
Towards Personalized Medicine in Myasthenia Gravis: Role of Circulating microRNAs miR-30e-5p, miR-150-5p and miR-21-5p

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patient Cohorts
2.2. Blood Samples, RNA Isolation and qPCR
2.3. Study Design and Statistical Analyses
3. Results
3.1. Patients and Controls Demographics
3.2. Serum miRNA Levels
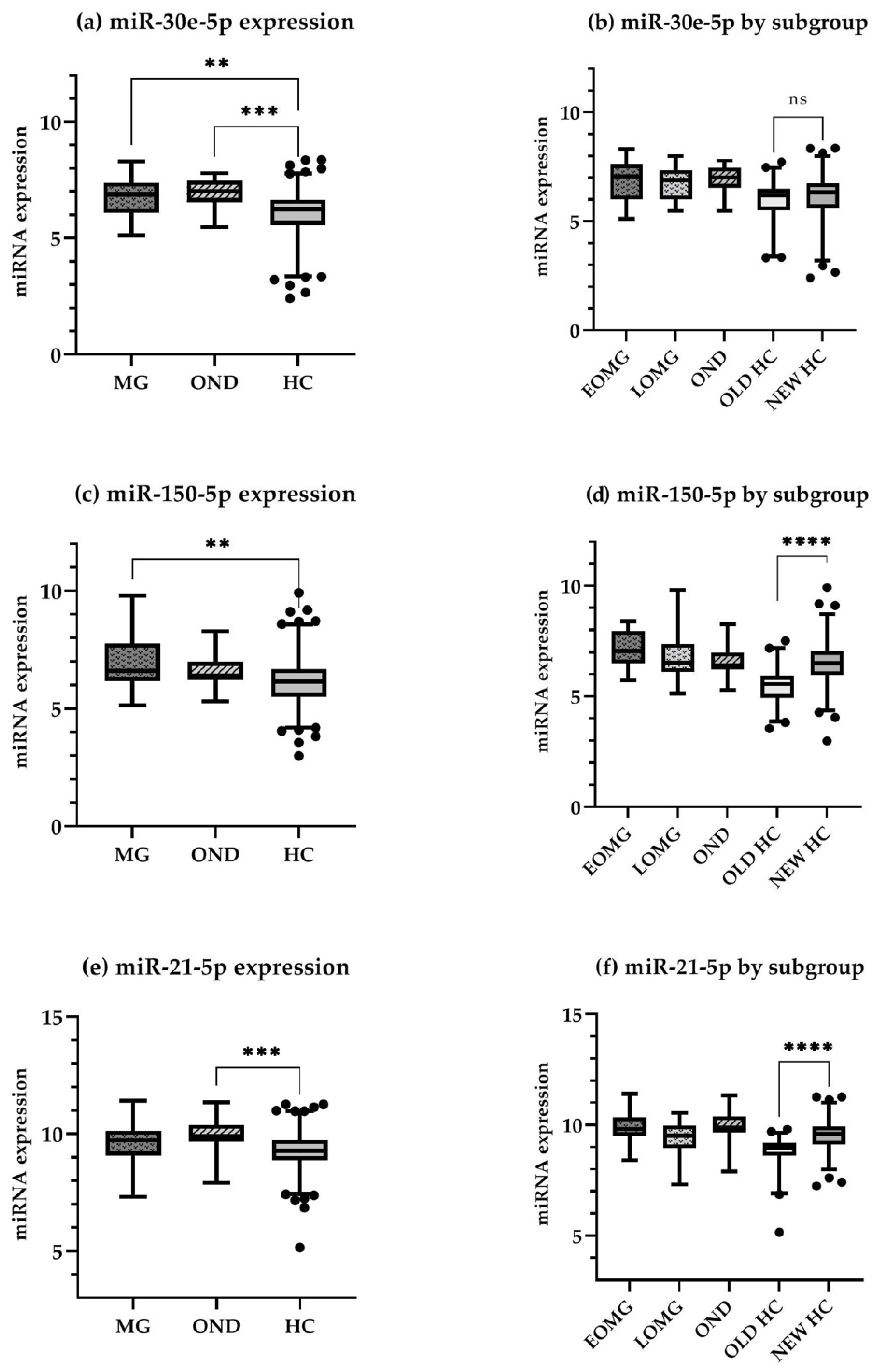
3.2.1. Primary Analyses
3.2.2. Secondary Analyses
3.2.3. Predictive Value of miR-30e-5p in MG Progression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target | Target Sequence | miRCURY® Assay | |
|---|---|---|---|
| Target miRNAs | miR-30e-5p | UGUAAACAUCCUUGACUGGAAG | YP00204714 |
| miR-150-5p | UCUCCCAACCCUUGUACCAGUG | YP00204660 | |
| miR-21-5p | UAGCUUAUCAGACUGAUGUUGA | YP00204230 | |
| Reference miRNAs candidates | miR-191-3p | CAACGGAAUCCCAAAAGCAGCUG | YP00204306 |
| miR-103a-3p | AGCAGCAUUGUACAGGGCUAUGA | YP00204063 | |
| Hemolysis index miRNAs | miR-23a-3p | AUCACAUUGCCAGGGAUUUCC | YP00204772 |
| miR-451a | AAACCGUUACCAUUACUGAGUU | YP02119305 | |
| Synthetic RNA spike-ins | UniSp2 | Unavailable | YP00203950 |
| UniSp4 | Unavailable | YP00203953 | |
| UniSp5 | Unavailable | YP00203955 | |
| UniSp6 | Unavailable | YP00203954 | |
| UniSp3 | Unavailable | YP02119288 |
References
- Punga, A.R.; Maddison, P.; Heckmann, J.M.; Guptill, J.T.; Evoli, A. Epidemiology, diagnostics and biomarkers of autoimmune neuromuscular junction disorders. Lancet Neurol. 2022, 21, 176–188. [Google Scholar] [CrossRef]
- Meriggioli, M.N.; Sanders, D.B. Autoimmune Myasthenia Gravis: Emerging Clinical and Biological Heterogeneity. Lancet Neurol. 2009, 8, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Borges, L.S.; Richman, D.P. Muscle-Specific Kinase Myasthenia Gravis. Front. Immunol. 2020, 11, 707. [Google Scholar] [CrossRef] [PubMed]
- Fichtner, M.L.; Jiang, R.; Bourke, A.; Nowak, R.J.; O’Connor, K.C. Autoimmune Pathology in Myasthenia Gravis Disease Subtypes Is Governed by Divergent Mechanisms of Immunopathology. Front. Immunol. 2020, 11, 776. [Google Scholar] [CrossRef]
- Grob, D.; Brunner, N.; Namba, T.; Pagala, M. Lifetime Course of Myasthenia Gravis. Muscle Nerve 2008, 37, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Berrih-Aknin, S.; Le Panse, R. Myasthenia Gravis: A Comprehensive Review of Immune Dysregulation and Etiological Mechanisms. J. Autoimmun. 2014, 52, 90–100. [Google Scholar] [CrossRef]
- Dalakas, M.C. Immunotherapy in Myasthenia Gravis in the Era of Biologics. Nat. Rev. Neurol. 2019, 15, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Sabre, L.; Punga, T.; Punga, A.R. Circulating MiRNAs as Potential Biomarkers in Myasthenia Gravis: Tools for Personalized Medicine. Front. Immunol. 2020, 11, 213. [Google Scholar] [CrossRef] [Green Version]
