
Impact of Mycobacterium tuberculosis Infection on Human B Cell Compartment and Antibody Responses

 ,
,  , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Characteristics of the Enrolled Individuals
2.2. Cell Staining, Flow Cytometry, and Quantitative Analysis
2.3. Dimensional Reduction and Exploratory Analysis
2.4. Quantitative and Qualitative Analysis of Serum Immunoglobulins
2.5. Differential Gene Expression Analysis and Pathway Analysis
2.6. Statistics
3. Results
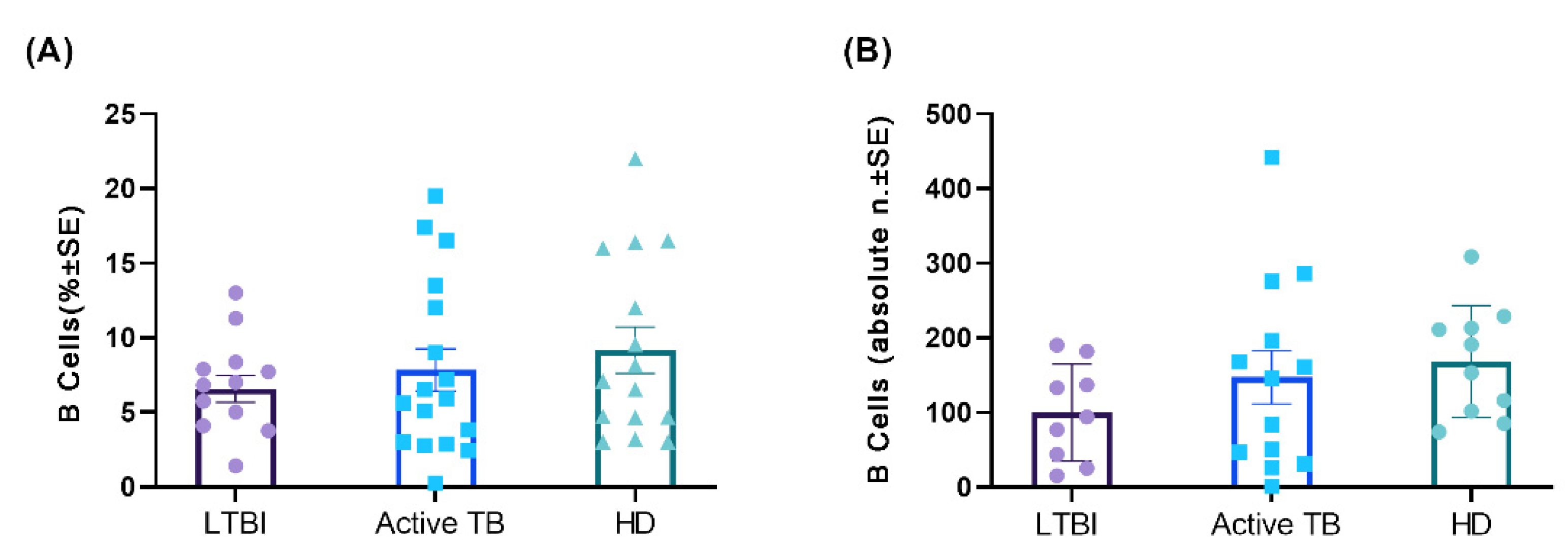
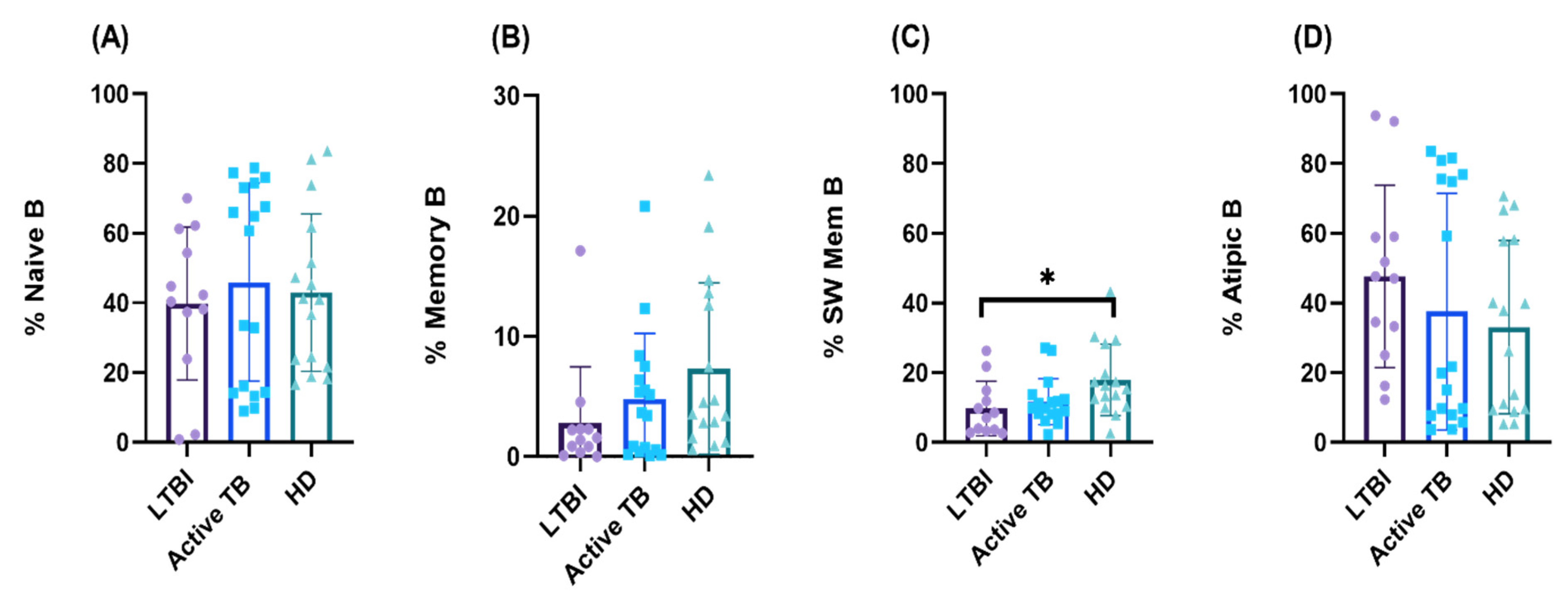
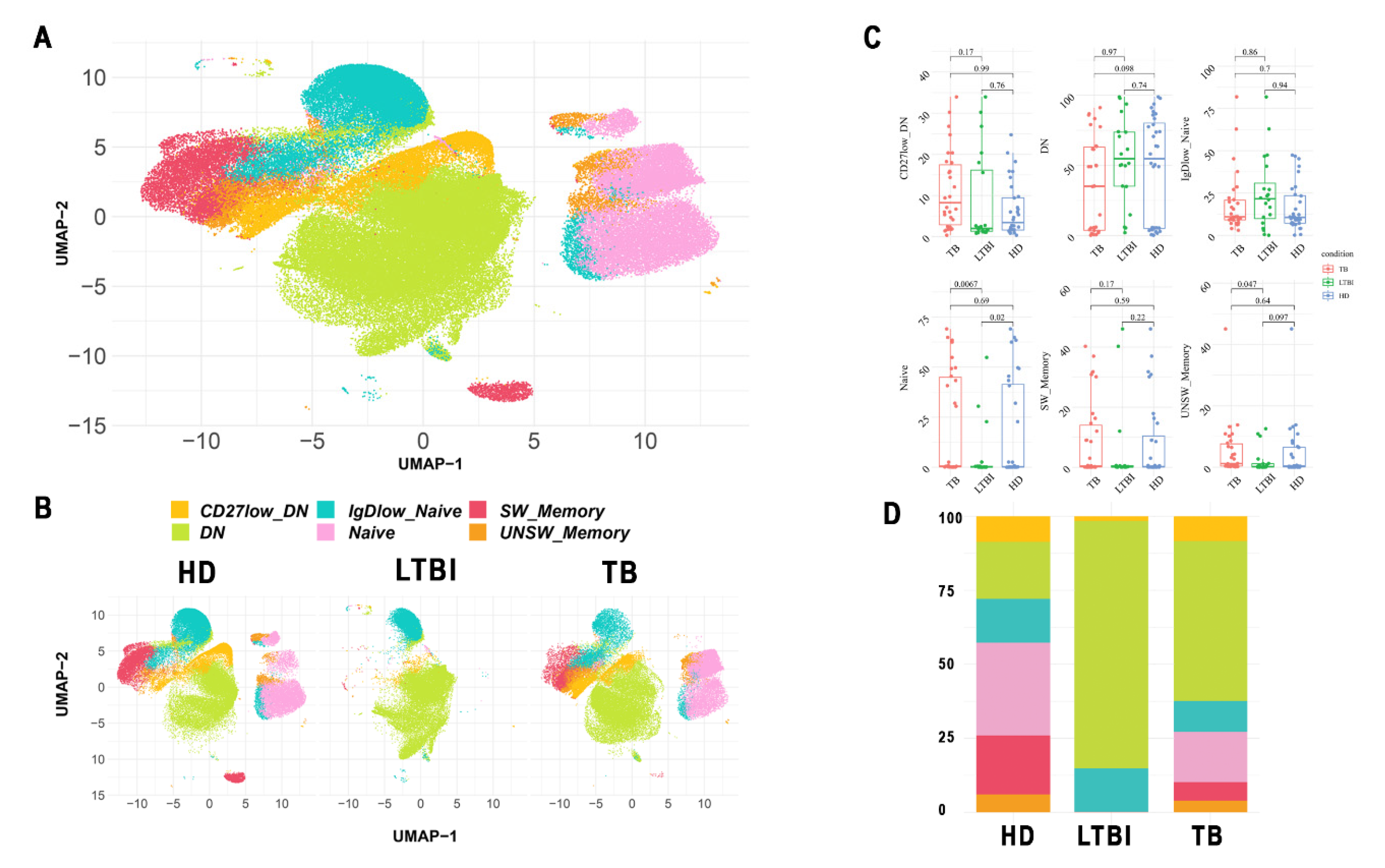
3.1. Circulating B lymphocyte Profiles during M. tuberculosis Infection
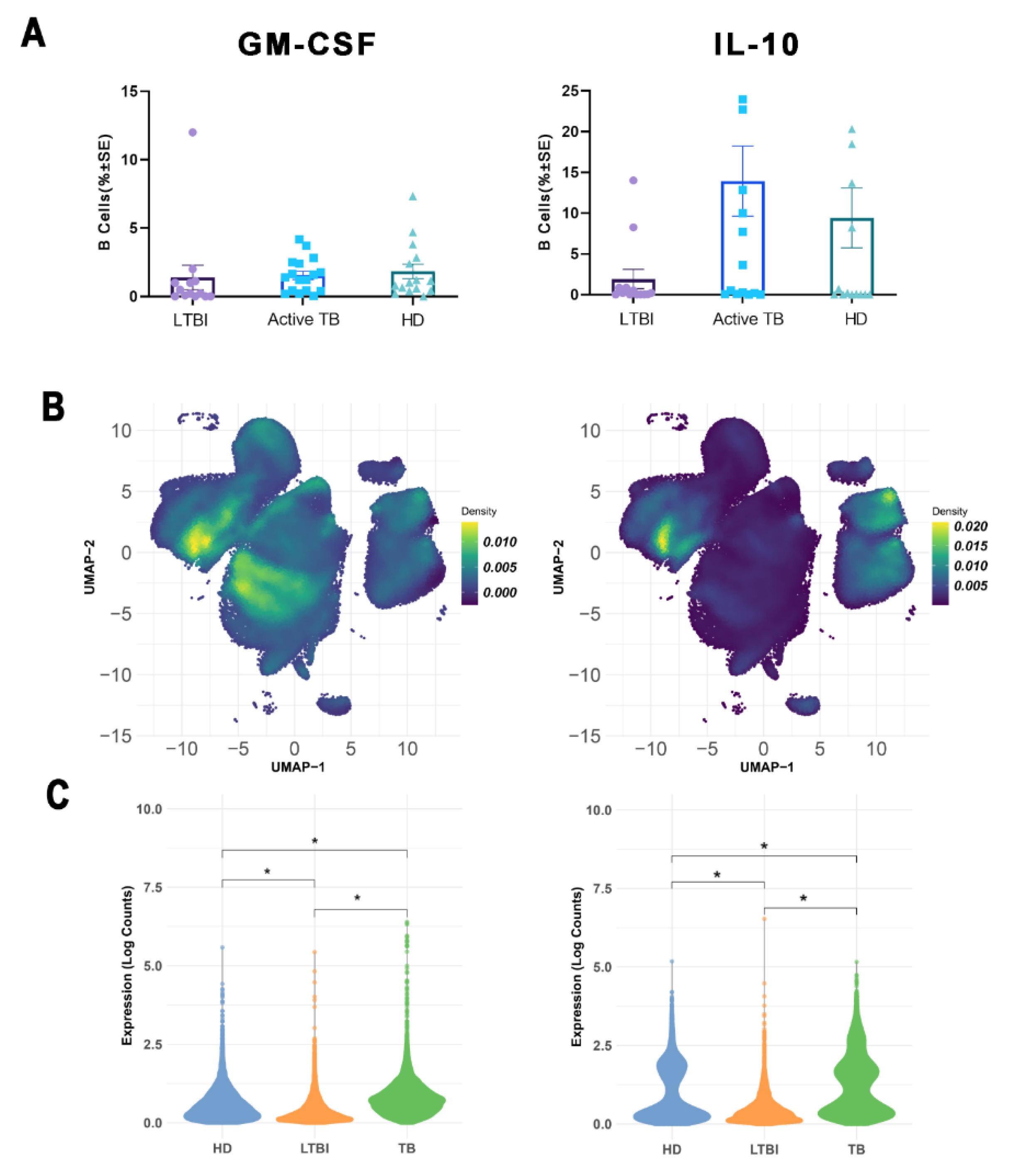
3.2. Effect of M. tuberculosis Infection on Pro-Inflammatory and Regulatory B Cell Subsets
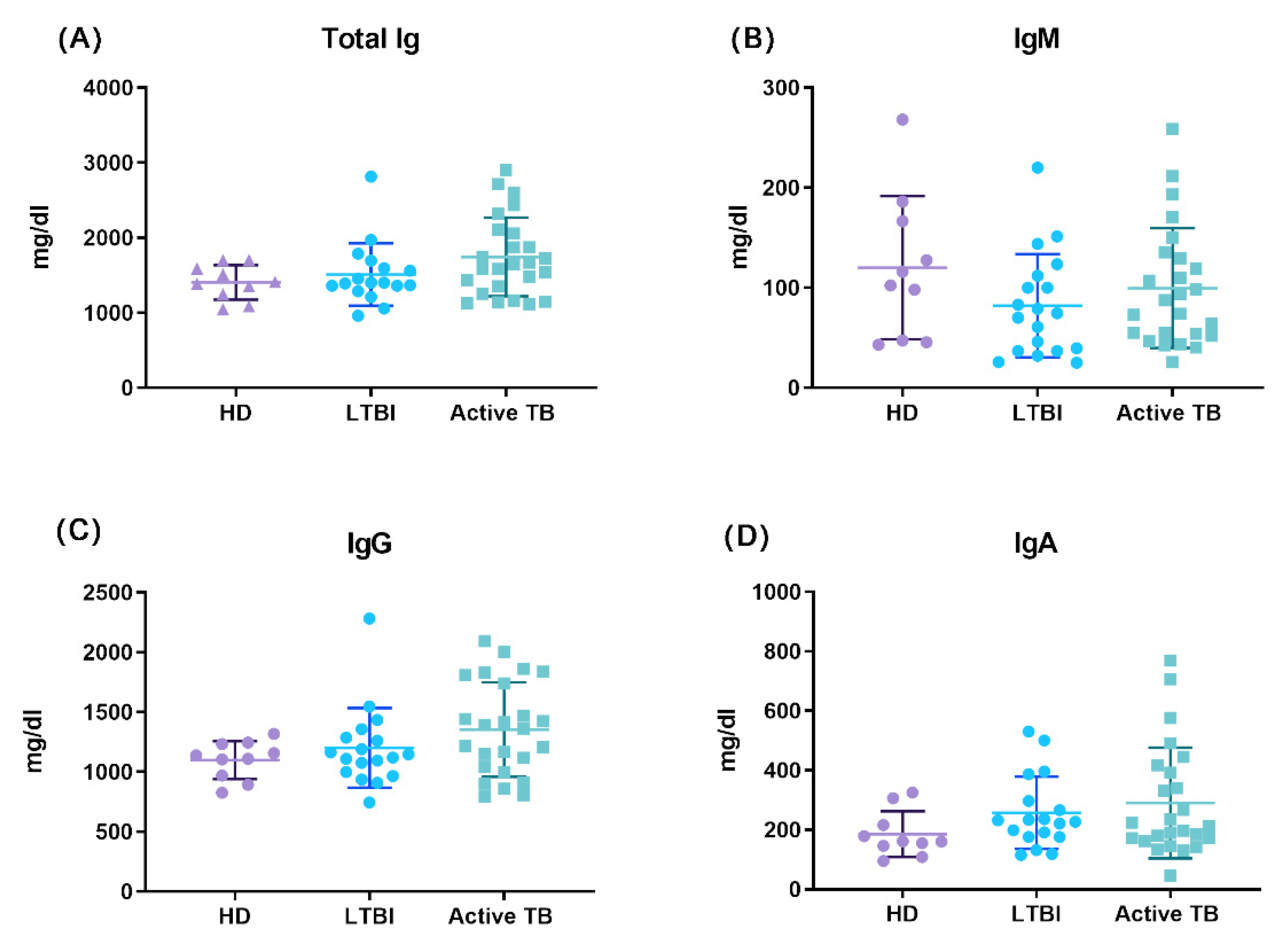
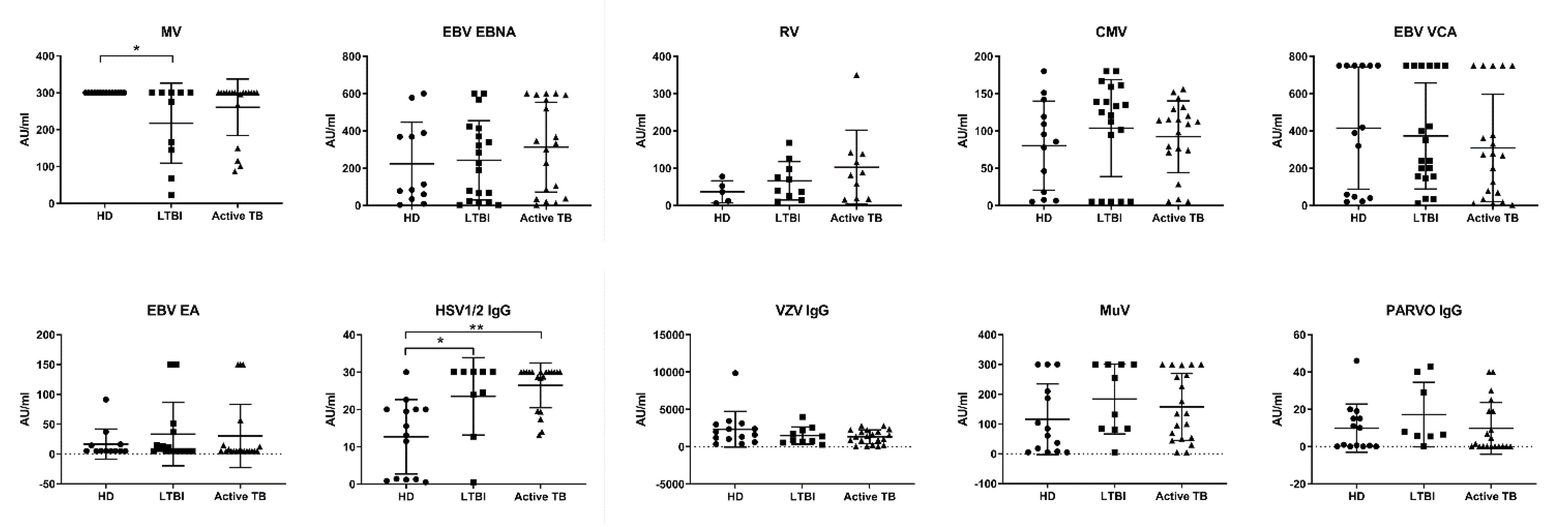
3.3. Impact of M. tuberculosis Infection on Antibody Repertoire and Preexisting Antibody Titers
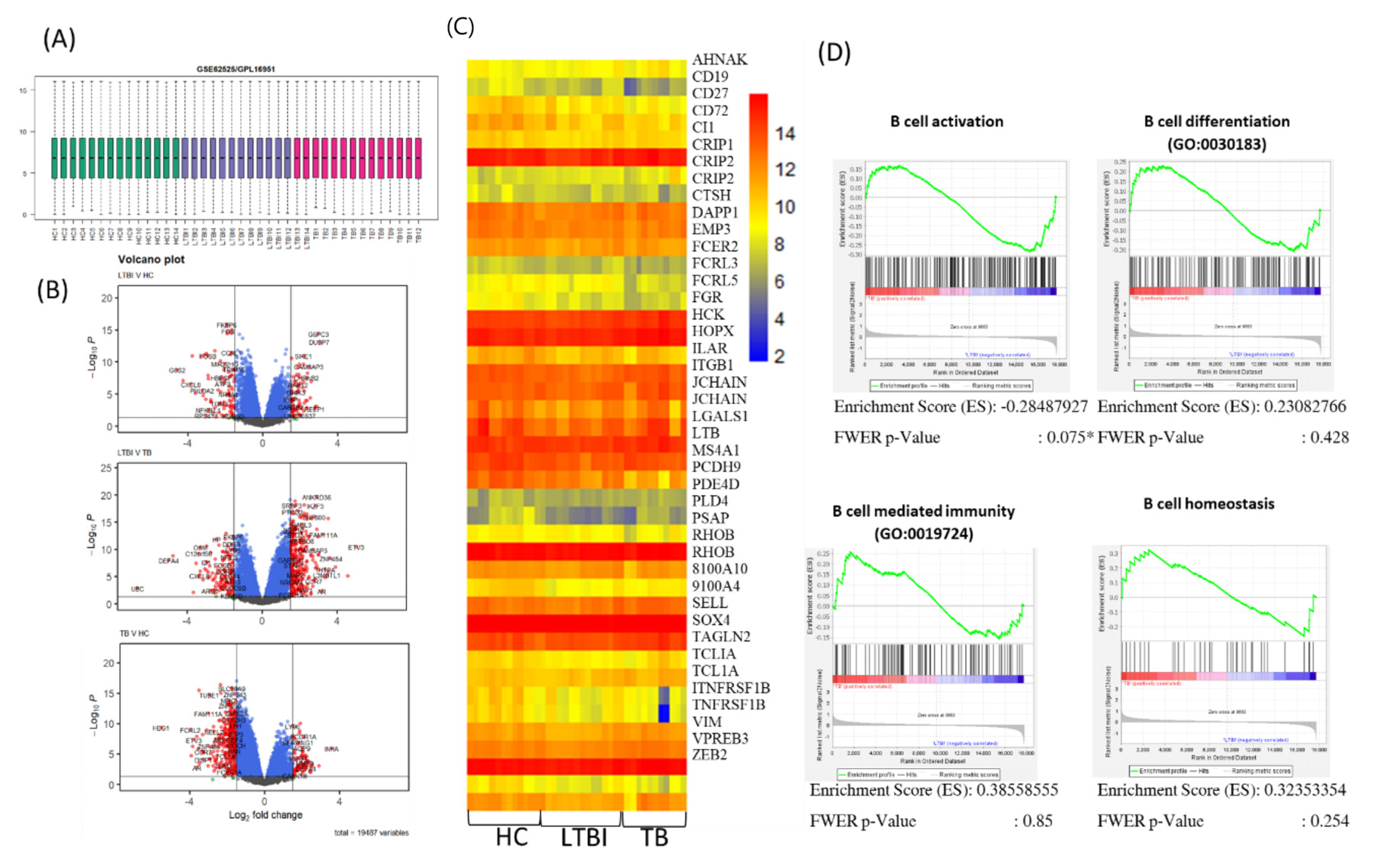
3.4. Transcriptional Profiles of Circulating B lymphocytes during M. tuberculosis Infection
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Netea, M.G.; van Crevel, R. (Eds.) BCG-Induced Protection: Effects on Innate Immune Memory; Elsevier: Amsterdam, The Netherlands, 2014. [Google Scholar]
- WHO. Global Tuberculosis Report 2021; World Health Organization: Geneva, Switzerland, 2021; Contract No.: 9789240037021. [Google Scholar]
- Cooper, A.M. Cell-Mediated Immune Responses in Tuberculosis. Annu. Rev. Immunol. 2009, 27, 393–422. [Google Scholar] [CrossRef] [PubMed]
- Walzl, G.; Ronacher, K.; Hanekom, W.; Scriba, T.; Zumla, A. Immunological biomarkers of tuberculosis. Nat. Rev. Immunol. 2011, 11, 343–354. [Google Scholar] [CrossRef]
