Towards a Comprehensive Understanding of UA-ADRCs (Uncultured, Autologous, Fresh, Unmodified, Adipose Derived Regenerative Cells, Isolated at Point of Care) in Regenerative Medicine

 , and
, and
Abstract
:1. Introduction: What Are UA-ADRCs and How Are They Used in Regenerative Medicine?
2. Why and How Regenerative Cells Should Be Isolated from Adipose Tissue Rather Than from Other Tissues, and How These Cells Are Characterized
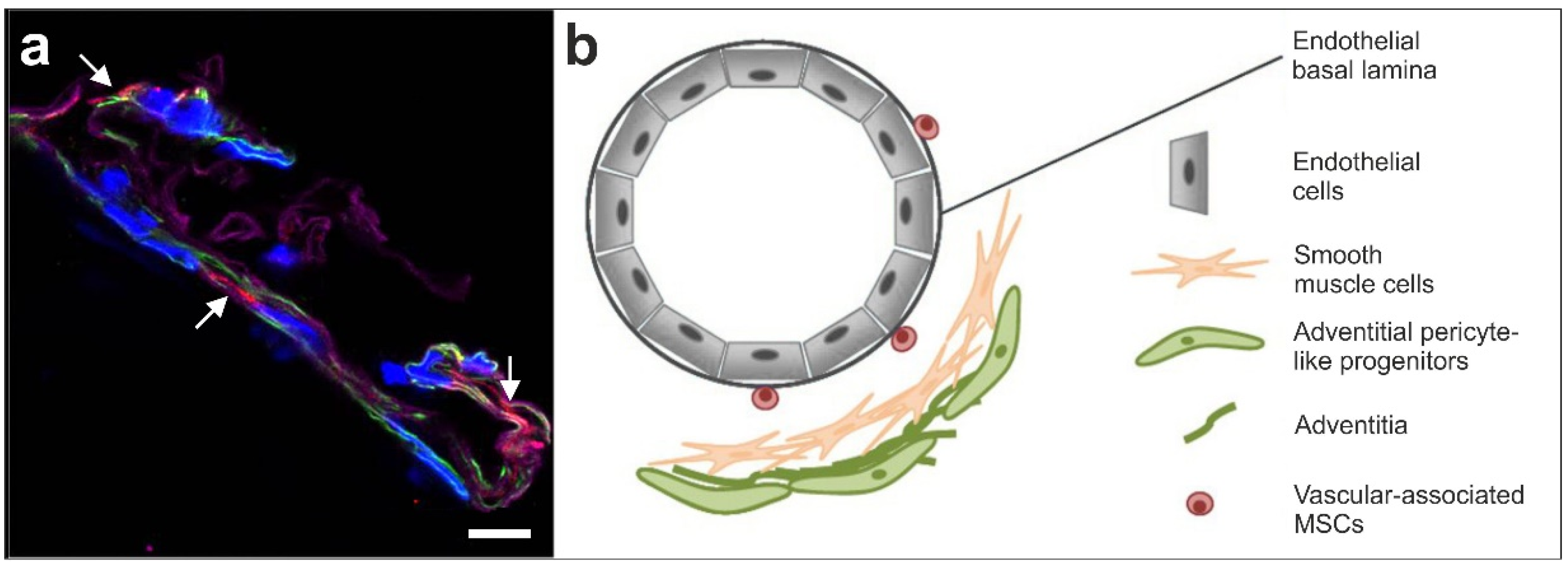
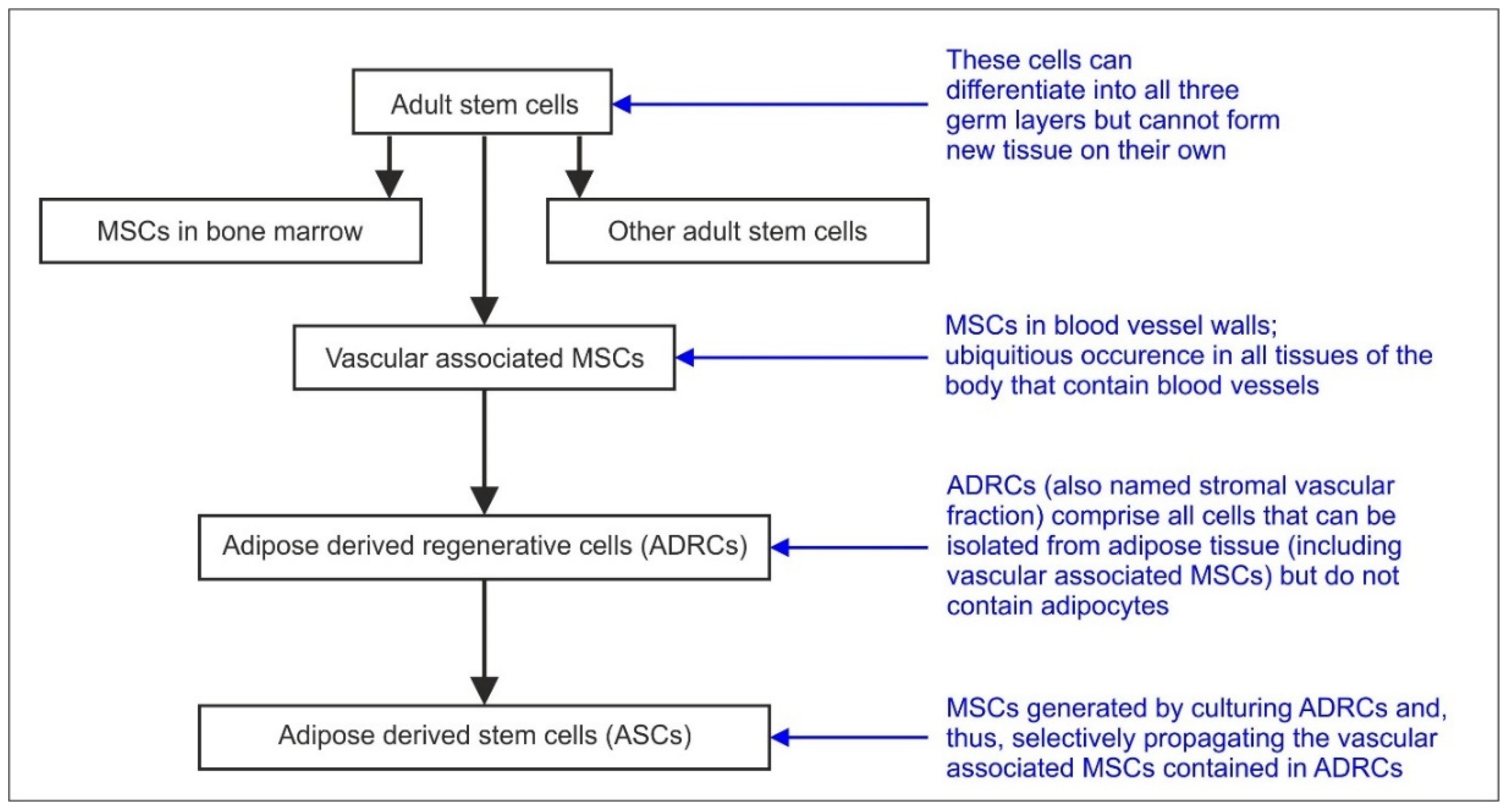
2.1. Statement #1: ADRCs Are Neither ‘Fat Stem Cells’ nor Could They Exclusively be Isolated from Adipose Tissue, as ADRCs Contain the Same Adult Stem Cells That are Ubiquitously Present in the Walls of Small Blood Vessels
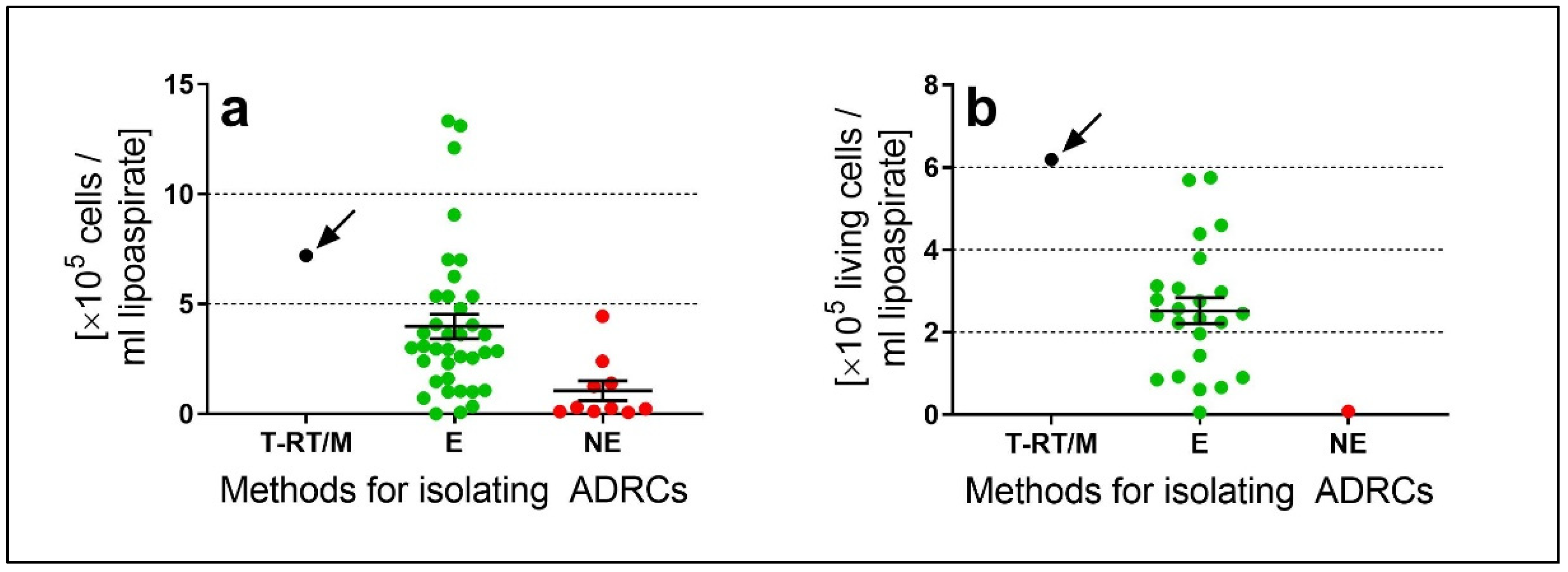
2.2. Statement #2: The Specific Isolation Procedure Used has a Significant Impact on Number and Viability of the Cells Recovered and Hence on Safety and Efficacy of UA-ADRCs
2.3. Statement #3: There is no Need to Further Separate Adipose-Derived Stem Cells (ASCs) from ADRCs if the Latter Were Adequately Isolated from Adipose Tissue
2.4. Statement #4: The Minimal Definitions of Stem Cells Established by the International Federation for Adipose Therapeutics and Science (IFATS) and the International Society for Cellular Therapy (ISCT) are Somewhat Inadequate and Misleading and Should be Amended
