
Sarcoidosis: A Clinical Overview from Symptoms to Diagnosis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Clinical Manifestations
2.1. General Symptoms
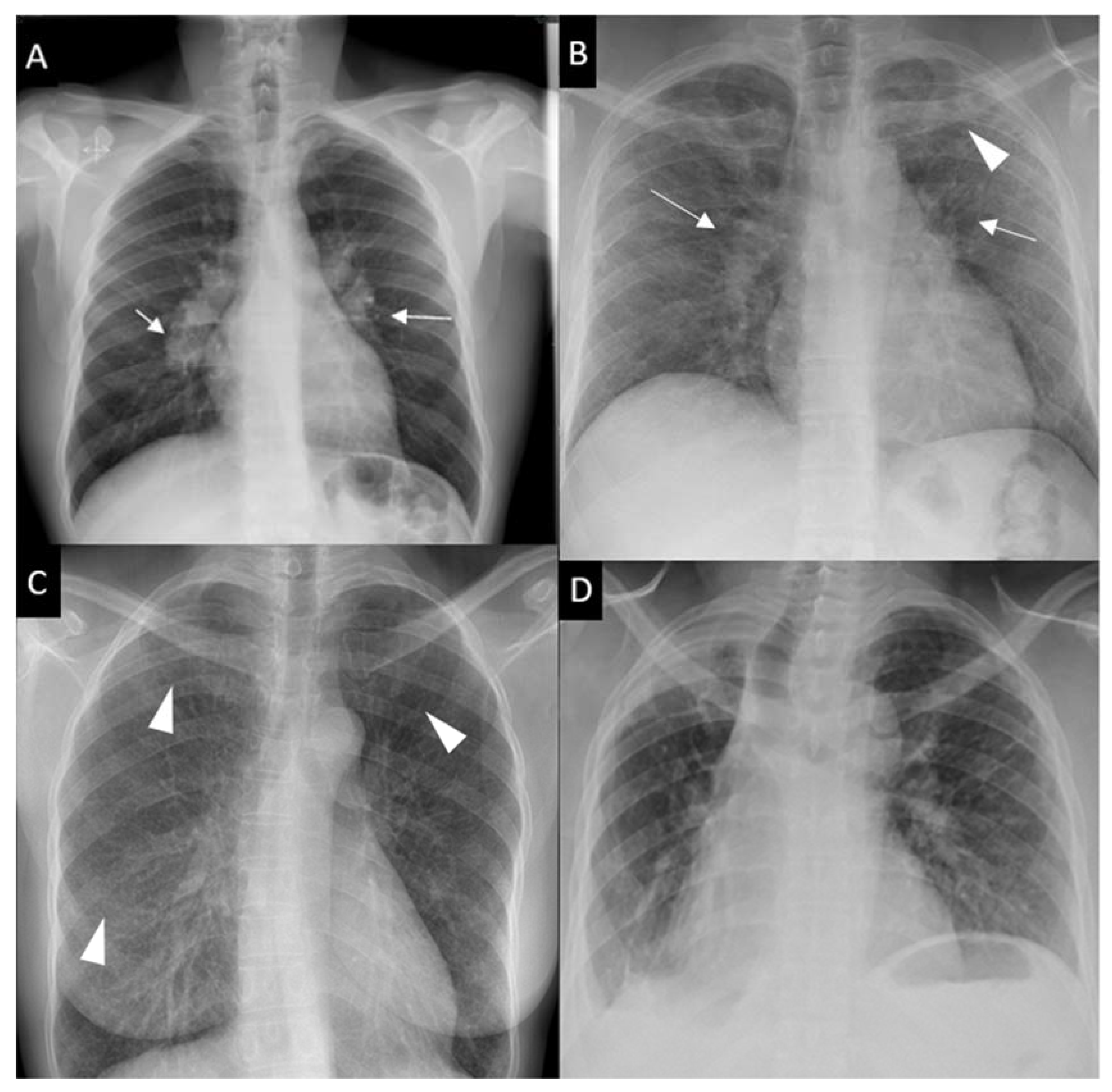
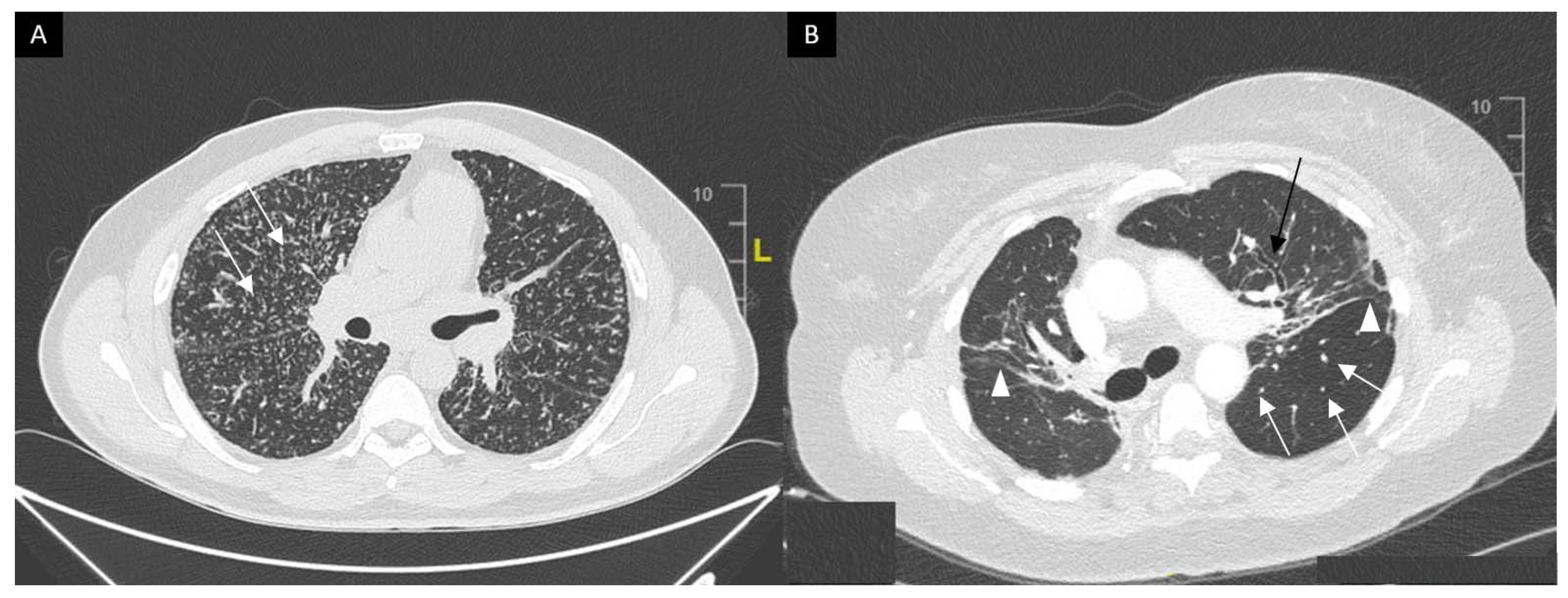
2.2. Lungs
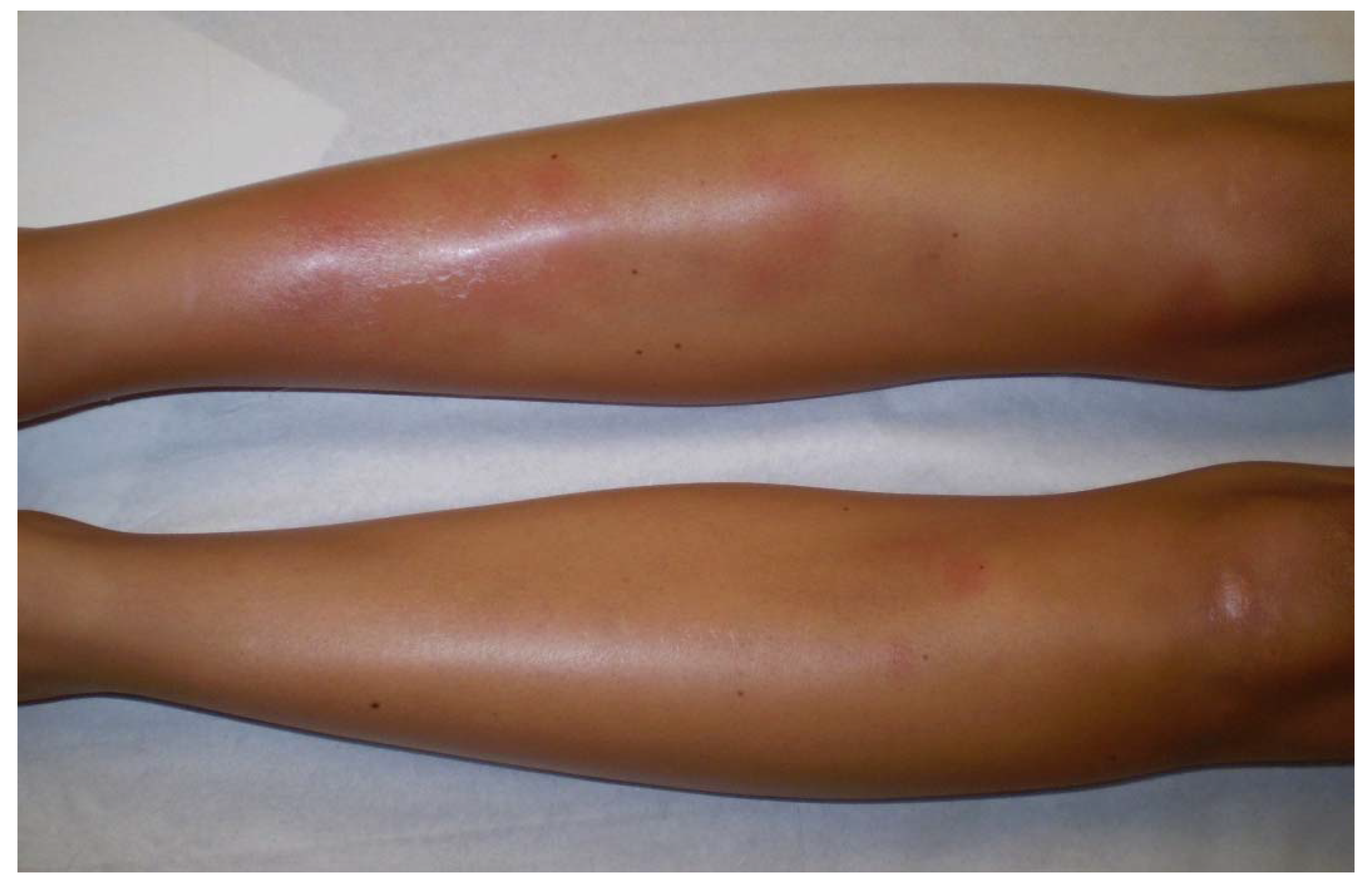
2.3. Löfgren’s Syndrome
2.4. Musculoskeletal Manifestations
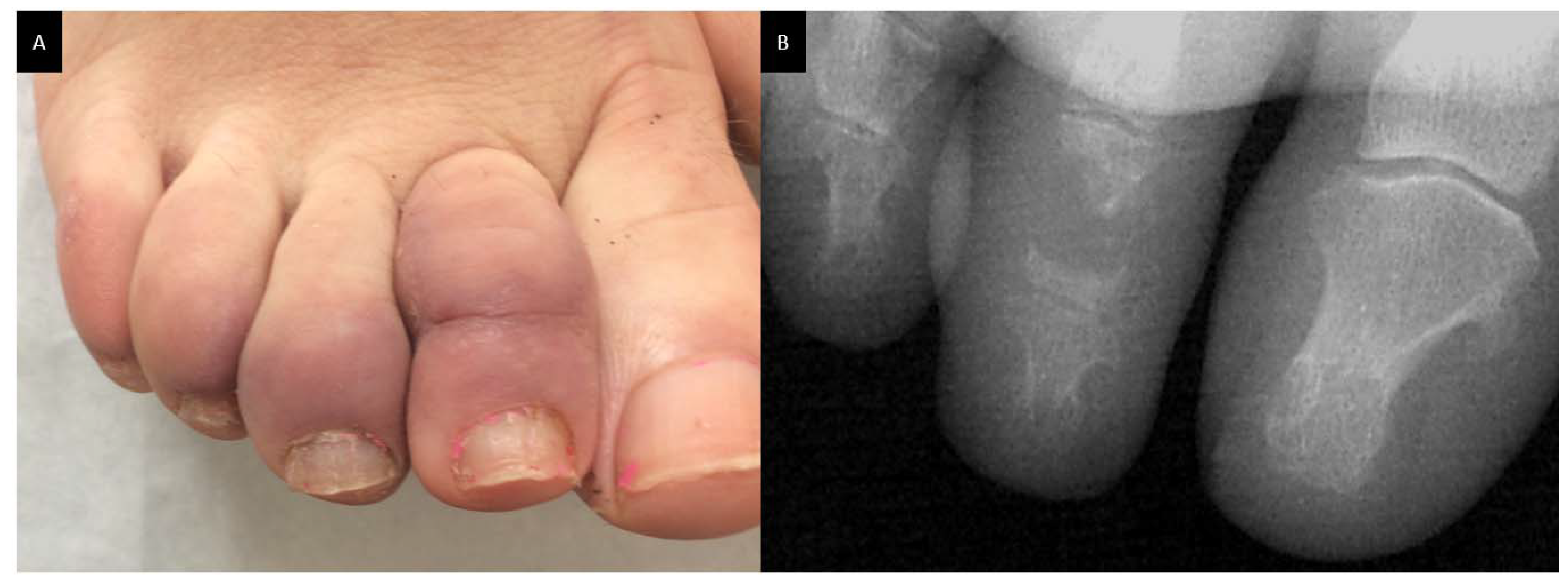
2.5. Skin
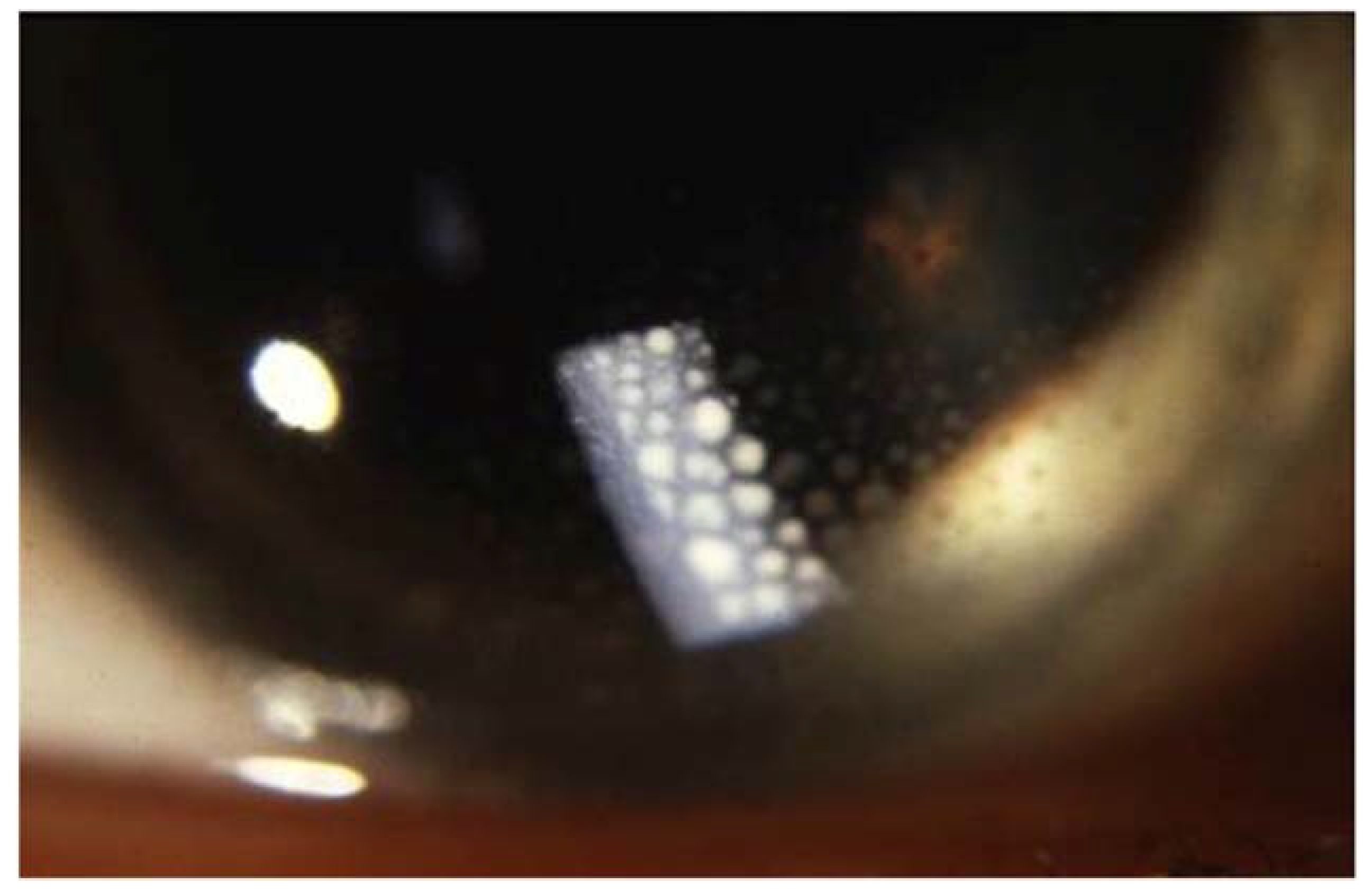
2.6. Eyes
2.7. Liver, Spleen and Gastrointestinal Involvement
2.8. Cardiac Sarcoidosis
2.9. Neurosarcoidosis
