1. Introduction
Human umbilical cord-derived mesenchymal stem cells (UC−MSCs) are considered a promising cell source for autologous and allogeneic cell therapy because of their relatively low immunogenicity compared to mesenchymal stem cells (MSCs) from adult counterparts, in which HLA-ABC is expressed very weakly [
1,
2]. UC−MSCs have strong biological activity and differentiation capacity even after repeated amplification [
3]. UC−MSCs are also compliant with standard amplification in potentially large quantities due to their fast self-renewing capacity [
4,
5], and UC−MSC banks can be established to cater to market demand after drug approval. Therefore, UC−MSCs are considered a promising cell source for clinical cell therapy [
6,
7].
In cell therapy, MSC transplantation is usually carried out by local or transcatheter injection of cell suspension. However, generally, only 10–20% of injected cells are available at the injured area within a few hours or days after delivery, and only a few cells actively engraft in the affected tissue [
8]. In addition, attached cells are digested by enzymes to produce a cell suspension, which destroys cellular connexins and greatly reduces cell activity and function [
9]. Therefore, cell suspension injection causes significant loss and death of cells and uneven local distribution, which greatly reduces the expected therapeutic effects [
8]. Cell sheet technology, developed by Prof. Okano’s team [
9,
10], eliminates the problem of retention, helps to retain cells, and provides the appropriate lifespan for the transplanted MSCs. Using this technology, cell sheets were prepared and they improved the cardiac function in mouse [
10] and porcine [
11] myocardial infarction models.
For extensive clinical promotion, robust cell sheet production, preservation, and quality control systems conforming to Good Manufacturing Practice (GMP) regulations are essential elements of successful cell therapy.
To date, the reported cell sheet-forming medium has been either fetal bovine serum (FBS)-containing media or serum-free mesenchymal stem cell culture media [
12,
13]. As a kind of exogenous macromolecule protein, bovine serum albumin (BSA) in FBS-containing media can cause allergic reactions. Exogenous growth factors or research-grade human/animal extracts—additives for supporting cell growth—in serum-free mesenchymal stem cell culture media could also cause safety risks in humans. For instance, excessive exogenous growth factor residues in cell therapy final products may pose a carcinogenic risk in humans. In addition, research-grade reagent residues in cell therapy final products do not meet the GMP regulations because no safety evaluations have been conducted in humans. Therefore, the serum-containing and serum-free media commonly used are not suitable for clinically safe cell sheet preparation.
Following production, the cell sheet products need to be transported to the clinical site that will administer the cells; therefore, the cell sheet preservation method and solution need to be developed. Several teams have reported a cell sheet preservation method and solution, but cultured cell sheets were used for preservation in all studies [
14,
15,
16,
17]. When reaching the clinical site, a series of complex operations, such as cell sheet detaching, were needed before usage, which would introduce high risks to the final product. Thus, the preservation methods were not in compliance with the GMP guidelines.
In order to ensure consistency and quality controllability of the UC−MSC sheet products, a two-tiered cell bank system should be established and quality controlled as intermediate products in the production process according to the “ICH Q5D: Derivation and Characterization of Cell Substrates Used for Production of Biotechnological/Biological Products”. Generally, a two-tiered cell bank system includes master cell banks (MCBs) and working cell banks (WCBs), in which a batch of MCB is used to generate several batches of WCBs. Therefore, the final UC−MSC sheet products can be produced from the quality controlled WCBs to ensure batch-to-batch consistency.
In this study, the preparation and preservation technology for UC−MSC sheets, which complied with the GMP guidelines, was developed for use in clinical trials and preclinical studies. First, a safe UC−MSC sheet production technology was successfully developed to ensure drug safety and efficacy. Second, an effective UC−MSC sheet preservation technology was developed to ensure storage and transportation, from which UC−MSC sheets could be preserved for 24 h with cell viability greater than 70%. Third, quality standards involving product characteristics, safety, and functionality were established according to the “ICH Q5A: Viral Safety Evaluation of Biotechnology Products Derived from Cell Lines of Human or Animal Origin”, “ICH Q6B: Test Procedures and Acceptance Criteria for Biotechnological/Biological Products”, “Guiding Principles for Quality Control of Stem Cell Preparations and Preclinical Research”, “Guidelines for Cell Therapy Products and Evaluation Technology”, and our research results. Fourth, the production process of UC−MSC sheets on a large scale was standardized, including donor screening, cell bank establishment and quality control, and cell sheet production and quality control. Finally, three batches of trial production were conducted according to the standardized production process. All three batches of MCBs and WCBs in trial production met the established quality standards. UC−MSC sheets with tight cell connections and an intact extracellular matrix in the three batches of trial production express surface markers of mesenchymal stem cells, secrete a variety of growth factors, reduce the immune response, promote the formation of angiogenesis, and inhibit apoptosis of cardiomyocytes in vitro. Both the fresh and 24 h preserved UC−MSC sheets met the established quality standards.
