Lifespans of Twins: Does Zygosity Matter?

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Danish Twin Registry
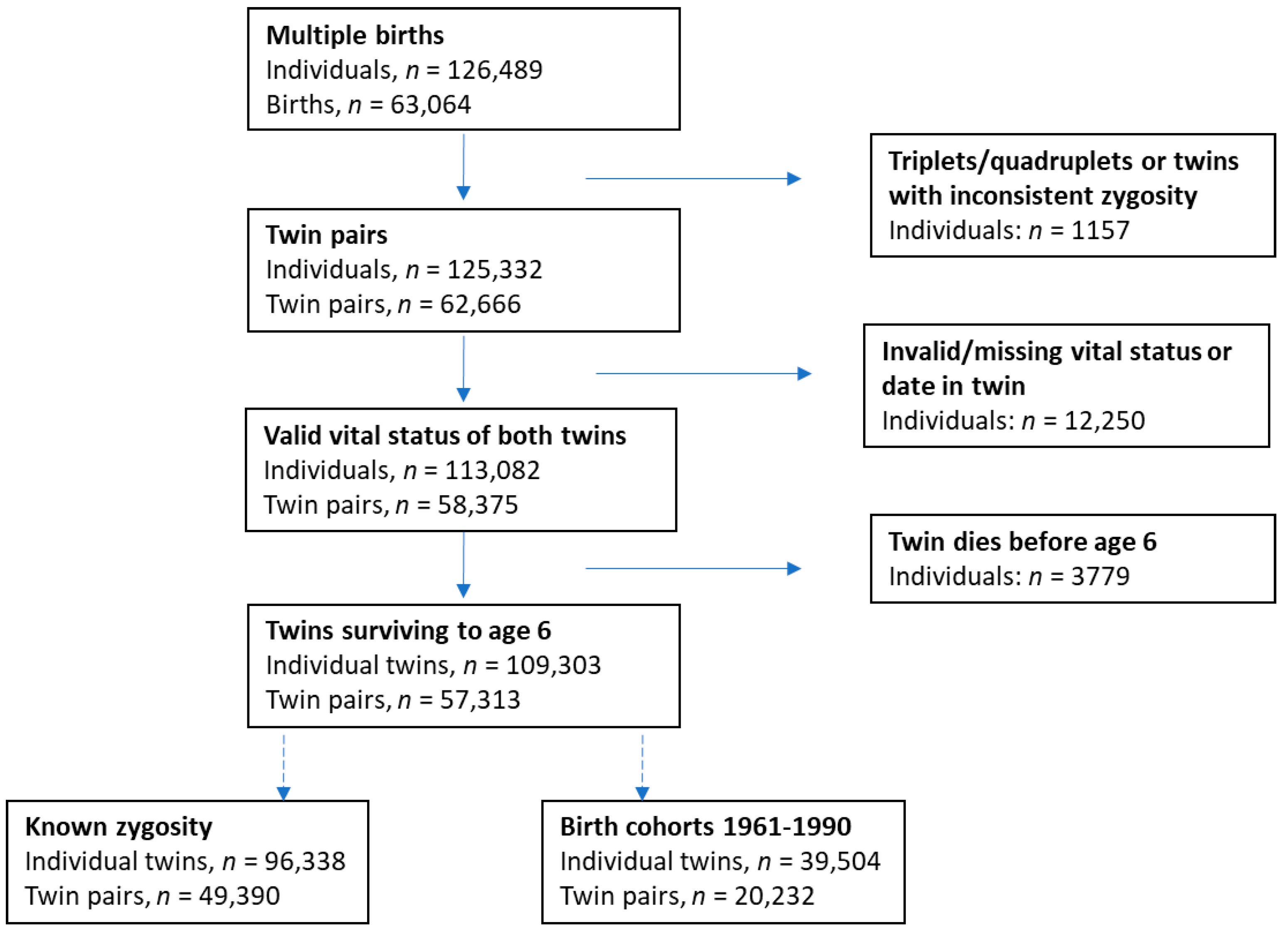
2.2. Study Population
2.3. Statistical Analyses
3. Results
4. Discussion
4.1. Main Findings
4.2. Comparisons with Other Studies
4.3. Strengths and Weaknesses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Polderman, T.J.; Benyamin, B.; de Leeuw, C.A.; Sullivan, P.F.; van Bochoven, A.; Visscher, P.M.; Posthuma, D. Meta-analysis of the heritability of human traits based on fifty years of twin studies. Nat. Genet. 2015, 47, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Ahrenfeldt, L.J.; Larsen, L.A.; Lindahl-Jacobsen, R.; Skytthe, A.; Hjelmborg, J.V.; Moller, S.; Christensen, K. Early-life mortality risks in opposite-sex and same-sex twins: A Danish cohort study of the twin testosterone transfer hypothesis. Ann. Epidemiol. 2017, 27, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Loos, R.; Derom, C.; Vlietinck, R.; Derom, R. The East Flanders Prospective Twin Survey (Belgium): A population-based register. Twin Res. 1998, 1, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Hjelmborg, J.V.B.; Iachine, I.; Skytthe, A.; Vaupel, J.W.; McGue, M.; Koskenvuo, M.; Kaprio, J.; Pedersen, N.L.; Christensen, K. Genetic influence on human lifespan and longevity. Hum. Genet. 2006, 119, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Scheike, T.H.; Holst, K.K.; von Bornemann Hjelmborg, J. Estimating twin concordance for bivariate competing risks twin data. Stat. Med. 2014, 33, 1193–1204. [Google Scholar] [CrossRef] [PubMed]
- Christensen, K.; Vaupel, J.W.; Holm, N.V.; Yashin, A.I. Mortality among twins after age 6: Fetal origins hypothesis versus twin method. BMJ 1995, 310, 432–436. [Google Scholar] [CrossRef] [PubMed]
- Kaprio, J. The Finnish Twin Cohort Study: An update. Twin Res. Hum. Genet. 2013, 16, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, J.C.; Fowler, M.G.; Kessel, S.S. Comparison of infant mortality among twins and singletons: United States 1960 and 1983. Am. J. Epidemiol. 1991, 133, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Sharrow, D.J.; Anderson, J.J. A Twin Protection Effect? Explaining Twin Survival Advantages with a Two-Process Mortality Model. PLoS ONE 2016, 11, e0154774. [Google Scholar] [CrossRef] [PubMed]
