
Correlation between Neutrophil Extracellular Traps (NETs) Expression and Primary Graft Dysfunction Following Human Lung Transplantation

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Quantification of Circulating NETs and Biomarkers
2.4. Lung Histology, Immunohistology and Confocal Imaging
2.5. Statistics
3. Results
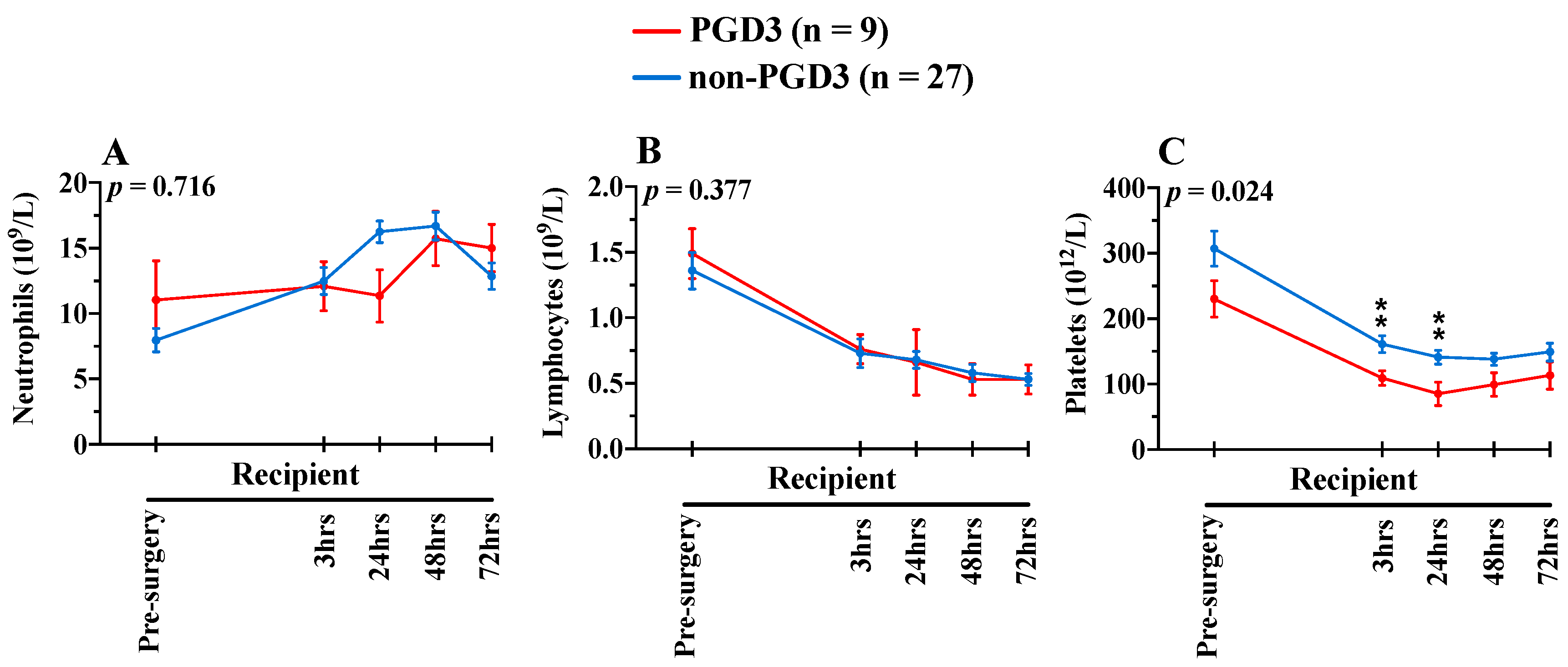
3.1. Clinical Results
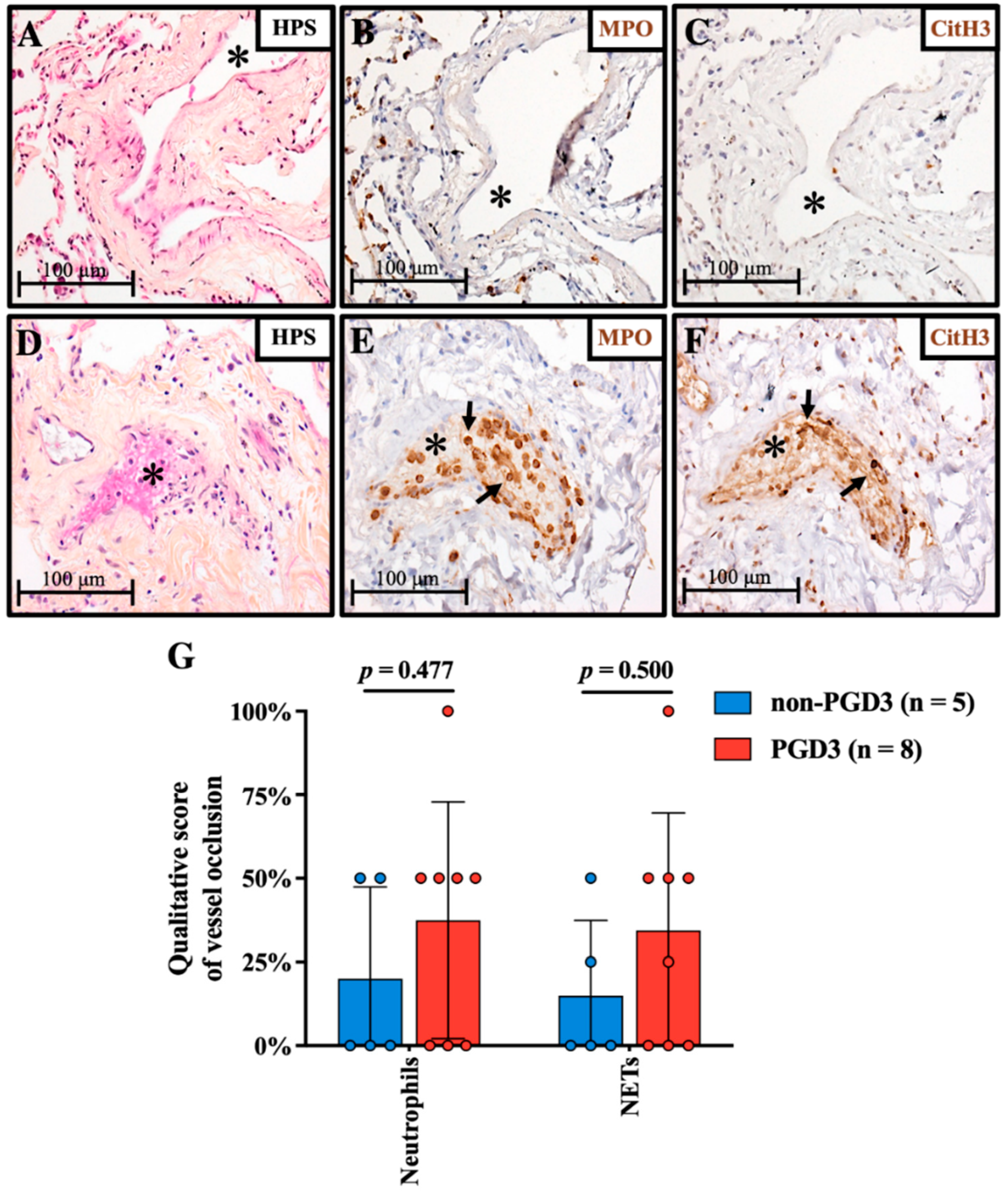
3.2. NETs-Mediated Vascular Occlusion in Grafts
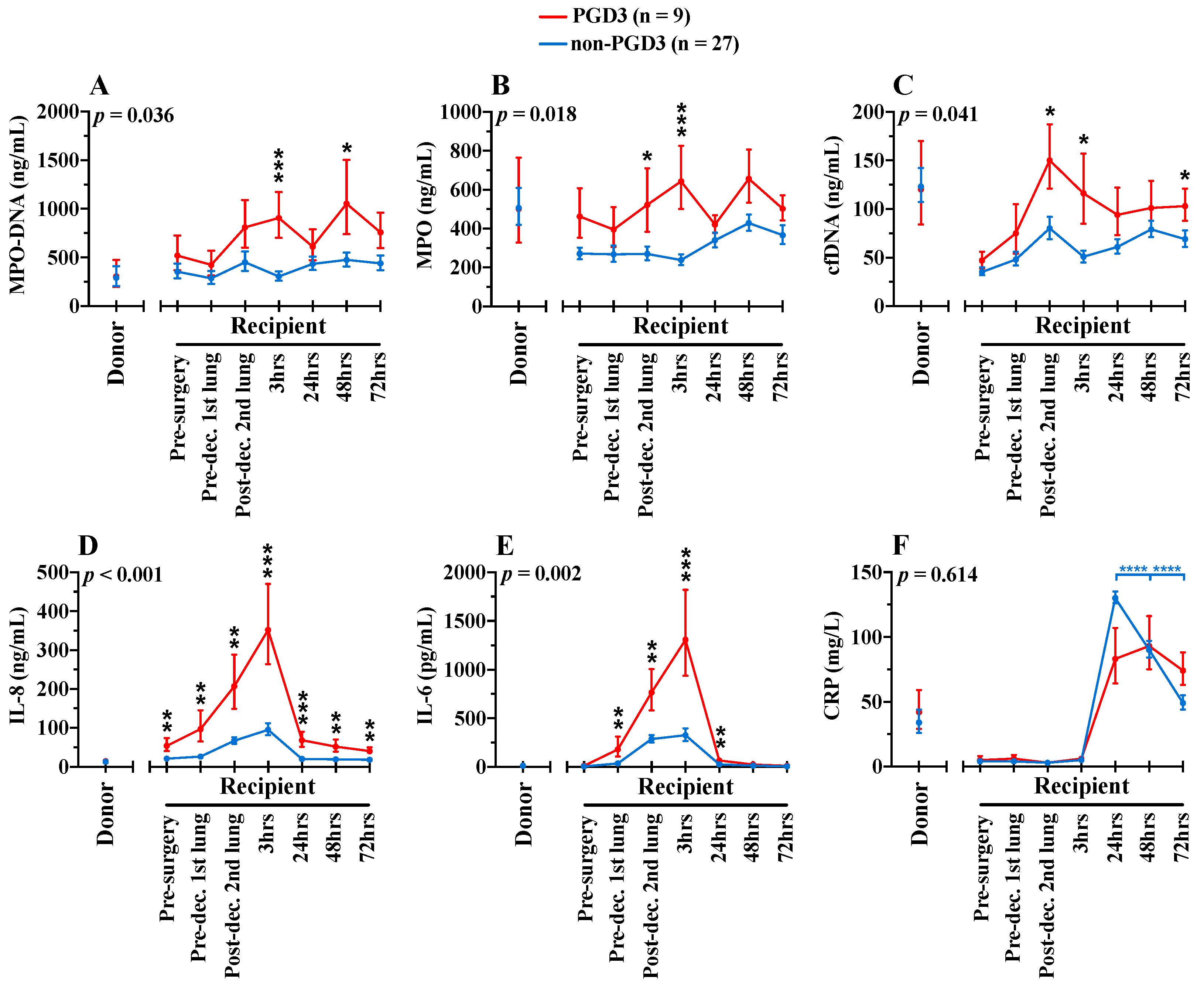
3.3. Circulating NETs Are Associated with PGD3
3.4. NETosis-Related Inflammation Is Associated with PGD3
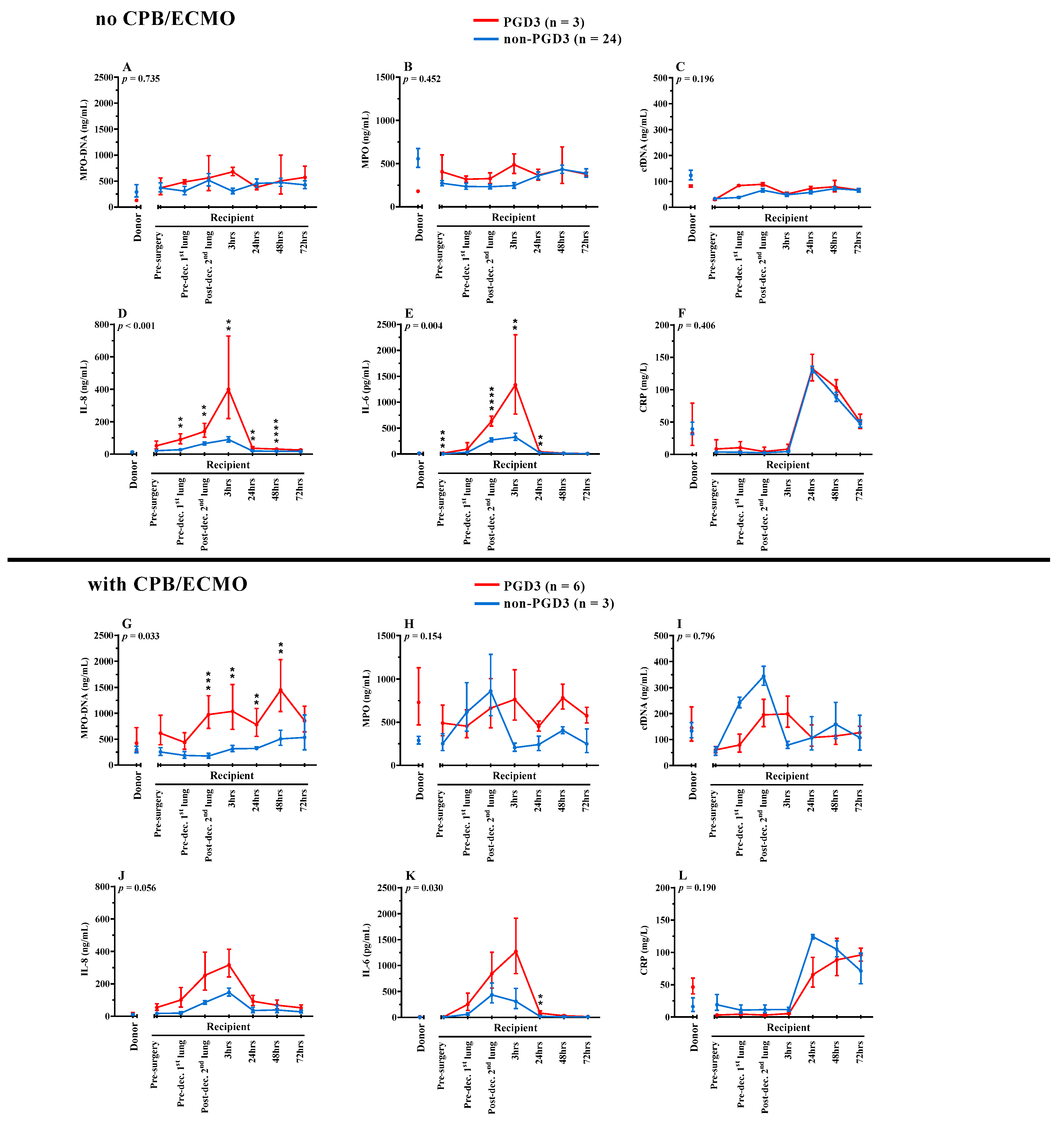
3.5. Impact of Identified Risk Factors on NETosis
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yeung, J.C.; Keshavjee, S. Overview of clinical lung transplantation. Cold Spring Harb. Perspect. Med. 2014, 4, a015628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snell, G.I.; Yusen, R.D.; Weill, D.; Strueber, M.; Garrity, E.; Reed, A.; Pelaez, A.; Whelan, T.P.; Perch, M.; Bag, R.; et al. Report of the ISHLT Working Group on Primary Lung Graft Dysfunction, part I: Definition and grading-A 2016 Consensus Group statement of the International Society for Heart and Lung Transplantation. J. Heart Lung Transplant. 2017, 36, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Meyer, K.C. Recent advances in lung transplantation. F1000Research 2018, 7, F1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porteous, M.K.; Diamond, J.M.; Christie, J.D. Primary graft dysfunction: Lessons learned about the first 72 h after lung transplantation. Curr. Opin. Organ Transplant. 2015, 20, 506–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diamond, J.M.; Lee, J.C.; Kawut, S.M.; Shah, R.J.; Localio, A.R.; Bellamy, S.L.; Lederer, D.J.; Cantu, E.; Kohl, B.A.; Lama, V.N.; et al. Clinical risk factors for primary graft dysfunction after lung transplantation. Am. J. Respir. Crit. Care Med. 2013, 187, 527–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreisel, D.; Krupnick, A.S.; Puri, V.; Guthrie, T.J.; Trulock, E.P.; Meyers, B.F.; Patterson, G.A. Short- and long-term outcomes of 1000 adult lung transplant recipients at a single center. J. Thorac. Cardiovasc. Surg. 2011, 141, 215–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantu, E.; Diamond, J.M.; Suzuki, Y.; Lasky, J.; Schaufler, C.; Lim, B.; Shah, R.; Porteous, M.; Lederer, D.J.; Kawut, S.M.; et al. Quantitative Evidence for Revising the Definition of Primary Graft Dysfunction after Lung Transplant. Am. J. Respir. Crit. Care Med. 2018, 197, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Christie, J.D.; Bellamy, S.; Ware, L.B.; Lederer, D.; Hadjiliadis, D.; Lee, J.; Robinson, N.; Localio, A.R.; Wille, K.; Lama, V.; et al. Construct validity of the definition of primary graft dysfunction after lung transplantation. J. Heart Lung Transplant. 