
3D Bioprinting of Hyaline Articular Cartilage: Biopolymers, Hydrogels, and Bioinks
 ,
,
Abstract
:
1. Hyaline Articular Cartilage Damages, Regeneration Process, and Current Treatment Approaches
- Superficial;
- Transitional;
- Deep;
- Calcified.
- Subchondral tunnelling;
- Microfracturing;
- Osteochondral autotransplantation;
- Allo-osteochondroplasty.
2. Regenerative Medicine and Tissue Engineering in the Treatment of Hyaline Articular Cartilage Injuries
- Stimulation of regeneration with bioactive factors accelerating cell reproduction, growth, and differentiation;
- Cell therapy using stem cells;
- Tissue engineering.
3. 3D Tissue Bioprinting
- Pre-bioprinting, or the “preparation” stage, includes computer modelling of the future 3D object; isolation and cultivation of cell cultures; and biomaterial adjustment.
- Bioprinting, or the “production” stage, involves the creation of a volume tissue-engineered construct in a 3D bioprinter by “layer-by-layer” deposition of biomaterials, auxiliary components, and living cells on a substrate.
- Post-bioprinting, or the “functionalization” stage, is necessary for the stabilization of the bioprinted construct and “maturation” of its cells; this stage is implemented in bioreactors, where basic structural and functional characteristics of a bioprinted construct such as mechanical strength, structural integrity, and others are formed.
- Equipment: 3D scanner (appropriate medical diagnostic equipment—MSCT, MRI, and 3D X-ray), personal computer (specialist workplace), 3D bioprinter, cell and tissue bioreactors, and equipment for input and output certification.
- 3D printing job preparation software, CAD software for product design, and special utilities for converting from the DICOM format (MSCT and MRI data storage format) to 3D printing data format (STL files).
- Cell culture, as well as biomaterials of a natural or synthetic origin (including their combinations), as the basis of the volume matrix (analogue of ECM), in which cells will be placed.
3.1. The Pre-Bioprinting Stage
3.1.1. Visualization and 3D Modelling
- Based on the data obtained by MRI or MSCT of the intervention area (recipient area).
- De novo, when a bioengineer uses 3D bioprinter software to create a model and set the conditions for the location of the final product in the body.
- Computer processing (transformation) of data from different sources (MSCT, MRI, 3D X-ray, CAD systems, or CAD-design) by special programs to create a digital model of the future 3D product; its location in the synthesis chamber, splitting into layers; and formation of support (if necessary).
- Consultation with medical personnel (surgeon and traumatologist) on the correctness of the digital model and its compatibility with the course, scope, and sequence of the planned operation. Biomaterial adjustment with the method and mode of the 3D bioprinting definition according to the tasks to be performed.
- 3D printing of a pre-product with usage of convenient and cheap material for visual, tactile, and volume–geometric diagnostics, as well as pre- and post-operative planning.
3.1.2. Preparation of Cell Culture
3.1.3. Adjustment of Biomaterial and Printing Technology
- With the formation of scaffolds;
- Without scaffold formation or scaffold-free;
- Hybrid.
3.1.4. Bioprinting with the Formation of Scaffolds
- Metals;
- Silica, including biosilicates;
- Hydroxyappatite and other calcium phosphates;
- Alumina;
- Polymer clays, including laponite;
- Nonresorbable synthetic biopolymers;
- Combinations of the aforementioned materials.
- Powder methods of 3D printing with biocompatible metals and alloys:
- Laser (E-beam) Powder Bed Fusion (L/E-PBF);
- Direct Energy Deposition (DED).
- 3D printing with liquid materials (photobiopolymers):
- Vat Photo Polymerization: Stereolithography (SLA, including two-photon) or Digital Light Processing (DLP);
- Ink Jet Printing (IJP).
- 3D printing with solid materials:
- Fused Deposition Modelling (FDM);
- Binder Jetting (BJ).
3.1.5. Scaffold-Free Bioprinting
- Biopolymer hydrogels without living cells or so-called biopaper;
- Cell-loaded (with spheroids) biopolymer hydrogels or so-called bioinks.
Biopolymer Hydrogels
- Irreversible or chemically cross-linked hydrogels are covalently “cross-linked” networks of biopolymers in which strong and more stable covalent bonds replace hydrogen bonds [161,174]. In such hydrogels, the equilibrium swelling state depends on the biopolymer–water interaction parameter and the density of covalent bonds [161,174,175].
- A method of ionic interaction in which ionic biopolymers are cross-linked by adding divalent or trivalent counterions, for example, sodium alginate with calcium chloride divalent [161].
- Method of hydrogel formation with hydrogen bonds. A hydrogel is obtained by lowering the pH of an aqueous solution of biopolymers carrying carboxyl groups. For example, sodium in carboxymethyl cellulose (CMC) is replaced with hydrogen in acid. A hydrogen-bonded network is formed by dispersing CMC in a 0.1 M hydrochloric acid solution [161,179,180].
- Freeze–thaw method. As an example, the formation of microcrystals in the biopolymer (polyvinyl alcohol and xanthan gels) structure due to a freeze–thaw [161,176,181,182]. Hydrogels formed by this method have sufficient mechanical strength and stability but are opaque in appearance and have a low ability to swell [161,176,181].
- Radiation cross-linking method. This method is quite common, does not require the addition of chemical agents, allows for combining modification with sterilization, and, at the same time, preserves the biocompatibility of the polymer. The method is premised on the releasing of free radicals in the polymer after exposure to an electromagnetic radiation source (gamma rays and X-rays) [161,183].
- The method of chemical cross-linking agents’ usage. Involves introducing new molecules between polymer chains to produce cross-linked chains, such as glutaric aldehyde, and epichlorohydrin [161].
- The method of monomer polymerization is based on a preformed biopolymer. Polymer chains are activated by the interaction of chemical reagents, whereby the growth of functional monomers leads to branching and further cross-linking of the hydrogel [161].
Bioinks
Quality Assessment Methods for Hydrogels, Bioinks, and Bioprinted Products
3.2. Bioprinting Stage
Bioprinters and the Bioprinting Process
- Sterile printing chamber with the option of a bioreactor for functionalization of the printed construct in the post-bioprinting stage;
- Laser sensor system for automatic calibration of printing elements;
- Interchangeable platforms (or worktables) and substrates for bioprinting;
- Camera for photo and video recording of the manufacturing process and its control.
- Pre-cross-link—processing the printed biomaterial in the cartridge;
- Post-cross-link—processing the printed biomaterial after it leaves the cartridge;
- In situ cross-linking is the processing of printed biomaterial in the nozzle area of the printhead.
- The usage of temporary (sacrificial) structures;
- Manufacturing of structures with internal reinforcement;
- Application of coordinated extrusion bioprinting;
- The usage of a modular assembly.
3.3. Post-Bioprinting Stage
Bioreactors In Vitro and In Vivo
4. Vectors for the Development of Tridimensional Bioprinting of Hyaline Articular Cartilage
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 3D | Three-dimensional |
| aFGF | Acidic fibroblast growth factor |
| bFGF | Basic fibroblast growth factor |
| BJ | Binder jetting |
| BMP-2, 3, 4, 6, 7 | Bone morphogenetic protein-2, 3, 4, 6, 7 |
| CAD | Computer-aided design (system) |
| CDS | Circular dichroism spectroscopy |
| CM | Confocal microscopy |
| CMC | Carboxymethylcellulose |
| dECM | Decellularized extracellular matrix |
| DED | Direct energy deposition |
| DICOM | Digital imaging and communications in medicine |
| DLP | Digital light processing |
| ECM | Extracellular matrix |
| FDM | Fused deposition modelling |
| FGF | Fibroblast growth factor |
| FS | Fluorescence spectroscopy |
| FTIR | Infrared spectroscopy with the Fourier transform |
| HAC | Hyaline articular cartilage |
| IGF I | Insulin-like growth factor I |
| IGF II | Insulin-like growth factor II |
| IJP | Ink jet printing |
| IUHP method | Isostatic ultrahigh pressure method |
| IUPAC | International Union of Pure and Applied Chemistry |
| L/E-PBF | Laser (E-beam) powder bed fusion |
| MRI | Magnetic resonance imaging |
| MSC | Mesenchymal stromal cells |
| MSCT | Multi-slice computed tomography |
| PCL | Polycaprolactone |
| PDGF | Platelet-derived growth factor |
| PEG | Polyethylene glycol |
| PLGA | Poly-lactic-co-glycolic acid |
| PRP | Platelet-rich plasma |
| PU | Polyurethane |
| PVA | Polyvinyl alcohol |
| SLA | Stereolithography |
| STL files | From stereolithography—a file format for storing three-dimensional models of objects for use in additive technologies. |
| TDB | Three-dimensional bioprinting |
| TGF-β | Transforming growth factor beta |
| VEGF | Vascular endothelial growth factor |
References
- Firner, S.; Zaucke, F.; Michael, J.; Dargel, J.; Schiwy-Bochat, K.H.; Heilig, J.; Rothschild, M.A.; Eysel, P.; Brüggemann, G.P.; Niehoff, A. Extracellular Distribution of Collagen II and Perifibrillar Adapter Proteins in Healthy and Osteoarthritic Human Knee Joint Cartilage. J. Histochem. Cytochem. 2017, 65, 593–606. [Google Scholar] [CrossRef] [PubMed]
- Kheir, E.; Shaw, D. Hyaline Articular Cartilage. Orthop. Trauma 2009, 23, 450–455. [Google Scholar] [CrossRef]
- Beddoes, C.M.; Whitehouse, M.R.; Briscoe, W.H.; Su, B. Hydrogels as a Replacement Material for Damaged Articular Hyaline Cartilage. Materials 2016, 9, 443. [Google Scholar] [CrossRef] [PubMed]
- Martel-Pelletier, J.; Barr, A.J.; Cicuttini, F.M.; Conaghan, P.G.; Cooper, C.; Goldring, M.B.; Goldring, S.R.; Jones, G.; Teichtahl, A.J.; Pelletier, J.P. Osteoarthritis. Nature Rev. Dis. Prim. 2016, 2, 16072. [Google Scholar] [CrossRef] [PubMed]
- Lories, R.J.; Luyten, F.P. The Bone-Cartilage Unit in Osteoarthritis. Nat. Rev. Rheumatol. 2011, 7, 43–49. [Google Scholar] [CrossRef]
- Madry, H.; van Dijk, C.N.; Mueller-Gerbl, M. The Basic Science of the Subchondral Bone. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 419–433. [Google Scholar] [CrossRef]
- Lepage, S.I.M.; Robson, N.; Gilmore, H.; Davis, O.; Hooper, A.; St John, S.; Kamesan, V.; Gelis, P.; Carvajal, D.; Hurtig, M.; et al. Beyond Cartilage Repair: The Role of the Osteochondral Unit in Joint Health and Disease. Tissue Eng. Part B Rev. 2019, 25, 114–125. [Google Scholar] [CrossRef]
- Armiento, A.R.; Alini, M.; Stoddart, M.J. Articular Fibrocartilage—Why Does Hyaline Cartilage Fail to Repair? Adv. Drug Deliv. Rev. 2019, 146, 289–305. [Google Scholar] [CrossRef]
- Karuppal, R. Current Concepts in the Articular Cartilage Repair and Regeneration. J. Orthop. 2017, 14, A1–A3. [Google Scholar] [CrossRef]
- Bergholt, M.S.; Serio, A.; Albro, M.B. Raman Spectroscopy: Guiding Light for the Extracellular Matrix. Front. Bioeng. Biotechnol. 2019, 7, 303. [Google Scholar] [CrossRef]
- Manou, D.; Caon, I.; Bouris, P.; Triantaphyllidou, I.E.; Giaroni, C.; Passi, A.; Karamanos, N.K.; Vigetti, D.; Theocharis, A.D. The Complex Interplay between Extracellular Matrix and Cells in Tissues. Methods Mol. Biol. 2019, 1952, 1–20. [Google Scholar] [CrossRef]
- Poole, C.A. Articular Cartilage Chondrons: Form, Function and Failure. J. Anat. 1997, 191, 1–13. [Google Scholar] [CrossRef]
- Kvist, A.J.; Nyström, A.; Hultenby, K.; Sasaki, T.; Talts, J.F.; Aspberg, A. The Major Basement Membrane Components Localize to the Chondrocyte Pericellular Matrix--a Cartilage Basement Membrane Equivalent? Matrix Biol. 2008, 27, 22–33. [Google Scholar] [CrossRef]
- Carballo, C.B.; Nakagawa, Y.; Sekiya, I.; Rodeo, S.A. Basic Science of Articular Cartilage. Clin. Sports Med. 2017, 36, 413–425. [Google Scholar] [CrossRef]
- Poole, A.R.; Kobayashi, M.; Yasuda, T.; Laverty, S.; Mwale, F.; Kojima, T.; Sakai, T.; Wahl, C.; El-Maadawy, S.; Webb, G.; et al. Type II Collagen Degradation and Its Regulation in Articular Cartilage in Osteoarthritis. Ann. Rheum. Dis. 2002, 61 (Suppl. 2), ii78–ii81. [Google Scholar] [CrossRef]
- Shoulders, M.D.; Raines, R.T. Collagen Structure and Stability. Annu. Rev. Biochem. 2009, 78, 929–958. [Google Scholar] [CrossRef]
- Sharma, U.; Carrique, L.; Vadon-Le Goff, S.; Mariano, N.; Georges, R.N.; Delolme, F.; Koivunen, P.; Myllyharju, J.; Moali, C.; Aghajari, N.; et al. Structural Basis of Homo- and Heterotrimerization of Collagen I. Nat. Commun. 2017, 8, 14671. [Google Scholar] [CrossRef]
- Stoilov, I.; Starcher, B.C.; Mecham, R.P.; Broekelmann, T.J. Measurement of Elastin, Collagen, and Total Protein Levels in Tissues. Methods Cell Biol. 2018, 143, 133–146. [Google Scholar] [CrossRef]
- Pfeiffer, E.; Vickers, S.M.; Frank, E.; Grodzinsky, A.J.; Spector, M. The Effects of Glycosaminoglycan Content on the Compressive Modulus of Cartilage Engineered in Type II Collagen Scaffolds. Osteoarthr. Cartil. 2008, 16, 1237–1244. [Google Scholar] [CrossRef]
- Deshmukh, A.S.; Murgia, M.; Nagaraj, N.; Treebak, J.T.; Cox, J.; Mann, M. Deep Proteomics of Mouse Skeletal Muscle Enables Quantitation of Protein Isoforms, Metabolic Pathways, and Transcription Factors. Mol. Cell. Proteom. 2015, 14, 841–853. [Google Scholar] [CrossRef]
- Hosseininia, S.; Önnerfjord, P.; Dahlberg, L.E. Targeted Proteomics of Hip Articular Cartilage in OA and Fracture Patients. J. Orthop. Res. 2019, 37, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Theocharis, A.D.; Skandalis, S.S.; Gialeli, C.; Karamanos, N.K. Extracellular Matrix Structure. Adv. Drug. Deliv. Rev. 2016, 97, 4–27. [Google Scholar] [CrossRef] [PubMed]
- Garantziotis, S.; Savani, R.C. Hyaluronan Biology: A Complex Balancing Act of Structure, Function, Location and Context. Matrix Biol. 2019, 78–79, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.H.; Jang, K.M.; Hahn, S.K.; Park, J.Y.; Jung, H.; Oh, K.; Park, K.M.; Yeom, J.; Park, S.H.; Kim, S.W.; et al. Three-Dimensional Bioprinting of Multilayered Constructs Containing Human Mesenchymal Stromal Cells for Osteochondral Tissue Regeneration in the Rabbit Knee Joint. Biofabrication 2016, 8, 014102. [Google Scholar] [CrossRef]