2.10. Kidney Involvement
2.11. Otolaryngological Involvement
3. Clinical Phenotypes
4. Diagnosis
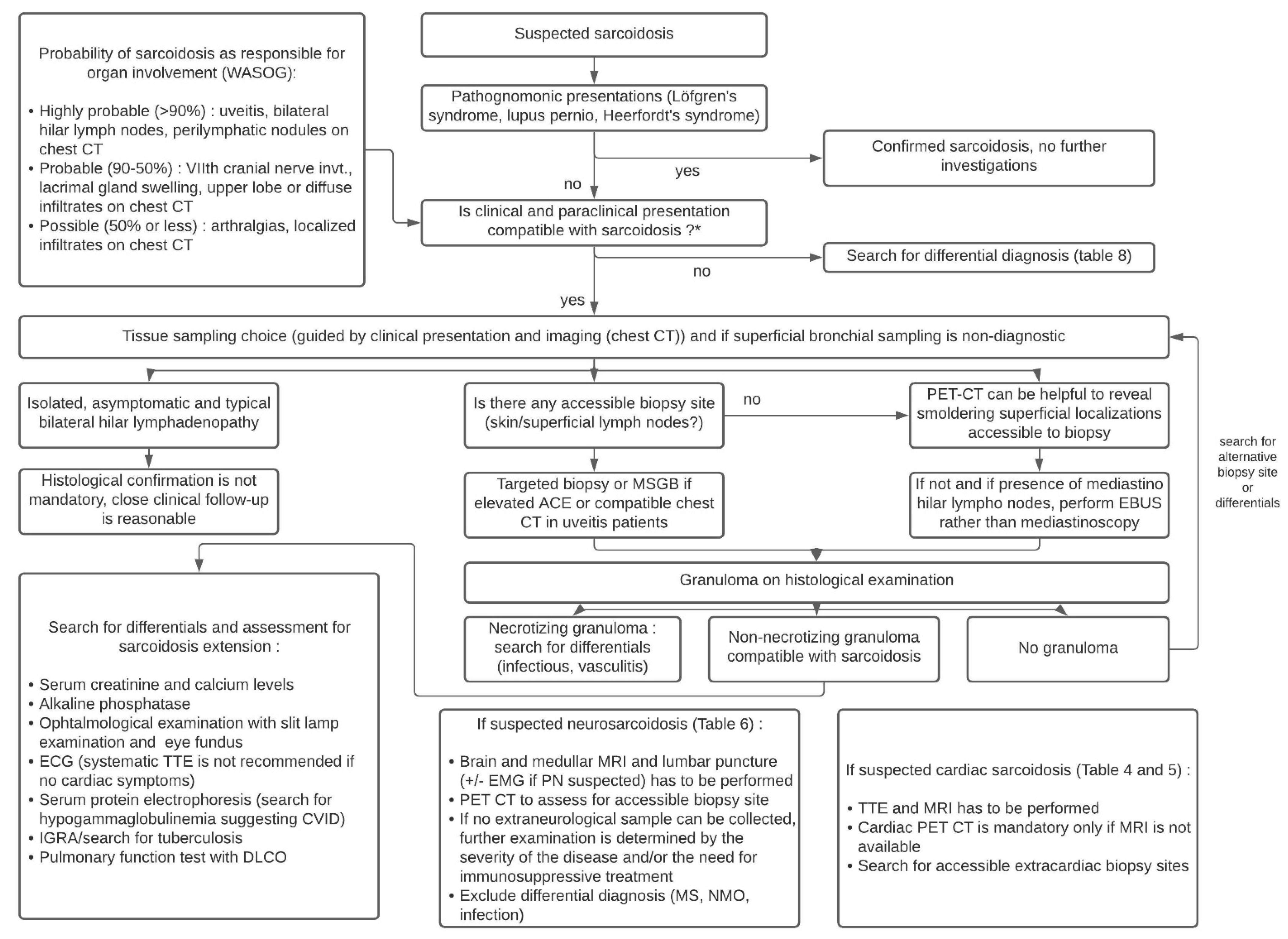
- highly probable: likelihood of sarcoidosis causing this manifestation of at least 90% (e.g., uveitis, bilateral hilar adenopathy, perilymphatic nodules on chest CT);
- probable: likelihood of sarcoidosis of 50–90% (e.g., seventh cranial nerve paralysis, lachrymal gland swelling, upper lobe or diffuse infiltrates);
- Possible: likelihood of sarcoidosis of less than 50% (e.g., arthralgias, localized infiltrate on CXR) [200].
