
Soluble Polymer Microneedles Loaded with Interferon Alpha 1b for Treatment of Hyperplastic Scar
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials and Animals
2.2. MN Fabrication Process
2.3. Characterization of Shape and Skin Puncture
2.4. In Vivo Dissolution
2.5. In Vivo Release
2.6. Scar Modeling and Treatment
2.7. Pathological Analysis
2.8. Gene Expression Analysis
2.9. Data Analysis
3. Results and Discussion
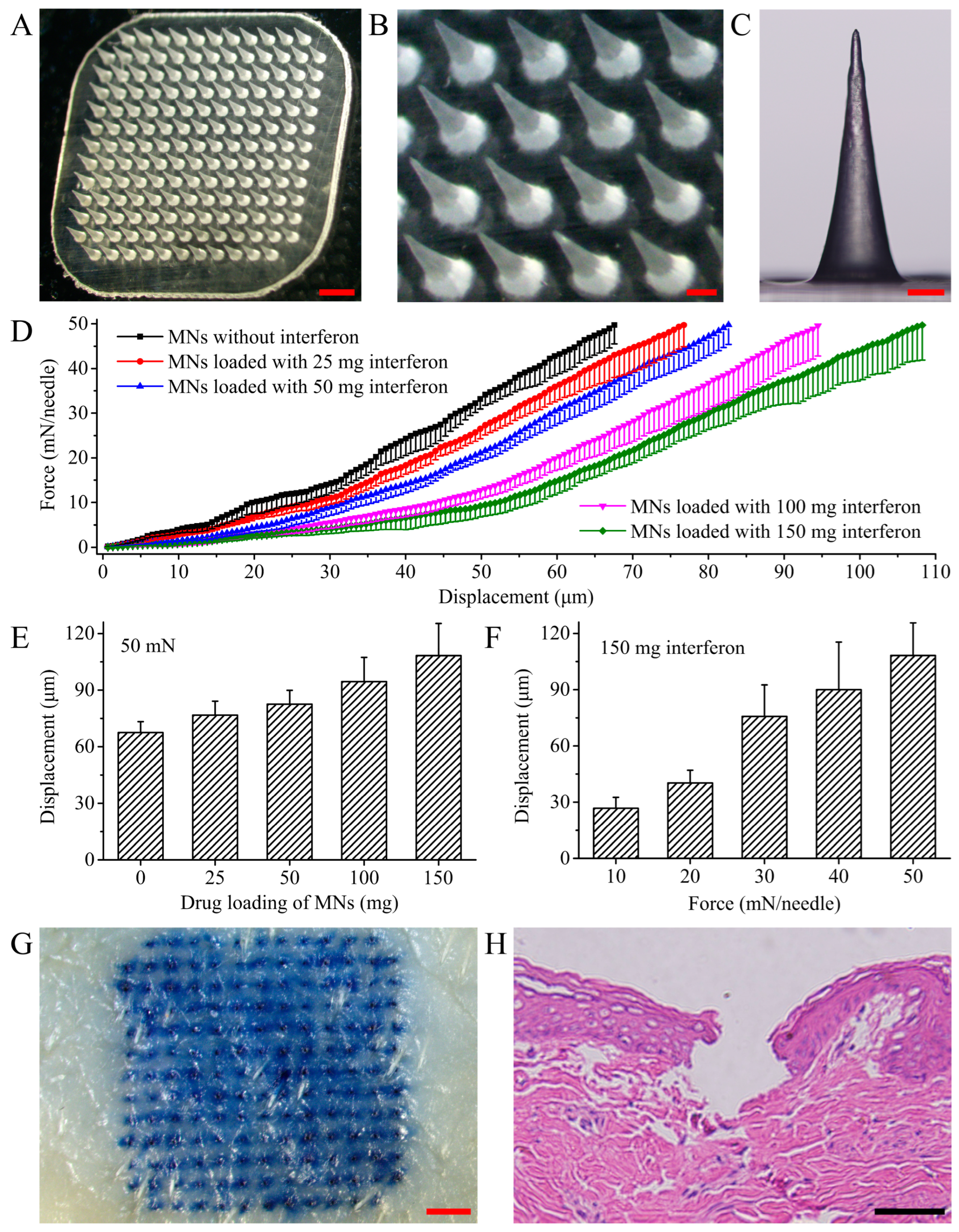
3.1. MN Shape and Mechanical Strength
3.2. In Vivo Dissolution of MNs
3.3. Depth of Skin Punctured
3.4. In Vivo Release of BSA-FITC from the MNs
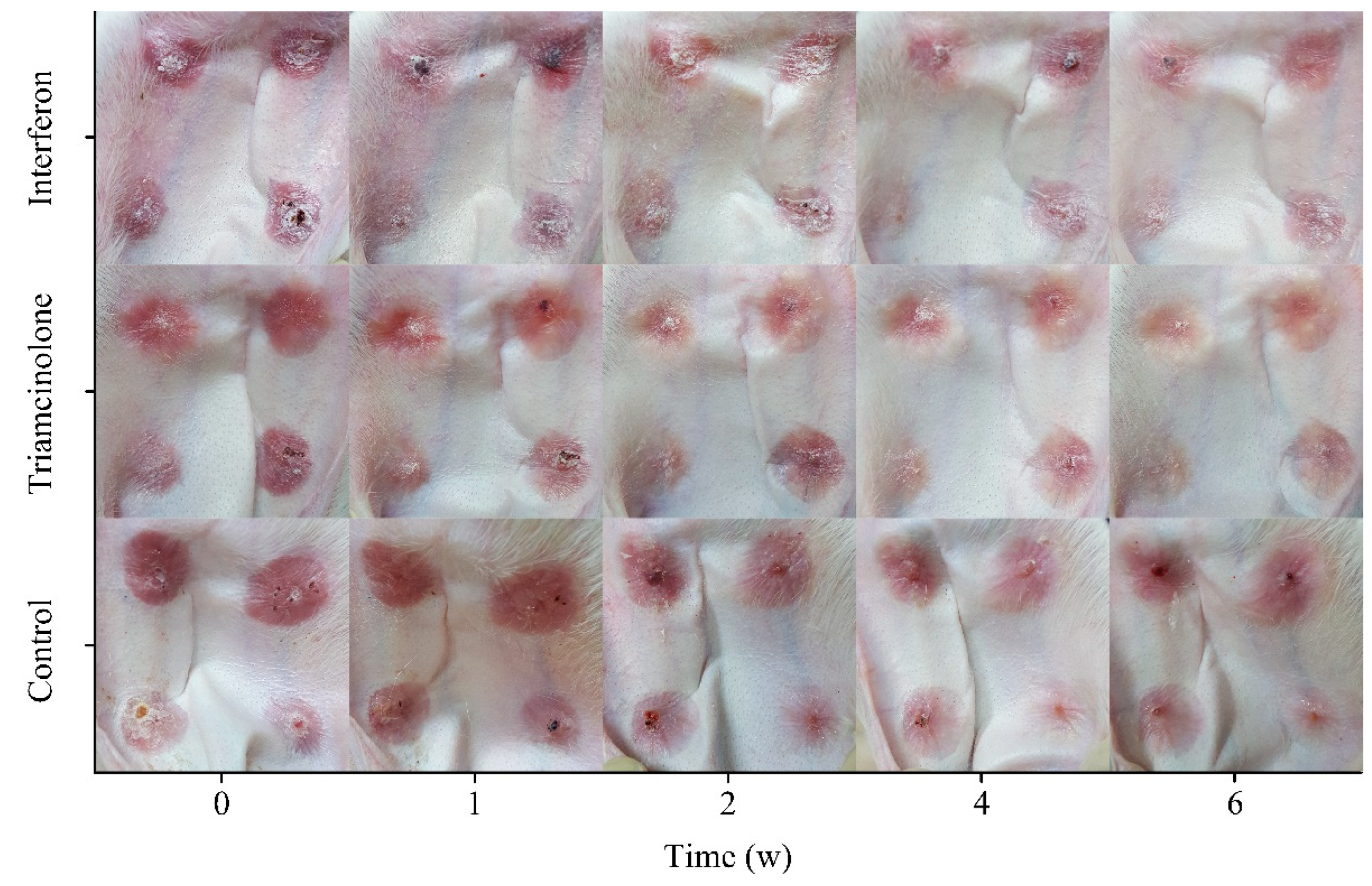
3.5. Scar Status
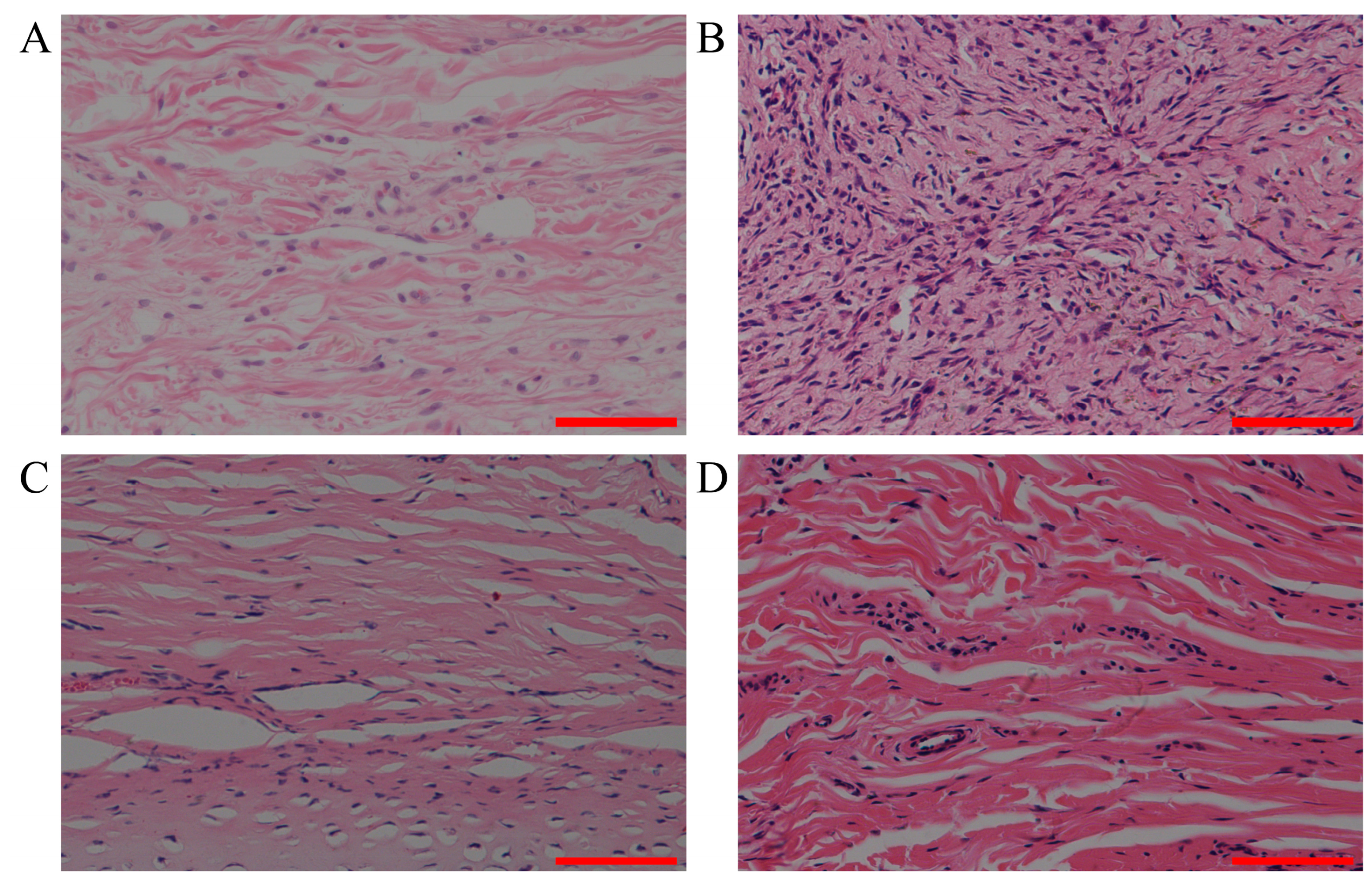
3.6. Analysis of Inflammation
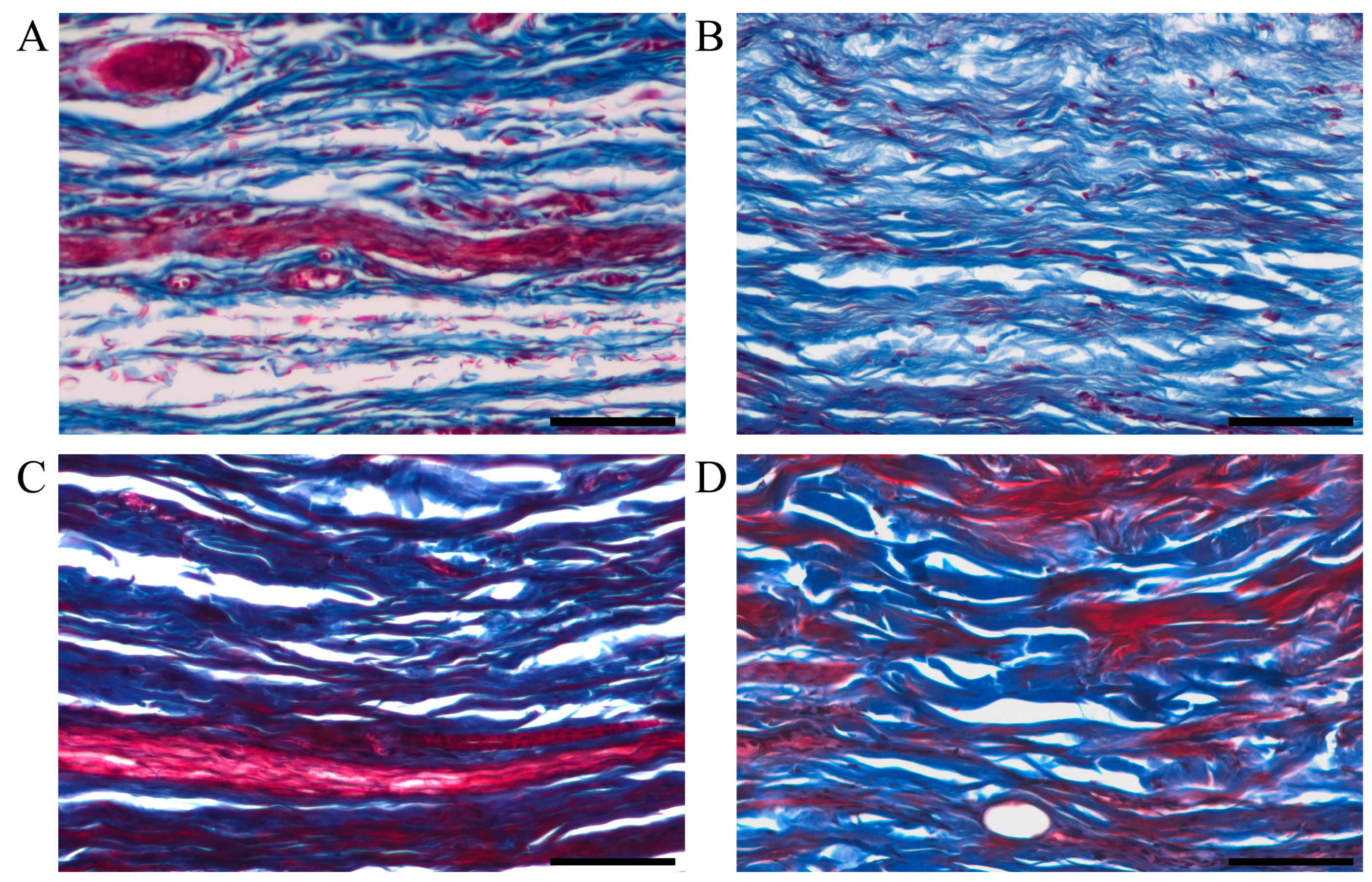
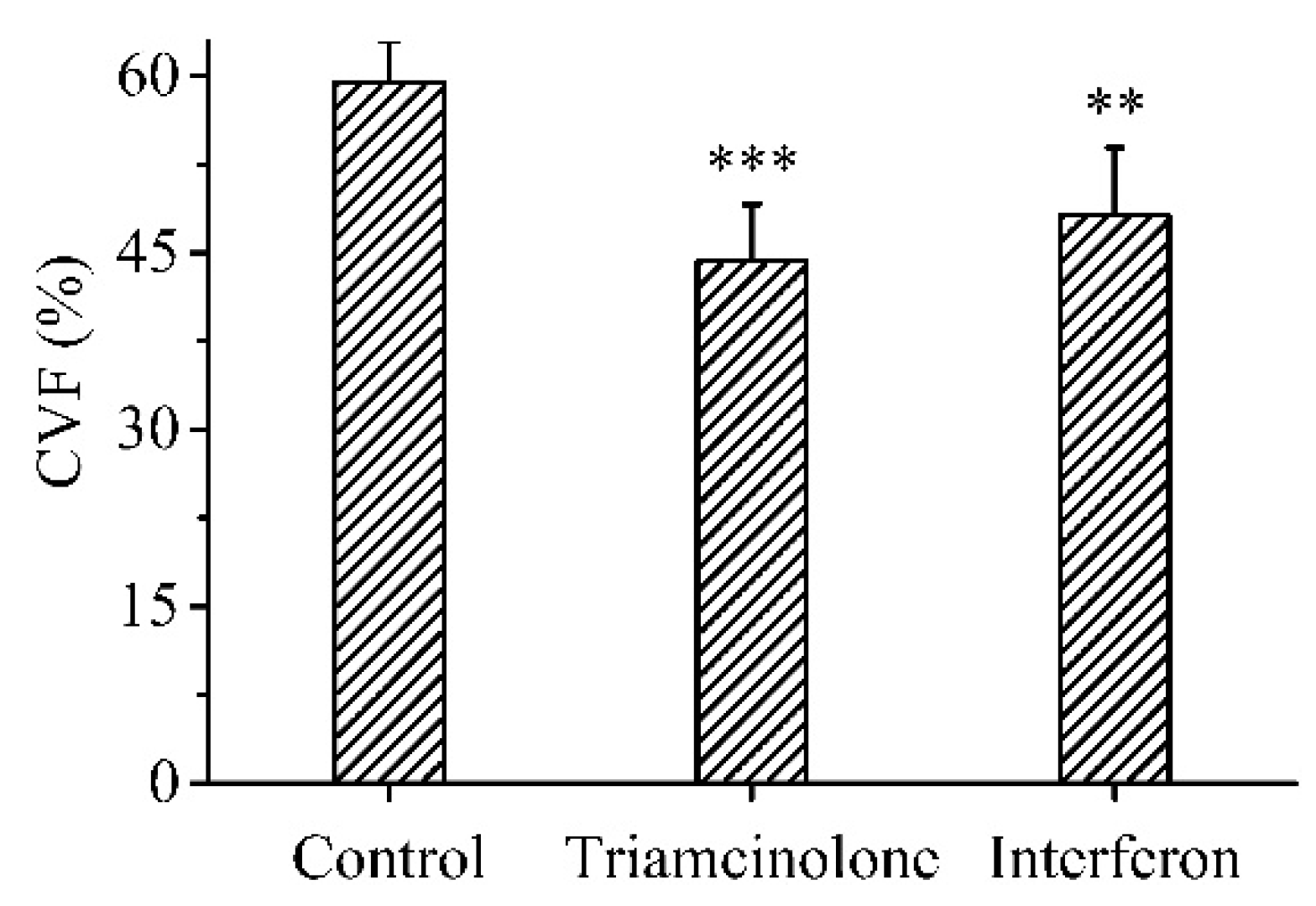
3.7. Deposition of Collagen
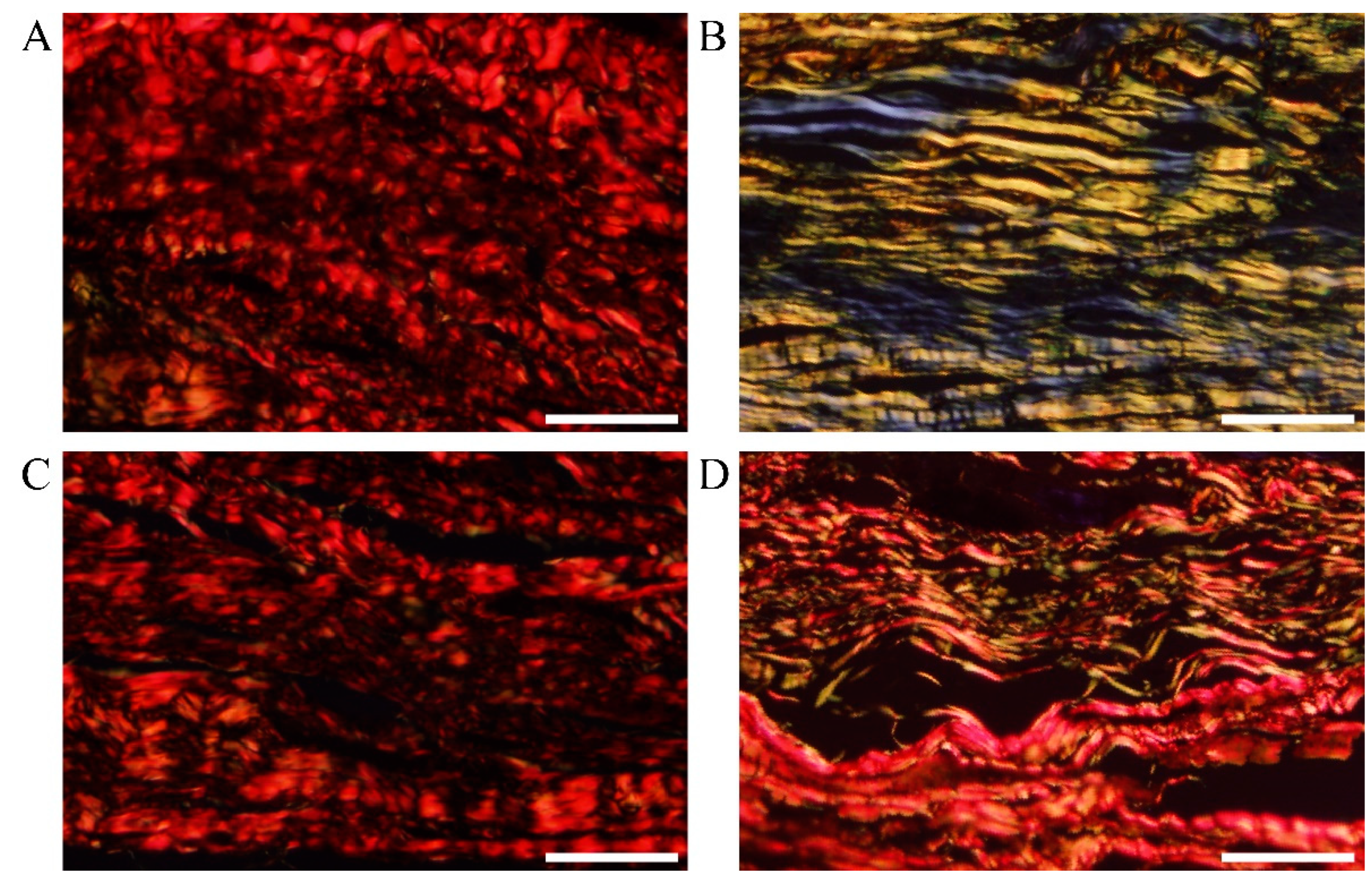
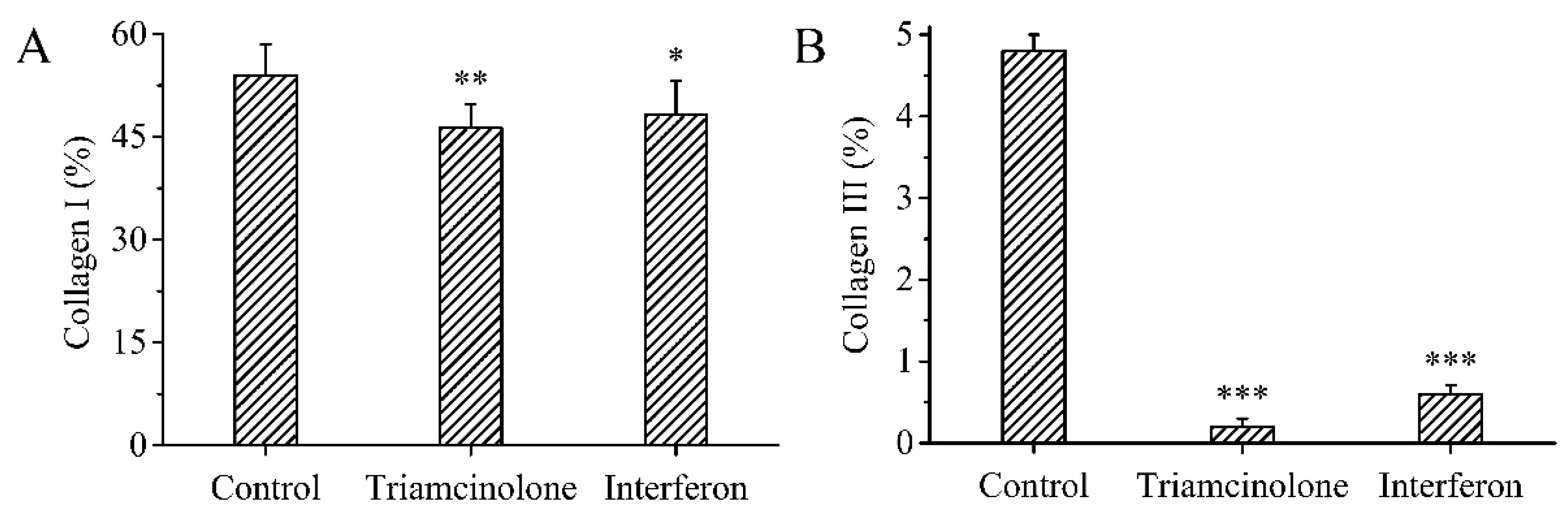
3.8. Type of Collagen
3.9. Gene Expression
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guo, R.; Xuan, W.; He, X.; Xu, K. Clinical efficacy and safety of pulsed dye laser combined with pingyangmycin on hyperplastic scar after acne. Mediat. Inflamm. 2022, 2022, 3305107. [Google Scholar] [CrossRef]