- Medvedeva, E.V.; Grebenik, E.A.; Gornostaeva, S.N.; Telpuhov, V.I.; Lychagin, A.V.; Timashev, P.S.; Chagin, A.S. Repair of Damaged Articular Cartilage: Current Approaches and Future Directions. Int. J. Mol. Sci. 2018, 19, 2366. [Google Scholar] [CrossRef]
- Zhang, S.; Hu, B.; Liu, W.; Wang, P.; Lv, X.; Chen, S.; Liu, H.; Shao, Z. Articular Cartilage Regeneration: The Role of Endogenous Mesenchymal Stem/Progenitor Cell Recruitment and Migration. Semin. Arthritis Rheum. 2020, 50, 198–208. [Google Scholar] [CrossRef]
- Guettler, J.H.; Demetropoulos, C.K.; Yang, K.H.; Jurist, K.A. Osteochondral defects in the human knee: Influence of defect size on cartilage rim stress and load redistribution to surrounding cartilage. Am. J. Sports Med. 2004, 32, 1451–1458. [Google Scholar] [CrossRef]
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 354 Diseases and Injuries for 195 Countries and Territories, 1990-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI Guidelines for the Non-Surgical Management of Knee, Hip, and Polyarticular Osteoarthritis. Polymers (Basel) 2019, 27, 1578–1589. [Google Scholar] [CrossRef]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Rheumatol. 2020, 72, 220–233. [Google Scholar] [CrossRef]
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The Global Burden of Hip and Knee Osteoarthritis: Estimates from the Global Burden of Disease 2010 Study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef]
- Wallace, I.J.; Worthington, S.; Felson, D.T.; Jurmain, R.D.; Wren, K.T.; Maijanen, H.; Woods, R.J.; Lieberman, D.E. Knee Osteoarthritis Has Doubled in Prevalence since the Mid-20th Century. Proc. Natl. Acad. Sci. USA 2017, 114, 9332–9336. [Google Scholar] [CrossRef]
- Peck, J.; Slovek, A.; Miro, P.; Vij, N.; Traube, B.; Lee, C.; Berger, A.A.; Kassem, H.; Kaye, A.D.; Sherman, W.F.; et al. A Comprehensive Review of Viscosupplementation in Osteoarthritis of the Knee. Orthop. Rev. 2021, 13, 25549. [Google Scholar] [CrossRef]
- Burdick, J.A.; Chung, C. Influence of Three-Dimensional Hyaluronic Acid Microenvironments on Mesenchymal Stem Cell Chondrogenesis. Tissue Eng. Part A 2009, 15, 243–254. [Google Scholar] [CrossRef]
- Zheng, Z.; Patel, M.; Patel, R. Hyaluronic Acid-Based Materials for Bone Regeneration: A Review. React. Funct. Polym. 2022, 171, 105151. [Google Scholar] [CrossRef]
- Felson, D.T. Clinical practice. Osteoarthritis of the knee. N. Engl. J. Med. 2006, 354, 841–848. [Google Scholar] [CrossRef]
- Collins, J.E.; Losina, E.; Nevitt, M.C.; Roemer, F.W.; Guermazi, A.; Lynch, J.A.; Katz, J.N.; Kent Kwoh, C.; Kraus, V.B.; Hunter, D.J. Semiquantitative Imaging Biomarkers of Knee Osteoarthritis Progression: Data From the Foundation for the National Institutes of Health Osteoarthritis Biomarkers Consortium. Arthritis Rheumatol. 2016, 68, 2422–2431. [Google Scholar] [CrossRef]
- Rim, Y.A.; Ju, J.H. The Role of Fibrosis in Osteoarthritis Progression. Life 2021, 11, 3. [Google Scholar] [CrossRef]
- Remst, D.F.G.; Davidson, E.N.B.; Van Der Kraan, P.M. Unravelling Osteoarthritis-Related Synovial Fibrosis: A Step Closer to Solving Joint Stiffness. Rheumatology (Oxford) 2015, 54, 1954–1963. [Google Scholar] [CrossRef]
- Li, D.; Wang, H.; He, J.Y.; Wang, C.L.; Feng, W.J.; Shen, C.; Zhu, J.F.; Wang, D.L.; Chen, X.D. Inflammatory and Fibrosis Infiltration in Synovium Associated with the Progression in Developmental Dysplasia of the Hip. Mol. Med. Rep. 2019, 19, 2808–2816. [Google Scholar] [CrossRef]
- Ulus, Y.; Tander, B.; Akyol, Y.; Durmus, D.; Buyukakincak, O.; Gul, U.; Canturk, F.; Bilgici, A.; Kuru, O. Therapeutic Ultrasound versus Sham Ultrasound for the Management of Patients with Knee Osteoarthritis: A Randomized Double-Blind Controlled Clinical Study. Int. J. Rheum. Dis. 2012, 15, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Chapurlat, R.; Al-Daghri, N.; Herrero-Beaumont, G.; Bruyère, O.; Rannou, F.; Roth, R.; Uebelhart, D.; Reginster, J.Y. Safety of Oral Non-Selective Non-Steroidal Anti-Inflammatory Drugs in Osteoarthritis: What Does the Literature Say? Drugs Aging 2019, 36, 15–24. [Google Scholar] [CrossRef]
- Cutolo, M.; Berenbaum, F.; Hochberg, M.; Punzi, L.; Reginster, J.Y. Commentary on Recent Therapeutic Guidelines for Osteoarthritis. Semin. Arthritis Rheum. 2015, 44, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Kamaruzaman, H.; Kinghorn, P.; Oppong, R. Cost-Effectiveness of Surgical Interventions for the Management of Osteoarthritis: A Systematic Review of the Literature. BMC Musculoskelet. Disord. 2017, 18, 183. [Google Scholar] [CrossRef] [PubMed]
- Gomoll, A.H.; Filardo, G.; Almqvist, F.K.; Bugbee, W.D.; Jelic, M.; Monllau, J.C.; Puddu, G.; Rodkey, W.G.; Verdonk, P.; Verdonk, R.; et al. Surgical Treatment for Early Osteoarthritis. Part II: Allografts and Concurrent Procedures. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 468–486. [Google Scholar] [CrossRef]
- Kirkley, A.; Birmingham, T.B.; Litchfield, R.B.; Giffin, J.R.; Willits, K.R.; Wong, C.J.; Feagan, B.G.; Donner, A.; Griffin, S.H.; D’Ascanio, L.M.; et al. A Randomized Trial of Arthroscopic Surgery for Osteoarthritis of the Knee. N. Engl. J. Med. 2008, 359, 1097–1107. [Google Scholar] [CrossRef]
- Nwachukwu, B.U.; Alpaugh, K.; McCormick, F.; Martin, S.D. All-Arthroscopic Reconstruction of the Acetabular Labrum by Capsular Augmentation. Arthrosc. Tech. 2015, 4, e127–e131. [Google Scholar] [CrossRef]
- Konopka, J.F.; Lee, Y.Y.; Su, E.P.; McLawhorn, A.S. Quality-Adjusted Life Years After Hip and Knee Arthroplasty: Health-Related Quality of Life After 12,782 Joint Replacements. JBJS Open Access 2018, 3, E0007. [Google Scholar] [CrossRef]
- Hamilton, D.; Henderson, G.R.; Gaston, P.; MacDonald, D.; Howie, C.; Simpson, A.H.R.W. Comparative Outcomes of Total Hip and Knee Arthroplasty: A Prospective Cohort Study. Postgrad. Med. J. 2012, 88, 627–631. [Google Scholar] [CrossRef]
- Dumenci, L.; Perera, R.A.; Keefe, F.J.; Ang, D.C.; Slover, J.; Jensen, M.P.; Riddle, D.L. Model-Based Pain and Function Outcome Trajectory Types for Patients Undergoing Knee Arthroplasty: A Secondary Analysis from a Randomized Clinical Trial. Osteoarthr. Cartil. 2019, 27, 878–884. [Google Scholar] [CrossRef]
- Jayakumar, P.; Bozic, K.J. Advanced Decision-Making Using Patient-Reported Outcome Measures in Total Joint Replacement. J. Orthop. Res. 2020, 38, 1414–1422. [Google Scholar] [CrossRef]
- Singh, J.A.; Yu, S.; Chen, L.; Cleveland, J.D. Rates of Total Joint Replacement in the United States: Future Projections to 2020–2040 Using the National Inpatient Sample. J. Rheumatol. 2019, 46, 1134–1140. [Google Scholar] [CrossRef]
- Bennett, C.G.; Lu, L.Y.; Thomas, K.A.; Giori, N.J. Joint Replacement Surgery in Homeless Veterans. Arthroplast. Today 2017, 3, 253–256. [Google Scholar] [CrossRef]
- Fang, M.; Noiseux, N.; Linson, E.; Cram, P. The Effect of Advancing Age on Total Joint Replacement Outcomes. Geriatr. Orthop. Surg. Rehabil. 2015, 6, 173. [Google Scholar] [CrossRef]
- Teterycz, D.; Ferry, T.; Lew, D.; Stern, R.; Assal, M.; Hoffmeyer, P.; Bernard, L.; Uçkay, I. Outcome of Orthopedic Implant Infections Due to Different Staphylococci. Int. J. Infect. Dis. 2010, 14, e913–e918. [Google Scholar] [CrossRef]
- Gu, A.; Malahias, M.A.; Selemon, N.A.; Wei, C.; Gerhard, E.F.; Cohen, J.S.; Fassihi, S.C.; Stake, S.; Bernstein, S.L.; Chen, A.Z.; et al. Increased Severity of Anaemia Is Associated with 30-Day Complications Following Total Joint Replacement. Bone Jt. J. 2020, 102, 485–494. [Google Scholar] [CrossRef]
- Dennis, D.A. Wound Complications in TKA. Orthopedics 2002, 25, 973–974. [Google Scholar] [CrossRef]
- Weber, M.; Renkawitz, T.; Voellner, F.; Craiovan, B.; Greimel, F.; Worlicek, M.; Grifka, J.; Benditz, A. Revision Surgery in Total Joint Replacement Is Cost-Intensive. Biomed. Res. Int. 2018, 2018, 8987104. [Google Scholar] [CrossRef]
- Smith, T.J.; Siddiqi, A.; Forte, S.A.; Judice, A.; Sculco, P.K.; Vigdorchik, J.M.; Schwarzkopf, R.; Springer, B.D. Periprosthetic Fractures Through Tracking Pin Sites Following Computer Navigated and Robotic Total and Unicompartmental Knee Arthroplasty: A Systematic Review. JBJS Rev. 2021, 9, e20. [Google Scholar] [CrossRef]
- Ashammakhi, N.; Ahadian, S.; Pountos, I.; Hu, S.K.; Tellisi, N.; Bandaru, P.; Ostrovidov, S.; Dokmeci, M.R.; Khademhosseini, A. In Situ Three-Dimensional Printing for Reparative and Regenerative Therapy. Biomed. Microdevices 2019, 21, 42. [Google Scholar] [CrossRef]
- Cohen, D.L.; Lipton, J.I.; Bonassar, L.J.; Lipson, H. Additive Manufacturing for in Situ Repair of Osteochondral Defects. Biofabrication 2010, 2, 035004. [Google Scholar] [CrossRef] [PubMed]
- Freitag, J.; Bates, D.; Boyd, R.; Shah, K.; Barnard, A.; Huguenin, L.; Tenen, A. Mesenchymal Stem Cell Therapy in the Treatment of Osteoarthritis: Reparative Pathways, Safety and Efficacy—A Review. BMC Musculoskelet. Disord. 2016, 17, 230. [Google Scholar] [CrossRef] [PubMed]
- Berthiaume, F.; Maguire, T.J.; Yarmush, M.L. Tissue Engineering and Regenerative Medicine: History, Progress, and Challenges. Annu. Rev. Chem. Biomol. Eng. 2011, 2, 403–430. [Google Scholar] [CrossRef] [PubMed]
- Madeira, C.; Santhagunam, A.; Salgueiro, J.B.; Cabral, J.M.S. Advanced Cell Therapies for Articular Cartilage Regeneration. Trends Biotechnol. 2015, 33, 35–42. [Google Scholar] [CrossRef]
- Facchin, F.; Bianconi, E.; Canaider, S.; Basoli, V.; Biava, P.M.; Ventura, C. Tissue Regeneration without Stem Cell Transplantation: Self-Healing Potential from Ancestral Chemistry and Physical Energies. Stem Cells Int. 2018, 3, 7412035. [Google Scholar] [CrossRef]
- Yang, Z.; Li, H.; Yuan, Z.; Fu, L.; Jiang, S.; Gao, C.; Wang, F.; Zha, K.; Tian, G.; Sun, Z.; et al. Endogenous Cell Recruitment Strategy for Articular Cartilage Regeneration. Acta Biomater. 2020, 114, 31–52. [Google Scholar] [CrossRef]
- Moraes, V.Y.; Lenza, M.; Tamaoki, M.J.; Faloppa, F.; Belloti, J.C. Platelet-Rich Therapies for Musculoskeletal Soft Tissue Injuries. Cochrane Database Syst. Rev. 2013, 12, CD010071. [Google Scholar] [CrossRef]
- Lee, J.K.; Link, J.M.; Hu, J.C.Y.; Athanasiou, K.A. The Self-Assembling Process and Applications in Tissue Engineering. Cold Spring Harb. Perspect. Med. 2017, 7, a025668. [Google Scholar] [CrossRef]
- Schon, B.S.; Hooper, G.J.; Woodfield, T.B.F. Modular Tissue Assembly Strategies for Biofabrication of Engineered Cartilage. Ann. Biomed. Eng. 2016, 45, 100–114. [Google Scholar] [CrossRef]
- Jakab, K.; Norotte, C.; Marga, F.; Murphy, K.; Vunjak-Novakovic, G.; Forgacs, G. Tissue Engineering by Self-Assembly and Bio-Printing of Living Cells. Biofabrication 2010, 2, 022001. [Google Scholar] [CrossRef]
- Mekhileri, N.V.; Lim, K.S.; Brown, G.C.J.; Mutreja, I.; Schon, B.S.; Hooper, G.J.; Woodfield, T.B.F. Automated 3D Bioassembly of Micro-Tissues for Biofabrication of Hybrid Tissue Engineered Constructs. Biofabrication 2018, 10, 024103. [Google Scholar] [CrossRef]
- Groll, J.; Boland, T.; Blunk, T.; Burdick, J.A.; Cho, D.W.; Dalton, P.D.; Derby, B.; Forgacs, G.; Li, Q.; Mironov, V.A.; et al. Biofabrication: Reappraising the Definition of an Evolving Field. Biofabrication 2016, 8, 013001. [Google Scholar] [CrossRef]
- Shishkovsky, I.; Volchkov, S.; Scherbakov, V.; Volova, L. Biocompatible Features of Magnetic Nano-Oxide Core/ PCL Shell 3D Composites Fabricated via SLS/M Process. Adv. Mater. Lett. 2018, 9, 31–35. [Google Scholar] [CrossRef]
- Shishkovsky, I.V. Fundamentals of Additive Technologies of High Resolutions; Peter Publish: Sankt-Peterburg, Russia, 2016; p. 400. Available online: http://fian.smr.ru/old-rp/presentations/Basis%20of%20Additive%20Manufacturing-RU-Shishkovsky2016.pdf (accessed on 7 June 2023).
- Lynch, C.R.; Kondiah, P.P.D.; Choonara, Y.E. Advanced Strategies for Tissue Engineering in Regenerative Medicine: A Biofabrication and Biopolymer Perspective. Molecules 2021, 26, 2518. [Google Scholar] [CrossRef]
- Klotz, B.J.; Gawlitta, D.; Rosenberg, A.J.W.P.; Malda, J.; Melchels, F.P.W. Gelatin-Methacryloyl Hydrogels: Towards Biofabrication-Based Tissue Repair. Trends Biotechnol. 2016, 34, 394–407. [Google Scholar] [CrossRef]
- Zhu, W.; Ma, X.; Gou, M.; Mei, D.; Zhang, K.; Chen, S. 3D Printing of Functional Biomaterials for Tissue Engineering. Curr. Opin. Biotechnol. 2016, 40, 103–112. [Google Scholar] [CrossRef]
- Vining, K.H.; Mooney, D.J. Mechanical Forces Direct Stem Cell Behaviour in Development and Regeneration. Nat. Rev. Mol. Cell Biol. 2017, 18, 728–742. [Google Scholar] [CrossRef]
- Bertlein, S.; Brown, G.; Lim, K.S.; Jungst, T.; Boeck, T.; Blunk, T.; Tessmar, J.; Hooper, G.J.; Woodfield, T.B.F.; Groll, J. Thiol-Ene Clickable Gelatin: A Platform Bioink for Multiple 3D Biofabrication Technologies. Adv. Mater. 2017, 29, 1703404. [Google Scholar] [CrossRef]
- Ford, S.; Minshall, T. Invited Review Article: Where and How 3D Printing Is Used in Teaching and Education. Addit. Manuf. 2019, 25, 131–150. [Google Scholar] [CrossRef]
- Campbell, I.; Diegel, O.; Kowen, J.; Wohlers, T. Wohlers Report 2018: 3D Printing and Additive Manufacturing State of the Industry: Annual Worldwide Progress Report, 23rd ed.; Wohlers: Hamburg, Germany, 2018; p. 343. Available online: https://researchspace.auckland.ac.nz/docs/uoa-docs/rights.htm (accessed on 7 June 2023).
- Michalski, M.H.; Ross, J.S. The Shape of Things to Come: 3D Printing in Medicine. JAMA 2014, 312, 2213–2214. [Google Scholar] [CrossRef]
- Mendes, L.; Kangas, A.; Kukko, K.; Mølgaard, B.; Säämänen, A.; Kanerva, T.; Flores Ituarte, I.; Huhtiniemi, M.; Stockmann-Juvala, H.; Partanen, J.; et al. Characterization of Emissions from a Desktop 3D Printer. J. Ind. Ecol. 2017, 21, S94–S106. [Google Scholar] [CrossRef]
- Shahrubudina, N.; Lee, T.C.; Ramlan, R. An Overview on 3D Printing Technology: Technological, Materials, and Applications. Procedia Manuf. 2019, 35, 1286–1296. [Google Scholar] [CrossRef]
- Huang, S.H.; Liu, P.; Mokasdar, A.; Hou, L. Additive Manufacturing and Its Societal Impact: A Literature Review. Int. J. Adv. Manuf. Technol. 2013, 67, 1191–1203. [Google Scholar] [CrossRef]
- Gupta, N.; Weber, C.; Newsome, S. Additive Manufacturing: Status and Opportunities; Science and Technology Policy Institute: Washington, DC, USA, 2012; Available online: https://www.researchgate.net/publication/312153354_Additive_Manufacturing_Status_and_Opportunities (accessed on 7 June 2023).