4.1. Specific Diagnostic Criteria in Cardiac, Neuro and Ocular Sarcoidosis
4.1.1. Cardiac Sarcoidosis
4.1.2. Neurosarcoidosis
4.1.3. Ocular Sarcoidosis
4.2. Histopathology
5. Differential Diagnosis
5.1. Infectious Granulomatosis
5.2. Other Inflammatory Diseases
5.3. Drug Induced Granulomatosis
5.4. Common Variable Immunodeficiency
5.5. Neoplastic Disorders
5.6. Differential Diagnosis of Neurosarcoidosis
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Besnier, E.H. Lupus Pernio de La Face; Synovites Fongueuses (Scrofulo-Tuberculeuses) Symétriques Des Extrémités Supérieures. Ann. Derm. Syph. 1889, 10, 333–336. [Google Scholar]
- Sakthivel, P.; Bruder, D. Mechanism of Granuloma Formation in Sarcoidosis. Curr. Opin. Hematol. 2017, 24, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Hunninghake, G.; Costabel, U. Statement on Sarcoidosis. Am. J. Respir. Crit. Care Med. 1999, 160, 20. [Google Scholar] [CrossRef] [Green Version]
- Arkema, E.V.; Cozier, Y.C. Epidemiology of Sarcoidosis: Current Findings and Future Directions. Ther. Adv. Chronic Dis. 2018, 9, 227–240. [Google Scholar] [CrossRef] [PubMed]
- Rybicki, B.A.; Major, M.; Popovich, J.; Maliank, M.J.; Lannuzzi, M.C. Racial Differences in Sarcoidosis Incidence: A 5-Year Study in a Health Maintenance Organization. Am. J. Epidemiol. 1997, 145, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Pereira, C.A.C.; Dornfeld, M.C.; Baughman, R.; Judson, M.A. Clinical Phenotypes in Sarcoidosis. Curr. Opin. Pulm. Med. 2014, 20, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Valeyre, D.; Prasse, A.; Nunes, H.; Uzunhan, Y.; Brillet, P.-Y.; Müller-Quernheim, J. Sarcoidosis. Lancet 2014, 383, 1155–1167. [Google Scholar] [CrossRef]
- Nunes, H.; Bouvry, D.; Soler, P.; Valeyre, D. Sarcoidosis. Orphanet J. Rare Dis. 2007, 2, 46. [Google Scholar] [CrossRef] [Green Version]
- Nardi, A.; Brillet, P.-Y.; Letoumelin, P.; Girard, F.; Brauner, M.; Uzunhan, Y.; Naccache, J.-M.; Valeyre, D.; Nunes, H. Stage IV Sarcoidosis: Comparison of Survival with the General Population and Causes of Death. Eur. Respir. J. 2011, 38, 1368–1373. [Google Scholar] [CrossRef]
- Swigris, J.J.; Olson, A.L.; Huie, T.J.; Fernandez-Perez, E.R.; Solomon, J.; Sprunger, D.; Brown, K.K. Sarcoidosis-Related Mortality in the United States from 1988 to 2007. Am. J. Respir. Crit. Care Med. 2011, 183, 1524–1530. [Google Scholar] [CrossRef]
- Kirkil, G.; Lower, E.E.; Baughman, R.P. Predictors of Mortality in Pulmonary Sarcoidosis. Chest 2018, 153, 105–113. [Google Scholar] [CrossRef]
- Morimoto, T.; Azuma, A.; Abe, S.; Usuki, J.; Kudoh, S.; Sugisaki, K.; Oritsu, M.; Nukiwa, T. Epidemiology of Sarcoidosis in Japan. Eur. Respir. J. 2008, 31, 372–379. [Google Scholar] [CrossRef] [Green Version]
- Jamilloux, Y.; Maucort-Boulch, D.; Kerever, S.; Gerfaud-Valentin, M.; Broussolle, C.; Eb, M.; Valeyre, D.; Seve, P. Sarcoidosis-Related Mortality in France: A Multiple-Cause-of-Death Analysis. Eur. Respir. J. 2016, 48, 1700–1709. [Google Scholar] [CrossRef] [Green Version]
- Baughman, R.P.; Teirstein, A.S.; Judson, M.A.; Rossman, M.D.; Yeager, H.; Bresnitz, E.A.; DePALO, L.; Hunninghake, G.; Iannuzzi, M.C.; Johns, C.J.; et al. Clinical Characteristics of Patients in a Case Control Study of Sarcoidosis. Am. J. Respir. Crit. Care Med. 2001, 164, 1885–1889. [Google Scholar] [CrossRef] [Green Version]
- Ungprasert, P.; Carmona, E.M.; Utz, J.P.; Ryu, J.H.; Crowson, C.S.; Matteson, E.L. Epidemiology of Sarcoidosis 1946–2013. Mayo Clin. Proc. 2016, 91, 183–188. [Google Scholar] [CrossRef] [Green Version]
- Mañá, J.; Rubio-Rivas, M.; Villalba, N.; Marcoval, J.; Iriarte, A.; Molina-Molina, M.; Llatjos, R.; García, O.; Martínez-Yélamos, S.; Vicens-Zygmunt, V.; et al. Multidisciplinary Approach and Long-Term Follow-up in a Series of 640 Consecutive Patients with Sarcoidosis: Cohort Study of a 40-Year Clinical Experience at a Tertiary Referral Center in Barcelona, Spain. Medicine 2017, 96, e7595. [Google Scholar] [CrossRef] [PubMed]
- Valeyre, D.; Bernaudin, J.-F.; Jeny, F.; Duchemann, B.; Freynet, O.; Planès, C.; Kambouchner, M.; Nunes, H. Pulmonary Sarcoidosis. Clin. Chest Med. 2015, 36, 631–641. [Google Scholar] [CrossRef] [PubMed]
- Judson, M.A. The Diagnosis of Sarcoidosis. Clin. Chest Med. 2008, 29, 415–427. [Google Scholar] [CrossRef]
- Drent, M.; Strookappe, B.; Hoitsma, E.; De Vries, J. Consequences of Sarcoidosis. Clin. Chest Med. 2015, 36, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Drent, M.; Lower, E.E.; Vries, J.D. Sarcoidosis-Associated Fatigue. Eur. Respir. J. 2012, 40, 255–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vries, J.; Michielsen, H.; Van Heck, G.L.; Drent, M. Measuring Fatigue in Sarcoidosis: The Fatigue Assessment Scale (FAS). Br. J. Health Psychol. 2004, 9, 279–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baughman, R.P.; Sparkman, B.K.; Lower, E.E. Six-Minute Walk Test and Health Status Assessment in Sarcoidosis. Chest 2007, 132, 207–213. [Google Scholar] [CrossRef]
- Drent, M.; Wirnsberger, R.M.; de Vries, J.; van Dieijen-Visser, M.P.; Wouters, E.F.M.; Schols, A.M.W.J. Association of Fatigue with an Acute Phase Response in Sarcoidosis. Eur. Respir. J. 1999, 13, 718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korenromp, I.H.E.; Heijnen, C.J.; Vogels, O.J.M.; van den Bosch, J.M.M.; Grutters, J.C. Characterization of Chronic Fatigue in Patients with Sarcoidosis in Clinical Remission. Chest 2011, 140, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Michielsen, H.J.; Drent, M.; Peros-Golubicic, T.; De Vries, J. Fatigue Is Associated with Quality of Life in Sarcoidosis Patients. Chest 2006, 130, 989–994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elfferich, M.D.; Nelemans, P.J.; Ponds, R.W.; Vries, J.D.; Wijnen, P.A.; Drent, M. Everyday Cognitive Failure in Sarcoidosis: The Prevalence and the Effect of Anti-TNF-α Treatment. RES 2010, 80, 212–219. [Google Scholar] [CrossRef]
- Crouser, E.D.; Maier, L.A.; Wilson, K.C.; Bonham, C.A.; Morgenthau, A.S.; Patterson, K.C.; Abston, E.; Bernstein, R.C.; Blankstein, R.; Chen, E.S.; et al. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2020, 201, e26–e51. [Google Scholar] [CrossRef]
- Telenti, A.; Hermans, P.E. Idiopathic Granulomatosis Manifesting as Fever of Unknown Origin. Mayo Clin. Proc. 1989, 64, 44–50. [Google Scholar] [CrossRef]
- Iannuzzi, M.C.; Rybicki, B.A.; Teirstein, A.S. Sarcoidosis. N. Engl. J. Med. 2007, 357, 2153–2165. [Google Scholar] [CrossRef] [PubMed]
- Judson, M.A.; Thompson, B.W.; Rabin, D.L.; Steimel, J.; Knattereud, G.L.; Lackland, D.T.; Rose, C.; Rand, C.S.; Baughman, R.P.; Teirstein, A.S. The Diagnostic Pathway to Sarcoidosis*. Chest 2003, 123, 406–412. [Google Scholar] [CrossRef] [Green Version]
- Sinha, A.; Lee, K.K.; Rafferty, G.F.; Yousaf, N.; Pavord, I.D.; Galloway, J.; Birring, S.S. Predictors of Objective Cough Frequency in Pulmonary Sarcoidosis. Eur. Respir. J. 2016, 47, 1461–1471. [Google Scholar] [CrossRef]
- Jeny, F.; Bernaudin, J.-F.; Cohen Aubart, F.; Brillet, P.-Y.; Bouvry, D.; Nunes, H.; Valeyre, D. Diagnosis Issues in Sarcoidosis. Respir. Med. Res. 2020, 77, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Jameson, A.; Revels, J.; Wang, L.L.; Wang, D.T.; Wang, S.S. Sarcoidosis, the Master Mimicker. Curr. Probl. Diagn. Radiol. 2020, S0363018820301973. [Google Scholar] [CrossRef]
- Venkata Ramanan, R.; Pudhiavan, A.; Venkataramanan, A. The “Cluster of Black Pearls” Sign of Sarcoid Lymphadenopathy: A New Sign on Thin-Section Contrast-Enhanced Multidetector CT. Clin. Radiol. 2017, 72, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.G.; Kronek, L.-P.; Valeyre, D.; Brauner, N.; Brillet, P.-Y.; Nunes, H.; Brauner, M.W.; Réty, F. High-Resolution Computed Tomography to Differentiate Chronic Diffuse Interstitial Lung Diseases with Predominant Ground-Glass Pattern Using Logical Analysis of Data. Eur. Radiol. 2010, 20, 1297–1310. [Google Scholar] [CrossRef] [PubMed]
- Valeyre, D.; Bernaudin, J.-F.; Uzunhan, Y.; Kambouchner, M.; Brillet, P.-Y.; Soussan, M.; Nunes, H. Clinical Presentation of Sarcoidosis and Diagnostic Work-Up. Semin. Respir. Crit. Care Med. 2014, 35, 336–351. [Google Scholar] [CrossRef]
- Sharma, S.K.; Verma, U.; Pande, J.N.; Murugesan, K.; Verma, K.; Guleria, J.S. Glucocorticoid Receptors in Bronchoalveolar Lavage Fluid in Sarcoidosis. Chest 1988, 93, 577–579. [Google Scholar] [CrossRef] [PubMed]
- Abehsera, M.; Valeyre, D.; Grenier, P.; Jaillet, H.; Battesti, J.P.; Brauner, M.W. Sarcoidosis with Pulmonary Fibrosis: CT Patterns and Correlation with Pulmonary Function. Am. J. Roentgenol. 2000, 174, 1751–1757. [Google Scholar] [CrossRef]
- Lavergne, F.; Clerici, C.; Sadoun, D.; Brauner, M.; Battesti, J.-P.; Valeyre, D. Airway Obstruction in Bronchial Sarcoidosis. Chest 1999, 116, 1194–1199. [Google Scholar] [CrossRef]
- Chambellan, A.; Turbie, P.; Nunes, H.; Brauner, M.; Battesti, J.-P.; Valeyre, D. Endoluminal Stenosis of Proximal Bronchi in Sarcoidosis. Chest 2005, 127, 472–481. [Google Scholar] [CrossRef] [Green Version]
- Udwadia, Z.F.; Pilling, J.R.; Jenkins, P.F.; Harrison, B.D. Bronchoscopic and Bronchographic Findings in 12 Patients with Sarcoidosis and Severe or Progressive Airways Obstruction. Thorax 1990, 45, 272–275. [Google Scholar] [CrossRef] [Green Version]
- Naccache, J.-M.; Lavolé, A.; Nunes, H.; Lamberto, C.; Letoumelin, P.; Brauner, M.; Valeyre, D.; Brillet, P.Y. High-Resolution Computed Tomographic Imaging of Airways in Sarcoidosis Patients With Airflow Obstruction. J. Comput. Assist. Tomogr. 2008, 32, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Wells, A.U.; Desai, S.R.; Rubens, M.B.; Goh, N.S.L.; Cramer, D.; Nicholson, A.G.; Colby, T.V.; du Bois, R.M.; Hansell, D.M. Idiopathic Pulmonary Fibrosis: A Composite Physiologic Index Derived from Disease Extent Observed by Computed Tomography. Am. J. Respir. Crit. Care Med. 2003, 167, 962–969. [Google Scholar] [CrossRef]
