

Current Status and Prospects of Targeted Therapy for Osteosarcoma
 , , ,
, , ,
Abstract
:1. Introduction
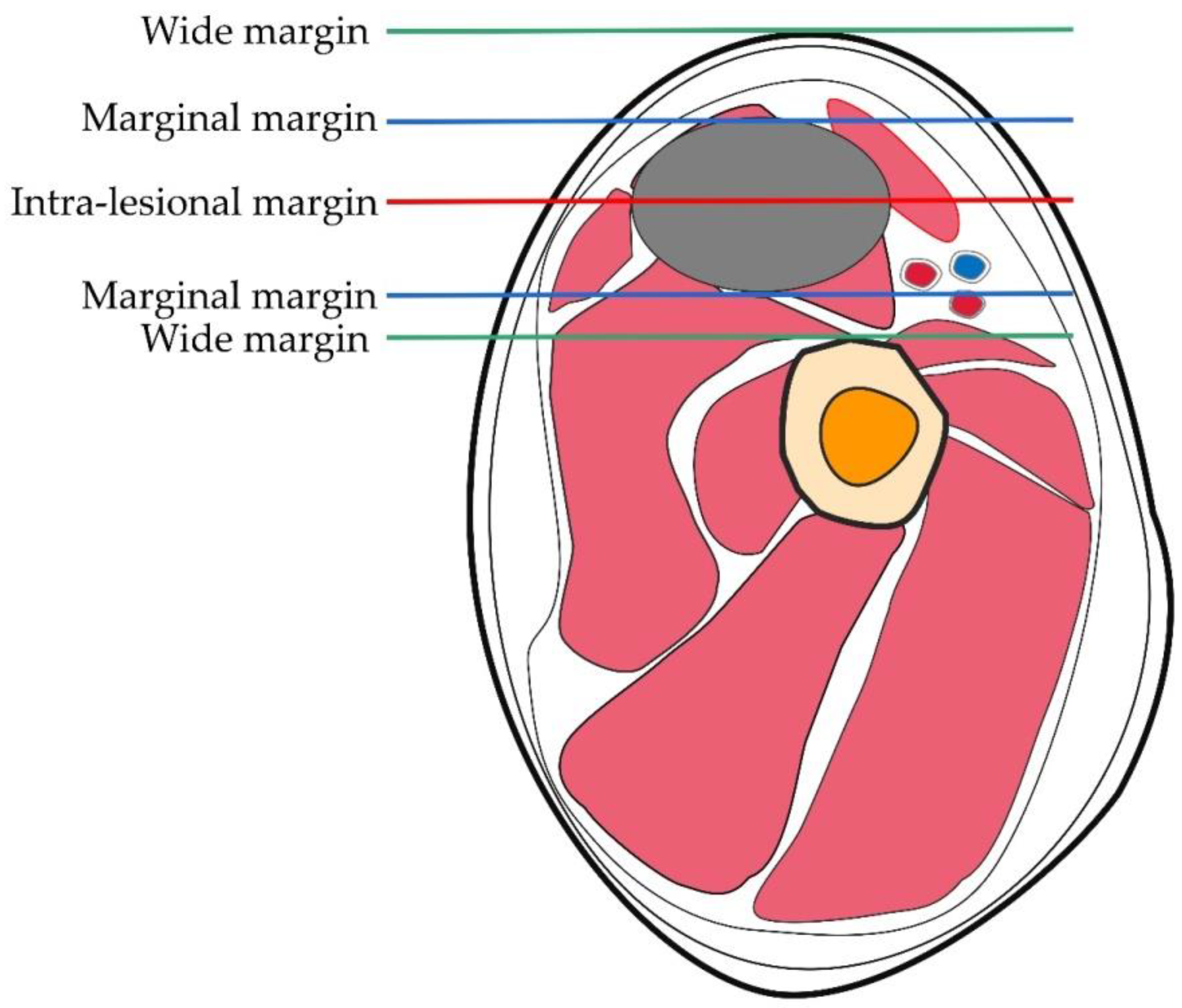
2. Surgical Treatment of OS
3. Chemotherapy for OS
4. Immunotherapy for OS
5. Targeted Therapy for OS
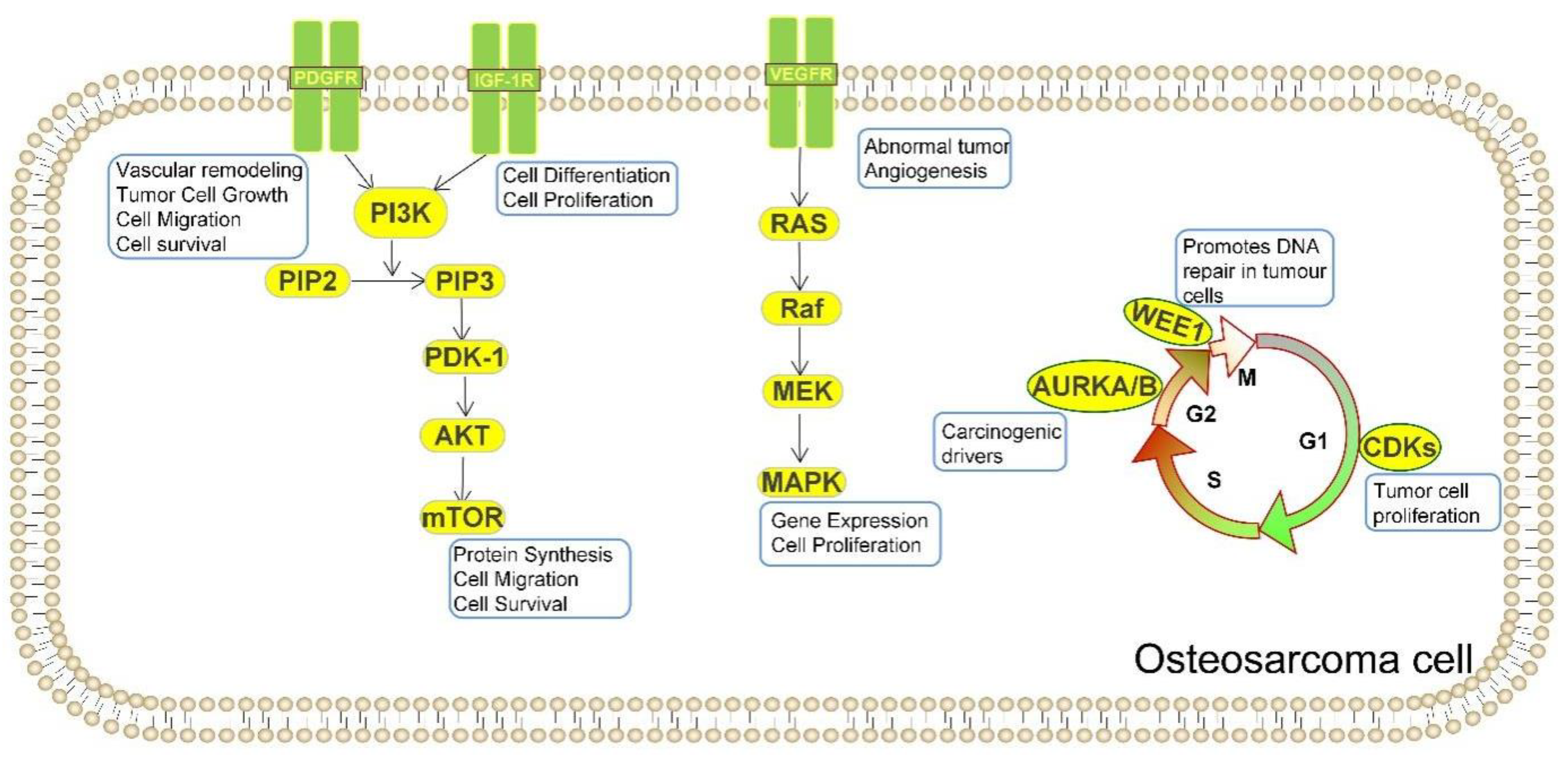
6. Different Targets for the Treatment of OS
6.1. Targeting DNA Damage Repair and Cell Cycle
6.2. Targeting Vascular Endothelial Growth Factor
6.3. Targeting Platelet-Derived Growth Factor
6.4. Targeting Insulin-like Growth Factor
6.5. Targeting PI3K/mTOR
6.6. Targeting MYC
6.7. Targeting OS Surfaceome
7. New Treatment for OS
8. Obstacles to OS Progress and Treatment
9. Conclusions and Prospects
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| OS | Osteosarcoma |
| MSTS | Musculoskeletal tumors |
| AJCC | American Joint Committee on Cancer |
| EFS | Event-free survival |
| NK | Natural killer cell |
| NKT | Natural killer T cell |
| COG | Children’s Oncology Group |
| PI3K | Phosphoinositide-3 kinase |
| PIK3CA | Phosphatidylinositol 3-kinase |
| mTOR | Mechanistic target of rapamycin |
| IGF | Insulin-like growth factor |
| IGF-1R | Insulin-like growth factor 1 receptor |
| VEGF | Vascular endothelial growth factor |
| VEGFA | Vascular endothelial growth factor A |
| KDR | Kinase insert domain receptor |
| PDGF | Platelet-derived growth factor |
| PDGFR | Platelet-derived growth factor receptor |
| DDR | DNA damage response |
| KIT | KIT proto-oncogene receptor tyrosine kinase |
| MYC | Avian myelocytomatosis viral oncogene homolog |
| CDK | Cyclin-dependent kinase |
| CCNE1 | Cyclin E1 |
| CCND2 | Recombinant human cyclin-D2 |
| PTEN | Phosphatase and tensin homolog deleted on chromosome ten |
| ADP | Adenosine diphosphate |
| PARP | Poly ADP-ribose polymerase |
| TP53 | Tumor protein p53 |
| RB1 | Retinoblastoma1 |
| PDX | Patient-derived xenograft |
| PDOX | Patient-derived orthotopic xenograft |
| ADR | Adriamycin |
| SCID | Server combined immune-deficiency |
| MEK | Mitogen-activated protein kinase kinase |
| MAPK | Mitogen-activated protein kinase |
| GPNMB | Glycoprotein non-metastatic melanoma protein B |
| CAR-T | Chimeric antigen receptor T |
| HER2 | Human epidermal growth factor receptor-2 |
| BsAb | Bispecific antibody |
References
- Gill, J.; Ahluwalia, M.K.; Geller, D.; Gorlick, R. New Targets and Approaches in Osteosarcoma. Pharmacol. Ther. 2012, 137, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, P.S.; Helman, L.J. New Horizons in the Treatment of Osteosarcoma. N. Engl. J. Med. 2021, 385, 2066–2076. [Google Scholar] [CrossRef] [PubMed]
- Kager, L.; Zoubek, A.; Pötschger, U.; Kastner, U.; Flege, S.; Kempf-Bielack, B.; Branscheid, D.; Kotz, R.; Salzer-Kuntschik, M.; Winkelmann, W.; et al. Primary Metastatic Osteosarcoma: Presentation and Outcome of Patients Treated on Neoadjuvant Cooperative Osteosarcoma Study Group Protocols. J. Clin. Oncol. 2003, 21, 2011–2018. [Google Scholar] [CrossRef] [PubMed]
- Bielack, S.S.; Kempf-Bielack, B.; Delling, G.; Exner, G.U.; Flege, S.; Helmke, K.; Winkler, K. Prognostic Factors in High-Grade Osteosarcoma of the Extremities or Trunk: An Analysis of 1,702 Patients Treated on Neoadjuvant Cooperative Osteosarcoma Study Group Protocols. J. Clin. Oncol. 2002, 20, 776–790. [Google Scholar] [CrossRef]
- Isakoff, M.S.; Bielack, S.S.; Meltzer, P.; Gorlick, R. Osteosarcoma: Current Treatment and a Collaborative Pathway to Success. J. Clin. Oncol. 2015, 33, 3029–3035. [Google Scholar] [CrossRef] [Green Version]
- Hattinger, C.; Patrizio, M.; Fantoni, L.; Casotti, C.; Riganti, C.; Serra, M. Drug Resistance in Osteosarcoma: Emerging Biomarkers, Therapeutic Targets and Treatment Strategies. Cancers 2021, 13, 2878. [Google Scholar] [CrossRef]
- Enneking, W.F.; Spanier, S.S.; Goodman, M.A. A System for the Surgical Staging of Musculoskeletal Sarcoma. Clin. Orthop. Relat. Res. 1980, 153, 106–120. [Google Scholar] [CrossRef]
- Enneking, W.F.; Maale, G.E. The Effect of Inadvertent Tumor Contamination of Wounds during the Surgical Resection of Musculoskeletal Neoplasms. Cancer 1988, 62, 1251–1256. [Google Scholar] [CrossRef]
- Cates, M.M.; Cates, J.M.M. Surgical Resection Margin Classifications for High-Grade Pleomorphic Soft Tissue Sarcomas of the Extremity or Trunk: Definitions of Adequate Resection Margins and Recommendations for Sampling Margins from Primary Resection Specimens. Mod. Pathol. 2019, 32, 1421–1433. [Google Scholar] [CrossRef]
- Jeys, L.M.; Thorne, C.J.; Parry, M.; Gaston, C.L.L.; Sumathi, V.P.; Grimer, R.J. A Novel System for the Surgical Staging of Primary High-grade Osteosarcoma: The Birmingham Classification. Clin. Orthop. Relat. Res. 2017, 475, 842–850. [Google Scholar] [CrossRef]