- Caccamo, N.R.; Guggino, G.; Joosten, S.A.; Gelsomino, G.; Di Carlo, P.; Titone, L.; Galati, D.; Bocchino, M.; Matarese, A.; Salerno, A.; et al. Multifunctional CD4+ T cells correlate with active Mycobacterium tuberculosis infection. Eur. J. Immunol. 2010, 40, 2211–2220. [Google Scholar] [CrossRef] [PubMed]
- Harari, A.; Rozot, V.; Enders, F.B.; Perreau, M.; Stalder, J.M.; Nicod, L.P.; Cavassini, M.; Calandra, T.; Blanchet, C.L.; Jaton, K.; et al. Dominant TNF-α+ Mycobacterium tuberculosis–specific CD4+ T cell responses discriminate between latent infection and active disease. Nat. Med. 2011, 17, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Basile, J.I.; Liu, R.; Mou, W.; Gao, Y.; Carow, B.; Rottenberg, M.E. Mycobacteria-Specific T Cells Are Generated in the Lung During Mucosal BCG Immunization or Infection With Mycobacterium tuberculosis. Front. Immunol. 2020, 11, 566319. [Google Scholar] [CrossRef] [PubMed]
- Mogues, T.; Goodrich, M.E.; Ryan, L.; LaCourse, R.; North, R.J. The Relative Importance of T Cell Subsets in Immunity and Immunopathology of Airborne Mycobacterium tuberculosis Infection in Mice. J. Exp. Med. 2001, 193, 271–280. [Google Scholar] [CrossRef]
- La Manna, M.P.; Orlando, V.; Prezzemolo, T.; Di Carlo, P.; Cascio, A.; Delogu, G.; Poli, G.; Sullivan, L.C.; Brooks, A.G.; Dieli, F.; et al. HLA-E–restricted CD8+ T lymphocytes efficiently control Mycobacterium tuberculosis and HIV-1 coinfection. Am. J. Respir. Cell Mol. Biol. 2020, 62, 430–439. [Google Scholar] [CrossRef]
- Flynn, J.L.; Goldstein, M.M.; Triebold, K.J.; Koller, B.; Bloom, B.R. Major histocompatibility complex class I-restricted T cells are required for resistance to Mycobacterium tuberculosis infection. Proc. Natl. Acad. Sci. USA 1992, 89, 12013–12017. [Google Scholar] [CrossRef]
- Lu, L.L.; Chung, A.W.; Rosebrock, T.R.; Ghebremichael, M.; Yu, W.H.; Grace, P.S.; Schoen, M.K.; Tafesse, F.; Martin, C.; Leung, V.; et al. A Functional Role for Antibodies in Tuberculosis. Cell 2016, 167, 433–443.e14. [Google Scholar] [CrossRef]