- Walsh, S.L.; Wells, A.U.; Sverzellati, N.; Keir, G.J.; Calandriello, L.; Antoniou, K.M.; Copley, S.J.; Devaraj, A.; Maher, T.M.; Renzoni, E.; et al. An Integrated Clinicoradiological Staging System for Pulmonary Sarcoidosis: A Case-Cohort Study. Lancet Respir. Med. 2014, 2, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Delobbe, A.; Hélène, P.; Jocelyne, M.; Sophie, R.; Claude, H.-F.; Benoît, W.; Bernard, A. Impaired Exercise Response in Sarcoid Patients with Normal Pulmonary Function. Sarcoidosis Vasc. Diffus. Lung Dis. 2002, 19, 148–153. [Google Scholar]
- Marcellis, R.G.J.; Lenssen, A.F.; de Vries, G.J.; Baughman, R.P.; van der Grinten, C.P.; Verschakelen, J.A.; De Vries, J.; Drent, M. Is There an Added Value of Cardiopulmonary Exercise Testing in Sarcoidosis Patients? Lung 2013, 191, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Wallaert, B.; Talleu, C.; Wemeau-Stervinou, L.; Duhamel, A.; Robin, S.; Aguilaniu, B. Reduction of Maximal Oxygen Uptake in Sarcoidosis: Relationship with Disease Severity. Respiration 2011, 82, 501–508. [Google Scholar] [CrossRef]
- Lopes, A.J.; Menezes, S.L.S.; Dias, C.M.; Oliveira, J.F.; Mainenti, M.R.M.; Guimarães, F.S. Cardiopulmonary Exercise Testing Variables as Predictors of Long-Term Outcome in Thoracic Sarcoidosis. Braz. J. Med. Biol. Res. 2012, 45, 256–263. [Google Scholar] [CrossRef] [Green Version]
- Kollert, F.; Geck, B.; Suchy, R.; Jörres, R.A.; Arzt, M.; Heidinger, D.; Hamer, O.W.; Prasse, A.; Müller-Quernheim, J.; Pfeifer, M.; et al. The Impact of Gas Exchange Measurement during Exercise in Pulmonary Sarcoidosis. Respir. Med. 2011, 105, 122–129. [Google Scholar] [CrossRef] [Green Version]
- Costabel, U.; Bonella, F.; Ohshimo, S.; Guzman, J. Diagnostic Modalities in Sarcoidosis: BAL, EBUS, and PET. Semin. Respir. Crit. Care Med. 2010, 31, 404–408. [Google Scholar] [CrossRef]
- Darlington, P.; Kullberg, S.; Eklund, A.; Grunewald, J. Subpopulations of Cells from Bronchoalveolar Lavage Can Predict Prognosis in Sarcoidosis. Eur. Respir. J. 2020, 55, 1901450. [Google Scholar] [CrossRef] [PubMed]
- Mota, P.C.; Morais, A.; Palmares, C.; Beltrão, M.; Melo, N.; Santos, A.C.; Delgado, L. Diagnostic Value of CD103 Expression in Bronchoalveolar Lymphocytes in Sarcoidosis. Respir. Med. 2012, 106, 1014–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heron, M.; Slieker, W.A.T.; Zanen, P.; van Lochem, E.G.; Hooijkaas, H.; van den Bosch, J.M.M.; van Velzen-Blad, H. Evaluation of CD103 as a Cellular Marker for the Diagnosis of Pulmonary Sarcoidosis. Clin. Immunol. 2008, 126, 338–344. [Google Scholar] [CrossRef]
- Boucly, A.; Weatherald, J.; Savale, L.; Jaïs, X.; Cottin, V.; Prevot, G.; Picard, F.; de Groote, P.; Jevnikar, M.; Bergot, E.; et al. Risk Assessment, Prognosis and Guideline Implementation in Pulmonary Arterial Hypertension. Eur. Respir. J. 2017, 50, 1700889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubio-Rivas, M.; Franco, J.; Corbella, X. Sarcoidosis Presenting with and without Löfgren’s Syndrome: Clinical, Radiological and Behavioral Differences Observed in a Group of 691 Patients. Jt. Bone Spine 2020, 87, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Karakaya, B.; Kaiser, Y.; van Moorsel, C.; Grunewald, J. Löfgren’s Syndrome: Diagnosis, Management, and Disease Pathogenesis. Semin. Respir. Crit. Care Med. 2017, 38, 463–476. [Google Scholar] [CrossRef] [PubMed]
- Goussault, C.; Albert, J.-D.; Coiffier, G.; Lamer, F.; Guillin, R.; Le Goff, B.; Bouvard, B.; Dernis, E.; Ferreyra, M.; Cormier, G.; et al. Ultrasound Characterization of Ankle Involvement in Löfgren Syndrome. Jt. Bone Spine 2018, 85, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Anandacoomarasamy, A.; Peduto, A.; Howe, G.; Maniolos, N.; Spencer, D. Magnetic Resonance Imaging in Löfgren’s Syndrome: Demonstration of Periarthritis. Clin. Rheumatol. 2006, 26, 572–575. [Google Scholar] [CrossRef]
- Cacciatore, C.; Belnou, P.; Thietart, S.; Desthieux, C.; Versini, M.; Abisror, N.; Ottaviani, S.; Cormier, G.; Deroux, A.; Dellal, A.; et al. Acute and Chronic Sarcoid Arthropathies: Characteristics and Treatments From a Retrospective Nationwide French Study. Front. Med. 2020, 7, 565420. [Google Scholar] [CrossRef]
- Bechman, K.; Christidis, D.; Walsh, S.; Birring, S.S.; Galloway, J. A Review of the Musculoskeletal Manifestations of Sarcoidosis. Rheumatology 2018, 57, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Sweiss, N.; Patterson, K.; Sawaqed, R.; Jabbar, U.; Korsten, P.; Hogarth, K.; Wollman, R.; Garcia, J.; Niewold, T.; Baughman, R. Rheumatologic Manifestations of Sarcoidosis. Semin. Respir. Crit. Care Med. 2010, 31, 463–473. [Google Scholar] [CrossRef] [Green Version]
- Visser, H. Sarcoid Arthritis: Clinical Characteristics, Diagnostic Aspects, and Risk Factors. Ann. Rheum. Dis. 2002, 61, 499–504. [Google Scholar] [CrossRef] [Green Version]
- Kobak, S.; Sever, F.; Usluer, O.; Goksel, T.; Orman, M. The Clinical Characteristics of Sarcoid Arthropathy Based on a Prospective Cohort Study. Ther. Adv. Musculoskelet. Dis. 2016, 8, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Sukenik, S.; Hendler, N.; Yerushalmi, B.; Buskila, D.; Liberman, N. Jaccoud’s-Type Arthropathy: An Association with Sarcoidosis. J. Rheumatol. 1991, 18, 915–917. [Google Scholar] [PubMed]
- Erb, N.; Cushley, M.J.; Kassimos, D.G.; Shave, R.M.; Kitas, G.D. An Assessment of Back Pain and the Prevalence of Sacroiliitis in Sarcoidosis. Chest 2005, 127, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Sparks, J.A.; McSparron, J.I.; Shah, N.; Aliabadi, P.; Paulson, V.; Fanta, C.H.; Coblyn, J.S. Osseous Sarcoidosis: Clinical Characteristics, Treatment, and Outcomes—Experience from a Large, Academic Hospital. Semin. Arthritis Rheum. 2014, 44, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Mostard, R.L.; Prompers, L.; Weijers, R.E.; van Kroonenburgh, M.J.; Wijnen, P.A.; Geusens, P.P.; Drent, M. F-18 FDG PET/CT for Detecting Bone and Bone Marrow Involvement in Sarcoidosis Patients. Clin. Nucl. Med. 2012, 37, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Rúa-Figueroa, I.; Gantes, M.A.; Erausquin, C.; Mhaidli, H.; Montesdeoca, A. Vertebral Sarcoidosis: Clinical and Imaging Findings. Semin. Arthritis Rheum. 2002, 31, 346–352. [Google Scholar] [CrossRef]
- Demaria, L.; Borie, R.; Benali, K.; Piekarski, E.; Goossens, G.; Palazzo, E.; Florien, M.; Dieudé, P.; Crestani, B.; Ottaviani, S. 18F-FDG PET/CT in Bone Sarcoidosis: An Observational Study. Clin. Rheumatol. 2020, 39, 2727–2734. [Google Scholar] [CrossRef]
- Berger, C.; Sommer, C.; Meinck, H.-M. Isolated Sarcoid Myopathy. Muscle Nerve 2002, 26, 553–556. [Google Scholar] [CrossRef]
- Douglas, A.C.; Macleod, J.G.; Matthews, J.D. Symptomatic Sarcoidosis of Skeletal Muscle. J. Neurol. Neurosurg. Psychiatry 1973, 36, 7. [Google Scholar] [CrossRef] [Green Version]
- Silverstein, A.; Siltzbach, L.E. Muscle Involvement in Sarcoidosis. Arch. Neurol. 1969, 21, 7. [Google Scholar] [CrossRef]
- Wolfe, S.M.; Pinals, R.S.; Aelion, J.A.; Goodman, R.E. Myopathy in Sarcoidosis: Clinical and Pathologic Study of Four Cases and Review of the Literature. Semin. Arthritis Rheum. 1987, 16, 300–306. [Google Scholar] [CrossRef]
- Cremers, J.P.; Van Kroonenburgh, M.J.; Mostard, R.L.; Vöö, S.A.; Wijnen, P.A.; Koek, G.H.; Drent, M. Extent of Disease Activity Assessed by 18F-FDG PET/CT in a Dutch Sarcoidosis Population. Sarcoidosis Vasc. Diffus. Lung Dis. 2014, 31, 37–45. [Google Scholar]
- Roux, K.L.; Streichenberger, N.; Vial, C.; Petiot, P.; Feasson, L.; Bouhour, F.; Ninet, J.; Lachenal, F.; Broussolle, C.; Sève, P. Granulomatous Myositis: A Clinical Study of Thirteen Cases. Muscle Nerve 2007, 35, 171–177. [Google Scholar] [CrossRef]
- Androdias, G.; Maillet, D.; Marignier, R.; Pinede, L.; Confavreux, C.; Broussolle, C.; Vukusic, S.; Seve, P. Mycophenolate Mofetil May Be Effective in CNS Sarcoidosis but Not in Sarcoid Myopathy. Neurology 2011, 76, 1168–1172. [Google Scholar] [CrossRef]
- Dieudonné, Y.; Allenbach, Y.; Benveniste, O.; Leonard-Louis, S.; Hervier, B.; Mariampillai, K.; Nespola, B.; Lannes, B.; Echaniz-Laguna, A.; Wendling, D.; et al. Granulomatosis-Associated Myositis: High Prevalence of Sporadic Inclusion Body Myositis. Neurology 2020, 94, e910–e920. [Google Scholar] [CrossRef] [PubMed]
- Ungprasert, P.; Crowson, C.S.; Matteson, E.L. Influence of Gender on Epidemiology and Clinical Manifestations of Sarcoidosis: A Population-Based Retrospective Cohort Study 1976-2013. Lung 2017, 195, 87–91. [Google Scholar] [CrossRef] [Green Version]
- James, D.G.; Neville, E.; Siltzbach, L.E.; Turiaf, J.; Battesti, J.P.; Sharma, O.P.; Hosoda, Y.; Mikami, R.; Odaka, M.; Villar, T.G.; et al. A Worldwide Review of Sarcoidosis*. Ann. N. Y. Acad. Sci. 1976, 278, 321–334. [Google Scholar] [CrossRef] [PubMed]
- Studdy, P.R.; Bird, R.; Neville, E.; James, D.G. Biochemical Findings in Sarcoidosis. J. Clin. Pathol. 1980, 33, 528–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baughman, R.P.; Janovcik, J.; Ray, M.; Sweiss, N.; Lower, E.E. Calcium and Vitamin D Metabolism in Sarcoidosis. Sarcoidosis Vasc. Diffus. Lung Dis. 2013, 30, 113–120. [Google Scholar]
- Gwadera, Ł.; Białas, A.J.; Iwański, M.A.; Górski, P.; Piotrowski, W.J. Sarcoidosis and Calcium Homeostasis Disturbances—Do We Know Where We Stand? Chron. Respir. Dis. 2019, 16. [Google Scholar] [CrossRef]
- Adams, J.S. Vitamin D Metabolite-Mediated Hypercalcemia. Endocrinol. Metab. Clin. N. Am. 1989, 18, 765–778. [Google Scholar] [CrossRef]