- Iwata, S.; Ishii, T.; Kawai, A.; Hiruma, T.; Yonemoto, T.; Kamoda, H.; Asano, N.; Takeyama, M. Prognostic Factors in Elderly Osteosarcoma Patients: A Multi-Institutional Retrospective Study of 86 Cases. Ann. Surg. Oncol. 2013, 21, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, T.E.; Cruz, A.; Binitie, O.; Cheong, D.; Letson, D.G. Do Surgical Margins Affect Local Recurrence and Survival in Extremity, Nonmetastatic, High-grade Osteosarcoma? Clin. Orthop. Relat. Res. 2015, 474, 677–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jauregui, J.J.; Nadarajah, V.; Munn, J.; Pivec, R.; Kapadia, B.H.; Lerman, D.M.; Maheshwari, A.V. Limb Salvage Versus Amputation in Conventional Appendicular Osteosarcoma: A Systematic Review. Indian J. Surg. Oncol. 2018, 9, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Odri, G.A.; Tchicaya-Bouanga, J.; Yoon, D.J.Y.; Modrowski, D. Metastatic Progression of Osteosarcomas: A Review of Current Knowledge of Environmental versus Oncogenic Drivers. Cancers 2022, 14, 360. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Huang, Z.; Wu, S.; Zang, X.; Liu, M.; Shi, J. Mir-33A Is Up-Regulated in Chemoresistant Osteosarcoma and Promotes Osteosarcoma Cell Resistance to Cisplatin by Down-Regulating TWIST. J. Exp. Clin. Cancer Res. 2014, 33, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gianferante, D.M.; Mirabello, L.; Savage, S.A. Germline and Somatic Genetics of Osteosarcoma—Connecting Aetiology, Biology and Therapy. Nat. Rev. Endocrinol. 2017, 13, 480–491. [Google Scholar] [CrossRef]
- Meyers, P.A. Systemic Therapy for Osteosarcoma and Ewing Sarcoma. Am. Soc. Clin. Oncol. Educ. Book 2015, 35, e644–e647. [Google Scholar] [CrossRef]
- Anninga, J.K.; Gelderblom, H.; Fiocco, M.; Kroep, J.R.; Taminiau, A.H.; Hogendoom, P.C.; Egeler, R.M. Chemotherapeutic Adjuvant Treatment for Osteosarcoma: Where Do We Stand? Eur. J. Cancer 2011, 47, 2431–2445. [Google Scholar] [CrossRef]
- Meyers, P.A.; Schwartz, C.L.; Krailo, M.; Kleinerman, E.S.; Betcher, D.; Bernstein, M.L.; Conrad, E.; Ferguson, W.; Gebhardt, M.; Goorin, A.M.; et al. Osteosarcoma: A Randomized, Prospective Trial of the Addition of Ifosfamide and/or Muramyl Tripeptide to Cisplatin, Doxorubicin, and High-Dose Methotrexate. J. Clin. Oncol. 2005, 23, 2004–2011. [Google Scholar] [CrossRef]
- Ferrari, S.; Ruggieri, P.; Cefalo, G.; Tamburini, A.; Capanna, R.; Fagioli, F.; Comandone, A.; Bertulli, R.; Bisogno, G.; Palmerini, E.; et al. Neoadjuvant Chemotherapy with Methotrexate, Cisplatin, and Doxorubicin with or without Ifosfamide in Nonmetastatic Osteosarcoma of the Extremity: An Italian Sarcoma Group Trial ISG/OS-1. J. Clin. Oncol. 2012, 30, 2112–2118. [Google Scholar] [CrossRef]
- Gaspar, N.; Occean, B.V.; Pacquement, H.; Bompas, E.; Bouvier, C.; Brisse, H.J.; Brugieres, L. Results of Methotrexate-Etoposide-Ifosfamide Based Regimen (M-EI) in Osteosarcoma Patients Included in the French OS2006/Sarcome-09 Study. Eur. J. Cancer 2018, 88, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Briccoli, A.; Rocca, M.; Salone, M.; Guzzardella, G.A.; Balladelli, A.; Bacci, G. High Grade Osteosarcoma of the Extremities Metastatic to the Lung: Long-Term Results in 323 Patients Treated Combining Surgery and Chemotherapy, 1985–2005. Surg. Oncol. 2010, 19, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Ballatori, S.E.; Hinds, P.W. Osteosarcoma: Prognosis Plateau Warrants Retinoblastoma Pathway Targeted Therapy. Signal Transduct. Target. Ther. 2016, 1, 16001. [Google Scholar] [CrossRef] [Green Version]
- Palmerini, E.; Jones, R.L.; Marchesi, E.; Paioli, A.; Cesari, M.; Longhi, A.; Meazza, C.; Coccoli, L.; Fagioli, F.; Asaftei, S.; et al. Gemcitabine and Docetaxel in Relapsed and Unresectable High-Grade Osteosarcoma and Spindle Cell Sarcoma of Bone. BMC Cancer 2016, 16, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Lagmay, J.P.; Krailo, M.D.; Dang, H.; Kim, A.; Hawkins, D.S.; Beaty III, O.; Janeway, K.A. Outcome of Patients with Recurrent Osteosarcoma Enrolled in Seven Phase II Trials Through Children’s Cancer Group, Pediatric Oncology Group, and Children’s Oncology Group: Learning From the Past to Move Forward. J. Clin. Oncol. 2016, 34, 3031–3038. [Google Scholar] [CrossRef] [PubMed]
- Arndt, C.A.; Koshkina, N.V.; Inwards, C.Y.; Hawkins, D.S.; Krailo, M.D.; Villaluna, D.; Anderson, P.M.; Goorin, A.M.; Blakely, M.L.; Bernstein, M.; et al. Inhaled Granulocyte-Macrophage Colony Stimulating Factor for First Pulmonary Recurrence of Osteosarcoma: Effects on Disease-Free Survival and Immunomodulation. A Report From the Children’s Oncology Group. Clin. Cancer Res. 2010, 16, 4024–4030. [Google Scholar] [CrossRef] [Green Version]
- Marina, N.M.; Smeland, S.; Bielack, S.S.; Bernstein, M.; Jovic, G.; Krailo, M.D.; Hook, J.M.; Arndt, C.; van den Berg, H.; Brennan, B.; et al. Comparison of MAPIE versus MAP in Patients with a Poor Response to Preoperative Chemotherapy for Newly Diagnosed High-Grade Osteosarcoma (EURAMOS-1): An Open-Label, International, Randomised Controlled Trial. Lancet Oncol. 2016, 17, 1396–1408. [Google Scholar] [CrossRef] [Green Version]
- Smrke, A.; Anderson, P.; Gulia, A.; Gennatas, S.; Huang, P.; Jones, R. Future Directions in the Treatment of Osteosarcoma. Cells 2021, 10, 172. [Google Scholar] [CrossRef]
- Lettieri, C.K.; Appel, N.; Labban, N.; Lussier, D.M.; Blattman, J.N.; Hingorani, P. Progress and Opportunities for Immune Therapeutics in Osteosarcoma. Immunotherapy 2016, 8, 1233–1244. [Google Scholar] [CrossRef]
- Wang, Z.; Li, B.; Ren, Y.; Ye, Z. T-Cell-Based Immunotherapy for Osteosarcoma: Challenges and Opportunities. Front. Immunol. 2016, 7, 353. [Google Scholar] [CrossRef]
