

Investigations on the Fatigue Behavior of 3D-Printed and Thermoformed Polylactic Acid Wrist–Hand Orthoses

Abstract
:1. Introduction
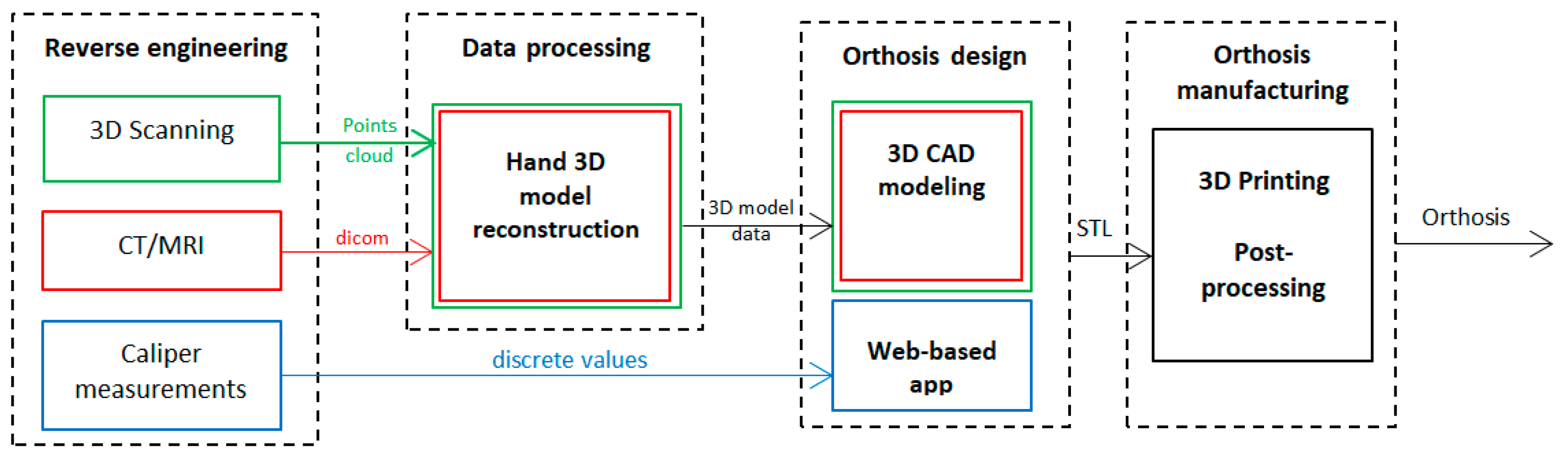
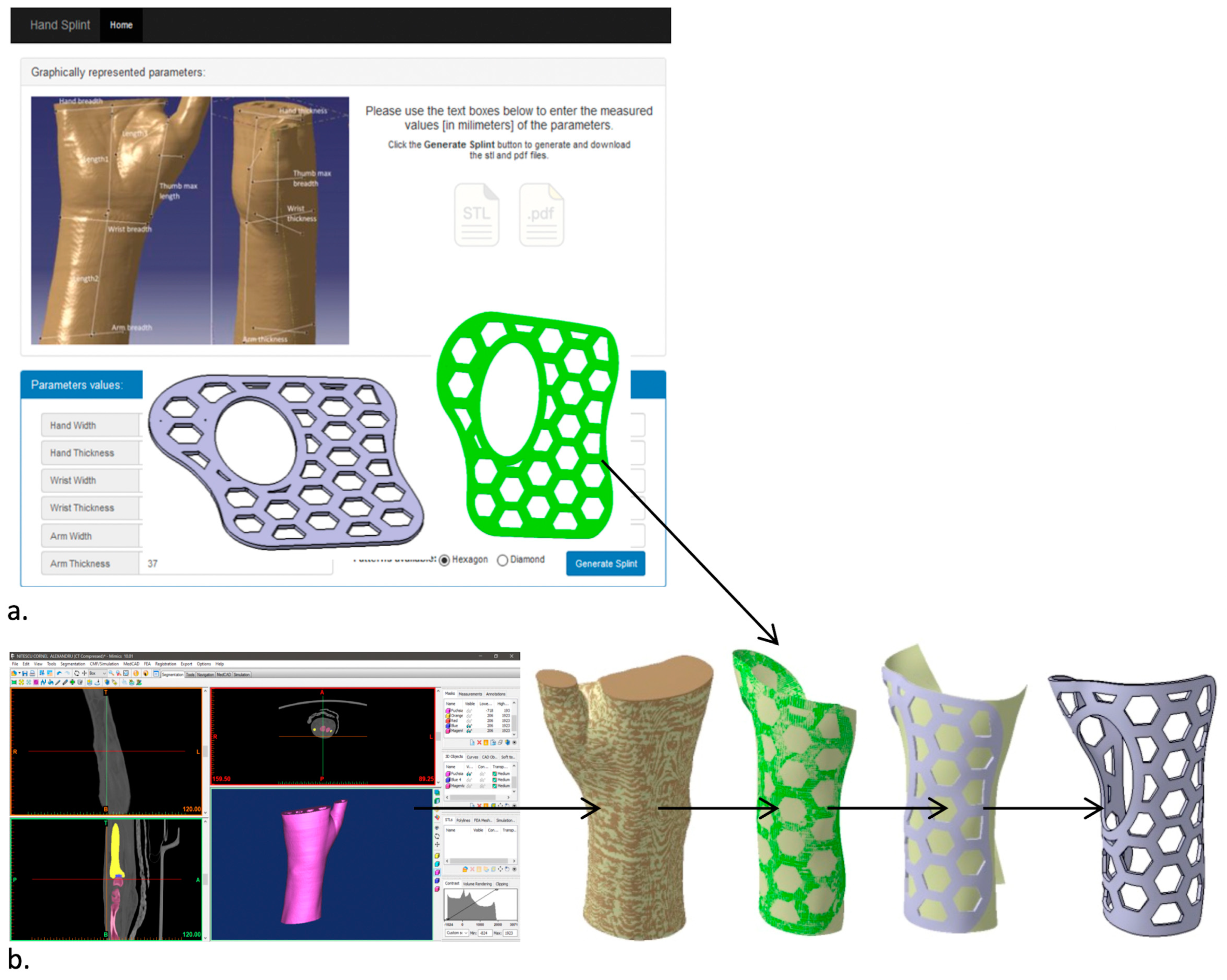
1.1. 3DP-WHOs’ Development Approaches
1.2. Literature Review
2. Materials and Methods
2.1. Wrist–Hand Orthoses and Forearm Dummy
2.2. 3D Printing
2.3. Experimental Tests
3. Results and Discussion
3.1. Literature Survey Outcomes
- Out of thirteen papers, four conducted experimental assessments on the mechanical behavior of 3D-printed wrist–hand orthoses (3DP-WHOs);
- No research has been conducted to compare the mechanical behavior of 3DP-WHOs manufactured in hand-shaped form with thermoformed 3D-printed orthoses;
- The most commonly used mechanical test for 3DP-WHOs is three-point bending, specifically for wrist flexion movement;
- Six papers focused on discussing WHO production through the MEX process, while the remaining papers discussed the utilization of SLS, SLA and Polyjet processes;
- For MEX orthoses, the following materials were used: PLA, ABS, PA12, HIPS;
- In two studies, multi-materials or hybrid manufacturing were used for producing the orthoses;
- For the purpose of reverse engineering the patient hand and designing the hand-shaped orthoses, eleven out of thirteen papers performed 3D laser scanning and associated data processing.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Acquisition Method | Manufacturing Process/Material | Mechanical Testing | FEA | Observations |
|---|---|---|---|---|---|
| WHO Design Method/Software | |||||
| Agudelo-Ardila, et al., 2019 [33] | 3D scanning, 3D handheld scanner | SLS process, ProX SLS 500 printer (3D Systems, Inc., Rock Hill, SC, USA, DuraForm ProX PA | No | Stress (load: 60N bending), thermal analysis (40 °C). | Comparison of manufacturing times for 3DP-WHOs vs. conventional WHOs. |
| Meshmixer, 2 parts WHO, Voronoi structure, 2.5 mm thickness | |||||
| Buonamici, et al., 2019 [18] | 3D scanning using a dedicated, in-house developed device | MEX process, Stratasys F370 (Stratasys Inc., Eden Prairie, MN, USA)—FDM printer, ABS M30 | No | FEA used for topology optimization for reducing weight by ventilation area. | Child WHO printing time 7h 21min; male adult 18h 6min; 52 min modeling time. |
| Customized semi-automatic design software based on Siemens NX 10; 2 parts WHO with zip ties; different designs for the ventilation holes (circular holes, Voronoi, topology optimization) | |||||