- Khera, A.K.; Afkhami, S.; Lai, R.; Jeyanathan, M.; Zganiacz, A.; Mandur, T.; Hammill, J.; Damjanovic, D.; Xing, Z. Role of B Cells in Mucosal Vaccine–Induced Protective CD8+ T Cell Immunity against Pulmonary Tuberculosis. J. Immunol. 2015, 195, 2900–2907. [Google Scholar] [CrossRef] [Green Version]
- Dyatlov, A.V.; Apt, A.S.; Linge, I.A. B lymphocytes in anti-mycobacterial immune responses: Pathogenesis or protection? Tuberculosis 2019, 114, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Segura-Cerda, C.A.; Marquina-Castillo, B.; Lozano-Ordaz, V.; Mata-Espinosa, D.; Barrios-Payán, J.A.; López-Torres, M.O.; Aceves-Sánchez, M.d.; Bielefeldt-Ohmann, H.; Hernández-Pando, R.; Flores-Valdez, M.A. BCG and BCGΔBCG1419c protect type 2 diabetic mice against tuberculosis via different participation of T and B lymphocytes, dendritic cells and pro-inflammatory cytokines. npj Vaccines 2020, 5, 21. [Google Scholar] [CrossRef]
- Rijnink, W.F.; Ottenhoff, T.H.; Joosten, S.A. B-Cells and Antibodies as Contributors to Effector Immune Responses in Tuberculosis. Front. Immunol. 2021, 12, 640168. [Google Scholar] [CrossRef] [PubMed]
- van Rensburg, I.C.; Loxton, A.G. Killer (FASL regulatory) B cells are present during latent TB and are induced by BCG stimulation in participants with and without latent tuberculosis. Tuberculosis 2018, 108, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Grace, P.S.; Dolatshahi, S.; Lu, L.L.; Cain, A.; Palmieri, F.; Petrone, L.; Fortune, S.M.; Ottenhoff, T.H.M.; Lauffenburger, D.A.; Goletti, D.; et al. Antibody Subclass and Glycosylation Shift Following Effective TB Treatment. Front. Immunol. 2021, 12, 679973. [Google Scholar] [CrossRef] [PubMed]
- Bitencourt, J.; Peralta-Álvarez, M.P.; Wilkie, M.; Jacobs, A.; Wright, D.; Li, S.; Harris, S.A.; Smith, S.G.; Elias, S.C.; White, A.D.; et al. Induction of Functional Specific Antibodies, IgG-Secreting Plasmablasts and Memory B Cells Following BCG Vaccination. Front. Immunol. 2021, 12, 798207. [Google Scholar] [CrossRef]