- DeMaria, O.; Cornen, S.; Daëron, M.; Morel, Y.; Medzhitov, R.; Vivier, E. Harnessing Innate Immunity in Cancer Therapy. Nature 2019, 574, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Corrales, L.; Matson, V.; Flood, B.; Spranger, S.; Gajewski, T.F. Innate Immune Signaling and Regulation in Cancer Immunotherapy. Cell Res. 2016, 27, 96–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koirala, P.; Roth, M.E.; Gill, J.; Piperdi, S.; Chinai, J.M.; Geller, D.S.; Hoang, B.H.; Park, A.; Fremed, M.A.; Zang, X.; et al. Immune infiltration and PD-L1 Expression in the Tumor Microenvironment Are Prognostic in Osteosarcoma. Sci. Rep. 2016, 6, 30093. [Google Scholar] [CrossRef] [Green Version]
- Corre, I.; Verrecchia, F.; Crenn, V.; Redini, F.; Trichet, V. The Osteosarcoma Microenvironment: A Complex but Targetable Ecosystem. Cells 2020, 9, 976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, K.; Okamoto, M.; Sasaki, J.; Kuroda, C.; Ishida, H.; Ueda, K.; Ideta, H.; Kamanaka, T.; Sobajima, A.; Takizawa, T.; et al. Anti-PD-1 Antibody Decreases Tumour-Infiltrating Regulatory T cells. BMC Cancer 2020, 20, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wedekind, M.F.; Wagner, L.M.; Cripe, T.P. Immunotherapy for Osteosarcoma: Where Do We Go from Here? Pediatr. Blood Cancer 2018, 65, e27227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Naggar, A.M.; Clarkson, P.W.; Negri, G.L.; Turgu, B.; Zhang, F.; Anglesio, M.S.; Sorensen, P.H. HACE1 is a Potential Tumor Suppressor in Osteosarcoma. Cell Death Dis. 2019, 10, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Forrest, S.J.; Kinnaman, M.D.; Livingston, J.A.; Vo, K.T.; Merriam, P.; Clinton, C.; Desmith, K.; Cavanaugh, K.; Felicetti, B.; Smith, S.; et al. Phase II Trial of Olaparib in Combination with Ceralasertib in Patients with Recurrent Osteosarcoma. J. Clin. Oncol. 2021, 39, TPS11575. [Google Scholar] [CrossRef]
- Bousquet, M.; Noirot, C.; Accadbled, F.; de Gauzy, J.S.; Castex, M.; Brousset, P.; Gomez-Brouchet, A. Whole-Exome Sequencing in Osteosarcoma Reveals Important Heterogeneity of Genetic Alterations. Ann. Oncol. 2016, 27, 738–744. [Google Scholar] [CrossRef]
- Ho, X.D.; Phung, P.; Le, V.Q.; Nguyen, V.H.; Reimann, E.; Prans, E.; Kõks, G.; Maasalu, K.; Le, N.T.; Trinh, L.H.; et al. Whole Transcriptome Analysis Identifies Differentially Regulated Networks between Osteosarcoma and Normal Bone Samples. Exp. Biol. Med. 2017, 242, 1802–1811. [Google Scholar] [CrossRef]
- Joseph, C.G.; Hwang, H.; Jiao, Y.; Wood, L.D.; Kinde, I.; Wu, J.; Mandahl, N.; Luo, J.; Hruban, R.H.; Diaz, L.; et al. Exomic Analysis of Myxoid Liposarcomas, Synovial Sarcomas, and Osteosarcomas. Genes. Chromosom. Cancer 2013, 53, 15–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiezun, A.; Perry, J.; Tonzi, P.; Van Allen, E.; Carter, S.L.; Baca, S.; Bhatt, A.; Lawrence, M.; Walensky, L.; Wagle, N.; et al. Abstract A41: Complementary Genomic Approaches Highlight the PI3K/mTOR Pathway as a Common Vulnerability in Osteosarcoma. Cancer Res. 2014, 74, A41. [Google Scholar] [CrossRef]
- Behjati, S.; Tarpey, P.S.; Haase, K.; Ye, H.; Young, M.D.; Alexandrov, L.B.; Farndon, S.J.; Collord, G.; Wedge, D.C.; Martincorena, I.; et al. Recurrent Mutation of IGF Signalling Genes and Distinct Patterns of Genomic Rearrangement in Osteosarcoma. Nat. Commun. 2017, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, K.; Bakiri, L.; Wolff, L.I.; Linder, M.; Mikels-Vigdal, A.; Patiño-García, A.; Lecanda, F.; Hartmann, C.; Sibilia, M.; Wagner, E.F. Wnt Signaling and Loxl2 Promote Aggressive Osteosarcoma. Cell Res. 2020, 30, 885–901. [Google Scholar] [CrossRef]
- Feng, W.; Dean, D.C.; Hornicek, F.J.; Spentzos, D.; Hoffman, R.M.; Shi, H.; Duan, Z. Myc is a Prognostic Biomarker and Potential Therapeutic Target in Osteosarcoma. Ther. Adv. Med Oncol. 2020, 12, 1758835920922055. [Google Scholar] [CrossRef] [PubMed]
- Kovac, M.; Blattmann, C.; Ribi, S.; Smida, J.; Mueller, N.S.; Engert, F.; Castro-Giner, F.; Weischenfeldt, J.; Kovacova, M.; Krieg, A.; et al. Exome Sequencing of Osteosarcoma Reveals Mutation Signatures Reminiscent of Brca Deficiency. Nat. Commun. 2015, 6, 8940. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.; Liu, Y.; Liu, Y.; Alexandrov, L.B.; Edmonson, M.N.; Gawad, C.; Zhou, X.; Li, Y.; Rusch, M.C.; Easton, J.; et al. Pan-Cancer Genome and Transcriptome Analyses of 1699 Paediatric Leukaemias and Solid Tumours. Nature 2018, 555, 371–376. [Google Scholar] [CrossRef]
- Chen, X.; Bahrami, A.; Pappo, A.; Easton, J.; Dalton, J.; Hedlund, E.; Ellison, D.; Shurtleff, S.; Wu, G.; Wei, L.; et al. Recurrent Somatic Structural Variations Contribute to Tumorigenesis in Pediatric Osteosarcoma. Cell Rep. 2014, 7, 104–112. [Google Scholar] [CrossRef] [Green Version]
- Engeland, K. Cell Cycle Regulation: P53-P21-Rb Signaling. Cell Death Differ. 2022, 29, 946–960. [Google Scholar] [CrossRef]
- Lu, L.; Jin, W.; Wang, L.L. RECQ DNA Helicases and Osteosarcoma. Curr. Adv. Sci. Osteosarcoma 2020, 1258, 37–54. [Google Scholar]
- Mo, D.; Zhao, Y.; Balajee, A.S. Human RecQL4 Helicase Plays Multifaceted Roles in the Genomic Stability of Normal and Cancer Cells. Cancer Lett. 2017, 413, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mirabello, L.; Zhu, B.; Koster, R.; Karlins, E.; Dean, M.; Yeager, M.; Gianferante, M.; Spector, L.G.; Morton, L.M.; Karyadi, D.; et al. Frequency of Pathogenic Germline Variants in Cancer-Susceptibility Genes in Patients With Osteosarcoma. JAMA Oncol. 2020, 6, 724–734. [Google Scholar] [CrossRef]