- Li, Z.; Wang, P.; Zhang, J.; Zhao, D. MicroRNA-497-5p downregulation inhibits cell viability, reduces extracellular matrix deposition and induces apoptosis in human hyperplastic scar fibroblasts by regulating Smad7. Exp. Ther. Med. 2021, 21, 384. [Google Scholar] [CrossRef]
- Sun, P.; Lu, X.; Zhang, H.; Hu, Z. The efficacy of drug injection in the treatment of pathological scar: A network meta-analysis. Aesth. Plast. Surg. 2021, 45, 791–805. [Google Scholar] [CrossRef] [PubMed]
- Qi, J.; Liu, Y.; Hu, K.; Zhang, Y.; Wu, Y.; Zhang, X. MicroRNA-205-5p regulates extracellular matrix production in hyperplastic scars by targeting Smad2. Exp. Ther. Med. 2019, 17, 2284–2290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogawa, R. Surgery for scar revision and reduction: From primary closure to flap surgery. Burn. Trauma 2019, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Song, S.; Fu, H.; He, B.; Wang, D.; Qin, M.; Yang, D.; Liu, D.; Song, G.; Shi, Y.; Zhang, H.; et al. Rho GTPases in A549 and Caco-2 cells dominating the endocytic pathways of nanocarbons with different morphologies. Int. J. Nanomed. 2018, 13, 4391–4404. [Google Scholar] [CrossRef] [Green Version]