| Cazon, et al., 2017 [27] | 3D scanning, ZScanner 800 3D laser scanner | Polyjet process, Object Connex printer (Stratasys Inc., Eden Prairie, MN, USA)—multi-material WHO: VeroWhitePlus, TangoBlackPlus | Yes, dedicated support for WHO testing, mechanical tests for radial, ulnar, flexion and extension movements | FEA using Creo 3.0, 4 hand movements: radial, ulnar, flexion and extension, torques (Vanwearingen torques used as reference: 14.8 Nm, 8.4 Nm, 11.4 Nm, and respectively 9.9 Nm) and loads on x and z directions. | Mechanical tests showed displacements of 3.46 mm, 0.97 mm, 3.53 mm, and 2.51 mm for flexors, extensors, radial deviators and ulnar deviators. In ulnar direction, 3DP-WHO had a greater displacement, as resulted in FEA. 3DP-WHO proved suitable for everyday use. |
| Geomagic Studio 2013 | |||||
| Chen, C.D. et al., 2019 [15] | 3D scanning, Creaform Go!Scan50 scanner | MEX process, PLA | No | ANSYS, 3 parameters with 2 design values (WHO thickness, ventilation holes diameter, holes center distance); -flexion 30 N; extension 25 N; radial deviation 30 N; ulnar deviation 30 N -impact with 40 mm diameter steel ball of 0.3768 kg. | Material properties used in FEA were experimentally determined on specimens–ASTM D638, ISO 180. |
| 2 parts WHO tied with Velcro strips, designed using in-house solutions | |||||
| Chen, Y, et al., 2020 [28] | CT, Mimics 10.01 for forearm reconstruction | SLS process, EOS P395 (EOS GmbH, Krailling, Germany), PA2200 | No | ANSYS Workbench 18; 6 loading conditions including anterior to posterior (AP), posterior to anterior (PA), medial to lateral (ML), lateral to medial (LM), inward (IR), and outward OR to calculate the displacement and stress; 400 N compression load on the palm along AP, PA, ML, LM; 1 Nm rotation moment toward the IR and OR of the palm, applied to the top end side of cast. | FE model for bone, soft tissue and cast. Immobilization using 3DP-WHO was effective. A total of 60 patients, 20 used 3DP-WHOs, patients satisfaction assessment. Long manufacturing times, not suitable for emergency situations. |
| Solidworks 2015; 2 parts WHO | |||||
| Gorski, et al., 2020 [26] | 3D scanning, David SLS-3 optical scanner | MEX process, Raise 3D Pro machine (Raise 3D Technologies, Nantong, China); ABS, PLA; PA12, HIPS; different infills, layer thicknesses; vertical and horizontal build orientation | Yes, three-point bending using a TPU phantom of the forearm | No | Different assessment criteria: manufacturing time and cost, strength dependence on process parameters and material, the patient wore the 3DP-WHOs for 15 min for yes/no comfort feedback. |