- Skytthe, A.; Kyvik, K.; Holm, N.V.; Vaupel, J.W.; Christensen, K. The Danish Twin Registry: 127 birth cohorts of twins. Twin Res. 2002, 5, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Skytthe, A.; Kyvik, K.O.; Holm, N.V.; Christensen, K. The Danish Twin Registry. Scand. J. Public Health 2011, 39, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Sarna, S.; Kaprio, J.; Sistonen, P.; Koskenvuo, M. Diagnosis of twin zygosity by mailed questionnaire. Hum. Hered. 1978, 28, 241–254. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, C.B.; Gotzsche, H.; Moller, J.O.; Mortensen, P.B. The Danish Civil Registration System. A cohort of eight million persons. Dan. Med. Bull. 2006, 53, 441–449. [Google Scholar] [PubMed]
- Christiansen, L.; Frederiksen, H.; Schousboe, K.; Skytthe, A.; von Wurmb-Schwark, N.; Christensen, K.; Kyvik, K. Age- and sex-differences in the validity of questionnaire-based zygosity in twins. Twin Res. 2003, 6, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Cederlof, R.; Friberg, L.; Jonsson, E.; Kaij, L. Studies on similarity diagnosis in twins with the aid of mailed questionnaires. Acta Genet. Stat. Med. 1961, 11, 338–362. [Google Scholar] [CrossRef] [PubMed]
- Hauge, M.; Harvald, B.; Fischer, M.; Gotlieb-Jensen, K.; Juel-Nielsen, N.; Raebild, I.; Shapiro, R.; Videbech, T. The Danish Twin Register. In Prospective Longitudinal Research: An Empirical Basis for the Primary Pervention of Psychological Disorders; Mednich, S.A., Ed.; Oxford University Press: Oxford, UK, 1981; pp. 217–221. [Google Scholar]
- Dignam, J.J.; Zhang, Q.; Kocherginsky, M. The use and interpretation of competing risks regression models. Clin. Cancer Res. 2012, 18, 2301–2308. [Google Scholar] [CrossRef] [PubMed]
- Arellano, M. PRACTITIONERS’ CORNER: Computing Robust Standard Errors for Within-groups Estimators. Oxf. Bull. Econ. Stat. 1987, 49, 431–434. [Google Scholar] [CrossRef]
- Coles, S. An Introduction to Statistical Modeling of Extreme Values; Springer: London, UK, 2001. [Google Scholar]
- Medford, A. Best-practice life expectancy: An extreme value approach. Demogr. Res. 2017, 36, 989–1014. [Google Scholar] [CrossRef]
- Gilleland, E.; Katz, R.W. extRemes 2.0: An Extreme Value Analysis Package in R. J. Stat. Soft. 2016, 72, 1–39. [Google Scholar] [CrossRef]
- Christensen, K.; McGue, M. Commentary: Twins, worms and life course epidemiology. Int. J. Epidemiol. 2012, 41, 1010–1011. [Google Scholar] [CrossRef] [PubMed]
- Petersen, I.; Nielsen, M.M.; Beck-Nielsen, H.; Christensen, K. No evidence of a higher 10 year period prevalence of diabetes among 77,885 twins compared with 215,264 singletons from the Danish birth cohorts 1910–1989. Diabetologia 2011, 54, 2016–2024. [Google Scholar] [CrossRef] [PubMed]