- Riquet, D.; Houel, N.; Bodnar, J.L. Effect of osteopathic treatment on a scar assessed by thermal infrared camera, pilot study. Complement. Ther. Med. 2019, 45, 130–135. [Google Scholar] [CrossRef]
- Kauvar, A.N.B.; Kubicki, S.L.; Suggs, A.K.; Friedman, P.M. Laser therapy of traumatic and surgical scars and an algorithm for their treatment. Lasers Surg. Med. 2020, 52, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Guo, P.; Wang, X.; Huo, R.; Li, Q.; Yin, S.; Cao, Y. Effective treatment for hypertrophic scar with dual-wave-length PDL and Nd:YAG in Chinese patients. J. Cosmet. Laser Ther. 2019, 21, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Lubczynska, A.; Garncarczyk, A.; Wcislo-Dziadecka, D. Effectiveness of various methods of manual scar therapy. Ski. Res. Technol. 2023, 29, e13272. [Google Scholar] [CrossRef]
- Sheng, M.; Chen, Y.; Li, H.; Zhang, Y.; Zhang, Z. The application of corticosteroids for pathological scar prevention and treatment: Current review and update. Burn. Trauma 2023, 11, tkad009. [Google Scholar] [CrossRef]
- Kuehlmann, B.; Stern-Buchbinder, Z.; Wan, D.C.; Friedstat, J.S.; Gurtner, G.C. Beneath the surface: A review of laser remodeling of hypertrophic scars and burns. Adv. Wound Care 2019, 8, 168–176. [Google Scholar] [CrossRef]