3. The Rationale and Advantages of Using Uncultured Autologous Adipose Derived Regenerative Cells (UA-ADRCs) in Regenerative Medicine
3.1. Statement #5: Published Peer Reviewed Clinical Research Demonstrates Tissue Regeneration with UA-ADRCs to be Safe and Effective
4. How UA-ADRCs Exert Their Functions in Tissue Regeneration
4.1. Statement #6: UA-ADRCs Have the Intrinsic Capacity to Adequately Regenerate Tissue without Need for More than Minimal Manipulation, Stimulation and/or (Genetic) Reprogramming of the Cells
4.2. Statement #7: Tissue Regeneration with UA-ADRCs Fulfills the Criteria of Homologous Use
4.3. Statement #8: A Certain Challenge in Research with UA-ADRCs Lays in the Fact that Labeling the Cells Would Render Them Modified, and Unmodified Cells Can Only be Indirectly Identified after Transplantation in a Target Tissue
5. Summary
Author Contributions
Funding
Conflicts of Interest
References
- Davidoff, M.S. The pluripotent microvascular pericytes are the adult stem cells even in the testis. Adv. Exp. Med. Biol. 2019, 1122, 235–267. [Google Scholar] [PubMed]
- Stem Cell Key Terms. Available online: https://www.cirm.ca.gov/patients/stem-cell-key-terms (accessed on 16 April 2020).