2010, 29, 1231–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talaie, T.; DiChiacchio, L.; Prasad, N.K.; Pasrija, C.; Julliard, W.; Kaczorowski, D.J.; Zhao, Y.; Lau, C.L. Ischemia-reperfusion Injury in the Transplanted Lung: A Literature Review. Transplant. Direct. 2021, 7, e652. [Google Scholar] [CrossRef] [PubMed]
- Sayah, D.M.; Mallavia, B.; Liu, F.; Ortiz-Munoz, G.; Caudrillier, A.; DerHovanessian, A.; Ross, D.J.; Lynch, J.P., 3rd; Saggar, R.; Ardehali, A.; et al. Neutrophil extracellular traps are pathogenic in primary graft dysfunction after lung transplantation. Am. J. Respir. Crit. Care Med. 2015, 191, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Mayadas, T.N.; Tsokos, G.C.; Tsuboi, N. Mechanisms of immune complex-mediated neutrophil recruitment and tissue injury. Circulation 2009, 120, 2012–2024. [Google Scholar] [CrossRef] [Green Version]
- Segerer, S.; Henger, A.; Schmid, H.; Kretzler, M.; Draganovici, D.; Brandt, U.; Noessner, E.; Nelson, P.J.; Kerjaschki, D.; Schlondorff, D.; et al. Expression of the chemokine receptor CXCR1 in human glomerular diseases. Kidney Int. 2006, 69, 1765–1773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Packard, R.R.; Lichtman, A.H.; Libby, P. Innate and adaptive immunity in atherosclerosis. Semin. Immunopathol. 2009, 31, 5–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soehnlein, O.; Steffens, S.; Hidalgo, A.; Weber, C. Neutrophils as protagonists and targets in chronic inflammation. Nat. Rev. Immunol. 2017, 17, 248–261. [Google Scholar] [CrossRef]
- Bharat, A.; Kreisel, D. Immunopathogenesis of Primary Graft Dysfunction after Lung Transplantation. Ann. Thorac. Surg. 2018, 105, 671–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capucetti, A.; Albano, F.; Bonecchi, R. Multiple Roles for Chemokines in Neutrophil Biology. Front. Immunol. 2020, 11, 1259. [Google Scholar] [CrossRef] [PubMed]
- den Hengst, W.A.; Gielis, J.F.; Lin, J.Y.; Van Schil, P.E.; De Windt, L.J.; Moens, A.L. Lung ischemia-reperfusion injury: A molecular and clinical view on a complex pathophysiological process. Am. J. Physiol. Heart Circ. Physiol. 2010, 299, H1283–H1299. [Google Scholar] [CrossRef] [Green Version]
- Kuhnle, G.E.; Reichenspurner, H.; Lange, T.; Wagner, F.; Groh, J.; Messmer, K.; Goetz, A.E. Microhemodynamics and leukocyte sequestration after pulmonary ischemia and reperfusion in rabbits. J. Thorac. Cardiovasc. Surg. 1998, 115, 937–944. [Google Scholar] [CrossRef] [Green Version]