- Tamburini, B.; Badami, G.D.; Azgomi, M.S.; Dieli, F.; La Manna, M.P.; Caccamo, N. Role of hematopoietic cells in Mycobacterium tuberculosis infection. Tuberculosis 2021, 130, 102109. [Google Scholar] [CrossRef]
- Baldridge, M.; King, K.Y.; Boles, N.C.; Weksberg, D.C.; Goodell, M.A. Quiescent haematopoietic stem cells are activated by IFN-γ in response to chronic infection. Nature 2010, 465, 793–797. [Google Scholar] [CrossRef]
- Khan, N.; Downey, J.; Sanz, J.; Kaufmann, E.; Blankenhaus, B.; Pacis, A.; Pernet, E.; Ahmed, E.; Cardoso, S.; Nijnik, A.; et al. M. tuberculosis Reprograms Hematopoietic Stem Cells to Limit Myelopoiesis and Impair Trained Immunity. Cell 2020, 183, 752–770.e22. [Google Scholar] [CrossRef]
- Du Plessis, W.J.; Keyser, A.; Walzl, G.; Loxton, A.G. Phenotypic analysis of peripheral B cell populations during Mycobacterium tuberculosis infection and disease. J. Inflamm. 2016, 13, 23. [Google Scholar] [CrossRef] [Green Version]
- Hernández, J.; Velazquez, C.; Valenzuela, O.; Zepeda, R.E.R.; Ruiz-Bustos, E.; Navarro, M.; Garibay-Escobar, A. Low number of peripheral blood B lymphocytes in patients with pulmonary tuberculosis. Immunol. Investig. 2010, 39, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Barcelos, W.; Martins-Filho, O.A.; Guimarães, T.M.P.D.; Oliveira, M.H.P.; Spíndola-de-Miranda, S.; Carvalho, B.N.; de Toledo, V.D.P.C.P. Peripheral blood mononuclear cells immunophenotyping in pulmonary tuberculosis patients before and after treatment. Microbiol. Immunol. 