- Caplan, A.; Rosenbach, M.; Imadojemu, S. Cutaneous Sarcoidosis. Semin. Respir. Crit. Care Med. 2020, 41, 689–699. [Google Scholar] [CrossRef] [PubMed]
- Marcoval, J.; Mañá, J.; Rubio, M. Specific Cutaneous Lesions in Patients with Systemic Sarcoidosis: Relationship to Severity and Chronicity of Disease. Clin. Exp. Dermatol. 2011, 36, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Haimovic, A.; Sanchez, M.; Judson, M.A.; Prystowsky, S. Sarcoidosis: A Comprehensive Review and Update for the Dermatologist. J. Am. Acad. Dermatol. 2012, 66, 719.e1–719.e10. [Google Scholar] [CrossRef] [PubMed]
- Bodaghi, B.; Touitou, V.; Fardeau, C.; Chapelon, C.; LeHoang, P. Ocular Sarcoidosis. La Presse Médicale 2012, 41, e349–e354. [Google Scholar] [CrossRef]
- Jamilloux, Y.; Kodjikian, L.; Broussolle, C.; Sève, P. Sarcoidosis and Uveitis. Autoimmun. Rev. 2014, 13, 840–849. [Google Scholar] [CrossRef]
- Coulon, C.; Kodjikian, L.; Rochepeau, C.; Perard, L.; Jardel, S.; Burillon, C.; Broussolle, C.; Jamilloux, Y.; Seve, P. Ethnicity and Association with Ocular, Systemic Manifestations and Prognosis in 194 Patients with Sarcoid Uveitis. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 2495–2503. [Google Scholar] [CrossRef]
- Birnbaum, A.D.; French, D.D.; Mirsaeidi, M.; Wehrli, S. Sarcoidosis in the National Veteran Population. Ophthalmology 2015, 122, 934–938. [Google Scholar] [CrossRef] [Green Version]
- Pasadhika, S.; Rosenbaum, J.T. Ocular Sarcoidosis. Clin. Chest Med. 2015, 36, 669–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, S.P.; Rogers, S.L.; Hall, A.J.; Hodgson, L.; Brennan, J.; Stawell, R.J.; Lim, L.L. Sarcoidosis-Related Uveitis: Clinical Presentation, Disease Course, and Rates of Systemic Disease Progression After Uveitis Diagnosis. Am. J. Ophthalmol. 2019, 198, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, G.; Anderson, R.; Sharpstone, P.; James, D.G. Enlargement of Parotid Gland Due to Sarcoidosis. Br. Med. J. 1964, 2, 861–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darlington, P.; Tallstedt, L.; Padyukov, L.; Kockum, I.; Cederlund, K.; Eklund, A.; Grunewald, J. HLA-DRB1* Alleles and Symptoms Associated with Heerfordt’s Syndrome in Sarcoidosis. Eur. Respir. J. 2011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heerfordt, C. Über Eine ‘Febris Uveoparotidea Subchronica’ an Der Glandula Parotis Der Uvea Des Auges Lokalisiert Und Häufig Mit Paresen Cerebrospinaler Nerver Kompliziert. Arch. Ophthalmol. 1909, 70, 254–273. [Google Scholar]
- Makimoto, G.; Kawakado, K.; Nakanishi, M.; Tamura, T.; Noda, M.; Makimoto, S.; Sato, Y.; Kuyama, S. Heerfordt’s Syndrome Associated with Trigeminal Nerve Palsy and Reversed Halo Sign. Intern. Med. 2020. [Google Scholar] [CrossRef]
- Mikulic, S.; Patel, P.; Sheffield, S.; Kandah, F.; Velarde, G. Heerfordt-Waldenström Syndrome Manifesting as Cardiac Sarcoidosis. Cureus 2020, 12, e10619. [Google Scholar] [CrossRef]
- Rochepeau, C.; Jamilloux, Y.; Kerever, S.; Febvay, C.; Perard, L.; Broussolle, C.; Burillon, C.; Kodjikian, L.; Seve, P. Long-Term Visual and Systemic Prognoses of 83 Cases of Biopsy-Proven Sarcoid Uveitis. Br. J. Ophthalmol. 2017, 101, 856–861. [Google Scholar] [CrossRef]
- Sève, P.; Jamilloux, Y.; Tilikete, C.; Gerfaud-Valentin, M.; Kodjikian, L.; El Jammal, T. Ocular Sarcoidosis. Semin. Respir. Crit. Care Med. 2020, 41, 673–688. [Google Scholar] [CrossRef]
- Paovic, J.; Paovic, P.; Sredovic, V.; Jovanovic, S. Clinical Manifestations, Complications and Treatment of Ocular Sarcoidosis: Correlation between Visual Efficiency and Macular Edema as Seen on Optical Coherence Tomography. Semin. Ophthalmol. 2016, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Miserocchi, E.; Modorati, G.; Di Matteo, F.; Galli, L.; Rama, P.; Bandello, F. Visual Outcome in Ocular Sarcoidosis: Retrospective Evaluation of Risk Factors. Eur. J. Ophthalmol. 2011, 21, 802–810. [Google Scholar] [CrossRef]
- Dana, M.-R.; Merayo-Lloves, J.; Schaumberg, D.A.; Foster, C.S. Prognosticators for Visual Outcome in Sarcoid Uveitis. Ophthalmology 1996, 103, 1846–1853. [Google Scholar] [CrossRef]
- Rothova, A. Ocular Involvement in Sarcoidosis. Br. J. Ophthalmol. 2000, 84, 110–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koczman, J.J.; Rouleau, J.; Gaunt, M.; Kardon, R.H.; Wall, M.; Lee, A.G. Neuro-Ophthalmic Sarcoidosis: The University of Iowa Experience. Semin. Ophthalmol. 2008, 23, 157–168. [Google Scholar] [CrossRef]
- Prabhakaran, V.C.; Saeed, P.; Esmaeli, B.; Sullivan, T.J.; McNab, A.; Davis, G.; Valenzuela, A.; Leibovitch, I.; Kesler, A.; Sivak-Callcott, J.; et al. Orbital and Adnexal Sarcoidosis. Arch. Ophthalmol. 2007, 125, 1657–1662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braswell, R.A.; Kline, L.B. Neuro-Ophthalmologic Manifestations of Sarcoidosis. Int. Ophthalmol. Clin. 2007, 47, 67–77. [Google Scholar] [CrossRef]
- Leclercq, M.; Langlois, V.; Girszyn, N.; Le Besnerais, M.; Benhamou, Y.; Levesque, H.; Muraine, M.; Gueudry, J. Comparison of Conventional Immunosuppressive Drugs versus Anti-TNF-α Agents in Non-Infectious Non-Anterior Uveitis. J. Autoimmun. 2020, 113, 102481. [Google Scholar] [CrossRef]
- Tadros, M.; Forouhar, F.; Wu, G.Y. Hepatic Sarcoidosis. J. Clin. Transl. Hepatol. 2013, 1, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Deutsch-Link, S.; Fortuna, D.; Weinberg, E.M. A Comprehensive Review of Hepatic Sarcoid. Semin. Liver Dis. 2018, 38, 284–297. [Google Scholar] [CrossRef]
- Judson, M. Extrapulmonary Sarcoidosis. Semin. Respir. Crit. Care Med. 2007, 28, 083–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bihari, C.; Rastogi, A.; Kumar, N.; Rajesh, S.; Sarin, S.K. Hepatic Sarcoidosis: Clinico-Pathological Characterization of Symptomatic Cases. Acta Gastroenterol. Belg. 2015, 78, 306–313. [Google Scholar]
- Moreno-Merlo, F.; Wanless, I.R.; Shimamatsu, K.; Sherman, M.; Greig, P.; Chiasson, D. The Role of Granulomatous Phlebitis and Thrombosis in the Pathogenesis of Cirrhosis and Portal Hypertension in Sarcoidosis. Hepatology 1997, 26, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Alam, I.; Levenson, S.D.; Ferrell, L.D.; Bass, N.M. Diffuse Intrahepatic Biliary Strictures in Sarcoidosis Resembling Sclerosing Cholangitis (Case Report and Review of the Literature). Dig. Dis. Sci. 1997, 42, 1295–1301. [Google Scholar] [CrossRef] [PubMed]
- Delfosse, V.; de Leval, L.; De Roover, A.; Delwaide, J.; Honoré, P.; Boniver, J.; Detry, O. Budd-Chiari Syndrome Complicating Hepatic Sarcoidosis: Definitive Treatment by Liver Transplantation: A Case Report. Transplant. Proc. 2009, 41, 3432–3434. [Google Scholar] [CrossRef] [PubMed]
- Ungprasert, P.; Crowson, C.S.; Simonetto, D.A.; Matteson, E.L. Clinical Characteristics and Outcome of Hepatic Sarcoidosis: A Population-Based Study 1976–2013. Am. J. Gastroenterol. 2017, 112, 1556–1563. [Google Scholar] [CrossRef]
- Warshauer, D.M.; Dumbleton, S.A.; Molina, P.L.; Yankaskas, B.C.; Parker, L.A.; Woosley, J.T. Abdominal CT Findings in Sarcoidosis: Radiologic and Clinical Correlation. Radiology 1994, 192, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Ungprasert, P.; Ryu, J.H.; Matteson, E.L. Clinical Manifestations, Diagnosis, and Treatment of Sarcoidosis. Mayo Clin. Proc. Innov. Qual. Outcomes 2019, 3, 358–375. [Google Scholar] [CrossRef] [Green Version]
- Syed, U.; Alkhawam, H.; Bakhit, M.; Companioni, R.A.C.; Walfish, A. Hepatic Sarcoidosis: Pathogenesis, Clinical Context, and Treatment Options. Scand. J. Gastroenterol. 2016, 51, 1025–1030. [Google Scholar] [CrossRef]
- Coash, M.; Forouhar, F.; Wu, C.H.; Wu, G.Y. Granulomatous Liver Diseases: A Review. J. Formos. Med. Assoc. 2012, 111, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagana, S.M.; Moreira, R.K.; Lefkowitch, J.H. Hepatic Granulomas: Pathogenesis and Differential Diagnosis. Clin. Liver Dis. 2010, 14, 605–617. [Google Scholar] [CrossRef]
- Gaya, D.R. Hepatic Granulomas: A 10 Year Single Centre Experience. J. Clin. Pathol. 2003, 56, 850–853. [Google Scholar] [CrossRef] [Green Version]
- Geri, G.; Cacoub, P. Granulomatose hépatique. Rev. Méd. Interne 2011, 32, 560–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wainwright, H. Hepatic Granulomas. Eur. J. Gastroenterol. Hepatol. 2007, 19, 93–95. [Google Scholar] [CrossRef]
- Esfeh, J.M.; Culver, D.; Plesec, T.; John, B. Clinical Presentation and Protocol for Management of Hepatic Sarcoidosis. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 349–358. [Google Scholar] [CrossRef]
- Britt, A.R.; Francis, I.R.; Glazer, G.M.; Ellis, J.H. Sarcoidosis: Abdominal Manifestations at CT. Radiology 1991, 178, 91–94. [Google Scholar] [CrossRef]
- Folz, S.J.; Johnson, C.D.; Swensen, S.J. Abdominal Manifestations of Sarcoidosis in CT Studies. J. Comput. Assist. Tomogr. 1995, 19, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Warshauer, D.M.; Molina, P.L.; Hamman, S.M.; Koehler, R.E.; Paulson, E.K.; Bechtold, R.E.; Perlmutter, M.L.; Hiken, J.N.; Francis, I.R.; Cooper, C.J. Nodular Sarcoidosis of the Liver and Spleen: Analysis of 32 Cases. Radiology 1995, 195, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Tetikkurt, C.; Yanardag, H.; Pehlivan, M.; Bilir, M. Clinical Features and Prognostic Significance of Splenic Involvement in Sarcoidosis. Monaldi Arch. Chest Dis. 2017, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warshauer, D.M.; Lee, J.K.T. Imaging Manifestations of Abdominal Sarcoidosis. Am. J. Roentgenol. 2004, 182, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Tana, C.; Donatiello, I.; Coppola, M.G.; Ricci, F.; Maccarone, M.T.; Ciarambino, T.; Cipollone, F.; Giamberardino, M.A. CT Findings in Pulmonary and Abdominal Sarcoidosis. Implications for Diagnosis and Classification. J. Clin. Med. 2020, 9, 3028. [Google Scholar] [CrossRef]