- de Perrot, M.; Bonser, R.S.; Dark, J.; Kelly, R.F.; McGiffin, D.; Menza, R.; Pajaro, O.; Schueler, S.; Verleden, G.M.; Dysfunction, I.W.G.o.P.L.G. Report of the ISHLT Working Group on Primary Lung Graft Dysfunction part III: Donor-related risk factors and markers. J. Heart Lung Transplant. 2005, 24, 1460–1467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bittner, H.B.; Kendall, S.W.; Chen, E.P.; Craig, D.; Van Trigt, P. The effects of brain death on cardiopulmonary hemodynamics and pulmonary blood flow characteristics. Chest 1995, 108, 1358–1363. [Google Scholar] [CrossRef] [PubMed]
- Mathur, A.; Baz, M.; Staples, E.D.; Bonnell, M.; Speckman, J.M.; Hess, P.J., Jr.; Klodell, C.T.; Knauf, D.G.; Moldawer, L.L.; Beaver, T.M. Cytokine profile after lung transplantation: Correlation with allograft injury. Ann. Thorac. Surg. 2006, 81, 1844–1849. [Google Scholar] [CrossRef] [PubMed]
- Moreno, I.; Vicente, R.; Ramos, F.; Vicente, J.L.; Barbera, M. Determination of interleukin-6 in lung transplantation: Association with primary graft dysfunction. Transplant. Proc. 2007, 39, 2425–2426. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.G.; Lee, M.T.; Weiss, E.S.; Arnaoutakis, G.J.; Shah, A.S.; Detrick, B. Preoperative recipient cytokine levels are associated with early lung allograft dysfunction. Ann. Thorac. Surg. 2012, 93, 1843–1849. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.J.; Donnelly, S.C.; Hirani, N.; Haslett, C.; Strieter, R.M.; Dark, J.H.; Corris, P.A. Elevated levels of interleukin-8 in donor lungs is associated with early graft failure after lung transplantation. Am. J. Respir. Crit. Care Med. 2001, 163, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Perrot, M.; Sekine, Y.; Fischer, S.; Waddell, T.K.; McRae, K.; Liu, M.; Wigle, D.A.; Keshavjee, S. Interleukin-8 release during early reperfusion predicts graft function in human lung transplantation. Am. J. Respir. Crit. Care Med. 2002, 165, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Brinkmann, V.; Reichard, U.; Goosmann, C.; Fauler, B.; Uhlemann, Y.; Weiss, D.S.; Weinrauch, Y.; Zychlinsky, A. Neutrophil extracellular traps kill bacteria. Science 2004, 303, 1532–1535. [Google Scholar] [CrossRef] [PubMed]
- Caldarone, L.; Mariscal, A.; Sage, A.; Khan, M.; Juvet, S.; Martinu, T.; Zamel, R.; Cypel, M.; Liu, M.; Palaniyar, N.; et al. Neutrophil extracellular traps in ex vivo lung perfusion perfusate predict the clinical outcome of lung transplant recipients. Eur. Respir. J. 2019, 53, 1801736. [Google Scholar] [CrossRef]