2006, 50, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.K.; Leisching, G.R.; Snyders, C.I.; Gutschmidt, A.; Van Rensburg, I.C.; Loxton, A.G. Immunoglobulin profile and B-cell frequencies are altered with changes in the cellular microenvironment independent of the stimulation conditions. Immun. Inflamm. Dis. 2020, 8, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zheng, X.; Zhang, J.; Zhu, Y.; Zhu, X.; Liu, H.; Zeng, M.; Graner, M.W.; Zhou, B.; Chen, X. CD19+CD1d+CD5+ B cell frequencies are increased in patients with tuberculosis and suppress Th17 responses. Cell. Immunol. 2012, 274, 89–97. [Google Scholar] [CrossRef]
- Joosten, S.A.; Van Meijgaarden, K.E.; Del Nonno, F.; Baiocchini, A.; Petrone, L.; Vanini, V.; Smits, H.; Palmieri, F.; Goletti, D.; Ottenhoff, T.H.M. Patients with Tuberculosis Have a Dysfunctional Circulating B-Cell Compartment, Which Normalizes following Successful Treatment. PLoS Pathog. 2016, 12, e1005687. [Google Scholar] [CrossRef] [PubMed]
- La Manna, M.P.; Orlando, V.; Dieli, F.; Di Carlo, P.; Cascio, A.; Cuzzi, G.; Palmieri, F.; Goletti, D.; Caccamo, N. Quantitative and qualitative profiles of circulating monocytes may help identifying tuberculosis infection and disease stages. PLoS ONE 2017, 12, e0171358. [Google Scholar] [CrossRef]
- Botta, C.; Maia, C.D.S.; Garcés, J.-J.; Termini, R.; Perez, C.; Manrique, I.; Burgos, L.; Zabaleta, A.; Alignani, D.; Sarvide, S.; et al. FlowCT for the analysis of large immunophenotypic data sets and biomarker discovery in cancer immunology. Blood Adv. 2022, 6, 690–703. [Google Scholar] [CrossRef]
- Subramanian, A.; Tamayo, P.; Mootha, V.K.; Mukherjee, S.; Ebert, B.L.; Gillette, M.A.; Paulovich, A.; Pomeroy, S.L.; Golub, T.R.; Lander, E.S.; et al. Gene set enrichment analysis: A knowledge-based approach for interpreting genome-wide expression profiles. Proc. Natl. Acad. Sci. USA 2005, 102, 15545–15550. [Google Scholar] [CrossRef]
- Petruccioli, E.; Scriba, T.J.; Petrone, L.; Hatherill, M.; Cirillo, D.M.; Joosten, S.A.; Ottenhoff, T.H.; Denkinger, C.M.; Goletti, D. Correlates of tuberculosis risk: Predictive biomarkers for progression to active tuberculosis. Eur. Respir. J. 2016, 48, 1751–1763. [Google Scholar] [CrossRef]
