] [Green Version]
- Delgado-Floody, P.; Guzmán-Guzmán, I.P.; Caamaño-Navarrete, F.; Jerez-Mayorga, D.; Zulic-Agramunt, C.; Cofré-Lizama, A. Depression is associated with lower levels of physical activity, body image dissatisfaction, and obesity in Chilean preadolescents. Psychol. Health Med. 2020, 26, 518–531. [Google Scholar] [CrossRef]
- Wanders, L.; Bakker, E.A.; van Hout, H.P.; Eijsvogels, T.M.; Hopman, M.T.; Visser, L.N.; Wouters, H.; Thijssen, D.H. Association between sedentary time and cognitive function: A focus on different domains of sedentary behavior. Prev. Med. 2021, 153, 106731. [Google Scholar] [CrossRef]
- Choi, K.W.; Chen, C.-Y.; Stein, M.B.; Klimentidis, Y.; Wang, M.-J.; Koenen, K.C.; Smoller, J.W.; For the Major Depressive Disorder Working Group of the Psychiatric Genomics Consortium. Assessment of Bidirectional Relationships Between Physical Activity and Depression Among Adults: A 2-Sample Mendelian Randomization Study. JAMA Psychiatry 2019, 76, 399–408. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.; Stubbs, B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef] [Green Version]
- Van de Vegte, Y.; Said, M.A.; Rienstra, M.; Van Der Harst, P.; Verweij, N. Genome-wide association studies and Mendelian randomization analyses for leisure sedentary behaviours. Nat. Commun. 2020, 11, 1770. [Google Scholar] [CrossRef] [Green Version]
- Kunkle, B.W.; Grenier-Boley, B.; Sims, R.; Bis, J.C.; Damotte, V.; Naj, A.C.; Boland, A.; Vronskaya, M.; Van Der Lee, S.J.; Amlie-Wolf, A.; et al. Genetic meta-analysis of diagnosed Alzheimer’s disease identifies new risk loci and implicates Aβ, tau, immunity and lipid processing. Nat. Genet. 2019, 51, 414–430. [Google Scholar] [CrossRef] [Green Version]
- Wray, N.R.; Ripke, S.; Mattheisen, M.; Trzaskowski, M.; Byrne, E.M.; Abdellaoui, A.; Adams, M.J.; Agerbo, E.; Air, T.M.; Andlauer, T.M.F.; et al. Genome-wide association analyses identify 44 risk variants and refine the genetic architecture of major depression. Nat. Genet. 2018, 50, 668–681. [Google Scholar] [CrossRef] [Green Version]
- Pardiñas, A.F.; Holmans, P.; Pocklington, A.J.; Escott-Price, V.; Ripke, S.; Carrera, N.; Legge, S.E.; Bishop, S.; Cameron, D.; Hamshere, M.L.; et al. Common schizophrenia alleles are enriched in mutation-intolerant genes and in regions under strong background selection. Nat. Genet. 2018, 50, 381–389. [Google Scholar] [CrossRef] [Green Version]
- Zhuang, Z.; Gao, M.; Yang, R.; Li, N.; Liu, Z.; Cao, W.; Huang, T. Association of physical activity, sedentary behaviours and sleep duration with cardiovascular diseases and lipid profiles: A Mendelian randomization analysis. Lipids Health Dis. 2020, 19, 86. [Google Scholar] [CrossRef]
- Bulik-Sullivan, B.K.; Loh, P.-R.; Finucane, H.K.; Ripke, S.; Yang, J.; Patterson, N.; Daly, M.J.; Price, A.L.; Neale, B.M. LD Score Regression Distinguishes Confounding from Polygenicity in Genome-Wide Association Studies. Nat. Genet. 2015, 47, 291–295. [Google Scholar] [CrossRef] [Green Version]
- Bulik-Sullivan, B.; Finucane, H.K.; Anttila, V.; Gusev, A.; Day, F.R.; Loh, P.-R.; Duncan, L.; Perry, J.R.B.; Patterson, N.; Robinson, E.B.; et al. An atlas of genetic correlations across human diseases and traits. Nat. Genet. 2015, 47, 1236–1241. [Google Scholar] [CrossRef] [Green Version]
- International HapMap 3 Consortium. Integrating common and rare genetic variation in diverse human populations. Nature 2010, 467, 52–58. [Google Scholar] [CrossRef]
