
Ratio of Urinary Proteins to Albumin Excretion Shifts Substantially during Progression of the Podocytopathy Alport Syndrome, and Spot Urine Is a Reliable Method to Detect These Pathologic Changes

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Data and Sampling of Urine
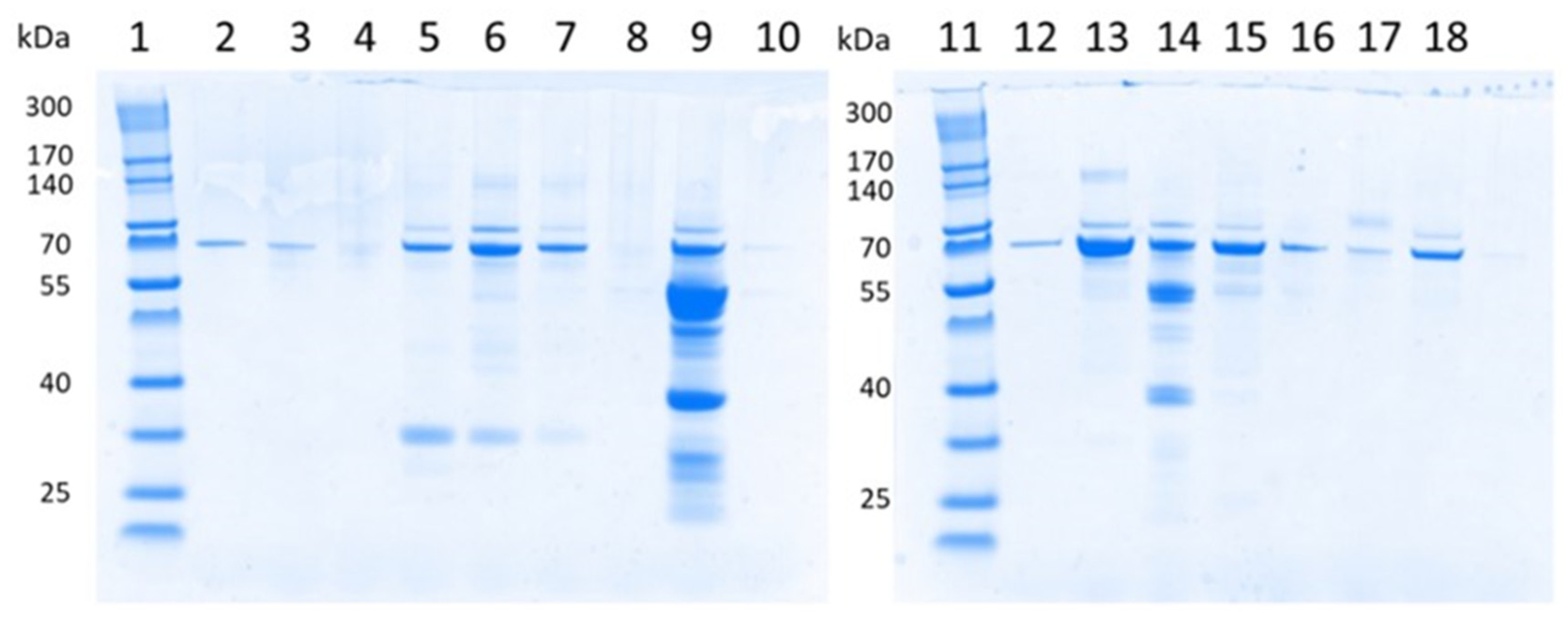
2.2. Sodium Dodecyl Sulfate Polyacrylamide Gel Electrophoresis (SDS-PAGE) of Urinary Proteins
2.3. Statistical Methods
3. Results
3.1. Baseline Characteristics
3.2. Albuminuria, Proteinuria and Albuminuria-to-Proteinuria Ratios in All Participants
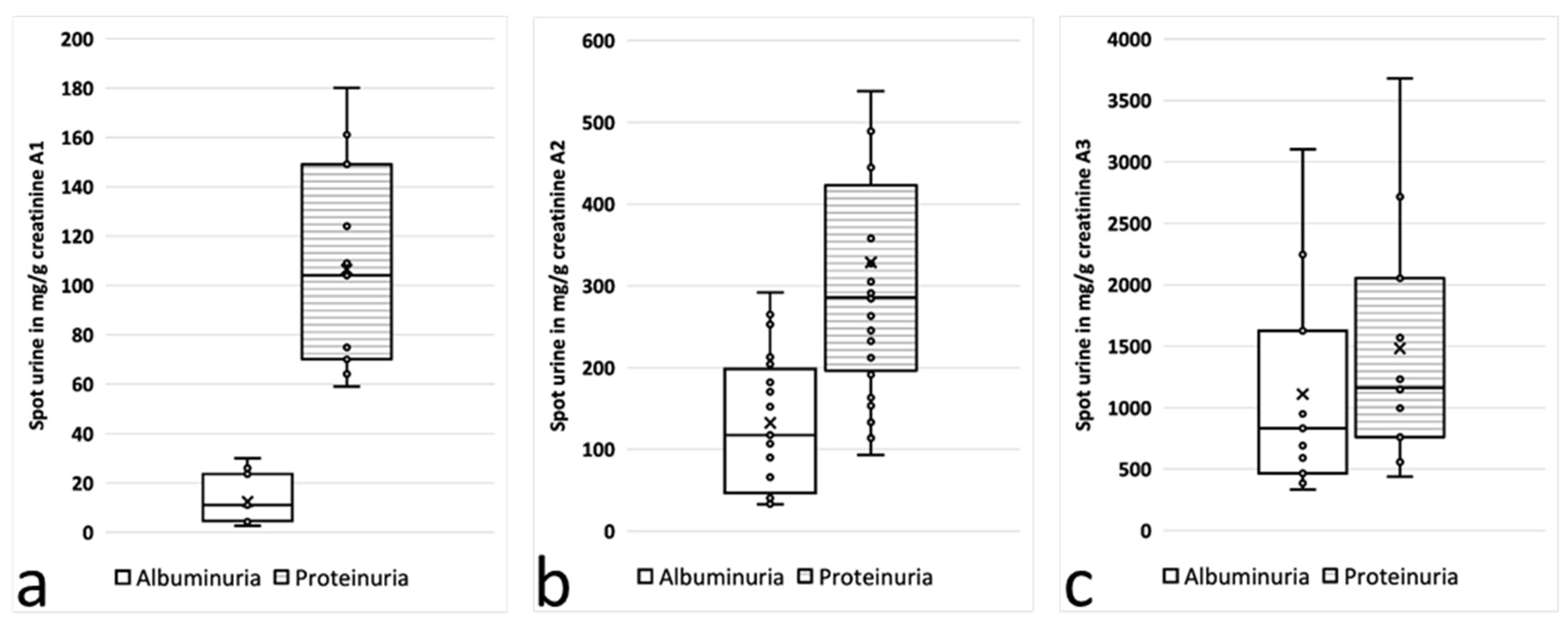
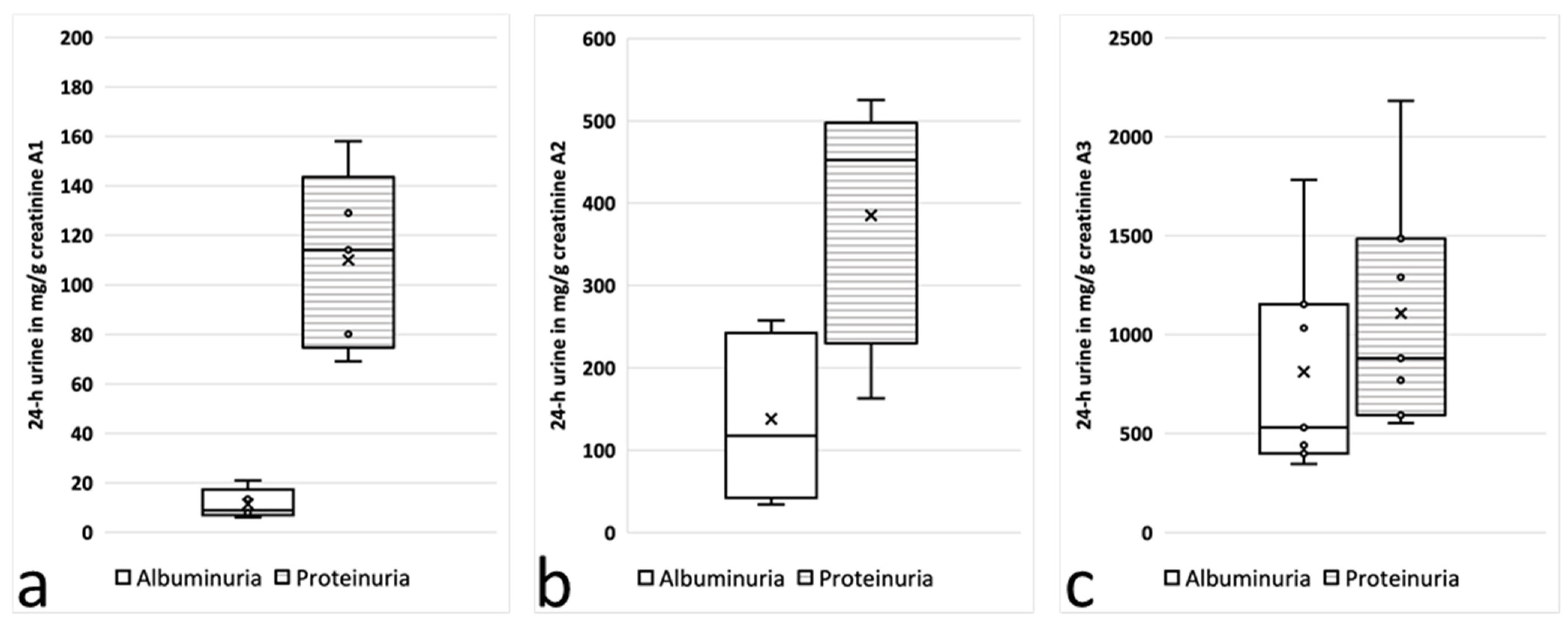
3.3. Albuminuria, Proteinuria and Albuminuria-to-Proteinuria Ratios in Alport Stage 0, 1 and 2 Subgroups
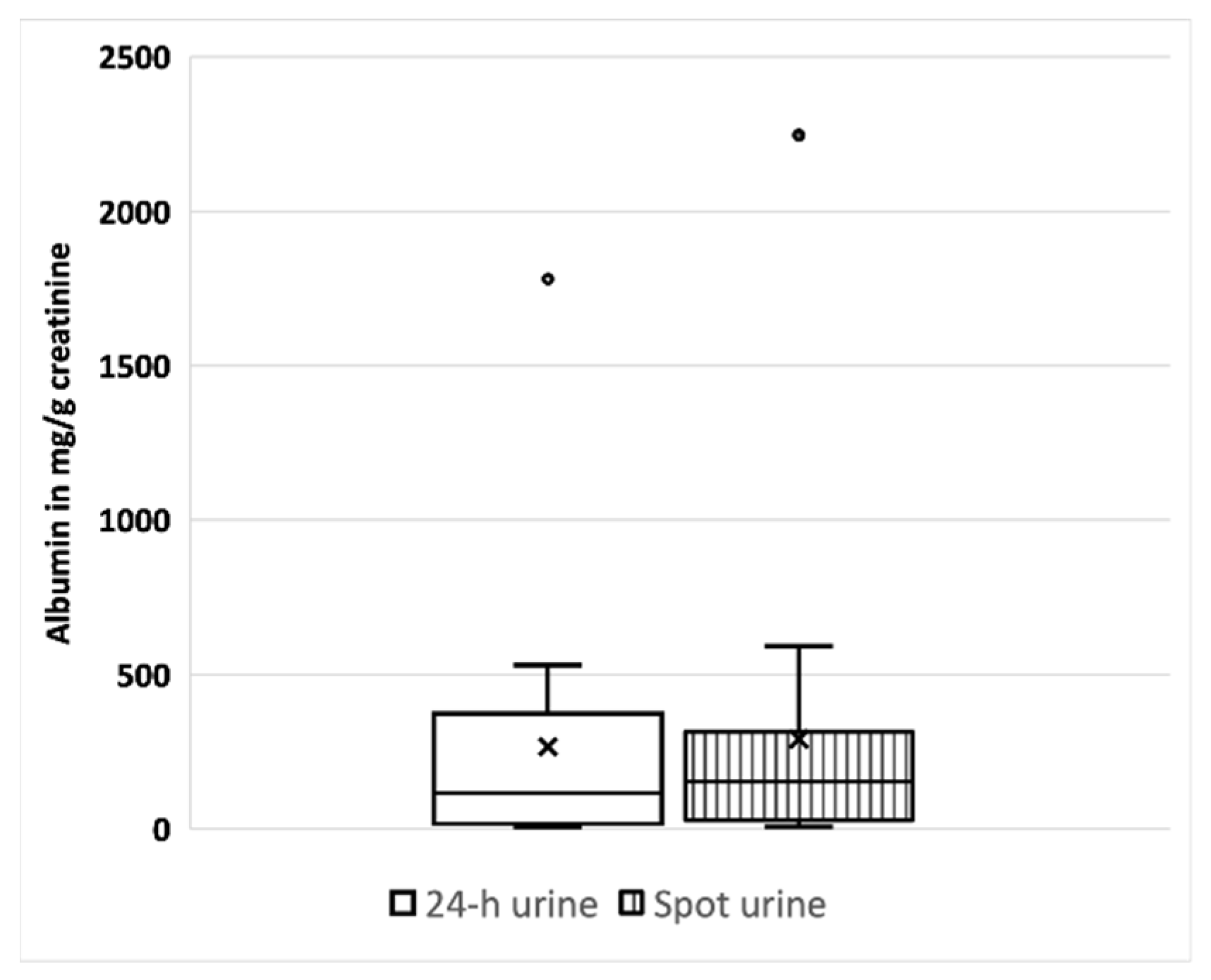
3.4. Comparison of Albuminuria, Proteinuria and Albuminuria-to-Proteinuria Ratios in 24 h Urine vs. Spot Urine
4. Discussion
5. Conclusions
- (1)
- Both the UACR and the UPCR are relevant diagnostic biomarkers in patients with AS. As UPCRs and UACRs differed significantly in patients with AS and with yet low amounts of albuminuria, our study findings advocate for simultaneous measurements of the UPCR and the UACR in daily practice in early stages of AS. Use of the UPCR seems to be a key parameter at very early stages of glomerular diseases such as AS, noticeably earlier than the UACR. In general, the UACR and the UPCR are both recommended in daily clinical practice. At the very beginning of Alport syndrome, however, the UPCR (and the UACR-to-UPCR ratio) might be a very significant parameter to indicate how kidney function has changed over time.
- (2)