- Goh, G.D.; Sing, S.L.; Yeong, W.Y. A Review on Machine Learning in 3D Printing: Applications, Potential, and Challenges. Artif. Intell. Rev. 2021, 54, 63–94. [Google Scholar] [CrossRef]
- Urhal, P.; Weightman, A.; Diver, C.; Bartolo, P. Robot Assisted Additive Manufacturing: A Review. Robot Comput. Integr. Manuf. 2019, 59, 335–345. [Google Scholar] [CrossRef]
- Dawood, A.; Marti, B.M.; Sauret-Jackson, V.; Darwood, A. 3D Printing in Dentistry. Br. Dent. J. 2015, 219, 521–529. [Google Scholar] [CrossRef]
- Rahman, Z.; Charoo, N.A.; Kuttolamadom, M.; Asadi, A.; Khan, M.A. Printing of Personalized Medication Using Binder Jetting 3D Printer. Precis. Med. Investig. Pract. Provid. 2020, 3, 473–481. [Google Scholar] [CrossRef]
- Ho, C.M.B.; Ng, S.H.; Yoon, Y.J. A Review on 3D Printed Bioimplants. Int. J. Precis. Eng. Manuf. 2015, 16, 1035–1046. [Google Scholar] [CrossRef]
- Naveau, A.; Smirani, R.; Catros, S.; de Oliveira, H.; Fricain, J.C.; Devillard, R. A Bibliometric Study to Assess Bioprinting Evolution. Appl. Sci. 2017, 7, 1331. [Google Scholar] [CrossRef]
- Duarte Campos, D.F.; Blaeser, A. 3D-Bioprinting. In Basic Concepts on 3D Cell Culture; Springer International Publishing: Cham, Switzerland, 2021; pp. 201–232. [Google Scholar] [CrossRef]
- Mandrycky, C.; Wang, Z.; Kim, K.; Kim, D.H. 3D Bioprinting for Engineering Complex Tissues. Biotechnol. Adv. 2016, 34, 422–434. [Google Scholar] [CrossRef]
- Ahn, S.H.; Lee, J.; Park, S.A.; Kim, W.D. Three-Dimensional Bio-Printing Equipment Technologies for Tissue Engineering and Regenerative Medicine. Tissue Eng. Regen. Med. 2016, 13, 663–676. [Google Scholar] [CrossRef]
- Gu, B.K.; Choi, D.J.; Park, S.J.; Kim, Y.J.; Kim, C.H. 3D Bioprinting Technologies for Tissue Engineering Applications. Adv. Exp. Med. Biol. 2018, 1078, 15–28. [Google Scholar] [CrossRef]
- Ozbolat, I.; Gudapati, H. A Review on Design for Bioprinting. Bioprinting 2016, 3–4, 1–14. [Google Scholar] [CrossRef]
- Vijayavenkataraman, S.; Fuh, J.Y.H.; Lu, W.F. 3D Printing and 3D Bioprinting in Pediatrics. Bioengineering 2017, 4, 63. [Google Scholar] [CrossRef]
- Bicudo, E.; Faulkner, A.; Li, P. Software, Risks, and Liabilities: Ongoing and Emergent Issues in 3D Bioprinting. J. Risk Res. 2020, 24, 1319–1334. [Google Scholar] [CrossRef]
- Nielsen, J.; Kaldor, J.; Irwin, A.; Stewart, C.; Nicol, D. Bespoke Regulation for Bespoke Medicine? A Comparative Analysis of Bioprinting Regulation in Europe, the USA and Australia. J. 3D Print. Med. 2021, 5, 155–167. [Google Scholar] [CrossRef]
- Ireland, R.G.; Simmons, C.A. Human Pluripotent Stem Cell Mechanobiology: Manipulating the Biophysical Microenvironment for Regenerative Medicine and Tissue Engineering Applications. Stem Cells 2015, 33, 3187–3196. [Google Scholar] [CrossRef]
- Kwon, H.; Brown, W.E.; Lee, C.A.; Wang, D.; Paschos, N.; Hu, J.C.; Athanasiou, K.A. Surgical and Tissue Engineering Strategies for Articular Cartilage and Meniscus Repair. Nat. Rev. Rheumatol. 2019, 15, 550–570. [Google Scholar] [CrossRef]
- Williams, D.F. On the Mechanisms of Biocompatibility. Biomaterials 2008, 29, 2941–2953. [Google Scholar] [CrossRef]
- Mehesz, A.N.; Brown, J.; Hajdu, Z.; Beaver, W.; Da Silva, J.V.L.; Visconti, R.P.; Markwald, R.R.; Mironov, V. Scalable Robotic Biofabrication of Tissue Spheroids. Biofabrication 2011, 3, 025002. [Google Scholar] [CrossRef]
- Vert, M.; Doi, Y.; Hellwich, K.H.; Hess, M.; Hodge, P.; Kubisa, P.; Rinaudo, M.; Schué, F.O. Terminology for biorelated polymers and applications (IUPAC Recommendations 2012). Pure Appl. Chem. 2012, 84, 377. [Google Scholar] [CrossRef]
- Prokoshkin, S.; Pustov, Y.; Zhukova, Y.; Kadirov, P.; Dubinskiy, S.; Sheremetyev, V.; Karavaeva, M. Effect of Thermomechanical Treatment on Functional Properties of Biodegradable Fe-30Mn-5Si Shape Memory Alloy. Met. Mater. Trans. A Phys. Met. Mater. Sci. 2021, 52, 2024–2032. [Google Scholar] [CrossRef]
- De Jong, W.H.; Carraway, J.W.; Geertsma, R.E. In vivo and in vitro testing for the biological safety evaluation of biomaterials and medical devices. In Biocompatibility and Performance of Medical Devices; Boutrand, J.-P., Ed.; Woodhead Publishing: Sawston, UK, 2012; pp. 120–158. [Google Scholar]
- Ge, Z.; Jin, Z.; Cao, T. Manufacture of Degradable Polymeric Scaffolds for Bone Regeneration. Biomed. Mater. 2008, 3, 22001. [Google Scholar] [CrossRef] [PubMed]
- Dorati, R.; DeTrizio, A.; Modena, T.; Conti, B.; Benazzo, F.; Gastaldi, G.; Genta, I. Biodegradable Scaffolds for Bone Regeneration Combined with Drug-Delivery Systems in Osteomyelitis Therapy. Pharmaceuticals 2017, 10, 96. [Google Scholar] [CrossRef]
- Dai, Z.; Ronholm, J.; Tian, Y.; Sethi, B.; Cao, X. Sterilization Techniques for Biodegradable Scaffolds in Tissue Engineering Applications. J. Tissue Eng. 2016, 7, 2041731416648810. [Google Scholar] [CrossRef]
- Taraballi, F.; Sushnitha, M.; Tsao, C.; Bauza, G.; Liverani, C.; Shi, A.; Tasciotti, E. Biomimetic Tissue Engineering: Tuning the Immune and Inflammatory Response to Implantable Biomaterials. Adv. Healthc. Mater. 2018, 7, 1800490. [Google Scholar] [CrossRef]
- Nikolova, M.P.; Chavali, M.S. Recent Advances in Biomaterials for 3D Scaffolds: A Review. Bioact. Mater. 2019, 4, 271–292. [Google Scholar] [CrossRef]
- Hinderer, S.; Layland, S.L.; Schenke-Layland, K. ECM and ECM-like Materials–Biomaterials for Applications in Regenerative Medicine and Cancer Therapy. Adv. Drug Deliv. Rev. 2016, 97, 260–269. [Google Scholar] [CrossRef]
- Crosby, C.O.; Zoldan, J. Mimicking the Physical Cues of the ECM in Angiogenic Biomaterials. Regen. Biomater. 2019, 6, 61–73. [Google Scholar] [CrossRef]
- O’Brien, F.J. Biomaterials & Scaffolds for Tissue Engineering. Mater. Today 2011, 14, 88–95. [Google Scholar] [CrossRef]
- Ozbolat, I.T. Scaffold-Based or Scaffold-Free Bioprinting: Competing or Complementing Approaches? J. Nanotechnol. Eng. Med. 2015, 6, 024701. [Google Scholar] [CrossRef]
- Makris, E.A.; Gomoll, A.H.; Malizos, K.N.; Hu, J.C.; Athanasiou, K.A. Repair and Tissue Engineering Techniques for Articular Cartilage. Nat. Rev. Rheumatol. 2015, 11, 21–34. [Google Scholar] [CrossRef]
- Golafshan, N.; Vorndran, E.; Zaharievski, S.; Brommer, H.; Kadumudi, F.B.; Dolatshahi-Pirouz, A.; Gbureck, U.; van Weeren, R.; Castilho, M.; Malda, J. Tough Magnesium Phosphate-Based 3D-Printed Implants Induce Bone Regeneration in an Equine Defect Model. Biomaterials 2020, 261, 120302. [Google Scholar] [CrossRef]
- Kilian, D.; Ahlfeld, T.; Akkineni, A.R.; Bernhardt, A.; Gelinsky, M.; Lode, A. 3D Bioprinting of Osteochondral Tissue Substitutes-in Vitro-Chondrogenesis in Multi-Layered Mineralized Constructs. Sci. Rep. 2020, 10, 8277. [Google Scholar] [CrossRef]
- Stratton, S.; Shelke, N.B.; Hoshino, K.; Rudraiah, S.; Kumbar, S.G. Bioactive Polymeric Scaffolds for Tissue Engineering. Bioact. Mater. 2016, 1, 93–108. [Google Scholar] [CrossRef]
- Yu, J.; Xia, H.; Ni, Q.Q. A Three-Dimensional Porous Hydroxyapatite Nanocomposite Scaffold with Shape Memory Effect for Bone Tissue Engineering. J. Mater. Sci. 2018, 53, 4734–4744. [Google Scholar] [CrossRef]
- Babuska, V.; Moztarzadeh, O.; Kubikova, T.; Moztarzadeh, A.; Hrusak, D.; Tonar, Z. Evaluating the Osseointegration of Nanostructured Titanium Implants in Animal Models: Current Experimental Methods and Perspectives (Review). Biointerphases 2016, 11, 030801. [Google Scholar] [CrossRef]
- Turnbull, G.; Clarke, J.; Picard, F.; Riches, P.; Jia, L.; Han, F.; Li, B.; Shu, W. 3D Bioactive Composite Scaffolds for Bone Tissue Engineering. Bioact. Mater. 2017, 3, 278–314. [Google Scholar] [CrossRef]
- Chen, Q.; Thouas, G.A. Metallic Implant Biomaterials. Mater. Sci. Eng. R Rep. 2015, 87, 1–57. [Google Scholar] [CrossRef]
- Chua, K.; Khan, I.; Malhotra, R.; Zhu, D. Additive Manufacturing and 3D Printing of Metallic Biomaterials. Eng. Regen. 2021, 2, 288–299. [Google Scholar] [CrossRef]
- Sing, S.L.; Tey, C.F.; Tan, J.H.K.; Huang, S.; Yeong, W.Y. 3D Printing of Metals in Rapid Prototyping of Biomaterials: Techniques in Additive Manufacturing. In Rapid Prototyping of Biomaterials; Techniques in Additive Manufacturing; Woodhead Publishing: Sawston, UK, 2020; pp. 17–40. [Google Scholar] [CrossRef]
- Shishkovsky, I.V.; Scherbakov, V.I. Additive Manufacturing of Polymer Composites with Nano-Titania Inclusions. Laser Phys. Lett. 2021, 18, 066001. [Google Scholar] [CrossRef]
- Khorsandi, D.; Fahimipour, A.; Saber, S.S.; Ahmad, A.; De Stephanis, A.A. Fused Deposition Modeling and Stereolithography 3D Bioprinting in Dental Science. EC Dent. Sci. 2019, 18, 110–115. [Google Scholar]
- Shishkovsky, I.V.; Volova, L.T.; Kuznetsov, M.V.; Morozov, Y.G.; Parkin, I.P. Porous Biocompatible Implants and Tissue Scaffolds Synthesized by Selective Laser Sintering from Ti and NiTi. J. Mater. Chem. 2008, 18, 1309–1317. [Google Scholar] [CrossRef]
- Albrektsson, T.; Johansson, C. Osteoinduction, Osteoconduction and Osseointegration. Eur. Spine J. 2001, 10 (Suppl. 2), S96–S101. [Google Scholar] [CrossRef] [PubMed]
- Roque, R.; Barbosa, G.F.; Guastaldi, A.C. Design and 3D Bioprinting of Interconnected Porous Scaffolds for Bone Regeneration. An Additive Manufacturing Approach. J. Manuf. Process. 2021, 64, 655–663. [Google Scholar] [CrossRef]
- Singh, L.; Kumar, V.; Ratner, B.D. Generation of Porous Microcellular 85/15 Poly (DL-Lactide-Co-Glycolide) Foams for Biomedical Applications. Biomaterials 2004, 25, 2611–2617. [Google Scholar] [CrossRef]
- Julien, M.; Khoshniat, S.; Lacreusette, A.; Gatius, M.; Bozec, A.; Wagner, E.F.; Wittrant, Y.; Masson, M.; Weiss, P.; Beck, L.; et al. Phosphate-Dependent Regulation of MGP in Osteoblasts: Role of ERK1/2 and Fra-1. J. Bone Min. Res. 2009, 24, 1856–1868. [Google Scholar] [CrossRef]
- Tada, H.; Nemoto, E.; Foster, B.L.; Somerman, M.J.; Shimauchi, H. Phosphate Increases Bone Morphogenetic Protein-2 Expression through CAMP-Dependent Protein Kinase and ERK1/2 Pathways in Human Dental Pulp Cells. Bone 2011, 48, 1409–1416. [Google Scholar] [CrossRef]
- Best, S.M.; Gibson, I.; Patel, N.; Best, S.M.; Bonfield, W.; Gibson, I.R.; Hing, K.A.; Damien, E.; Revell, P.A. A Comparative Study on the in Vivo Behavior of Hydroxyapatite and Silicon Substituted Hydroxyapatite Granules. J. Mater. Sci. Mater. Med. 2002, 13, 1199–1206. [Google Scholar] [CrossRef]
- Chen, Q.Z.; Thompson, I.D.; Boccaccini, A.R. 45S5 Bioglass®-Derived Glass–Ceramic Scaffolds for Bone Tissue Engineering. Biomaterials 2006, 27, 2414–2425. [Google Scholar] [CrossRef]
- Lien, S.M.; Ko, L.Y.; Huang, T.J. Effect of Pore Size on ECM Secretion and Cell Growth in Gelatin Scaffold for Articular Cartilage Tissue Engineering. Acta Biomater. 2009, 5, 670–679. [Google Scholar] [CrossRef]
- Wang, X.; Tolba, E.; Der, H.C.S.; Neufurth, M.; Feng, Q.; Diehl-Seifert, B.R.; Mü Ller, W.E.G. Effect of Bioglass on Growth and Biomineralization of SaOS-2 Cells in Hydrogel after 3D Cell Bioprinting. PLoS ONE 2014, 9, e112497. [Google Scholar] [CrossRef]
- Poh, P.S.P.; Hutmacher, D.W.; Holzapfel, B.M.; Solanki, A.K.; Stevens, M.M.; Woodruff, M.A. In Vitro and in Vivo Bone Formation Potential of Surface Calcium Phosphate-Coated Polycaprolactone and Polycaprolactone/Bioactive Glass Composite Scaffolds. Acta Biomater. 2016, 30, 319–333. [Google Scholar] [CrossRef]
- Pina, S.; Ferreira, J.M.F. Brushite-Forming Mg-, Zn- and Sr-Substituted Bone Cements for Clinical Applications. Materials 2010, 3, 519–535. [Google Scholar] [CrossRef]
- Zreiqat, H.; Ramaswamy, Y.; Wu, C.; Paschalidis, A.; Lu, Z.F.; James, B.; Birke, O.; McDonald, M.; Little, D.; Dunstan, C.R. The Incorporation of Strontium and Zinc into a Calcium–Silicon Ceramic for Bone Tissue Engineering. Biomaterials 2010, 31, 3175–3184. [Google Scholar] [CrossRef]
- Lode, A.; Heiss, C.; Knapp, G.; Thomas, J.; Nies, B.; Gelinsky, M.; Schumacher, M. Strontium-Modified Premixed Calcium Phosphate Cements for the Therapy of Osteoporotic Bone Defects. Acta Biomater. 2018, 65, 475–485. [Google Scholar] [CrossRef]
- Bohner, M.; Galea, L.; Doebelin, N. Calcium Phosphate Bone Graft Substitutes: Failures and Hopes. J. Eur. Ceram. Soc. 2012, 32, 2663–2671. [Google Scholar] [CrossRef]
- Geffers, M.; Groll, J.; Gbureck, U. Reinforcement Strategies for Load-Bearing Calcium Phosphate Biocements. Materials 2015, 8, 2700–2717. [Google Scholar] [CrossRef]
- Mazur, E.; Shishkovsky, I. Additively Manufactured Hierarchical Auxetic Mechanical Metamaterials. Materials 2022, 15, 5600. [Google Scholar] [CrossRef]
- Warnke, P.H.; Seitz, H.; Warnke, F.; Becker, S.T.; Sivananthan, S.; Sherry, E.; Liu, Q.; Wiltfang, J.; Douglas, T. Ceramic Scaffolds Produced by Computer-Assisted 3D Printing and Sintering: Characterization and Biocompatibility Investigations. J. Biomed. Mater. Res. B Appl. Biomater. 2010, 93, 212–217. [Google Scholar] [CrossRef]
- Sabree, I.; Gough, J.E.; Derby, B. Mechanical Properties of Porous Ceramic Scaffolds: Influence of Internal Dimensions. Ceram. Int. 2015, 41, 8425–8432. [Google Scholar] [CrossRef]
- Groll, J.; Burdick, J.A.; Cho, D.W.; Derby, B.; Gelinsky, M.; Heilshorn, S.C.; Jüngst, T.; Malda, J.; Mironov, V.A.; Nakayama, K.; et al. A Definition of Bioinks and Their Distinction from Biomaterial Inks. Biofabrication 2018, 11, 013001. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Gao, M.; Syed, S.; Zhuang, J.; Xu, X.; Zhang, X.Q. Bioactive Hydrogels for Bone Regeneration. Bioact. Mater. 2018, 3, 401–417. [Google Scholar] [CrossRef] [PubMed]
- Mancha Sánchez, E.; Gómez-Blanco, J.C.; López Nieto, E.; Casado, J.G.; Macías-García, A.; Díaz Díez, M.A.; Carrasco-Amador, J.P.; Torrejón Martín, D.; Sánchez-Margallo, F.M.; Pagador, J.B. Hydrogels for Bioprinting: A Systematic Review of Hydrogels Synthesis, Bioprinting Parameters, and Bioprinted Structures Behavior. Front. Bioeng. Biotechnol. 2020, 8, 776. [Google Scholar] [CrossRef]
- Shhipunov, J.A.; Koneva, E.L.; Postnova, I.V. Vysokomolekuljarnye soedinenija. Serija A 2002, 44, 1201–1211. Available online: https://cyberleninka.ru/article/n/gomogennye-alginatnye-geli-fazovoe-povedenie-i-reologicheskie-svoystva/viewer (accessed on 17 March 2023).