- Rickel, K.; Fang, F.; Tao, J. Molecular Genetics of Osteosarcoma. Bone 2017, 102, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Farmer, H.; McCabe, N.; Lord, C.J.; Tutt, A.N.J.; Johnson, D.A.; Richardson, T.B.; Santarosa, M.; Dillon, K.J.; Hickson, I.; Knights, C.; et al. Targeting the DNA Repair Defect in BRCA Mutant Cells as a Therapeutic Strategy. Nature 2005, 434, 917–921. [Google Scholar] [CrossRef] [PubMed]
- Kohlmeyer, J.L.; Gordon, D.J.; Tanas, M.R.; Monga, V.; Dodd, R.D.; Quelle, D.E. CDKs in Sarcoma: Mediators of Disease and Emerging Therapeutic Targets. Int. J. Mol. Sci. 2020, 21, 3018. [Google Scholar] [CrossRef]
- Ragland, B.D.; Bell, W.C.; Lopez, R.R.; Siegal, G.P. Cytogenetics and Molecular Biology of Osteosarcoma. Lab. Investig. 2002, 82, 365–373. [Google Scholar] [CrossRef] [Green Version]
- Czarnecka, A.M.; Synoradzki, K.; Firlej, W.; Bartnik, E.; Sobczuk, P.; Fiedorowicz, M.; Grieb, P.; Rutkowski, P. Molecular Biology of Osteosarcoma. Cancers 2020, 12, 2130. [Google Scholar] [CrossRef]
- Carter, J.M.; Inwards, C.Y.; Jin, L.; Evers, B.; Wenger, D.E.; Oliveira, A.M.; Fritchie, K.J. Activating GNAS Mutations in Parosteal Osteosarcoma. Am. J. Surg. Pathol. 2014, 38, 402–409. [Google Scholar] [CrossRef]
- Jackson, S.P.; Bartek, J. The DNA-Damage Response in Human Biology and Disease. Nature 2009, 461, 1071–1078. [Google Scholar] [CrossRef] [Green Version]
- Geenen, J.J.J.; Schellens, J.H.M. Molecular Pathways: Targeting the Protein Kinase Wee1 in Cancer. Clin. Cancer Res. 2017, 23, 4540–4544. [Google Scholar] [CrossRef] [Green Version]
- Kolb, E.A.; Houghton, P.J.; Kurmasheva, R.T.; Mosse, Y.P.; Maris, J.M.; Erickson, S.W.; Guo, Y.; Teicher, B.A.; Smith, M.A.; Gorlick, R. Preclinical Evaluation of the Combination of AZD1775 and Irinotecan against Selected Pediatric Solid Tumors: A Pediatric Preclinical Testing Consortium report. Pediatr. Blood Cancer 2020, 67, e28098. [Google Scholar] [CrossRef] [PubMed]
- Matheson, C.J.; Backos, D.S.; Reigan, P. Targeting WEE1 Kinase in Cancer. Trends Pharmacol. Sci. 2016, 37, 872–881. [Google Scholar] [CrossRef] [PubMed]
- Gill, J.; Gorlick, R. Advancing Therapy for Osteosarcoma. Nat. Rev. Clin. Oncol. 2021, 18, 609–624. [Google Scholar] [CrossRef] [PubMed]
- Sayles, L.C.; Breese, M.R.; Koehne, A.L.; Leung, S.G.; Lee, A.G.; Liu, H.-Y.; Spillinger, A.; Shah, A.T.; Tanasa, B.; Straessler, K.; et al. Genome-Informed Targeted Therapy for Osteosarcoma. Cancer Discov. 2019, 9, 46–63. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Shen, J.K.; Yu, Z.; Hornicek, F.J.; Kan, Q.; Duan, Z. Expression and Therapeutic Implications of Cyclin-Dependent Kinase 4 (CDK4) in Osteosarcoma. Biochim. Biophys. Acta (BBA)—Mol. Basis Dis. 2018, 1864, 1573–1582. [Google Scholar] [CrossRef]
- Higuchi, T.; Sugisawa, N.; Miyake, K.; Oshiro, H.; Yamamoto, N.; Hayashi, K.; Kimura, H.; Miwa, S.; Igarashi, K.; Chawla, S.P.; et al. Sorafenib and Palbociclib Combination Regresses a Cisplatinum-Resistant Osteosarcoma in a PDOX Mouse Model. Anticancer Res. 2019, 39, 4079–4084. [Google Scholar] [CrossRef]
- Fu, W.; Sharma, S.S.; Ma, L.; Chu, B.; Bui, M.M.; Reed, D.; Pledger, W.J. Apoptosis of Osteosarcoma Cultures by the Combination of the Cyclin-Dependent Kinase Inhibitor SCH727965 and a Heat Shock Protein 90 Inhibitor. Cell Death Dis. 2013, 4, e566. [Google Scholar] [CrossRef]
- Tavanti, E.; Sero, V.; Vella, S.; Fanelli, M.; Michelacci, F.; Landuzzi, L.; Magagnoli, G.; Versteeg, R.; Picci, P.; Hattinger, C.; et al. Preclinical Validation of Aurora Kinases-Targeting Drugs in Osteosarcoma. Br. J. Cancer 2013, 109, 2607–2618. [Google Scholar] [CrossRef]
- Zhou, S.-F.; Niu, N.-K.; Wang, Z.-L.; Pan, S.-T.; Ding, H.-Q.; Au, G.H.T.; He, Z.-X.; Zhou, Z.-W.; Xiao, G.; Yang, Y.-X.; et al. Pro-Apoptotic and Pro-Autophagic Effects of the Aurora Kinase A Inhibitor Alisertib (MLN8237) on Human Osteosarcoma U-2 OS and MG-63 Cells through the Activation of Mitochondria-Mediated Pathway and Inhibition of p38 MAPK/PI3K/Akt/mTOR Signaling Pathway. Drug Des. Dev. Ther. 2015, 9, 1555–1584. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Z.; Jin, G.; Yao, K.; Liu, K.; Liu, F.; Chen, H.; Wang, K.; Gorja, D.R.; Reddy, K.; Bode, A.M.; et al. Aurora B Kinase as a Novel Molecular Target for Inhibition the Growth of Osteosarcoma. Mol. Carcinog. 2019, 58, 1056–1067. [Google Scholar] [CrossRef]
- Wu, C.-C.; Livingston, J.A. Genomics and the Immune Landscape of Osteosarcoma. Curr. Adv. Sci. Osteosarcoma 2020, 1258, 21–36. [Google Scholar] [CrossRef]
