
Cytoplasmic Colocalization of RXRα and PPARγ as an Independent Negative Prognosticator for Breast Cancer Patients

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Immunohistochemical Stainings
2.3. Immunoreactive Score (IRS)
2.4. Statistical and Survival Analysis
3. Results
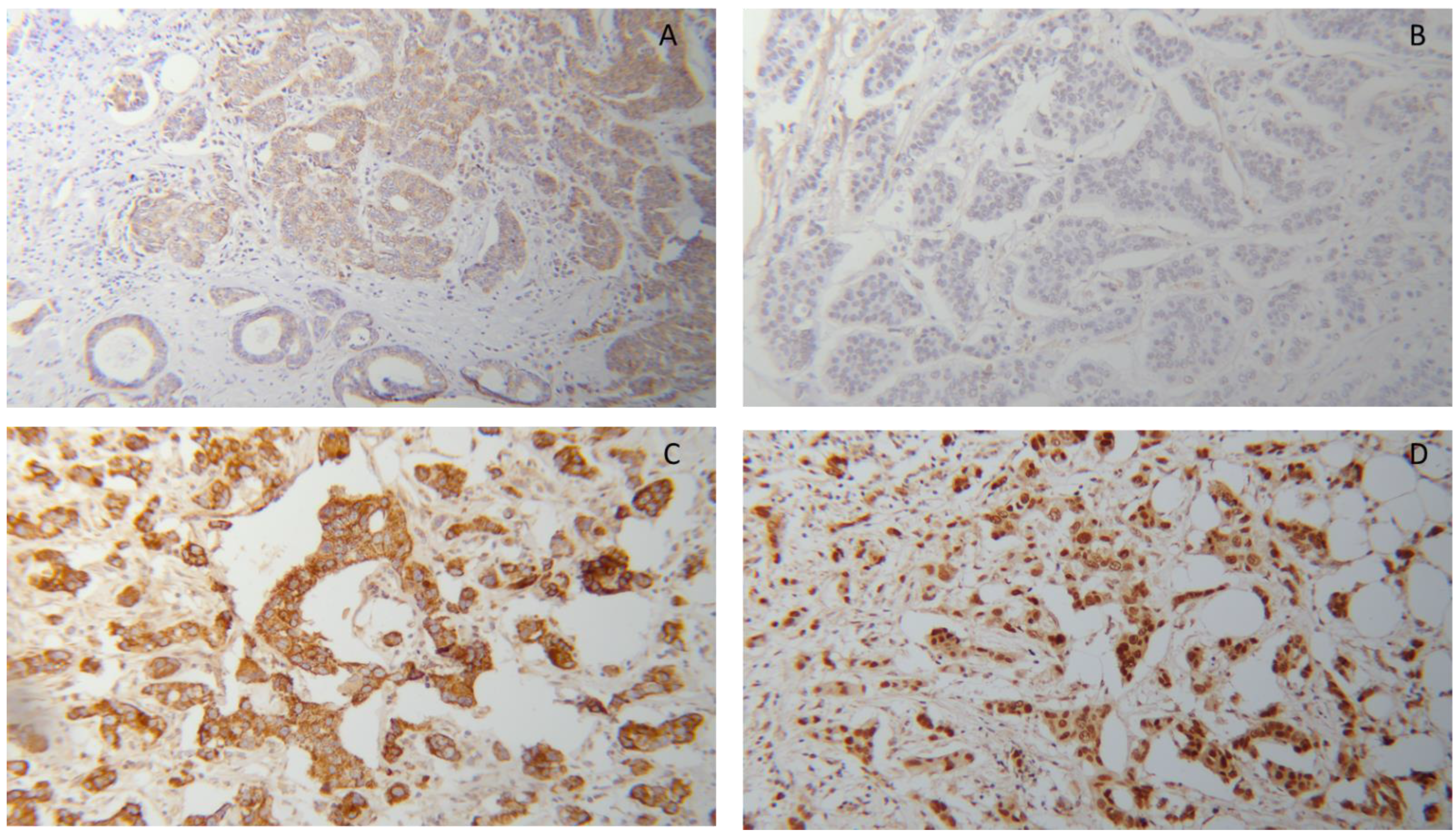
3.1. Co-Expression of RXRα and PPARγ in BC Tissues
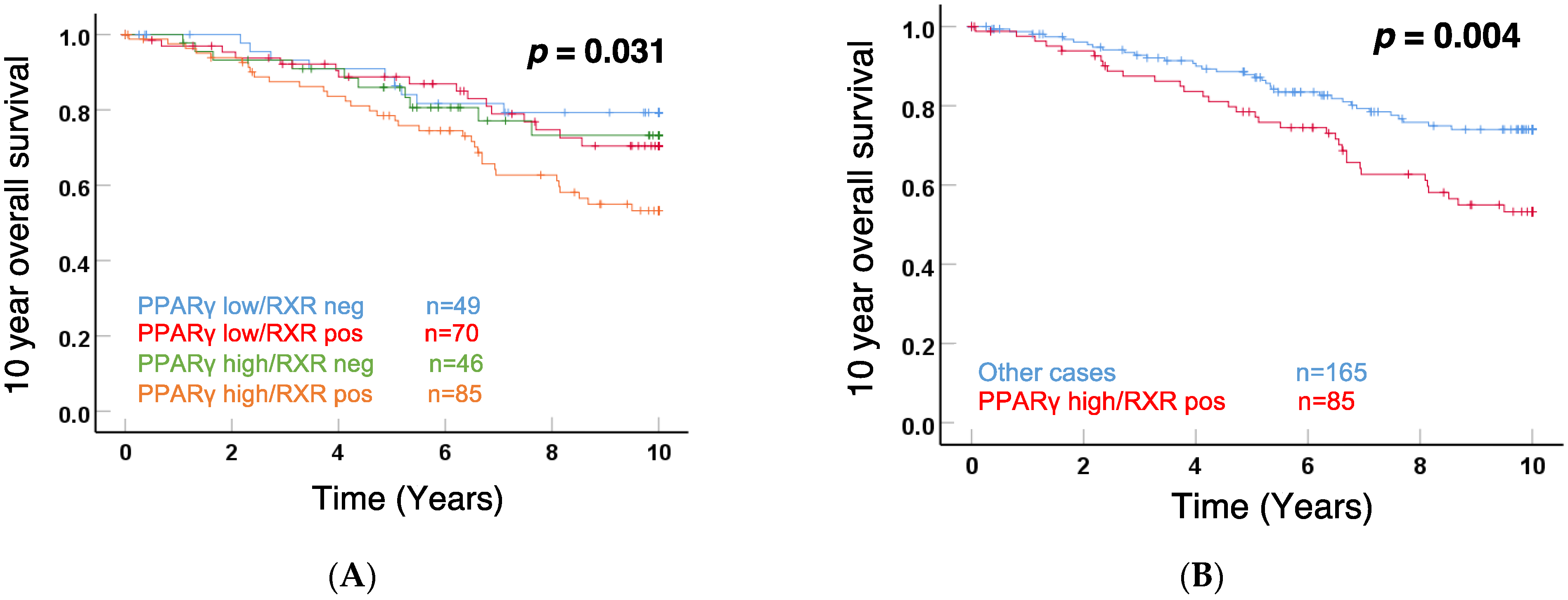
3.2. Cytoplasmic RXRα and PPARγ Expression Correlated with Patient 10-Year OS
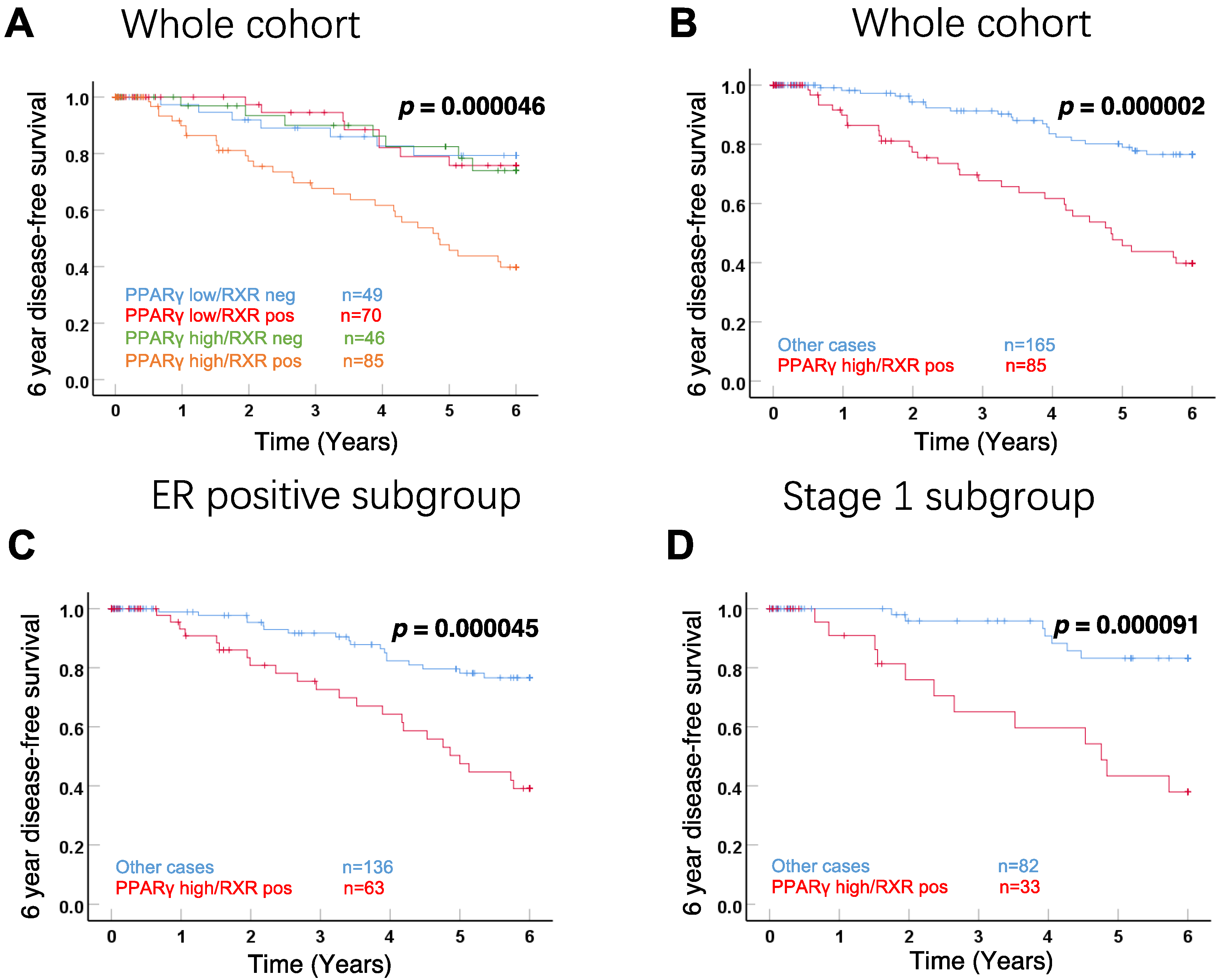
3.3. Correlation with DFS in the Whole Cohort and Subgroups
3.4. Correlation of Cytoplasmic Positive RXRα/High Expression PPARγ with Clinical Parameters
3.5. Cytoplasmic Expression of RXRα/PPARγ as an Independent Prognostic Factor
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Valerio, M.R.; Bajardi, A.E.; Arcara, C.C.; Borsellino, N.; Lo Mauro, M.; Cipolla, C.; Santarpia, M.; Firenze, A.; Motta, G.; Vigneri, P.; et al. Eribulin Mesylate for the Treatment of Metastatic Hormone-refractory and Triple-negative Breast Cancer: A Multi-institutional Real-world Report on Efficacy and Safety. Am. J. Clin. Oncol. 2021, 44, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Walbaum, B.; Acevedo, F.; Medina, L.; Bravo, M.L.; Merino, T.; Camus, M.; Dominguez, F.; Mondaca, S.; Galindo, H.; Nervi, B.; et al. Pathological complete response to neoadjuvant chemotherapy, but not the addition of carboplatin, is associated with improved survival in Chilean triple negative breast cancer patients: A report of real world data. Ecancermedicalscience 2021, 15, 1178. [Google Scholar] [CrossRef]
- Fisher, B.; Costantino, J.P.; Wickerham, D.L.; Cecchini, R.S.; Cronin, W.M.; Robidoux, A.; Bevers, T.B.; Kavanah, M.T.; Atkins, J.N.; Margolese, R.G.; et al. Tamoxifen for the prevention of breast cancer: Current status of the National Surgical Adjuvant Breast and Bowel Project P-1 study. J. Natl. Cancer Inst. 2005, 97, 1652–1662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cauley, J.A.; Norton, L.; Lippman, M.E.; Eckert, S.; Krueger, K.A.; Purdie, D.W.; Farrerons, J.; Karasik, A.; Mellstrom, D.; Ng, K.W.; et al. Continued breast cancer risk reduction in postmenopausal women treated with raloxifene: 4-year results from the MORE trial. Multiple outcomes of raloxifene evaluation. Breast Cancer Res. Treat. 