

CXCR4-CXCL12-CXCR7 and PD-1/PD-L1 in Pancreatic Cancer: CXCL12 Predicts Survival of Radically Resected Patients

 , , , , , , ,
, , , , , , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Tissues
2.2. Immunohistochemistry
2.3. Statistical Analysis
2.4. Validation Cohort and Tissues
3. Results
3.1. Epithelial and Stromal PDAC Cells Express CXCR4
3.2. Epithelial and Stromal PDAC Cell Express CXCR7
3.3. PDAC Cancer Cells Express CXCL12
3.4. PD-L1 Is Predominantly Expressed by TME in PDAC
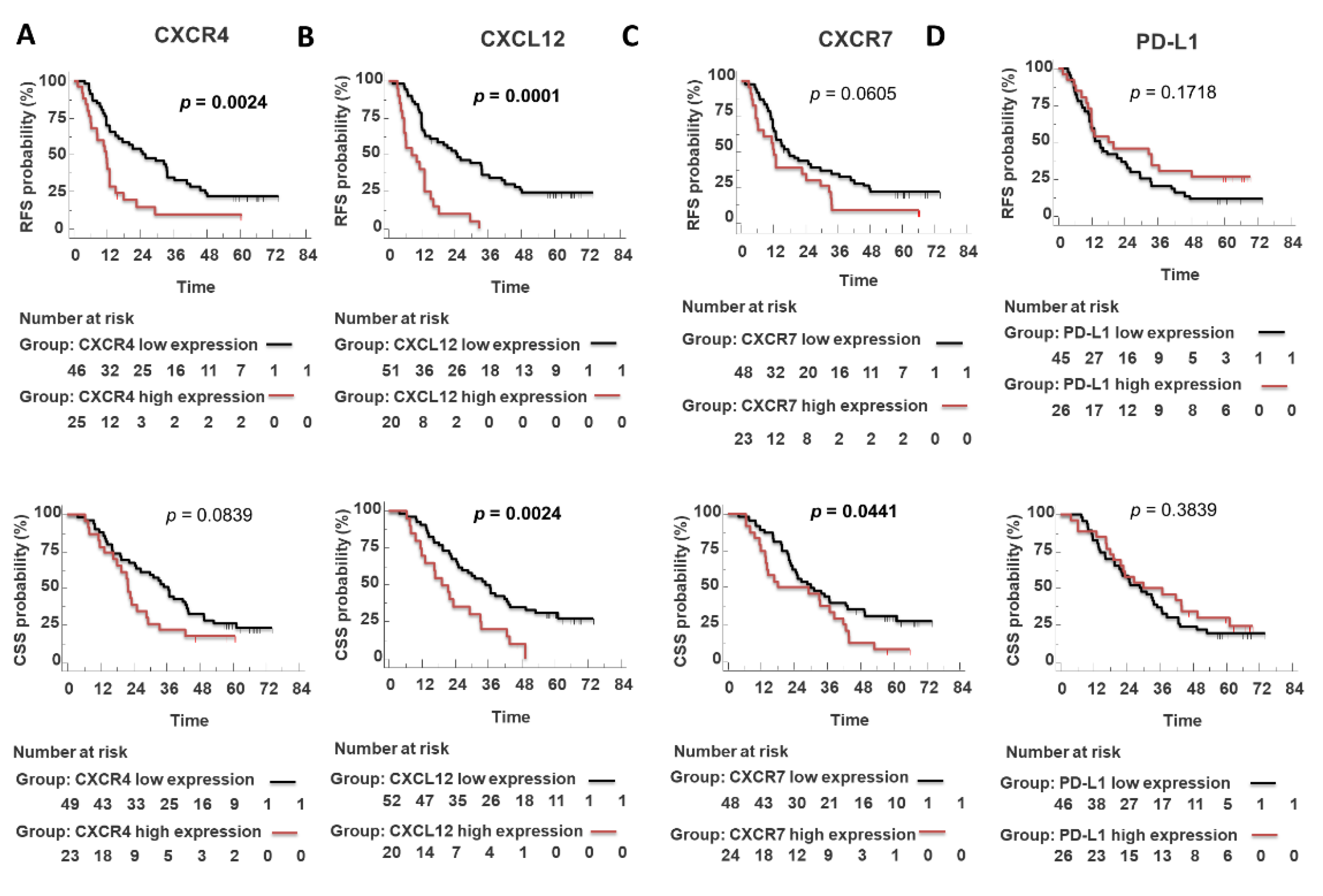
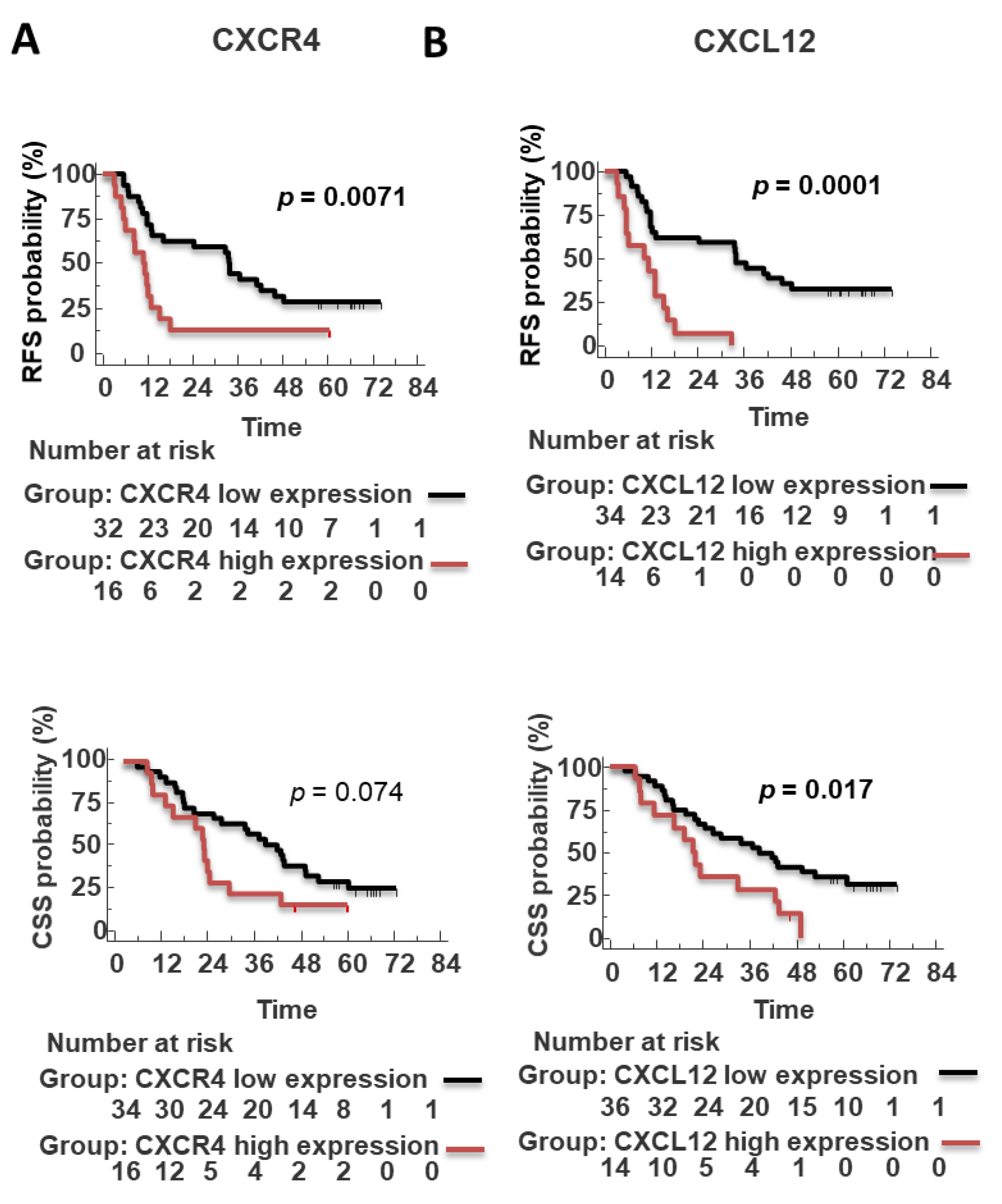
3.5. Prognostic Significance of Epithelial and Stroma CXCL12, CXCR4, CXCR7 and PD-L1 in PDAC
3.6. Tumoral CXCL12 Is an Independent Poor Prognostic Factor at the Multivariate Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Maisonneuve, P.; Lowenfels, A.B. Risk factors for pancreatic cancer: A summary review of meta-analytical studies. Int. J. Epidemiol. 2015, 44, 186–198. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hidalgo, M. Pancreatic cancer. N. Engl. J. Med. 2010, 362, 1605–1617. [Google Scholar] [CrossRef] [Green Version]
- Mizrahi, J.D.; Surana, R.; Valle, J.W.; Shroff, R.T. Pancreatic cancer. Lancet 2020, 395, 2008–2020. [Google Scholar] [CrossRef]
- Soer, E.; Brosens, L.; van de Vijver, M.; Dijk, F.; van Velthuysen, M.-L.; Farina-Sarasqueta, A.; Morreau, H.; Offerhaus, J.; Koens, L.; Verheij, J. Dilemmas for the pathologist in the oncologic assessment of pancreatoduodenectomy specimens. Virchows Arch. 2018, 472, 533–543. [Google Scholar] [CrossRef] [Green Version]
- Wagner, M.; Redaelli, C.; Lietz, M.; Seiler, C.A.; Friess, H.; Büchler, M.W. Curative resection is the single most important factor determining outcome in patients with pancreatic adenocarcinoma. BJS 2004, 91, 586–594. [Google Scholar] [CrossRef]
- Moutinho-Ribeiro, P.; Macedo, G.; Melo, S.A. Pancreatic Cancer Diagnosis and Management: Has the Time Come to Prick the Bubble? Front. Endocrinol. 2019, 9, 779. [Google Scholar] [CrossRef]
- Pompella, L.; Tirino, G.; Pappalardo, A.; Caterino, M.; Ventriglia, A.; Nacca, V.; Orditura, M.; Ciardiello, F.; De Vita, F. Pancreatic Cancer Molecular Classifications: From Bulk Genomics to Single Cell Analysis. Int. J. Mol. Sci. 2020, 21, 2814. [Google Scholar] [CrossRef] [Green Version]
- Lutz, E.R.; Wu, A.A.; Bigelow, E.; Sharma, R.; Mo, G.; Soares, K.; Solt, S.; Dorman, A.; Wamwea, A.; Yager, A.; et al. Immunotherapy converts nonimmunogenic pancreatic tumors into immunogenic foci of immune regulation. Cancer Immunol. Res. 2014, 2, 616–631. [Google Scholar] [CrossRef]