- Alt, E.U.; Schmitz, C.; Bai, X. Fundamentals of stem cells: Why and how patients’ own adult stem cells are the next generation of medicine. In Bioethics and Research on Adult Stem Cells; Trafny, T., Spiri, S., Eds.; IF Press Pontifical Council for Culture: Rome, Italy, 2020; in press. [Google Scholar]
- Winnier, G.E.; Valenzuela, N.; Peters-Hall, J.; Kellner, J.; Alt, C.; Alt, E.U. Isolation of adipose tissue derived regenerative cells from human subcutaneous tissue with or without the use of an enzymatic reagent. PLoS ONE 2019, 14, e0221457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crisan, M.; Yap, S.; Casteilla, L.; Chen, C.W.; Corselli, M.; Park, T.S.; Andriolo, G.; Sun, B.; Zheng, B.; Zhang, L.; et al. A perivascular origin for mesenchymal stem cells in multiple human organs. Cell Stem Cell 2008, 3, 301–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Słynarski, K.; Baszczeski, F.; Lipinski, L. Treatment of osteoarthritis—Adipose derived stem cell & PRP therapy. Sportärztezeitung 2017, 3, 14–19. [Google Scholar]
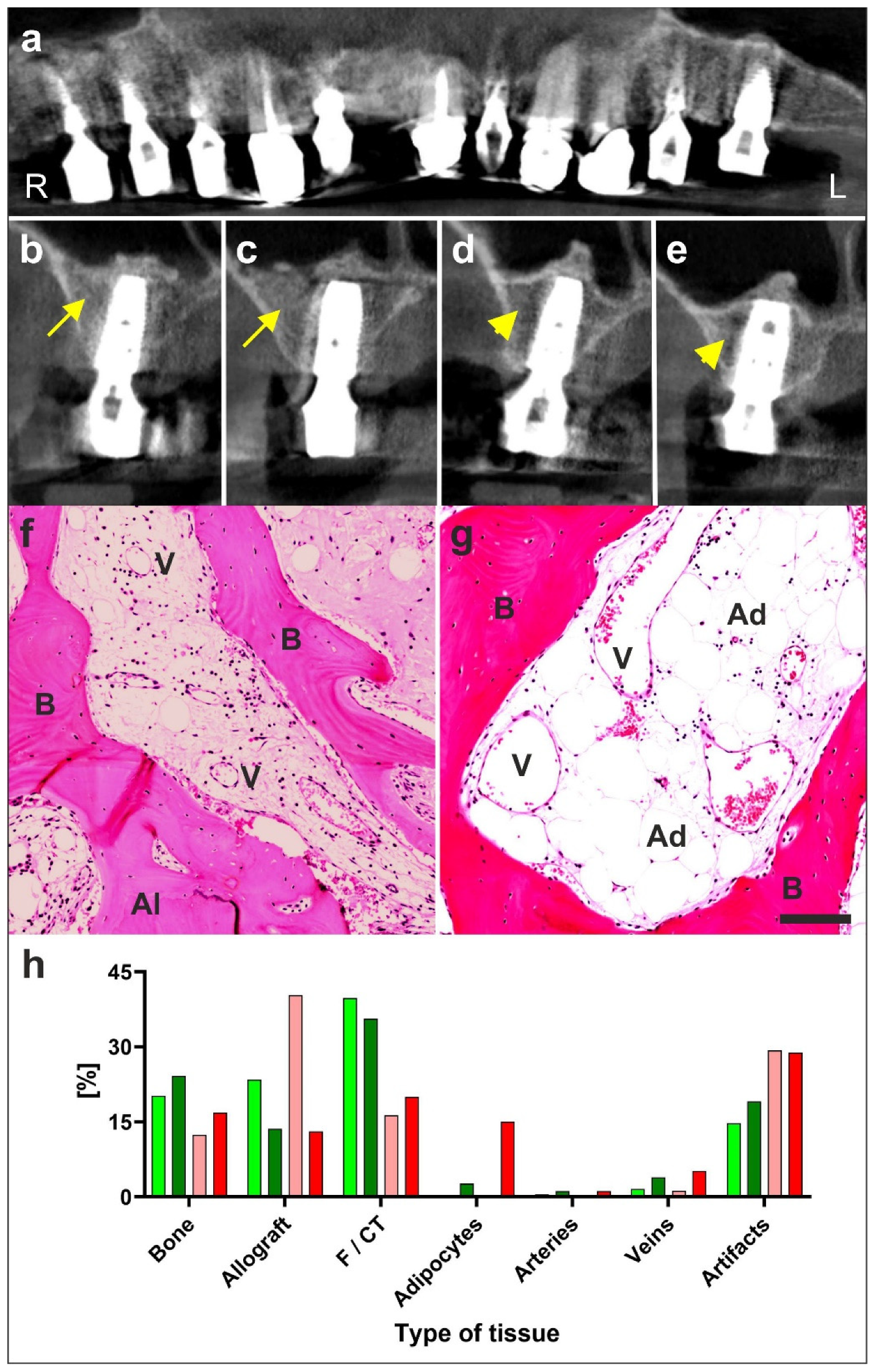
- Solakoglu, Ö.; Götz, W.; Kiessling, M.C.; Alt, C.; Schmitz, C.; Alt, E.U. Improved guided bone regeneration by combined application of unmodified, fresh autologous adipose derived regenerative cells and plasma rich in growth factors: A first-in-human case report and literature review. World J. Stem Cells 2019, 11, 124–146. [Google Scholar] [CrossRef]
- Haenel, A.; Ghosn, M.; Karimi, T.; Vykoukal, J.; Shah, D.; Valderrabano, M.; Schulz, D.G.; Raizner, A.; Schmitz, C.; Alt, E.U. Unmodified autologous stem cells at point of care for chronic myocardial infarction. World J. Stem Cells 2019, 11, 831–858. [Google Scholar] [CrossRef]
- Hurd, J.L.; Facile, T.R.; Weiss, J.; Hayes, M.; Hayes, M.; Furia, J.P.; Maffulli, N.; Winnier, G.E.; Alt, C.; Schmitz, C.; et al. Safety and efficacy of treating symptomatic, partial-thickness rotator cuff tear with fresh, uncultured, unmodified, autologous adipose derived regenerative cells (UA-ADRCs) isolated at the point of care: A prospective, randomized, controlled first-in-human pilot study. J. Orthop. Surg. Res. 2020, 15, 122. [Google Scholar]
- Tsekes, D.; Konstantopoulos, G.; Khan, W.S.; Rossouw, D.; Elvey, M.; Singh, J. Use of stem cells and growth factors in rotator cuff tendon repair. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 747–757. [Google Scholar] [CrossRef]
- Cohen, S.R.; Tiryaki, T.; Womack, H.A.; Canikyan, S.; Schlaudraff, K.U.; Scheflan, M. Cellular optimization of nanofat: Comparison of two nanofat processing devices in terms of cell count and viability. Aesth. S. J. Open Forum 2019, 1, ojz028. [Google Scholar] [CrossRef] [Green Version]
- Van Dongen, J.A.; Stevens, H.P.; Parvizi, M.; van der Lei, B.; Harmsen, M.C. The fractionation of adipose tissue procedure to obtain stromal vascular fractions for regenerative purposes. Wound Repair Regen. 2016, 24, 994–1003. [Google Scholar] [CrossRef] [Green Version]
- Cossu, G.; Birchall, M.; Brown, T.; De Coppi, P.; Culme-Seymour, E.; Gibbon, S.; Hitchcock, J.; Mason, C.; Montgomery, J.; Morris, S.; et al. Lancet Commission: Stem cells and regenerative medicine. Lancet 2018, 391, 883–910. [Google Scholar] [CrossRef] [Green Version]
- Ong, W.K.; Sugii, S. Adipose-derived stem cells: Fatty potentials for therapy. Int. J. Biochem. Cell Biol. 2013, 45, 1083–1086. [Google Scholar] [CrossRef] [PubMed]
- Bateman, M.E.; Strong, A.L.; Gimble, J.M.; Bunnell, B.A. Concise review: Using fat to fight disease: A systematic review of nonhomologous adipose-derived stromal/stem cell therapies. Stem Cells 2018, 36, 1311–1328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, D.T.; Nguyen Thi Phuong, T.; Tien, N.L.B.; Tran, D.K.; Minh, L.B.; Thanh, V.V.; Gia Anh, P.; Pham, V.H.; Thi Nga, V. Adipose tissue stem cells for therapy: An update on the progress of isolation, culture, storage, and clinical application. J. Clin. Med. 2019, 8, 917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, J.C.; Katz, A.J. Stem cells derived from fat. In Principles of Regenerative Medicine, 3rd ed.; Atala, A., Lanza, R., Mikos, A.G., Nerem, R., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 295–305. [Google Scholar]
- Gerecht-Nir, S.; Osenberg, S.; Nevo, O.; Ziskind, A.; Coleman, R.; Itskovitz-Eldor, J. Vascular development in early human embryos and in teratomas derived from human embryonic stem cells. Biol. Reprod. 2004, 71, 2029–2036. [Google Scholar] [CrossRef]
- Fraser, J.K.; Wulur, I.; Alfonso, Z.; Hedrick, M.H. Fat tissue: An underappreciated source of stem cells for biotechnology. Trends Biotechnol. 2006, 24, 150–154. [Google Scholar] [CrossRef]
- Yu, H.; Lu, K.; Zhu, J.; Wang, J. Stem cell therapy for ischemic heart diseases. Br. Med. Bull. 2017, 121, 135–154. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Liu, T.; Song, K.; Fan, X.; Ma, X.; Cui, Z. Adipose-derived stem cell: A better stem cell than BMSC. Cell. Biochem. Funct. 2008, 26, 664–675. [Google Scholar] [CrossRef]