- At early stages of CKD with a normal GFR and a low amount of albuminuria, spot urine can be used as a reliable and convenient alternative to 24 h urine to monitor disease progression with the UACR and UPCR. The differences in proteinuria and albuminuria between spot urine and 24 h urine in our study were minimal. This finding has an important impact on future clinical trials in patients in early stages of CKD.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tryggvason, K.; Pettersson, E. Causes and consequences of proteinuria: The kidney filtration barrier and progressive renal failure. J. Intern. Med. 2003, 254, 216–224. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef] [PubMed]
- Song, F.; Loke, Y.K.; Walsh, T.; Glenny, A.M.; Eastwood, A.J.; Altman, D.G. Methodological problems in the use of indirect comparisons for evaluating healthcare interventions: Survey of published systematic reviews. BMJ 2009, 338, b1147. [Google Scholar] [CrossRef]
- Hertz, J.M.; Thomassen, M.; Storey, H.; Flinter, F. Clinical utility gene card for: Alport syndrome—Update 2014. Eur. J. Hum. Genet. 2015, 23, 1269. [Google Scholar] [CrossRef]
- Kruegel, J.; Rubel, D.; Gross, O. Alport syndrome—Insights from basic and clinical research. Nat. Rev. Nephrol. 2013, 9, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Hudson, B.G.; Tryggvason, K.; Sundaramoorthy, M.; Neilson, E.G. Alport’s Syndrome, Goodpasture’s Syndrome, and Type IV Collagen. N. Engl. J. Med. 2003, 348, 2543–2556. [Google Scholar] [CrossRef]
- Kashtan, C.E.; Ding, J.; Garosi, G.; Heidet, L.; Massella, L.; Nakanishi, K.; Nozu, K.; Renieri, A.; Rheault, M.; Wang, F.; et al. Alport syndrome: A unified classification of genetic disorders of collagen IV α345: A position paper of the Alport Syndrome Classification Working Group. Kidney Int. 2018, 93, 1045–1051. [Google Scholar] [CrossRef]
