
Rethinking Oncologic Treatment Strategies with Interleukin-2

Abstract
:1. Introduction
2. Interleukin-2 (IL-2)
3. Targeting IL-2 as Cancer Immunotherapy
4. Limitations of IL-2 Immunotherapy
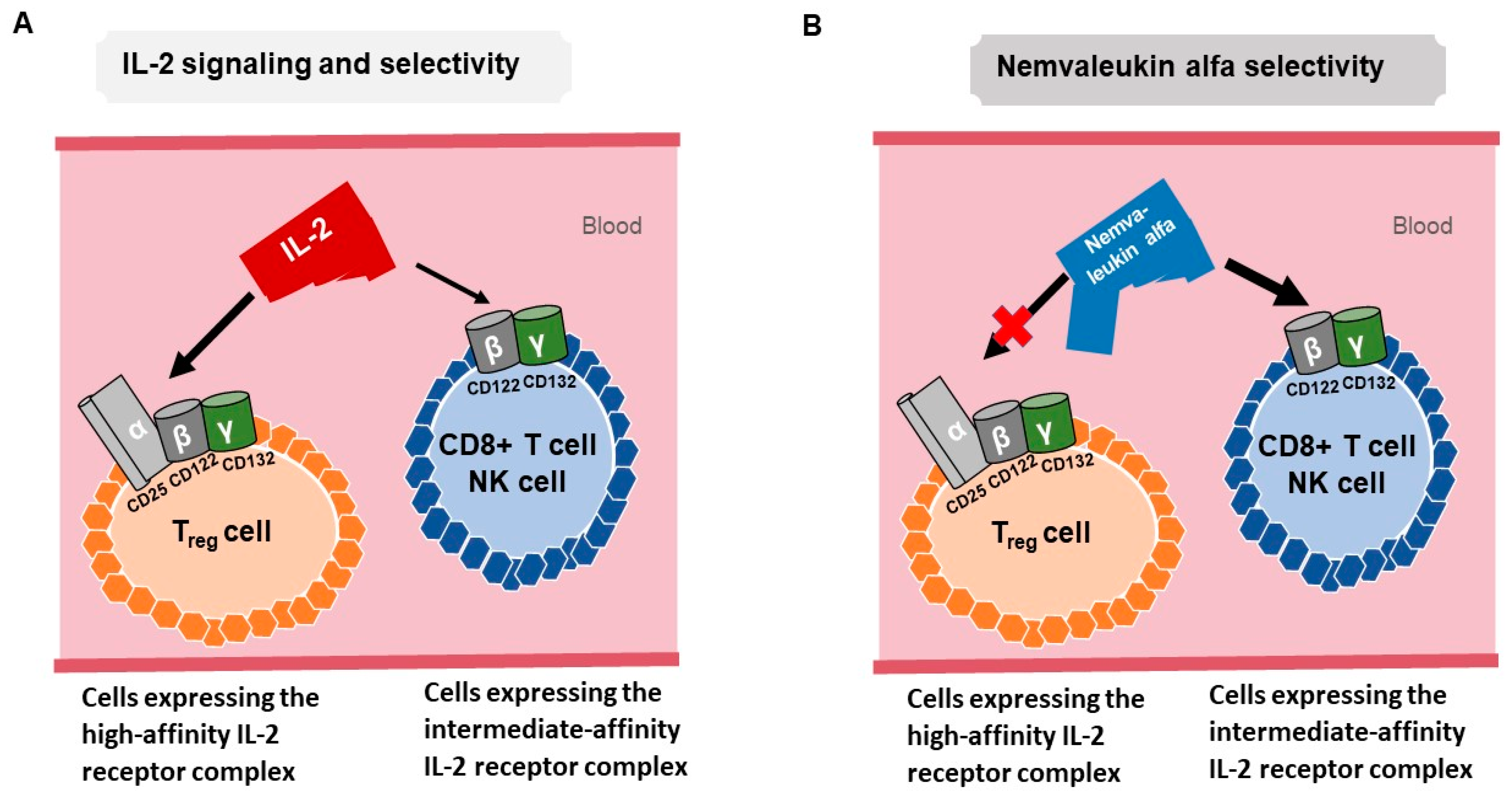
5. Nemvaleukin Alfa
6. Nemvaleukin Alfa Clinical Data
7. Bempegaldesleukin
8. THOR-707 (SAR444245)
9. TransCon IL-2 β/γ
10. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gatla, H.R.; Muniraj, N.; Thevkar, P.; Yavvari, S.; Sukhavasi, S.; Makena, M.R. Regulation of Chemokines and Cytokines by Histone Deacetylases and an Update on Histone Decetylase Inhibitors in Human Diseases. Int. J. Mol. Sci. 2019, 20, 1110. [Google Scholar] [CrossRef]
- Cytokines in the balance. Nat. Immunol. 2019, 20, 1557. [CrossRef] [PubMed]
- Dinarello, C.A. Historical insights into cytokines. Eur. J. Immunol. 2007, 37, S34–S45. [Google Scholar] [CrossRef] [PubMed]
- Morris, R.; Kershaw, N.J.; Babon, J.J. The molecular details of cytokine signaling via the JAK/STAT pathway. Protein Sci. 2018, 27, 1984–2009. [Google Scholar] [CrossRef] [PubMed]
- Briukhovetska, D.; Dörr, J.; Endres, S.; Libby, P.; Dinarello, C.A.; Kobold, S. Interleukins in cancer: From biology to therapy. Nat. Rev. Cancer 2021, 21, 481–499. [Google Scholar] [CrossRef] [PubMed]
- Del Valle, D.M.; Kim-Schulze, S.; Huang, H.H.; Beckmann, N.D.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T.H.; Madduri, D.; Stock, A.; et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat. Med. 2020, 26, 1636–1643. [Google Scholar] [CrossRef] [PubMed]
- Monastero, R.N.; Pentyala, S. Cytokines as biomarkers and their respective clinical cutoff levels. Int. J. Inflamm. 2017, 2017, 4309485. [Google Scholar] [CrossRef] [PubMed]
- Vaillant, A.A.J.; Qurie, A. Interleukin. In StatPearls; StatPearls Publishing: St. Petersburg, FL, USA, 2021. [Google Scholar]
- Morgan, D.A.; Ruscetti, F.W.; Gallo, R. Selective in vitro growth of T lymphocytes from normal human bone marrows. Science 1976, 193, 1007–1008. [Google Scholar] [CrossRef]
- Kalia, V.; Sarkar, S. Regulation of effector and memory CD8 T cell differentiation by IL-2—A balancing act. Front. Immunol. 2018, 9, 2987. [Google Scholar] [CrossRef]
- Liao, W.; Lin, J.-X.; Leonard, W.J. Interleukin-2 at the crossroads of effector responses, tolerance, and immunotherapy. Immunity 2013, 38, 13–25. [Google Scholar] [CrossRef]
- Ross, S.H.; Cantrell, D.A. Signaling and function of interleukin-2 in T lymphocytes. Annu. Rev. Immunol. 2018, 36, 411. [Google Scholar] [CrossRef]