- The American Society for Aesthetic Plastic Surgery’s Cosmetic Surgery National Data Bank. Statistics 2018. Aesthet. Surg. J. 2019, 39 (Suppl. 4), 1–27. [Google Scholar] [CrossRef]
- Housman, T.S.; Lawrence, N.; Mellen, B.G.; George, M.N.; Filippo, J.S.; Cerveny, K.A.; DeMarco, M.; Feldman, S.R.; Fleischer, A.B. The safety of liposuction: Results of a national survey. Dermatol. Surg. 2002, 28, 971–978. [Google Scholar] [CrossRef]
- Kaoutzanis, C.; Gupta, V.; Winocour, J.; Layliev, J.; Ramirez, R.; Grotting, J.C.; Higdon, K. Cosmetic liposuction: Preoperative risk factors, major complication rates, and safety of combined procedures. Aesthet. Surg. J. 2017, 37, 680–694. [Google Scholar] [CrossRef] [PubMed]
- Crisan, M.; Corselli, M.; Chen, W.C.; Péault, B. Perivascular cells for regenerative medicine. J. Cell. Mol. Med. 2012, 16, 2851–2860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sá da Bandeira, D.; Casamitjana, J.; Crisan, M. Pericytes, integral components of adult hematopoietic stem cell niches. Pharmacol. Ther. 2017, 171, 104–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binamé, F. Transduction of extracellular cues into cell polarity: The role of the transmembrane proteoglycan NG2. Mol. Neurobiol. 2014, 50, 482–493. [Google Scholar] [CrossRef]
- Viganò, F.; Dimou, L. The heterogeneous nature of NG2-glia. Brain Res. 2016, 1638, 129–137. [Google Scholar] [CrossRef] [Green Version]
- Richardson, W.D.; Young, K.M.; Tripathi, R.B.; McKenzie, I. NG2-glia as multipotent neural stem cells: Fact or fantasy? Neuron 2011, 70, 661–673. [Google Scholar] [CrossRef] [Green Version]
- Sims, D.E. The pericyte—A review. Tissue Cell. 1986, 18, 153–174. [Google Scholar] [CrossRef]
- Díaz-Flores, L.; Gutiérrez, R.; Varela, H.; Rancel, N.; Valladares, F. Microvascular pericytes: A review of their morphological and functional characteristics. Histol. Histopathol. 1991, 6, 269–286. [Google Scholar]
- Guillemin, G.J.; Brew, B.J. Microglia, macrophages, perivascular macrophages, and pericytes: A review of function and identification. J. Leukoc. Biol. 2004, 75, 388–397. [Google Scholar] [CrossRef]
- Fernández-Klett, F.; Priller, J. Diverse functions of pericytes in cerebral blood flow regulation and ischemia. J. Cereb. Blood Flow Metab. 2015, 35, 883–887. [Google Scholar] [CrossRef] [Green Version]
- Avolio, E.; Madeddu, P. Discovering cardiac pericyte biology: From physiopathological mechanisms to potential therapeutic applications in ischemic heart disease. Vascul. Pharmacol. 2016, 86, 53–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilmer, M.; Vykoukal, J.; Recio Boiles, A.; Coleman, M.; Alt, E. Two sides of the same coin: Stem cells in cancer and regenerative medicine. FASEB J. 2014, 28, 2748–2761. [Google Scholar] [CrossRef] [PubMed]
- Aronowitz, J.A.; Lockhart, R.A.; Hakakian, C.S. Mechanical versus enzymatic isolation of stromal vascular fraction cells from adipose tissue. Springerplus 2015, 4, 713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oberbauer, E.; Steffenhagen, C.; Wurzer, C.; Gabriel, C.; Redl, H.; Wolbank, S. Enzymatic and non-enzymatic isolation systems for adipose tissue-derived cells: Current state of the art. Cell Regen. 2015, 4, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Condé-Green, A.; Kotamarti, V.S.; Sherman, L.S.; Keith, J.D.; Lee, E.S.; Granick, M.S.; Rameshwar, P. Shift toward mechanical isolation of adipose-derived stromal vascular fraction: Review of upcoming techniques. Plast. Reconstr. Surg. Glob. Open 2016, 4, e1017. [Google Scholar] [CrossRef]
- Van Dongen, J.A.; Tuin, A.J.; Spiekman, M.; Jansma, J.; van der Lei, B.; Harmsen, M.C. Comparison of intraoperative procedures for isolation of clinical grade stromal vascular fraction for regenerative purposes: A systematic review. J. Tissue Eng. Regen. Med. 2018, 12, e261–e274. [Google Scholar] [CrossRef] [Green Version]
- Snyder, A.G.; Hubbard, N.W.; Messmer, M.N.; Kofman, S.B.; Hagan, C.E.; Orozco, S.L.; Chiang, K.; Daniels, B.P.; Baker, D.; Oberst, A. Intratumoral activation of the necroptotic pathway components RIPK1 and RIPK3 potentiates antitumor immunity. Sci. Immunol. 2019, 4, pii:eaaw2004. [Google Scholar] [CrossRef]
- Badimon, L.; Oñate, B.; Vilahur, G. Adipose-derived mesenchymal stem cells and their reparative potential in ischemic heart disease. Rev. Esp. Cardiol. (Engl. Ed.) 2015, 68, 599–611. [Google Scholar] [CrossRef]
- Mitchell, J.B.; McIntosh, K.; Zvonic, S.; Garrett, S.; Floyd, Z.E.; Kloster, A.; Di Halvorsen, Y.; Storms, R.W.; Goh, B.; Kilroy, G.; et al. Immunophenotype of human adipose-derived cells: Temporal changes in stromal-associated and stem cell-associated markers. Stem Cells 2006, 24, 376–385. [Google Scholar] [CrossRef]
- Electronic Code of Federal Regulations. Part 1271—Human Cells, Tissues, and Cellular and Tissue-Based Products. Available online: https://www.ecfr.gov/cgi-bin/text-idx?SID=a76b9e404fcea7463c6a0b7228b9afbc&mc=true&node=pt21.8.1271&rgn=div5#_top (accessed on 8 April 2020).