- Ghrenassia, E.; Mekinian, A.; Chapelon-Albric, C.; Levy, P.; Cosnes, J.; Sève, P.; Lefèvre, G.; Dhôte, R.; Launay, D.; Prendki, V.; et al. Digestive-Tract Sarcoidosis: French Nationwide Case-Control Study of 25 Cases. Medicine 2016, 95, e4279. [Google Scholar] [CrossRef]
- Munker, M.; Sharma, O.P. Fatal Gastrointestinal Haemorrhage in Sarcoidosis: A Previously Unreported Occurrence. Sarcoidosis 1987, 4, 55–57. [Google Scholar] [PubMed]
- Inomata, M.; Ikushima, S.; Awano, N.; Kondoh, K.; Satake, K.; Masuo, M.; Moriya, A.; Kamiya, H.; Ando, T.; Azuma, A.; et al. Upper Gastrointestinal Sarcoidosis: Report of Three Cases. Intern. Med. 2012, 51, 1689–1694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubio-Rivas, M.; Corbella, X. Clinical Phenotypes and Prediction of Chronicity in Sarcoidosis Using Cluster Analysis in a Prospective Cohort of 694 Patients. Eur. J. Intern. Med. 2020, 77, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Schupp, J.C.; Freitag-Wolf, S.; Bargagli, E.; Mihailović-Vučinić, V.; Rottoli, P.; Grubanovic, A.; Müller, A.; Jochens, A.; Tittmann, L.; Schnerch, J.; et al. Phenotypes of Organ Involvement in Sarcoidosis. Eur. Respir. J. 2018, 51, 1700991. [Google Scholar] [CrossRef] [Green Version]
- Chapelon-Abric, C.; De Zuttere, D.; Duhaut, P.; Veyssier, P.; Wechsler, B.; Huong, D.L.T.; De Gennes, C.; Papo, T.; Blétry, O.; Godeau, P.; et al. Cardiac Sarcoidosis: A Retrospective Study of 41 Cases. Medicine 2004, 83, 315–334. [Google Scholar] [CrossRef]
- Han, Y.S.; Rivera-Grana, E.; Salek, S.; Rosenbaum, J.T. Distinguishing Uveitis Secondary to Sarcoidosis From Idiopathic Disease: Cardiac Implications. Jama Ophthalmol. 2018, 136, 109. [Google Scholar] [CrossRef]
- Birnie, D.H.; Sauer, W.H.; Bogun, F.; Cooper, J.M.; Culver, D.A.; Duvernoy, C.S.; Judson, M.A.; Kron, J.; Mehta, D.; Cosedis Nielsen, J.; et al. HRS Expert Consensus Statement on the Diagnosis and Management of Arrhythmias Associated with Cardiac Sarcoidosis. Heart Rhythm. 2014, 11, 1304–1323. [Google Scholar] [CrossRef]
- Mehta, D.; Lubitz, S.A.; Frankel, Z.; Wisnivesky, J.P.; Einstein, A.J.; Goldman, M.; Machac, J.; Teirstein, A. Cardiac Involvement in Patients with Sarcoidosis: Diagnostic and Prognostic Value of Outpatient Testing. Chest 2008, 133, 1426–1435. [Google Scholar] [CrossRef]
- Kouranos, V.; Tzelepis, G.E.; Rapti, A.; Mavrogeni, S.; Aggeli, K.; Douskou, M.; Prasad, S.; Koulouris, N.; Sfikakis, P.; Wells, A.; et al. Complementary Role of CMR to Conventional Screening in the Diagnosis and Prognosis of Cardiac Sarcoidosis. JACC Cardiovasc. Imaging 2017, 10, 1437–1447. [Google Scholar] [CrossRef]
- Silverman, K.J.; Hutchins, G.M.; Bulkley, B.H. Cardiac Sarcoid: A Clinicopathologic Study of 84 Unselected Patients with Systemic Sarcoidosis. Circulation 1978, 58, 1204–1211. [Google Scholar] [CrossRef] [Green Version]
- Iwai, K.; Tachibana, T.; Takemura, T.; Matsui, Y.; Kitalchi, M.; Kawabata, Y. Pathological Studies on Sarcoidosis Autopsy. I. Epidemiological Features of 320 Cases in Japan. Pathol. Int. 1993, 43, 372–376. [Google Scholar] [CrossRef]
- Nunes, H.; Freynet, O.; Naggara, N.; Soussan, M.; Weinman, P.; Diebold, B.; Brillet, P.-Y.; Valeyre, D. Cardiac Sarcoidosis. Semin. Respir. Crit. Care Med. 2010, 31, 428–441. [Google Scholar] [CrossRef]
- Kandolin, R.; Lehtonen, J.; Airaksinen, J.; Vihinen, T.; Miettinen, H.; Ylitalo, K.; Kaikkonen, K.; Tuohinen, S.; Haataja, P.; Kerola, T.; et al. Cardiac Sarcoidosis: Epidemiology, Characteristics, and Outcome over 25 Years in a Nationwide Study. Circulation 2015, 131, 624–632. [Google Scholar] [CrossRef]
- Ribeiro Neto, M.L.; Jellis, C.L.; Joyce, E.; Callahan, T.D.; Hachamovitch, R.; Culver, D.A. Update on Cardiac Sarcoidosis. Ann. Am. Thorac. Soc. 2019. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Lower, E.E.; Li, H.-P.; Costea, A.; Attari, M.; Baughman, R.P. Cardiac Sarcoidosis: The Impact of Age and Implanted Devices on Survival. Chest 2017, 151, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Kurmann, R. Echocardiography in Sarcoidosis. Curr. Cardiol. Rep. 2018, 20, 118. [Google Scholar] [CrossRef] [PubMed]
- Terasaki, F.; Yoshinaga, K. New Guidelines for Diagnosis of Cardiac Sarcoidosis in Japan. Ann. Nucl. Cardiol. 2017, 3, 42–45. [Google Scholar] [CrossRef] [Green Version]
- Murtagh, G.; Laffin, L.J.; Beshai, J.F.; Maffessanti, F.; Bonham, C.A.; Patel, V.A.; Yu, Z.; Addetia, K.; Mor-Avi, V.; Moss, J.D.; et al. Prognosis of Myocardial Damage in Sarcoidosis Patients with Preserved Left Ventricular Ejection Fraction: Risk Stratification Using Cardiovascular Magnetic Resonance. Circ. Cardiovasc. Imaging 2016, 9, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Hulten, E.; Agarwal, V.; Cahill, M.; Cole, G.; Vita, T.; Parrish, S.; Bittencourt, M.S.; Murthy, V.L.; Kwong, R.; Di Carli, M.F.; et al. Presence of Late Gadolinium Enhancement by Cardiac Magnetic Resonance Among Patients With Suspected Cardiac Sarcoidosis Is Associated With Adverse Cardiovascular Prognosis. Circ. Cardiovasc. Imaging 2016, 9, 139–148. [Google Scholar] [CrossRef] [Green Version]
- Nadel, J.; Lancefield, T.; Voskoboinik, A.; Taylor, A.J. Late Gadolinium Enhancement Identified with Cardiacmagnetic Resonance Imaging in Sarcoidosis Patients Is Associated with Long-Term Ventricular Arrhythmia and Sudden Cardiac Death. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 634–641. [Google Scholar] [CrossRef] [Green Version]
- Shafee, M.A.; Fukuda, K.; Wakayama, Y.; Nakano, M.; Kondo, M.; Hasebe, Y.; Kawana, A.; Shimokawa, H. Delayed Enhancement on Cardiac Magnetic Resonance Imaging Is a Poor Prognostic Factor in Patients with Cardiac Sarcoidosis. J. Cardiol. 2012, 60, 448–453. [Google Scholar] [CrossRef] [Green Version]
- Vita, T.; Okada, D.R.; Veillet-Chowdhury, M.; Bravo, P.E.; Mullins, E.; Hulten, E.; Agrawal, M.; Madan, R.; Taqueti, V.R.; Steigner, M.; et al. Complementary Value of Cardiac Magnetic Resonance Imaging and Positron Emission Tomography/Computed Tomography in the Assessment of Cardiac Sarcoidosis. Circ. Cardiovasc. Imaging 2018, 11, e007030. [Google Scholar] [CrossRef] [PubMed]
- Birnie, D.; Beanlands, R.S.B.; Nery, P.; Aaron, S.D.; Culver, D.A.; DeKemp, R.A.; Gula, L.; Ha, A.; Healey, J.S.; Inoue, Y.; et al. Cardiac Sarcoidosis Multi-Center Randomized Controlled Trial (CHASM CS- RCT). Am. Heart J. 2020, 220, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Ardehali, H.; Howard, D.L.; Hariri, A.; Qasim, A.; Hare, J.M.; Baughman, K.L.; Kasper, E.K. A Positive Endomyocardial Biopsy Result for Sarcoid Is Associated with Poor Prognosis in Patients with Initially Unexplained Cardiomyopathy. Am. Heart J. 2005, 150, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Fritz, D.; van de Beek, D.; Brouwer, M.C. Clinical Features, Treatment and Outcome in Neurosarcoidosis: Systematic Review and Meta-Analysis. BMC Neurol. 2016, 16, 220. [Google Scholar] [CrossRef] [Green Version]
- Cação, G.; Branco, A.; Meireles, M.; Alves, J.E.; Mateus, A.; Silva, A.M.; Santos, E. Neurosarcoidosis According to Zajicek and Scolding Criteria: 15 Probable and Definite Cases, Their Treatment and Outcomes. J. Neurol. Sci. 2017, 379, 84–88. [Google Scholar] [CrossRef]
- Kidd, D.P. Neurosarcoidosis: Clinical Manifestations, Investigation and Treatment. Pract. Neurol. 2020, 20, 199–212. [Google Scholar] [CrossRef]
- Ungprasert, P.; Crowson, C.S.; Matteson, E.L. Characteristics and Long-Term Outcome of Neurosarcoidosis: A Population-Based Study from 1976-2013. Neuroepidemiology 2017, 48, 87–94. [Google Scholar] [CrossRef]
- Ungprasert, P.; Matteson, E.L. Neurosarcoidosis. Rheum. Dis. Clin. N. Am. 2017, 43, 593–606. [Google Scholar] [CrossRef]
- Culver, D.A.; Neto, M.L.R.; Moss, B.P.; Willis, M.A. Neurosarcoidosis. Semin. Respir. Crit. Care Med. 2017, 38, 499–513. [Google Scholar] [CrossRef]
- Joubert, B.; Chapelon-Abric, C.; Biard, L.; Saadoun, D.; Demeret, S.; Dormont, D.; Resche-Rigon, M.; Cacoub, P. Association of Prognostic Factors and Immunosuppressive Treatment With Long-Term Outcomes in Neurosarcoidosis. JAMA Neurol. 2017, 74, 1336–1344. [Google Scholar] [CrossRef]
- Bridel, C.; Courvoisier, D.S.; Vuilleumier, N.; Lalive, P.H. Cerebrospinal Fluid Angiotensin-Converting Enzyme for Diagnosis of Neurosarcoidosis. J. Neuroimmunol. 2015, 285, 1–3. [Google Scholar] [CrossRef]
- Arun, T.; Pattison, L.; Palace, J. Distinguishing Neurosarcoidosis from Multiple Sclerosis Based on CSF Analysis: A Retrospective Study. Neurology 2020, 94, e2545–e2554. [Google Scholar] [CrossRef] [PubMed]
- Chazal, T.; Costopoulos, M.; Maillart, E.; Fleury, C.; Psimaras, D.; Legendre, P.; Pineton de Chambrun, M.; Haroche, J.; Lubetzki, C.; Amoura, Z.; et al. The Cerebrospinal Fluid CD4/CD8 Ratio and Interleukin-6 and -10 Levels in Neurosarcoidosis: A Multicenter, Pragmatic, Comparative Study. Eur. J. Neurol. 2019, 26, 1274–1280. [Google Scholar] [CrossRef] [PubMed]
- Stern, B.J.; Aksamit, A.; Clifford, D.; Scott, T.F. Neurosarcoidosis Study Group Neurologic Presentations of Sarcoidosis. Neurol. Clin. 2010, 28, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Scott, T.F.; Yandora, K.; Valeri, A.; Chieffe, C.; Schramke, C. Aggressive Therapy for Neurosarcoidosis: Long-Term Follow-up of 48 Treated Patients. Arch. Neurol. 2007, 64, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Bogousslavsky, J.; Hungerbühler, J.P.; Regli, F.; Graf, H.J. Subacute Myelopathy as the Presenting Manifestation of Sarcoidosis. Acta Neurochir. 1982, 65, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Durel, C.-A.; Marignier, R.; Maucort-Boulch, D.; Iwaz, J.; Berthoux, E.; Ruivard, M.; André, M.; Le Guenno, G.; Pérard, L.; Dufour, J.-F.; et al. Clinical Features and Prognostic Factors of Spinal Cord Sarcoidosis: A Multicenter Observational Study of 20 BIOPSY-PROVEN Patients. J. Neurol. 2016, 263, 981–990. [Google Scholar] [CrossRef] [PubMed]
