

Experimental Early Stimulation of Bone Tissue Neo-Formation for Critical Size Elimination Defects in the Maxillofacial Region

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
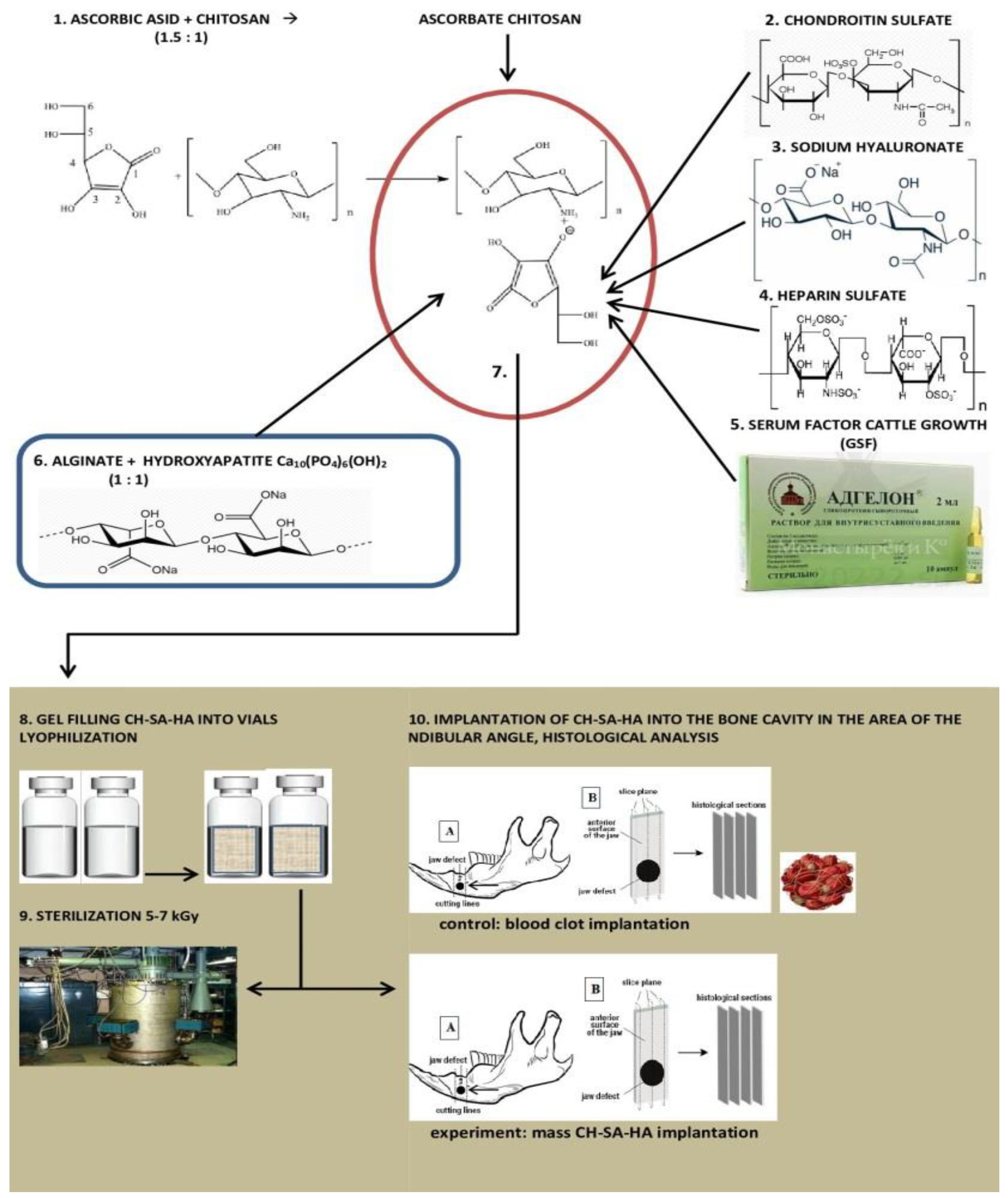
2.1. Composition of CH–SA–HA Construction
2.2. Experimental Animals
2.3. Modeling Defects of the Critical Size of the Mandibular Angle in Rats
2.4. Morphological Analysis of Bone Tissue
2.5. Statistical Analysis
3. Results
3.1. Morphological Analysis of Bone Tissue Restoration in the Early Stages in the Defect Zone
3.2. Regeneration of Bone Tissue in the Defect Area within 2–4 Weeks
3.3. Regeneration of Bone Tissue in the Defect Area within 6–10 Weeks
4. Summary
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lou, X. Induced pluripotent stem cells as a new strategy for osteogenesis and bone regeneration. Stem Cell Rev. Rep. 2015, 11, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Raposo-Amaral, C.E.; Bueno, D.F.; Almeida, A.B.; Jorgetti, V.; Costa, C.C.; Gouveia, C.H.; Vulcano, L.C.; Fanganiello, R.D.; Passos-Bueno, M.R.; Alonso, N. Is bone transplantation the gold standard for repair of alveolar bone defects? J. Tissue Eng. 2014, 5, 2041731413519352. [Google Scholar] [CrossRef] [PubMed]
- Shanbhag, S.; Pandis, N.; Mustafa, K.; Nyengaard, J.R.; Stavropoulos, A. Alveolar bone tissue engineering in critical-size defects of experimental animal models: A systematic review and meta-analysis. J. Tissue Eng. Regen. Med. 2017, 11, 2935–2949. [Google Scholar] [CrossRef]
- Khan, F.; Tanaka, M.; Rafi, S. Ahmad fabrication of polymeric biomaterials: A strategy for tissue engineering and medical devices. J. Mater. Chem. B. 2015, 3, 8224–8249. [Google Scholar] [CrossRef] [PubMed]
- Henkel, J.; Woodruff, M.A.; Epari, D.R.; Steck, R.; Glatt, V.; Dickinson, I.C.; Choong, P.F.M.; Schuetz, M.A.; Hutmacher, D.W. Bone regeneration based on tissue engineering conceptions—A 21st century perspective. Bone Res. 2013, 3, 216–248. [Google Scholar] [CrossRef]
- Bolshakov, I.N.; Levenetz, A.A.; Furtsev, T.V.; Kotikov, A.R.; Patlataya, N.N.; Ryaboshapko, E.I.; Dmitrienko, A.E.; Nikolaenko, M.M.; Matveeva, N.D.; Ibragimov, I.G. Experimental Reconstruction of Critical Size Defect of Bone Tissue in the Maxillofacial Region When Using Modified Chitosan. Biomed. Transl. Sci. 2022, 12, 1–8. [Google Scholar]
- Bolshakov, I.N.; Gornostaev, L.M.; Fominykh, O.I.; Svetlakov, A.V. Synthesis, Chemical and Biomedical Aspects of the Use of Sulfated Chitosan. Polymers 2022, 14, 3431. [Google Scholar] [CrossRef]
- Li, Y.; Kim, J.H.; Choi, E.H.; Han, I. Promotion of osteogenic differentiation by non-thermal biocompatible plasma treated chitosan scaffold. Sci. Rep. 2019, 9, 3712. [Google Scholar] [CrossRef]
- Carletti, E.; Motta, A.; Migliaresi, C. Scaffolds for tissue engineering and 3D cell culture. Methods Mol. Biol. 2011, 695, 17–39. [Google Scholar]
- Jiang, T.; Khan, Y.; Nair, L.S.; Abdel-Fattah, W.I.; Laurencin, C.T. Functionalization of chitosan/poly(lactic acid-glycolic acid) sintered microsphere scaffolds via surface heparinization for bone tissue engineering. J. Biomed. Mater. Res. A. 2010, 93, 1193–1208. [Google Scholar] [CrossRef]
- Sukpaita, T.; Chirachanchai, S.; Suwattanachai, P.; Everts, V.; Pimkhaokham, A.; Ampornaramveth, R.S. In vivo bone regeneration induced by a scaffold of chitosan/dicarboxylic acid seeded with human periodontal ligament cells. Int. J. Mol. Sci. 2019, 20, 4883. [Google Scholar] [CrossRef] [PubMed]
- Dhandayuthapani, B.; Yoshida, Y.; Maekawa, T.; Kumar, D.S. Polymeric scaffolds in tissue engineering application: A review. Int. J. Polym. Sci. 2011, 2011, 290602. [Google Scholar] [CrossRef]
- Chatzipetros, E.; Christopoulos, P.; Donta, C.; Tosios, K.-I.; Tsiambas, E.; Tsiourvas, D.; Kalogirou, E.-M.; Tsiklakis, K. Research application of nano-hydroxyapatite/chitosan scaffolds on rat calvarial critical-sized defects: A pilot study. Med. Oral Patol. Oral Cir. Bucal. 2018, 23, e625–e632. [Google Scholar] [PubMed]