- Oto, T.; Levvey, B.J.; Snell, G.I. Potential refinements of the International Society for Heart and Lung Transplantation primary graft dysfunction grading system. J. Heart Lung Transplant. 2007, 26, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Prekker, M.E.; Nath, D.S.; Walker, A.R.; Johnson, A.C.; Hertz, M.I.; Herrington, C.S.; Radosevich, D.M.; Dahlberg, P.S. Validation of the proposed International Society for Heart and Lung Transplantation grading system for primary graft dysfunction after lung transplantation. J. Heart Lung Transplant. 2006, 25, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Sommer, W.; Tudorache, I.; Kuhn, C.; Avsar, M.; Salman, J.; Ius, F.; Gras, C.; Weber, P.; Welte, T.; Gottlieb, J.; et al. C1-esterase-inhibitor for primary graft dysfunction in lung transplantation. Transplantation 2014, 97, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Y.; Yalavarthi, S.; Shi, H.; Gockman, K.; Zuo, M.; Madison, J.A.; Blair, C.; Weber, A.; Barnes, B.J.; Egeblad, M.; et al. Neutrophil extracellular traps in COVID-19. JCI Insight 2020, 5, e138999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vigneswaran, W.T.; Garrity, E.R.; Odell, J.A. Lung Transplantation: Principles and Practice; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar] [CrossRef]
- Dupuis, J.; Sirois, M.G.; Rhéaume, E.; Nguyen, Q.T.; Clavet-Lanthier, M.; Brand, G.; Mihalache-Avram, T.; Théberge-Julien, G.; Charpentier, D.; Rhainds, D.; et al. Colchicine reduces lung injury in experimental acute respiratory distress syndrome. PLoS ONE 2020, 15, e0242318. [Google Scholar] [CrossRef] [PubMed]
- Mason, D.P.; Batizy, L.H.; Wu, J.; Nowicki, E.R.; Murthy, S.C.; McNeill, A.M.; Budev, M.M.; Mehta, A.C.; Pettersson, G.B.; Blackstone, E.H. Matching donor to recipient in lung transplantation: How much does size matter? J. Thorac. Cardiovasc. Surg. 2009, 137, 1234–1240.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavoie, S.S.; Dumas, E.; Vulesevic, B.; Neagoe, P.E.; White, M.; Sirois, M.G. Synthesis of Human Neutrophil Extracellular Traps Contributes to Angiopoietin-Mediated In Vitro Proinflammatory and Proangiogenic Activities. J. Immunol. 2018, 200, 3801–3813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vulesevic, B.; Lavoie, S.S.; Neagoe, P.E.; Dumas, E.; Rakel, A.; White, M.; Sirois, M.G. CRP Induces NETosis in Heart Failure Patients with or without Diabetes. Immunohorizons 2019, 3, 378–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joshi, M.B.; Lad, A.; Bharath Prasad, A.S.; Balakrishnan, A.; Ramachandra, L.; Satyamoorthy, K. High glucose modulates IL-6 mediated immune homeostasis through impeding neutrophil extracellular trap formation. FEBS Lett. 2013, 587, 2241–2246. [Google Scholar] [CrossRef] [Green Version]