- Gkiourtzis, N.; Glava, A.; Moutafi, M.; Vasileiadou, T.; Delaporta, T.; Michou, P.; Printza, N.; Makedou, K.; Tramma, D. The efficacy and safety of corticosteroids in pediatric kidney scar prevention after urinary tract infection: A systematic review and meta-analysis of randomized clinical trials. Pediatr. Nephrol. 2023, 38, 1–9. [Google Scholar] [CrossRef]
- Wang, Y.; Niu, Y.; Lin, F.; Su, P.; Chen, L.; Liu, D.; Sun, Y. X-ray irradiation improves neurological function recovery of injured spinal cord by inhibiting inflammation and glial scar formation. J. Mol. Neurosci. 2022, 72, 1008–1017. [Google Scholar] [CrossRef]
- Barrat, F.J.; Crow, M.K.; Ivashkiv, L.B. Interferon target-gene expression and epigenomic signatures in health and disease. Nat. Immunol. 2019, 20, 1574–1583. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Schnepf, D.; Staeheli, P. Interferon-lambda orchestrates innate and adaptive mucosal immune responses. Nat. Rev. Immunol. 2019, 19, 614–625. [Google Scholar] [CrossRef]
- Yang, E.; Li, M.M.H. All about the RNA: Interferon-stimulated genes that interfere with viral RNA processes. Front. Immunol. 2020, 11, 605024. [Google Scholar] [CrossRef] [PubMed]
- Wittling, M.C.; Cahalan, S.R.; Levenson, E.A.; Rabin, R.L. Shared and unique features of human interferon-beta and interferon-alpha subtypes. Front. Immunol. 2021, 11, 605673. [Google Scholar] [CrossRef] [PubMed]
- Feng, H.; Zhang, Y.B.; Gui, J.F.; Lemon, S.M.; Yamane, D. Interferon regulatory factor 1 (IRF1) and anti-pathogen innate immune responses. PLoS Pathog. 2021, 17, e1009220. [Google Scholar] [CrossRef]
- Zhang, R.; Liu, D.; Xie, Q.; Hu, Q.; Wang, Q.; Shan, C.; Yang, J. Inhibition of miR-9 attenuates fibroblast proliferation in human hyperplastic scar by regulating TGF-β1. Am. J. Transl. Res. 2019, 11, 3645–3650. [Google Scholar]
- Meng, X.; Gao, X.; Shi, K.; Zhao, J.; Zhang, X.; Zhou, X.; Liu, X.; Yu, J. Interferon-α2b-induced RARRES3 upregulation inhibits hypertrophic scar fibroblasts’ proliferation and migration through wnt/β-catenin pathway suppression. J. Interferon. Cytokine Res. 2023, 43, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Dorrier, C.E.; Aran, D.; Haenelt, E.A.; Sheehy, R.N.; Hoi, K.K.; Pintaric, L.; Chen, Y.; Lizama, C.O.; Cautivo, K.M.; Weiner, G.A.; et al. CNS fibroblasts form a fibrotic scar in response to immune cell infiltration. Nat. Neurosci. 2021, 24, 234–244. [Google Scholar] [CrossRef]