- Waddell, N.; Pajic, M.; Patch, A.M.; Chang, D.K.; Kassahn, K.S.; Bailey, P.; Johns, A.L.; Miller, D.; Nones, K.; Quek, K.; et al. Whole genomes redefine the mutational landscape of pancreatic cancer. Nature 2015, 518, 495–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, L.D.; Hruban, R.H. Pathology and molecular genetics of pancreatic neoplasms. Cancer J. 2012, 18, 492–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feig, C.; Gopinathan, A.; Neesse, A.; Chan, D.S.; Cook, N.; Tuveson, D.A. The pancreas cancer microenvironment. Clin. Cancer Res. An. Off. J. Am. Assoc. Cancer Res. 2012, 18, 4266–4276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Bosch, N.; Vinaixa, J.; Navarro, P. Immune Evasion in Pancreatic Cancer: From Mechanisms to Therapy. Cancers 2018, 10, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wojtowicz, M.E.; Dunn, B.K.; Umar, A. Immunologic approaches to cancer prevention-current status, challenges, and future perspectives. Semin. Oncol. 2016, 43, 161–172. [Google Scholar] [CrossRef]
- Kabacaoglu, D.; Ciecielski, K.J.; Ruess, D.A.; Algül, H. Immune Checkpoint Inhibition for Pancreatic Ductal Adenocarcinoma: Current Limitations and Future Options. Front. Immunol 2018, 9, 1878. [Google Scholar] [CrossRef]
- Liang, X.; Sun, J.; Wu, H.; Luo, Y.; Wang, L.; Lu, J.; Zhang, Z.; Guo, J.; Liang, Z.; Liu, T. PD-L1 in pancreatic ductal adenocarcinoma: A retrospective analysis of 373 Chinese patients using an in vitro diagnostic assay. Diagn. Pathol. 2018, 13, 5. [Google Scholar] [CrossRef]
- Wang, L.; Ma, Q.; Li, D.; Mu, S.; Li, Y.; Wang, Y.; Shi, P.; Yu, H.; Gao, C.; Guo, K.; et al. Indoleamine 2, 3-dioxygenase and B7-H1 expressions as prognostic and follow-up markers in human pancreatic carcinoma. Pathol. Res. Pract. 2018, 214, 1309–1314. [Google Scholar] [CrossRef]
- Hu, Y.; Chen, W.; Yan, Z.; Ma, J.; Zhu, F.; Huo, J. Prognostic value of PD-L1 expression in patients with pancreatic cancer: A PRISMA-compliant meta-analysis. Medicine 2019, 98, e14006. [Google Scholar] [CrossRef]
- Righetti, A.; Giulietti, M.; Šabanović, B.; Occhipinti, G.; Principato, G.; Piva, F. CXCL12 and Its Isoforms: Different Roles in Pancreatic Cancer? J. Oncol. 2019, 2019, 9681698. [Google Scholar] [CrossRef]
- Balic, A.; Sørensen, M.D.; Trabulo, S.M.; Sainz, B.; Cioffi, M.; Vieira, C.R.; Miranda-Lorenzo, I.; Hidalgo, M.; Kleeff, J.; Erkan, M.; et al. Chloroquine Targets Pancreatic Cancer Stem Cells via Inhibition of CXCR4 and Hedgehog Signaling. Mol. Cancer Ther. 2014, 13, 1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morimoto, M.; Matsuo, Y.; Koide, S.; Tsuboi, K.; Shamoto, T.; Sato, T.; Saito, K.; Takahashi, H.; Takeyama, H. Enhancement of the CXCL12/CXCR4 axis due to acquisition of gemcitabine resistance in pancreatic cancer: Effect of CXCR4 antagonists. BMC Cancer 2016, 16, 305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laise, P.; Turunen, M.; Maurer, H.C.; Curiel, A.G.; Elyada, E.; Schmierer, B.; Tomassoni, L.; Worley, J.; Alvarez, M.J.; Kesner, J.; et al. Pancreatic Ductal Adenocarcinoma Comprises Coexisting Regulatory States with both Common and Distinct Dependencies. Biorxiv 2010, 2020.2010.2027.357269. [Google Scholar] [CrossRef]
- Singh, S.; Srivastava, S.K.; Bhardwaj, A.; Owen, L.B.; Singh, A.P. CXCL12-CXCR4 signalling axis confers gemcitabine resistance to pancreatic cancer cells: A novel target for therapy. Br. J. Cancer 2010, 103, 1671–1679. [Google Scholar] [CrossRef] [Green Version]