- La, W.-G.; Jang, J.; Kim, B.S.; Lee, M.S.; Cho, D.-W.; Yang, H.S. Systemically replicated organic and inorganic bony microenvironment for new bone formation generated by a 3D printing technology. RSC Adv. 2016, 6, 11546–11553. [Google Scholar] [CrossRef]
- Ko, H.F.; Sfeir, C.; Kumta, P.N. Novel synthesis strategies for natural polymer and composite biomaterials as potential scaffolds for tissue engineering. Philos. Trans. R. Soc. A 2010, 28, 1981–1997. [Google Scholar] [CrossRef]
- Vukajlovic, D.; Parker, J.; Bretcanu, O.; Novakovic, K. Chitosan based polymer/bioglass composites for tissue engineering applications. Mater. Sci. Eng. C-Mater. Biol. Appl. 2019, 96, 955–967. [Google Scholar] [CrossRef]
- Kirichenko, A.K.; Patlataya, N.N.; Sharkova, A.F.; Pevnev, A.A.; Kontorev, K.V.; Shapovalova, O.V.; Gorban, M.E.; Bolshakov, I.N. Pathomorphism of Limb Major Vessels in Experimental Atherogenic Inflammation. The Role of Adventitial Intimal Relations. Review. Mod. Technol. Med. 2017, 9, 157–163. [Google Scholar] [CrossRef]
- Waters, D.J.; Engberg, K.; Parke-Houben, R.; Ta, C.N.; Jackson, A.J.; Toney, M.F.; Frank, C.W. Structure and mechanism of strength enhancement in interpenetrating polymer network hydrogels. Macromolecules 2011, 44, 5776–5787. [Google Scholar] [CrossRef]
- TiǧlI, R.S.; Gumüşderelioǧlu, M. Evaluation of alginate-chitosan semi IPNs as cartilage scaffolds. J. Mater. Sci. Mater. Med. 2009, 20, 699–709. [Google Scholar] [CrossRef]
- Matricardi, P.; Di Meo, C.; Coviello, T.; Hennink, W.E.; Alhaique, F. Interpenetrating polymer networks polysaccharide hydrogels for drug delivery and tissue engineering. Adv. Drug Deliv. Rev. 2013, 65, 1172–1187. [Google Scholar] [CrossRef]
- Venkatesan, J.; Bhatnagar, I.; Manivasagan, P.; Kang, K.-H.; Kim, S.-K. Alginate composites for bone tissue engineering: A review. Int. J. Biol. Macromol. 2015, 72, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.-H.; Lee, C.-H.; Lee, W.-K.; Lee, J.-K.; Park, H.-C.; Yoon, S.-Y. In-situ formation of the hydroxyapatite/chitosan-alginate composite scaffolds. Mater. Lett. 2008, 62, 1630–1633. [Google Scholar] [CrossRef]
- Liu, D.; Liu, Z.; Zou, J.; Li, L.; Sui, X.; Wang, B.; Yang, N.; Wang, B. Synthesis and characterization of a hydroxyapatite-sodium alginate-chitosan scaffold for bone regeneration. Front. Mater. 2021, 8, 69. [Google Scholar] [CrossRef]
- Bolshakov, I.N.; Gorbunov, N.S.; Shamova, E.S.; Eremeev, A.V.; Sizykh, A.G.; Surkov, E.V.; Nasibov, S.M.; Maly, V.P.; Setkov, N.A. Wound coating based on collagen-chitosan. complex. Patent RF 2254145, 20 June 2005. [Google Scholar]
- Censi, R.; Di Martino, P.; Vermonden, T.; Hennink, W.E. Hydrogels for protein delivery in tissue engineering. J. Control Release 2012, 61, 680–692. [Google Scholar] [CrossRef] [PubMed]
- Jeong, C.H.; Kim, J.; Kim, H.S.; Lim, S.Y.; Han, D.; Huser, A.J.; Lee, S.B.; Gim, Y.; Ji, J.H.; Kim, D.; et al. Acceleration of bone formation by octacalcium phosphate composite in a rat tibia critical-sized defect. J. Orthop. Transl. 2022, 37, 100–112. [Google Scholar] [CrossRef]
- Draget, K.I.; Skjfik, G.B.; Smidsrod, O. Alginic acid gels: The effect of alginate chemical composition and molecular weight. Carbohydr. Polym. 1994, 25, 31–38. [Google Scholar] [CrossRef]
- Filardo, G.; Perdisa, F.; Gelinsky, M.; Despang, F.; Fini, M.; Marcacci, M.; Parrilli, A.P.; Roffi, A.; Salamanna, F.; Sartori, M. Novel alginate biphasic scaffold for osteochondral regeneration: An in vivo evaluation in rabbit and sheep models. J. Mater. Sci. Mater. Med. 2018, 29, 74. [Google Scholar] [CrossRef]
- Torres, A.L.; Gaspar, V.M.; Serra, I.R.; Diogo, G.S.; Fradique, R.; Silva, A.P.; Correia, I.J. Bioactive polymeric–ceramic hybrid 3D scaffold for application in bone tissue regeneration. Mater. Sci. Eng. C. 2013, 33, 4460–4469. [Google Scholar] [CrossRef]