- Naahidi, S.; Jafari, M.; Logan, M.; Wang, Y.; Yuan, Y.; Bae, H.; Dixon, B.; Chen, P. Biocompatibility of Hydrogel-Based Scaffolds for Tissue Engineering Applications. Biotechnol. Adv. 2017, 35, 530–544. [Google Scholar] [CrossRef]
- Bashir, S.; Hina, M.; Iqbal, J.; Rajpar, A.H.; Mujtaba, M.A.; Alghamdi, N.A.; Wageh, S.; Ramesh, K.; Ramesh, S. Fundamental Concepts of Hydrogels: Synthesis, Properties, and Their Applications. Polymers 2020, 12, 2702. [Google Scholar] [CrossRef]
- Chamkouri, H. A Review of Hydrogels, Their Properties and Applications in Medicine. Am. J. Biomed. Sci. Res. 2021, 11, 485–493. [Google Scholar] [CrossRef]
- Annabi, N.; Tamayol, A.; Uquillas, J.A.; Akbari, M.; Bertassoni, L.E.; Cha, C.; Camci-Unal, G.; Dokmeci, M.R.; Peppas, N.A.; Khademhosseini, A. 25th Anniversary Article: Rational Design and Applications of Hydrogels in Regenerative Medicine. Adv. Mater. 2014, 26, 85–124. [Google Scholar] [CrossRef]
- Thiele, J.; Ma, Y.; Bruekers, S.M.C.; Ma, S.; Huck, W.T.S. 25th Anniversary Article: Designer Hydrogels for Cell Cultures: A Materials Selection Guide. Adv. Mater. 2014, 26, 125–148. [Google Scholar] [CrossRef]
- Yue, K.; Trujillo-de Santiago, G.; Alvarez, M.M.; Tamayol, A.; Annabi, N.; Khademhosseini, A. Synthesis, Properties, and Biomedical Applications of Gelatin Methacryloyl (GelMA) Hydrogels. Biomaterials 2015, 73, 254–271. [Google Scholar] [CrossRef]
- Luo, Y.; Shoichet, M.S. A Photolabile Hydrogel for Guided Three-Dimensional Cell Growth and Migration. Nat. Mater. 2004, 3, 249–254. [Google Scholar] [CrossRef]
- West, J.L. Protein-Patterned Hydrogels: Customized Cell Microenvironments. Nat. Mater. 2011, 10, 727–729. [Google Scholar] [CrossRef]
- Anderson, J.M.; Langone, J.J. Issues and Perspectives on the Biocompatibility and Immunotoxicity Evaluation of Implanted Controlled Release Systems. J. Control. Release 1999, 57, 107–113. [Google Scholar] [CrossRef]
- Khare, A.R.; Peppas, N.A. Swelling/Deswelling of Anionic Copolymer Gels. Biomaterials 1995, 16, 559–567. [Google Scholar] [CrossRef]
- Sun, W.; Starly, B.; Daly, A.C.; Burdick, J.A.; Groll, J.; Skeldon, G.; Shu, W.; Sakai, Y.; Shinohara, M.; Nishikawa, M.; et al. The Bioprinting Roadmap. Biofabrication 2020, 12, 022002. [Google Scholar] [CrossRef]
- Gulrez, S.K.; Al-Assaf, S.; Phillips, G.O. Hydrogels: Methods of Preparation, Characterisation and Applications. Prog. Mol. Environ. Bioeng. Anal. Model. Technol. Appl. 2011, 5, 117–150. [Google Scholar] [CrossRef]
- Bootsma, K.; Fitzgerald, M.M.; Free, B.; Dimbath, E.; Conjerti, J.; Reese, G.; Konkolewicz, D.; Berberich, J.A.; Sparks, J.L. 3D Printing of an Interpenetrating Network Hydrogel Material with Tunable Viscoelastic Properties. J. Mech. Behav. Biomed. Mater. 2017, 70, 84–94. [Google Scholar] [CrossRef]
- Chaudhary, S.; Chakraborty, E. Hydrogel Based Tissue Engineering and Its Future Applications in Personalized Disease Modeling and Regenerative Therapy. Beni-Suef Univ. J. Basic Appl. Sci. 2022, 11, 3. [Google Scholar] [CrossRef]
- Dubey, N.K.; Deng, W.-P. Polymeric Gels for Cartilage Tissue Engineering. In Polymeric Gels; Woodhead Publishing: Sawston, UK, 2018; pp. 505–525. [Google Scholar] [CrossRef]
- Kirchmajer, D.M.; Gorkin, R.; In Het Panhuis, M. An Overview of the Suitability of Hydrogel-Forming Polymers for Extrusion-Based 3D-Printing. J. Mater. Chem. B 2015, 3, 4105–4117. [Google Scholar] [CrossRef]
- Rastogi, P.; Kandasubramanian, B. Review of Alginate-Based Hydrogel Bioprinting for Application in Tissue Engineering. Biofabrication 2019, 11, 042001. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, B.V.; Khurshid, S.S.; Fisher, O.Z.; Khademhosseini, A.; Peppas, N.A. Hydrogels in Regenerative Medicine. Adv. Mater. 2009, 21, 3307–3329. [Google Scholar] [CrossRef] [PubMed]
- Chimene, D.; Lennox, K.K.; Kaunas, R.R.; Gaharwar, A.K. Advanced Bioinks for 3D Printing: A Materials Science Perspective. Ann. Biomed. Eng. 2016, 44, 2090–2102. [Google Scholar] [CrossRef] [PubMed]
- Antich, C.; de Vicente, J.; Jiménez, G.; Chocarro, C.; Carrillo, E.; Montañez, E.; Gálvez-Martín, P.; Marchal, J.A. Bio-Inspired Hydrogel Composed of Hyaluronic Acid and Alginate as a Potential Bioink for 3D Bioprinting of Articular Cartilage Engineering Constructs. Acta Biomater. 2020, 106, 114–123. [Google Scholar] [CrossRef]
- Jiao, W.; Li, X.; Shan, J.; Wang, X. Study of Several Alginate-Based Hydrogels for In Vitro 3D Cell Cultures. Gels 2022, 8, 147. [Google Scholar] [CrossRef]
- Habib, A.; Sathish, V.; Mallik, S.; Khoda, B. 3D Printability of Alginate-Carboxymethyl Cellulose Hydrogel. Materials 2018, 11, 454. [Google Scholar] [CrossRef]
- Hennink, W.E.; Van Nostrum, C.F. Novel Crosslinking Methods to Design Hydrogels. Adv. Drug Deliv. Rev. 2002, 54, 13–36. [Google Scholar] [CrossRef]
- Rosiak, J.M.; Yoshii, F. Hydrogels and Their Medical Applications. Nucl. Instrum. Methods Phys. Res. B 1999, 151, 56–64. [Google Scholar] [CrossRef]
- Hoffman, A.S. Hydrogels for Biomedical Applications. Adv. Drug. Deliv. Rev. 2002, 54, 3–12. [Google Scholar] [CrossRef]
- Szepes, A.; Makai, Z.; Blümer, C.; Mäder, K.; Kása, P.; Szabó-Révész, P. Characterization and Drug Delivery Behaviour of Starch-Based Hydrogels Prepared via Isostatic Ultrahigh Pressure. Carbohydr. Polym. 2008, 72, 571–578. [Google Scholar] [CrossRef]
- Esteban, C.; Severian, D. Polyionic Hydrogels Based on Xanthan and Chitosan for Stabilising and Controlled Release of Vitamins; Kemestrie Inc.: Sherbrooke, CA, USA, 1999; Available online: https://patents.google.com/patent/EP1098931B1/en (accessed on 7 June 2023).
- Takigami, M.; Amada, H.; Nagasawa, N.; Yagi, T.; Kasahara, T.; Takigami, S.; Tamada, M. Preparation and Properties of CMC Gel. Trans. Mater. Res. Soc. Jpn. 2007, 32, 713–716. [Google Scholar] [CrossRef]
- Kim, Y.H.; Priyadarshi, R.; Kim, J.-W.; Kim, J.; Alekseev, D.G.; Rhim, J.-W. 3D-Printed Pectin/Carboxymethyl Cellulose/ZnO Bio-Inks: Comparative Analysis with the Solution Casting Method. Polymers 2022, 14, 4711. [Google Scholar] [CrossRef]
- Giannouli, P.; Morris, E.R. Cryogelation of Xanthan. Food Hydrocoll. 2003, 17, 495–501. [Google Scholar] [CrossRef]
- Nikolaos, A.; Peppas, J.; Scott, E. Scott. Controlled release from poly (vinyl alcohol) gels prepared by freezing-thawing processes. J. Control. Release 1992, 18, 95–100. [Google Scholar] [CrossRef]
- Lugao, A.B.; Malmonge, S.M. Use of Radiation in the Production of Hydrogels. Nucl. Instrum. Methods Phys. Res. B 2001, 185, 37–42. [Google Scholar] [CrossRef]
- Funami, T.; Hiroe, M.; Noda, S.; Asai, I.; Ikeda, S.; Nishinari, K. Influence of Molecular Structure Imaged with Atomic Force Microscopy on the Rheological Behavior of Carrageenan Aqueous Systems in the Presence or Absence of Cations. Food Hydrocoll. 2007, 21, 617–629. [Google Scholar] [CrossRef]
- Guo, B.L.; Gao, Q.Y. Preparation and Properties of a PH/Temperature-Responsive Carboxymethyl Chitosan/Poly(N-Isopropylacrylamide)Semi-IPN Hydrogel for Oral Delivery of Drugs. Carbohydr. Res. 2007, 342, 2416–2422. [Google Scholar] [CrossRef]
- Schuetz, Y.B.; Gurny, R.; Jordan, O. A Novel Thermoresponsive Hydrogel Based on Chitosan. Eur. J. Pharm. Biopharm. 2008, 68, 19–25. [Google Scholar] [CrossRef]
- Knudson, C.B. Hyaluronan and CD44: Strategic Players for Cell-Matrix Interactions during Chondrogenesis and Matrix Assembly. Birth Defects Res. C Embryo Today 2003, 69, 174–196. [Google Scholar] [CrossRef]
- Jammalamadaka, U.; Tappa, K. Recent Advances in Biomaterials for 3D Printing and Tissue Engineering. J. Funct. Biomater. 2018, 9, 22. [Google Scholar] [CrossRef]
- Demirtaş, T.T.; Irmak, G.; Gümüşderelioǧlu, M. A Bioprintable Form of Chitosan Hydrogel for Bone Tissue Engineering. Biofabrication 2017, 9, 035003. [Google Scholar] [CrossRef] [PubMed]
- Jia, J.; Richards, D.J.; Pollard, S.; Tan, Y.; Rodriguez, J.; Visconti, R.P.; Trusk, T.C.; Yost, M.J.; Yao, H.; Markwald, R.R.; et al. Engineering Alginate as Bioink for Bioprinting. Acta Biomater. 2014, 10, 4323–4331. [Google Scholar] [CrossRef] [PubMed]
- Raza, M.H.; Abdullah, M.; Rehman, M.U.; Mubarak, Z.; Arshad, M. Development of An Extrusion 3D Bioprinter for Bioprinting of Hydrogel Based Biomaterials. In Proceedings of the 2019 International Conference on Robotics and Automation in Industry, Montreal, QC, Canada, 20–24 May 2019. [Google Scholar] [CrossRef]
- Dravid, A.; McCaughey-Chapman, A.; Raos, B.; O’Carroll, S.J.; Connor, B.; Svirskis, D. Development of Agarose-Gelatin Bioinks for Extrusion-Based Bioprinting and Cell Encapsulation. Biomed. Mater. 2022, 17, 055001. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, R.; Orgill, D.P.; Murphy, G.F.; Mizuno, S. Hydrostatic Pressure-Driven Three-Dimensional Cartilage Induction Using Human Adipose-Derived Stem Cells and Collagen Gels. Tissue Eng. Part. A 2015, 21, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, T.; Kajave, N.; Cai, H.H.; Gu, L.; Albanna, M.; Kishore, V. In Vitro Characterization of Xeno-Free Clinically Relevant Human Collagen and Its Applicability in Cell-Laden 3D Bioprinting. J. Biomater. Appl. 2021, 35, 912–923. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.C.J.; Lim, K.S.; Farrugia, B.L.; Hooper, G.J.; Woodfield, T.B.F. Covalent Incorporation of Heparin Improves Chondrogenesis in Photocurable Gelatin-Methacryloyl Hydrogels. Macromol. Biosci. 2017, 17, 1700158. [Google Scholar] [CrossRef]
- Kim, S.; Fan, J.; Lee, C.S.; Chen, C.; Bubukina, K.; Lee, M. Heparinized Chitosan Stabilizes the Bioactivity of BMP-2 and Potentiates the Osteogenic Efficacy of Demineralized Bone Matrix. J. Biol. Eng. 2020, 14, 6. [Google Scholar] [CrossRef]
- Dare, E.V.; Griffith, M.; Poitras, P.; Wang, T.; Dervin, G.F.; Giulivi, A.; Hincke, M.T. Fibrin Sealants from Fresh or Fresh/Frozen Plasma as Scaffolds for in Vitro Articular Cartilage Regeneration. Tissue Eng. Part A 2009, 15, 2285–2297. [Google Scholar] [CrossRef]
- Van Susante, J.L.C.; Buma, P.; Schuman, L.; Homminga, G.N.; Van Den Berg, W.B.; Veth, R.P.H. Resurfacing Potential of Heterologous Chondrocytes Suspended in Fibrin Glue in Large Full-Thickness Defects of Femoral Articular Cartilage: An Experimental Study in the Goat. Biomaterials 1999, 20, 1167–1175. [Google Scholar] [CrossRef]
- Cai, W.; Gupta, R.B. Hydrogels. In Kirk-Otmer Encyclopedia of Chemical Technology; John Wiley & Sons: Hoboken, NJ, USA, 2012; Volume 13, pp. 729–759. [Google Scholar]
- Vassallo, V.; Tsianaka, A.; Alessio, N.; Grübel, J.; Cammarota, M.; Tovar, G.E.M.; Southan, A.; Schiraldi, C. Evaluation of novel biomaterials for cartilage regeneration based on gelatin methacryloyl interpenetrated with extractive chondroitin sulfate or unsulfated biotechnological chondroitin. J. Biomed. Mater. Res. A 2022, 110, 1210–1223. [Google Scholar] [CrossRef]
- Miyata, T.; Taira, T.; Noishiki, Y. Collagen Engineering for Biomaterial Use. Clin. Mater. 1992, 9, 139–148. [Google Scholar] [CrossRef]
- Seidlits, S.K.; Drinnan, C.T.; Petersen, R.R.; Shear, J.B.; Suggs, L.J.; Schmidt, C.E. Fibronectin-Hyaluronic Acid Composite Hydrogels for Three-Dimensional Endothelial Cell Culture. Acta Biomater. 2011, 7, 2401–2409. [Google Scholar] [CrossRef]
- Yusova, A.A.; Gusev, I.V.; Lipatova, I.M. Properties of hydrogels based on mixtures of sodium alginate with other polysaccharides of natural origin. Chem. Plant Raw Mater. 2014, 4, 59–66. Available online: https://cyberleninka.ru/article/n/svoystva-gidrogeley-na-osnove-smesey-alginata-natriya-s-drugimi-polisaharidami-prirodnogo-proishozhdeniya (accessed on 7 June 2023).