- Christensen, K.; Petersen, I.; Skytthe, A.; Herskind, A.M.; McGue, M.; Bingley, P. Comparison of academic performance of twins and singletons in adolescence: Follow-up study. BMJ 2006, 333, 1095. [Google Scholar] [CrossRef] [PubMed]
- Oberg, S.; Cnattingius, S.; Sandin, S.; Lichtenstein, P.; Morley, R.; Iliadou, A.N. Twinship influence on morbidity and mortality across the lifespan. Int. J. Epidemiol. 2012, 41, 1002–1009. [Google Scholar] [CrossRef] [PubMed]
- Ahrenfeldt, L.J.; Skytthe, A.; Moller, S.; Czene, K.; Adami, H.O.; Mucci, L.A.; Kaprio, J.; Petersen, I.; Christensen, K.; Lindahl-Jacobsen, R. Risk of Sex-Specific Cancers in Opposite-Sex and Same-Sex Twins in Denmark and Sweden. Cancer Epidemiol. Biomarkers Prev. 2015, 24, 1622–1628. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All cohorts 1870–1990 | Cohort 1 1870–1900 | Cohort 2 1901–1930 | Cohort 3 1931–1960 | Cohort 4 1961–1990 | |
|---|---|---|---|---|---|
| Total, n (pairs) | 96,338 (49,390) | 9037 (4907) | 15,645 (8060) | 37,330 (19,114) | 34,326 (17,309) |
| Age at FU a, mean (SD) | 58.5 (18.3) | 69.0 (19.8) | 74.0 (16.8) | 65.3 (11.2) | 41.2 (9.2) |
| Sex, n (%) | |||||
| Male | 49,100 (51.0) | 4496 (49.8) | 7480 (47.8) | 20,133 (53.9) | 16,991 (49.5) |
| Female | 47,238 (49.0) | 4541 (50.3) | 8165 (52.2) | 17,197 (46.1) | 17,335 (50.5) |
| Zygosity, n (%) | |||||
| MZ | 23,888 (24.8) | 2247 (24.9) | 4613 (29.5) | 7122 (19.1) | 9906 (28.9) |
| SSDZ | 39,728 (41.2) | 4029 (44.6) | 9156 (58.5) | 14,440 (38.9) | 12,103 (35.3) |
| OSDZ | 32,722 (34.0) | 2761 (30.6) | 1876 (12.0) | 15,768 (42.2) | 12,317 (35.9) |
| Dead during FU a, n (%) | |||||
| No/censored | 62,459 (64.8) | 208 (2.3) | 959 (6.1) | 27,806 (74.5) | 33,486 (97.6) |
| Yes | 33,879 (35.2) | 8829 (97.7) | 14,686 (93.9) | 9524 (25.5) | 840 (2.4) |
| All Ages, n = 96,338 a | Ages ≤50, n = 96,338 a | Ages 51–75, n = 65,107 a | Ages >75, n = 20,839 a | |
|---|---|---|---|---|
| Both sexes | HR (95%-CI) | HR (95%-CI) | HR (95%-CI) | HR (95%-CI) |
| Zygosity, n (%) | ||||
| MZ | Ref. | Ref. | Ref. | Ref. |
| SSDZ | 1.09 (1.06, 1.12) *** | 1.19 (1.11, 1.29) *** | 1.11 (1.06, 1.17) *** | 1.04 (1.00, 1.09) * |
| OSDZ | 1.17 (1.13, 1.21) *** | 1.53 (1.41, 1.66) *** | 1.12 (1.06, 1.18) *** | 1.09 (1.04, 1.15) *** |
| Males | ||||
| Zygosity, n (%) | ||||
| MZ | Ref. | Ref. | Ref. | Ref. |
| SSDZ | 1.11 (1.07, 1.16) *** | 1.23 (1.11, 1.36) *** | 1.11 (1.04, 1.18) *** | 1.07 (1.00, 1.13) * |
| OSDZ | 1.16 (1.11, 1.21) *** | 1.44 (1.30, 1.60) *** | 1.10 (1.03, 1.18) ** | 1.11 (1.03, 1.19) ** |
| Females | ||||
| Zygosity, n (%) | ||||