- Shen, B.; Zheng, M.Q.; Lu, J.W.; Jiang, Q.; Wang, T.H.; Huang, X.E. CXCL12-CXCR4 promotes proliferation and invasion of pancreatic cancer cells. Asian Pac. J. Cancer Prev. APJCP 2013, 14, 5403–5408. [Google Scholar] [CrossRef] [Green Version]
- Samarendra, H.; Jones, K.; Petrinic, T.; Silva, M.A.; Reddy, S.; Soonawalla, Z.; Gordon-Weeks, A. A meta-analysis of CXCL12 expression for cancer prognosis. Br. J. Cancer 2017, 117, 124–135. [Google Scholar] [CrossRef]
- Guo, J.C.; Li, J.; Zhou, L.; Yang, J.Y.; Zhang, Z.G.; Liang, Z.Y.; Zhou, W.X.; You, L.; Zhang, T.P.; Zhao, Y.P. CXCL12-CXCR7 axis contributes to the invasive phenotype of pancreatic cancer. Oncotarget 2016, 7, 62006–62018. [Google Scholar] [CrossRef] [Green Version]
- Hong, T.S.; Ryan, D.P.; Borger, D.R.; Blaszkowsky, L.S.; Yeap, B.Y.; Ancukiewicz, M.; Deshpande, V.; Shinagare, S.; Wo, J.Y.; Boucher, Y.; et al. A phase 1/2 and biomarker study of preoperative short course chemoradiation with proton beam therapy and capecitabine followed by early surgery for resectable pancreatic ductal adenocarcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 830–838. [Google Scholar] [CrossRef] [Green Version]
- Ding, Y.; Du, Y. Clinicopathological significance and prognostic role of chemokine receptor CXCR4 expression in pancreatic ductal adenocarcinoma, a meta-analysis and literature review. Int. J. Surg. 2019, 65, 32–38. [Google Scholar] [CrossRef]
- Tempero, M.A. NCCN Guidelines Updates: Pancreatic Cancer. J. Natl. Compr. Cancer Netw. JNCCN 2019, 17, 603–605. [Google Scholar] [CrossRef]
- Gebauer, F.; Tachezy, M.; Effenberger, K.; von Loga, K.; Zander, H.; Marx, A.; Kaifi, J.T.; Sauter, G.; Izbicki, J.R.; Bockhorn, M. Prognostic impact of CXCR4 and CXCR7 expression in pancreatic adenocarcinoma. J. Surg. Oncol. 2011, 104, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Kawashima, H.; Ohno, E.; Ishikawa, T.; Tanaka, H.; Nakamura, M.; Miyahara, R.; Ishigami, M.; Hirooka, Y.; Fujishiro, M. Diagnosis of vascular invasion in pancreatic ductal adenocarcinoma using endoscopic ultrasound elastography. BMC Gastroenterol. 2020, 20, 81. [Google Scholar] [CrossRef] [Green Version]
- Underwood, P.W.; Zhang, D.Y.; Cameron, M.E.; Gerber, M.H.; Delitto, D.; Maduka, M.U.; Cooper, K.J.; Han, S.; Hughes, S.J.; Judge, S.M.; et al. Nicotine Induces IL-8 Secretion from Pancreatic Cancer Stroma and Worsens Cancer-Induced Cachexia. Cancers 2020, 12, 329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirata, K.; Kodama, S.; Nakano, Y.; Minaki-Nakagawa, Y.; Aoyama, Y.; Sakikubo, M.; Goto, T.; Yoshida, M.; Masui, T.; Yamamoto, T.; et al. Exocrine tissue-driven TFF2 prevents apoptotic cell death of endocrine lineage during pancreas organogenesis. Sci. Rep. 2019, 9, 1636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvucci, O.; Yao, L.; Villalba, S.; Sajewicz, A.; Pittaluga, S.; Tosato, G. Regulation of endothelial cell branching morphogenesis by endogenous chemokine stromal-derived factor. Blood 2002, 99, 2703–2711. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Liu, C.; Mo, X.; Shi, H.; Li, S. Mechanisms by which CXCR4/CXCL12 cause metastatic behavior in pancreatic cancer. Oncol. Lett. 2018, 15, 1771–1776. [Google Scholar] [CrossRef] [Green Version]