| In-house dedicated design app (AutoMedPrint), 2 parts WHOs with snap fit connection, 4 mm thickness | |||||
| Hoogervorst, et al., 2019 [25] | 3D scanning, 3D Structure Sensor infrared scanner | MJF process, HP Multi Jet Fusion Printer (HP Inc., Palo Alto, CA, USA), PA12 | Yes, using a cadaver forearm; -flexion and extension of digits (1000 loading cycles (20–100 N tensile force), -pronation and supination of the hand (1000 cycles of torque (−0.5 to 0.5 Nm)), -three-point bending (1000 cycles (50–500 N)) | No | Cadaver biomechanical study for assessing the stabilizing properties of 3DP-WHOs in comparison with traditional fiberglass cast. Only three-point bending results were statistically different, but with a very small value of the absolute motion: 0.44 (±0.48)mm. |
| Open lattice design | |||||
| Kim & Jeong, 2015 [29] | 3D scanning | Hybrid manufacturing PolyJet, Objet500 Connex (Stratasys Inc., Eden Prairie, MN, USA), ABS, (inner frame, 2 part) and injection molding (outer cover, 2 parts, PC) | No | ANSYS 13, FEA for determining the thickness of WHO outer cover subjected to 200 N impact force | Manufacturing time and cost reduction by customizing just the inner frame and its connection bumps, while the outer frame is available on sizes |
| 3D CAD software for inner frame, outer frame designed based on population forearm measurements data | |||||
| Li & Tanaka, 2018 [31] | 3D scanning, Sense handheld 3D scanner | MEX process, Qidi Tech 1 3D printer (Qidi Tech, Ruian, China), ABS | No | FEA using Fusion 360 software; 30 N loads on the distal edge of the splint and lattice-structure area along three directions for simulating possible hits and stresses. | 3DP-WHO tested on 10 healthy subjects, no significant discomfort reported (3 reports of itching) |
| Semi-automated design using in-house app based on Rhinoceros 5 and Grasshopper 3D; 2–3 parts WHO connected with M3 screws, lattice structure | |||||
| Lin, et al., 2016 [32] | 3D scanning, Artec Eva and Artec Space Spider 3D scanners | SLA process, RS6000 3D printer (UnionTech, Beijing, China), PP | No | FEA using ANSYS for strength assessment, 3MPa impact pressure applied on the ventilation holes zones. | - |
| In-house modeling app for semi-automating the design process, 2 parts WHO, 2 mm thickness | |||||