- Beaubien-Souligny, W.; Neagoe, P.E.; Gagnon, D.; Denault, A.Y.; Sirois, M.G. Increased Circulating Levels of Neutrophil Extracellular Traps During Cardiopulmonary Bypass. CJC Open 2020, 2, 39–48. [Google Scholar] [CrossRef] [Green Version]
- Paunel-Görgülü, A.; Wacker, M.; El Aita, M.; Hassan, S.; Schlachtenberger, G.; Deppe, A.; Choi, Y.-H.; Kuhn, E.; Mehler, T.O.; Wahlers, T. cfDNA correlates with endothelial damage after cardiac surgery with prolonged cardiopulmonary bypass and amplifies NETosis in an intracellular TLR9-independent manner. Sci. Rep. 2017, 7, 17421. [Google Scholar] [CrossRef] [Green Version]
- Caudrillier, A.; Kessenbrock, K.; Gilliss, B.M.; Nguyen, J.X.; Marques, M.B.; Monestier, M.; Toy, P.; Werb, Z.; Looney, M.R. Platelets induce neutrophil extracellular traps in transfusion-related acute lung injury. J. Clin. Investig. 2012, 122, 2661–2671. [Google Scholar] [CrossRef]
- Leppkes, M.; Knopf, J.; Naschberger, E.; Lindemann, A.; Singh, J.; Herrmann, I.; Sturzl, M.; Staats, L.; Mahajan, A.; Schauer, C.; et al. Vascular occlusion by neutrophil extracellular traps in COVID-19. eBioMedicine 2020, 58, 102925. [Google Scholar] [CrossRef]
- Kaplan, M.J.; Radic, M. Neutrophil extracellular traps: Double-edged swords of innate immunity. J. Immunol. 2012, 189, 2689–2695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grassle, S.; Huck, V.; Pappelbaum, K.I.; Gorzelanny, C.; Aponte-Santamaria, C.; Baldauf, C.; Grater, F.; Schneppenheim, R.; Obser, T.; Schneider, S.W. von Willebrand factor directly interacts with DNA from neutrophil extracellular traps. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1382–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolaczkowska, E.; Jenne, C.N.; Surewaard, B.G.; Thanabalasuriar, A.; Lee, W.Y.; Sanz, M.J.; Mowen, K.; Opdenakker, G.; Kubes, P. Molecular mechanisms of NET formation and degradation revealed by intravital imaging in the liver vasculature. Nat. Commun. 2015, 6, 6673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorensen, O.E.; Borregaard, N. Neutrophil extracellular traps—The dark side of neutrophils. J. Clin. Investig. 2016, 126, 1612–1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, T.A.; Brill, A.; Duerschmied, D.; Schatzberg, D.; Monestier, M.; Myers, D.D., Jr.; Wrobleski, S.K.; Wakefield, T.W.; Hartwig, J.H.; Wagner, D.D. Extracellular DNA traps promote thrombosis. Proc. Natl. Acad. Sci. USA 2010, 107, 15880–15885. [Google Scholar] [CrossRef] [Green Version]