- Werner, R.A.; Kircher, S.; Higuchi, T.; Kircher, M.; Schirbel, A.; Wester, H.J.; Buck, A.K.; Pomper, M.G.; Rowe, S.P.; Lapa, C. CXCR4-Directed Imaging in Solid Tumors. Front. Oncol. 2019, 9, 770. [Google Scholar] [CrossRef] [Green Version]
- Trotta, A.M.; Aurilio, M.; D’Alterio, C.; Ieranò, C.; Di Martino, D.; Barbieri, A.; Luciano, A.; Gaballo, P.; Santagata, S.; Portella, L.; et al. Novel Peptide-Based PET Probe for Non-invasive Imaging of C-X-C Chemokine Receptor Type 4 (CXCR4) in Tumors. J. Med. Chem. 2021, 64, 3449–3461. [Google Scholar] [CrossRef]
- Demir, I.E.; Kujundzic, K.; Pfitzinger, P.L.; Saricaoglu, Ö.C.; Teller, S.; Kehl, T.; Reyes, C.M.; Ertl, L.S.; Miao, Z.; Schall, T.J.; et al. Early pancreatic cancer lesions suppress pain through CXCL12-mediated chemoattraction of Schwann cells. Proc. Natl. Acad. Sci. USA 2017, 114, E85. [Google Scholar] [CrossRef] [Green Version]
- Salazar, N.; Zabel, B.A. Support of Tumor Endothelial Cells by Chemokine Receptors. Front. Immunol. 2019, 10, 147. [Google Scholar] [CrossRef]
- Takbiri Osgoei, L.; Parivar, K.; Ebrahimi, M.; Mortaz, E. Nicotine Modulates the Release of Inflammatory Cytokines and Expression of TLR2, TLR4 of Cord Blood Mononuclear Cells. Iran. J. Allergy Asthma Immunol. 2018, 17, 372–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, R.K.; Lokeshwar, B.L. The IL-8–Regulated Chemokine Receptor CXCR7 Stimulates EGFR Signaling to Promote Prostate Cancer Growth. Cancer Res. 2011, 71, 3268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, N.; Xu, H.; Ou, Y.; Feng, Z.; Zhang, Q.; Zhu, Q.; Cai, Z. LPS-induced CXCR7 expression promotes gastric Cancer proliferation and migration via the TLR4/MD-2 pathway. Diagn. Pathol. 2019, 14, 3. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, G.J. Regulation of heterogeneous cancer-associated fibroblasts: The molecular pathology of activated signaling pathways. J. Exp. Clin. Cancer Res. CR 2020, 39, 112. [Google Scholar] [CrossRef] [PubMed]
- Bracci, P.M.; Wang, F.; Hassan, M.M.; Gupta, S.; Li, D.; Holly, E.A. Pancreatitis and pancreatic cancer in two large pooled case–control studies. Cancer Causes Control. 2009, 20, 1723–1731. [Google Scholar] [CrossRef] [Green Version]
- Lowenfels, A.B.; Maisonneuve, P.; Cavallini, G.; Ammann, R.W.; Lankisch, P.G.; Andersen, J.R.; Dimagno, E.P.; Andrén-Sandberg, A.; Domellöf, L. Pancreatitis and the risk of pancreatic cancer. International Pancreatitis Study Group. N. Engl. J. Med. 1993, 328, 1433–1437. [Google Scholar] [CrossRef]