- Hemani, G.; Zheng, J.; Elsworth, B.; Wade, K.H.; Haberland, V.; Baird, D.; Laurin, C.; Burgess, S.; Bowden, J.; Langdon, R.; et al. The MR-Base platform supports systematic causal inference across the human phenome. eLife 2018, 7, e34408. [Google Scholar] [CrossRef]
- Greco, M.F.D.; Minelli, C.; Sheehan, N.; Thompson, J.R. Detecting pleiotropy in Mendelian randomisation studies with summary data and a continuous outcome. Stat. Med. 2015, 34, 2926–2940. [Google Scholar] [CrossRef] [Green Version]
- Bowden, J.; Del Greco, M.F.; Minelli, C.; Davey Smith, G.; Sheehan, N.; Thompson, J. A framework for the investigation of pleiotropy in two-sample summary data Mendelian randomization. Stat. Med. 2017, 36, 1783–1802. [Google Scholar] [CrossRef] [Green Version]
- Verbanck, M.; Chen, C.-Y.; Neale, B.; Do, R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat. Genet. 2018, 50, 693–698. [Google Scholar] [CrossRef]
- Hemani, G.; Tilling, K.; Smith, G.D. Orienting the causal relationship between imprecisely measured traits using GWAS summary data. PLoS Genet. 2017, 13, e1007081. [Google Scholar] [CrossRef] [Green Version]
- Bowden, J.; Smith, G.D.; Haycock, P.C.; Burgess, S. Consistent Estimation in Mendelian Randomization with Some Invalid Instruments Using a Weighted Median Estimator. Genet. Epidemiol. 2016, 40, 304–314. [Google Scholar] [CrossRef] [Green Version]
- Hartwig, F.P.; Smith, G.D.; Bowden, J. Robust inference in summary data Mendelian randomization via the zero modal pleiotropy assumption. Int. J. Epidemiol. 2017, 46, 1985–1998. [Google Scholar] [CrossRef] [Green Version]
- Palmer, T.M.; Lawlor, D.A.; Harbord, R.; Sheehan, N.; Tobias, J.; Timpson, N.; Smith, G.D.; Sterne, J. Using multiple genetic variants as instrumental variables for modifiable risk factors. Stat. Methods Med. Res. 2011, 21, 223–242. [Google Scholar] [CrossRef] [Green Version]
- Tu, C.-H.; Macdonald, I.; Chen, Y.-H. The Effects of Acupuncture on Glutamatergic Neurotransmission in Depression, Anxiety, Schizophrenia, and Alzheimer’s Disease: A Review of the Literature. Front. Psychiatry 2019, 10, 14. [Google Scholar] [CrossRef] [Green Version]
- Arango, C.; Díaz-Caneja, C.M.; McGorry, P.D.; Rapoport, J.; Sommer, I.E.; Vorstman, J.A.; McDaid, D.; Marín, O.; Serrano-Drozdowskyj, E.; Freedman, R.; et al. Preventive strategies for mental health. Lancet Psychiatry 2018, 5, 591–604. [Google Scholar] [CrossRef]
- Hoare, E.; Milton, K.; Foster, C.; Allender, S. The associations between sedentary behaviour and mental health among adolescents: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 108. [Google Scholar] [CrossRef] [Green Version]
- Yan, S.; Fu, W.; Wang, C.; Mao, J.; Liu, B.; Zou, L.; Lv, C. Association between sedentary behavior and the risk of dementia: A systematic review and meta-analysis. Transl. Psychiatry 2020, 10, 112. [Google Scholar] [CrossRef]
- Hallgren, M.; Nguyen, T.-T.; Owen, N.; Vancampfort, D.; Smith, L.; Dunstan, D.W.; Andersson, G.; Wallin, P.; Ekblom-Bak, E. Associations of interruptions to leisure-time sedentary behaviour with symptoms of depression and anxiety. Transl. Psychiatry 2020, 10, 128. [Google Scholar] [CrossRef]
- Soundy, A.; Wampers, M.; Probst, M.; De Hert, M.; Stubbs, B.; Vancampfort, D.; Attux, C.; Leutwyler, H.; Ströhle, A. Physical activity and sedentary behaviour in outpatients with schizophrenia: A systematic review and meta-analysis. Int. J. Ther. Rehabil. 2013, 20, 588–595. [Google Scholar] [CrossRef]
- Kandola, A.; Ashdown-Franks, G.; Hendrikse, J.; Sabiston, C.M.; Stubbs, B. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav. Rev. 2019, 107, 525–539. [Google Scholar] [CrossRef]