2001, 65, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Goss, P.E.; Ingle, J.N.; Ales-Martinez, J.E.; Cheung, A.M.; Chlebowski, R.T.; Wactawski-Wende, J.; McTiernan, A.; Robbins, J.; Johnson, K.C.; Martin, L.W.; et al. Exemestane for breast-cancer prevention in postmenopausal women. N. Engl. J. Med. 2011, 364, 2381–2391. [Google Scholar] [CrossRef] [Green Version]
- Khazal, K.F.; Hill, D.L. Withania somnifera extract reduces the invasiveness of MDA-MB-231 breast cancer and inhibits cytokines associated with metastasis. J. Cancer Metastasis Treat. 2015, 1, 94–100. [Google Scholar] [CrossRef] [Green Version]
- Fisher, B.; Costantino, J.P.; Wickerham, D.L.; Redmond, C.K.; Kavanah, M.; Cronin, W.M.; Vogel, V.; Robidoux, A.; Dimitrov, N.; Atkins, J.; et al. Tamoxifen for prevention of breast cancer: Report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J. Natl. Cancer Inst. 1998, 90, 1371–1388. [Google Scholar] [CrossRef] [PubMed]
- Muscat, G.E.; Eriksson, N.A.; Byth, K.; Loi, S.; Graham, D.; Jindal, S.; Davis, M.J.; Clyne, C.; Funder, J.W.; Simpson, E.R.; et al. Research resource: Nuclear receptors as transcriptome: Discriminant and prognostic value in breast cancer. Mol. Endocrinol. 2013, 27, 350–365. [Google Scholar] [CrossRef] [PubMed]
- Escriva, H.; Bertrand, S.; Laudet, V. The evolution of the nuclear receptor superfamily. Essays Biochem. 2004, 40, 11–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawson, M.I.; Xia, Z. The retinoid X receptors and their ligands. Biochim. Biophys. Acta 2012, 1821, 21–56. [Google Scholar] [CrossRef] [Green Version]
- Hua, S.; Kittler, R.; White, K.P. Genomic antagonism between retinoic acid and estrogen signaling in breast cancer. Cell 2009, 137, 1259–1271. [Google Scholar] [CrossRef] [Green Version]