- Mahmoud, E.; Sayed, M.; El-Kady, A.M.; Elsayed, H.; Naga, S. In vitro and in vivo study of naturally derived alginate/hydroxyapatite bio composite scaffolds. Int. J. Biol. Macromol. 2020, 165, 1346–1360. [Google Scholar] [CrossRef]
- Ocando, C.; Dinescu, S.; Samoila, I.; Ghitulica, C.D.; Cucuruz, A.; Costache, M.; Averous, L. Fabrication and properties of alginate-hydroxyapatite biocomposites as efficient biomaterials for bone regeneration. Eur. Polym. J. 2021, 151, 110444. [Google Scholar] [CrossRef]
- Kurobane, T.; Shiwaku, Y.; Anada, T.; Hamai, R.; Tsuchiya, K.; Baba, K.; Iikubo, M.; Takahashi, T.; Suzuki, O. Angiogenesis involvement by octacalcium phosphate-gelatin composite-driven bone regeneration in rat calvaria critical-sized defect. Acta Biomater. 2019, 88, 514–526. [Google Scholar] [CrossRef] [PubMed]
- Kargozar, S.; Baino, F.; Hamzehlou, S.; Hill, R.G.; Mozafari, M. Bioactive glasses: Sprouting angiogenesis in tissue engineering. Trends Biotechnol. 2018, 36, 430–444. [Google Scholar] [CrossRef] [PubMed]
- Saito, K.; Anada, T.; Shiwaku, Y.; Chiba, S.; Miyatake, N.; Suzuki, K.; Tsuchiya, K.; Suzuki, O. Dose-dependent enhancement of oc-tacalcium phosphate biodegradation with a gelatin matrix during bone regeneration in a rabbit tibial defect model. RSC Adv. 2016, 6, 64165–64174. [Google Scholar] [CrossRef]
- Wang, P.W.; Liu, J.L.; Zhang, T. In vitro biocompatibility of electrospun chitosan/collagen scaffold. J. Nanomater. 2013, 2013, 958172. [Google Scholar] [CrossRef]
- Tumshevits, O.N.; Bolshakov, I.N.; Belousova, Y.B.; Zykova, L.D.; Tumshevits, V.O. Method for Treatment of Periodontitis with Insulin-Dependent Diabetes Mellitus with “HAG-BOL”. Drugs. Patent RF No 2309748, 1 October 2006. [Google Scholar]
- Kamakura, S.; Nakajo, S.; Suzuki, O.; Sasano, Y. New scaffold for recombinant human bonemorphogenetic protein-2. J. Biomed. Mater. Res. A 2004, 71, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Suzuki, O.; Matsui, K.; Tanuma, Y.; Takahashi, T.; Kamakura, S. Octacalcium phosphate collagen composite facilitates bone regeneration of large mandibular bone defect in humans. J. Tissue Eng. Reg. Med. 2017, 11, 1641–1647. [Google Scholar] [CrossRef]
- Vojtová, L.; Pavliňáková, V.; Muchová, J.; Kacvinská, K.; Bortníková, J.; Knoz, M.; Lipový, B.; Faldyna, M.; Göpfert, E.; Holoubek, J.; et al. Healing and angiogenic properties of collagen/chitosan scaffolds enriched with hyperstable FGF2-STAB® protein: In vitro, ex novo and in vivo comprehensive evaluation. Biomedicines 2021, 9, 590. [Google Scholar] [CrossRef]
- Chan, B.P.; Leong, K.W. Scaffolding in tissue engineering: General approaches and tissue-specific considerations. Eur. Spine J. 2008, 17, 467–479. [Google Scholar] [CrossRef]
- Dong, C.; Lv, Y. Application of collagen scaffold in tissue engineering: Recent advances and new perspectives. Polymers 2016, 8, 42. [Google Scholar] [CrossRef]
- O’Brien, F.J. Biomaterials and scaffolds for tissue engineering. Mater. Today 2011, 14, 88–95. [Google Scholar] [CrossRef]
- Vaidehi, A.; Masters, P.K.S. Engineered Collagen Matrices. Bioengineering 2020, 7, 163. [Google Scholar]
- Melly, L.; Banfi, A. Fibrin-based factor delivery for therapeutic angiogenesis: Friend or foe? Cell Tissue Res. 2022, 387, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Li, M. Application of collagen composite scaffold in vascular tissue engineering. Zhongguo Xiufu Chongjian Waike Zazhi 2011, 25, 859–862. [Google Scholar] [PubMed]
- Tong, C.; Hao, H.; Xia, L.; Liu, J.; Ti, D.; Dong, L.; Hou, Q.; Song, H.; Liu, H.; Zhao, Y.; et al. Hypoxia pretreatment of bone marrow-derived mesenchymal stem cells seeded in a collagen-chitosan sponge scaffold promotes skin wound healing in diabetic rats with hind limb ischemia. Wound Repair Regen. 2016, 24, 45–56. [Google Scholar] [CrossRef]
- Kaczmarek, B.; Sionkowska, A. Chitosan/collagen blends with inorganic and organic additive. A review. Adv. Polym. Technol. 2018, 37, 2367–2376. [Google Scholar] [CrossRef]