- Burns, T.M. History of Outcome Measures for Myasthenia Gravis. Muscle Nerve 2010, 42, 5–13. [Google Scholar] [CrossRef]
- Thomsen, J.L.S.; Andersen, H. Outcome Measures in Clinical Trials of Patients With Myasthenia Gravis. Front. Neurol. 2020, 11, 596382. [Google Scholar] [CrossRef]
- Kaminski, H.J.; Kusner, L.L.; Wolfe, G.I.; Aban, I.; Minisman, G.; Conwit, R.; Cutter, G. Biomarker Development for Myasthenia Gravis. Ann. N. Y. Acad. Sci. 2012, 1275, 101–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mori, M.A.; Ludwig, R.G.; Garcia-Martin, R.; Brandão, B.B.; Kahn, C.R. Extracellular MiRNAs: From Biomarkers to Mediators of Physiology and Disease. Cell Metab. 2019, 30, 656–673. [Google Scholar] [CrossRef] [PubMed]
- Sabre, L.; Maddison, P.; Sadalage, G.; Ambrose, P.A.; Punga, A.R. Circulating MicroRNA MiR-21-5p, MiR-150-5p and MiR-30e-5p Correlate with Clinical Status in Late Onset Myasthenia Gravis. J. Neuroimmunol. 2018, 321, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Molin, C.J.; Sabre, L.; Weis, C.A.; Punga, T.; Punga, A.R. Thymectomy Lowers the Myasthenia Gravis Biomarker MiR-150-5p. Neurol. Neuroimmunol. Neuroinflamm. 2018, 5, e450. [Google Scholar] [CrossRef] [Green Version]
- Punga, T.; Le Panse, R.; Andersson, M.; Truffault, F.; Berrih-Aknin, S.; Punga, A.R. Circulating miRNAs in Myasthenia Gravis: miR-150-5p as a new potential biomarker. Ann. Clin. Transl. Neurol. 2014, 1, 49–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Punga, A.R.; Andersson, M.; Alimohammadi, M.; Punga, T. Disease Specific Signature of Circulating MiR-150-5p and MiR-21-5p in Myasthenia Gravis Patients. J. Neurol. Sci. 2015, 356, 90–96. [Google Scholar] [CrossRef]
- Zhong, H.; Lu, J.; Jing, S.; Xi, J.; Yan, C.; Song, J.; Luo, S.; Zhao, C. Low-Dose Rituximab Lowers Serum Exosomal MiR-150-5p in AChR-Positive Refractory Myasthenia Gravis Patients. J. Neuroimmunol. 2020, 348, 5777383. [Google Scholar] [CrossRef]
- Sabre, L.; Maddison, P.; Wong, S.H.; Sadalage, G.; Ambrose, P.A.; Plant, G.T.; Punga, A.R. MiR-30e-5p as Predictor of Generalization in Ocular Myasthenia Gravis. Ann. Clin. Transl. Neurol. 2019, 6, 243–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Ronde, M.W.J.; Ruijter, J.M.; Lanfear, D.; Bayes-Genis, A.; Kok, M.G.M.; Creemers, E.E.; Pinto, Y.M.; Pinto-Sietsma, S.-J. Practical Data Handling Pipeline Improves Performance of qPCR-Based Circulating miRNA Measurements. RNA 2017, 23, 811–821. [Google Scholar] [CrossRef]
- Parker, V.L.; Cushen, B.F.; Gavriil, E.; Marshall, B.; Waite, S.; Pacey, A.; Heath, P.R. Comparison and Optimisation of MicroRNA Extraction from the Plasma of Healthy Pregnant Women. Mol. Med. Rep. 2021, 23, 1. [Google Scholar] [CrossRef]