- Gandhi, S.; de la Fuente, J.; Murad, M.H.; Majumder, S. Chronic Pancreatitis Is a Risk Factor for Pancreatic Cancer, and Incidence Increases With Duration of Disease: A Systematic Review and Meta-analysis. Clin. Transl. Gastroenterol. 2022, 13, e00463. [Google Scholar] [CrossRef]
- Mujica, V.R.; Barkin, J.S.; Go, V.L. Acute pancreatitis secondary to pancreatic carcinoma. Study Group Participants. Pancreas 2000, 21, 329–332. [Google Scholar] [CrossRef]
- Wang, L.; Ma, Q.; Chen, X.; Guo, K.; Li, J.; Zhang, M. Clinical Significance of B7-H1 and B7-1 Expressions in Pancreatic Carcinoma. World J. Surg. 2010, 34, 1059–1065. [Google Scholar] [CrossRef]
- Nomi, T.; Sho, M.; Akahori, T.; Hamada, K.; Kubo, A.; Kanehiro, H.; Nakamura, S.; Enomoto, K.; Yagita, H.; Azuma, M.; et al. Clinical Significance and Therapeutic Potential of the Programmed Death-1 Ligand/Programmed Death-1 Pathway in Human Pancreatic Cancer. Clin. Cancer Res. 2007, 13, 2151–2157. [Google Scholar] [CrossRef]
- Tessier-Cloutier, B.; Kalloger, S.E.; Al-Kandari, M.; Milne, K.; Gao, D.; Nelson, B.H.; Renouf, D.J.; Sheffield, B.S.; Schaeffer, D.F. Programmed cell death ligand 1 cut-point is associated with reduced disease specific survival in resected pancreatic ductal adenocarcinoma. BMC Cancer 2017, 17, 618. [Google Scholar] [CrossRef] [PubMed]
- Karamitopoulou, E.; Andreou, A.; Pahud de Mortanges, A.; Tinguely, M.; Gloor, B.; Perren, A. PD-1/PD-L1–Associated Immunoarchitectural Patterns Stratify Pancreatic Cancer Patients into Prognostic/Predictive Subgroups. Cancer Immunol. Res. 2021, 9, 1439–1450. [Google Scholar] [CrossRef] [PubMed]
- Diana, A.; Wang, L.M.; D’Costa, Z.; Allen, P.; Azad, A.; Silva, M.A.; Soonawalla, Z.; Liu, S.; McKenna, W.G.; Muschel, R.J.; et al. Prognostic value, localization and correlation of PD-1/PD-L1, CD8 and FOXP3 with the desmoplastic stroma in pancreatic ductal adenocarcinoma. Oncotarget 2016, 7, 40992–41004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Lin, J.; Cui, J.; Han, T.; Jiao, F.; Meng, Z.; Wang, L. Prognostic value and clinicopathological features of PD-1/PD-L1 expression with mismatch repair status and desmoplastic stroma in Chinese patients with pancreatic cancer. Oncotarget 2017, 8, 9354–9365. [Google Scholar] [CrossRef] [Green Version]
- Rahn, S.; Krüger, S.; Mennrich, R.; Goebel, L.; Wesch, D.; Oberg, H.-H.; Vogel, I.; Ebsen, M.; Röcken, C.; Helm, O.; et al. POLE Score: A comprehensive profiling of programmed death 1 ligand 1 expression in pancreatic ductal adenocarcinoma. Oncotarget 2019, 10, 1572–1588. [Google Scholar] [CrossRef] [Green Version]
- Seo, Y.D.; Jiang, X.; Sullivan, K.M.; Jalikis, F.G.; Smythe, K.S.; Abbasi, A.; Vignali, M.; Park, J.O.; Daniel, S.K.; Pollack, S.M.; et al. Mobilization of CD8(+) T Cells via CXCR4 Blockade Facilitates PD-1 Checkpoint Therapy in Human Pancreatic Cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2019, 25, 3934–3945. [Google Scholar] [CrossRef] [Green Version]
- Collier, J.L.; Weiss, S.A. Not-so-opposite ends of the spectrum: CD8(+) T cell dysfunction across chronic infection, cancer and autoimmunity. Nat. Immunol. 2021, 22, 809–819. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N of Patients (%) | N Patients |