- Liu, H.; Wang, C.; Li, C.; Qin, Y.; Wang, Z.; Yang, F.; Li, Z.; Wang, J. A functional chitosan-based hydrogel as a wound dressing and drug delivery system in the treatment of wound healing. RSC Adv. 2018, 8, 7533–7549. [Google Scholar] [CrossRef]
- Zwingenberger, B.; Vater, C.; Bell, R.; Bolte, J.; Mehnert, E.; Brunler, R.; Aibibu, D.; Zwingenberger, S. Treatment of Critical-Size Femoral Bone Defects with Chitosan Scaffolds Produced by a Novel Process from Textile Engineering. Biomedicines 2021, 9, 1015. [Google Scholar] [CrossRef]
- Casillas-Santana, M.A.; Slavin, Y.N.; Zhang, P.; Nino-Martinez, N.; Bach, H.; Martinez-Castañón, G.A. Osteoregeneration of Critical-Size Defects Using Hydroxy-apatite–Chitosan and Silver–Chitosan Nanocomposites. Nanomaterials 2023, 13, 321. [Google Scholar] [CrossRef]
- Kanczler, J.M.; Ginty, P.J.; White, L.; Clarke, N.M.P.; Howdle, S.M.; Shakesheff, K.M.; Oreffo, R.O.C. The effect of the delivery of vascular endothelial growth factor and bone morphogenic protein-2 to osteoprogenitor cell populations on bone formation. Biomaterials 2010, 31, 1242–1250. [Google Scholar] [CrossRef]
- Sheikh, Z.; Hamdan, N.; Ikeda, Y.; Grynpas, M.; Ganss, B.; Glogauer, M. Natural graft tissues and synthetic biomaterials for periodontal and alveolar bone reconstructive applications: A review. Biomater. Res. 2017, 21, 9. [Google Scholar] [CrossRef]
- Lovett, M.; Lee, K.; Edwards, A.; Kaplan, D.L. Vascularization strategies for tissue engineering. Tissue Eng. Part B Rev. 2009, 15, 353–370. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Yamamoto, T.; Tsuchiya, E.; Hongo, H.; Tsuboi, K.; Kudo, A.; Abe, M.; Yoshida, T.; Nagai, T.; Khadiza, N.; et al. Ultrastructural and biochemical aspects of matrix vesiclemediated mineralization. Jpn. Dent. Sci. Rev. 2017, 53, 34–45. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.M.; Gomez, A.J.; Palma, J.L.; Yap, W.T.; Shea, L.D. Heparin-chitosan nanoparticle functionalization of porous poly(ethylene glycol) hydrogels for localized lentivirus delivery of angiogenic factors. Biomaterials 2014, 35, 8687–8693. [Google Scholar] [CrossRef] [PubMed]
- Sivaraj, K.K.; Adams, R.H. Blood vessel formation and function in bone. Development 2016, 143, 2706–2715. [Google Scholar] [CrossRef]
- Li, H.; Chang, J. Stimulation of proangiogenesis by calcium silicate bioactive ceramic. Acta Biomater. 2013, 9, 5379–5389. [Google Scholar] [CrossRef]
- Gorustovich, A.A.; Roether, J.A.; Boccaccini, A.R. Effect of bioactive glasses on angiogenesis: A Review of in vitro and in vivo evidences. Tissue Eng. Part B Rev. 2010, 16, 199–207. [Google Scholar] [CrossRef]
- Kuttappan, S.; Mathew, D.; Jo, J.-I.; Tanaka, R.; Menon, D.; Ishimoto, T.; Nakano, T.; Nair, S.V.; Nair, M.B.; Tabata, Y. Dual release of growth factor from nanocomposite fibrous scaffold promotes vascularisation and bone regeneration in rat critical sized calvarial defect. Acta Biomater. 2018, 78, 36–47. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Annabi, N.; Nikkhah, M.; Bae, H.; Binan, L.; Park, S.; Kang, Y.; Yang, Y.; Khademhosseini, A. Vascularized bone tissue engineering: Approaches for potential improvement. Tissue Eng. Part B Rev. 2012, 18, 363–382. [Google Scholar] [CrossRef]
- Sheridan, M.H.; Shea, L.D.; Peters, M.C.; Mooney, D.J. Bioabsorbable polymer scaffolds for tissue engineering capable of sustained growth factor delivery. J. Control Release 2000, 64, 91–102. [Google Scholar] [CrossRef]
- Amaral, I.F.; Neiva, I.; da Silva, F.F.; Sousa, S.R.; Piloto, A.M.; Lopes, C.D.F.; Barbosa, M.A.; Kirkpatrick, C.J.; Pego, A.P. Endothelialization of chitosan porous conduits via immobilization of a recombinant fibronectin fragment (rhFNIII(7-10)). Acta Biomater. 2013, 9, 5643–5652. [Google Scholar] [CrossRef]