- Spencer, T.S.; Campellone, J.V.; Maldonado, I.; Huang, N.; Usmani, Q.; Reginato, A.J. Clinical and Magnetic Resonance Imaging Manifestations of Neurosarcoidosis. Semin. Arthritis Rheum. 2005, 34, 649–661. [Google Scholar] [CrossRef]
- Murphy, O.; Salazar-Camelo, A.; Jimenez, J.; Barreras, P.; Reyes, M.; Garcia, M.; Moller, D.; Chen, E.; Pardo, C. Clinical and MRI Phenotypes of Sarcoidosis-Associated Myelopathy. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7, e722. [Google Scholar] [CrossRef] [Green Version]
- Freda, P.U.; Post, K.D. Differential Diagnosis of Sellar Masses. Endocrinol. Metab. Clin. N. Am. 1999, 28, 81–117. [Google Scholar] [CrossRef]
- Langrand, C.; Bihan, H.; Raverot, G.; Varron, L.; Androdias, G.; Borson-Chazot, F.; Brue, T.; Cathebras, P.; Pinede, L.; Muller, G.; et al. Hypothalamo-Pituitary Sarcoidosis: A Multicenter Study of 24 Patients. QJM 2012, 105, 981–995. [Google Scholar] [CrossRef] [Green Version]
- Tavee, J.O.; Karwa, K.; Ahmed, Z.; Thompson, N.; Parambil, J.; Culver, D.A. Sarcoidosis-Associated Small Fiber Neuropathy in a Large Cohort: Clinical Aspects and Response to IVIG and Anti-TNF Alpha Treatment. Respir. Med. 2017, 126, 135–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoitsma, E.; Reulen, J.P.H.; de Baets, M.; Drent, M.; Spaans, F.; Faber, C.G. Small Fiber Neuropathy: A Common and Important Clinical Disorder. J. Neurol. Sci. 2004, 227, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Parambil, J.G.; Tavee, J.O.; Zhou, L.; Pearson, K.S.; Culver, D.A. Efficacy of Intravenous Immunoglobulin for Small Fiber Neuropathy Associated with Sarcoidosis. Respir. Med. 2011, 105, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Hoitsma, E.; De Vries, J.; Drent, M. The Small Fiber Neuropathy Screening List: Construction and Cross-Validation in Sarcoidosis. Respir. Med. 2011, 105, 95–100. [Google Scholar] [CrossRef] [Green Version]
- Hebel, R.; Dubaniewicz-Wybieralska, M.; Dubaniewicz, A. Overview of Neurosarcoidosis: Recent Advances. J. Neurol. 2015, 262, 258–267. [Google Scholar] [CrossRef] [Green Version]
- Colvin, I.B. Audiovestibular Manifestations of Sarcoidosis: A Review of the Literature. Laryngoscope 2006, 116, 75–82. [Google Scholar] [CrossRef]
- Hoitsma, E.; Faber, C.G.; Drent, M.; Sharma, O.P. Neurosarcoidosis: A Clinical Dilemma. Lancet Neurol 2004, 3, 397–407. [Google Scholar] [CrossRef]
- Burns, T.M.; Dyck, P.J.B.; Aksamit, A.J.; Dyck, P.J. The Natural History and Long-Term Outcome of 57 Limb Sarcoidosis Neuropathy Cases. J. Neurol. Sci. 2006, 244, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Jachiet, V.; Lhote, R.; Rufat, P.; Pha, M.; Haroche, J.; Crozier, S.; Dupel-Potier, C.; Psimaras, D.; Amoura, Z.; Cohen Aubart, F. Clinical, Imaging, and Histological Presentations and Outcomes of Stroke Related to Sarcoidosis. J. Neurol. 2018, 265, 2333–2341. [Google Scholar] [CrossRef]
- Mahévas, M.; Lescure, F.X.; Boffa, J.-J.; Delastour, V.; Belenfant, X.; Chapelon, C.; Cordonnier, C.; Makdassi, R.; Piette, J.-C.; Naccache, J.-M.; et al. Renal Sarcoidosis: Clinical, Laboratory, and Histologic Presentation and Outcome in 47 Patients. Medicine 2009, 88, 98–106. [Google Scholar] [CrossRef]
- Cozier, Y.C.; Berman, J.S.; Palmer, J.R.; Boggs, D.A.; Serlin, D.M.; Rosenberg, L. Sarcoidosis in Black Women in the United States: Data from the Black Women’s Health Study. Chest 2011, 139, 144–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Judson, M.A.; Boan, A.D.; Lackland, D.T. The Clinical Course of Sarcoidosis: Presentation, Diagnosis, and Treatment in a Large White and Black Cohort in the United States. Sarcoidosis Vasc. Diffus. Lung Dis. 2012, 29, 119–127. [Google Scholar]
- Kamata, Y.; Sato, H.; Joh, K.; Tsuchiya, Y.; Kunugi, S.; Shimizu, A.; Konta, T.; Baughman, R.P.; Azuma, A. Clinical Characteristics of Biopsy-Proven Renal Sarcoidosis in Japan. Sarcoidosis Vasc. Diffus. Lung Dis. 2018, 35, 252–260. [Google Scholar] [CrossRef]
- Javaud, N.; Belenfant, X.; Stirnemann, J.; Laederich, J.; Ziol, M.; Callard, P.; Ronco, P.; Rondeau, E.; Fain, O. Renal Granulomatoses: A Retrospective Study of 40 Cases and Review of the Literature. Medicine 2007, 86, 170–180. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Carter-Monroe, N.; Atta, M.G. Granulomatous Interstitial Nephritis. Clin. Kidney J. 2015, 8, 516–523. [Google Scholar] [CrossRef] [Green Version]
- Clive, D.M.; Vanguri, V.K. The Syndrome of Tubulointerstitial Nephritis With Uveitis (TINU). Am. J. Kidney Dis. 2018, 72, 118–128. [Google Scholar] [CrossRef]
- Bergner, R.; Hoffmann, M.; Waldherr, R.; Uppenkamp, M. Frequency of Kidney Disease in Chronic Sarcoidosis. Sarcoidosis Vasc. Diffus. Lung Dis. 2003, 20, 126–132. [Google Scholar]
- Bergner, R.; Löffler, C. Renal Sarcoidosis: Approach to Diagnosis and Management. Curr. Opin. Pulm. Med. 2018, 24, 513–520. [Google Scholar] [CrossRef]
- Mrówka-Kata, K.; Kata, D.; Lange, D.; Namysłowski, G.; Czecior, E.; Banert, K. Sarcoidosis and Its Otolaryngological Implications. Eur. Arch. Oto-Rhino-Laryngol. Off. J. Eur. Fed. Oto-Rhino-Laryngol. Soc. (Eufos) Affil. Ger. Soc. Oto-Rhino-Laryngol. Head Neck Surg. 2010, 267, 1507–1514. [Google Scholar] [CrossRef] [PubMed]
- Aubart, F.C.; Ouayoun, M.; Brauner, M.; Attali, P.; Kambouchner, M.; Valeyre, D.; Nunes, H. Sinonasal Involvement in Sarcoidosis: A Case-Control Study of 20 Patients. Medicine 2006, 85, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Lawson, W.; Jiang, N.; Cheng, J. Sinonasal Sarcoidosis: A New System of Classification Acting as a Guide to Diagnosis and Treatment. Am. J. Rhinol. Allergy 2014, 28, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Edriss, H.; Kelley, J.S.; Demke, J.; Nugent, K. Sinonasal and Laryngeal Sarcoidosis—An Uncommon Presentation and Management Challenge. Am. J. Med. Sci. 2019, 357, 93–102. [Google Scholar] [CrossRef]
- Duchemann, B.; Lavolé, A.; Naccache, J.-M.; Nunes, H.; Benzakin, S.; Lefevre, M.; Kambouchner, M.; Périé, S.; Valeyre, D.; Cadranel, J. Laryngeal Sarcoidosis: A Case-Control Study. Sarcoidosis Vasc. Diffus. Lung Dis. 2014, 31, 227–234. [Google Scholar]
- Rotman, A.; Maughan, E.F.; Rouhani, M.J.; Holroyd, A.; Ashcroft, M.; Al Yaghchi, C.; Sandhu, G. Laryngeal Sarcoidosis at a Tertiary Airway Centre: Our Experience with 32 Patients. Clin. Otolaryngol. 2020. [Google Scholar] [CrossRef]
- Lhote, R.; Annesi-Maesano, I.; Nunes, H.; Launay, D.; Borie, R.; Sacré, K.; Schleinitz, N.; Hamidou, M.; Mahevas, M.; Devilliers, H.; et al. Clinical Phenotypes of Extrapulmonary Sarcoidosis: An Analysis of a French, Multiethnic, Multicenter Cohort. Eur. Respir. J. 2020, 2001160. [Google Scholar] [CrossRef]
- Kreider, M.E.; Christie, J.D.; Thompson, B.; Newman, L.; Rose, C.; Barnard, J.; Bresnitz, E.; Judson, M.A.; Lackland, D.T.; Rossman, M.D. Relationship of Environmental Exposures to the Clinical Phenotype of Sarcoidosis. Chest 2005, 128, 207–215. [Google Scholar] [CrossRef]
- Judson, M.A.; Costabel, U.; Drent, M.; Wells, A.; Maier, L.; Koth, L.; Shigemitsu, H.; Culver, D.A.; Gelfand, J.; Valeyre, D.; et al. The WASOG Sarcoidosis Organ Assessment Instrument: An Update of a Previous Clinical Tool. Sarcoidosis Vasc. Diffus. Lung Dis. 2014, 31, 19–27. [Google Scholar]
- Bickett, A.N.; Lower, E.E.; Baughman, R.P. Sarcoidosis Diagnostic Score. Chest 2018, 154, 1052–1060. [Google Scholar] [CrossRef]
- Agrawal, A.; Ghori, U.; Chaddha, U.; Murgu, S. Combined EBUS-IFB and EBUS-TBNA vs. EBUS-TBNA Alone for Intrathoracic Adenopathy: A Meta-Analysis. Ann. Thorac. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Bernard, C.; Kodjikian, L.; Bancel, B.; Isaac, S.; Broussolle, C.; Seve, P. Ocular Sarcoidosis: When Should Labial Salivary Gland Biopsy Be Performed? Graefes Arch. Clin. Exp. Ophthalmol. 2013, 251, 855–860. [Google Scholar] [CrossRef]
- Blaise, P.; Fardeau, C.; Chapelon, C.; Bodaghi, B.; Le Hoang, P. Minor Salivary Gland Biopsy in Diagnosing Ocular Sarcoidosis. Br. J. Ophthalmol. 2011, 95, 1731–1734. [Google Scholar] [CrossRef] [PubMed]
- Keijsers, R.G.M.; Grutters, J.C. In Which Patients with Sarcoidosis Is FDG PET/CT Indicated? J. Clin. Med. 2020, 9, 890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahmi, A.; Deshayes, E.; Maucort-Boulch, D.; Varron, L.; Grange, J.D.; Kodjikian, L.; Seve, P. Intraocular Sarcoidosis: Association of Clinical Characteristics of Uveitis with Findings from 18 F-Labelled Fluorodeoxyglucose Positron Emission Tomography. Br. J. Ophthalmol. 2012, 96, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.L.; Fong, H.K.; Birati, E.Y.; Han, Y. Cardiac Sarcoidosis. Am. J. Cardiol. 2019, 123, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Yoshinaga, K.; Miyagawa, M.; Kiso, K.; Ishida, Y. Japanese Guidelines for Cardiac Sarcoidosis. Ann. Nucl. Cardiol. 2017, 3, 121–124. [Google Scholar] [CrossRef] [Green Version]
- Stern, B.J.; Royal, W.; Gelfand, J.M.; Clifford, D.B.; Tavee, J.; Pawate, S.; Berger, J.R.; Aksamit, A.J.; Krumholz, A.; Pardo, C.A.; et al. Definition and Consensus Diagnostic Criteria for Neurosarcoidosis: From the Neurosarcoidosis Consortium Consensus Group. JAMA Neurol. 2018, 75, 1546. [Google Scholar] [CrossRef] [PubMed]
- Herbort, C.P.; Rao, N.A.; Mochizuki, M. The members of the Scientific Commi International Criteria for the Diagnosis of Ocular Sarcoidosis: Results of the First International Workshop on Ocular Sarcoidosis (IWOS). Ocul. Immunol. Inflamm. 2009, 17, 160–169. [Google Scholar] [CrossRef]