- Ditsch, N.; Heublein, S.; Jeschke, U.; Sattler, C.; Kuhn, C.; Hester, A.; Czogalla, B.; Trillsch, F.; Mahner, S.; Engel, J.; et al. Cytoplasmic versus nuclear THR alpha expression determines survival of ovarian cancer patients. J. Cancer Res. Clin. Oncol. 2020, 146, 1923–1932. [Google Scholar] [CrossRef]
- Zehni, Z.A.; Jacob, S.N.; Mumm, J.N.; Heidegger, H.H.; Ditsch, N.; Mahner, S.; Jeschke, U.; Vilsmaier, T. Hormone Receptor Expression in Multicentric/Multifocal versus Unifocal Breast Cancer: Especially the VDR Determines the Outcome Related to Focality. Int. J. Mol. Sci. 2019, 20, 5740. [Google Scholar] [CrossRef] [Green Version]
- Zehni, Z.A.; Batz, F.; Cavailles, V.; Sixou, S.; Kaltofen, T.; Keckstein, S.; Heidegger, H.H.; Ditsch, N.; Mahner, S.; Jeschke, U.; et al. Cytoplasmic Localization of RXRalpha Determines Outcome in Breast Cancer. Cancers 2021, 13, 3756. [Google Scholar] [CrossRef]
- Shao, W.; Kuhn, C.; Mayr, D.; Ditsch, N.; Kailuwait, M.; Wolf, V.; Harbeck, N.; Mahner, S.; Jeschke, U.; Cavailles, V.; et al. Cytoplasmic PPARgamma is a marker of poor prognosis in patients with Cox-1 negative primary breast cancers. J. Transl. Med. 2020, 18, 94. [Google Scholar] [CrossRef] [PubMed]
- Ditsch, N.; Vrekoussis, T.; Lenhard, M.; Ruhl, I.; Gallwas, J.; Weissenbacher, T.; Friese, K.; Mayr, D.; Makrigiannakis, A.; Jeschke, U. Retinoid X receptor alpha (RXRalpha) and peroxisome proliferator-activated receptor gamma (PPARgamma) expression in breast cancer: An immunohistochemical study. In Vivo 2012, 26, 87–92. [Google Scholar]
- Nagi, C.; Guttman, M.; Jaffer, S.; Qiao, R.; Keren, R.; Triana, A.; Li, M.; Godbold, J.; Bleiweiss, I.J.; Hazan, R.B. N-cadherin expression in breast cancer: Correlation with an aggressive histologic variant–invasive micropapillary carcinoma. Breast Cancer Res. Treat. 2005, 94, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, I.; Mylona, E.; Giannopoulou, I.; Markaki, S.; Keramopoulos, A.; Nakopoulou, L. PPARgamma expression in breast cancer: Clinical value and correlation with ERbeta. Histopathology 2005, 46, 37–42. [Google Scholar] [CrossRef]