- Assi, T.; Watson, S.; Samra, B.; Rassy, E.; Le Cesne, A.; Italiano, A.; Mir, O. Targeting the VEGF Pathway in Osteosarcoma. Cells 2021, 10, 1240. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Yang, D.; Sun, Y.; Sun, B.; Wang, G.; Trent, J.C.; Araujo, D.M.; Chen, K.; Zhang, W. Genetic Amplification of the Vascular Endothelial Growth Factor (VEGF) Pathway Genes, Including VEGFA, in Human Osteosarcoma. Cancer 2011, 117, 4925–4938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, X.W.; Wu, T.Y.; Yi, X.; Ren, W.P.; Zhou, Z.B.; Sun, Y.Q.; Zhang, C.Q. Prognostic Significance of VEGF Expression in Osteosarcoma: A Meta-Analysis. Tumour Biol. 2014, 35, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Italiano, A.; Mir, O.; Mathoulin-Pelissier, S.; Penel, N.; Piperno-Neumann, S.; Bompas, E.; Chevreau, C.; Duffaud, F.; Entz-Werlé, N.; Saada, E.; et al. Cabozantinib in Patients with Advanced Ewing Sarcoma or Osteosarcoma (CABONE): A Multicentre, Single-Arm, Phase 2 Trial. Lancet Oncol. 2020, 21, 446–455. [Google Scholar] [CrossRef]
- Gaspar, N.; Casanova, M.; Sirvent, F.J.B.; Venkatramani, R.; Morland, B.; Gambart, M.; Thebaud, E.; Strauss, S.J.; Locatelli, F.; Melcon, S.G.; et al. Single-Agent Expansion Cohort of Lenvatinib (Len) and Combination Dose-Finding Cohort of LEN + Etoposide (ETP) + Ifosfamide (IFM) in Patients (pts) Aged 2 to ≤25 Years with Relapsed/Refractory Osteosarcoma (OS). J. Clin. Oncol. 2018, 36, 11527. [Google Scholar] [CrossRef]
- Gaspar, N.; Campbell-Hewson, Q.; Melcon, S.G.; Locatelli, F.; Venkatramani, R.; Hecker-Nolting, S.; Gambart, M.; Bautista, F.; Thebaud, E.; Aerts, I.; et al. Phase I/II Study of Single-Agent Lenvatinib in Children and Adolescents with Refractory or Relapsed Solid Malignancies and Young Adults with Osteosarcoma (ITCC-050)☆. ESMO Open 2021, 6, 100250. [Google Scholar] [CrossRef]
- Duffaud, F.; Mir, O.; Boudou-Rouquette, P.; Piperno-Neumann, S.; Penel, N.; Bompas, E.; Delcambre, C.; Kalbacher, E.; Italiano, A.; Collard, O.; et al. Efficacy and Safety of Regorafenib in Adult Patients with Metastatic Osteosarcoma: A Non-Comparative, Randomised, Double-Blind, Placebo-Controlled, Phase 2 Study. Lancet Oncol. 2018, 20, 120–133. [Google Scholar] [CrossRef]
- Davis, L.E.; Bolejack, V.; Ryan, C.W.; Ganjoo, K.N.; Loggers, E.T.; Chawla, S.; Agulnik, M.; Livingston, M.B.; Reed, D.; Keedy, V.; et al. Randomized Double-Blind Phase II Study of Regorafenib in Patients With Metastatic Osteosarcoma. J. Clin. Oncol. 2019, 37, 1424–1431. [Google Scholar] [CrossRef]
- Li, X.; Pontén, A.; Aase, K.; Karlsson, L.; Abramsson, A.; Uutela, M.; Bäckström, G.; Hellström, M.; Boström, H.; Li, H.; et al. PDGF-C Is a New Protease-Activated Ligand for the PDGF α-Receptor. Nat. Cell Biol. 2000, 2, 302–309. [Google Scholar] [CrossRef]
- LaRochelle, W.J.; Jeffers, M.; McDonald, W.F.; Chillakuru, R.A.; Giese, N.A.; Lokker, N.A.; Sullivan, C.; Boldog, F.L.; Yang, M.; Vernet, C.; et al. PDGF-D, a New Protease-Activated Growth Factor. Nat. Cell Biol. 2001, 3, 517–521. [Google Scholar] [CrossRef] [PubMed]
- Bartoschek, M.; Pietras, K. PDGF Family Function and Prognostic Value in Tumor Biology. Biochem. Biophys. Res. Commun. 2018, 503, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Heldin, C.-H.; Lennartsson, J.; Westermark, B. Involvement of Platelet-Derived Growth Factor Ligands and Receptors in Tumorigenesis. J. Intern. Med. 2018, 283, 16–44. [Google Scholar] [CrossRef] [Green Version]
- Kubo, T.; Bs, S.P.; Rosenblum, J.; Antonescu, C.R.; Chen, W.; Kim, H.-S.; Huvos, A.G.; Bs, R.S.; Meyers, P.A.; Healey, J.H.; et al. Platelet-Derived Growth Factor Receptor as a Prognostic Marker and a Therapeutic Target for Imatinib Mesylate Therapy in Osteosarcoma. Cancer 2008, 112, 2119–2129. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, I.; Melo-Alvim, C.; Lopes-Brás, R.; Esperança-Martins, M.; Costa, L. Osteosarcoma Pathogenesis Leads the Way to New Target Treatments. Int. J. Mol. Sci. 2021, 22, 813. [Google Scholar] [CrossRef]
- Yamaguchi, S.I.; Ueki, A.; Sugihara, E.; Onishi, N.; Yaguchi, T.; Kawakami, Y.; Horiuchi, K.; Morioka, H.; Matsumoto, M.; Nakamura, M.; et al. Synergistic Antiproliferative Effect of Imatinib and Adriamycin in Platelet-Derived Growth Factor Receptor-Expressing Osteosarcoma Cells. Cancer Sci. 2015, 106, 875–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadopoulos, N.; Lennartsson, J. The PDGF/PDGFR Pathway as a Drug Target. Mol. Asp. Med. 2018, 62, 75–88. [Google Scholar] [CrossRef] [PubMed]
- Shen, G.; Zheng, F.; Ren, D.; Du, F.; Dong, Q.; Wang, Z.; Zhao, F.; Ahmad, R.; Zhao, J. Anlotinib: A Novel Multi-Targeting Tyrosine Kinase Inhibitor in Clinical Development. J. Hematol. Oncol. 2018, 11, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Kumar, R.M.R.; Arlt, M.J.; Kuzmanov, A.; Born, W.; Fuchs, B. Sunitinib Malate (SU-11248) Reduces Tumour Burden and Lung Metastasis in an Intratibial Human Xenograft Osteosarcoma Mouse Model. Am. J. Cancer Res. 2015, 5, 2156. [Google Scholar] [CrossRef]
- McCarthy, T.L.; Centrella, M. Local IGF-I Expression and Bone Formation. Growth Horm. IGF Res. 2001, 11, 213–219. [Google Scholar] [CrossRef]
- Majidinia, M.; Sadeghpour, A.; Yousefi, B. The Roles of Signaling Pathways in Bone Repair and Regeneration. J. Cell. Physiol. 2018, 233, 2937–2948. [Google Scholar] [CrossRef] [PubMed]
- Mancarella, C.; Morrione, A.; Scotlandi, K. Unraveling the IGF System Interactome in Sarcomas Exploits Novel Therapeutic Options. Cells 2021, 10, 2075. [Google Scholar] [CrossRef]
- Tzanakakis, G.; Giatagana, E.-M.; Berdiaki, A.; Spyridaki, I.; Hida, K.; Neagu, M.; Tsatsakis, A.; Nikitovic, D. The Role of IGF/IGF-IR-Signaling and Extracellular Matrix Effectors in Bone Sarcoma Pathogenesis. Cancers 2021, 13, 2478. [Google Scholar] [CrossRef]