- Mina, M.J.; Kula, T.; Leng, Y.; Li, M.; de Vries, R.D.; Knip, M.; Siljander, H.; Rewers, M.; Choy, D.F.; Wilson, M.S.; et al. Measles virus infection diminishes preexisting antibodies that offer protection from other pathogens. Science 2019, 366, 599–606. [Google Scholar] [CrossRef] [Green Version]
- Petrova, V.N.; Sawatsky, B.; Han, A.X.; Laksono, B.M.; Walz, L.; Parker, E.; Pieper, K.; Anderson, C.A.; de Vries, R.D.; Lanzavecchia, A.; et al. Incomplete genetic reconstitution of B cell pools contributes to prolonged immunosuppression after measles. Sci. Immunol. 2019, 4, eaay6125. [Google Scholar] [CrossRef] [PubMed]
- Andersen, P.; Kaufmann, S.H.E. Novel vaccination strategies against tuberculosis. Cold Spring Harb. Perspect. Med. 2014, 4, a018523. [Google Scholar] [CrossRef] [PubMed]
- McShane, H. Tuberculosis vaccines: Beyond bacille Calmette–Guérin. Philos. Trans. R. Soc. B Biol. Sci. 2011, 366, 2782–2789. [Google Scholar] [CrossRef]
- Orme, I.M. Vaccine Development for Tuberculosis: Current Progress. Drugs 2013, 73, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Li, J.S.-Y.; Winslow, G.M. Survival, replication, and antibody susceptibility of Ehrlichia chaffeensis outside of host cells. Infect. Immun. 2003, 71, 4229–4237. [Google Scholar] [CrossRef] [PubMed]
- Woelbing, F.; Kostka, S.L.; Moelle, K.; Belkaid, Y.; Sunderkötter, C.; Verbeek, S.; Waisman, A.; Nigg, A.P.; Knop, J.; Udey, M.C.; et al. Uptake of Leishmania major by dendritic cells is mediated by Fcγ receptors and facilitates acquisition of protective immunity. J. Exp. Med. 2006, 203, 177–188. [Google Scholar] [CrossRef]
- Gibson-Corley, K.N.; Boggiatto, P.M.; Bockenstedt, M.M.; Petersen, C.A.; Waldschmidt, T.J.; Jones, D.E. Promotion of a Functional B Cell Germinal Center Response after Leishmania Species Co-Infection Is Associated with Lesion Resolution. Am. J. Pathol. 2012, 180, 2009–2017. [Google Scholar] [CrossRef]