2. Materials and Methods
2.1. Ethics Statements
Umbilical cord sample collection was approved by the OASIS International Hospital local ethics committee (No: LLPJ2018[001]). Written informed consent was obtained from the puerperas. Before parturition, puerperas should test negative for human immunodeficiency virus (HIV), human hepatitis B virus (HBV), human hepatitis C virus (HCV), Treponema pallidum (TP), human T-cell leukemia virus (HTLV), cytomegalovirus (CMV), and Epstein–Barr virus (EBV). Umbilical cord samples were preserved in sterile saline at 4 °C after collection and transferred to the laboratory within 24 h.
2.2. Cell Isolation and Culture
The human umbilical cord was washed with phosphate buffer saline (PBS) to remove blood. Then, blood vessels and tunica externa were removed, and Wharton’s jelly was separated. After being cut into small pieces, Wharton’s jelly was seeded into 100 mm Petri dishes coated with fetal bovine serum (FBS). Then, the Petri dishes were cultured at 37 °C, 5% CO2, and 95% humidity with umbilical cord mesenchymal stem cell (UC−MSC) medium consisting of minimum essential medium-α (α-MEM, Corning (Corning, NY, USA)), supplemented with 10% FBS (Gibco (Carlsbad, CA, USA)), 1% L-glutamine (Corning), 1% nonessential amino acid (NEAA, Gibco (Carlsbad, CA, USA)), and 20 IU/mL basic fibroblast growth factor (bFGF) (Langtai (Foshan, China)). UC−MSCs that migrated from the explants were defined as P0 UC−MSCs.
When reaching 90% confluence, UC−MSCs were detached using TrypLE (Gibco (Carlsbad, CA, USA)) and passaged to new flasks at a cell density of 2 × 104 cells/cm2. P1 UC−MSCs cryopreserved at a density of 2 × 106 cells/mL in cell freezing medium (FBS with 10% dimethyl sulfoxide (DMSO) (Sigma (St. Louis, MO, USA))) were defined as MCBs. UC−MSCs from the master cell bank (MCB) were recovered and passaged to P4 as mentioned above. Then, UC−MSCs at P4 were cryopreserved and defined as working cell banks (WCBs).
2.3. Cell Sheet Production and Preservation
UC−MSCs from the WCB were recovered and cultured to 100% confluence with UC−MSC medium. After being digested to single-cell suspension with TrypLE, UC−MSCs were washed three times with PBS to remove exogenous FBS and basic fibroblast growth factor (bFGF). Then, the UC−MSCs were suspended in a cell sheet-forming medium, which consisted of α-MEM supplemented with 0.1% human serum albumin (HSA) (Shandong Taibang, Taian, China). A total of 6 × 107 cells were seeded into 100 mm temperature-responsive culture dishes (ThermoFisher (Waltham, MA, USA)) and cultured at 37 °C with 5% CO2 and 95% humidity overnight. Then, the UC−MSC sheet was detached from the temperature-responsive culture dishes at room temperature (20–25 °C).