- Savige, J.; Huang, M.; Croos Dabrera, M.S.; Shukla, K.; Gibson, J. Genotype-Phenotype Correlations for Pathogenic COL4A3–COL4A5 Variants in X-Linked, Autosomal Recessive, and Autosomal Dominant Alport Syndrome. Front. Med. 2022, 9, 865034. [Google Scholar] [CrossRef]
- Gross, O.; Beirowski, B.; Koepke, M.L.; Kuck, J.; Reiner, M.; Addicks, K.; Smyth, N.; Schulze-Lohoff, E.; Weber, M. Preemptive ramipril therapy delays renal failure and reduces renal fibrosis in COL4A3-knockout mice with Alport syndrome1. Kidney Int. 2003, 63, 438–446. [Google Scholar] [CrossRef]
- Gross, O.; Licht, C.; Anders, H.J.; Hoppe, B.; Beck, B.; Tönshoff, B.; Höcker, B.; Wygoda, S.; Ehrich, J.H.; Pape, L.; et al. Early angiotensin-converting enzyme inhibition in Alport syndrome delays renal failure and improves life expectancy. Kidney Int. 2012, 81, 494–501. [Google Scholar] [CrossRef]
- Gross, O.; Tönshoff, B.; Weber, L.T.; Pape, L.; Latta, K.; Fehrenbach, H.; Lange-Sperandio, B.; Zappel, H.; Hoyer, P.; Staude, H.; et al. A multicenter, randomized, placebo-controlled, double-blind phase 3 trial with open-arm comparison indicates safety and efficacy of nephroprotective therapy with ramipril in children with Alport’s syndrome. Kidney Int. 2020, 97, 1275–1286. [Google Scholar] [CrossRef]
- Boeckhaus, J.; Hoefele, J.; Riedhammer, K.M.; Tönshoff, B.; Ehren, R.; Pape, L.; Latta, K.; Fehrenbach, H.; Lange-Sperandio, B.; Kettwig, M.; et al. Precise variant interpretation, phenotype ascertainment, and genotype–phenotype correlation of children in the EARLY PRO-TECT Alport trial. Clin. Genet. 2021, 99, 143–156. [Google Scholar] [CrossRef]