- Trujillo, S.; Seow, M.; Lueckgen, A.; Salmeron-Sanchez, M.; Cipitria, A. Dynamic Mechanical Control of Alginate-Fibronectin Hydrogels with Dual Crosslinking: Covalent and Ionic. Polymers 2021, 13, 433. [Google Scholar] [CrossRef]
- Perdisa, F.; Gostyńska, N.; Roffi, A.; Filardo, G.; Marcacci, M.; Kon, E. Adipose-Derived Mesenchymal Stem Cells for the Treatment of Articular Cartilage: A Systematic Review on Preclinical and Clinical Evidence. Stem Cells Int. 2015, 2015, 597652. [Google Scholar] [CrossRef]
- Ferreira, A.M.; Gentile, P.; Chiono, V.; Ciardelli, G. Collagen for Bone Tissue Regeneration. Acta Biomater. 2012, 8, 3191–3200. [Google Scholar] [CrossRef]
- Gelse, K.; Pöschl, E.; Aigner, T. Collagens-Structure, Function, and Biosynthesis. Adv. Drug Deliv. Rev. 2003, 55, 1531–1546. [Google Scholar] [CrossRef]
- Agapova, O.I. Scanning Probe Nanotomography for Studying 3D Structure of Matrixes for Tissue Engineering and Regenerative Medicine: Abstract of Dissertation … D. in Biology: 14.01.24/Agapova Olga Igorevna; Federal Research Center for Transplantology and Artificial Organs of Acad. V.I. Shumakov: Moscow, Russia, 2015; Volume 159, Available online: https://transpl.ru/files/agapova/dissertation.pdf (accessed on 26 November 2022).
- Markel, M.D.; Hayashi, K.; Thabit, G. Basic Properties of Collagen Shrinkage and Laser-Collagen Interactions. In Lasers in the Musculoskeletal System; Springer: Berlin/Heidelberg, Germany, 2001; pp. 162–169. [Google Scholar] [CrossRef]
- Dawson, J.; Schussler, O.; Al-Madhoun, A.; Menard, C.; Ruel, M.; Skerjanc, I.S. Collagen Scaffolds with or without the Addition of RGD Peptides Support Cardiomyogenesis after Aggregation of Mouse Embryonic Stem Cells. Vitr. Cell Dev. Biol. Anim. 2011, 47, 653–664. [Google Scholar] [CrossRef]
- Chaisri, P.; Chingsungnoen, A.; Siri, S. Repetitive Gly-Leu-Lys-Gly-Glu-Asn-Arg-Gly-Asp Peptide Derived from Collagen and Fibronectin for Improving Cell-Scaffold Interaction. Appl. Biochem. Biotechnol. 2015, 175, 2489–2500. [Google Scholar] [CrossRef]
- Brodsky, B.; Eikenberry, E.F. Characterization of Fibrous Forms of Collagen. Methods Enzym. 1982, 82, 127–174. [Google Scholar] [CrossRef]
- Glowacki, J.; Mizuno, S. Collagen Scaffolds for Tissue Engineering. Biopolymers 2008, 89, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Werkmeister, J.; Edwards, G.; Ramshaw, J. Collagen-Based Vascular Prostheses. In Biomaterials Engineering and Devices: Human Applications; Humana Press: Totowa, NJ, USA, 2000. [Google Scholar]
- Bhat, S.V. Cardiovascular Implants and Extracorporeal Devices. In Biomaterials; Springer: Dordrecht, The Netherlands, 2002; pp. 130–162. [Google Scholar] [CrossRef]
- Kretzschmar, M.; Bieri, O.; Miska, M.; Wiewiorski, M.; Hainc, N.; Valderrabano, V.; Studler, U. Characterization of the Collagen Component of Cartilage Repair Tissue of the Talus with Quantitative MRI: Comparison of T2 Relaxation Time Measurements with a Diffusion-Weighted Double-Echo Steady-State Sequence (DwDESS). Eur. Radiol. 2015, 25, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Togo, S.; Sato, T.; Sugiura, H.; Wang, X.; Basma, H.; Nelson, A.; Liu, X.; Bargar, T.W.; Sharp, J.G.; Rennard, S.I. Differentiation of Embryonic Stem Cells into Fibroblast-like Cells in Three-Dimensional Type I Collagen Gel Cultures. Vitr. Cell Dev. Biol. Anim. 2011, 47, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Mochalov, K.E.; Efimov, A.E.; Bobrovsky, A.; Agapov, I.I.; Chistyakov, A.A.; Oleinikov, V.; Sukhanova, A.; Nabiev, I. Combined Scanning Probe Nanotomography and Optical Microspectroscopy: A Correlative Technique for 3D Characterization of Nanomaterials. ACS Nano 2013, 7, 8953–8962. [Google Scholar] [CrossRef] [PubMed]
- Ji, S.; Guvendiren, M. Recent Advances in Bioink Design for 3D Bioprinting of Tissues and Organs. Front. Bioeng. Biotechnol. 2017, 5, 23. [Google Scholar] [CrossRef] [PubMed]
- Khotimchenko, Y.S.; Kovalev, V.V.; Savchenko, O.V.; Ziganshina, O.A. Physical–Chemical Properties, Physiological Activity, and Usage of Alginates, the Polysaccharides of Brown Algae. Russ. J. Marine Biol. 2001, 27, S53–S64. [Google Scholar] [CrossRef]
- Osidak, E.O.; Kozhukhov, V.I.; Osidak, M.S.; Domogatsky, S.P. Collagen as Bioink for Bioprinting: A Comprehensive Review. Int. J. Bioprint. 2020, 6, 270. [Google Scholar] [CrossRef]
- Eyre, D. Collagen of Articular Cartilage. Arthritis Res. 2002, 4, 30–35. [Google Scholar] [CrossRef]
- Lee, C.R.; Grodzinsky, A.J.; Spector, M. The Effects of Cross-Linking of Collagen-Glycosaminoglycan Scaffolds on Compressive Stiffness, Chondrocyte-Mediated Contraction, Proliferation and Biosynthesis. Biomaterials 2001, 22, 3145–3154. [Google Scholar] [CrossRef]
- Lu, Z.; Doulabi, B.Z.; Huang, C.; Bank, R.A.; Helder, M.N. Collagen Type II Enhances Chondrogenesis in Adipose Tissue-Derived Stem Cells by Affecting Cell Shape. Tissue Eng. Part A 2010, 16, 81–90. [Google Scholar] [CrossRef]
- Chai, Q.; Jiao, Y.; Yu, X. Hydrogels for Biomedical Applications: Their Characteristics and the Mechanisms behind Them. Gels 2017, 3, 6. [Google Scholar] [CrossRef]
- Safonova, M.A.; Antonova, D.S. Basic types of gelatin and its application in the food industry. Bull. Master Degree 2017, 11, 74. Available online: https://cyberleninka.ru/article/n/osnovnye-vidy-zhelatina-i-ego-primenenie-v-pischevoy-promyshlennosti (accessed on 7 June 2023).
- Sokolova, N.A.; Kochetkov, V.G.; Novopoltseva, O.M.; Kablov, V.F. Chemistry of Biopolymers. VolgGTU VPI (Branch). Electronic Text Data. Volzhsky. 2018. Available online: http://lib.volpi.ru (accessed on 26 November 2022).
- Van den Steen, P.E.; Dubois, B.; Nelissen, I.; Rudd, P.M.; Dwek, R.A.; Opdenakker, G. Biochemistry and molecular biology of gelatinase B or matrix metalloproteinase-9 (MMP-9). Crit. Rev. Biochem. Mol. Biol. 2002, 37, 375–536. [Google Scholar] [CrossRef]
- Gorgieva, S.; Kokol, V. Collagen- vs. Gelatine-Based Biomaterials and Their Biocompatibility: Review and Perspectives. Biomater. Appl. Nanomed. 2011, 2, 17–52. [Google Scholar] [CrossRef]
- Maurer, P.H., II. Antigenicity of Gelatin in Rabbits and Other Species. J. Exp. Med. 1954, 100, 515–523. [Google Scholar] [CrossRef]
- Aubin, H.; Nichol, J.W.; Hutson, C.B.; Bae, H.; Sieminski, A.L.; Cropek, D.M.; Akhyari, P.; Khademhosseini, A. Directed 3D Cell Alignment and Elongation in Microengineered Hydrogels. Biomaterials 2010, 31, 6941–6951. [Google Scholar] [CrossRef]
- Djabourov, M.; Papon, P. Influence of Thermal Treatments on the Structure and Stability of Gelatin Gels. Polymer 1983, 24, 537–542. [Google Scholar] [CrossRef]
- Nichol, J.W.; Koshy, S.T.; Bae, H.; Hwang, C.M.; Yamanlar, S.; Khademhosseini, A. Cell-Laden Microengineered Gelatin Methacrylate Hydrogels. Biomaterials 2010, 31, 5536–5544. [Google Scholar] [CrossRef]
- Van Den Bulcke, A.I.; Bogdanov, B.; De Rooze, N.; Schacht, E.H.; Cornelissen, M.; Berghmans, H. Structural and Rheological Properties of Methacrylamide Modified Gelatin Hydrogels. Biomacromolecules 2000, 1, 31–38. [Google Scholar] [CrossRef]
- Naumov, V.S. Dissolution and Diffusion of Chitosan in Aqueous Medium and Its Coordination with Insulin: A Molecular Dynamic Study: Dissertation … D. in Chemistry: 02.00.04/Naumov Vladimir Sergeevich; Federal State Educational Institution of Higher Professional Education, National Research Nizhny Novgorod State University, N.I. Lobachevsky: Nizhny Novgorod, Russia, 2019; p. 127. Available online: https://diss.unn.ru/files/2019/1002/diss-Naumov-1002.pdf (accessed on 7 June 2023).
- Velasco, D.; Tumarkin, E.; Kumacheva, E. Microfluidic Encapsulation of Cells in Polymer Microgels. Small 2012, 8, 1633–1642. [Google Scholar] [CrossRef]
- Workshop on Marine Algae Biotechnology: Summary Report, Indonesian National Research Council National Research Council (U.S.). Office of International Affairs. 1985. Available online: https://books.google.ru/books?id=YHMrAAAAYAAJ (accessed on 7 June 2023).
- Normand, V.; Lootens, D.L.; Amici, E.; Plucknett, K.P.; Aymard, P. New Insight into Agarose Gel Mechanical Properties. Biomacromolecules 2000, 1, 730–738. [Google Scholar] [CrossRef] [PubMed]
- Mauck, R.L.; Soltz, M.A.; Wang, C.C.B.; Wong, D.D.; Chao, P.H.G.; Valhmu, W.B.; Hung, C.T.; Ateshian, G.A. Functional Tissue Engineering of Articular Cartilage through Dynamic Loading of Chondrocyte-Seeded Agarose Gels. J. Biomech. Eng. 2000, 122, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Serwer, P. Agarose Gels: Properties and Use for Electrophoresis. Electrophoresis 1983, 4, 375–382. [Google Scholar] [CrossRef]
- Bougault, C.; Paumier, A.; Aubert-Foucher, E.; Mallein-Gerin, F. Investigating Conversion of Mechanical Force into Biochemical Signaling in Three-Dimensional Chondrocyte Cultures. Nat. Protoc. 2009, 4, 928–938. [Google Scholar] [CrossRef] [PubMed]
- Chang, F.; Ishii, T.; Yanai, T.; Mishima, H.; Akaogi, H.; Ogawa, T.; Ochiai, N. Repair of Large Full-Thickness Articular Cartilage Defects by Transplantation of Autologous Uncultured Bone-Marrow-Derived Mononuclear Cells. J. Orthop. Res. 2008, 26, 18–26. [Google Scholar] [CrossRef]
- Vasiliev, S.A.; Gorgidze, L.A.; Efremov, E.E.; Belinin, G.Y.; Moiseeva, T.N.; Al-Radi, L.S.; Sokolova, M.A.; Guria, G.T.; Zozulya, N.I.; Kokhno, A.V. Fibronectin: Structure, function, clinical significance. Atherothrombosis 2022, 1, 138–158. Available online: https://cyberleninka.ru/article/n/fibronektin-struktura-funktsii-klinicheskaya-znachimost-obzor (accessed on 7 June 2023). [CrossRef]
- Pankov, R.; Yamada, K.M. Fibronectin at a Glance. J. Cell Sci. 2002, 115, 3861–3863. [Google Scholar] [CrossRef]
- Maxson, S.; Lopez, E.A.; Yoo, D.; Danilkovitch-Miagkova, A.; LeRoux, M.A. Concise Review: Role of Mesenchymal Stem Cells in Wound Repair. Stem Cells Transl. Med. 2012, 1, 142–149. [Google Scholar] [CrossRef]
- Natal, C.; Osés-Prieto, J.A.; Pelacho, B.; Iraburu, M.J.; López-Zabalza, M.J. Regulation of Apoptosis by Peptides of Fibronectin in Human Monocytes. Apoptosis 2006, 11, 209–219. [Google Scholar] [CrossRef]