- Blondal, T.; Jensby Nielsen, S.; Baker, A.; Andreasen, D.; Mouritzen, P.; Wrang Teilum, M.; Dahlsveen, I.K. Assessing Sample and MiRNA Profile Quality in Serum and Plasma or Other Biofluids. Methods 2013, 59, S1–S6. [Google Scholar] [CrossRef] [PubMed]
- Schmittgen, T.D.; Livak, K.J. Analyzing Real-Time PCR Data by the Comparative CT Method. Nat. Protoc. 2008, 3, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Kroesen, B.J.; Teteloshvili, N.; Smigielska-Czepiel, K.; Brouwer, E.; Boots, A.M.H.; van den Berg, A.; Kluiver, J. Immuno-MiRs: Critical Regulators of T-Cell Development, Function and Ageing. Immunology 2015, 144, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Cron, M.A.; Maillard, S.; Truffault, F.; Gualeni, A.V.; Gloghini, A.; Fadel, E.; Guihaire, J.; Behin, A.; Berrih-Aknin, S.; Le Panse, R. Causes and Consequences of MiR-150-5p Dysregulation in Myasthenia Gravis. Front. Immunol. 2019, 10, 539. [Google Scholar] [CrossRef] [Green Version]
- Gong, W.-J.; Zhou, T.; Wu, S.-L.; Huang, Y.-F.; Xiang, L.-P.; Xu, J.-Q.; Han, Y.; Lv, Y.-N.; Zeng, F.; Zhang, Y. A Novel Immune-Related ceRNA Network That Predicts Prognosis and Immunotherapy Response in Lung Adenocarcinoma. Ann. Transl. Med. 2021, 9, 1484. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Zhu, X.; Sun, Q.; Qin, X.; Zhang, Z.; Feng, Y.; Yan, M.; Chen, W. Identification and Confirmation of the MiR-30 Family as a Potential Central Player in Tobacco-Related Head and Neck Squamous Cell Carcinoma. Front. Oncol. 2021, 11, 616372. [Google Scholar] [CrossRef]
- Fiorillo, A.A.; Heier, C.R.; Huang, Y.F.; Tully, C.B.; Punga, T.; Punga, A.R. Estrogen Receptor, Inflammatory, and FOXO Transcription Factors Regulate Expression of Myasthenia Gravis-Associated Circulating MicroRNAs. Front. Immunol. 2020, 11, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, A.; Leidinger, P.; Lange, J.; Borries, A.; Schroers, H.; Scheffler, M.; Lenhof, H.P.; Ruprecht, K.; Meese, E. Multiple Sclerosis: MicroRNA Expression Profiles Accurately Differentiate Patients with Relapsing-Remitting Disease from Healthy Controls. PLoS ONE 2009, 4, e7440. [Google Scholar] [CrossRef]
- Gandhi, R.; Healy, B.; Gholipour, T.; Egorova, S.; Musallam, A.; Hussain, M.S.; Nejad, P.; Patel, B.; Hei, H.; Khoury, S.; et al. Circulating MicroRNAs as Biomarkers for Disease Staging in Multiple Sclerosis. Ann. Neurol. 2013, 73, 729–740. [Google Scholar] [CrossRef]
- Kim, B.S.; Jung, J.Y.; Jeon, J.Y.; Kim, H.A.; Suh, C.H. Circulating Hsa-MiR-30e-5p, Hsa-MiR-92a-3p, and Hsa-MiR-223-3p May Be Novel Biomarkers in Systemic Lupus Erythematosus. HLA 2016, 88, 187–193. [Google Scholar] [CrossRef]