- Tun, P.A.; Lachman, M.E. The association between computer use and cognition across adulthood: Use it so you won’t lose it? Psychol. Aging 2010, 25, 560–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.-H.; Lewis, M.; Rigaud, A.-S. Cognitive Function and Digital Device Use in Older Adults Attending a Memory Clinic. Gerontol. Geriatr. Med. 2019, 5, 2333721419844886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapman, J.J.; Fraser, S.J.; Brown, W.J.; Burton, N.W. Physical activity and sedentary behaviour of adults with mental illness. J. Sci. Med. Sport 2015, 19, 579–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rashid, N.A.A.; Nurjono, M.; Lee, J. Clinical determinants of physical activity and sedentary behaviour in individuals with schizophrenia. Asian J. Psychiatry 2019, 46, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Bueno-Antequera, J.; Oviedo-Caro, M.; Munguía-Izquierdo, D. Relationship between objectively measured sedentary behavior and health outcomes in schizophrenia patients: The PsychiActive project. Schizophr. Res. 2018, 197, 87–92. [Google Scholar] [CrossRef]
- Boberska, M.; Szczuka, Z.; Kruk, M.; Knoll, N.; Keller, J.; Hohl, D.H.; Luszczynska, A. Sedentary behaviours and health-related quality of life. A systematic review and meta-analysis. Health Psychol. Rev. 2017, 12, 195–210. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Constrained Intercept | Unconstrained Intercept | ||||||
|---|---|---|---|---|---|---|---|
| Television Watching | Computer Use | Driving | Television Watching | Computer Use | Driving | ||
| Outcome: AD | |||||||
| Cross-trait | Genetic correlation (rg ± SE) | 0.1500 ± 0.0259 | −0.1741 ± 0.0258 | 0.0926 ± 0.0338 | 0.2232 ± 0.0701 | −0.2475 ± 0.0675 | 0.1112 ± 0.0815 |
| LDSC | Prg | 6.74 × 10−9 | 1.59 × 10−11 | 6.08 × 10−3 | 1.50 × 10−3 | 2.00 × 10−4 | 1.72 × 10−1 |
| Outcome: SCZ | |||||||
| Cross-trait | Genetic correlation (rg ± SE) | −0.08 ± 0.0119 | −0.0747 ± 0.0135 | −0.1581 ± 0.0171 | −0.0981 ± 0.0175 | −0.0682 ± 0.0209 | −0.1869 ± 0.0272 |
| LDSC | Prg | 1.97 × 10−11 | 3.28 × 10−8 | 3.04 × 10−20 | 2.02 × 10−8 | 1.12 × 10−3 | 5.93 × 10−12 |
| Outcome: MDD | |||||||
| Cross-trait | Genetic correlation (rg ± SE) | 0.194 ± 0.0128 | 0.0392 ± 0.0169 | −0.1611 ± 0.0200 | 0.125 ± 0.0193 | 0.0182 ± 0.0257 | −0.0652 ± 0.0285 |
| LDSC | Prg | 9.87 × 10−52 | 2.03 × 10−2 | 1.02 × 10−17 | 9.24 × 10−11 | 4.77 × 10−1 | 2.22 × 10−2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, Q.; Bennett, A.N.; Fan, B.; Han, X.; Liu, J.; Wu, K.C.H.; Huang, R.; Chan, J.C.N.; Chan, K.H.K. Assessment of Bidirectional Relationships between Leisure Sedentary Behaviors and Neuropsychiatric Disorders: A Two-Sample Mendelian Randomization Study. Genes 2022, 13, 962. https://doi.org/10.3390/genes13060962
He Q, Bennett AN, Fan B, Han X, Liu J, Wu KCH, Huang R, Chan JCN, Chan KHK. Assessment of Bidirectional Relationships between Leisure Sedentary Behaviors and Neuropsychiatric Disorders: A Two-Sample Mendelian Randomization Study. Genes. 2022; 13(6):962. https://doi.org/10.3390/genes13060962
Chicago/Turabian StyleHe, Qian, Adam N. Bennett, Beifang Fan, Xue Han, Jundong Liu, Kevin Chun Hei Wu, Ruixuan Huang, Juliana C. N. Chan, and Kei Hang Katie Chan. 2022. "Assessment of Bidirectional Relationships between Leisure Sedentary Behaviors and Neuropsychiatric Disorders: A Two-Sample Mendelian Randomization Study" Genes 13, no. 6: 962. https://doi.org/10.3390/genes13060962