- Setrerrahmane, S.; Xu, H. Tumor-related interleukins: Old validated targets for new anti-cancer drug development. Mol. Cancer 2017, 16, 153. [Google Scholar] [CrossRef]
- Rosenberg, S.A.; Lotze, M.T.; Muul, L.M.; Leitman, S.; Chang, A.E.; Ettinghausen, S.E.; Matory, Y.L.; Skibber, J.M.; Shiloni, E.; Vetto, J.T. Observations on the systemic administration of autologous lymphokine-activated killer cells and recombinant interleukin-2 to patients with metastatic cancer. N. Engl. J. Med. 1985, 313, 1485–1492. [Google Scholar] [CrossRef]
- Rosenberg, S.A. Immersion in the search for effective cancer immunotherapies. Mol. Med. 2021, 27, 63. [Google Scholar] [CrossRef]
- Rosenberg, S.A. IL-2: The first effective immunotherapy for human cancer. J. Immunol. 2014, 192, 5451–5458. [Google Scholar] [CrossRef]
- Rosenberg, S.A.; Yang, J.C.; White, D.E.; Steinberg, S.M. Durability of complete responses in patients with metastatic cancer treated with high-dose interleukin-2: Identification of the antigens mediating response. Ann. Surg. 1998, 228, 307. [Google Scholar] [CrossRef]
- Holder, P.G.; Lim, S.A.; Huang, C.S.; Sharma, P.; Dagdas, Y.; Bulutoglu, B.; Sockolosky, J.T. Engineering interferons and interleukins for cancer immunotherapy. Adv. Drug Deliv. Rev. 2022, 182, 114112. [Google Scholar] [CrossRef]
- Krieg, C.; Létourneau, S.; Pantaleo, G.; Boyman, O. Improved IL-2 immunotherapy by selective stimulation of IL-2 receptors on lymphocytes and endothelial cells. Proc. Natl. Acad. Sci. USA 2010, 107, 11906–11911. [Google Scholar] [CrossRef]
- Jiang, T.; Zhou, C.; Ren, S. Role of IL-2 in cancer immunotherapy. Oncoimmunology 2016, 5, e1163462. [Google Scholar] [CrossRef]
- Malek, T.R.; Castro, I. Interleukin-2 receptor signaling: At the interface between tolerance and immunity. Immunity 2010, 33, 153–165. [Google Scholar] [CrossRef]
- Skrombolas, D.; Frelinger, J.G. Challenges and developing solutions for increasing the benefits of IL-2 treatment in tumor therapy. Expert Rev. Clin. Immunol. 2014, 10, 207–217. [Google Scholar] [CrossRef]
- Boyman, O.; Arenas-Ramirez, N. Development of a novel class of interleukin-2 immunotherapies for metastatic cancer. Swiss Med. Wkly. 2019, 149, w14697. [Google Scholar] [CrossRef] [PubMed]
- Lopes, J.E.; Fisher, J.L.; Flick, H.L.; Wang, C.; Sun, L.; Ernstoff, M.S.; Alvarez, J.C.; Losey, H.C. ALKS 4230: A novel engineered IL-2 fusion protein with an improved cellular selectivity profile for cancer immunotherapy. J. Immunother. Cancer 2020, 8, e000673. [Google Scholar] [CrossRef]
