
Cyclin-Dependent Kinase Subunit 2 (CKS2) as a Prognostic Marker for Stages I–III Invasive Non-Mucinous Lung Adenocarcinoma and Its Role in Affecting Drug Sensitivity

Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinicopathological Slides
2.2. Transcriptome Data
2.3. Immunohistochemical Staining
2.4. Acquiring Drug Sensitivity Data
2.5. Functional Enrichment Analysis
2.6. Statistical Analysis
3. Results
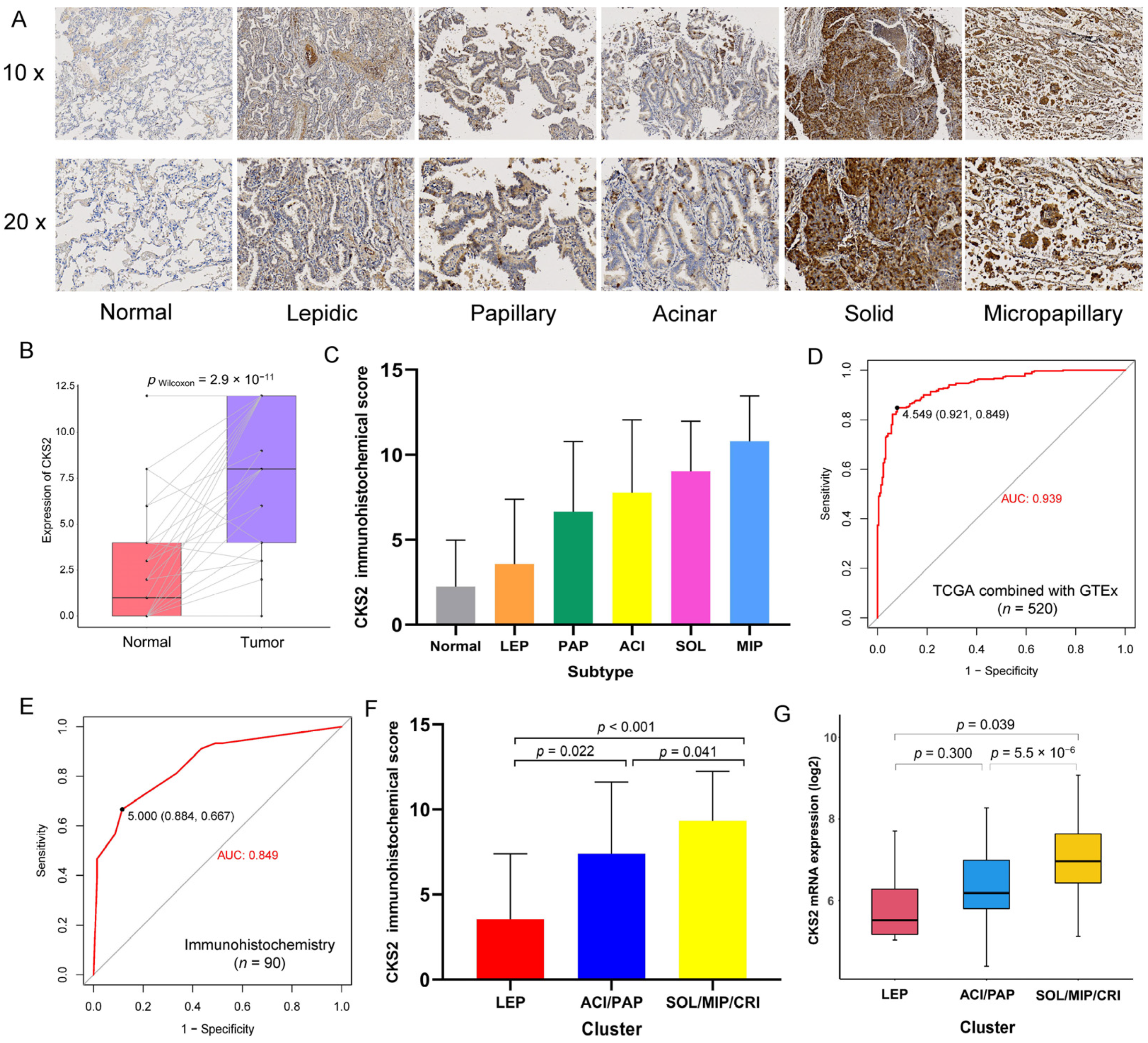
3.1. Expression of CKS2 in Stages I–III Invasive Non-Mucinous Lung Adenocarcinoma
3.2. Prognostic Significance of CKS2 and Different Histological Subtype Clusters
3.3. Relationship between CKS2 and MKI67 and PCNA
3.4. CKS2 Immunohistochemical Score and Clinicopathological Parameters
3.5. CKS2 and Drug Sensitivity
3.6. CKS2 and Immune Cell Infiltration
3.7. The Underlying Mechanism of CKS2 Aberrant Expression
3.8. Enrichment Analysis of Biological Functions Related to CKS2
3.9. CKS2 Protein-Protein Interactions (PPI) Network
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Herbst, R.S.; Morgensztern, D.; Boshoff, C. The biology and management of non-small cell lung cancer. Nature 2018, 553, 446–454. [Google Scholar] [CrossRef]
- Osmani, L.; Askin, F.; Gabrielson, E.; Li, Q.K. Current WHO guidelines and the critical role of immunohistochemical markers in the subclassification of non-small cell lung carcinoma (NSCLC): Moving from targeted therapy to immunotherapy. Semin. Cancer Biol. 2018, 52, 103–109. [Google Scholar] [CrossRef]
- Nicholson, A.G.; Tsao, M.S.; Beasley, M.B.; Borczuk, A.C.; Brambilla, E.; Cooper, W.A.; Dacic, S.; Jain, D.; Kerr, K.M.; Lantuejoul, S.; et al. The 2021 WHO classification of lung tumors: Impact of advances since 2015. J. Thorac. Oncol. 2022, 17, 362–387. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Noguchi, M.; Nicholson, A.G.; Geisinger, K.R.; Yatabe, Y.; Beer, D.G.; Powell, C.A.; Riely, G.J.; Van Schil, P.E.; et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J. Thorac. Oncol. 2011, 6, 244–285. [Google Scholar] [CrossRef] [Green Version]
- Moreira, A.L.; Ocampo, P.S.; Xia, Y.; Zhong, H.; Russell, P.A.; Minami, Y.; Cooper, W.A.; Yoshida, A.; Bubendorf, L.; Papotti, M.; et al. A grading system for invasive pulmonary adenocarcinoma: A proposal from the International Association for the Study of Lung Cancer Pathology Committee. J. Thorac. Oncol. 2020, 15, 1599–1610. [Google Scholar] [CrossRef]