- Boeckhaus, J.; Strenzke, N.; Storz, C.; Gross, O. Characterization of Sensorineural Hearing Loss in Children with Alport Syndrome. Life 2020, 10, 360. [Google Scholar] [CrossRef]
- Laemmli, U.K. Cleavage of Structural Proteins during the Assembly of the Head of Bacteriophage T4. Nature 1970, 227, 680–685. [Google Scholar] [CrossRef]
- Wessel, D.; Flügge, U.I. A method for the quantitative recovery of protein in dilute solution in the presence of detergents and lipids. Anal. Biochem. 1984, 138, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Atkins, R.C.; Briganti, E.M.; Zimmet, P.Z.; Chadban, S.J. Association between albuminuria and proteinuria in the general population: The AusDiab Study. Nephrol. Dial. Transplant. 2003, 18, 2170–2174. [Google Scholar] [CrossRef] [PubMed]
- Collier, G.; Greenan, M.C.; Brady, J.J.; Murray, B.; Cunningham, S.K. A study of the relationship between albuminuria, proteinuria and urinary reagent strips. Ann. Clin. Biochem. 2009, 46, 247–249. [Google Scholar] [CrossRef]
- Weaver, R.G.; James, M.T.; Ravani, P.; Weaver, C.G.W.; Lamb, E.J.; Tonelli, M.; Manns, B.J.; Quinn, R.R.; Jun, M.; Hemmelgarn, B.R. Estimating Urine Albumin-to-Creatinine Ratio from Protein-to-Creatinine Ratio: Development of Equations using Same-Day Measurements. J. Am. Soc. Nephrol. 2020, 31, 591–601. [Google Scholar] [CrossRef]
- Boeckhaus, J.; Hoefele, J.; Riedhammer, K.M.; Nagel, M.; Beck, B.B.; Choi, M.; Gollasch, M.; Bergmann, C.; Sonntag, J.E.; Troesch, V.; et al. Lifelong Effect of Therapy in Young Patients with the COL4A5 Alport Missense Variant p.(Gly624Asp): A Prospective Cohort Study. Nephrol. Dial. Transplant. 2022, 37, 2496–2504. [Google Scholar] [CrossRef] [PubMed]