- Massberg, S.; Grahl, L.; von Bruehl, M.L.; Manukyan, D.; Pfeiler, S.; Goosmann, C.; Brinkmann, V.; Lorenz, M.; Bidzhekov, K.; Khandagale, A.B.; et al. Reciprocal coupling of coagulation and innate immunity via neutrophil serine proteases. Nat. Med. 2010, 16, 887–896. [Google Scholar] [CrossRef]
- Wong, S.L.; Wagner, D.D. Peptidylarginine deiminase 4: A nuclear button triggering neutrophil extracellular traps in inflammatory diseases and aging. FASEB J. 2018, 32, fj201800691R. [Google Scholar] [CrossRef]
- McDonald, B.; Davis, R.P.; Kim, S.J.; Tse, M.; Esmon, C.T.; Kolaczkowska, E.; Jenne, C.N. Platelets and neutrophil extracellular traps collaborate to promote intravascular coagulation during sepsis in mice. Blood 2017, 129, 1357–1367. [Google Scholar] [CrossRef] [Green Version]
- von Meijenfeldt, F.A.; Burlage, L.C.; Bos, S.; Adelmeijer, J.; Porte, R.J.; Lisman, T. Elevated Plasma Levels of Cell-Free DNA during Liver Transplantation Are Associated with Activation of Coagulation. Liver Transplant. 2018, 24, 1716–1725. [Google Scholar] [CrossRef] [Green Version]
- Kotani, N.; Hashimoto, H.; Sessler, D.I.; Muraoka, M.; Wang, J.S.; O’Connor, M.F.; Matsuki, A. Neutrophil number and interleukin-8 and elastase concentrations in bronchoalveolar lavage fluid correlate with decreased arterial oxygenation after cardiopulmonary bypass. Anesth. Analg. 2000, 90, 1046–1051. [Google Scholar] [CrossRef] [Green Version]
- Millar, J.E.; Fanning, J.P.; McDonald, C.I.; McAuley, D.F.; Fraser, J.F. The inflammatory response to extracorporeal membrane oxygenation (ECMO): A review of the pathophysiology. Crit. Care 2016, 20, 387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aigner, C.; Slama, A.; Barta, M.; Mitterbauer, A.; Lang, G.; Taghavi, S.; Matilla, J.; Ullrich, R.; Krenn, K.; Jaksch, P.; et al. Treatment of primary graft dysfunction after lung transplantation with orally inhaled AP301: A prospective, randomized pilot study. J. Heart Lung Transplant. 2018, 37, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wei, L.; Han, Z.; Chen, Z.; Zhang, Q. Long non-coding RNA X-inactive specific transcript silencing ameliorates primary graft dysfunction following lung transplantation through microRNA-21-dependent mechanism. eBioMedicine 2020, 52, 102600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallavia, B.; Liu, F.; Lefrançais, E.; Cleary, S.J.; Kwaan, N.; Tian, J.J.; Magnen, M.; Sayah, D.M.; Soong, A.; Chen, J.; et al. Mitochondrial DNA Stimulates TLR9-Dependent Neutrophil Extracellular Trap Formation in Primary Graft Dysfunction. Am. J. Respir. Cell Mol. Biol. 2020, 62, 364–372. [Google Scholar] [CrossRef]