- Code of Federal Regulations—Title 21—Food and Drugs. Available online: https://www.fda.gov/medical-devices/medical-device-databases/code-federal-regulations-title-21-food-and-drugs (accessed on 8 April 2020).
- Regulatory Considerations for Human Cells, Tissues, and Cellular and Tissue-Based Products: Minimal Manipulation and Homologous Use—Guidance for Industry and Food and Drug Administration Staff. Available online: https://www.fda.gov/media/124138/download (accessed on 8 April 2020).
- Advanced Therapy Medicinal Products. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/advanced-therapy-medicinal-products-overview (accessed on 8 April 2020).
- Sheu, J.J.; Lee, M.S.; Wallace, C.G.; Chen, K.H.; Sung, P.H.; Chua, S.; Lee, F.Y.; Chung, S.Y.; Chen, Y.L.; Li, Y.C.; et al. Therapeutic effects of adipose derived fresh stromal vascular fraction-containing stem cells versus cultured adipose derived mesenchymal stem cells on rescuing heart function in rat after acute myocardial infarction. Am. J. Transl. Res. 2019, 11, 67–86. [Google Scholar]
- Polly, S.S.; Nichols, A.E.C.; Donnini, E. Adipose-derived stromal vascular fraction and cultured stromal cells as trophic mediators for tendon healing. J. Orthop. Res. 2019, 37, 1429–1439. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, E.; Farris, A.; O’Sullivan, A.; Rodriguez, R.; Grayson, W.L. Comparison of SVF and passaged ASCs as point-of-care agents for bone regeneration. Tissue Eng. Part A. 2019, 25, 1459–1469. [Google Scholar] [CrossRef] [PubMed]
- You, D.; Jang, M.J.; Kim, B.H.; Song, G.; Lee, C.; Suh, N.; Jeong, I.G.; Ahn, T.Y.; Kim, C.S. Comparative study of autologous stromal vascular fraction and adipose-derived stem cells for erectile function recovery in a rat model of cavernous nerve injury. Stem Cells Transl. Med. 2015, 4, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Bora, P.; Majumdar, A.S. Adipose tissue-derived stromal vascular fraction in regenerative medicine: A brief review on biology and translation. Stem Cell Res. Ther. 2017, 8, 145. [Google Scholar] [CrossRef] [PubMed]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315.e7. [Google Scholar] [CrossRef] [PubMed]
- Alt, E.; Yan, Y.; Gehmert, S.; Song, Y.H.; Altman, A.; Gehmert, S.; Vykoukal, D.; Bai, X. Fibroblasts share mesenchymal phenotypes with stem cells, but lack their differentiation and colony-forming potential. Biol. Cell. 2011, 103, 197–208. [Google Scholar] [CrossRef]
- Bourin, P.; Bunnell, B.A.; Casteilla, L.; Dominici, M.; Katz, A.J.; March, K.L.; Redl, H.; Rubin, J.P.; Yoshimura, K.; Gimble, J.M. Stromal cells from the adipose tissue-derived stromal vascular fraction and culture expanded adipose tissue-derived stromal/stem cells: A joint statement of the International Federation for Adipose Therapeutics and Science (IFATS) and the International Society for Cellular Therapy (ISCT). Cytotherapy 2013, 5, 641–648. [Google Scholar]
- Nürnberger, S.; Lindner, C.; Maier, J.; Strohmeier, K.; Wurzer, C.; Slezak, P.; Suessner, S.; Holnthoner, W.; Redl, H.; Wolbank, S.; et al. Adipose-tissue-derived therapeutic cells in their natural environment as an autologous cell therapy strategy: The microtissue-stromal vascular fraction. Eur. Cell. Mater. 2019, 37, 113–133. [Google Scholar] [CrossRef]
- Fraser, J.K.; Hicok, K.C.; Shanahan, R.; Zhu, M.; Miller, S.; Arm, D.M. The Celution® system: Automated processing of adipose-derived regenerative cells in a functionally closed system. Adv. Wound Care 2014, 3, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Shah, F.S.; Wu, X.; Dietrich, M.; Rood, J.; Gimble, J.M. A non-enzymatic method for isolating human adipose tissue-derived stromal stem cells. Cytotherapy 2013, 15, 979–985. [Google Scholar] [CrossRef]
- Aronowitz, J.A.; Ellenhorn, J.D. Adipose stromal vascular fraction isolation: A head-to-head comparison of four commercial cell separation systems. Plast. Reconstr. Surg. 2013, 132, 932e–939e. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.; Matsubara, Y.; Masuda, Y.; Togashi, K.; Ohno, T.; Tamura, T.; Toyoshima, Y.; Sugimachi, K.; Toyoda, M.; Marc, H.; et al. Characterization of adipose tissue-derived cells isolated with the Celution system. Cytotherapy 2008, 10, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Domenis, R.; Lazzaro, L.; Calabrese, S.; Mangoni, D.; Gallelli, A.; Bourkoula, E.; Manini, I.; Bergamin, N.; Toffoletto, B.; Beltrami, C.A.; et al. Adipose tissue derived stem cells: In vitro and in vivo analysis of a standard and three commercially available cell-assisted lipotransfer techniques. Stem Cell Res. Ther. 2015, 6, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marks, P.W.; Witten, C.M.; Califf, R.M. Clarifying stem-cell therapy’s benefits and risks. N. Engl. J. Med. 2017, 376, 1007–1009. [Google Scholar] [CrossRef] [Green Version]
- Berkowitz, A.L.; Miller, M.B.; Mir, S.A.; Cagney, D.; Chavakula, V.; Guleria, I.; Aizer, A.; Ligon, K.L.; Chi, J.H. Glioproliferative lesion of the spinal cord as a complication of “stem-cell tourism”. N. Engl. J. Med. 2016, 375, 196–198. [Google Scholar] [CrossRef]
- Kuriyan, A.E.; Albini, T.A.; Townsend, J.H.; Rodriguez, M.; Pandya, H.K.; Leonard, R.E., 2nd; Parrott, M.B.; Rosenfeld, P.J.; Flynn, H.W., Jr.; Goldberg, J.L. Vision loss after intravitreal injection of autologous “stem cells” for AMD. N. Engl. J. Med. 2017, 376, 1047–1053. [Google Scholar] [CrossRef] [Green Version]
- El-Jawahri, A.R.; Schaefer, P.W.; El Khoury, J.B.; Martinez-Lage, M. Case 5-2018: A 63-year-old man with confusion after stem-cell transplantation. N. Engl. J. Med. 2018, 378, 659–669. [Google Scholar] [CrossRef]
- Toyserkani, N.M.; Jørgensen, M.G.; Tabatabaeifar, S.; Jensen, C.H.; Sheikh, S.P.; Sørensen, J.A. Concise Review: A Safety Assessment of Adipose-Derived Cell Therapy in Clinical Trials: A Systematic Review of Reported Adverse Events. Stem Cells Transl. Med. 2017, 6, 1786–1794. [Google Scholar] [CrossRef] [Green Version]
- Hurd, J. Autologous Adult Adipose-Derived Regenerative Cell Injection into Chronic Partial-Thickness Rotator Cuff Tears. ClinicalTrials.gov Identifier: NCT03752827. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03752827 (accessed on 10 February 2020).