| Lukaszewski et al., 2020 [34] | 3D scanning | MEX process, FlashForge Creator Pro (Zhejiang Flashforge 3D Technology Co., Ltd., Jinhua, China); ABS; 5 types of samples in different build orientations, 15% infill density, linear pattern, 2 shells | Yes, three-point bending parts for: specimen, part of WHO, part of WHO with ventilation holes, full WHO | FEA using ABAQUS for calculating WHO modulus of elasticity, 100 N loads in the middle of the WHO placed in a horizontal position. | The WHO parts with ventilation holes built in horizontal plane have higher stiffness than those built vertically. |
| WHO of 4mm thickness | |||||
| Modi, et al., 2020 [30] | 3D scanning, HandySCAN 3D laser scanner | SLS process, EOSINT P395 (EOS GmbH, Krailling, Germany), PA 2200 | No | FEA using Fusion 360; 100 N on the forearm area near proximal end of splint (as in impact), 30 N loads at the distal end of the splint near fingers as in accidental fingers bending. | The mechanical properties used in FEA were experimentally determined using specimens. Long development process (19 h). |
| Design process using Meshlab, GeoMagic Studio and CATIA V5 | |||||
| Sorimpuk, et al., 2022 [20] | Average dimensions of the forearms and hand circumference of Malaysian adults applied to a hand model from GrabCAD | MEX process, PLA (Ultimaker BV, Geldermalsen, NL) | No | FEA using Inventor 2017; 400 N load in X and Z directions of the cast, and 1 Nm bending moment along the Y direction of the cast. | FEA was performed on the digitally wrapped model of the 3DP-WHO. Results were compared with plaster traditional casts and SLS manufactured cast [28]. Reported printing time 3h 15 min. No process parameters details. No comparison with real 3DP-WHO. |
| Flat-designed WHO with different ventilation pockets and specific adaptive pattern for the wrist joint curvature |
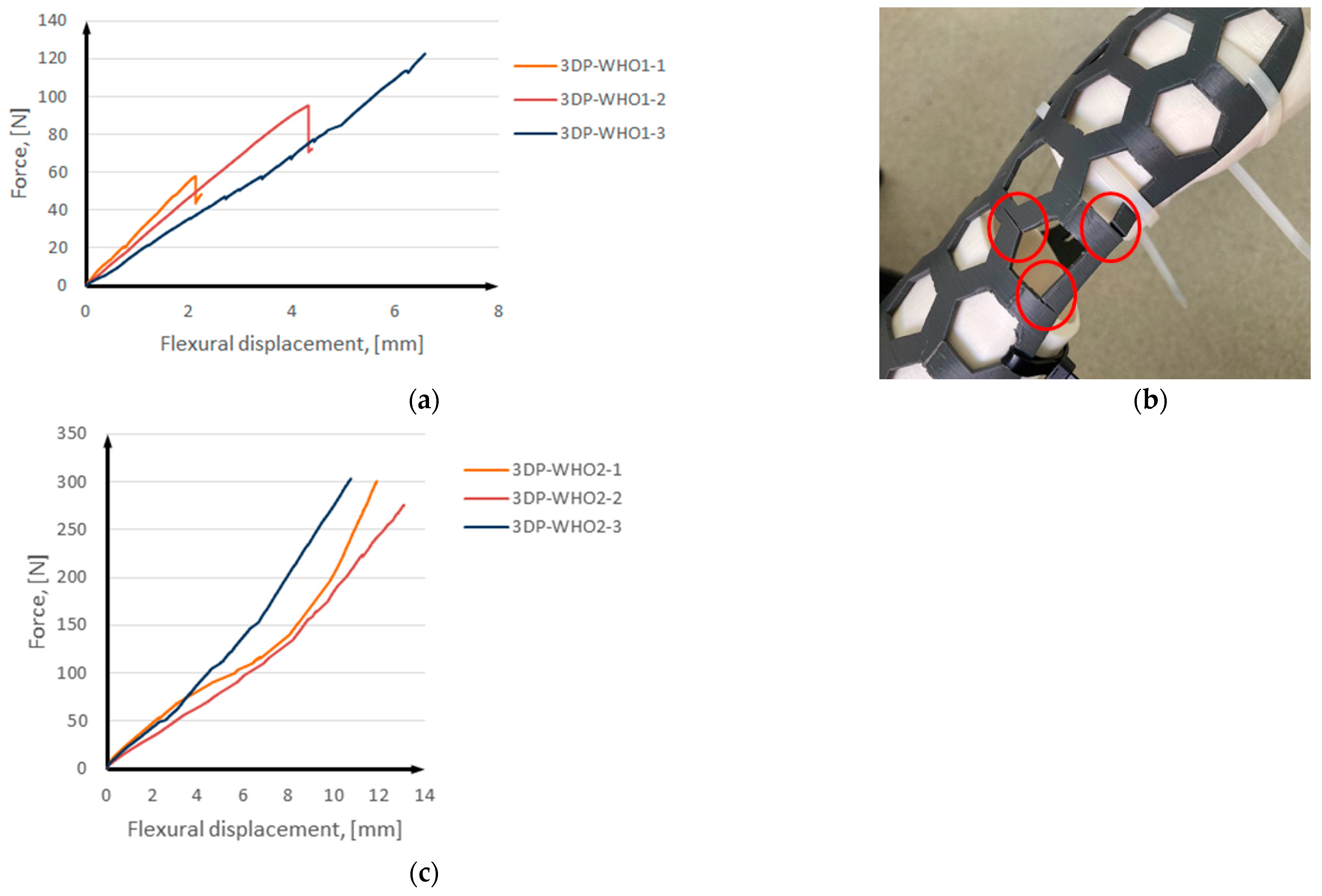
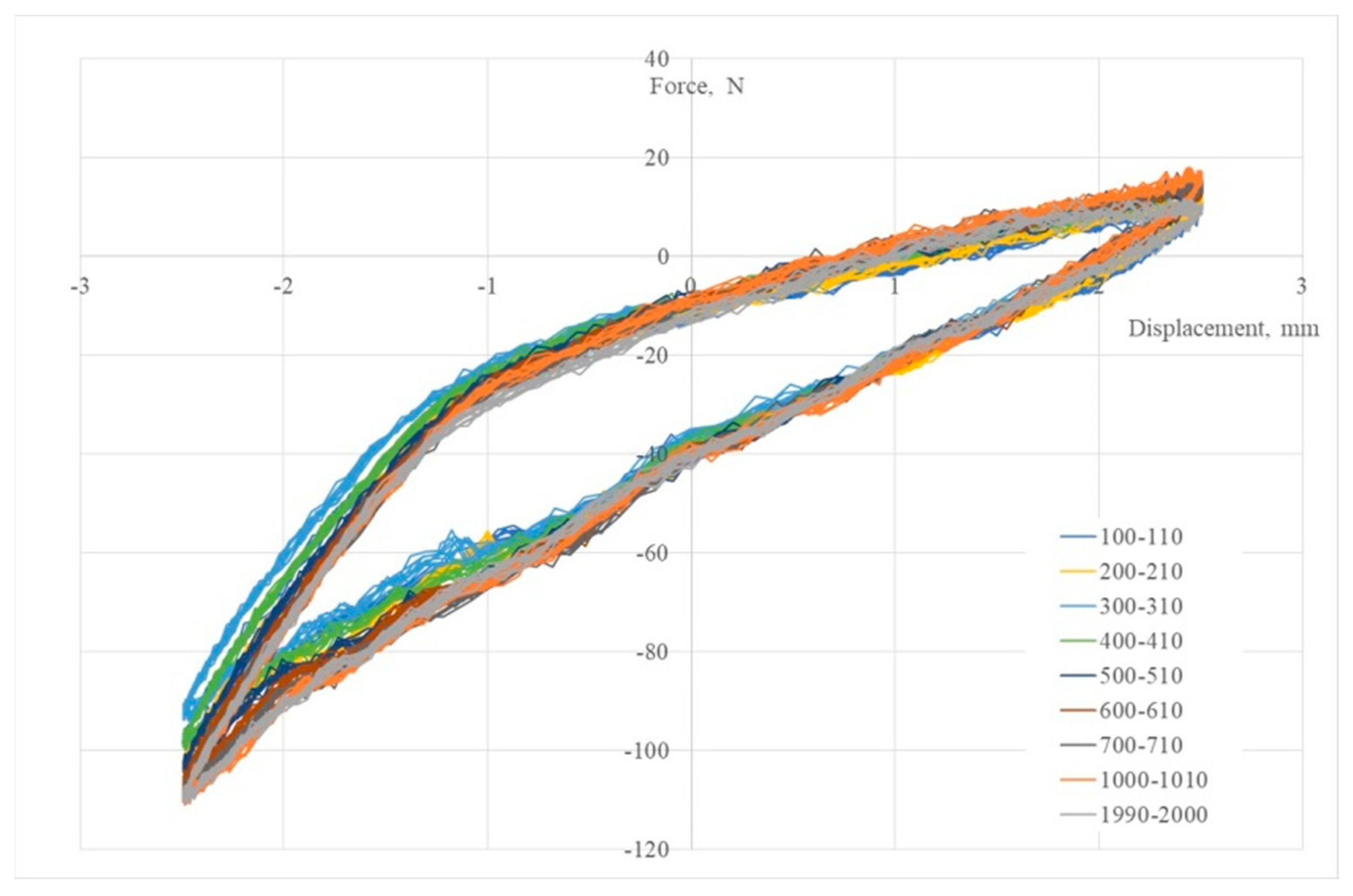
3.2. Results of Mechanical Tests
3.3. Discussion on 3D-Printed PLA Orthoses’ Thermoforming
4. Conclusions and Further Work
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Li, C.; Pisignano, D.; Zhao, Y.; Xue, J. Advances in Medical Applications of Additive Manufacturing. Engineering 2020, 6, 1222–1231. [Google Scholar] [CrossRef]
- Aimar, A.; Palermo, A.; Innocenti, B. The Role of 3D Printing in Medical Applications: A State of the Art. J. Healthc. Eng. 2019, 2019, 5340616. [Google Scholar] [CrossRef] [Green Version]
- Javaid, M.; Haleem, A. Additive manufacturing applications in medical cases: A literature based review. Alex. J. Med. 2018, 54, 411–422. [Google Scholar] [CrossRef] [Green Version]
- Shree, M.V.; Dhinakaran, V.; Rajkumar, V.; Ram, P.B.; Vijayakumar, M.; Sathish, T. Effect of 3D printing on supply chain management. Mater. Today Proc. 2020, 21, 958–963. [Google Scholar] [CrossRef]