- Rodriguez-Pinto, D.; Saravia, N.G.; McMahon-Pratt, D. CD4 T cell activation by B cells in human Leishmania (Viannia)infection. BMC Infect. Dis. 2014, 14, 108. [Google Scholar] [CrossRef]
- Lund, F.E.; Randall, T.D. Effector and regulatory B cells: Modulators of CD4+ T cell immunity. Nat. Rev. Immunol. 2010, 10, 236–247. [Google Scholar] [CrossRef]
- Maglione, P.J.; Chan, J. How B cells shape the immune response againstMycobacterium tuberculosis. Eur. J. Immunol. 2009, 39, 676–686. [Google Scholar] [CrossRef] [Green Version]
- Vinuesa, C.G.; Tangye, S.G.; Moser, B.; Mackay, C.R. Follicular B helper T cells in antibody responses and autoimmunity. Nat. Rev. Immunol. 2005, 5, 853–865. [Google Scholar] [CrossRef] [PubMed]
- Crotty, S. Follicular helper CD4 T cells (Tfh). Annu. Rev. Immunol. 2011, 29, 621–663. [Google Scholar] [CrossRef] [PubMed]
- Victora, G.D.; Nussenzweig, M.C. Germinal centers. Annu. Rev. Immunol. 2012, 30, 429–457. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.; Mehta, S.; Bharrhan, S.; Chen, Y.; Achkar, J.M.; Casadevall, A.; Flynn, J. (Eds.) The Role of B Cells and Humoral Immunity in Mycobacterium Tuberculosis Infection; Elsevier: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Chowdhury, R.R.; Vallania, F.; Yang, Q.; Angel, C.J.L.; Darboe, F.; Penn-Nicholson, A.; Rozot, V.; Nemes, E.; Malherbe, S.T.; Ronacher, K.; et al. Author Correction: A multi-cohort study of the immune factors associated with M. tuberculosis infection outcomes. Nature 2018, 564, E5. [Google Scholar] [CrossRef] [PubMed]
- Corominas, M.; Cardona, V.; Gonzalez, L.; Caylà, J.A.; Rufi, G.; Mestre, M.; Buendia, E. B-lymphocytes and co-stimulatory molecules in Mycobacterium tuberculosis infection. Int. J. Tuberc. Lung Dis. 2004, 8, 98–105. [Google Scholar]