- Trujillo, S.; Gonzalez-Garcia, C.; Rico, P.; Reid, A.; Windmill, J.; Dalby, M.J.; Salmeron-Sanchez, M. Engineered 3D Hydrogels with Full-Length Fibronectin That Sequester and Present Growth Factors. Biomaterials 2020, 252, 120104. [Google Scholar] [CrossRef]
- To, W.S.; Midwood, K.S. Plasma and Cellular Fibronectin: Distinct and Independent Functions during Tissue Repair. Fibrogenesis Tissue Repair 2011, 4. [Google Scholar] [CrossRef]
- Leahy, D.J.; Aukhil, I.; Erickson, H.P. 2.0 A Crystal Structure of a Four-Domain Segment of Human Fibronectin Encompassing the RGD Loop and Synergy Region. Cell 1996, 84, 155–164. [Google Scholar] [CrossRef]
- Hynes, R.O. Introduction and Historical Overview. In Fibronectins; Springer: New York, NY, USA, 1990; pp. 1–6. [Google Scholar] [CrossRef]
- Kapila, Y.L.; Lancero, H.; Johnson, P.W. The Response of Periodontal Ligament Cells to Fibronectin. J. Periodontol. 1998, 69, 1008–1019. [Google Scholar] [CrossRef]
- Martino, M.M.; Tortelli, F.; Mochizuki, M.; Traub, S.; Ben-David, D.; Kuhn, G.A.; Müller, R.; Livne, E.; Eming, S.A.; Hubbell, J.A. Engineering the Growth Factor Microenvironment with Fibronectin Domains to Promote Wound and Bone Tissue Healing. Sci. Transl. Med. 2011, 3, 100ra89. [Google Scholar] [CrossRef]
- Fayet, C.; Bendeck, M.P.; Gotlieb, A.I. Cardiac Valve Interstitial Cells Secrete Fibronectin and Form Fibrillar Adhesions in Response to Injury. Cardiovasc. Pathol. 2007, 16, 203–211. [Google Scholar] [CrossRef]
- Lai, Y.H.; Wang, H.Z.; Lin, C.P.; Hong, S.J.; Chang, S.J. Endothelin-1 Enhances Corneal Fibronectin Deposition and Promotes Corneal Epithelial Wound Healing after Photorefractive Keratectomy in Rabbits. Kaohsiung J. Med. Sci. 2008, 24, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Luomanen, M.; Virtanen, I. Fibronectins in Healing Incision, Excision and Laser Wounds. J. Oral. Pathol. Med. 1991, 20, 133–138. [Google Scholar] [CrossRef]
- Lefcort, F.; Venstrom, K.; McDonald, J.A.; Reichardt, L.F. Regulation of Expression of Fibronectin and Its Receptor, Alpha 5 Beta 1, during Development and Regeneration of Peripheral Nerve. Development 1992, 116, 767–782. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, W.; Yang, M. Application of Hydrogels in Cartilage Tissue Engineering. Curr. Stem Cell Res. 2018, 13, 497–516. [Google Scholar] [CrossRef]
- Alexander, A.; Ajazuddin; Khan, J.; Saraf, S.; Saraf, S. Poly(Ethylene Glycol)-Poly(Lactic-Co-Glycolic Acid) Based Thermosensitive Injectable Hydrogels for Biomedical Applications. J. Control. Release 2013, 172, 715–729. [Google Scholar] [CrossRef]
- Zhao, X.; Papadopoulos, A.; Ibusuki, S.; Bichara, D.A.; Saris, D.B.; Malda, J.; Anseth, K.S.; Gill, T.J.; Randolph, M.A. Articular Cartilage Generation Applying PEG-LA-DM/PEGDM Copolymer Hydrogels. BMC Musculoskelet. Disord. 2016, 17, 245. [Google Scholar] [CrossRef] [PubMed]
- Peppas, N.A.; Merrill, E.W. Development of Semicrystalline Poly(Vinyl Alcohol) Hydrogels for Biomedical Applications. J. Biomed. Mater. Res. 1977, 11, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Bodugoz-Senturk, H.; Macias, C.E.; Kung, J.H.; Muratoglu, O.K. Poly(Vinyl Alcohol)-Acrylamide Hydrogels as Load-Bearing Cartilage Substitute. Biomaterials. 2009, 30, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Mansur, H.S.; Sadahira, C.M.; Souza, A.N.; Mansur, A.A.P. FTIR Spectroscopy Characterization of Poly (Vinyl Alcohol) Hydrogel with Different Hydrolysis Degree and Chemically Crosslinked with Glutaraldehyde. Mater. Sci. Eng. C 2008, 28, 539–548. [Google Scholar] [CrossRef]
- Wang, B.; Mukataka, S.; Kokufuta, E.; Kodama, M. The Influence of Polymer Concentration on the Radiation-Chemical Yield of Intermolecular Crosslinking of Poly(Vinyl Alcohol) by γ-Rays in Deoxygenated Aqueous Solution. Radiat. Phys. Chem. 2000, 59, 91–95. [Google Scholar] [CrossRef]
- Bray, J.C.; Merrill, E.W. Poly(Vinyl Alcohol) Hydrogels for Synthetic Articular Cartilage Material. J. Biomed. Mater. Res. 1973, 7, 431–443. [Google Scholar] [CrossRef]
- Chen, Y.N.; Peng, L.; Liu, T.; Wang, Y.; Shi, S.; Wang, H. Poly(Vinyl Alcohol)-Tannic Acid Hydrogels with Excellent Mechanical Properties and Shape Memory Behaviors. ACS Appl. Mater. Interfaces 2016, 8, 27199–27206. [Google Scholar] [CrossRef]
- Maher, S.A.; Doty, S.B.; Torzilli, P.A.; Thornton, S.; Lowman, A.M.; Thomas, J.D.; Warren, R.; Wright, T.M.; Myers, E. Nondegradable Hydrogels for the Treatment of Focal Cartilage Defects. J. Biomed. Mater. Res. A 2007, 83, 145–155. [Google Scholar] [CrossRef]
- Spiller, K.L.; Holloway, J.L.; Gribb, M.E.; Lowman, A.M. Design of Semi-Degradable Hydrogels Based on Poly(Vinyl Alcohol) and Poly(Lactic-Co-Glycolic Acid) for Cartilage Tissue Engineering. J. Tissue Eng. Regen. Med. 2011, 5, 636–647. [Google Scholar] [CrossRef]
- Makadia, H.K.; Siegel, S.J. Poly Lactic-Co-Glycolic Acid (PLGA) as Biodegradable Controlled Drug Delivery Carrier. Polymers 2011, 3, 1377–1397. [Google Scholar] [CrossRef]
- Yang, Y.Y.; Chung, T.S.; Ping Ng, N. Morphology, Drug Distribution, and in Vitro Release Profiles of Biodegradable Polymeric Microspheres Containing Protein Fabricated by Double-Emulsion Solvent Extraction/Evaporation Method. Biomaterials 2001, 22, 231–241. [Google Scholar] [CrossRef]
- Weber, F.E.; Eyrich, G.; Grätz, K.W.; Maly, F.E.; Sailer, H.F. Slow and Continuous Application of Human Recombinant Bone Morphogenetic Protein via Biodegradable Poly(Lactide-Co-Glycolide) Foamspheres. Int. J. Oral. Maxillofac. Surg. 2002, 31, 60–65. [Google Scholar] [CrossRef]
- Tang, Y.; Wang, H.; Sun, Y.; Jiang, Y.; Fang, S.; Kan, Z.; Lu, Y.; Liu, S.; Zhou, X.; Li, Z. Using Platelet-Rich Plasma Hydrogel to Deliver Mesenchymal Stem Cells into Three-Dimensional PLGA Scaffold for Cartilage Tissue Engineering. ACS Appl. Bio. Mater. 2021, 4, 8607–8614. [Google Scholar] [CrossRef]
- Basu, A.; Kunduru, K.R.; Doppalapudi, S.; Domb, A.J.; Khan, W. Poly(Lactic Acid) Based Hydrogels. Adv. Drug Deliv. Rev. 2016, 107, 192–205. [Google Scholar] [CrossRef]
- Issabayeva, Z.; Shishkovsky, I. Prediction of The Mechanical Behavior of Polylactic Acid Parts with Shape Memory Effect Fabricated by FDM. Polymers 2023, 15, 1162. [Google Scholar] [CrossRef]
- Shen, J.; Zhang, H.; Zhu, J.; Ma, Y.; He, H.; Zhu, F.; Jia, L.; Zheng, Q. Simple Preparation of a Waterborne Polyurethane Crosslinked Hydrogel Adhesive with Satisfactory Mechanical Properties and Adhesion Properties. Front. Chem. 2022, 10, 855352. [Google Scholar] [CrossRef]
- Backes, E.H.; Harb, S.V.; Beatrice, C.A.G.; Shimomura, K.M.B.; Passador, F.R.; Costa, L.C.; Pessan, L.A. Polycaprolactone Usage in Additive Manufacturing Strategies for Tissue Engineering Applications: A Review. J. Biomed. Mater. Res. B Appl. Biomater. 2022, 110, 1479–1503. [Google Scholar] [CrossRef]
- Park, K.M.; Lee, S.Y.; Joung, Y.K.; Na, J.S.; Lee, M.C.; Park, K.D. Thermosensitive Chitosan-Pluronic Hydrogel as an Injectable Cell Delivery Carrier for Cartilage Regeneration. Acta Biomater. 2009, 5, 1956–1965. [Google Scholar] [CrossRef]
- Chen, W.; Xu, Y.; Liu, Y.; Wang, Z.; Li, Y.; Jiang, G.; Mo, X.; Zhou, G. Three-Dimensional Printed Electrospun Fiber-Based Scaffold for Cartilage Regeneration. Mater. Des. 2019, 179, 107886. [Google Scholar] [CrossRef]
- Kundu, J.; Shim, J.H.; Jang, J.; Kim, S.W.; Cho, D.W. An Additive Manufacturing-Based PCL-Alginate-Chondrocyte Bioprinted Scaffold for Cartilage Tissue Engineering. J. Tissue Eng. Regen. Med. 2015, 9, 1286–1297. [Google Scholar] [CrossRef]
- Shie, M.Y.; Chang, W.C.; Wei, L.J.; Huang, Y.H.; Chen, C.H.; Shih, C.T.; Chen, Y.W.; Shen, Y.F. 3D Printing of Cytocompatible Water-Based Light-Cured Polyurethane with Hyaluronic Acid for Cartilage Tissue Engineering Applications. Materials 2017, 10, 136. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.T.; Wysoczynski, K.; Hadley, D.J.; Silva, E.A. Computational-Based Design of Hydrogels with Predictable Mesh Properties. ACS Biomater. Sci. Eng. 2020, 6, 308–319. [Google Scholar] [CrossRef] [PubMed]
- Bhosale, A.M.; Richardson, J.B. Articular Cartilage: Structure, Injuries and Review of Management. Br. Med. Bull. 2008, 87, 77–95. [Google Scholar] [CrossRef] [PubMed]
- Marques, C.F.; Diogo, G.S.; Pina, S.; Oliveira, J.M.; Silva, T.H.; Reis, R.L. Collagen-Based Bioinks for Hard Tissue Engineering Applications: A Comprehensive Review. J. Mater. Sci. Mater. Med. 2019, 30, 32. [Google Scholar] [CrossRef]
- Fellows, C.R.; Matta, C.; Zakany, R.; Khan, I.M.; Mobasheri, A. Adipose, Bone Marrow and Synovial Joint-Derived Mesenchymal Stem Cells for Cartilage Repair. Front. Genet. 2016, 7, 213. [Google Scholar] [CrossRef]
- Zhao, S.; Wehner, R.; Bornhäuser, M.; Wassmuth, R.; Bachmann, M.; Schmitz, M. Immunomodulatory Properties of Mesenchymal Stromal Cells and Their Therapeutic Consequences for Immune-Mediated Disorders. Stem Cells Dev. 2010, 19, 607–614. [Google Scholar] [CrossRef]
- Dinescu, S.; Galateanu, B.; Radu, E.; Hermenean, A.; Lungu, A.; Stancu, I.C.; Jianu, D.; Tumbar, T.; Costache, M. A 3D Porous Gelatin-Alginate-Based-IPN Acts as an Efficient Promoter of Chondrogenesis from Human Adipose-Derived Stem Cells. Stem Cells Int. 2015, 2015, 252909. [Google Scholar] [CrossRef]
- Kazakova, V.S.; Chuev, V.P.; Novikov, O.O.; Zhilyakova, E.T.; Fadeeva, D.A. The use of growth factors in the restoration of bone tissue (review). Actual. Probl. Med. 2011, 4, 99. Available online: https://cyberleninka.ru/article/n/ispolzovanie-faktorov-rosta-v-vosstanovlenii-kostnoy-tkani-obzor (accessed on 7 June 2023).
- Pertungaro, P.S. The Use of Platelet-Rich Plasma with Growth Factors (Autologous Platelet Gel) to Improve Hard and Soft Tissue Healing During Bone Augmentation in the Area of the Pneumatized Sinus/P.S. Pertungaro. Available online: https://scholars.uthscsa.edu/en/publications/agarose-gels-properties-and-use-for-electrophoresis (accessed on 7 June 2023).
- Sarsenova, M.; Raimagambetov, Y.; Issabekova, A.; Karzhauov, M.; Kudaibergen, G.; Akhmetkarimova, Z.; Batpen, A.; Ramankulov, Y.; Ogay, V. Regeneration of Osteochondral Defects by Combined Delivery of Synovium-Derived Mesenchymal Stem Cells, TGF-Β1 and BMP-4 in Heparin-Conjugated Fibrin Hydrogel. Polymers 2022, 14, 5343. [Google Scholar] [CrossRef]