- Mai, S.H.; Khan, M.; Dwivedi, D.J.; Ross, C.A.; Zhou, J.; Gould, T.J.; Gross, P.L.; Weitz, J.I.; Fox-Robichaud, A.E.; Liaw, P.C.; et al. Delayed but not Early Treatment with DNase Reduces Organ Damage and Improves Outcome in a Murine Model of Sepsis. Shock 2015, 44, 166–172. [Google Scholar] [CrossRef]
- Sohrabipour, S.; Muniz, V.S.; Sharma, N.; Dwivedi, D.J.; Liaw, P.C. Mechanistic Studies of Dnase I Activity: Impact of Heparin Variants and PAD4. Shock 2021, 56, 975–987. [Google Scholar] [CrossRef]
- Wang, S.; Xie, T.; Sun, S.; Wang, K.; Liu, B.; Wu, X.; Ding, W. DNase-1 Treatment Exerts Protective Effects in a Rat Model of Intestinal Ischemia-Reperfusion Injury. Sci. Rep. 2018, 8, 17788. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.; Tohme, S.; Al-Khafaji, A.B.; Tai, S.; Loughran, P.; Chen, L.; Wang, S.; Kim, J.; Billiar, T.; Wang, Y.; et al. Damage-associated molecular pattern-activated neutrophil extracellular trap exacerbates sterile inflammatory liver injury. Hepatology 2015, 62, 600–614. [Google Scholar] [CrossRef] [Green Version]
- Peer, V.; Abu Hamad, R.; Berman, S.; Efrati, S. Renoprotective Effects of DNAse-I Treatment in a Rat Model of Ischemia/Reperfusion-Induced Acute Kidney Injury. Am. J. Nephrol. 2016, 43, 195–205. [Google Scholar] [CrossRef]
- Davis, J.C., Jr.; Manzi, S.; Yarboro, C.; Rairie, J.; McInnes, I.; Averthelyi, D.; Sinicropi, D.; Hale, V.G.; Balow, J.; Austin, H.; et al. Recombinant human Dnase I (rhDNase) in patients with lupus nephritis. Lupus 1999, 8, 68–76. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 36) | Non-PGD3 (n = 27) | PGD3 (n = 9) | p Value | |
|---|---|---|---|---|
| Donor characteristics | ||||
| Male | 18 (50%) | 14 (52%) | 4 (44%) | 1.000 |
| Age (years) | 45 ± 17 | 43 ± 16 | 50 ± 15 | 0.281 |
| Body mass index (kg/m2) | 26 (23–29) | 25 (23–30) | 25 (25–27) | 0.889 |
| Cause of death | 0.766 | |||
| - Trauma | 15 (43%) | 12 (44%) | 3 (33%) | |
| - Stroke | 12 (33%) | 9 (33%) | 3 (33%) | |
| - Suicide | 9 (25%) | 6 (22%) | 3 (33%) | |
| Type of organ donation | 0.392 | |||
| Donation after brain death | 26 (72%) | 18 (67%) | 8 (89%) | |
| Donation after circulatory death | 10 (28%) | 9 (33%) | 1 (11%) | |
| Duration of cold ischemia (minutes) | 242 (137–278) | 237 (137–278) | 263 (177–287) | 0.406 |
| pTLC donor-to-recipient ratio | 1.02 (0.85–1.09) | 1.03 (0.85–1.09) | 0.96 (0.84–1.06) | 0.618 |
| PaO2/FiO2 ratio prior to organ harvest (mmHg) | 441 ± 73 | 448 ± 60 | 418 ± 105 | 0.436 |
| White blood cells (109/L) | 13 (11–18) | 13 (11–16) | 18 (12–24) | 0.107 |
| Recipient characteristics | ||||
| Male | 28 (78%) | 22 (82%) | 6 (67%) | 0.352 |
| Age (years) | 62 (53–64) | 62 (46–64) | 62 (58–66) | 0.368 |