- Chen, Y.J.; Cheng, H.W.; Yen, W.Y.; Tsai, J.H.; Yeh, C.Y.; Chen, C.J.; Liu, J.T.; Chen, S.Y.; Chang, S.J. The treatment of keloid scars via modulating heterogeneous gelatin-structured composite microneedles to control transdermal dual-drug release. Polymers 2022, 14, 4436. [Google Scholar] [CrossRef]
- Amani, H.; Shahbazi, M.A.; D’Amico, C.; Fontana, F.; Abbaszadeh, S.; Santos, H.A. Microneedles for painless transdermal immunotherapeutic applications. J. Control. Release 2021, 330, 185–217. [Google Scholar] [CrossRef]
- Zhou, Z.; Zhang, S.; Yang, G.; Gao, Y. Enhanced delivery efficiency and sustained release of biopharmaceuticals by complexation-based gel encapsulated coated microneedles: rhIFNα-1b example. Asian J. Pharm. Sci. 2021, 16, 612–622. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Namjoshi, S.; Benson, H.A.E.; Mohammed, Y.; Kumeria, T. Dissolvable polymer microneedles for drug delivery and diagnostics. J. Control. Release 2022, 347, 561–589. [Google Scholar] [CrossRef] [PubMed]
- Bao, C.; Li, Z.; Liang, S.; Hu, Y.; Wang, X.; Fang, B.; Wang, P.; Chen, S.; Li, Y. Microneedle patch delivery of capsaicin-containing α-lactalbumin nanomicelles to adipocytes achieves potent anti-obesity effects. Adv. Funct. Mater. 2021, 31, 2011130. [Google Scholar] [CrossRef]
- Chen, J.; Qiu, Y.; Zhang, S.; Gao, Y. Dissolving microneedle-based intradermal delivery of interferon-α-2b. Drug Dev. Ind. Pharm. 2016, 42, 890–896. [Google Scholar] [CrossRef]
- Chen, S.X.; Ma, M.; Xue, F.; Shen, S.; Chen, Q.; Kuang, Y.; Liang, K.; Wang, X.; Chen, H. Construction of microneedle-assisted co-delivery platform and its combining photodynamic/immunotherapy. J. Control. Release 2020, 324, 218–227. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, Y.; Xian, Y.; Singh, P.; Feng, J.; Cui, S.; Carrier, A.; Oakes, K.; Luan, T.; Zhang, X. Multifunctional graphene-oxide-reinforced dissolvable polymeric microneedles for transdermal drug delivery. ACS Appl. Mater. Interfaces 2020, 12, 352–360. [Google Scholar] [CrossRef]
- Choo, S.; Jin, S.; Jung, J. Fabricating high-resolution and high-dimensional microneedle mold through the resolution improvement of stereolithography 3D printing. Pharmaceutics 2022, 14, 766. [Google Scholar] [CrossRef] [PubMed]