|---|---|---|
| Age (yr); mean ± SD; median (range) | 66.02 ± 9.6; 67 (42–84) | 76 |
| ≤60 | 16(21.1%) | |
| >60 | 60(78.9%) | |
| Gender | 76 | |
| Female | 34(46.6%) | |
| Male | 42(55.4%) | |
| Pancreas tumor location | 76 | |
| Head | 61 (80.3%) | |
| Others | 15(19.7%) | |
| CA 19–9 (U/mL), mean ± SD; median (range) | 337.8 ± 753.6; 88.6(0.6–4443) | 76 |
| 0(0–100 U/mL) | 39(51.3%) | |
| 1(100–350 U/mL) | 20(26.3%) | |
| 2(>350 U/mL) | 17(22.4%) | |
| Histologic Tumour grade | 76 | |
| G2 | 69(90.8%) | |
| G3 | 7(9.2%) | |
| Histotype | 76 | |
| Pancreatic ductal adenocarcinoma | 72(94.7%) | |
| Pancreatic ductal adenocarcinoma + IPMN | 4(5.3%) | |
| AJCC Stage 8th ed. | 76 | |
| IA | 6(7.9%) | |
| IB | 6(7.9%) | |
| IIA | 2(2.6%) | |
| IIB | 28(36.8%) | |
| III | 34(44.7%) | |
| Tumour size (mm), mean ± SD; median (range) | 28.6 ± 9.8; 25(10–60) | 76 |
| 0–20 | 19(25.0%) | |
| >20 | 57(75.0%) | |
| Positive lymph nodes | 4.6 ± 4.9; 3(0–24) | 76 |
| N0(0) | 14(18,4%) | |
| N1(1–3) | 28(36.8%) | |
| N2(>4) | 34(44.7%) | |
| R Status | 76 | |
| R0 | 51(67.1%) | |
| R1 | 26(32.9%) | |
| Vascular neoplastic emboli | 76 | |
| No | 10(13.2%) | |
| Yes | 66(86.8%) | |
| Vascular Invasion | 76 | |
| No | 65(82.9%) | |
| Yes | 11(17.1%) | |
| Perineural Invasion | 76 | |
| No | 11(14.5%) | |
| Yes | 65(85.5%) | |
| Adjuvant Chemotherapy | 70 | |
| No | 10(14.3%) | |
| Yes | 60(85.7%) | |
| Adjuvant Radiotherapy | 70 | |
| No | 50(71.4%) | |
| Yes | 20(28.6%) |
| CXCR4 | CXCR7 | CXCL12 | PD-L1 | |||||
|---|---|---|---|---|---|---|---|---|
| Tumor | Stroma | Tumor | Stroma | Tumor | Stroma | Tumor | Stroma | |
| N Patients assessable | 76 | 76 | 76 | 76 | 76 | 76 | 76 | 76 |
| mean (±SD) | 46.88(±51.23) | 13.4(±10.8) | 13.3(±16.7) | 3.6(±7.5) | 3.7(±7.2) | 1.2(±3.6) | 3.4(±7.1) | 5.8(±8.6) |
| Median (range) | 37.5(0–210) | 10(0–40) | 5(0–50) | 0(0–60) | 0(0–30) | 0 (0–20) | 0(0–30) | 0 (0–30) |
| Positive case (%) | 25 (32.9%) | 53(69.7%) | 26(34.2%) | 43(56.6%) | 20(26.3%) | 15(19.7%) | 29(38.2%) | 32(42.2%) |
| Negative case (%) | 51(67.1%) | 23(30,3%) | 50(65.8%) | 33(43.4%) | 56(73.7%) | 61 (80.3%) | 47(62.8%) | 44(57.9%) |
| CXCR4 | CXCR7 | CXCL12 | PD-L1 | |||||
|---|---|---|---|---|---|---|---|---|
| Tumor | Stroma | Tumor | Stroma | Tumor | Stroma | Tumor | Stroma | |
| Age(yr) (≤60 vs. >60) | ─ | ─ | ─ | ─ | ─ | ─ | ─ | ─ |
| Tumor location (Head vs body/tail) | 0.071 | ─ | ─ | ─ | ─ | ─ | ─ | 0.077 |
| AJCC Stage 8th ed. (I–II vs. III) | ─ | ─ | ─ | ─ | ─ | ─ | ─ | ─ |
| Positive Lymph node (N0 vs. N1–2) | ─ | ─ | ─ | ─ | ─ | ─ | ─ | ─ |
| Smoke habit (yes vs. no) | ─ | ─ | ─ | 0.002 | ─ | ─ | ─ | ─ |
| Vacular invasion | 0.042 | 0.045 | ─ | ─ | ─ | ─ | ─ | ─ |
| Perineural invasion | ─ | 0.056 | ─ | ─ | ─ | ─ | ─ | ─ |
| American Joint Committee on Cancer (AJCC) Stage | ||||||||