- Andia, I.; Maffulli, N.; Burgos-Alonso, N. Stromal vascular fraction technologies and clinical applications. Expert Opin. Biol. Ther. 2019, 19, 1289–1305. [Google Scholar] [CrossRef]
- Hong, Z.; Chen, J.; Zhang, S.; Zhao, C.; Bi, M.; Chen, X.; Bi, Q. Intra-articular injection of autologous adipose-derived stromal vascular fractions for knee osteoarthritis: A double-blind randomized self-controlled trial. Int. Orthop. 2019, 43, 1123–1134. [Google Scholar] [CrossRef]
- Albano, D.; Messina, C.; Usuelli, F.G.; De Girolamo, L.; Grassi, M.; Maccario, C.; Bignotti, B.; Tagliafico, A.; Sconfienza, L.M. Magnetic resonance and ultrasound in achilles tendinopathy: Predictive role and response assessment to platelet-rich plasma and adipose-derived stromal vascular fraction injection. Eur. J. Radiol. 2017, 95, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Zollino, I.; Campioni, D.; Sibilla, M.G.; Tessari, M.; Malagoni, A.M.; Zamboni, P. A phase II randomized clinical trial for the treatment of recalcitrant chronic leg ulcers using centrifuged adipose tissue containing progenitor cells. Cytotherapy 2019, 21, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Houtgraaf, J.H.; den Dekker, W.K.; van Dalen, B.M.; Springeling, T.; de Jong, R.; van Geuns, R.J.; Geleijnse, M.L.; Fernandez-Aviles, F.; Zijlsta, F.; Serruys, P.W.; et al. First experience in humans using adipose tissue-derived regenerative cells in the treatment of patients with ST-segment elevation myocardial infarction. J. Am. Coll. Cardiol. 2012, 59, 539–540. [Google Scholar] [CrossRef] [Green Version]
- Perin, E.C.; Sanz-Ruiz, R.; Sánchez, P.L.; Lasso, J.; Pérez-Cano, R.; Alonso-Farto, J.C.; Pérez-David, E.; Fernández-Santos, M.E.; Serruys, P.W.; Duckers, H.J.; et al. Adipose-derived regenerative cells in patients with ischemic cardiomyopathy: The PRECISE Trial. Am. Heart J. 2014, 168, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Henry, T.D.; Pepine, C.J.; Lambert, C.R.; Traverse, J.H.; Schatz, R.; Costa, M.; Povsic, T.J.; David Anderson, R.; Willerson, J.T.; Kesten, S.; et al. The Athena trials: Autologous adipose-derived regenerative cells for refractory chronic myocardial ischemia with left ventricular dysfunction. Catheter Cardiovasc. Interv. 2017, 89, 169–177. [Google Scholar] [CrossRef]
- Madonna, R.; Van Laake, L.W.; Davidson, S.M.; Engel, F.B.; Hausenloy, D.J.; Lecour, S.; Leor, J.; Perrino, C.; Schulz, R.; Ytrehus, K.; et al. Position Paper of the European Society of Cardiology Working Group Cellular Biology of the Heart: Cell-based therapies for myocardial repair and regeneration in ischemic heart disease and heart failure. Eur. Heart J. 2016, 37, 1789–1798. [Google Scholar] [CrossRef]
- Usuelli, F.G.; Grassi, M.; Maccario, C.; Vigano’, M.; Lanfranchi, L.; Alfieri Montrasio, U.; de Girolamo, L. Intratendinous adipose-derived stromal vascular fraction (SVF) injection provides a safe, efficacious treatment for Achilles tendinopathy: Results of a randomized controlled clinical trial at a 6-month follow-up. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 2000–2010. [Google Scholar] [CrossRef]
- Koh, Y.G.; Kwon, O.R.; Kim, Y.S.; Choi, Y.J. Comparative outcomes of open-wedge high tibial osteotomy with platelet-rich plasma alone or in combination with mesenchymal stem cell treatment: A prospective study. Arthroscopy 2014, 30, 1453–1460. [Google Scholar] [CrossRef]
- Koh, Y.G.; Kwon, O.R.; Kim, Y.S.; Choi, Y.J.; Tak, D.H. Adipose-Derived Mesenchymal Stem Cells with Microfracture Versus Microfracture Alone: 2-Year Follow-up of a Prospective Randomized Trial. Arthroscopy 2016, 32, 97–109. [Google Scholar] [CrossRef]
- Han, S.K.; Kim, H.R.; Kim, W.K. The treatment of diabetic foot ulcers with uncultured, processed lipoaspirate cells: A pilot study. Wound Repair Regen. 2010, 18, 342–348. [Google Scholar] [CrossRef]
- Raposio, E.; Bertozzi, N.; Bonomini, S.; Bernuzzi, G.; Formentini, A.; Grignaffini, E.; Pio Grieco, M. Adipose-derived Stem Cells Added to Platelet-rich Plasma for Chronic Skin Ulcer Therapy. Wounds 2016, 28, 126–131. [Google Scholar] [PubMed]
- Malik, P.; Gaba, S.; Ahuja, C.; Sharma, R.R.; Sharma, R.K.; Khandelwal, N. Role of Fat Graft Alone versus Enriched Fat Graft with Stromal Vascular Filtrate in Painful Amputation Stump. Indian J. Orthop. 2019, 53, 452–458. [Google Scholar] [PubMed]
- Stem Cell Clinics Likely to Flourish Despite Judge’s Rebuke. Available online: https://www.washingtonpost.com/health/stem-cell-clinics-likely-to-flourish-despite-judges-rebuke/2019/06/07/7fc677cc-891f-11e9-98c1-e945ae5db8fb_story.html (accessed on 8 April 2020).
- Murray, I.R.; Chahla, J.; Frank, R.M.; Piuzzi, N.S.; Mandelbaum, B.R.; Dragoo, J.L. Members of the Biologics Association. Rogue stem cell clinics. Bone Joint J. 2020, 102-B, 148–154. [Google Scholar] [CrossRef] [PubMed]
- FDA Warns about Stem Cell Therapies. Available online: https://www.fda.gov/consumers/consumer-updates/fda-warns-about-stem-cell-therapies (accessed on 8 April 2020).