- Liu, S.; Hu, Y.; Zhang, J.; Bao, S.; Xian, L.; Dong, X.; Zheng, W.; Li, Y.; Gao, H.; Zhou, W. Bioactive and biocompatible macroporous scaffolds with tunable performances prepared based on 3D printing of the pre-crosslinked sodium alginate/hydroxyapatite hydrogel ink. Macromol. Mater. Eng. 2019, 304, 1800698. [Google Scholar] [CrossRef]
- Sancilio, S.; Marsich, E.; Schweikl, H.; Cataldi, A.; Gallorini, M. Redox control of IL-6-mediated dental pulp stem-cell differentiation on alginate/hydroxyapatite biocomposites for bone ingrowth. Nanomaterials 2019, 9, 1656. [Google Scholar] [CrossRef] [PubMed]
- Sumayya, A.S.; Muraleedhara Kurup, G. Marine macromolecules cross-linked hydrogel scaffolds as physiochemically and biologically favorable entities for tissue engineering applications. J. Biomater. Sci. Polym. Ed. 2017, 28, 807–825. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Liao, Y.; Li, D.; Li, D.; Wang, H.; Sun, X.; Chen, X.; Yan, H.; Lin, Q. Design and properties of alginate/gelatin/cellulose nanocrystals interpenetrating polymer network composite hydrogels based on in situ cross-linking. Res. Sq. 2022, preprint. [Google Scholar]
- Yeo, Y.J.; Jeon, D.W.; Kim, C.S.; Choi, S.H.; Cho, K.S.; Lee, Y.K.; Kim, C.-K. Effects of chitosan nonwoven membrane on periodontal healing of surgically created one-wall intrabony defects in beagle dogs. J. Biomed. Mater. Res. B Appl. Biomater. 2005, 72, 86–93. [Google Scholar] [CrossRef]
- Darnell, M.; Sun, J.; Mehta, M.; Johnson, C.; Arany, P.R.; Suo, Z.; Mooney, D.J. Performance and biocompatibility of extremely tough alginate/polyacrylamide hydrogels. Biomaterials 2013, 34, 8042–8048. [Google Scholar] [CrossRef]
- Shchipunov, Y.A.; Postnova, I. Formation of calcium alginate-based macroporous materials comprising chitosan and hydroxyapatite. Colloid J. 2011, 73, 565–574. [Google Scholar] [CrossRef]
- Sharma, C.; Dinda, A.K.; Potdar, P.D.; Chou, C.-F.; Mishra, N.C. Fabrication and characterization of novel nano-biocomposite scaffold of chitosan–gelatin–alginate–hydroxyapatite for bone tissue engineering. Mater. Sci. Eng. C 2016, 64, 416–427. [Google Scholar] [CrossRef]
- Park, J.S.; Choi, S.H.; Moon, I.S.; Cho, K.S.; Chai, J.K.; Kim, C.K. Eight-week histological analysis on the effect of chitosan on surgically created one-wall intrabony defects in beagle dogs. J. Clin. Periodontol. 2003, 30, 443–453. [Google Scholar] [CrossRef]
- Minardi, S.; Pandolfi, L.; Taraballi, F.; Wang, X.; De Rosa, E.; Mills, Z.D.; Liu, X.; Ferrari, M.; Tasciotti, E. Enhancing Vascularization through the Controlled Release of Platelet-Derived Growth Factor-BB. ACS Appl. Mater. Interfaces 2017, 9, 14566–14575. [Google Scholar] [CrossRef]
- Hurtado, A.; Aljabali, A.A.A.; Mishra, V.; Tambuwala, M.M.; Serrano-Aroca, Á. Alginate: Enhancement Strategies for Advanced Applications. Int. J. Mol. Sci. 2022, 23, 4486. [Google Scholar] [CrossRef] [PubMed]
- Ho, Y.C.; Mi, F.L.; Sung, H.W.; Kuo, P.L. Heparin-functionalized chitosan-alginate scaffolds for controlled release of growth factor. Int. J. Pharm. 2009, 376, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Lazarous, D.F.; Unger, E.F.; Epstein, S.E.; Stine, A.; Arevalo, J.L.; Chew, E.Y.; Quyyumi, A.A. Basic fibroblast growth factor in patients with intermittent claudication: Results of a phase I trial. J. Am. Coll. Cardiol. 2000, 36, 1239–1244. [Google Scholar] [CrossRef] [PubMed]


 ). Hematoxylin–eosin staining; (B)—control group, 2nd week of the experiment; the osteoblastic surface of the bone beams is significantly smaller in comparison with the experimental group (↑). Hematoxylin–eosin staining.
). Hematoxylin–eosin staining; (B)—control group, 2nd week of the experiment; the osteoblastic surface of the bone beams is significantly smaller in comparison with the experimental group (↑). Hematoxylin–eosin staining.
). Hematoxylin–eosin staining; (B)—control group, 2nd week of the experiment; the osteoblastic surface of the bone beams is significantly smaller in comparison with the experimental group (↑). Hematoxylin–eosin staining.