| * RFS (n = 71) | # CSS (n = 72) | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | n (Median RFS) | HR | 95% CI | p-Value | n (Median CSS) | HR | 95% CI | p-Value |
| Age (yr) | 0.8389 | 0.2156–0.9088 | 0.0264 | 0.5559 | 0.2484–0.9766 | 0.0423 | ||
| ≤60 | 16(11.9) | 18(21.4) | ||||||
| >60 | 55(21.3) | 54(35.0) | ||||||
| Gender | — | — | 0.530 | — | — | 0.240 | ||
| Female | 33 (16.1) | 33 (36.6) | ||||||
| Male | 38 (15.3) | 39(26.6) | ||||||
| Pancreas tumor location | — | — | 0.8223 | — | — | 0.7551 | ||
| Head | 56(13.1) | 57(28.7) | ||||||
| Others | 15(22.7) | 15(419) | ||||||
| Δ Pathological AJCC Stage 8th ed. | 2.2316 | 1.4382–4.6816 | 0.0015 | 3.2258 | 2.3430–8.1967 | 0.0001 | ||
| I–II | 42(24.3) | 43(42.7) | ||||||
| III | 29(10.9) | 29(16.4) | ||||||
| l AJCC Positive lymph nodes | 2.2457 | 1.1094–3.4819 | 0.0206 | 2.1580 | 1.0707–3.4294 | 0.0285 | ||
| N0 | 14(41.0) | 15(43.7) | ||||||
| N1–2 | 57(12.7) | 57(24.9) | ||||||
| Tumor size (mm) | — | — | 0.8909 | — | — | 0.8102 | ||
| 0–20 | 20(14.9) | 20(33.8) | ||||||
| >20 | 51(15.1) | 52(26.6) | ||||||
| ‡ Histologic Tumour grade | — | — | 0.1598 | — | — | 0.1080 | ||
| G2 | 65 (16.0) | 66(28.7) | ||||||
| G3 | 6 (49) | 6(41.9) | ||||||
| ¢ Margin status after resection R | — | — | 0.0895 | — | — | 0.2013 | ||
| R0 | 48(15.1) | 50(33.1) | ||||||
| R1 | 23(14.9) | 22(29.2) | ||||||
| Vascular Invasion | 2.0173 | 1.1204–5.7405 | 0.0255 | 2.1227 | 1.1315–6.9784 | 0.0260 | ||
| No | 58(17.7) | 61(33.5) | ||||||
| Yes | 13(9.5) | 11(19.6) | ||||||
| Perineural Invasion | 4.5956 | 1.5267–5.1440 | 0.0009 | 3.7651 | 1.3060–4.6577 | 0.0054 | ||
| No | 11(–) | 10 (–) | ||||||
| Yes | 60(12.9) | 62 (25.3) | ||||||
| ø CA 19–9 | — | — | 0.8940 | — | — | 0.4018 | ||
| (0–100 U/mL) | 37 (13.1) | 38(29.9) | ||||||
| (100–350 U/mL) | 19 (16.0) | 18(38.5) | ||||||
| (>350 U/mL) | 15(13.1) | 16(21.9) | ||||||
| ¢ Histotype | 0.1385 | 0.1642–0.8569 | 0.0200 | — | — | 0.0966 | ||
| Ductal adenocarcinoma | 67(13.1) | 69(28.7) | ||||||
| Ductal adenocarcinoma + IPMN | 4(–) | 3(–) | ||||||
| Adjuvant chemotherapy | — | — | 0.1976 | — | — | 0.2427 | ||
| No | 10(29.5) | 7(49.4) | ||||||
| Yes | 57(14.9) | 59(29.9) | ||||||
| Adjuvant Radiotherapy | — | — | 0.7986 | — | — | 0.6187 | ||
| No | 48(18.1) | 47(33.8) | ||||||
| Yes | 19(13.1) | 9(24.4) | ||||||
| Progression local and distant spread | — | — | 0.4466 | — | — | 0.5034 | ||
| Local | 14 (18.1) | 14(35.5) | ||||||
| Distant | 41 (11.8) | 40(22.8) | ||||||
| Local and Distant | 4 (11.6) | 4(24,3) | ||||||
| Chronic pancreatitis | — | — | 0.0980 | 1.7575 | 1.0417–3.5112 | 0.0365 | ||
| No | 48(14.9) | 49(31.1) | ||||||
| Yes | 23(18.1) | 23(23.3) | ||||||
| Vascular neoplastic emboli | 3.2648 | 1.1825–4.4287 | 0.0140 | 3.3647 | 1.2124–4.5434 | 0.0113 | ||
| No | 9(–) | 10(–) | ||||||
| Yes | 62(13.1) | 62(26.6) | ||||||
| CXCL12 | 3.3167 | 3.0193–14.2857 | 0.0001 | 2.4845 | 1.7280–6.9204 | 0.0024 | ||
| Low expression | 51(24.9) | 52(35.0) | ||||||
| High expression | 20(8.4) | 20(19.2) | ||||||