- Cheng, T.; Ding, S.; Liu, S.; Li, X.; Tang, X.; Sun, L. Resolvin D1 Improves the Treg/Th17 Imbalance in Systemic Lupus Erythematosus Through MiR-30e-5p. Front. Immunol. 2021, 12, 668760. [Google Scholar] [CrossRef] [PubMed]
- Alevizos, I.; Alexander, S.; Turner, R.J.; Illei, G.G. MicroRNA Expression Profiles as Biomarkers of Minor Salivary Gland Inflammation and Dysfunction in Sjögren’s Syndrome. Arthritis Rheum. 2011, 63, 535–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, A.P.; Hillen, M.R.; Chouri, E.; Blokland, S.L.M.; Bekker, C.P.J.; Kruize, A.A.; Rossato, M.; van Roon, J.A.G.; Radstake, T.R.D.J. Circulating Small Non-Coding RNAs Reflect IFN Status and B Cell Hyperactivity in Patients with Primary Sjögren’s Syndrome. PLoS ONE 2018, 13, e0193157. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.Q.; Papp, G.; Póliska, S.; Szabó, K.; Tarr, T.; Bálint, B.L.; Szodoray, P.; Zeher, M. MicroRNA Expression Profiles Identify Disease-Specific Alterations in Systemic Lupus Erythematosus and Primary Sjögren’s Syndrome. PLoS ONE 2017, 12, e0174585. [Google Scholar] [CrossRef] [PubMed]
- Bergman, P.; Piket, E.; Khademi, M.; James, T.; Brundin, L.; Olsson, T.; Piehl, F.; Jagodic, M. Circulating MiR-150 in CSF Is a Novel Candidate Biomarker for Multiple Sclerosis. Neurol. Neuroimmunol. Neuroinflamm. 2016, 3, e219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Z.; Cui, Y.; Qiao, X.; He, X.; Li, F.; Luo, C.; Wang, S.; Li, C.; Dai, R. Silencing MiR-150 Ameliorates Experimental Autoimmune Encephalomyelitis. Front. Neurosci. 2018, 12, 465. [Google Scholar] [CrossRef] [Green Version]
- Nakamaru, K.; Tomiyama, T.; Kobayashi, S.; Ikemune, M.; Tsukuda, S.; Ito, T.; Tanaka, T.; Yamaguchi, T.; Ando, Y.; Ikeura, T.; et al. Extracellular Vesicles MicroRNA Analysis in Type 1 Autoimmune Pancreatitis: Increased Expression of MicroRNA-21. Pancreatology 2020, 20, 318–324. [Google Scholar] [CrossRef]
- Wade, S.M.; McGarry, T.; Wade, S.C.; Fearon, U.; Veale, D.J. Serum Microrna Signature as a Diagnostic and Therapeutic Marker in Patients with Psoriatic Arthritis. J. Rheumatol. 2020, 47, 1760–1767. [Google Scholar] [CrossRef]
- Baulina, N.; Kulakova, O.; Kiselev, I.; Osmak, G.; Popova, E.; Boyko, A.; Favorova, O. Immune-Related MiRNA Expression Patterns in Peripheral Blood Mononuclear Cells Differ in Multiple Sclerosis Relapse and Remission. J. Neuroimmunol. 2018, 317, 67–76. [Google Scholar] [CrossRef]
- Amini-Farsani, Z.; Yadollahi-Farsani, M.; Arab, S.; Forouzanfar, F.; Yadollahi, M.; Asgharzade, S. Prediction and Analysis of MicroRNAs Involved in COVID-19 Inflammatory Processes Associated with the NF-KB and JAK/STAT Signaling Pathways. Int. Immunopharmacol. 2021, 100, 108071. [Google Scholar] [CrossRef]