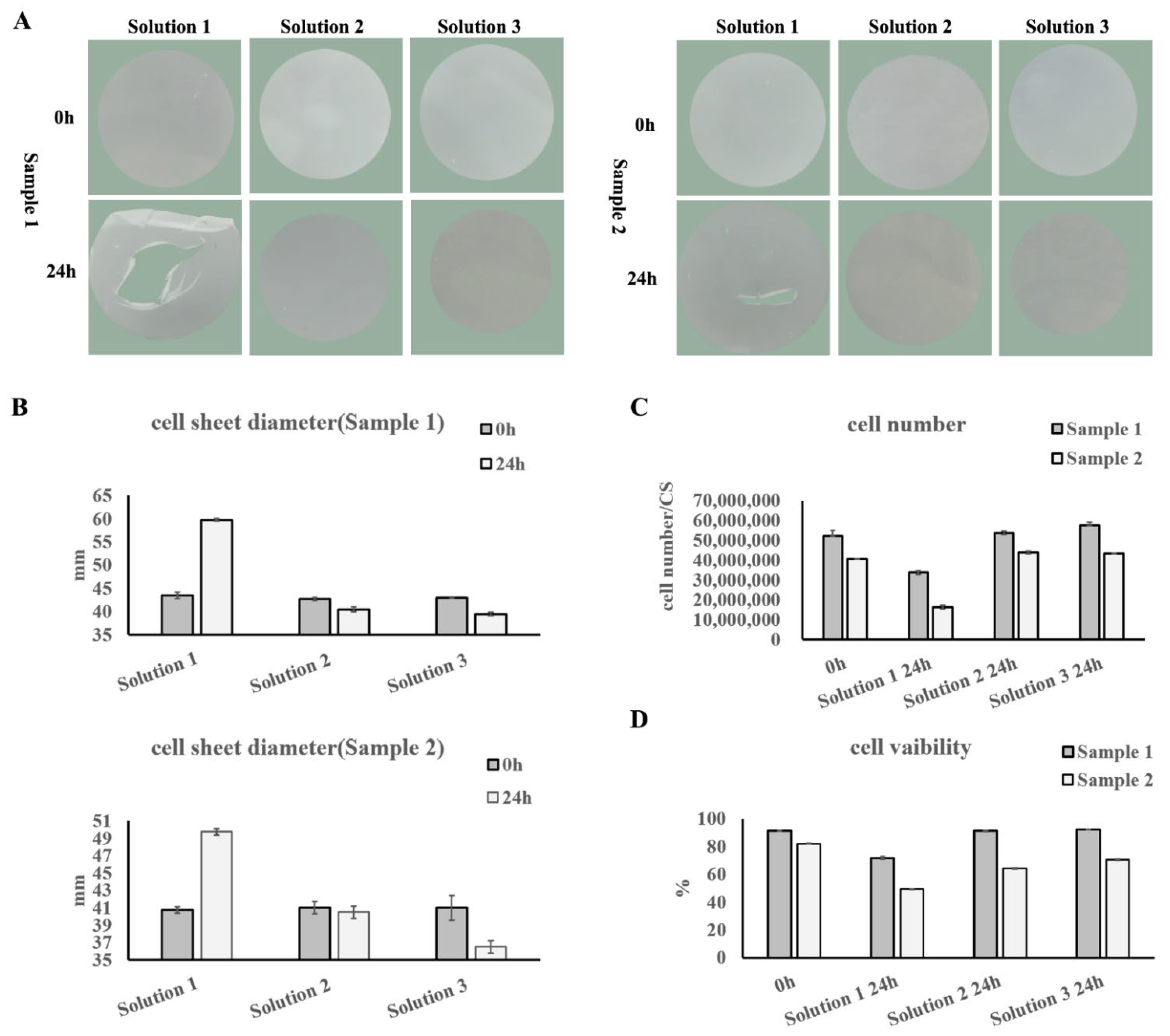
After washing with saline solution, 5–10 mL of the corresponding UC−MSC sheet preservation solution was added to the UC−MSC sheet for preservation at 4 °C. The preservation solutions were: (1) normal saline solution with 1% HSA (Solution 1); (2) a commercial preservation solution, which is a kind of category III medical device (Solution 2); (3) Hypothermosol (Biolife Solutions (Bothell, WA, USA)) (Solution 3).
2.4. Cell Amount, Cell Viability, and Cell Apoptosis Assays
Cell amount and viability were evaluated by Acridine Orange and Propidium Iodide (AOPI) staining and automatic fluorescent cell counter (Countstar S2 (Shanghai, China)) detection, according to the manufacturer’s instructions. Cell apoptosis was tested with the Annexin V-FITC Apoptosis Detection Kit (eBioscience (Carlsbad, CA, USA)), according to the manufacturer’s instructions.
Samples were prepared as follows. For MCB and WCB cells, UC−MSCs were recovered and suspended in UC−MSC medium for detection. For UC−MSC sheets, the UC−MSC sheet was digested by TrypLE into single-cell suspension for detection.
2.5. Cell Growth Curve
UC−MSCs in MCB and WCB were recovered and seeded into 96-well plates at a concentration of 6000 cells/well in UC−MSC medium. Cell growth was evaluated each day by Cell Counting Kit-8 (CCK-8) assay (TransGen (Beijing, China)), according to the manufacturer’s instructions.
2.6. Cell Cycle Analysis
UC−MSCs in MCB and WCB were recovered and seeded in T75 flasks at a cell density of 2 × 104 cells/cm2. When reaching 60–70% confluence, UC−MSCs were harvested, and the cell cycle was tested with the Cell Cycle Detection Kit (KeyGEN Biotech (Nanjing, China)), according to the manufacturer’s instructions.
2.7. Colony-Forming Unit (CFU) Assay
UC−MSCs in MCB and WCB were recovered and seeded in 96-well plates at a concentration of 1 cell/well. After culturing for 14 days, wells containing 50 or more cells were counted with a microscope (CKX41, OLYMPUS, Tokyo, Japan). The colony formation proportion is = the ratio of the number of wells containing 50 or more cells in/the number of total seeding wells.