). Hematoxylin–eosin staining; (B)—control group, 2nd week of the experiment; the osteoblastic surface of the bone beams is significantly smaller in comparison with the experimental group (↑). Hematoxylin–eosin staining.
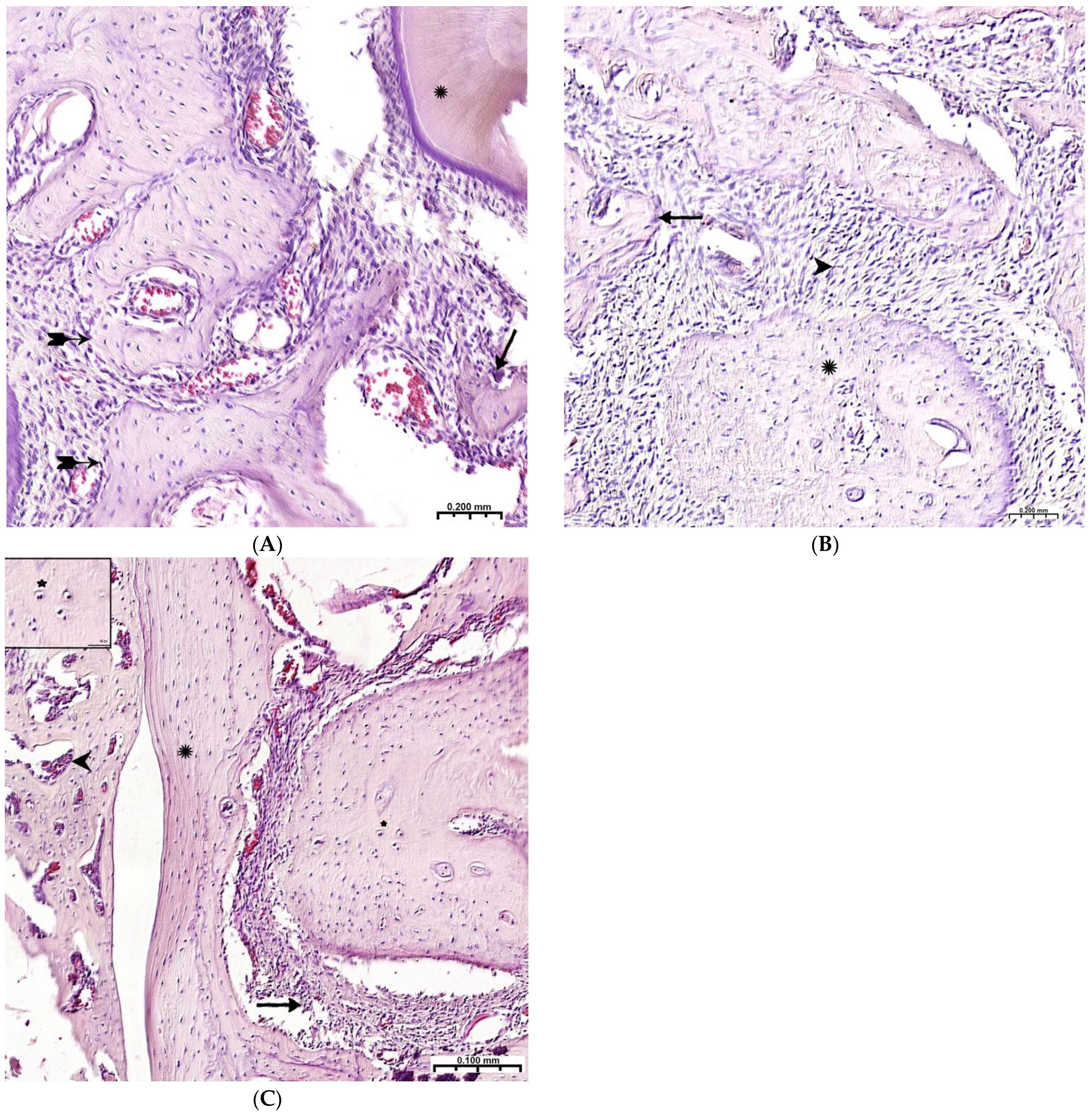
 ); bone trabeculae are covered with cell mass (^); (B)—CH–SA–HA group, 4 weeks. Visible bone beams with predominantly free surfaces (↑) and intertrabecular spaces (^); the adjacent peripheral area with the growth of maturing connective tissue (*). Hematoxylin–eosin staining.
); bone trabeculae are covered with cell mass (^); (B)—CH–SA–HA group, 4 weeks. Visible bone beams with predominantly free surfaces (↑) and intertrabecular spaces (^); the adjacent peripheral area with the growth of maturing connective tissue (*). Hematoxylin–eosin staining.
); bone trabeculae are covered with cell mass (^); (B)—CH–SA–HA group, 4 weeks. Visible bone beams with predominantly free surfaces (↑) and intertrabecular spaces (^); the adjacent peripheral area with the growth of maturing connective tissue (*). Hematoxylin–eosin staining.
); bone trabeculae are covered with cell mass (^); (B)—CH–SA–HA group, 4 weeks. Visible bone beams with predominantly free surfaces (↑) and intertrabecular spaces (^); the adjacent peripheral area with the growth of maturing connective tissue (*). Hematoxylin–eosin staining.



 ), adjacent peripheral area with proliferation of maturing connective tissue, active vascular endothelialization of bone regeneration, single osteoclasts (↑), organization of compact bone and periodontal ligament (*); (B)—8 weeks, large amount of spongy (^) and compact (*) bone tissue with cellular reaction on the bone beams (↑) and the formation of many micro-vessels; (C)—experimental group, 10 weeks, the mandibular defect is closed by a compact bone, in the border zone there is mature connective tissue (↑), in the adjacent bone tissue (*)—reactive bone marrow structures (^), formed osteons (*), many Haversian canals with a vascular component; Hematoxylin–eosin staining.