- Daoud, G.E.; Pezzutti, D.L.; Dolatowski, C.J.; Carrau, R.L.; Pancake, M.; Herderick, E.; VanKoevering, K.K. Establishing a point-of-care additive manufacturing workflow for clinical use. J. Mater. Res. 2021, 26, 3761–3780. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Schofield, K.A. Utilization of 3D printed orthoses for musculoskeletal conditions of the upper extremity: A systematic review. J. Hand Ther. 2021, 36, 166–178. [Google Scholar] [CrossRef]
- Skibicki, H.E.; Katt, B.M.; Lutsky, K.; Wang, M.L.; McEntee, R.; Vaccaro, A.R.; Beredjiklian, P.; Rivlin, M. Three Dimensionally Printed Versus Conventional Casts in Pediatric Wrist Fractures. Cureus 2021, 13, e19090. [Google Scholar] [CrossRef]
- Guida, P.; Casaburi, A.; Busiello, T.; Lamberti, D.; Sorrentino, A.; Iuppariello, L.; D’albore, M.; Colella, F.; Clemente, F. An alternative to plaster cast treatment in a pediatric trauma center using the CAD/CAM technology to manufacture customized three-dimensional-printed orthoses in a totally hospital context: A feasibility study. J. Pediatr. Orthop. B 2019, 28, 248–255. [Google Scholar] [CrossRef]
- Kim, S.J.; Kim, S.J.; Cha, Y.H.; Lee, K.H.; Kwon, J.-Y. Effect of personalized wrist orthosis for wrist pain with three-dimensional scanning and printing technique. Prosthetics Orthot. Int. 2018, 42, 636–643. [Google Scholar] [CrossRef]
- Oud, T.A.M.; Lazzari, E.; Gijsbers, H.J.H.; Gobbo, M.; Nollet, F.; Brehm, M.A. Effectiveness of 3D-printed orthoses for traumatic and chronic hand conditions: A scoping review. PLoS ONE 2021, 16, e0260271. [Google Scholar] [CrossRef]
- Graham, J.; Wang, M.; Frizzell, K.; Watkins, C.; Beredjiklian, P.; Rivlin, M. Conventional vs 3-Dimensional Printed Cast Wear Comfort. Hand 2020, 15, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Waldburger, L.; Schaller, R.; Furthmüller, C.; Schrepfer, L.; Schaefer, D.J.; Kaempfen, A. 3D-Printed Hand Splints versus Thermoplastic Splints: A Randomized Controlled Pilot Feasibility Trial. Int. J. Bioprint. 2021, 8, 474. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.; Paterson, A.M.J.; Bibb, R.J. A Review of Wrist Splint Designs for Additive Manufacture. In Proceedings of the 2015 14th Rapid Design, Prototyping and Manufacture conference (RDPM 14), Loughborough, UK, 15–16 December 2015. [Google Scholar]