2.8. Cell Surface Marker Detection
UC−MSCs in MCB and WCB were recovered and seeded in T75 flasks at a cell density of 2 × 104 cells/cm2. When they reached 90–100% confluence, UC−MSCs were harvested for cell surface marker detection. For UC−MSC sheets, the sheet was digested using TrypLE into single-cell suspension for detection. UC−MSCs were aliquoted into 1 × 106 cells/tube in the staining buffer, consisting of phosphate buffer saline (PBS, Corning (Corning, NY, USA)), supplemented with 1% FBS (Gibco). Then, anti-CD73-FITC (BD (Becton, NJ, USA)), anti-CD90-FITC (BD), anti-CD105-APC (BioLegend (San Diego, CA, USA)), anti-CD11b-FITC (BD), anti-CD19-FITC (BioLegend), anti-CD34-PE (BioLegend), anti-CD45-FITC (BD), anti-HLA-DR-FITC (BD), anti-IgG-FITC (BD), anti-IgG-PE (BD), and anti-IgG-APC (BD) were added to the tubes separately. After staining for 30 min at room temperature in the dark, the cells were washed twice with PBS and resuspended in the staining buffer for flow cytometry analysis.
2.9. Differentiation Assays
UC−MSCs in MCB and WCB were recovered and resuspended in UC−MSC medium for differentiation. For UC−MSC sheets, the cell sheet was digested by TrypLE into single-cell suspension for differentiation.
For adipogenic differentiation, cells were seeded in 24-well plates at a density of 8 × 104 cells/well and cultured at 37 °C, 5% CO2, and 95% humidity. When the cells reached 100% confluence, the culture medium was changed to adipogenic differentiation medium (BI (Kibbutz Beit-Haemek, Israel)) to induce differentiation. After culturing for 14–21 days with medium change every three days, the cells were fixed and stained with an MSC Adipo-Staining Kit (VivaCell, Shanghai, China).
For osteogenic differentiation, cells were seeded in 24-well plates at a density of 4 × 104 cells/well and cultured at 37 °C, 5% CO2, and 95% humidity. When the cells reached 70% confluence, the culture medium was changed to osteogenic differentiation medium (BI) to induce differentiation. After culturing for 14–21 days with medium change every three days, the cells were fixed and stained with an MSC Osteo-Staining Kit (VivaCell).
For chondrogenic differentiation, cells were seeded in 15 mL tubes at a density of 4 × 105 cells/tube in chondrogenic differentiation medium (BI) as pellets and cultured at 37 °C, 5% CO2, and 95% humidity for 14–21 days with medium change every three days. The cells were fixed and stained with an MSC Chondro-Staining Kit (VivaCell).
2.10. Growth Factor Detection Assays
Cell banks: UC−MSCs in MCB and WCB were recovered and seeded in T75 flasks at a cell density of 2 × 104 cells/cm2. Twenty-four hours before cell passage, the culture medium was replaced with 10 mL fresh UC−MSC medium. When passaging cells, the culture medium was collected and centrifuged at 300× g for 5 min to remove dead cells for growth factor detection. The number of viable cells was monitored using AOPI in the automatic fluorescent cell counter to calculate the amount of factor secretion per 1 × 106 cells in 24 h.
Cell sheet-forming medium: Cell sheet-forming medium was collected and centrifuged at 300× g for 5 min to remove dead cells for growth factor detection.
Cell sheet reattachment medium: The freshly produced and 24 h preserved cell sheets were attached to 100 mm Petri dishes in UC−MSC medium and cultured for 24 h. The medium was collected and centrifuged at 300× g for 5 min to remove dead cells for growth factor detection.
Hepatocyte growth factor (HGF) (Invitrogen (Carlsbad, CA, USA)), vascular endothelial growth factor (VEGF) (NOVUS (Centennial, CO, USA)), interleukin-8 (IL-8) (R&D (Minneapolis, MN, USA)), and interleukin-6 (IL-6) (NOVUS) were quantified using commercial enzyme-linked immunosorbent assay (ELISA) kits, following the manufacturer’s instructions.
2.11. High-Risk Substance Residue Detection Assays
The final cell washing solution before cell sheet fabrication was used for bFGF residue detection by following the manufacturer’s instructions for the Human bFGF ELISA Kit (Life Technologies (Carlsbad, CA, USA)).
Cell sheets were digested with 3 mL TrypLE, and the digestion was quenched with 7 mL PBS. The single-cell suspension was centrifuged at 300× g for 5 min, and the supernatant was harvested for human serum albumin (HSA) residue detection by following the manufacturer’s instructions for the Human Albumin ELISA Kit (BETHYL (Hamburg, Germany)).