- Tsuta, K.; Kawago, M.; Inoue, E.; Yoshida, A.; Takahashi, F.; Sakurai, H.; Watanabe, S.-I.; Takeuchi, M.; Furuta, K.; Asamura, H.; et al. The utility of the proposed IASLC/ATS/ERS lung adenocarcinoma subtypes for disease prognosis and correlation of driver gene alterations. Lung Cancer 2013, 81, 371–376. [Google Scholar] [CrossRef]
- Šutić, M.; Vukić, A.; Baranašić, J.; Försti, A.; Džubur, F.; Samaržija, M.; Jakopović, M.; Brčić, L.; Knežević, J. Diagnostic, predictive, and prognostic biomarkers in non-small cell lung cancer (NSCLC) management. J. Pers. Med. 2021, 11, 1102. [Google Scholar] [CrossRef]
- Demetrick, D.; Zhang, H.; Beach, D. Chromosomal mapping of the human genes CKS1 to 8q21 and CKS2 to 9q22. Cytogenet. Cell Genet 1996, 73, 250–254. [Google Scholar] [CrossRef]
- Lan, Y.; Zhang, Y.; Wang, J.; Lin, C.; Ittmann, M.M.; Wang, F. Aberrant expression of Cks1 and Cks2 contributes to prostate tumorigenesis by promoting proliferation and inhibiting programmed cell death. Int. J. Cancer 2008, 123, 543–551. [Google Scholar] [CrossRef] [Green Version]
- Martinsson-Ahlzén, H.-S.; Liberal, V.; Grünenfelder, B.R.; Chaves, S.R.; Spruck, C.H.; Reed, S.I. Cyclin-dependent kinase-associated proteins Cks1 and Cks2 are essential during early embryogenesis and for cell cycle progression in somatic cells. Mol. Cell Biol. 2008, 28, 5698–5709. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, F.; Matsuzaki, S.; Mimori, K.; Kita, Y.; Inoue, H.; Mori, M. Clinicopathological and biological significance of CDC28 protein kinase regulatory subunit 2 overexpression in human gastric cancer. Int. J. Oncol. 2011, 39, 361–372. [Google Scholar] [PubMed]
- Zhang, J.; Song, Q.; Liu, J.; Lu, L.; Xu, Y.; Zheng, W. Cyclin-dependent kinase regulatory subunit 2 indicated poor prognosis and facilitated aggressive phenotype of hepatocellular carcinoma. Dis. Markers 2019, 2019, 8964015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, R.; Feng, C.; Xu, Y. Cyclin-dependent kinase-associated protein Cks2 is associated with bladder cancer progression. J. Int. Med. Res. 2011, 39, 533–540. [Google Scholar] [CrossRef]
- Huang, N.; Wu, Z.; Hong, H.; Wang, X.; Yang, F.; Li, H. Overexpression of CKS2 is associated with a poor prognosis and promotes cell proliferation and invasion in breast cancer. Mol. Med. Rep. 2019, 19, 4761–4769. [Google Scholar] [CrossRef]