- Michalik, L.; Desvergne, B.; Wahli, W. Peroxisome-proliferator-activated receptors and cancers: Complex stories. Nat. Rev. Cancer 2004, 4, 61–70. [Google Scholar] [CrossRef]
- Yang, Y.; Burke, R.V.; Jeon, C.Y.; Chang, S.C.; Chang, P.Y.; Morgenstern, H.; Tashkin, D.P.; Mao, J.; Cozen, W.; Mack, T.M.; et al. Polymorphisms of peroxisome proliferator-activated receptors and survival of lung cancer and upper aero-digestive tract cancers. Lung Cancer 2014, 85, 449–456. [Google Scholar] [CrossRef] [Green Version]
- Grommes, C.; Landreth, G.E.; Heneka, M.T. Antineoplastic effects of peroxisome proliferator-activated receptor gamma agonists. Lancet Oncol. 2004, 5, 419–429. [Google Scholar] [CrossRef]
- Sertznig, P.; Seifert, M.; Tilgen, W.; Reichrath, J. Present concepts and future outlook: Function of peroxisome proliferator-activated receptors (PPARs) for pathogenesis, progression, and therapy of cancer. J. Cell. Physiol. 2007, 212, 1–12. [Google Scholar] [CrossRef]
- Stoll, B.A. Linkage between retinoid and fatty acid receptors: Implications for breast cancer prevention. Eur. J. Cancer Prev. 2002, 11, 319–325. [Google Scholar] [CrossRef] [PubMed]
- von Knethen, A.; Tzieply, N.; Jennewein, C.; Brune, B. Casein-kinase-II-dependent phosphorylation of PPARgamma provokes CRM1-mediated shuttling of PPARgamma from the nucleus to the cytosol. J. Cell Sci. 2010, 123, 192–201. [Google Scholar] [CrossRef] [Green Version]
- Heublein, S.; Mayr, D.; Meindl, A.; Kircher, A.; Jeschke, U.; Ditsch, N. Vitamin D receptor, Retinoid X receptor and peroxisome proliferator-activated receptor gamma are overexpressed in BRCA1 mutated breast cancer and predict prognosis. J. Exp. Clin. Cancer Res. 2017, 36, 57. [Google Scholar] [CrossRef] [Green Version]
- Calvo, V.; Beato, M. BRCA1 counteracts progesterone action by ubiquitination leading to progesterone receptor degradation and epigenetic silencing of target promoters. Cancer Res. 2011, 71, 3422–3431. [Google Scholar] [CrossRef] [Green Version]
- Tsao, W.C.; Wu, H.M.; Chi, K.H.; Chang, Y.H.; Lin, W.W. Proteasome inhibitors induce peroxisome proliferator-activated receptor transactivation through RXR accumulation and a protein kinase C-dependent pathway. Exp. Cell Res. 2005, 304, 234–243. [Google Scholar] [CrossRef]