- Chmielowski, B. Insulin-Like Growth Factor 1 Receptor Inhibitors: Where Do We Come from? What Are We? Where Are We Going? Cancer 2014, 120, 2384–2387. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.H.; Leroith, D. Obesity, Type 2 Diabetes and Cancer: The Insulin and IGF Connection. Endocr.-Relat. Cancer 2012, 19, F27–F45. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Yee, D. Disrupting Insulin and IGF Receptor Function in Cancer. Int. J. Mol. Sci. 2021, 22, 555. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-H.; Han, X.-D.; Qiu, Y.; Xiong, J.; Yu, Y.; Wang, B.; Zhu, Z.-Z.; Qian, B.-P.; Chen, Y.-X.; Wang, S.-F.; et al. Increased Expression of Insulin-Like Growth Factor-1 Receptor is Correlated with Tumor Metastasis and Prognosis in Patients with Osteosarcoma. J. Surg. Oncol. 2011, 105, 235–243. [Google Scholar] [CrossRef]
- Morrow, J.J.; Bayles, I.; Funnell, A.P.W.; Miller, T.E.; Saiakhova, A.; Lizardo, M.M.; Bartels, C.F.; Kapteijn, M.Y.; Hung, S.; Mendoza, A.; et al. Positively Selected Enhancer Elements Endow Osteosarcoma Cells with Metastatic Competence. Nat. Med. 2018, 24, 176–185. [Google Scholar] [CrossRef]
- Goudarzi, A.; Gokgoz, N.; Gill, M.; Pinnaduwage, D.; Merico, D.; Wunder, J.S.; Andrulis, I.L. Protein Kinase C Epsilon and Genetic Networks in Osteosarcoma Metastasis. Cancers 2013, 5, 372–403. [Google Scholar] [CrossRef] [Green Version]
- Mansky, P.J.; Liewehr, D.J.; Steinberg, S.M.; Chrousos, G.P.; Avila, N.A.; Long, L.; Bernstein, D.; Mackall, C.L.; Hawkins, D.S.; Helman, L.J. Treatment of Metastatic Osteosarcoma With the Somatostatin Analog OncoLar: Significant Reduction of Insulin-Like Growth Factor-1 Serum Levels. J. Pediatr. Hematol. 2002, 24, 440–446. [Google Scholar] [CrossRef]
- Beck, O.; Paret, C.; Russo, A.; Burhenne, J.; Fresnais, M.; Steimel, K.; Seidmann, L.; Wagner, D.-C.; Vewinger, N.; Lehmann, N.; et al. Safety and Activity of the Combination of Ceritinib and Dasatinib in Osteosarcoma. Cancers 2020, 12, 793. [Google Scholar] [CrossRef] [PubMed]
- Pappo, A.S.; Vassal, G.; Crowley, J.J.; Bolejack, V.; Hogendoorn, P.C.; Chugh, R.; Ladanyi, M.; Grippo, J.F.; Dall, G.; Staddon, A.P.; et al. A Phase 2 Trial of R1507, a Monoclonal Antibody to the Insulin-Like Growth Factor-1 Receptor (IGF-1R), in Patients with Recurrent or Refractory Rhabdomyosarcoma, Osteosarcoma, Synovial Sarcoma, and Other Soft Tissue Sarcomas: Results of a Sarcoma Alliance for Research Through Collaboration study. Cancer 2014, 120, 2448–2456. [Google Scholar] [PubMed] [Green Version]
- Hattinger, C.M.; Pasello, M.; Ferrari, S.; Picci, P.; Serra, M. Emerging Drugs for High-Grade Osteosarcoma. Expert Opin. Emerg. Drugs 2010, 15, 615–634. [Google Scholar] [CrossRef]
- Chawla, S.P.; Staddon, A.P.; Baker, L.H.; Schuetze, S.M.; Tolcher, A.W.; D’Amato, G.Z.; Blay, J.-Y.; Mita, M.M.; Sankhala, K.K.; Berk, L.; et al. Phase II Study of the Mammalian Target of Rapamycin Inhibitor Ridaforolimus in Patients With Advanced Bone and Soft Tissue Sarcomas. J. Clin. Oncol. 2012, 30, 78–84, Coriggendum in 2017, 35, 2722. [Google Scholar] [CrossRef] [PubMed]
- Gazitt, Y.; Kolaparthi, V.; Moncada, K.; Thomas, C.; Freeman, J. Targeted Therapy of Human Osteosarcoma with 17AAG or Rapamycin: Characterization of Induced Apoptosis and Inhibition of mTOR and Akt/MAPK/Wnt Pathways. Int. J. Oncol. 1992, 34, 551–561. [Google Scholar] [CrossRef] [Green Version]
- Ding, L.; Congwei, L.; Bei, Q.; Tao, Y.; Ruiguo, W.; Heze, Y.; Bo, D.; Zhihong, L. Mtor: An Attractive Therapeutic Target for Osteosarcoma? Oncotarget 2016, 7, 50805–50813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gobin, B.; Battaglia, S.; Lanel, R.; Chesneau, J.; Amiaud, J.; Rédini, F.; Ory, B.; Heymann, D. NVP-BEZ235, a Dual PI3K/mTOR Inhibitor, Inhibits Osteosarcoma Cell Proliferation and Tumor Development in Vivo with an Improved Survival Rate. Cancer Lett. 2014, 344, 291–298. [Google Scholar] [CrossRef]
- Zhu, Y.-R.; Min, H.; Fang, J.-F.; Zhou, F.; Deng, X.-W.; Zhang, Y.-Q. Activity of the Novel Dual Phosphatidylinositol 3-Kinase/Mammalian Target of Rapamycin Inhibitor NVP-BEZ235 against Osteosarcoma. Cancer Biol. Ther. 2015, 16, 602–609. [Google Scholar] [CrossRef] [Green Version]
- Bavelloni, A.; Focaccia, E.; Piazzi, M.; Orsini, A.; Ramazzotti, G.; Cocco, L.; Blalock, W.; Faenza, I. Therapeutic Potential of Nvp-bkm120 in Human Osteosarcomas Cells. J. Cell. Physiol. 2018, 234, 10907–10917. [Google Scholar] [CrossRef]
- Yu, W.-X.; Lu, C.; Wang, B.; Ren, X.-Y.; Xu, K. Effects of Rapamycin on Osteosarcoma Cell Proliferation and Apoptosis by Inducing Autophagy. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 915–921. [Google Scholar]
- Oshiro, H.; Tome, Y.; Miyake, K.; Higuchi, T.; Sugisawa, N.; Kanaya, F.; Nishida, K.; Hoffman, R.M. An mTOR and VEGFR Inhibitor Combination Arrests a Doxorubicin Resistant Lung Metastatic Osteosarcoma in a PDOX Mouse Model. Sci. Rep. 2021, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Tang, F.; Min, L.; Hornicek, F.; Duan, Z.; Tu, C. PTEN in Osteosarcoma: Recent Advances and the Therapeutic Potential. Biochim. Biophys. Acta 2020, 1874, 188405. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Shen, X.; Ma, M.; Liu, W.; Yang, W.; Wang, P.; Cai, Z.; Mi, R.; Lu, Y.; Zhuang, J.; et al. ZIP10 Drives Osteosarcoma Proliferation and Chemoresistance through ITGA10-Mediated Activation of the PI3K/AKT Pathway. J. Exp. Clin. Cancer Res. 2021, 40, 1–16. [Google Scholar] [CrossRef]