- Russell, P.A.; Wainer, Z.; Wright, G.M.; Daniels, M.; Conron, M.; Williams, R.A. Does lung adenocarcinoma subtype predict patient survival? A clinicopathologic study based on the new International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society international multidisciplinary lung adenocarcinoma classification. J. Thorac. Oncol. 2011, 6, 1496–1504. [Google Scholar]
- Maeser, D.; Gruener, R.F.; Huang, R.S. oncoPredict: An R package for predicting in vivo or cancer patient drug response and biomarkers from cell line screening data. Brief. Bioinform. 2021, 22, bbab260. [Google Scholar] [CrossRef]
- Ashburner, M.; Ball, C.A.; Blake, J.A.; Botstein, D.; Butler, H.; Cherry, J.M.; Davis, A.P.; Dolinski, K.; Dwight, S.S.; Eppig, J.T.; et al. Gene ontology: Tool for the unification of biology. The Gene Ontology Consortium. Nat. Genet. 2000, 25, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Consortium, G.O. The Gene Ontology resource: Enriching a GOld mine. Nucleic Acids Res. 2021, 49, D325–D334. [Google Scholar] [CrossRef]
- Kanehisa, M.; Goto, S. KEGG: Kyoto encyclopedia of genes and genomes. Nucleic Acids Res. 2000, 28, 27–30. [Google Scholar] [CrossRef]
- Kanehisa, M.; Sato, Y.; Kawashima, M.; Furumichi, M.; Tanabe, M. KEGG as a reference resource for gene and protein annotation. Nucleic Acids Res. 2016, 44, D457–D462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subramanian, A.; Tamayo, P.; Mootha, V.K.; Mukherjee, S.; Ebert, B.L.; Gillette, M.A.; Paulovich, A.; Pomeroy, S.L.; Golub, T.R.; Lander, E.S.; et al. Gene set enrichment analysis: A knowledge-based approach for interpreting genome-wide expression profiles. Proc. Natl. Acad. Sci. USA 2005, 102, 15545–15550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, L.; Banerji, S.; Murphy, L.; Dawe, D.E.; Harlos, C.; Myal, Y.; Nugent, Z.; Blanchard, A.; Penner, C.R.; Qing, G.; et al. Androgen receptor and Ki67 expression and survival outcomes in non-small cell lung cancer. Horm. Cancer 2018, 9, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Folescu, R.; Levai, C.M.; Grigoraş, M.L.; Arghirescu, T.S.; Talpoş, I.C.; Gîndac, C.M.; Zamfir, C.L.; Poroch, V.; Anghel, M.D. Expression and significance of Ki-67 in lung cancer. Rom. J. Morphol. Embryol. 2018, 59, 227–233. [Google Scholar]
- Strzalka, W.; Ziemienowicz, A. Proliferating cell nuclear antigen (PCNA): A key factor in DNA replication and cell cycle regulation. Ann. Bot. 2011, 107, 1127–1140. [Google Scholar] [CrossRef] [Green Version]