- Lopes, J.E.; Sun, L.; Flick, H.L.; Murphy, E.A.; Losey, H.C. Pharmacokinetics and pharmacodynamic effects of nemvaleukin alfa, a selective agonist of the intermediate-affinity IL-2 receptor, in cynomolgus monkeys. J. Pharmacol. Exp. Ther. 2021, 379, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Ulka, N.V.; Tomczak, P.; Muzaffar, J.; Winer, I.S.; Rosen, S.D.; Hoimes, C.J.; Chauhan, A.; Spreafico, A.; Lewis, K.D.; Bruno, D.S.; et al. Nemvaleukin alfa monotherapy and in combination with pembrolizumab in patients (pts) with advanced solid tumors: ARTISTRY-1. J. Clin. Oncol. 2022, 40, 2500. [Google Scholar] [CrossRef]
- Hamid, O.; Liu, S.V.; Boccia, R.V.; Call, J.A.; Wise-Draper, T.M.; Alistar, A.T.; Powderly, J.D.; Carthon, B.C.; Vaishampayan, U.N.; Olszanski, A.J.; et al. Selection of the recommended phase 2 dose (RP2D) for subcutaneous nemvaleukin alfa: ARTISTRY-2. J. Clin. Oncol. 2021, 39, 2552. [Google Scholar] [CrossRef]
- Diab, A.; Gogas, H.J.; Sandhu, S.K.; Long, G.V.; Ascierto, P.A.; Larkin, J.; Sznol, M.; Franke, F.A.; Ciuleanu, T.; Couselo, E.M.; et al. First disclosure of efficacy and safety of bempegaldesleukin (BEMPEG) plus nivolumab (NIVO) vs NIVO monotherapy in advanced melanoma (MEL). Ann. Oncol. 2022, 33, 7850. [Google Scholar] [CrossRef]
- Tannir, N.; Formiga, M.N.; Agarwal, N.; Pal, S.K.; Cho, D.; George, D.J.; Hong, W.; Tang, L.; Qureshi, A.; Tagliaferri, M.A.; et al. Bempegaldesleukin (BEMPEG) plus nivolumab (NIVO) compared to the investigator’s choice of sunitinib or cabozantinib in previously untreated advanced renal cell carcinoma (RCC): Results from a phase III randomized study (PIVOT-09). Ann. Oncol. 2022, 33, S808–S869. [Google Scholar] [CrossRef]
- Janku, F.; Abdul-Karim, R.; Azad, A.; Bendell, J.; Falchook, G.; Gan, H.K.; Tan, T.; Wang, J.S.; Chee, C.E.; Ma, L.; et al. THOR-707 (SAR444245), a novel not-alpha IL-2 as monotherapy and in combination with pembrolizumab in advanced/metastatic solid tumors: Interim results from HAMMER, an open-label, multicenter phase 1/2 Study. Cancer Res. 2021, 81, 13. [Google Scholar] [CrossRef]
- Zhang, Y.; Ptacin, J.L.; Fischer, E.C.; Aerni, H.R.; Caffaro, C.E.; San Jose, K.; Feldman, A.W.; Turner, C.R.; Romesberg, F.E. A semi-synthetic organism that stores and retrieves increased genetic information. Nature 2017, 551, 644–647. [Google Scholar] [CrossRef]