), adjacent peripheral area with proliferation of maturing connective tissue, active vascular endothelialization of bone regeneration, single osteoclasts (↑), organization of compact bone and periodontal ligament (*); (B)—8 weeks, large amount of spongy (^) and compact (*) bone tissue with cellular reaction on the bone beams (↑) and the formation of many micro-vessels; (C)—experimental group, 10 weeks, the mandibular defect is closed by a compact bone, in the border zone there is mature connective tissue (↑), in the adjacent bone tissue (*)—reactive bone marrow structures (^), formed osteons (*), many Haversian canals with a vascular component; Hematoxylin–eosin staining.
), adjacent peripheral area with proliferation of maturing connective tissue, active vascular endothelialization of bone regeneration, single osteoclasts (↑), organization of compact bone and periodontal ligament (*); (B)—8 weeks, large amount of spongy (^) and compact (*) bone tissue with cellular reaction on the bone beams (↑) and the formation of many micro-vessels; (C)—experimental group, 10 weeks, the mandibular defect is closed by a compact bone, in the border zone there is mature connective tissue (↑), in the adjacent bone tissue (*)—reactive bone marrow structures (^), formed osteons (*), many Haversian canals with a vascular component; Hematoxylin–eosin staining.
), adjacent peripheral area with proliferation of maturing connective tissue, active vascular endothelialization of bone regeneration, single osteoclasts (↑), organization of compact bone and periodontal ligament (*); (B)—8 weeks, large amount of spongy (^) and compact (*) bone tissue with cellular reaction on the bone beams (↑) and the formation of many micro-vessels; (C)—experimental group, 10 weeks, the mandibular defect is closed by a compact bone, in the border zone there is mature connective tissue (↑), in the adjacent bone tissue (*)—reactive bone marrow structures (^), formed osteons (*), many Haversian canals with a vascular component; Hematoxylin–eosin staining.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Area of Mandibular Defect | |||
|---|---|---|---|
| Experiment Period | Experience CH–SA–HA 1 | Control Healing under a Blood Clot 1 | Defect Periphery 1 Control + Experience |
| Numerical density of inflammatory infiltrate (unit/0.043 mm2) | |||
| 3 day 1 | 56.1[46.4;67.6] | 67.4[57.6;72.1] ** | 9.3[7.9;9.7] ** |
| 5 day 1 | 85.7[72.1;90.7] | 93.7[86.1;99.4] ** | 14.6[13.4;15.7] ** |
| 7 day 1 | 88.1[74.6;91.9] | 91.4[81.5;99.4] ** | 11.3[10.1;12.3] ** |
| Volumetric density of bone tissue (BV (%)) | |||
| 5 day 1 | 1.1[0.9;1.3] | 1.1[0.8;1.5] | 65.3[64.2;66.4] ** |
| 7 day 1 | 15.1[13.0;16.7] | 16.2[14.9;17.9] | 66.5[65.6;68.8] ** |
| Trabeculae thickness (mm) | |||
| 5 day 1 | 0.04[0.03;0.05] | 0.04[0.04;0.05] | 0.15[0.15;0.16] ** |
| 7 day 1 | 0.06[0.05;0.07] | 0.06[0.05;0.06] | 0.15[0.15;0.16] ** |
| Intertrabecular spaces (mm) | |||
| 5 day 1 | 0.61[0.60;0.63] | 0.61[0.59;0.63] | 0.21[0.21;0.23] ** |
| 7 day 1 | 0.43[0.42;0.45] | 0.43[0.43;0.45] | 0.20[0.19;0.21] ** |
| Osteoblastic surface (%) | |||
| 5 day 1 | 70.5[66.4;74.8] | 64.3[62.0;67.1] ** | 25.3[24.0;26.4] ** |
| 7 day 1 | 65.6[63.2;68.5] | 59.2[57.9;60.2] ** | 21.8[20.2;23.5] ** |
| Eroded bone surface (%) | |||
| 5 day 1 | 0.8[0.7;0.9] | 1.0[.0.9;1.1] ** | 12.0[11.3;13.3] ** |
| 7 day 1 | 1.5[1.4;1.8] | 1.9[1.6;2.1] ** | 7.9[7.7;8.0] ** |
| Area of Mandibular Defect | |||
|---|---|---|---|
| Experiment Period | Experience CH–SA–HA 1 | Control Healing under a Blood Clot 1 | Defect Periphery 1 Control + Experience |
| Numerical density of inflammatory infiltrate (unit/0.043 mm2) | |||
| 2 weeks 1 | 26.8[24.2;28.5] | 31.5[28.8;33.7] ** | 13.2[11.3;14.4] ** |
| 3 weeks 1 | 17.2[15.8;19.9] | 17.5[15.7;22.6] | 6.2[5.7;7.1] ** |
| Volumetric density of bone tissue (BV %) | |||
| 2 weeks 1 | 30.0[28.8;31.0] | 28.3[25.8;29.9] ** | 65.0[63.8;66.5] ** |