- Newman, A.M.; Liu, C.L.; Green, M.R.; Gentles, A.J.; Feng, W.; Xu, Y.; Hoang, C.D.; Diehn, M.; Alizadeh, A.A. Robust enumeration of cell subsets from tissue expression profiles. Nat. Methods 2015, 12, 453–457. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Hsu, P.J.; Chen, Y.-S.; Yang, Y.-G. Dynamic transcriptomic m6A decoration: Writers, erasers, readers and functions in RNA metabolism. Cell Res. 2018, 28, 616–624. [Google Scholar] [CrossRef] [Green Version]
- Salmena, L.; Poliseno, L.; Tay, Y.; Kats, L.; Pandolfi, P.P. A ceRNA hypothesis: The Rosetta Stone of a hidden RNA language? Cell 2011, 146, 353–358. [Google Scholar] [CrossRef] [Green Version]
- Zhao, M.; Feng, J.; Tang, L.L. Competing endogenous RNAs in lung cancer. Cancer Biol. Med. 2021, 18, 1–20. [Google Scholar] [CrossRef]
- Li, J.-H.; Liu, S.; Zhou, H.; Qu, L.-H.; Yang, J.-H. starBase v2. 0: Decoding miRNA-ceRNA, miRNA-ncRNA and protein–RNA interaction networks from large-scale CLIP-Seq data. Nucleic Acids Res. 2014, 42, D92–D97. [Google Scholar] [CrossRef] [Green Version]
- Ritchie, M.E.; Phipson, B.; Wu, D.; Hu, Y.; Law, C.W.; Shi, W.; Smyth, G.K. limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic Acids Res. 2015, 43, e47. [Google Scholar] [CrossRef] [PubMed]
- Szklarczyk, D.; Gable, A.L.; Nastou, K.C.; Lyon, D.; Kirsch, R.; Pyysalo, S.; Doncheva, N.T.; Legeay, M.; Fang, T.; Bork, P.; et al. The STRING database in 2021: Customizable protein–protein networks, and functional characterization of user-uploaded gene/measurement sets. Nucleic Acids Res. 2021, 49, D605–D612. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- Foley, E.A.; Kapoor, T.M. Microtubule attachment and spindle assembly checkpoint signalling at the kinetochore. Nat. Rev. Mol. Cell Biol. 2013, 14, 25–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weaver, B.A. How Taxol/paclitaxel kills cancer cells. Mol. Biol. Cell 2014, 25, 2677–2681. [Google Scholar] [CrossRef]
- Chen, K.; Shi, W.J. Autophagy regulates resistance of non-small cell lung cancer cells to paclitaxel. Tumour Biol. 2016, 37, 10539–10544. [Google Scholar] [CrossRef]
- Johnstone, T.C.; Suntharalingam, K.; Lippard, S.J. The next generation of platinum drugs: Targeted Pt (II) agents, nanoparticle delivery, and Pt (IV) prodrugs. Chem. Rev. 2016, 116, 3436–3486. [Google Scholar] [CrossRef] [Green Version]