- Lattuada, D.; Vigano, P.; Mangioni, S.; Sassone, J.; Di Francesco, S.; Vignali, M.; Di Blasio, A.M. Accumulation of retinoid X receptor-alpha in uterine leiomyomas is associated with a delayed ligand-dependent proteasome-mediated degradation and an alteration of its transcriptional activity. Mol. Endocrinol. 2007, 21, 602–612. [Google Scholar] [CrossRef] [Green Version]
- Desreumaux, P.; Dubuquoy, L.; Nutten, S.; Peuchmaur, M.; Englaro, W.; Schoonjans, K.; Derijard, B.; Desvergne, B.; Wahli, W.; Chambon, P.; et al. Attenuation of colon inflammation through activators of the retinoid X receptor (RXR)/peroxisome proliferator-activated receptor gamma (PPARgamma) heterodimer. A basis for new therapeutic strategies. J. Exp. Med. 2001, 193, 827–838. [Google Scholar] [CrossRef] [Green Version]
- Ray, D.M.; Bernstein, S.H.; Phipps, R.P. Human multiple myeloma cells express peroxisome proliferator-activated receptor gamma and undergo apoptosis upon exposure to PPARgamma ligands. Clin. Immunol. 2004, 113, 203–213. [Google Scholar] [CrossRef]
- Giaginis, C.; Katsamangou, E.; Tsourouflis, G.; Zizi-Serbetzoglou, D.; Kouraklis, G.; Theocharis, S. Peroxisome proliferator-activated receptor-gamma and retinoid X receptor-alpha expression in pancreatic ductal adenocarcinoma: Association with clinicopathological parameters, tumor proliferative capacity, and patients’ survival. Med. Sci. Monit. 2009, 15, BR148–BR156. [Google Scholar] [PubMed]
- He, B.C.; Chen, L.; Zuo, G.W.; Zhang, W.; Bi, Y.; Huang, J.; Wang, Y.; Jiang, W.; Luo, Q.; Shi, Q.; et al. Synergistic antitumor effect of the activated PPARgamma and retinoid receptors on human osteosarcoma. Clin. Cancer Res. 2010, 16, 2235–2245. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.Y.; Wang, J.J.; Lee, H.C.; Chi, C.W.; Lee, C.H.; Hsu, Y.C. Combination of peroxisome proliferator-activated receptor gamma and retinoid X receptor agonists induces sodium/iodide symporter expression and inhibits cell growth of human thyroid cancer cells. J. Chin. Med. Assoc. 