| MZ | Ref. | Ref. | Ref. | Ref. |
| SSDZ | 1.07 (1.03, 1.12) ** | 1.20 (1.11, 1.30) *** | 1.12 (1.07, 1.17) *** | 1.04 (1.00, 1.08) |
| OSDZ | 1.18 (1.13, 1.24) *** | 1.52 (1.40, 1.64) *** | 1.11 (1.06, 1.17) *** | 1.09 (1.04, 1.15) *** |
| All Subjects 1961–1990 | Males 1961–1990 | Females 1961–1990 | |
|---|---|---|---|
| Total, n (pairs) | 39,504 (20,232) | 19,964 (13,266) | 19,540 (13,000) |
| Age at FU a, mean (SD) | 40.3 (9.6) | 40.2 (9.5) | 40.5 (9.6) |
| Sex, n (%) | |||
| Male | 19,964 (50.5) | 19,964 (100.0) | - |
| Female | 19,540 (49.5) | - | 19,540 (100.0) |
| Zygosity, n (%) | |||
| MZ | 9906 (25.1) | 4689 (23.5) | 5217 (26.7) |
| SSDZ | 12,103 (30.6) | 6159 (30.9) | 5944 (30.4) |
| OSDZ | 12,317 (31.2) | 6143 (30.8) | 6174 (31.6) |
| UZ | 5178 (13.1) | 2973 (14.9) | 2205 (11.3) |
| Dead during FU a, n (%) | |||
| No | 38,519 (97.5) | 19,334 (96.8) | 19,185 (98.2) |
| Yes | 985 (2.5) | 630 (3.2) | 355 (1.8) |
| All Ages, n = 39,504 | Ages ≤50, n = 39,504 | Ages >50, n = 8711 | |
|---|---|---|---|
| Both sexes a | HR (95%-CI) | HR (95%-CI) | HR (95%-CI) |
| Zygosity | |||
| MZ | Ref. | Ref. | Ref. |
| SSDZ | 1.07 (0.89, 1.13) | 1.10 (0.91, 1.34) | 0.80 (0.46, 1.40) |
| OSDZ | 1.21 (1.01, 1.45) * | 1.23 (1.02, 1.48) * | 1.05 (0.61, 1.79) |
| UZ | 1.83 (1.47, 2.28) *** | 1.89 (1.51, 2.37) *** | 1.25 (0.49, 3.20) |
| Males | |||
| Zygosity | |||
| MZ | Ref. | Ref. | Ref. |
| SSDZ | 1.01 (0.80, 1.28) | 1.06 (0.83, 1.35) | 0.63 (0.29, 1.37) |
| OSDZ | 1.22 (0.97, 1.53) | 1.23 (0.97, 1.55) | 1.14 (0.56, 2.29) |
| UZ | 1.86 (1.43, 2.42) *** | 1.92 (1.46, 2.51) *** | 1.26 (0.39, 4.11) |
| Females | |||
| Zygosity | |||
| MZ | Ref. | Ref. | Ref. |
| SSDZ | 1.17 (0.88, 1.56) | 1.19 (0.88, 1.62) | 1.04 (0.46, 2.31) |
| OSDZ | 1.19 (0.90, 1.58) | 1.23 (0.91, 1.67) | 1.14 (0.56, 2.28) |
| UZ | 1.71 (1.13, 2.60) * | 1.78 (1.15, 2.75) ** | 1.18 (0.26, 5.45) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hjelmborg, J.; Larsen, P.; Kaprio, J.; McGue, M.; Scheike, T.; Hougaard, P.; Christensen, K. Lifespans of Twins: Does Zygosity Matter? Genes 2019, 10, 166. https://doi.org/10.3390/genes10020166
Hjelmborg J, Larsen P, Kaprio J, McGue M, Scheike T, Hougaard P, Christensen K. Lifespans of Twins: Does Zygosity Matter? Genes. 2019; 10(2):166. https://doi.org/10.3390/genes10020166
Chicago/Turabian StyleHjelmborg, Jacob, Pia Larsen, Jaakko Kaprio, Matt McGue, Thomas Scheike, Philip Hougaard, and Kaare Christensen. 2019. "Lifespans of Twins: Does Zygosity Matter?" Genes 10, no. 2: 166. https://doi.org/10.3390/genes10020166