- Wan, Z.; Wang, L.; Yang, D.; Li, P.; Liu, Q.; Wang, B. CKS2 Promotes the Growth in Non-Small-Cell Lung Cancer by Downregulating Cyclin-Dependent Kinase Inhibitor. Pathobiology 2022, 89, 13–22. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, M.; Wu, Y.; Yu, Y.; Zheng, Q.; Li, J. CKS2 Overexpression Correlates with Prognosis and Immune Cell Infiltration in Lung Adenocarcinoma: A Comprehensive Study based on Bioinformatics and Experiments. J. Cancer 2021, 12, 6964–6978. [Google Scholar] [CrossRef]
- Xiao, D.; Dong, S.; Yang, S.; Liu, Z. CKS2 and RMI2 are two prognostic biomarkers of lung adenocarcinoma. PeerJ 2020, 8, e10126. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | No. of Patients | CKS2 Immunohistochemical Score | p Value | |
|---|---|---|---|---|
| Low Score | High Score | |||
| Total | 90 | 39 | 51 | |
| Age (year) | 0.953 | |||
| <60 | 58 | 25 | 33 | |
| ≥60 | 32 | 14 | 18 | |
| Gender | 0.172 | |||
| male | 48 | 24 | 24 | |
| female | 42 | 15 | 27 | |
| Pathological Stage | 0.029 | |||
| Ⅰ–Ⅱ | 63 | 32 | 31 | |
| Ⅲ | 27 | 7 | 20 | |
| Pathological T | 0.417 | |||
| T1 | 56 | 26 | 30 | |
| T2 | 25 | 9 | 16 | |
| T3 | 7 | 4 | 3 | |
| T4 | 2 | 0 | 2 | |
| Pathological N | 0.024 | |||
| N0 | 55 | 29 | 26 | |
| N1–N3 | 35 | 10 | 25 | |
| STAS 1 | 0.015 | |||
| Negative | 34 | 19 | 15 | |
| Positive | 35 | 9 | 26 | |
| Histological subtypes | 0.013 | |||
| Solid | 27 | 7 | 20 | |
| Micropapillary | 5 | 1 | 4 | |
| Papillary | 17 | 9 | 8 | |
| Acinar | 32 | 14 | 18 | |
| Lepidic | 9 | 8 | 1 | |
| Pathologic differentiation | <0.001 | |||
| Low | 43 | 8 | 35 | |
| Median | 38 | 23 | 15 | |
| High | 9 | 8 | 1 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feng, J.; Hu, M.; Li, Z.; Hu, G.; Han, Y.; Zhang, Y.; Zhang, M.; Ren, J. Cyclin-Dependent Kinase Subunit 2 (CKS2) as a Prognostic Marker for Stages I–III Invasive Non-Mucinous Lung Adenocarcinoma and Its Role in Affecting Drug Sensitivity. Cells 2022, 11, 2611. https://doi.org/10.3390/cells11162611
Feng J, Hu M, Li Z, Hu G, Han Y, Zhang Y, Zhang M, Ren J. Cyclin-Dependent Kinase Subunit 2 (CKS2) as a Prognostic Marker for Stages I–III Invasive Non-Mucinous Lung Adenocarcinoma and Its Role in Affecting Drug Sensitivity. Cells. 2022; 11(16):2611. https://doi.org/10.3390/cells11162611
Chicago/Turabian StyleFeng, Junkai, Menglong Hu, Zongkuo Li, Guiming Hu, Yuting Han, Yan Zhang, Min Zhang, and Jingli Ren. 2022. "Cyclin-Dependent Kinase Subunit 2 (CKS2) as a Prognostic Marker for Stages I–III Invasive Non-Mucinous Lung Adenocarcinoma and Its Role in Affecting Drug Sensitivity" Cells 11, no. 16: 2611. https://doi.org/10.3390/cells11162611