- Tojo, A.; Endou, H. Intrarenal handling of proteins in rats using fractional micropuncture technique. Am. J. Physiol. Ren. Physiol. 1992, 263, F601–F606. [Google Scholar] [CrossRef]
- Gburek, J.; Konopska, B.; Gołąb, K. Renal Handling of Albumin—From Early Findings to Current Concepts. Int. J. Mol. Sci. 2021, 22, 5809. [Google Scholar] [CrossRef] [PubMed]
- Kashtan, C.E.; Gross, O. Clinical practice recommendations for the diagnosis and management of Alport syndrome in children, adolescents, and young adults–an update for 2020. Pediatr. Nephrol. 2021, 36, 711–719. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, N.J.; Taal, M.W. How to measure proteinuria? Curr. Opin. Nephrol. Hypertens. 2008, 17, 600–603. [Google Scholar] [CrossRef] [PubMed]
- Gaspari, F.; Perico, N.; Remuzzi, G. Timed Urine Collections Are Not Needed to Measure Urine Protein Excretion in Clinical Practice. Am. J. Kidney Dis. 2006, 47, 1–7. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subgroup: Albuminuria (mg/gCrea) | Albuminuria in mg/gCrea (SD) | Proteinuria in mg/gCrea (SD) | Albuminuria/Proteinuria (%) | Age in Years (SD) | ACEi Therapy | n | p |
|---|---|---|---|---|---|---|---|
| 24 h Urine | |||||||
| <30 (Alport stage 0) | 11.4 (±6.0) | 110 (±36.3) | 10.4 | 12.2 (±3.6) | 4/5 (80%) | 5 | <0.05 |
| 30–300 (Alport stage 1) | 138 (±94.7) | 385 (±140.8) | 35.8 | 9.6 (±4.9) | 9/9 (100%) | 9 | <0.05 |
| >300 (Alport stage 2) | 812.4 (±533.3) | 1106.6 (±586.8) | 73.4 | 13.7 (±4.7) | 7/7 (100%) | 7 | 0.35 |
| Spontaneous (Spot) Urine | |||||||
| <30 (Alport stage 0) | 12.5 (±9.7) | 106.4 (±42.2) | 11.7 | 9.8 (±3.7) | 9/11 (82%) | 11 | <0.05 |
| 30–300 (Alport stage 1) | 132.3 (±80.5) | 328.5 (±210.1) | 40.3 | 10.2 (±4.9) | 20/24 (83%) | 24 | <0.05 |