Cell sheets were digested with 1 mL TrypLE supplemented with 50 μL 20% HSA, and the digestion was quenched with 1 mL cell sheet-forming medium. The single-cell suspension was centrifuged at 300× g for 5 min, and the supernatant was harvested for bovine serum albumin (BSA) and gentamicin residue detection by following the manufacturer’s instructions for the Bovine Albumin ELISA Kit (BETHYL) and GENTAMINCIN ELISA Kit (REAGEN (San Diego, CA USA)), respectively.
Cell sheets were harvested and lysed with 5 mL lysis buffer, which consisted of normal saline supplemented with protease inhibitor (Roche (Basel, Switzerland)), by a repeated liquid nitrogen freeze–thaw method. The lysate was centrifuged at 12,000× g for 20 min at 4 °C, and the supernatant was harvested for TrypLE and fibrinogen residue detection by following the manufacturer’s instructions for the TrypLE ELISA Kit (JunYan (Guangzhou, China)) and Human Fibrinogen ELISA Kit (Novus (Centennial, CO, USA)), respectively.
The residual amount of bFGF is presented in pg/mL. The residual amounts of BSA, HSA, gentamicin, TrypLE, and fibrinogen are presented in ng per cell sheet.
2.12. Immunoregulatory Test Assay
UC−MSCs in MCB and WCB were recovered and seeded in 6-well plates at a density of 5 × 105 cells/well in UC−MSC medium. Cell sheets were digested as described in the “cell amount, cell viability and cell apoptosis assays” and seeded in 6-well plates at a density of 5 × 105 cells/well in UC−MSC medium. After overnight culture, the cells were treated with 10 μg/mL mitomycin to inhibit division. Then, human peripheral blood mononuclear cells (PBMCs) were recovered and seeded into wells with or without UC−MSCs in PBMC medium, which consisted of Roswell Park Memorial Institute 1640 (RPMI 1640) (Gibco (Carlsbad, CA, USA)) supplemented with 10% FBS, 1% L-glutamine, and 1% NEAA, at a density of 1 × 106 cells/well.
For Th1 lymphocyte detection, PBMCs were co-cultured with UC−MSCs overnight. Cell Stimulation Cocktail (plus protein transport inhibitors) (500X) (eBioscience (Carlsbad, CA, USA)) was added to the wells for Th1 lymphocyte activation, according to the manufacturer’s descriptions. PBMCs co-cultured with UC−MSCs without activation were used as the negative control. PBMCs cultured alone with activation were used as the positive control. Then, the proportions of Th1 lymphocytes were detected by anti-CD3-APC (BD), anti-CD8-FITC (BD), and anti-IFNγ-PE (BD) staining. A minimum of 10,000 events were acquired on a BD FACS Canto II flow cytometer, and the proportions of CD3+CD8−IFNγ+ Th1 lymphocytes were analyzed using the FlowJo VX software (BD (Becton, NJ, USA)).
For lymphocyte proliferation detection, 10 μg/mL phytohemagglutinin M (PHA-M) (Sigma (St. Louis, MO, USA)) was added to activate PBMCs co-cultured with UC−MSCs. PBMCs co-cultured with UC−MSCs without activation were used as the negative control. PBMCs cultured alone with PHA-M activation were used as the positive control. After 3 days of co-culturing, 10 μM BrdU was added to each well overnight. Then, the PBMCs were harvested and stained with the BrdU Staining Kit (eBioscience (Carlsbad, CA, USA)), according to the manufacturer’s instructions. A minimum of 10,000 events were acquired on a BD FACS Canto II flow cytometer, and the proportions of BrdU-positive proliferating lymphocytes were analyzed using the FlowJo software.
For TNFα detection, the culture medium in the lymphocyte proliferation detection before BrdU staining was harvested for tumor necrosis factor α (TNFα) detection by the Human TNFα ELISA Kit (Invitrogen (Carlsbad, CA, USA)), according to the manufacturer’s descriptions.
2.13. Angiogenesis Assay
Human umbilical vein epithelial cells were seeded in 48-well plates pre-coated with 100 μL Matrigel (BD) at a density of 1000 cells/well. Conditioned cell sheet-forming medium was added to the wells and cultured for 12 h. Fresh cell sheet-forming medium was used as the negative control. Images were taken using an inverted microscope and analyzed using the angiogenesis analyzer.
2.14. Cardiomyocyte Apoptosis Inhibition Assay
H9C2 rat cardiomyocytes were seeded in 6-well plates at a density of 15,000 cells/cm2. When the cells reached 80% confluence, 300 μM CoCl2 was added to the culture medium for 24 h to induce H9C2 apoptosis. Conditioned cell sheet-forming medium was added to the wells and cultures for 24 h. Fresh cell sheet-forming medium was used as the negative control. Cell apoptosis was tested with the Annexin V-FITC Apoptosis Detection Kit (eBioscience), according to the manufacturer’s instructions.