2020, 83, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Bonofiglio, D.; Cione, E.; Vizza, D.; Perri, M.; Pingitore, A.; Qi, H.; Catalano, S.; Rovito, D.; Genchi, G.; Ando, S. Bid as a potential target of apoptotic effects exerted by low doses of PPARgamma and RXR ligands in breast cancer cells. Cell Cycle 2011, 10, 2344–2354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papi, A.; De Carolis, S.; Bertoni, S.; Storci, G.; Sceberras, V.; Santini, D.; Ceccarelli, C.; Taffurelli, M.; Orlandi, M.; Bonafe, M. PPARgamma and RXR ligands disrupt the inflammatory cross-talk in the hypoxic breast cancer stem cells niche. J. Cell. Physiol. 2014, 229, 1595–1606. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Clinical and Pathological Characteristics a | n = 250 b |
|---|---|
| Age, median (years) | 57.76 |
| Molecular subtype (IHC) | |
| Luminal A (Ki67 ≤ 14%) | 135 |
| Luminal B (Ki67 > 14%) | 56 |
| HER2 positive | 16 |
| HER2 non luminal | 9 |
| Triple negative | 33 |
| Unknown | 1 |
| Grade | |
| I | 12 |
| II | 90 |
| III | 41 |
| Unknown | 107 |
| Tumor size | |
| pT1 | 165 |
| pT2 | 71 |
| pT3 | 4 |
| pT4 | 10 |
| Lymph node metastasis | |
| Yes | 105 |
| No | 140 |
| Unknown | 5 |
| ER status | |
| Positive | 199 |
| Negative | 51 |
| PR status | |
| Positive | 145 |
| Negative | 105 |
| Cytoplasmic PPARγ expression | |
| Low (IRS < 3.5) | 119 |
| High (IRS > 3.5) | 131 |
| Cytoplasmic RXRα expression | |
| Negative | 95 |
| Positive | 155 |
| Correlation Coefficient | p | n | |
|---|---|---|---|
| Age | 0.002 | 0.755 | 250 |
| pT | 0.106 | 0.094 | 250 |
| pN | 0.05 | 0.433 | 245 |
| Grade | −0.029 | 0.733 | 143 |
| ER | −0.0099 | 0.109 | 261 |
| PR | −0.034 | 0.580 | 261 |
| Her2 | 0.160 ** | 0.010 | 261 |
| Triple-negative | 0.074 | 0.231 | 262 |
| Ki-67 | 0.020 | 0.773 | 203 |
| Focality | 0.035 | 0.572 | 262 |
| CD133 | 0.172 ** | 0.007 | 244 |
| NCAD | 0.262 *** | 0.000036 | 243 |
| Group | p | HR | 95% CI | 5-Year OS Rate | 10-Year OS Rate |
|---|---|---|---|---|---|