- Oud, T.; Kerkum, Y.; Groot, P.; Gijsbers, H.; Nollet, F.; Brehm, M. Production time and user satisfaction of 3-dimensional printed orthoses for chronic hand conditions compared with conventional orthoses: A prospective case series. J. Rehabil. Med. Clin. Commun. 2021, 4, 1000048. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-D.; Chen, C.-H.; Lin, C.-L.; Lin, C.-K.; Wang, C.-T.; Lin, R.-M.; Fang, J.-J. Developments, mechanical property measurements and strength evaluations of the wrist braces for the wrist fracture patients. J. Mech. Med. Biol. 2019, 19, 1940021. [Google Scholar] [CrossRef]
- Keller, M.; Guebeli, A.; Thieringer, F.; Honigmann, P. In-hospital professional production of patient-specific 3D-printed devices for hand and wrist rehabilitation. Hand Surg. Rehabil. 2021, 40, 126–133. [Google Scholar] [CrossRef]
- Formisano, M.; Iuppariello, L.; Casaburi, A.; Guida, P.; Clemente, F. An industrial oriented workflow for 3D printed, patient specific orthopedic cast. SN Appl. Sci. 2021, 3, 830. [Google Scholar] [CrossRef]
- Buonamici, F.; Furferi, R.; Governi, L.; Lazzeri, S.; McGreevy, K.S.; Servi, M.; Talanti, E.; Uccheddu, F.; Volpe, Y. A practical methodology for computer-aided design of custom 3D printable casts for wrist fractures. Vis. Comput. 2020, 36, 375–390. [Google Scholar] [CrossRef]
- Portnoy, S.; Barmin, N.; Elimelech, M.; Assaly, B.; Oren, S.; Shanan, R.; Levanon, Y. Automated 3D-printed finger orthosis versus manual orthosis preparation by occupational therapy students: Preparation time, product weight, and user satisfaction. J. Hand Ther. 2020, 33, 174–179. [Google Scholar] [CrossRef]
- Sorimpuk, N.P.; Choong, W.H.; Chua, B.L. Design of thermoformable three dimensional-printed PLA cast for fractured wrist. IOP Conf. Ser. Mater. Sci. Eng. 2022, 1217, 012002. [Google Scholar] [CrossRef]
- Popescu, D.; Zapciu, A.; Tarba, C.; Laptoiu, D. Fast production of customized three-dimensional-printed hand splints. Rapid Prototyp. J. 2020, 26, 134–144. [Google Scholar] [CrossRef]
- Baronio, G.; Harran, S.; Signoroni, A. A Critical Analysis of a Hand Orthosis Reverse Engineering and 3D Printing Process. Appl. Bionics Biomech. 2016, 2016, 8347478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winter, D.A. (Ed.) Chapter 9: Kinesiological Electromyography. In Biomechanics and Motor Control of Human Movement, 3rd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2005. [Google Scholar]
- Breger-Lee, D.E.; Buford, W.L. Properties of Thermoplastic Splinting Materials. J. Hand Ther. 1992, 5, 202–211. [Google Scholar] [CrossRef]
- Hoogervorst, P.; Knox, R.; Tanaka, K.; Working, Z.M.; El Naga, A.N.; Herfat, S.; Lee, N. A Biomechanical Comparison of Fiberglass Casts and 3-Dimensional–Printed, Open-Latticed, Ventilated Casts. Hand 2020, 5, 842–849. [Google Scholar] [CrossRef] [PubMed]