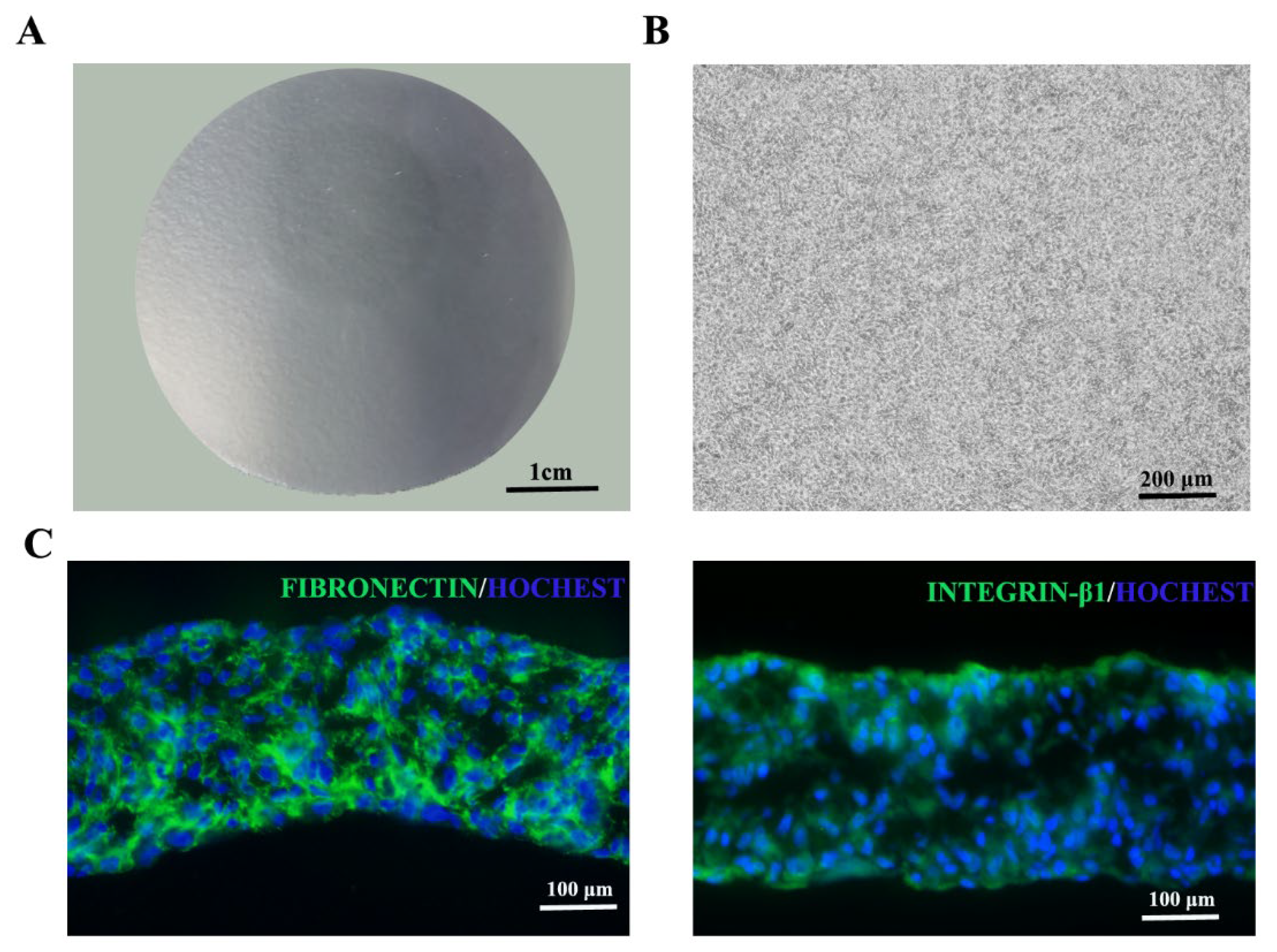
2.15. Immunofluorescence Staining
UC−MSC sheets were fixed with 4% paraformaldehyde and embedded in the optimal cutting temperature compound (Sakura Finetek (Tokyo, Japan)). After being cut into 10 μm sections using a cryostat (Leica), the cell sheets were blocked for 1 h at room temperature with blocking buffer, which consisted of PBS supplemented with 2% BSA. They were then labeled with primary antibodies against fibronectin (Abcam) or integrin β1 (Abcam) at 4 °C overnight, followed by incubation with FITC-conjugated donkey anti-rabbit antibody (Jackson ImmunoResearch (West Grove, PA, USA)) for visualization at room temperature for 2 h. Nuclei were counterstained with Hoechst (Life Technologies (Carlsbad, CA, USA)) at room temperature for 10 min. Then, the sections were assessed by confocal laser-scanning microscopy.