| RXRα neg/PPARγ low | 0.086 | 0.54 | 0.26–1.09 | 79.59% | 51.02% |
| RXRα neg/PPARγ high | 0.507 | 0.79 | 0.40–1.37 | 71.74% | 32.61% |
| RXRα pos/PPARγ low | 0.394 | 0.78 | 0.44–1.37 | 71.43% | 35.71% |
| RXRα pos/PPARγ high | 0.005 ** | 1.97 | 1.23–3.16 | 69.41% | 31.76% |
| p | HR | 95% CI | |
|---|---|---|---|
| Histology | 0.225 | 1.018 | 0.989–1.047 |
| pT | 0.066 | 1.252 | 0.985–1.590 |
| pN | 0.016 * | 1.269 | 1.046–1.541 |
| Grading | 0.414 | 1.363 | 0.648–2.865 |
| ER | 0.242 | 0.495 | 0.153–1.607 |
| PR | 0.810 | 1.117 | 0.453–2.750 |
| Her2 | 0.167 | 2.197 | 0.720–6.708 |
| Triple-negative | 0.627 | 1.489 | 0.299–7.416 |
| PPARγ high/RXR pos | 0.035 * | 2.175 | 1.054–4.487 |
| p | HR | 95% CI | |
|---|---|---|---|
| Histology | 0.233 | 0.833 | 0.618–1.124 |
| pT | 0.269 | 4.441 | 0.315–62.589 |
| pN | - | - | - |
| Grading | 0.332 | 0.454 | 0.092–2.238 |
| ER | 0.521 | 0.364 | 0.017–8.004 |
| PR | 0.657 | 1.810 | 0.132–24.726 |
| Her2 | 0.185 | 7.835 | 0.374–163.958 |
| Triple-negative | 0.487 | 4.336 | 0.069–272.193 |
| PPARγ high/RXR pos | 0.013 * | 10.065 | 1.644–61.617 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shao, W.; Köpke, M.B.; Vilsmaier, T.; Zati Zehni, A.; Kessler, M.; Sixou, S.; Schneider, M.; Ditsch, N.; Cavaillès, V.; Jeschke, U. Cytoplasmic Colocalization of RXRα and PPARγ as an Independent Negative Prognosticator for Breast Cancer Patients. Cells 2022, 11, 1244. https://doi.org/10.3390/cells11071244
Shao W, Köpke MB, Vilsmaier T, Zati Zehni A, Kessler M, Sixou S, Schneider M, Ditsch N, Cavaillès V, Jeschke U. Cytoplasmic Colocalization of RXRα and PPARγ as an Independent Negative Prognosticator for Breast Cancer Patients. Cells. 2022; 11(7):1244. https://doi.org/10.3390/cells11071244
Chicago/Turabian StyleShao, Wanting, Melitta B. Köpke, Theresa Vilsmaier, Alaleh Zati Zehni, Mirjana Kessler, Sophie Sixou, Mariella Schneider, Nina Ditsch, Vincent Cavaillès, and Udo Jeschke. 2022. "Cytoplasmic Colocalization of RXRα and PPARγ as an Independent Negative Prognosticator for Breast Cancer Patients" Cells 11, no. 7: 1244. https://doi.org/10.3390/cells11071244