- Rosen, D.B.; Kvarnhammar, A.M.; Laufer, B.; Knappe, T.; Karlsson, J.J.; Hong, E.; Lee, Y.C.; Thakar, D.; Zuniga, L.A.; Bang, K.; et al. TransCon IL-2 beta/gamma: A novel long-acting prodrug with sustained release of an IL-2Rbeta/gamma-selective IL-2 variant with improved pharmacokinetics and potent activation of cytotoxic immune cells for the treatment of cancer. J. Immunother. Cancer 2022, 10, e004991. [Google Scholar] [CrossRef]
- MacDonald, A.; Wu, T.C.; Hung, C.F. Interleukin 2-Based Fusion Proteins for the Treatment of Cancer. J. Immunol. Res. 2021, 2021, 7855808. [Google Scholar] [CrossRef]


{kind=link}
| Title | Cancer Type | Phase of Clinical Trial and Status | Clinical Trial.gov Number |
|---|---|---|---|
| Less Frequent IV Dosing & Tumor Microenvironment (TME) Study of Nemvaleukin Alfa Monotherapy and in Combination with Pembrolizumab (ARTISTRY-3) | Advanced solid tumors | Phase 1/2, recruiting | NCT04592653 |
| A Dose Escalation and Cohort Expansion Study of Subcutaneously-Administered Cytokine Nemvaleukin Alfa as a Single Agent and in Combination with Anti-PD-1 Antibody (Pembrolizumab) in Subjects with Select Advanced or Metastatic Solid Tumors (ARTISTRY-2) | Advanced solid tumors | Phase 1/2, active, not recruiting | NCT03861793 |
| A Study of the Effects of Nemvaleukin Alfa on Subjects with Solid Tumors (ARTISTRY-1) | Advanced solid tumors | Phase 1/2, active, not recruiting | NCT02799095 |
| A Study of Nemvaleukin Alfa with Pembrolizumab in Head and Neck Cancer | Non-cutaneous squamous cell carcinoma of head and neck | Phase 2, completed | NCT04144517 |
| Nemvaleukin Alfa Monotherapy in Patients with Advanced Cutaneous Melanoma or Advanced Mucosal Melanoma (ARTISTRY-6) | Cutaneous and mucosal melanoma | Phase 2, recruiting | NCT04830124 |
| Phase 3 Study of Nemvaleukin Alfa in Combination with Pembrolizumab in Patients with Platinum-Resistant Epithelial Ovarian Cancer (ARTISTRY-7) | Platinum-resistant ovarian cancer, fallopian tube cancer, and primary peritoneal cancer | Phase 3, recruiting | NCT05092360 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ko, B.; Takebe, N.; Andrews, O.; Makena, M.R.; Chen, A.P. Rethinking Oncologic Treatment Strategies with Interleukin-2. Cells 2023, 12, 1316. https://doi.org/10.3390/cells12091316
Ko B, Takebe N, Andrews O, Makena MR, Chen AP. Rethinking Oncologic Treatment Strategies with Interleukin-2. Cells. 2023; 12(9):1316. https://doi.org/10.3390/cells12091316
Chicago/Turabian StyleKo, Brian, Naoko Takebe, Omozusi Andrews, Monish Ram Makena, and Alice P. Chen. 2023. "Rethinking Oncologic Treatment Strategies with Interleukin-2" Cells 12, no. 9: 1316. https://doi.org/10.3390/cells12091316