- Górski, F.; Wichniarek, R.; Kuczko, W.; Żukowska, M.; Lulkiewicz, M.; Zawadzki, P. Experimental Studies on 3D Printing of Automatically Designed Customized Wrist-Hand Orthoses. Materials 2020, 13, 4091. [Google Scholar] [CrossRef] [PubMed]
- Cazón, A.; Kelly, S.; Paterson, A.M.; Bibb, R.J.; Campbell, R.I. Analysis and comparison of wrist splint designs using the finite element method: Multi-material three-dimensional printing compared to typical existing practice with thermoplastics. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2017, 231, 881–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Lin, H.; Yu, Q.; Zhang, X.; Wang, D.; Shi, L.; Huang, W.; Zhong, S. Application of 3D-Printed Orthopedic Cast for the Treatment of Forearm Fractures: Finite Element Analysis and Comparative Clinical Assessment. BioMed Res. Int. 2020, 2020, 32775455. [Google Scholar] [CrossRef]
- Kim, H.; Jeong, S. Case study: Hybrid model for the customized wrist orthosis using 3D printing. J. Mech. Sci. Technol. 2015, 29, 5151–5156. [Google Scholar] [CrossRef]
- Modi, Y.K.; Khare, N. Patient-specific polyamide wrist splint using reverse engineering and selective laser sintering. Mater. Technol. 2020, 37, 71–78. [Google Scholar] [CrossRef]
- Li, J.; Tanaka, H. Rapid customization system for 3D-printed splint using programmable modeling technique—A practical approach. 3D Print. Med. 2018, 4, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.; Shi, L.; Wang, D. A rapid and intelligent designing technique for patient-specific and 3D-printed orthopedic cast. 3D Print. Med. 2016, 2, 4. [Google Scholar] [CrossRef] [Green Version]
- Agudelo-Ardila, C.P.; Prada-Botía, G.C.; Rodrigues, G.P.H. Orthotic prototype for upper limb printed in 3D: A efficient solution. J. Phys. Conf. Ser. 2019, 1388, 012016. [Google Scholar] [CrossRef]
- Łukaszewski, K.; Wichniarek, R.; Górski, F. Determination of the Elasticity Modulus of Additively Manufactured Wrist Hand Orthoses. Materials 2020, 13, 4379. [Google Scholar] [CrossRef] [PubMed]
- Galati, M.; Minetola, P.; Marchiandi, G.; Atzeni, E.; Calignano, F.; Salmi, A.; Iuliano, L. A methodology for evaluating the aesthetic quality of 3D printed parts. Procedia CIRP 2019, 79, 95–100. [Google Scholar] [CrossRef]
- Salaffi, F.; Carotti, M.; Farah, S.; Ceccarelli, L.; Di Carlo, M. Handgrip Strength Features in Rheumatoid Arthritis Patients Assessed Using an Innovative Cylindrical-Shaped Device: Relationships With Demographic, Anthropometric and Clinical Variables. J. Med. Syst. 2021, 45, 100. [Google Scholar] [CrossRef]