- Mochizuki, M.; Smith, J.R.; Takase, H.; Kaburaki, T.; Acharya, N.R.; Rao, N.A. Revised Criteria of International Workshop on Ocular Sarcoidosis (IWOS) for the Diagnosis of Ocular Sarcoidosis. Br. J. Ophthalmol. 2019, 103, 1418–1422. [Google Scholar] [CrossRef]
- Rosen, Y. Four Decades of Necrotizing Sarcoid Granulomatosis: What Do We Know Now? Arch. Pathol. Lab. Med. 2015, 139, 252–262. [Google Scholar] [CrossRef] [Green Version]
- Criado, E.; Sánchez, M.; Ramírez, J.; Arguis, P.; de Caralt, T.M.; Perea, R.J.; Xaubet, A. Pulmonary Sarcoidosis: Typical and Atypical Manifestations at High-Resolution CT with Pathologic Correlation. RadioGraphics 2010, 30, 1567–1586. [Google Scholar] [CrossRef] [Green Version]
- Park, H.J.; Jung, J.I.; Chung, M.H.; Song, S.W.; Kim, H.L.; Baik, J.H.; Han, D.H.; Kim, K.J.; Lee, K.-Y. Typical and Atypical Manifestations of Intrathoracic Sarcoidosis. Korean J. Radiol. 2009, 10, 623. [Google Scholar] [CrossRef] [Green Version]
- Spagnolo, P.; Luppi, F.; Roversi, P.; Cerri, S.; Fabbri, L.M.; Richeldi, L. Sarcoidosis: Challenging Diagnostic Aspects of an Old Disease. Am. J. Med. 2012, 125, 118–125. [Google Scholar] [CrossRef] [Green Version]
- El Jammal, T.; Jamilloux, Y.; Gerfaud-Valentin, M.; Valeyre, D.; Sève, P. Refractory Sarcoidosis: A Review. TCRM 2020, 16, 323–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gousseff, M.; Mechaï, F.; Lecuit, M.; Lortholary, O. Les granulomatoses systémiques d’origine infectieuse. La Rev. De Médecine Interne 2008, 29, 15–27. [Google Scholar] [CrossRef]
- Piotrowski, W.J.; Żądło, P.P.L.J.; Górski, W.; Kumor-Kisielewska, A.; Fijałkowski, M.; Kurmanowska, Z.; Marczak, J.; Gwadera, Ł.; Angowski, W.; Górski, P.; et al. QuantiFERON-TB-GOLD In-Tube in Patients with Sarcoidosis. Adv. Respir. Med. 2018, 86, 234–239. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, C.E.; Miller, D.R.; Schneider, P.S.; Roberts, G.D. Evaluation of Gen-Probe Amplified Mycobacterium Tuberculosis Direct Test by Using Respiratory and Nonrespiratory Specimens in a Tertiary Care Center Laboratory. J. Clin. Microbiol. 2002, 40, 1723–1727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhooria, S.; Gupta, N.; Bal, A. Role of Xpert MTB/RIF in Differentiating Tuberculosis from Sarcoidosis in Patients with Mediastinal Lymphadenopathy Undergoing EBUS-TBNA: A Study of 147 Patients. Sarcoidosis Vasc. Diffus. Lung Dis. 2016, 33, 258–266. [Google Scholar]
- Ohshimo, S.; Guzman, J.; Costabel, U.; Bonella, F. Differential Diagnosis of Granulomatous Lung Disease: Clues and Pitfalls: Number 4 in the Series “Pathology for the Clinician” Edited by Peter Dorfmüller and Alberto Cavazza. Eur. Respir. Rev. 2017, 26, 170012. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Casals, M.; Mañá, J.; Nardi, N.; Brito-Zerón, P.; Xaubet, A.; Sánchez-Tapias, J.M.; Cervera, R.; Font, J. Sarcoidosis in Patients With Chronic Hepatitis C Virus Infection: Analysis of 68 Cases. Medicine 2005, 84, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Chopra, A.; Nautiyal, A.; Kalkanis, A.; Judson, M.A. Drug-Induced Sarcoidosis-Like Reactions. Chest 2018, 154, 664–677. [Google Scholar] [CrossRef] [PubMed]
- Cohen Aubart, F.; Lhote, R.; Amoura, A.; Valeyre, D.; Haroche, J.; Amoura, Z.; Lebrun-Vignes, B. Drug-induced Sarcoidosis: An Overview of the WHO Pharmacovigilance Database. J. Intern. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Bouvry, D.; Mouthon, L.; Brillet, P.-Y.; Kambouchner, M.; Ducroix, J.-P.; Cottin, V.; Haroche, J.; Viallard, J.-F.; Lazor, R.; Lebargy, F.; et al. Granulomatosis-Associated Common Variable Immunodeficiency Disorder: A Case-Control Study versus Sarcoidosis. Eur. Respir. J. 2013, 41, 115–122. [Google Scholar] [CrossRef] [Green Version]
- El Jammal, T.; Pavic, M.; Gerfaud-Valentin, M.; Jamilloux, Y.; Seve, P. Sarcoidosis and Cancer: A Complex Relationship. Front. Med. 2020. Accepted for publication. [Google Scholar] [CrossRef]
- Lococo, F.; Muoio, B.; Chiappetta, M.; Nachira, D.; Petracca Ciavarella, L.; Margaritora, S.; Treglia, G. Diagnostic Performance of PET or PET/CT with Different Radiotracers in Patients with Suspicious Lung Cancer or Pleural Tumours According to Published Meta-Analyses. Contrast Media Mol. Imaging 2020, 2020, 1–7. [Google Scholar] [CrossRef]
- Law, L.Y.; Riminton, D.S.; Nguyen, M.; Barnett, M.H.; Reddel, S.W.; Hardy, T.A. The Spectrum of Immune-Mediated and Inflammatory Lesions of the Brainstem: Clues to Diagnosis. Neurology 2019, 93, 390–405. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Common | Papules and papulonodules |
|
| Plaques |
| |
| Lupus pernio |
| |
| Subcutaneous Nodules |
| |
| Uncommon | Ichtyosiform |
|
| Atrophic and ulcerative |
| |
| Mucosal |
| |
| Erythroderma |
| |
| Alopecia |
| |
| Nail sarcoidosis |
|
| Location | Description |
|---|---|
| Lacrimal glands and Lacrimal drainage system (10–69%) | Often asymptomatic. Keratoconjunctivitis sicca (15–31%). Enlargement of the lacrimal glands is less frequent; the diagnosis can be made on Lacrimal gland biopsy. |
| Orbit | Women over 50. Diffuse orbital inflammation, usually unilateral, which can result in ptosis, limitations of ocular movements and diplopia. |
| Ocular nerve palsy can occur from sarcoid involvement of the 3rd, 4th and 6th cranial nerves | |
| Eyelid | Granuloma |
| Conjunctiva (6–40%) | Paucisymptomatic. Granuloma, conjunctivitis |
| Sclera (<3%) | Scleritis, episcleritis: diffuse inflammation, plaque or nodule; the diagnosis may be made with biopsy of a scleral nodule |
| Cornea | Interstitial keratitis (extremely rare). |
| Optic nerve (1–5%) | Optic neuropathy (++), granuloma, retrobulbar optic neuritis |
| Predominantly Caucasian females. Frequently accompanied with uveitis and other findings of neurosarcoidosis. Prognosis is not favorable and permanent impaired visual acuity occurs in about one third of the patients. Sarcoidosis patients with opitc neuritis often experience a chronic course of the disease and steroid-sparing alternatives are commonly used. | |
| Other neuro-ophthalmic manifestations | Rare: Horner’s syndrome, tonic pupil and optic-tract involvement |
| Common | Cranial nerves |
|
| Meningeal |
| |
| Brain parenchyma |
| |
| Uncommon | Spinal cord |
|
| Pituitary |
| |
| Peripheral neuropathy |
| |
| Stroke |
|
| Histological Diagnosis | Clinical Diagnosis |
|---|---|
| Presence of extracardiac sarcoidosis based on histological or clinical criteria plus either of the following:
|
| Histological Diagnosis | Clinical Diagnosis |
|---|---|
| It is probable cardiac sarcoidosis if:
|
| Definite |
|---|
|
| Probable |
|
| Possible |
|
| I. Other causes of granulomatous uveitis must be ruled out |
| II. Intraocular signs suggestive of ocular sarcoidosis |
|
|
|
|
|
|
|
| III. Systemic investigations results in suspected ocular sarcoidosis |
|
|
|
|
|
|
|
|
| Diagnostic criteria of ocular sarcoidosis |
| Diagnostic criteria of ocular sarcoidosis were worked out in 3 levels of certainty: |
|
|
|
| Sarcoidosis Subtype | Possible Differential Diagnosis |
|---|---|
| Mediastino pulmonary sarcoidosis | Tuberculosis and mycobacterial infections |
| Hodgkin’s disease and non Hodgkin’s lymphoma | |
| Histoplasmosis, coccidioidomycosis, aspergillosis | |
| Pneumoconiosis: chronic beryllium disease, titanium, aluminium, talc | |
| Hypersensitivity pneumonitis | |
| Drug reactions | |
| Granulomatosis with polyangiitis, granulomatosis with eosinophilia and polyangiitis | |
| Extra thoracic sarcoidosis | Tuberculosis and mycobacterial infections |
| Whipple disease, bartonellosis, Q fever, brucellosis, syphilis, toxoplasmosis, fungal infections | |
| Hodgkin disease and non Hodgkin’s lymphoma | |
| Tumor associated sarcoid reaction | |
| Crohn’s disease, primary biliary cirrhosis | |
| Drug induced sarcoidosis (interferon α and β, intravesical BCG therapy, TNFα inhibitors, immune check point inhibitors) | |
| Common variable immunodeficiency |
| Infectious diseases Tuberculosis Whipple’s disease Toxoplasmosis Histoplasmosis Toxocarosis Treponemal infections Lyme disease |
| Granulomatous diseases (exclusion of infectious diseases) Granulomatosis with polyangiitis Lymphomatoid granulomas |
| Tumors Neurolymphomas (e.g., Intravascular lymphoma) Histiocytic disorders (e.g., Erdheim–Chester disease) Gliomas Menineomas Leptmeningeal metastases |
| Vasculitis Behçet’s disease |
| Systemic diseases Lupus Sjôgren Amyloidosis Ig4-related disease |
| Lymphocytic adenohypophysitis |
| Neurological diseases Multiple sclerosis Neuromyelitis optica spectrum disorder spectrum and myelin oligodendrocyte antibody-induced demyelination Autoimmune/paraneoplastic encephalitis Susac syndrome Chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids (CLIPPERS) Acute demyelinating encephalomyelitis Primary angiitis of the central nervous system |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sève, P.; Pacheco, Y.; Durupt, F.; Jamilloux, Y.; Gerfaud-Valentin, M.; Isaac, S.; Boussel, L.; Calender, A.; Androdias, G.; Valeyre, D.; et al. Sarcoidosis: A Clinical Overview from Symptoms to Diagnosis. Cells 2021, 10, 766. https://doi.org/10.3390/cells10040766
Sève P, Pacheco Y, Durupt F, Jamilloux Y, Gerfaud-Valentin M, Isaac S, Boussel L, Calender A, Androdias G, Valeyre D, et al. Sarcoidosis: A Clinical Overview from Symptoms to Diagnosis. Cells. 2021; 10(4):766. https://doi.org/10.3390/cells10040766
Chicago/Turabian StyleSève, Pascal, Yves Pacheco, François Durupt, Yvan Jamilloux, Mathieu Gerfaud-Valentin, Sylvie Isaac, Loïc Boussel, Alain Calender, Géraldine Androdias, Dominique Valeyre, and et al. 2021. "Sarcoidosis: A Clinical Overview from Symptoms to Diagnosis" Cells 10, no. 4: 766. https://doi.org/10.3390/cells10040766