- Angst, F.; Schwyzer, H.K.; Aeschlimann, A.; Simmen, B.R.; Goldhahn, J. Measures of adult shoulder function: Disabilities of the Arm, Shoulder, and Hand Questionnaire (DASH) and its short version (QuickDASH), Shoulder Pain and Disability Index (SPADI), American Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form, Constant (Murley) Score (CS), Simple Shoulder Test (SST), Oxford Shoulder Score (OSS), Shoulder Disability Questionnaire (SDQ), and Western Ontario Shoulder Instability Index (WOSI). Arthritis Care Res. 2011, 63 (Suppl. 11), S174–S188. [Google Scholar]
- Wylie, J.D.; Beckmann, J.T.; Granger, E.; Tashjian, R.Z. Functional outcomes assessment in shoulder surgery. World J. Orthop. 2014, 5, 623–633. [Google Scholar] [CrossRef]
- Konstantinow, A.; Arnold, A.; Djabali, K.; Kempf, W.; Gutermuth, J.; Fischer, T.; Biedermann, T. Therapy of ulcus cruris of venous and mixed venous arterial origin with autologous, adult, native progenitor cells from subcutaneous adipose tissue: A prospective clinical pilot study. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 2104–2118. [Google Scholar] [CrossRef]
- Alt, E.; Milz, S.; Frank, H.G.; Rothoerl, R.; Hoppert, M.; Alt, C.; Winnier, G.; Schmitz, C. Rotator cuff tear treated with adipose derived regenerative cells. 2020; under review. [Google Scholar]
- Oranges, C.M.; Striebel, J.; Tremp, M.; Madduri, S.; Kalbermatten, D.F.; Harder, Y.; Schaefer, D.J. The preparation of the recipient site in fat grafting: A comprehensive review of the preclinical evidence. Plast. Reconstr. Surg. 2019, 143, 1099–1107. [Google Scholar] [CrossRef]
- Guo, J.; Nguyen, A.; Banyard, D.A.; Fadavi, D.; Toranto, J.D.; Wirth, G.A.; Paydar, K.Z.; Evans, G.R.; Widgerow, A.D. Stromal vascular fraction: A regenerative reality? Part 2: Mechanisms of regenerative action. J. Plast. Reconstr. Aesthet. Surg. 2016, 69, 180–188. [Google Scholar] [CrossRef]
- Marlicz, W.; Zuba-Surma, E.; Kucia, M.; Blogowski, W.; Starzynska, T.; Ratajczak, M.Z. Various types of stem cells, including a population of very small embryonic-like stem cells, are mobilized into peripheral blood in patients with Crohn’s disease. Inflamm. Bowel Dis. 2012, 18, 1711–1722. [Google Scholar] [CrossRef]
- Drukała, J.; Paczkowska, E.; Kucia, M.; Młyńska, E.; Krajewski, A.; Machaliński, B.; Madeja, Z.; Ratajczak, M.Z. Stem cells, including a population of very small embryonic-like stem cells, are mobilized into peripheral blood in patients after skin burn injury. Stem Cell Rev. Rep. 2012, 8, 184–194. [Google Scholar] [CrossRef]
- Wojakowski, W.; Tendera, M.; Zebzda, A.; Michalowska, A.; Majka, M.; Kucia, M.; Maslankiewicz, K.; Wyderka, R.; Król, M.; Ochala, A.; et al. Mobilization of CD34(+), CD117(+), CXCR4(+), c-met(+) stem cells is correlated with left ventricular ejection fraction and plasma NT-proBNP levels in patients with acute myocardial infarction. Eur. Heart J. 2006, 27, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Dutta, P.; Courties, G.; Wei, Y.; Leuschner, F.; Gorbatov, R.; Robbins, C.S.; Iwamoto, Y.; Thompson, B.; Carlson, A.L.; Heidt, T.; et al. Myocardial infarction accelerates atherosclerosis. Nature 2012, 487, 325–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loder, S.J.; Agarwal, S.; Chung, M.T.; Cholok, D.; Hwang, C.; Visser, N.; Vasquez, K.; Sorkin, M.; Habbouche, J.; Sung, H.H.; et al. Characterizing the circulating cell populations in traumatic heterotopic ossification. Am. J. Pathol. 2018, 188, 2464–2473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeom, Y.I.; Fuhrmann, G.; Ovitt, C.E.; Brehm, A.; Ohbo, K.; Gross, M.; Hübner, K.; Schöler, H.R. Germline regulatory element of Oct-4 specific for the totipotent cycle of embryonal cells. Development 1996, 122, 881–894. [Google Scholar] [PubMed]
- Chambers, I.; Colby, D.; Robertson, M.; Nichols, J.; Lee, S.; Tweedie, S.; Smith, A. Functional expression cloning of Nanog, a pluripotency sustaining factor in embryonic stem cells. Cell 2003, 113, 643–655. [Google Scholar] [CrossRef] [Green Version]
- Thomson, J.A.; Kalishman, J.; Golos, T.G.; Durning, M.; Harris, C.P.; Becker, R.A.; Hearn, J.P. Isolation of a primate embryonic stem cell line. Proc. Natl. Acad. Sci. USA 1995, 92, 7844–7848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, Y.R.; Kottmann, A.H.; Kuroda, M.; Taniuchi, I.; Littman, D.R. Function of the chemokine receptor CXCR4 in haematopoiesis and in cerebellar development. Nature 1998, 393, 595–599. [Google Scholar] [CrossRef]
- Alvarez-Gonzalez, C.; Duggleby, R.; Vagaska, B.; Querol, S.; Gomez, S.G.; Ferretti, P.; Madrigal, A. Cord blood Lin(-)CD45(-) embryonic-like stem cells are a heterogeneous population that lack self-renewal capacity. PLoS ONE 2013, 8, e67968. [Google Scholar] [CrossRef] [Green Version]
- Kucia, M.; Reca, R.; Campbell, F.R.; Zuba-Surma, E.; Majka, M.; Ratajczak, J.; Ratajczak, M.Z. A population of very small embryonic-like (VSEL) CXCR4(+)SSEA-1(+)Oct-4+ stem cells identified in adult bone marrow. Leukemia 2006, 20, 857–869. [Google Scholar] [CrossRef]
- Zaman, W.S.; Makpol, S.; Santhapan, S.; Chua, K.H. Stemness gene expression profile of human adipose derived stem cells in long-term culture. Med. J. Malaysia 2008, 63 (Suppl. A), 61–62. [Google Scholar]
- Mihaila, S.M.; Frias, A.M.; Pirraco, R.P.; Rada, T.; Reis, R.L.; Gomes, M.E.; Marques, A.P. Human adipose tissue-derived SSEA-4 subpopulation multi-differentiation potential towards the endothelial and osteogenic lineages. Tissue Eng. Part A 2013, 19, 235–246. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Zhang, A.; Tao, C.; Li, X.; Jin, P. The role of SDF-1-CXCR4/CXCR7 axis in biological behaviors of adipose tissue-derived mesenchymal stem cells in vitro. Biochem. Biophys. Res. Commun. 2013, 441, 675–680. [Google Scholar] [CrossRef]