| >300 (Alport stage 2) | 1109.7 (±873.6) | 1481.9 (±983.4) | 74.9 | 11.7 (±4.6) | 11/11 (100%) | 11 | 0.36 |
| Albuminuria 24 h Urine | Albuminuria Spot Urine | Proteinuria 24 h Urine | Proteinuria Spot Urine | Age (Years) at Collection |
|---|---|---|---|---|
| 266.8 (±426.4) | 291.2 (±530.2) | 471.5 (±504.9) | 480.2 (±632.1) | 11.4 (±4.4) |
| 120.4 (±153.4) | 116 (±120.3) | 279.6 (±187.1) | 253.8 (±152.9) | 11.5 (±4.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boeckhaus, J.; Mohr, L.; Dihazi, H.; Tönshoff, B.; Weber, L.T.; Pape, L.; Latta, K.; Fehrenbach, H.; Lange-Sperandio, B.; Kettwig, M.; et al. Ratio of Urinary Proteins to Albumin Excretion Shifts Substantially during Progression of the Podocytopathy Alport Syndrome, and Spot Urine Is a Reliable Method to Detect These Pathologic Changes. Cells 2023, 12, 1333. https://doi.org/10.3390/cells12091333
Boeckhaus J, Mohr L, Dihazi H, Tönshoff B, Weber LT, Pape L, Latta K, Fehrenbach H, Lange-Sperandio B, Kettwig M, et al. Ratio of Urinary Proteins to Albumin Excretion Shifts Substantially during Progression of the Podocytopathy Alport Syndrome, and Spot Urine Is a Reliable Method to Detect These Pathologic Changes. Cells. 2023; 12(9):1333. https://doi.org/10.3390/cells12091333
Chicago/Turabian StyleBoeckhaus, Jan, Lea Mohr, Hassan Dihazi, Burkhard Tönshoff, Lutz T. Weber, Lars Pape, Kay Latta, Henry Fehrenbach, Baerbel Lange-Sperandio, Matthias Kettwig, and et al. 2023. "Ratio of Urinary Proteins to Albumin Excretion Shifts Substantially during Progression of the Podocytopathy Alport Syndrome, and Spot Urine Is a Reliable Method to Detect These Pathologic Changes" Cells 12, no. 9: 1333. https://doi.org/10.3390/cells12091333