- An, H.; Bai, X.; Liang, J.; Wang, T.; Wang, Z.; Xue, Y.; Liu, Y.; Wang, L.; Wu, X. The relationship between absolute counts of lymphocyte subsets and clinical features in patients with pulmonary tuberculosis. Clin. Respir. J. 2022, 16, 369–379. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HD | LTBI | Active TB | |
|---|---|---|---|
| Subjects | 16 | 20 | 25 |
| Male (%) | 9 (56) | 12 (60) | 14 (56) |
| Mean Age (±SD) | 34 (±12) | 47 (±14) | 52 (±18) |
| Origin | |||
| Italy (%) | 14 (87) | 14 (70) | 12 (48) |
| Eastern Europe (%) | 2 (13) | 5 (20) | |
| Asia (%) | 2 (10) | 1 (4) | |
| Africa (%) | 4 (20) | 7 (28) | |
| QFT-IT pos. (%) | 0 (0) | 20 (100) | 25 (100) |
| Microbiological pos. (%) | 15 (75) | ||
| ZN pos. (%) | 15 (75) | ||
| Molecular pos. (%) | 20 (80) | ||
| Tuberculosis localization | |||
| Lung (%) | 22 (88) | ||
| Lymph node (%) | 2 (8) | ||
| Disseminated (%) | 1 (4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Manna, M.P.; Shekarkar-Azgomi, M.; Badami, G.D.; Tamburini, B.; Dieli, C.; Di Carlo, P.; Fasciana, T.; Marcianò, V.; Lo Sasso, B.; Giglio, R.V.; et al. Impact of Mycobacterium tuberculosis Infection on Human B Cell Compartment and Antibody Responses. Cells 2022, 11, 2906. https://doi.org/10.3390/cells11182906
La Manna MP, Shekarkar-Azgomi M, Badami GD, Tamburini B, Dieli C, Di Carlo P, Fasciana T, Marcianò V, Lo Sasso B, Giglio RV, et al. Impact of Mycobacterium tuberculosis Infection on Human B Cell Compartment and Antibody Responses. Cells. 2022; 11(18):2906. https://doi.org/10.3390/cells11182906
Chicago/Turabian StyleLa Manna, Marco P., Mojtaba Shekarkar-Azgomi, Giusto D. Badami, Bartolo Tamburini, Costanza Dieli, Paola Di Carlo, Teresa Fasciana, Vito Marcianò, Bruna Lo Sasso, Rosaria V. Giglio, and et al. 2022. "Impact of Mycobacterium tuberculosis Infection on Human B Cell Compartment and Antibody Responses" Cells 11, no. 18: 2906. https://doi.org/10.3390/cells11182906