- Dang, C.V.; O’Donnell, K.A.; Zeller, K.I.; Nguyen, T.; Osthus, R.C.; Li, F. The C-Myc Target Gene Network. Semin. Cancer Biol. 2006, 16, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Dhanasekaran, R.; Deutzmann, A.; Mahauad-Fernandez, W.D.; Hansen, A.S.; Gouw, A.M.; Felsher, D.W. The MYC Oncogene—The Grand Orchestrator of Cancer Growth and Immune Evasion. Nat. Rev. Clin. Oncol. 2021, 19, 23–36. [Google Scholar] [CrossRef]
- Dong, Y.; Tu, R.; Liu, H.; Qing, G. Regulation of Cancer Cell Metabolism: Oncogenic MYC in the Driver’s Seat. Signal Transduct. Target. Ther. 2020, 5, 1–11. [Google Scholar] [CrossRef]
- Dang, C.V. MYC on the Path to Cancer. Cell 2012, 149, 22–35. [Google Scholar] [CrossRef] [Green Version]
- Baluapuri, A.; Wolf, E.; Eilers, M. Target Gene-Independent Functions of MYC Oncoproteins. Nat. Rev. Mol. Cell Biol. 2020, 21, 255–267. [Google Scholar] [CrossRef]
- Han, G.; Wang, Y.; Bi, W. C-Myc Overexpression Promotes Osteosarcoma Cell Invasion via Activation of MEK-ERK Pathway. Oncol. Res. Featur. Preclin. Clin. Cancer Ther. 2012, 20, 149–156. [Google Scholar] [CrossRef]
- Chen, D.; Zhao, Z.; Huang, Z.; Chen, D.C.; Zhu, X.X.; Wang, Y.Z.; Yan, Y.W.; Tang, S.; Madhavan, S.; Ni, W.; et al. Super enhancer inhibitors suppress MYC driven transcriptional amplification and tumor progression in osteosarcoma. Bone Res. 2018, 6, 11. [Google Scholar] [CrossRef]
- Lee, D.H.; Qi, J.; Bradner, J.E.; Said, J.W.; Doan, N.B.; Forscher, C.; Yang, H.; Koeffler, H.P. Synergistic Effect of JQ1 and Rapamycin for Treatment of Human Osteosarcoma. Int. J. Cancer 2014, 136, 2055–2064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth, M.; Barris, D.M.; Piperdi, S.; Kuo, V.; Everts, S.; Geller, D.; Houghton, P.; Kolb, E.A.; Hawthorne, T.; Gill, J.; et al. Targeting Glycoprotein NMB with Antibody-Drug Conjugate, Glembatumumab Vedotin, for the Treatment of Osteosarcoma. Pediatr. Blood Cancer 2015, 63, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, Q.; Chen, W.; Shan, B.; Ding, Y.; Zhang, G.; Cao, N.; Liu, L.; Zhang, Y. B7-H3 is Overexpressed in Patients Suffering Osteosarcoma and Associated with Tumor Aggressiveness and Metastasis. PLoS ONE 2013, 8, e70689. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Dean, D.; Wei, R.; Hornicek, F.J.; Ulmert, D.; Duan, Z. Expression and Clinical Implications of Leucine-Rich Repeat Containing 15 (LRRC15) in Osteosarcoma. J. Orthop. Res. 2020, 38, 2362–2372. [Google Scholar] [CrossRef] [PubMed]
- Kopp, L.M.; Malempati, S.; Krailo, M.; Gao, Y.; Buxton, A.; Weigel, B.J.; Hawthorne, T.; Crowley, E.; Moscow, J.A.; Hawthorne, T.; et al. Phase II Trial of the Glycoprotein Non-Metastatic B-Targeted Antibody-Drug Conjugate, Glembatumumab Vedotin (CDX-011), in Recurrent Osteosarcoma AOST1521: A Report from the Children’s Oncology Group. Eur. J. Cancer 2019, 121, 177–183. [Google Scholar] [CrossRef]
- Hingorani, P.; Roth, M.E.; Wang, Y.; Zhang, W.; Gill, J.B.; Harrison, D.J.; Teicher, B.; Erickson, S.; Gatto, G.; Smith, M.A.; et al. ABBV-085, Antibody–Drug Conjugate Targeting LRRC15, Is Effective in Osteosarcoma: A Report by the Pediatric Preclinical Testing Consortium. Mol. Cancer Ther. 2021, 20, 535–540. [Google Scholar] [CrossRef]
- Park, J.A.; Cheung, N.-K.V. GD2 or HER2 Targeting T Cell Engaging Bispecific Antibodies to Treat Osteosarcoma. J. Hematol. Oncol. 2020, 13, 1–16. [Google Scholar] [CrossRef]
- Agostinis, P.; Berg, K.; Cengel, K.A.; Foster, T.H.; Girotti, A.W.; Gollnick, S.O.; Hahn, S.M.; Hamblin, M.R.; Juzeniene, A.; Kessel, D.; et al. Photodynamic Therapy of Cancer: An Update. CA Cancer J. Clin. 2011, 61, 250–281. [Google Scholar] [CrossRef]
- Nakamura, T.; Kusuzaki, K.; Matsubara, T.; Matsumine, A.; Murata, H.; Uchida, A. A New Limb Salvage Surgery in Cases of High-Grade Soft Tissue Sarcoma Using Photodynamic Surgery, Followed by Photo and Radiodynamic Therapy with Acridine Orange. J. Surg. Oncol. 2008, 97, 523–528. [Google Scholar] [CrossRef]
- Yu, W.; Zhu, J.; Wang, Y.; Wang, J.; Fang, W.; Xia, K.; Shao, J.; Wu, M.; Liu, B.; Liang, C.; et al. A Review and Outlook in the Treatment of Osteosarcoma and Other Deep Tumors with Photodynamic Therapy: From Basic to Deep. Oncotarget 2017, 8, 39833–39848. [Google Scholar] [CrossRef] [Green Version]
- Tan, G.; Xu, J.; Yu, Q.; Yang, Z.; Zhang, H. The Safety and Efficiency of Photodynamic Therapy for the Treatment of Osteosarcoma: A Systematic Review of in Vitro Experiment and Animal Model Reports. Photodiagnosis Photodyn. Ther. 2022, 40, 103093. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.; Zhao, L.; Yang, Z.; Liu, Z.; Gu, J.; Bai, B.; Liu, J.; Xu, J.; Yang, H. Mechanisms of Oxidative Stress, Apoptosis, and Autophagy Involved in Graphene Oxide Nanomaterial Anti-Osteosarcoma Effect. Int. J. Nanomed. 2018, 13, 2907–2919. [Google Scholar] [CrossRef] [PubMed]