| 3 weeks 1 | 41.3[39.6;43.6] | 38.6[36.1;40.2] ** | 67.8[67.0;69.3] ** |
| 4 weeks 1 | 62.9[60.7;66.8] | 60.9[58.0;62.0] ** | 66.5[64.3;68.1] ** |
| Trabeculae thickness (TT mm) | |||
| 2 weeks 1 | 0.12[0.11;0.13] | 0.11[0.10;0.12] * | 0.16[0.16;0.17] ** |
| 3 weeks 1 | 0.13[0.11;0.14] | 0.12[0,12;0.13] * | 0.15[0.14;0.16] ** |
| 4 weeks 1 | 0.16[0.15;0.17] | 0.14[0.13;0.15] * | 0.16[0.15;0.17] ** |
| Inter-trabecular spaces (ITS mm) | |||
| 2 weeks 1 | 0.37[0.36;0.37] | 0.39[0.38;0.40] ** | 0.22[0.22;0.24] ** |
| 3 weeks 1 | 0.29[0.28;0.30] | 0.30[0.29;0.31] ** | 0.24[0.23;0.25] ** |
| 4 weeks 1 | 0.21[0.21;0.22] | 0.22[0.21;0.22] ** | 0.21[0.20;0.22] |
| Osteoblastic surface (OS %) | |||
| 2 weeks 1 | 58.9[57.0;60.2] | 49.9[49.5;50.4] ** | 13.1[12.4;13.7] ** |
| 3 weeks 1 | 50.8[49.0;53.1] | 42.0[39.6;43.9] ** | 9.1[8.4;9.8] ** |
| 4 weeks 1 | 38.9[37.1;40.1] | 36.0[34.7;37.0] ** | 7.2[6.3;7.8] ** |
| Eroded bone surface (ES %) | |||
| 2 weeks 1 | 3.5[3.3;3.6] | 3.9[3.7;3.9] ** | 6.1[5.5;6.9] ** |
| 3 weeks 1 | 5.9[5.6;6.1] | 6.4[6.1;6.6] ** | 2.9[2.7;3.0] ** |
| 4 weeks 1 | 9.9[9.7;10.0] | 10.7[10.5;11.1] ** | 1.3[1.2;1.4] ** |
| Area of Mandibular Defect | |||
|---|---|---|---|
| Experiment Period | Experience CH–SA–HA 1 | Control Healing under a Blood Clot 1 | Defect Periphery 1 Control + Experience |
| Volumetric density of bone tissue (BV %) | |||
| 6 weeks 1 | 67.5[65.4;68.6] | 62.6[60.0;64.2] ** | 68.7[67.2;69.8] * |
| 8 weeks | 67.1[63.2;69.1] | 65.2[63.4;69.2] | 67.0[65.4;68.5] |
| 10 weeks | 67.3[65.1;68.2] | 68.3[66.6;69.2] | 67.8[66.3;69.2] |
| Trabeculae thickness (TT mm) | |||
| 6 weeks | 0.16[0.15;0.17] | 0.16[0.15;0.16] | 0.15[0.14;0.17] |
| 8 weeks 1 | 0.16[0.15;0.16] | 0.15[0.14;0.16] * | 0.15[0.14;0.15] |
| 10 weeks | 0.16[0.16;0.17] | 0.16[0.15;0.17] | 0.16[0.16;0.17] |
| Inter-trabecular spaces (ITS mm) | |||
| 6 weeks 1 | 0.21[0.19;0.22] | 0.21[0.20;0.22] | 0.19[0.18;0.20] ** |
| 8 weeks 1 | 0.20[0.19;0.20] | 0.21[0.19;0.21] | 0.19[0.18;0.19] ** |
| 10 weeks 1 | 0.20[0.19;0.20] | 0.22[0.21;0.23] | 0.18[0.17;0.20] ** |
| Osteoblastic surface (OS %) | |||
| 6 weeks 1 | 20.2[19.0;21.5] | 16.4[14.9;18.0] ** | 4.0[2.8;4.7] ** |
| 8 weeks 1 | 8.7[8.1;9.9] | 8.4[7.1;9.6] | 1.5[1.3;1.8] * |
| 10 weeks 1 | 3.6[2.8;4.0] | 5.0[3.6;6.1] ** | 1.6[1.1;1.9] ** |
| Eroded bone surface (ES %) | |||
| 6 weeks 1 | 4.8[4.6;4.9] | 5.1[4.7;5.6] | 0.8[0.7;0.9] ** |
| 8 weeks 1 | 2.6[2.5;2.8] | 3.1[3.0;3.4] ** | 0.7[0.5;0.9] ** |
| 10 weeks 1 | 1.6[1.5;1.7] | 1.3[1.2;1.4] ** | 0.9[0.8;0.9] ** |
| Bone growth rate (% per day) | |||
| 1–28 days | 2.24[2.17;2.39] | 2.17[2.07;2.21] ** | |
| 6–14 days | 28.9 [26.3;30.4] | 27.2 [25.2;29.0] ** | |
| 15–28 days | 3.23[2.85;3.36] | 3.15[2.64;3.52] | |
| 29–70 days | 0.96[0.92;0.97] | 0.97[0.95;0.99] | |
| 1–70 days (total) | 0.94[0.82;1.25] | 0.96[0.85;1.15] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patlataya, N.N.; Bolshakov, I.N.; Levenets, A.A.; Medvedeva, N.N.; Khorzhevskii, V.A.; Cherkashina, M.A. Experimental Early Stimulation of Bone Tissue Neo-Formation for Critical Size Elimination Defects in the Maxillofacial Region. Polymers 2023, 15, 4232. https://doi.org/10.3390/polym15214232
Patlataya NN, Bolshakov IN, Levenets AA, Medvedeva NN, Khorzhevskii VA, Cherkashina MA. Experimental Early Stimulation of Bone Tissue Neo-Formation for Critical Size Elimination Defects in the Maxillofacial Region. Polymers. 2023; 15(21):4232. https://doi.org/10.3390/polym15214232
Chicago/Turabian StylePatlataya, Nadezhda Nicolaevna, Igor Nicolaevich Bolshakov, Anatoliy Alexandrovich Levenets, Nadezhda Nicolaevna Medvedeva, Vladimir Alexeevich Khorzhevskii, and Mariya Arturovna Cherkashina. 2023. "Experimental Early Stimulation of Bone Tissue Neo-Formation for Critical Size Elimination Defects in the Maxillofacial Region" Polymers 15, no. 21: 4232. https://doi.org/10.3390/polym15214232