| Body mass index (kg/m2) | 24 ± 4 | 24 ± 4 | 25 ± 5 | 0.382 |
| pTLC (L) | 6.5 (5.6–6.9) | 6.7 (6.1–7.0) | 6.3 (5.3–6.4) | 0.136 |
| Diabetes | 14 (39%) | 9 (33%) | 5 (56%) | 0.194 |
| Smoking | 0.431 | |||
| Never | 14 (39%) | 12 (44%) | 2 (22%) | |
| Former | 21 (58%) | 15 (56%) | 6 (67%) | |
| Lung disease | 0.160 | |||
| Pulmonary hypertension | 2 (6%) | 0 (0%) | 2 (22%) | |
| Idiopathic lung fibrosis | 12 (33%) | 10 (37%) | 2 (22%) | |
| Cystic fibrosis | 5 (14%) | 4 (15%) | 1 (11%) | |
| Chronic obstructive pulmonary disease | 12 (33%) | 9 (33%) | 3 (33%) | |
| Interstitial pulmonary disease | 5 (14%) | 4 (15%) | 1 (11%) | |
| White blood cells (109/L) | 10 (7–15) | 10 (7–11) | 12 (7–15) | 0.355 |
| Intraoperative characteristics | ||||
| Duration of surgery (minutes) | 250 ± 51 | 240 ± 43 | 280 ± 63 | 0.044 |
| EVLP | 0 (0%) | 0 (0%) | 0 (0%) | 1.000 |
| CPB/ECMO | 8 (22%) | 3 (11%) | 5 (55%) | 0.005 |
| Red blood cells transfusion | 28 (78%) | 21 (78%) | 6 (67%) | 0.505 |
| Platelets transfusion | 8 (22%) | 4 (15%) | 4 (44%) | 0.064 |
| Volume of blood loss (liters) | 1.2 (1.0–2.0) | 1.2 (1.0–1.5) | 1.5 (1.5–3.0) | 0.101 |
| Postoperative characteristics | ||||
| Postoperative hemorrhage | 4 (11%) | 1 (4%) | 3 (33%) | 0.014 |
| ECMO | 4 (11%) | 0 (0%) | 4 (44%) | 0.001 |
| Mechanical ventilation > 72 h | 8 (22%) | 4 (11%) | 4 (44%) | 0.064 |
| PGD3 at 72 h | 4 (11%) | 0 (0%) | 4 (44%) | 0.001 |
| Death in first year following surgery | 5 (13%) | 1 (4%) | 4 (44%) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonneau, S.; Landry, C.; Bégin, S.; Adam, D.; Villeneuve, L.; Clavet-Lanthier, M.-É.; Dasilva, A.; Charles, E.; Dumont, B.L.; Neagoe, P.-E.; et al. Correlation between Neutrophil Extracellular Traps (NETs) Expression and Primary Graft Dysfunction Following Human Lung Transplantation. Cells 2022, 11, 3420. https://doi.org/10.3390/cells11213420
Bonneau S, Landry C, Bégin S, Adam D, Villeneuve L, Clavet-Lanthier M-É, Dasilva A, Charles E, Dumont BL, Neagoe P-E, et al. Correlation between Neutrophil Extracellular Traps (NETs) Expression and Primary Graft Dysfunction Following Human Lung Transplantation. Cells. 2022; 11(21):3420. https://doi.org/10.3390/cells11213420
Chicago/Turabian StyleBonneau, Steven, Caroline Landry, Stéphanie Bégin, Damien Adam, Louis Villeneuve, Marie-Élaine Clavet-Lanthier, Ariane Dasilva, Elcha Charles, Benjamin L. Dumont, Paul-Eduard Neagoe, and et al. 2022. "Correlation between Neutrophil Extracellular Traps (NETs) Expression and Primary Graft Dysfunction Following Human Lung Transplantation" Cells 11, no. 21: 3420. https://doi.org/10.3390/cells11213420