- Barani, M.; Mukhtar, M.; Rahdar, A.; Sargazi, S.; Pandey, S.; Kang, M. Recent Advances in Nanotechnology-Based Diagnosis and Treatments of Human Osteosarcoma. Biosensors 2021, 11, 55. [Google Scholar] [CrossRef] [PubMed]
- Yao, M.; Ma, L.; Li, L.; Zhang, J.; Lim, R.X.; Chen, W.; Zhang, Y. A New Modality for Cancer Treatment—Nanoparticle Mediated Microwave Induced Photodynamic Therapy. J. Biomed. Nanotechnol. 2016, 12, 1835–1851. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Ye, M.; Zhu, J.; Wang, Y.; Liang, C.; Tang, J.; Tao, H.; Shen, Y. Zinc Phthalocyanine Encapsulated in Polymer Micelles as a Potent Photosensitizer for the Photodynamic Therapy of Osteosarcoma. Nanomed. Nanotechnol. Biol. Med. 2018, 14, 1099–1110. [Google Scholar] [CrossRef]
- Gao, Z.; Zhang, L.; Hu, J.; Sun, Y. Mesenchymal Stem Cells: A Potential Targeted-Delivery Vehicle for Anti-Cancer Drug Loaded Nanoparticles. Nanomed. Nanotechnol. Biol. Med. 2013, 9, 174–184. [Google Scholar] [CrossRef]
- Layek, B.; Sadhukha, T.; Panyam, J.; Prabha, S. Nano-Engineered Mesenchymal Stem Cells Increase Therapeutic Efficacy of Anticancer Drug Through True Active Tumor Targeting. Mol. Cancer Ther. 2018, 17, 1196–1206. [Google Scholar] [CrossRef] [Green Version]
- Lenna, S.; Bellotti, C.; Duchi, S.; Martella, E.; Columbaro, M.; Dozza, B.; Ballestri, M.; Guerrini, A.; Sotgiu, G.; Frisoni, T.; et al. Mesenchymal Stromal Cells Mediated Delivery of Photoactive Nanoparticles Inhibits Osteosarcoma Growth in Vitro and in a Murine in Vivo Ectopic Model. J. Exp. Clin. Cancer Res. 2020, 39, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Martin, J.W.; Squire, J.; Zielenska, M. The Genetics of Osteosarcoma. Sarcoma 2012, 2012, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Li, F.P.; Fraumeni, J.F. Soft-Tissue Sarcomas, Breast Cancer, and Other Neoplasms. A Familial Syndrome? Ann. Intern. Med. 1969, 71, 747–752. [Google Scholar] [CrossRef] [Green Version]
- Moukengue, B.; Lallier, M.; Marchandet, L.; Baud’Huin, M.; Verrecchia, F.; Ory, B.; Lamoureux, F. Origin and Therapies of Osteosarcoma. Cancers 2022, 14, 3503. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Li, Y.; Hu, C.; Chen, Y.; Chen, Z.; Chen, Z.S.; Zhang, J.Y.; Fang, S. CDK6-PI3K Signaling Axis is an Efficient Target for Attenuating ABCB1/P-Gp Mediated Multi-Drug Resistance (MDR) in Cancer Cells. Mol. Cancer 2022, 21, 103. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, S.; Pothuraju, R.; Rachagani, S.; Siddiqui, J.A.; Atri, P.; Mallya, K.; Nasser, M.W.; Sayed, Z.; Lyden, E.R.; Smith, L.; et al. Dual Blockade of EGFR and CDK4/6 Delays Head and Neck Squamous Cell Carcinoma Progression by Inducing Metabolic Rewiring. Cancer Lett. 2021, 510, 79–92. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.-Y.; Liu, J.-B.; Wang, X.-F.; Ma, Y.-S.; Fu, D. Current Status and Prospects of Clinical Treatment of Osteosarcoma. Technol. Cancer Res. Treat. 2022, 21, 15330338221124696. [Google Scholar] [CrossRef]
- Xie, D.; Wang, Z.; Li, J.; Guo, D.-A.; Lu, A.; Liang, C. Targeted Delivery of Chemotherapeutic Agents for Osteosarcoma Treatment. Front. Oncol. 2022, 12, 643. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Classification | Sensitivity | Negative Predictive Value | Preoperative Planning Instructions |
|---|---|---|---|
| AJCCR | Generally | Usually | None |
| MSTS | Very | Better | Include |
| Signaling Pathway | Genes | References |
|---|---|---|
| PI3K-mTOR | EGFR, GNAQ, ALK, PDGFRA, PDGFRB, CBL, PIK3CA, PIK3R1, PDPK1, AKT1, AKT2, E1F4B, PTEN, TSC2 | [42,53] |
| DNA damage control | WRN, ATM, CDKN2A, TP53, BRCA1, BRCA2, MLH1, BAP1 | [46,53,54] |
| RAS | EGFR, GNAQ, ALK, PDGFRA, PDGFRB, CBL, NF1 | [53] |
| Cell cycle/apoptosis | CDK4, MDM2, MYC, CARD11, CTNND1, BLM, CCNE1, COPS3, PRKCA, TWIST1, TP53, CDKN2A | [55,56,57] |
| TGF | GNAS, EP300 | [53,58] |
| Action Pathway | Drugs | Target of Action | References |
|---|---|---|---|
| DNA damage repair and cell cycle | AZD1775 Palbociclib Dinaciclib Alisertib AZD1152 HOI-07 | WEE1 inhibitor CDK4/6 inhibitors multi-CDK inhibitors AURKA inhibitor AURKB inhibitor | [61] [65] [67] [69] [70] [70] |
| VEGF and PDGF | Sorafenib Cabozantinib Lenvatinib Regorafenib Anlotinib Sunitinib | VEGFR inhibitors VEGFR and PDGFR inhibitors | [66] [75] [76,77] [78] [88] [89] |
| IGF | R1507 | IGF-1R inhibitor | [101] |
| PI3K/mTOR | Buparlisib Rapamycin Everolimus | PI3K inhibitor mTOR inhibitors | [109] [110] [109,111] |
| MYC | THZ1 JQ1 | MYC super-enhancer inhibitors | [120] [121] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, Z.; Wen, S.; Huo, Z.; Wang, Q.; Zhao, J.; Wang, Z.; Chen, Y.; Zhang, L.; Zhou, F.; Guo, Z.; et al. Current Status and Prospects of Targeted Therapy for Osteosarcoma. Cells 2022, 11, 3507. https://doi.org/10.3390/cells11213507
Hu Z, Wen S, Huo Z, Wang Q, Zhao J, Wang Z, Chen Y, Zhang L, Zhou F, Guo Z, et al. Current Status and Prospects of Targeted Therapy for Osteosarcoma. Cells. 2022; 11(21):3507. https://doi.org/10.3390/cells11213507
Chicago/Turabian StyleHu, Zunguo, Shuang Wen, Zijun Huo, Qing Wang, Jiantao Zhao, Zihao Wang, Yanchun Chen, Lingyun Zhang, Fenghua Zhou, Zhangyu Guo, and et al. 2022. "Current Status and Prospects of Targeted Therapy for Osteosarcoma" Cells 11, no. 21: 3507. https://doi.org/10.3390/cells11213507