| CXCR4 | 0.4572 | 0.1971–0.7051 | 0.0024 | — | — | 0.0839 | ||
| low expression | 46(26.0) | 49(36.6) | ||||||
| High expression | 25(11.7) | 23(21.9) | ||||||
| CXCR7 | — | — | 0.0605 | 1.7173 | 1.0162–3.3146 | 0.0441 | ||
| Low expression | 48(17.6) | 48(29.9) | ||||||
| High expression | 23(12.0) | 24(29.2) | ||||||
| PD-L1 | — | — | 0.1718 | — | — | 0.3989 | ||
| Low expression | 45(14.9) | 46(29.2) | ||||||
| High expression | 26(19.8) | 26(36.8) | ||||||
| * RFS (n =71) | # CSS (n = 72) | |||||
|---|---|---|---|---|---|---|
| Variables | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Age (yr) | — | — | — | — | — | — |
| ≤60 | ||||||
| >60 | ||||||
| Δ Pathological AJCC Stage 8th ed. | 1.2125 | 1.0012–1.4757 | 0.0490 | 1.5416 | 1.2779–1.8597 | 0.00007 |
| I-II | ||||||
| III | ||||||
| AJCC Positive lymph nodes | 1.9816 | 0.8912–4.4062 | 0.0951 | — | — | — |
| N0 | ||||||
| N1-2 | ||||||
| ¢ Margin status after resection R | — | — | — | |||
| R0 | ||||||
| R1 | ||||||
| Vascular Invasion | 1.808 | 0.9243–3.5366 | 0.0852 | 2.6831 | 1.3190–5.4581 | 0.0067 |
| No | ||||||
| Yes | ||||||
| Perineural Invasion | 3.9024 | 1.3777–11.0535 | 0.01077 | 2.5256 | 0.9001–7.0869 | 0.0799 |
| No | ||||||
| Yes | ||||||
| Histotype | — | — | — | — | — | — |
| Ductal adenocarcinoma | ||||||
| Ductal adenocarcinoma+IPMN | ||||||
| Adjuvant chemotherapy | — | — | — | |||
| No | ||||||
| Yes | ||||||
| Chronic pancreatitis | — | — | — | 1.7577 | 0.9731–3.1750 | 0.06286 |
| No | ||||||
| Yes | ||||||
| Vascular neoplastic emboli | — | — | — | — | — | — |
| No | ||||||
| Yes | ||||||
| CXCL12 | 3.7184 | 2.0537–6.7325 | 0.00002 | 2.3515 | 1.2784–4.3253 | 0.0062 |
| Low expression | ||||||
| High expression | ||||||
| CXCR4 | — | — | — | — | — | — |
| low expression | ||||||
| High expression | ||||||
| CXCR7 | — | — | — | — | — | — |
| Low expression | ||||||
| High expression |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Alterio, C.; Giardino, A.; Scognamiglio, G.; Butturini, G.; Portella, L.; Guardascione, G.; Frigerio, I.; Montella, M.; Gobbo, S.; Martignoni, G.; et al. CXCR4-CXCL12-CXCR7 and PD-1/PD-L1 in Pancreatic Cancer: CXCL12 Predicts Survival of Radically Resected Patients. Cells 2022, 11, 3340. https://doi.org/10.3390/cells11213340
D’Alterio C, Giardino A, Scognamiglio G, Butturini G, Portella L, Guardascione G, Frigerio I, Montella M, Gobbo S, Martignoni G, et al. CXCR4-CXCL12-CXCR7 and PD-1/PD-L1 in Pancreatic Cancer: CXCL12 Predicts Survival of Radically Resected Patients. Cells. 2022; 11(21):3340. https://doi.org/10.3390/cells11213340
Chicago/Turabian StyleD’Alterio, Crescenzo, Alessandro Giardino, Giosuè Scognamiglio, Giovanni Butturini, Luigi Portella, Giuseppe Guardascione, Isabella Frigerio, Marco Montella, Stefano Gobbo, Guido Martignoni, and et al. 2022. "CXCR4-CXCL12-CXCR7 and PD-1/PD-L1 in Pancreatic Cancer: CXCL12 Predicts Survival of Radically Resected Patients" Cells 11, no. 21: 3340. https://doi.org/10.3390/cells11213340