- Zhang, Q.; Liu, Y.; Li, J.; Wang, J.; Liu, C. Recapitulation of Growth Factor-Enriched Microenvironment via BMP Receptor Activating Hydrogel. Bioact. Mater. 2022, 20, 638–650. [Google Scholar] [CrossRef]
- Reddi, A.H. Bone Morphogenetic Proteins: From Basic Science to Clinical Applications. J. Bone Jt. Surg. Am. 2001, 83 (Suppl. 1), S1–S6. [Google Scholar] [CrossRef]
- Wozney, J.M.; Rosen, V. Bone Morphogenetic Protein and Bone Morphogenetic Protein Gene Family in Bone Formation and Repair. Clin. Orthop. Relat. Res. 1998, 346, 26–37. [Google Scholar] [CrossRef]
- Kudłacik-Kramarczyk, S.; Głąb, M.; Drabczyk, A.; Kordyka, A.; Godzierz, M.; Wróbel, P.S.; Krzan, M.; Uthayakumar, M.; Kędzierska, M.; Tyliszczak, B. Physicochemical Characteristics of Chitosan-Based Hydrogels Containing Albumin Particles and Aloe Vera Juice as Transdermal Systems Functionalized in the Viewpoint of Potential Biomedical Applications. Materials (Basel) 2021, 14, 5832. [Google Scholar] [CrossRef]
- Tamosaityte, S.; Galli, R.; Uckermann, O.; Sitoci-Ficici, K.H.; Later, R.; Beiermeister, R.; Doberenz, F.; Gelinsky, M.; Leipnitz, E.; Schackert, G.; et al. Biochemical Monitoring of Spinal Cord Injury by FT-IR Spectroscopy--Effects of Therapeutic Alginate Implant in Rat Models. PLoS ONE 2015, 10, e0142660. [Google Scholar] [CrossRef]
- Olăreț, E.; Bălănucă, B.; Onaș, A.M.; Ghițman, J.; Iovu, H.; Stancu, I.C.; Serafim, A. Double-Cross-Linked Networks Based on Methacryloyl Mucin. Polymers 2021, 13, 1706. [Google Scholar] [CrossRef]
- Kwak, S.; Lafleur, M. Raman Spectroscopy as a Tool for Measuring Mutual-Diffusion Coefficients in Hydrogels. Appl. Spectrosc. 2003, 57, 768–773. [Google Scholar] [CrossRef]
- Zhang, S. Discovery of the First Self-Assembling Peptide, Study of Peptide Dynamic Behaviors, and G Protein-Coupled Receptors Using an Aviv Circular Dichroism Spectropolarimeter. Biopolymers 2018, 109, e23235. [Google Scholar] [CrossRef]
- Ionita, G. Characterization and Tailoring the Properties of Hydrogels Using Spectroscopic Methods. In Emerging Concepts in Analysis and Applications of Hydrogels; Intech Open: London, UK, 2016; pp. 39–68. [Google Scholar] [CrossRef]
- Raeburn, J.; Cardoso, A.Z.; Adams, D.J. The Importance of the Self-Assembly Process to Control Mechanical Properties of Low Molecular Weight Hydrogels. Chem. Soc. Rev. 2013, 42, 5143–5156. [Google Scholar] [CrossRef]
- Sorber, J.; Steiner, G.; Schulz, V.; Guenther, M.; Gerlach, G.; Salzer, R.; Arndt, K.F. Hydrogel-Based Piezoresistive PH Sensors: Investigations Using FT-IR Attenuated Total Reflection Spectroscopic Imaging. Anal. Chem. 2008, 80, 2957–2962. [Google Scholar] [CrossRef]
- Rivero, R.; Alustiza, F.; Capella, V.; Liaudat, C.; Rodriguez, N.; Bosch, P.; Barbero, C.; Rivarola, C. Physicochemical Properties of Ionic and Non-Ionic Biocompatible Hydrogels in Water and Cell Culture Conditions: Relation with Type of Morphologies of Bovine Fetal Fibroblasts in Contact with the Surfaces. Colloids Surf. B Biointerfaces 2017, 158, 488–497. [Google Scholar] [CrossRef]
- Mather, M.L.; Tomlins, P.E. Hydrogels in Regenerative Medicine: Towards Understanding Structure-Function Relationships. Regen. Med. 2010, 5, 809–821. [Google Scholar] [CrossRef] [PubMed]
- Ou-Yang, L.; Zhu, L.; Ruan, Y.; Tang, H. Preparation of a Native β-Cyclodextrin Modified Plasmonic Hydrogel Substrate and Its Use as a Surface-Enhanced Raman Scattering Scaffold for Antibiotics Identification. J. Mater. Chem. C Mater. 2015, 3, 7575–7582. [Google Scholar] [CrossRef]
- Lauer, M.H.; Gehlen, M.H.; De Jesus, K.; Berlinck, R.G.S. Fluorescence Spectroscopy and Confocal Microscopy of the Mycotoxin Citrinin in Condensed Phase and Hydrogel Films. J. Fluoresc. 2014, 24, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Uguz, A. Book Review: Confocal and Two-Photon Microscopy: Foundations, Applications, and Advances, Edited by Alberto Diaspro. Ann. Biomed. Eng. 2002, 30, 984. [Google Scholar] [CrossRef]
- Dai, W.S.; Barbari, T.A. Characterization of Mesh Size Asymmetry in Hydrogel Membranes Using Confocal Microscopy. J. Memb. Sci. 2000, 171, 45–58. [Google Scholar] [CrossRef]
- Harper, D.E.; Pallazola, V.; Williams, D.A.; Harte, S.; Clauw, D.J.; Shtein, R.M. Confocal Microscopy Reveals Nerve Fiber Similarities in Fibromyalgia and Patients with Dry Eyes with a Normal Ophthalmic Exam. Mol. Pain 2014, 10, P2. [Google Scholar] [CrossRef]
- Nandi, R.; Yucknovsky, A.; Mazo, M.M.; Amdursky, N. Exploring the Inner Environment of Protein Hydrogels with Fluorescence Spectroscopy towards Understanding Their Drug Delivery Capabilities. J. Mater. Chem. B 2020, 8, 6964–6974. [Google Scholar] [CrossRef]
- Choudhury, D.; Anand, S.; Naing, M.W. The Arrival of Commercial Bioprinters–Towards 3D Bioprinting Revolution! Int. J. Bioprint. 2018, 4, 139. [Google Scholar] [CrossRef]
- Elemoso, A.; Shalunov, G.; Balakhovsky, Y.M.; Ostrovskiy, A.Y.; Khesuani, Y.D. 3D Bioprinting: The Roller Coaster Ride to Commercialization. Int. J. Bioprint. 2020, 6, 62–76. [Google Scholar] [CrossRef]
- Schwab, A.; Levato, R.; D’Este, M.; Piluso, S.; Eglin, D.; Malda, J. Printability and Shape Fidelity of Bioinks in 3D Bioprinting. Chem. Rev. 2020, 120, 11028–11055. [Google Scholar] [CrossRef]
- Miller, J.S.; Burdick, J.A. Editorial: Special Issue on 3D Printing of Biomaterials. ACS Biomater. Sci. Eng. 2016, 2, 1658–1661. [Google Scholar] [CrossRef]
- Malda, J.; Visser, J.; Melchels, F.P.; Jüngst, T.; Hennink, W.E.; Dhert, W.J.A.; Groll, J.; Hutmacher, D.W. 25th Anniversary Article: Engineering Hydrogels for Biofabrication. Adv. Mater. 2013, 25, 5011–5028. [Google Scholar] [CrossRef]
- Derakhshanfar, S.; Mbeleck, R.; Xu, K.; Zhang, X.; Zhong, W.; Xing, M. 3D Bioprinting for Biomedical Devices and Tissue Engineering: A Review of Recent Trends and Advances. Bioact. Mater. 2018, 3, 144–156. [Google Scholar] [CrossRef]
- Rhee, S.; Puetzer, J.L.; Mason, B.N.; Reinhart-King, C.A.; Bonassar, L.J. 3D Bioprinting of Spatially Heterogeneous Collagen Constructs for Cartilage Tissue Engineering. ACS Biomater. Sci. Eng. 2016, 2, 1800–1805. [Google Scholar] [CrossRef]
- Ren, X.; Wang, F.; Chen, C.; Gong, X.; Yin, L.; Yang, L. Engineering Zonal Cartilage through Bioprinting Collagen Type II Hydrogel Constructs with Biomimetic Chondrocyte Density Gradient. BMC Musculoskelet. Disord. 2016, 17, 301. [Google Scholar] [CrossRef]
- Saunders, R.E.; Derby, B. Inkjet Printing Biomaterials for Tissue Engineering: Bioprinting. Int. Mater. Rev. 2014, 59, 430–448. [Google Scholar] [CrossRef]
- Dufour, A.; Gallostra, X.B.; O’Keeffe, C.; Eichholz, K.; Von Euw, S.; Garcia, O.; Kelly, D.J. Integrating Melt Electrowriting and Inkjet Bioprinting for Engineering Structurally Organized Articular Cartilage. Biomaterials 2022, 283, 121405. [Google Scholar] [CrossRef]
- Tarassoli, S.P.; Jessop, Z.M.; Al-Sabah, A.; Gao, N.; Whitaker, S.; Doak, S.; Whitaker, I.S. Skin Tissue Engineering Using 3D Bioprinting: An Evolving Research Field. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 615–623. [Google Scholar] [CrossRef]
- Sun, J.; Ng, J.H.; Fuh, Y.H.; Wong, Y.S.; Loh, H.T.; Xu, Q. Comparison of Micro-Dispensing Performance between Micro-Valve and Piezoelectric Printhead. Microsyst. Technol. 2009, 15, 1437–1448. [Google Scholar] [CrossRef]
- Ng, W.L.; Yeong, W.Y.; Naing, M.W. Polyvinylpyrrolidone-Based Bio-Ink Improves Cell Viability and Homogeneity during Drop-On-Demand Printing. Materials 2017, 10, 190. [Google Scholar] [CrossRef]
- Cidonio, G.; Alcala-Orozco, C.R.; Lim, K.S.; Glinka, M.; Mutreja, I.; Kim, Y.H.; Dawson, J.I.; Woodfield, T.B.F.; Oreffo, R.O.C. Osteogenic and Angiogenic Tissue Formation in High Fidelity Nanocomposite Laponite-Gelatin Bioinks. Biofabrication 2019, 11, 035027. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Li, K.; Mohideen, M.; Ramakrishna, S. Three-Dimensional (3D) Printing Based on Controlled Melt Electrospinning in Polymeric Biomedical Materials. Melt. Electrospinning 2019, 159–172. [Google Scholar] [CrossRef]
- Dai, X.; Liu, L.; Ouyang, J.; Li, X.; Zhang, X.; Lan, Q.; Xu, T. Coaxial 3D Bioprinting of Self-Assembled Multicellular Heterogeneous Tumor Fibers. Sci. Rep. 2017, 7, 1457. [Google Scholar] [CrossRef] [PubMed]
- Kjar, A.; McFarland, B.; Mecham, K.; Harward, N.; Huang, Y. Engineering of Tissue Constructs Using Coaxial Bioprinting. Bioact. Mater. 2020, 6, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Shahabipour, F.; Tavafoghi, M.; Aninwene, G.E.; Bonakdar, S.; Oskuee, R.K.; Shokrgozar, M.A.; Potyondy, T.; Alambeigi, F.; Ahadian, S. Coaxial 3D Bioprinting of Tri-Polymer Scaffolds to Improve the Osteogenic and Vasculogenic Potential of Cells in Co-Culture Models. J. Biomed. Mater. Res. A 2022, 110, 1077–1089. [Google Scholar] [CrossRef]
- Shao, L.; Gao, Q.; Xie, C.; Fu, J.; Xiang, M.; He, Y. Synchronous 3D Bioprinting of Large-Scale Cell-Laden Constructs with Nutrient Networks. Adv. Healthc. Mater. 2020, 9, 1901142. [Google Scholar] [CrossRef]
- Ventura, R.D. An Overview of Laser-Assisted Bioprinting (LAB) in Tissue Engineering Applications. Med. Lasers Eng. Basic Res. Clin. Appl. 2021, 10, 76–81. [Google Scholar] [CrossRef]
- Guillotin, B.; Souquet, A.; Catros, S.; Duocastella, M.; Pippenger, B.; Bellance, S.; Bareille, R.; Rémy, M.; Bordenave, L.; Amédée, J.J.; et al. Laser Assisted Bioprinting of Engineered Tissue with High Cell Density and Microscale Organization. Biomaterials 2010, 31, 7250–7256. [Google Scholar] [CrossRef]
- Catros, S.; Fricain, J.C.; Guillotin, B.; Pippenger, B.; Bareille, R.; Remy, M.; Lebraud, E.; Desbat, B.; Amédée, J.; Guillemot, F. Laser-Assisted Bioprinting for Creating on-Demand Patterns of Human Osteoprogenitor Cells and Nano-Hydroxyapatite. Biofabrication 2011, 3, 025001. [Google Scholar] [CrossRef]