2.16. STR Authentication
UC−MSCs in MCB and WCB and cell sheets were prepared as described in the “cell amount, cell viability and cell apoptosis assay”. One million cells were collected and used for short tandem repeat (STR) authentication by the fluorescence STR method. The detected gene loci included D5S818, D13S317, D7S820, D16S539, VWA, TH01, TPOX, CSF1PO, D3S1358, Penta E, D2S441, D2S1338, Penta D, D10S1248, D19S433, D21S11, D18S51, D6S1043, D8S1179, D12S391, and FGA.
2.17. Telomerase Activity Detection
UC−MSCs in MCB and WCB and cell sheets were prepared as described in the “Cell amount, cell viability and cell apoptosis assay” section. One million cells were collected and used for telomerase activity detection with the fluorescence real-time quantitative PCR detection kit for telomerase activity (human) (KeyGEN BioTECH (Shanghai, China)), according to the manufacturer’s instructions.
2.18. Sterility Testing
The culture method was used for sterility testing. Briefly, cell sheet was digested with 3 mL TrypLE (Gibco (Carlsbad, CA, USA)) at 37 °C for 3 min. After quenching the digestion with 7 mL PBS, 3 mL of the cell suspension was used for sterility testing. For MCB and WCB cells, UC−MSCs were thawed, and 3 mL of the cell suspension was used for sterility testing. After membrane filtration and culture for 14 days, the results were evaluated.
2.19. Mycoplasma Detection
Cell culture supernatant before cryopreservation and cell sheet-forming supernatant before cell sheet detachment were tested by the culture method and indicated cell culture method.
For the quantitative polymerase chain reaction (Q-PCR) method, cells in MCB, WCB, and cell sheets were prepared as described in the “Cell amount, cell viability and cell apoptosis assay” section. One million cells were collected and used for mycoplasma detection with the Mycoplasma DNA Extraction and Purification Kit (magnetic bead method) and Mycoplasma DNA Detection Kit (PCR-Fluorescent Probe Method), both from Houzhou Shenke (Huzhou, China), according to the manufacturer’s instructions.
2.20. Endotoxin Test
Cell sheets were digested as described in “Sterility testing”, and the digestion supernatant was used for endotoxin test by the Gel Clot LAL Assay.
2.21. Exogenous Virus Detection
Exogenous virus was tested both in vitro and in vivo.
For in vitro different indicator cell inoculation and culture methods, monkey-derived Vero cells, human-derived MRC-5 cells, and human MSC cells were used as indicator cells.
For in vivo methods, mouse intraperitoneal and intracerebral vaccination, suckling mouse intraperitoneal and intracerebral vaccination, 5–6 days of chicken embryo yolk sac vaccination, and 9–11 days of chicken embryo allantois vaccination were conducted.
2.22. Bovine Virus Detection
The cell culture and fluorescent antibody detection methods were used for bovine virus detection.
2.23. Human Virus Detection
Either cell culture supernatant or one million cells was used for HIV, HBV, HCV, CMV, EBV, TP, Human cell virus B19 (HB19), and Human spore virus type 6 (HHV-6) detection using the following kits according to the manufacturer’s instructions: Human Immunodeficiency Virus Type I (HIV-1) Nucleic Acid Quantitative Determination Kit (PCR-Fluorescence Probe Method), Hepatitis B virus nucleic acid determination kit (PCR fluorescent probe method), Hepatitis C virus nucleic acid determination kit (PCR fluorescent probe method), Human cytomegalovirus nucleic acid quantitative detection kit (PCR fluorescence method), EB virus nucleic acid amplification (PCR) fluorescence quantitative detection kit, Treponema pallidum nucleic acid detection kit (fluorescence PCR method), Human cell virus B19 nucleic acid detection kit (PCR-fluorescent probe method), and Human spore virus type 6 nucleic acid detection kit (PCR-fluorescent probe method). The HIV, HBV, HCV, CMV, EBV, HB19, and HHV-6 kits were from Zhongshan Da’an (Guangzhou, China), and the TP kit was from Suzhou Tianlong (Suzhou, China).
2.24. Retroviral Detection
Product-enhanced reverse transcriptase assay (PERT) method was used for retroviral detection.
4. Discussion
To meet the needs of clinical trials for product safety, quality consistency, and large quantity, we developed the production and preservation technology of umbilical cord mesenchymal stem cell (UC−MSC) sheets and established a large-scale production and multi-level quality control system conforming to Good Manufacturing Practice (GMP) regulations, which is in preparation for clinical trials of UC−MSC sheet products in the development stage of new drugs and which could lay the foundation for industrial large-scale production after the new drug is launched.