- Naaijkens, B.A.; Krijnen, P.A.; Meinster, E.; Ter Horst, E.N.; Vo, K.; Musters, R.J.; Kamp, O.; Niessen, H.W.; Juffermans, L.J.; van Dijk, A. Acute myocardial infarction does not affect functional characteristics of adipose-derived stem cells in rats, but reduces the number of stem cells in adipose tissue. Cell Tissue Res. 2015, 362, 623–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, X.; Yan, Y.; Coleman, M.; Wu, G.; Rabinovich, B.; Seidensticker, M.; Alt, E. Tracking long-term survival of intramyocardially delivered human adipose tissue-derived stem cells using bioluminescence imaging. Mol. Imaging Biol. 2011, 13, 633–645. [Google Scholar] [CrossRef] [PubMed]
- Sadat, S.; Gehmert, S.; Song, Y.H.; Yen, Y.; Bai, X.; Gaiser, S.; Klein, H.; Alt, E. The cardioprotective effect of mesenchymal stem cells is mediated by IGF-I and VEGF. Biochem. Biophys. Res. Commun. 2007, 363, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Shih, Y.C.; Lee, P.Y.; Cheng, H.; Tsai, C.H.; Ma, H.; Tarng, D.C. Adipose-derived stem cells exhibit antioxidative and antiapoptotic properties to rescue ischemic acute kidney injury in rats. Plast. Reconstr. Surg. 2013, 132, 940e–951e. [Google Scholar] [CrossRef]
- Wang, C.; Song, W.; Chen, B.; Liu, X.; He, Y. Exosomes isolated from adipose-derived stem cells: A new cell-free approach to prevent the muscle degeneration associated with torn rotator cuffs. Am. J. Sports Med. 2019, 47, 3247–3255. [Google Scholar] [CrossRef]
- González, M.A.; Gonzalez-Rey, E.; Rico, L.; Büscher, D.; Delgado, M. Adipose-derived mesenchymal stem cells alleviate experimental colitis by inhibiting inflammatory and autoimmune responses. Gastroenterology 2009, 136, 978–989. [Google Scholar] [CrossRef]
- Leto Barone, A.A.; Khalifian, S.; Lee, W.P.; Brandacher, G. Immunomodulatory effects of adipose-derived stem cells: Fact or fiction? Biomed. Res. Int. 2013, 2013, 383685. [Google Scholar] [CrossRef] [Green Version]
- Haenel, A.; Ghosn, M.; Karimi, T.; Vykoukal, J.; Kettlun, C.; Shah, D.; Dave, A.; Valderrabano, M.; Schulz, D.; Azares, A.; et al. Unmodified, Autologous Adipose-Derived Regenerative Cells Improve Cardiac Function, Structure and Revascularization in a Porcine Model of Chronic Myocardial Infarction. Available online: https://doi.org/10.1101/286468 (accessed on 8 April 2020).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Why and How Regenerative Cells Should be Isolated from Adipose Tissue rather than from Other Tissues, and How these Cells are Characterized | |
|---|---|
| 1. | ADRCs are neither ‘fat stem cells’ nor could they exclusively be isolated from adipose tissue, as ADRCs contain the same adult stem cells that are ubiquitously present in the walls of small blood vessels that are capable of differentiating into somatic cells of the three germ layers. |
| 2. | The specific isolation procedure used has a significant impact on the number and viability of the cells and hence on safety and efficacy of UA-ADRCs. |
| 3. | There is no need to further separate adipose-derived stem cells (ASCs) from ADRCs if the latter were adequately isolated from adipose tissue. |
| 4. | The minimal definitions of stem cells established by the International Federation for Adipose Therapeutics and Science (IFATS) and the International Society for Cellular Therapy (ISCT) are somewhat inadequate and misleading and should be amended. |
| The Rationale and Advantages of Using UA-ADRCs in Regenerative Medicine | |
| 5. | Published peer reviewed clinical research demonstrates tissue regeneration with UA-ADRCs to be safe and effective. |
| How UA-ADRCs Exert Their Function in Tissue Regeneration | |
| 6. | UA-ADRCs have the intrinsic capacity to adequately regenerate tissue without need for more than minimal manipulation, stimulation and/or (genetic) reprogramming of the cells. |
| 7. | Tissue regeneration with UA-ADRCs fulfills the criteria of homologous use. |
| 8. | A certain challenge in research with UA-ADRCS lays in the fact that labeling the cells would render them modified, and unmodified cells can only be indirectly identified after transplantation in a target tissue. |
| Study | Usuelli et al. (2018) [75] | Koh et al. (2014) [76] | Koh et al. (2016) [77] | Han et al. (2010) [78] | Raposio et al. (2016) [79] | Malik et al. (2019) [80] |
|---|---|---|---|---|---|---|
| Indication | Achilles tendinopathy | Knee OA | Knee OA | Skin ulcers | Skin ulcers | Painful amputation stump |
| N (Tr) | 21 | 26 | 30 | 28 | 16 | 5 |
| Tr | UA-ADRCs | HTO + UA-ADRCs + PRP | MF + UA-ADRCs | UA-ADRCs + Fibrin | UA-ADRCs + PRP | UA-ADRCs + Fat |
| I-PoC | Yes | No (1 day before) | No (1 day before) | Yes | Yes | Yes |
| N (C) | 23 | 26 | 27 | 26 | 24 | 5 |
| C | PRP | HTO + PRP | MF | Fibrin | PRP | Fat |
| E/NE | NE | E | E | E | E | E |
| Follow-up | M6 | M24 | M26-M30 | W8 | M18 | M6 |
| Tr > C | No | Yes | Yes* | Yes | No** | No |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alt, E.U.; Winnier, G.; Haenel, A.; Rothoerl, R.; Solakoglu, O.; Alt, C.; Schmitz, C. Towards a Comprehensive Understanding of UA-ADRCs (Uncultured, Autologous, Fresh, Unmodified, Adipose Derived Regenerative Cells, Isolated at Point of Care) in Regenerative Medicine. Cells 2020, 9, 1097. https://doi.org/10.3390/cells9051097
Alt EU, Winnier G, Haenel A, Rothoerl R, Solakoglu O, Alt C, Schmitz C. Towards a Comprehensive Understanding of UA-ADRCs (Uncultured, Autologous, Fresh, Unmodified, Adipose Derived Regenerative Cells, Isolated at Point of Care) in Regenerative Medicine. Cells. 2020; 9(5):1097. https://doi.org/10.3390/cells9051097
Chicago/Turabian StyleAlt, Eckhard U., Glenn Winnier, Alexander Haenel, Ralf Rothoerl, Oender Solakoglu, Christopher Alt, and Christoph Schmitz. 2020. "Towards a Comprehensive Understanding of UA-ADRCs (Uncultured, Autologous, Fresh, Unmodified, Adipose Derived Regenerative Cells, Isolated at Point of Care) in Regenerative Medicine" Cells 9, no. 5: 1097. https://doi.org/10.3390/cells9051097