- Gruene, M.; Pflaum, M.; Hess, C.; Diamantouros, S.; Schlie, S.; Deiwick, A.; Koch, L.; Wilhelmi, M.; Jockenhoevel, S.; Haverich, A.; et al. Laser Printing of Three-Dimensional Multicellular Arrays for Studies of Cell-Cell and Cell-Environment Interactions. Tissue Eng. Part C Methods 2011, 17, 973–982. [Google Scholar] [CrossRef]
- Koch, L.; Deiwick, A.; Schlie, S.; Michael, S.; Gruene, M.; Coger, V.; Zychlinski, D.; Schambach, A.; Reimers, K.; Vogt, P.M.; et al. Skin Tissue Generation by Laser Cell Printing. Biotechnol. Bioeng. 2012, 109, 1855–1863. [Google Scholar] [CrossRef]
- Makris, E.A.; Hu, J.C.; Athanasiou, K.A. Hypoxia-Induced Collagen Crosslinking as a Mechanism for Enhancing Mechanical Properties of Engineered Articular Cartilage. Osteoarthr. Cartil./OARS Osteoarthr. Res. Soc. 2013, 21, 634. [Google Scholar] [CrossRef]
- Alcala-Orozco, C.R.; Cui, X.; Hooper, G.J.; Lim, K.S.; Woodfield, T.B.F. Converging Functionality: Strategies for 3D Hybrid-Construct Biofabrication and the Role of Composite Biomaterials for Skeletal Regeneration. Acta Biomater. 2021, 132, 188–216. [Google Scholar] [CrossRef]
- Li, H.; Dai, J.; Wang, Z.; Zheng, H.; Li, W.; Wang, M.; Cheng, F. Digital Light Processing (DLP)-based (Bio)Printing Strategies for Tissue Modeling and Regeneration. Aggregate 2022, 4, e270. [Google Scholar] [CrossRef]
- Visser, J.; Peters, B.; Burger, T.J.; Boomstra, J.; Dhert, W.J.A.; Melchels, F.P.W.; Malda, J. Biofabrication of Multi-Material Anatomically Shaped Tissue Constructs. Biofabrication 2013, 5, 035007. [Google Scholar] [CrossRef]
- Duarte Campos, D.F.; Blaeser, A.; Weber, M.; Jäkel, J.; Neuss, S.; Jahnen-Dechent, W.; Fischer, H. Three-Dimensional Printing of Stem Cell-Laden Hydrogels Submerged in a Hydrophobic High-Density Fluid. Biofabrication 2013, 5, 015003. [Google Scholar] [CrossRef]
- Louis, F.; Piantino, M.; Liu, H.; Kang, D.-H.; Sowa, Y.; Kitano, S.; Matsusaki, M. Bioprinted Vascularized Mature Adipose Tissue with Collagen Microfibers for Soft Tissue Regeneration. Cyborg. Bionic. Syst. 2021, 2021, 1412542. [Google Scholar] [CrossRef]
- Kilian, D.; Ahlfeld, T.; Akkineni, A.R.; Lode, A.; Gelinsky, M. Three-Dimensional Bioprinting of Volumetric Tissues and Organs. MRS Bull. 2017, 42, 585–592. [Google Scholar] [CrossRef]
- Kim, M.H.; Banerjee, D.; Celik, N.; Ozbolat, I.T. Aspiration-Assisted Freeform Bioprinting of Mesenchymal Stem Cell Spheroids within Alginate Microgels. Biofabrication 2022, 14, 024103. [Google Scholar] [CrossRef]
- Blaeser, A.; Duarte Campos, D.F.; Weber, M.; Neuss, S.; Theek, B.; Fischer, H.; Jahnen-Dechent, W. Biofabrication under Fluorocarbon: A Novel Freeform Fabrication Technique to Generate High Aspect Ratio Tissue-Engineered Constructs. Biores Open Access 2013, 2, 374–384. [Google Scholar] [CrossRef]
- Ramiah, P.; du Toit, L.C.; Choonara, Y.E.; Kondiah, P.P.D.; Pillay, V. Hydrogel-Based Bioinks for 3D Bioprinting in Tissue Regeneration. Front. Mater. 2020, 7, 76. [Google Scholar] [CrossRef]
- Cha, C.; Soman, P.; Zhu, W.; Nikkhah, M.; Camci-Unal, G.; Chen, S.; Khademhosseini, A. Structural Reinforcement of Cell-Laden Hydrogels with Microfabricated Three Dimensional Scaffolds. Biomater. Sci. 2014, 2, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Coburn, J.; Gibson, M.; Bandalini, P.A.; Laird, C.; Mao, H.Q.; Moroni, L.; Seliktar, D.; Elisseeff, J. Biomimetics of the Extracellular Matrix: An Integrated Three-Dimensional Fiber-Hydrogel Composite for Cartilage Tissue Engineering. Smart Struct. Syst. 2011, 7, 213. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, A.S.; George, P.A.; Cooper-White, J.J. Directing Osteogenic and Myogenic Differentiation of MSCs: Interplay of Stiffness and Adhesive Ligand Presentation. Am. J. Physiol. Cell Physiol. 2008, 295, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Shih, Y.R.V.; Tseng, K.F.; Lai, H.Y.; Lin, C.H.; Lee, O.K. Matrix Stiffness Regulation of Integrin-Mediated Mechanotransduction during Osteogenic Differentiation of Human Mesenchymal Stem Cells. J. Bone Miner. Res. 2011, 26, 730–738. [Google Scholar] [CrossRef] [PubMed]
- Schuurman, W.; Khristov, V.; Pot, M.W.; Van Weeren, P.R.; Dhert, W.J.A.; Malda, J. Bioprinting of Hybrid Tissue Constructs with Tailorable Mechanical Properties. Biofabrication 2011, 3, 021001. [Google Scholar] [CrossRef]
- Manning, W.K.; Bonner Jr, W.M. Isolation and Culture of Chondrocytes from Human Adult Articular Cartilage. Arthritis Rheum. 1967, 10, 235–239. [Google Scholar] [CrossRef]
- Salinas, E.Y.; Hu, J.C.; Athanasiou, K. A Guide for Using Mechanical Stimulation to Enhance Tissue-Engineered Articular Cartilage Properties. Tissue Eng. Part B Rev. 2018, 24, 345–358. [Google Scholar] [CrossRef]
- Corradetti, B.; Taraballi, F.; Corbo, C.; Cabrera, F.; Pandolfi, L.; Minardi, S.; Wang, X.; Van Eps, J.; Bauza, G.; Weiner, B.; et al. Immune Tuning Scaffold for the Local Induction of a Pro-Regenerative Environment. Sci. Rep. 2017, 7, 17030. [Google Scholar] [CrossRef]
- Lee, J.K.; Huwe, L.W.; Paschos, N.; Aryaei, A.; Gegg, C.A.; Hu, J.C.; Athanasiou, K.A. Tension Stimulation Drives Tissue Formation in Scaffold-Free Systems. Nat. Mater. 2017, 16, 864–873. [Google Scholar] [CrossRef]
- Bergholt, M.S.; Albro, M.B.; Stevens, M.M. Online Quantitative Monitoring of Live Cell Engineered Cartilage Growth Using Diffuse Fiber-Optic Raman Spectroscopy. Biomaterials 2017, 140, 128–137. [Google Scholar] [CrossRef]
- Murdoch, A.D.; Hardingham, T.E.; Eyre, D.R.; Fernandes, R.J. The Development of a Mature Collagen Network in Cartilage from Human Bone Marrow Stem Cells in Transwell Culture. Matrix Biol. 2016, 50, 16. [Google Scholar] [CrossRef]
- Lee, J.; Kim, H.C.; Choi, J.W.; Lee, I.H. A Review on 3D Printed Smart Devices for 4D Printing. Int. J. Precis. Eng. Manuf.-Green Technol. 2017, 4, 373–383. [Google Scholar] [CrossRef]
- Salehi-Nik, N.; Amoabediny, G.; Pouran, B.; Tabesh, H.; Shokrgozar, M.A.; Haghighipour, N.; Khatibi, N.; Anisi, F.; Mottaghy, K.; Zandieh-Doulabi, B. Engineering Parameters in Bioreactor’s Design: A Critical Aspect in Tissue Engineering. Biomed. Res. Int. 2013, 2013, 762132. [Google Scholar] [CrossRef]
- Kurobe, H.; Maxfield, M.W.; Tara, S.; Rocco, K.A.; Bagi, P.S.; Yi, T.; Udelsman, B.; Zhuang, Z.W.; Cleary, M.; Iwakiri, Y.; et al. Development of Small Diameter Nanofiber Tissue Engineered Arterial Grafts. PLoS ONE 2015, 10, e0120328. [Google Scholar] [CrossRef]
- Tsiklin, I.L.; Pugachev, E.I.; Kolsanov, A.V.; Timchenko, E.V.; Boltovskaya, V.V.; Timchenko, P.E.; Volova, L.T. Biopolymer Material from Human Spongiosa for Regenerative Medicine Application. Polymers 2022, 14, 941. [Google Scholar] [CrossRef]
- Campanacci, D.A.; Puccini, S.; Caff, G.; Beltrami, G.; Piccioli, A.; Innocenti, M.; Capanna, R. Vascularised Fibular Grafts as a Salvage Procedure in Failed Intercalary Reconstructions after Bone Tumour Resection of the Femur. Injury 2014, 45, 399–404. [Google Scholar] [CrossRef]
- Epple, C.; Haumer, A.; Ismail, T.; Lunger, A.; Scherberich, A.; Schaefer, D.J.; Martin, I. Prefabrication of a Large Pedicled Bone Graft by Engineering the Germ for de Novo Vascularization and Osteoinduction. Biomaterials 2019, 192, 118–127. [Google Scholar] [CrossRef]
- Butter, A.; Aliyev, K.; Hillebrandt, K.H.; Raschzok, N.; Kluge, M.; Seiffert, N.; Tang, P.; Napierala, H.; Muhamma, A.I.; Reutzel-Selke, A.; et al. Evolution of Graft Morphology and Function after Recellularization of Decellularized Rat Livers. J. Tissue Eng. Regen. Med. 2018, 12, e807–e816. [Google Scholar] [CrossRef]
- Nagarajan, N.; Dupret-Bories, A.; Karabulut, E.; Zorlutuna, P.; Vrana, N.E. Enabling Personalized Implant and Controllable Biosystem Development through 3D Printing. Biotechnol. Adv. 2018, 36, 521–533. [Google Scholar] [CrossRef]
- Irawan, V.; Sung, T.C.; Higuchi, A.; Ikoma, T. Collagen Scaffolds in Cartilage Tissue Engineering and Relevant Approaches for Future Development. Tissue Eng. Regen. Med. 2018, 15, 673–697. [Google Scholar] [CrossRef] [PubMed]








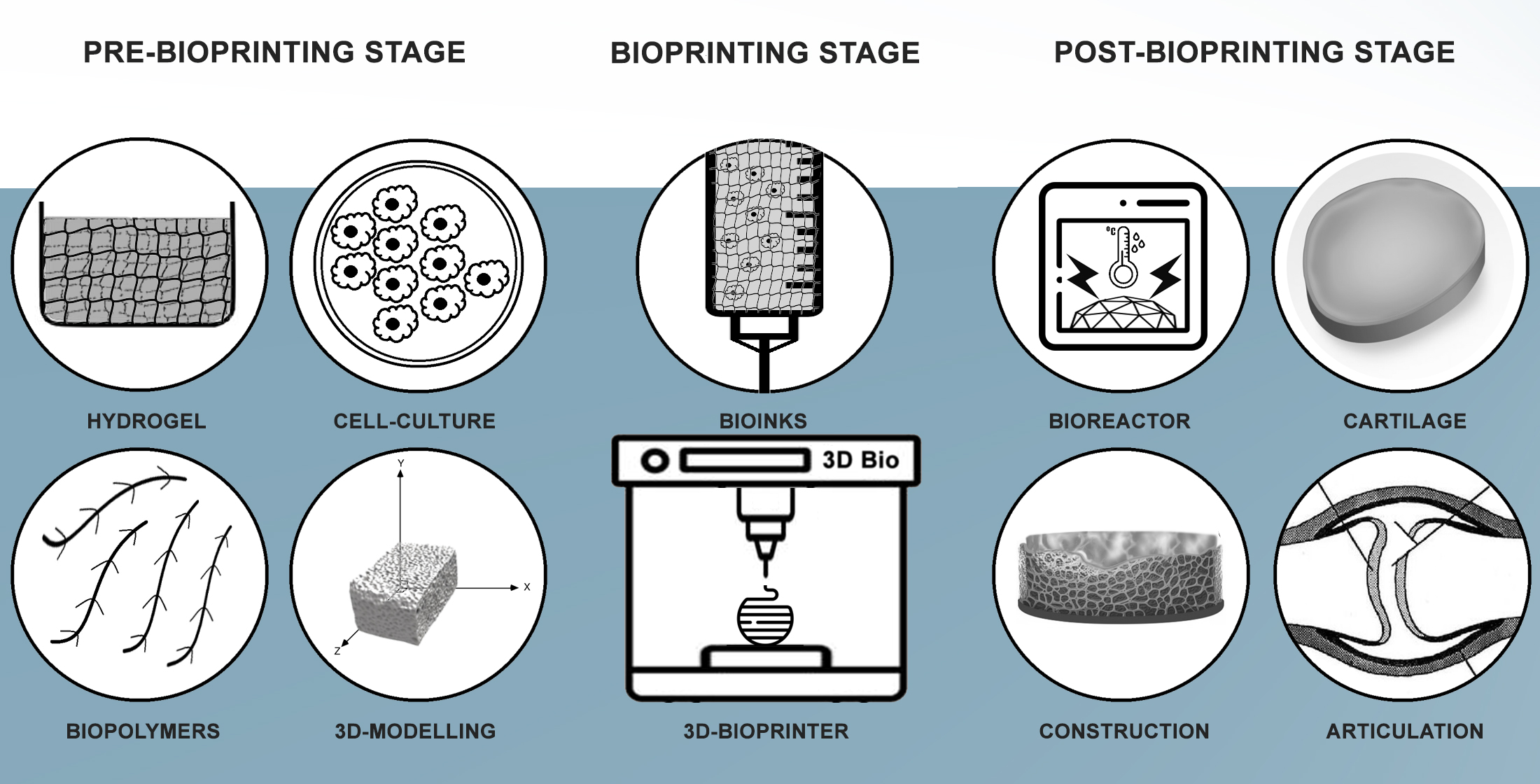{kind=link}
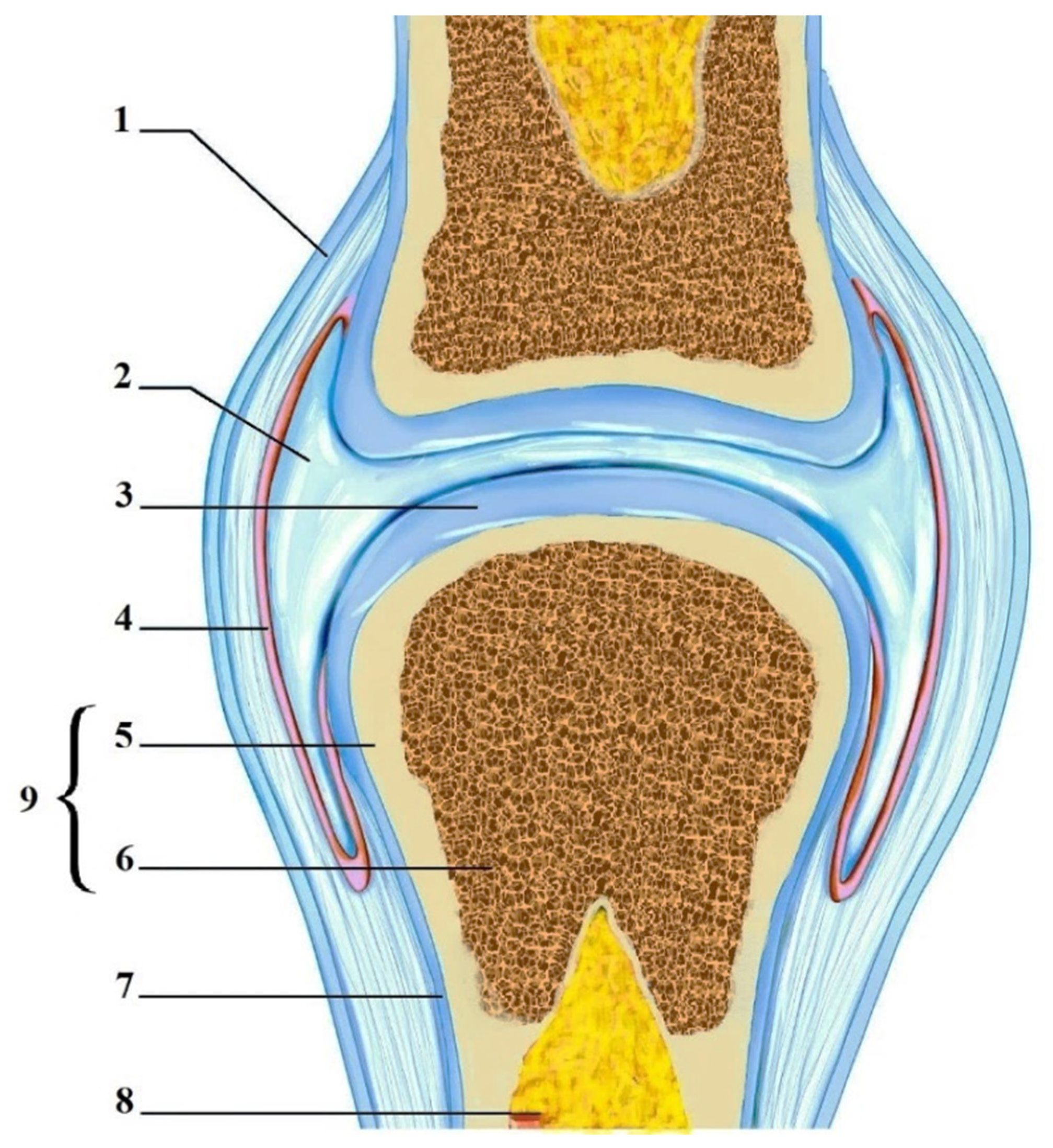{kind=link}
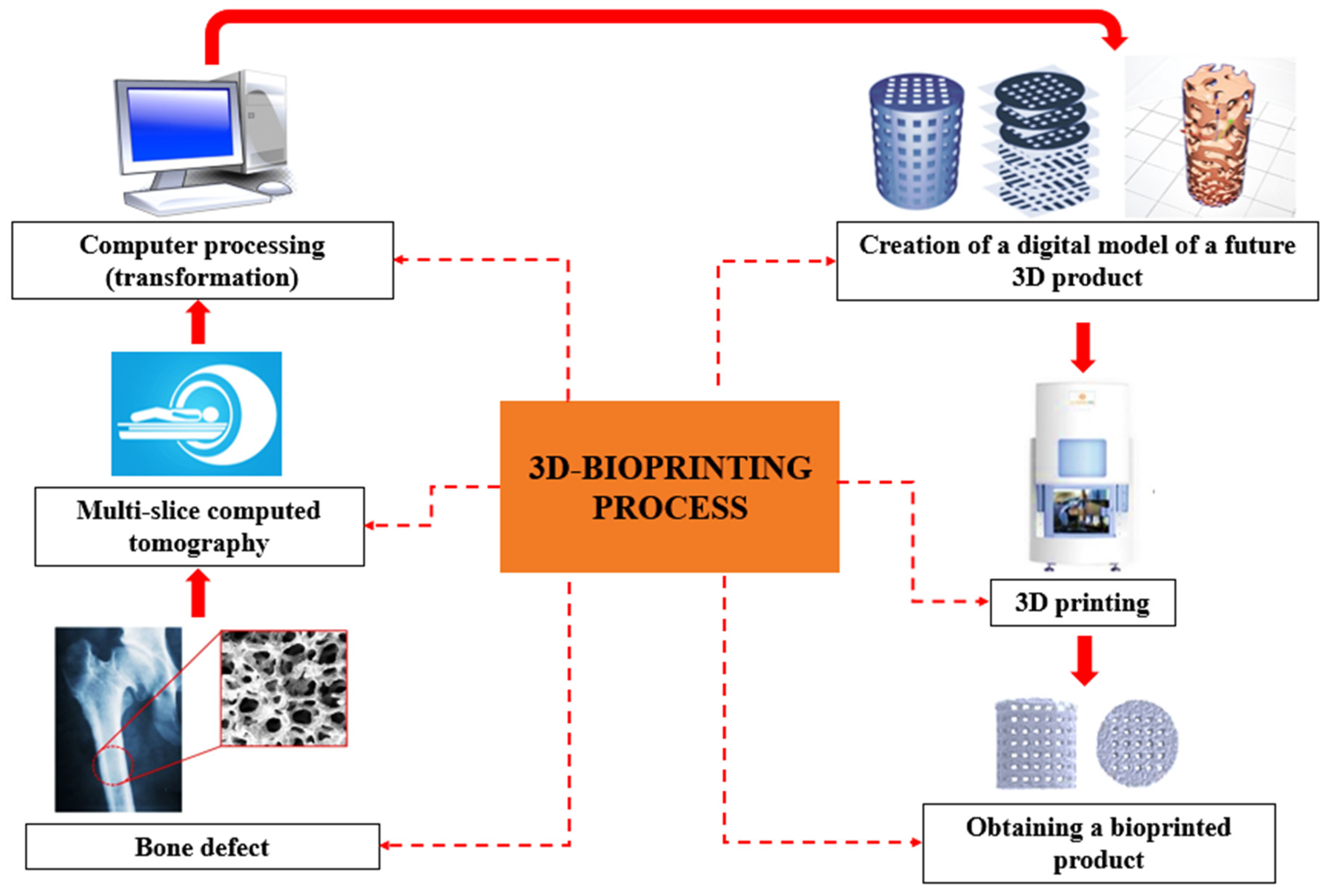{kind=link}
{kind=link}
{kind=link}
{kind=link}
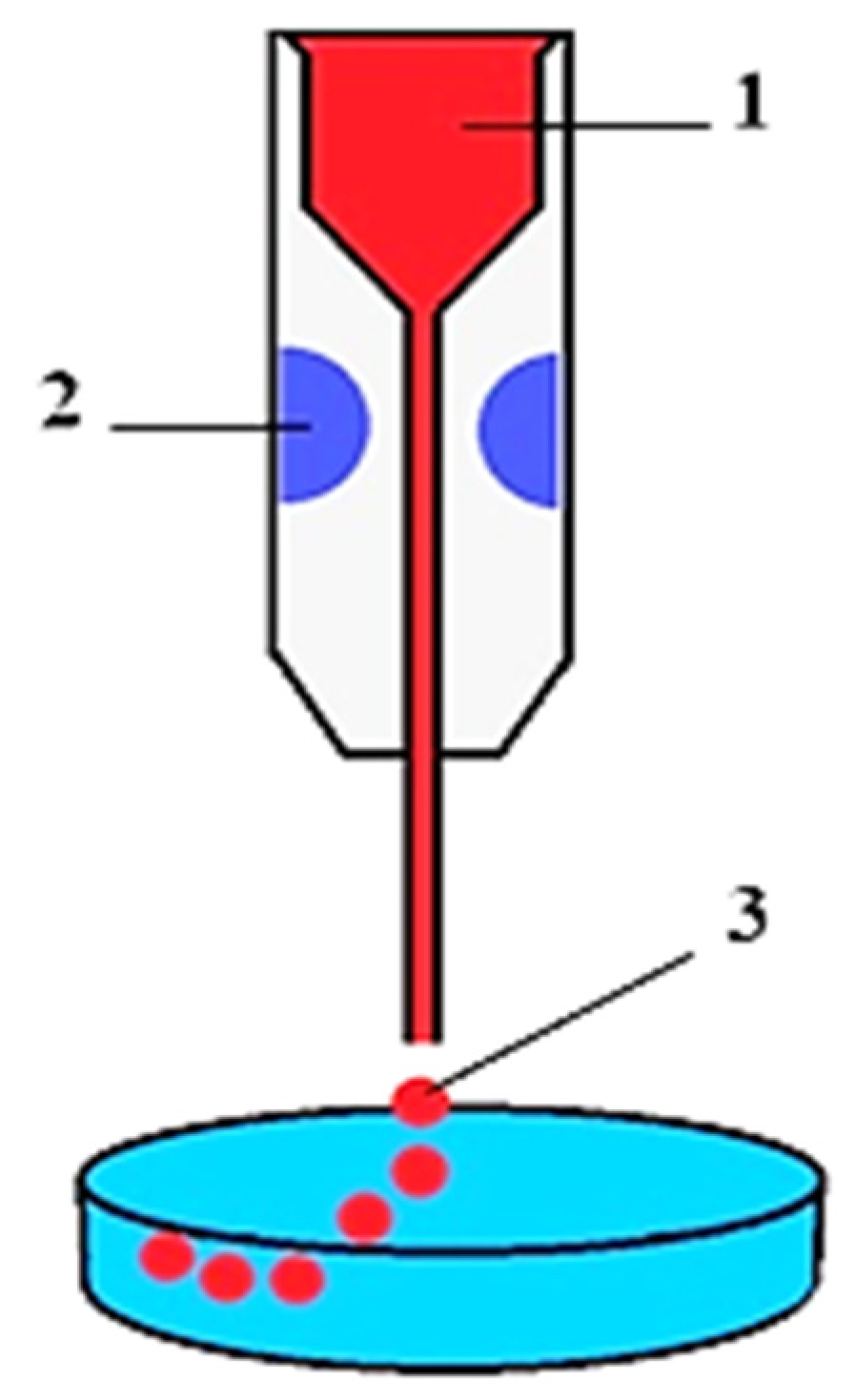{kind=link}
{kind=link}
| № | Properties of Hydrogels | Description of Properties | Sources Cited |
|---|---|---|---|
| 1 | Physical | Gelation temperature; gelation kinetics; rheology (flowability, viscosity, elasticity, and solidification/glazing ability); hydrophobicity/hydrophilicity; wettability; adhesion; polarization; and light transmission. | [151,154,163,165] |
| 2 | Chemical | pH; ion concentration; molecular weight of polymers; cross-linking ability; reactivity; and polarity. | [154,161,163] |
| 3 | Mechanical | Elasticity (ability to compress and swell); ultimate tensile strength; stress relaxation; and self-restoration and degradation. | [154,160,161,171] |
| 4 | Morphological | Porosity of structure and properties and size of pores. | [161] |
| 5 | Biological properties | Biocompatibility; cytocompatibility; biodegradability; inductivity; conductivity; and absence of irritant, toxic, inflammatory, and carcinogenic effects on surrounding tissues. | [154,160,161,170,171] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Volova, L.T.; Kotelnikov, G.P.; Shishkovsky, I.; Volov, D.B.; Ossina, N.; Ryabov, N.A.; Komyagin, A.V.; Kim, Y.H.; Alekseev, D.G. 3D Bioprinting of Hyaline Articular Cartilage: Biopolymers, Hydrogels, and Bioinks. Polymers 2023, 15, 2695. https://doi.org/10.3390/polym15122695
Volova LT, Kotelnikov GP, Shishkovsky I, Volov DB, Ossina N, Ryabov NA, Komyagin AV, Kim YH, Alekseev DG. 3D Bioprinting of Hyaline Articular Cartilage: Biopolymers, Hydrogels, and Bioinks. Polymers. 2023; 15(12):2695. https://doi.org/10.3390/polym15122695
Chicago/Turabian StyleVolova, Larisa T., Gennadiy P. Kotelnikov, Igor Shishkovsky, Dmitriy B. Volov, Natalya Ossina, Nikolay A. Ryabov, Aleksey V. Komyagin, Yeon Ho Kim, and Denis G. Alekseev. 2023. "3D Bioprinting of Hyaline Articular Cartilage: Biopolymers, Hydrogels, and Bioinks" Polymers 15, no. 12: 2695. https://doi.org/10.3390/polym15122695