For cell sheet production, the culture medium and Petri dish coating matrix are two key factors. Due to the high density and multilayer cells in the cell sheet, the residual culture medium and coating matrix cannot be eliminated thoroughly by the cell sheet postharvest washing procedures. The safety and efficacy of UC−MSC sheets may be significantly influenced by the chosen media and Petri dish coating matrix.
According to the GMP guidelines and cell therapy drug standards, the safe cell sheet-forming medium with simple composition, containing only a basic cell culturing medium (minimum essential medium-α (α-MEM)) and a certain concentration of human serum albumin (HSA) (parenteral drug), and the safe coating matrix, fibrinogen, a component of the human fibrin sealant kit (drug), were developed for cell sheet production in this study. Therefore, the cell sheet products are safe and GMP compliant.
The preparation of cell sheets requires a large number of cells, in the range of 20–100 million UC−MSCs/sheet. To meet the huge demand for expanded cells, expansion processes need to be in place. In fact, exogenous growth factor basic fibroblast growth factor (bFGF), a spray drug for external use, and fetal bovine serum (FBS), a research-grade animal extract, were still used in the cell culture process. Before cell sheet fabrication, FBS and bFGF were removed by constant washing and controlled in the final cell sheet products. Ideally, the culture medium in the whole process of cell sheet manufacture, including cell culture, should be chemically defined and not contain animal extracts, research-grade human extracts, or research-grade exogenous growth factors. Although several serum-free media have been investigated for human mesenchymal stem cell (MSC) expansion [
21,
22,
23,
24], ingredients of these mediums could not be risk-evaluated and controlled in final products due to their confidentiality, which does not meet the GMP guidelines and drug standards. In addition, these media contain a variety of research-grade exogenous growth factors or human/animal extracts, which would also cause safety risks for clinical applications. This is also our next challenge. We will further optimize the cell expansion medium to realize risk-free clinical safety in the manufacturing process.
To meet the needs of clinical trials for large quantity and quality consistency of the product, we standardized the production process of UC−MSC sheets on a large scale, including donor screening, cell bank establishment and quality control, and cell sheet production and quality control in this study. However, these are linear scale-ups based on strict production process control and strict quality control, including the UC−MSC culture process and UC−MSC sheet production process. The current production process cannot meet the needs of large-scale production after the product is put on the market. Industrial UC−MSC expansion and UC−MSC sheet production systems need to be developed. Now, research on large-scale cell expansion by automation equipment, which could monitor changes in various key parameters, such as pH and temperature, during cell culture is on the way and has been utilized in some cell types [
25,
26,
27,
28,
29]. Moreover, the Quantum
® equipment has been used for MSC expansion [
30]. Based on the GMP-compliant UC−MSC expansion and quality control systems in this study and the research foundations of automation cell expansion equipment, industrial large-scale expansion of UC−MSCs that could be used for UC−MSC sheet production will soon be realized. As for cell sheet fabrication, Ayako and colleagues researched an equipment that could allow 10 cell sheets to be simultaneously cultured in parallel [
31]. Based on the equipment and our UC−MSC sheet fabrication standard operation procedures (SOPs) and quality control systems, we will develop an automated cell sheet fabrication equipment for larger-scale UC−MSC sheet fabrication to meet the needs of new drug launches in the future.
Following production, the cell sheet products need to be transported to the clinical site that will administer the products. Although the cell sheet preservation technology, which was compliant with the GMP practice, developed in this study confirmed the safety of the cell sheets in the process of transportation and preservation before clinical use, limitations still existed. The validity period of the UC−MSC sheets was only 24 h, which limits the time for cell sheet transplantation for clinical application. Therefore, further study is needed to develop long-term preservation or freezing technology for cell sheets, including cryopreservation in liquid nitrogen technology. Several teams have successfully cryopreserved epithelial cell sheets [
32,
33]. When thawed, the epithelial cell sheets maintained a tissue repair function [
33]. With the development of tissue cryopreservation technology, cryopreserving mesenchymal stem cell sheets would soon be realized.
UC−MSC sheets produced and preserved according to the process described in this study express surface markers of mesenchymal stem cells, secrete a variety of growth factors, reduce the immune response, promote the formation of microvasculature, and inhibit apoptosis of cardiomyocytes in vitro. For the safety of UC−MSC sheets, our other study showed that there was no tumor formation, and the cell sheets only existed in the transplanted tissues or organs in Severe Combined Immunodeficient (SCID) mice [
34]. For the function of UC−MSC sheets, the research results showed UC−MSC sheets could obviously improve left ventricular heart function, and ejection fraction (EF) improved from 30% to 50% in mouse infarction models [
10] and from 40% to 67% in porcine infarction models [
34]. These all indicated that the UC−MSC sheets in this study could be used as a cell therapy drug in future clinical trials after being administrated by the National Medical Products Administration.















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}