- Laurence, M.; Benito-León, J. Epstein–Barr Virus and Multiple Sclerosis: Updating Pender’s Hypothesis. Mult. Scler. Relat. Disord. 2017, 16, 8–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez, Y.; Vatti, N.; Ramírez-Santana, C.; Chang, C.; Mancera-Páez, O.; Gershwin, M.E.; Anaya, J.M. Chronic Inflammatory Demyelinating Polyneuropathy as an Autoimmune Disease. J. Autoimmun. 2019, 102, 8–37. [Google Scholar] [CrossRef] [PubMed]
- Jaretzki, A., III; Barohn, R.J.; Ernstoff, R.M.; Kaminski, H.J.; Keesey, J.C.; Penn, A.S.; Sanders, D.B. Myasthenia Gravis: Recommendations for Clinical Research Standards. Neurology 2000, 55, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Freedman, L.S. Tables Of The Number Of Patients Required In Clinical Trials Using The Logrank Test. Stat. Med. 1982, 1, 121–129. [Google Scholar] [CrossRef] [PubMed]



| All MG | EOMG | LOMG | |
|---|---|---|---|
| Total patients | 27 | 10 | 17 |
| Sex | |||
| F | 15 (55.5%) | 8 (80%) | 7 (41%) |
| M | 12 (44.5%) | 2 (20%) | 10 (59%) |
| Age (y) [median (IQR)] | 58 (39; 69.5) | 32.5 (25; 41.5) | 68 (52; 75) |
| Time from diagnosis (months; mean ± SD) | 3.9 ± 4.7 | 5 ± 4.7 | 3.4 ± 4.8 |
| Serology: | |||
| AChR+ | 17 (63%) | 4 (40%) | 13 (76%) |
| MuSK+ | 3 (11%) | 2 (20%) | 1 (6%) |
| AChR/MuSK seronegative | 7 (30%) | 4 (40%) | 3 (18%) |
| Comorbidities: | |||
| none | 6 (22%) | 3 (30%) | 3 (18%) |
| thymoma | 3 (11%) | 2 (20%) | 1 (6%) |
| autoimmune | 8 (30%) | 3 (30%) | 5 (29%) |
| other | 10 (37%) | 2 (20%) | 8 (47%) |
| OMG at diagnosis | 10 (37%) | 4 (40%) | 6 (35%) |
| GMG at diagnosis | 17 (67%) | 6 (60%) | 11 (65%) |
| Immunosuppressive naïve (at testing) | 19 (70%) | 7 (70%) | 12 (71%) |
| Thymectomy | 9 (33%) | 5 (50%) | 4 (23,5%) |
| Generalized during FU | 8 (30%) | 4 (100%) | 4 (67%) |
| Time to generalization (m) [median (IQR)] | 6 (3.75; 7.25) | 7 (6.25; 7.25) | 4 (2.75; 6.75) |
| Disease relapse during FU | 15 (55.5%) | 6 (60%) | 9 (53%) |
| Time to relapse (m) [median (IQR)] | 7 (3.5; 13) | 7 (6.25; 7.75) | 5 (3; 16) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beretta, F.; Huang, Y.-F.; Punga, A.R. Towards Personalized Medicine in Myasthenia Gravis: Role of Circulating microRNAs miR-30e-5p, miR-150-5p and miR-21-5p. Cells 2022, 11, 740. https://doi.org/10.3390/cells11040740
Beretta F, Huang Y-F, Punga AR. Towards Personalized Medicine in Myasthenia Gravis: Role of Circulating microRNAs miR-30e-5p, miR-150-5p and miR-21-5p. Cells. 2022; 11(4):740. https://doi.org/10.3390/cells11040740
Chicago/Turabian StyleBeretta, Francesca, Yu-Fang Huang, and Anna Rostedt Punga. 2022. "Towards Personalized Medicine in Myasthenia Gravis: Role of Circulating microRNAs miR-30e-5p, miR-150-5p and miR-21-5p" Cells 11, no. 4: 740. https://doi.org/10.3390/cells11040740