- Ezeh, O.; Susmel, L. Fatigue strength of additively manufactured polylactide (PLA): Effect of raster angle and non-zero mean stresses. Int. J. Fatigue 2019, 126, 319–326. [Google Scholar] [CrossRef]
- Jerez-Mesa, R.; Travieso-Rodriguez, J.; Llumà-Fuentes, J.; Gomez-Gras, G.; Puig, D. Fatigue lifespan study of PLA parts obtained by additive manufacturing. Procedia Manuf. 2017, 13, 872–879. [Google Scholar] [CrossRef] [Green Version]
- Mäntyjärvi, K.; Iso-Junno, T.; Mustakangas, A.; Jokelainen, T.; Keskitalo, M.; Järvenpää, A. Exploitation of forming of the 3D printed materials. AIP Conf. Proc. 2019, 2113, 150007. [Google Scholar] [CrossRef]
- Wang, G.; Yang, Y.; Guo, M.; Zhu, K.; Yan, Z.; Cui, Q.; Zhou, Z.; Ji, J.; Li, J.; Luo, D.; et al. ThermoFit: Thermoforming Smart Orthoses via Metamaterial Structures for Body-Fitting and Component-Adjusting. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2023, 7, 1–27. [Google Scholar] [CrossRef]
- Wei, H. Optimisation on Thermoforming of Biodegradable Poly (Lactic Acid) (PLA) by Numerical Modelling. Polymers 2021, 13, 654. [Google Scholar] [CrossRef]
- Milovanovic, S.; Pajnik, J.; Lukic, I. Tailoring of advanced poly(lactic acid)-based materials: A review. J. Appl. Polym. Sci. 2021, 139, 51839. [Google Scholar] [CrossRef]









| 3DP-WHO1 | 3DP-WHO2 | Process Parameters |
|---|---|---|
Hand-tailored form–build orientation | Flat form–build orientation | Printing temperature: 215 °C Bed temperature: 70 °C Infill pattern: grid 2 shells Top/bottom layers: 2 Infill density WHO1: 40% Infill density WHO2: 97% |
| Printing time: 7 h 8 min | Printing time: 2 h 39 min |
| Samples | Force at Break, [N] | Displacement at Break, [mm] |
|---|---|---|
| 3DP-WHO1 | 81.13 | 4.41 |
| 3DP-WHO2 | 292.9 | 11.89 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popescu, D.; Baciu, F.; Vlăsceanu, D.; Marinescu, R.; Lăptoiu, D. Investigations on the Fatigue Behavior of 3D-Printed and Thermoformed Polylactic Acid Wrist–Hand Orthoses. Polymers 2023, 15, 2737. https://doi.org/10.3390/polym15122737
Popescu D, Baciu F, Vlăsceanu D, Marinescu R, Lăptoiu D. Investigations on the Fatigue Behavior of 3D-Printed and Thermoformed Polylactic Acid Wrist–Hand Orthoses. Polymers. 2023; 15(12):2737. https://doi.org/10.3390/polym15122737
Chicago/Turabian StylePopescu, Diana, Florin Baciu, Daniel Vlăsceanu, Rodica Marinescu, and Dan Lăptoiu. 2023. "Investigations on the Fatigue Behavior of 3D-Printed and Thermoformed Polylactic Acid Wrist–Hand Orthoses" Polymers 15, no. 12: 2737. https://doi.org/10.3390/polym15122737