- Desai, V.M.; Priya, S.; Gorantla, S.; Singhvi, G. Revolutionizing therapeutic delivery with microneedle technology for tumor treatment. Pharmaceutics 2022, 15, 14. [Google Scholar] [CrossRef] [PubMed]
- Du, G.; He, P.; Zhao, J.; He, C.; Jiang, M.; Zhang, Z.; Zhang, Z.; Sun, X. Polymeric microneedle-mediated transdermal delivery of melittin for rheumatoid arthritis treatment. J. Control. Release 2021, 336, 537–548. [Google Scholar] [CrossRef] [PubMed]
- AL-Japairai, K.A.S.; Mahmood, S.; Almurisi, H.S.; Venugopal, J.R.; Hilles, A.R.; Azmana, M.; Raman, S. Current trends in polymer microneedle for transdermal drug delivery. Int. J. Pharm. 2020, 587, 119673. [Google Scholar] [CrossRef]
- Yang, L.; Yang, Y.; Chen, H.; Mei, L.; Zeng, X. Polymeric microneedle-mediated sustained release systems: Design strategies and promising applications for drug delivery. Asian J. Pharm. Sci. 2021, 17, 70–86. [Google Scholar] [CrossRef]
- Wu, M.; Xia, T.; Li, Y.; Wang, T.; Yang, S.; Yu, J.; Liang, Q.; Shen, T.; Yu, M.; Zhao, B. Design and fabrication of r-hirudin loaded dissolving microneedle patch for minimally invasive and long-term treatment of thromboembolic disease. Asian J. Pharm. Sci. 2022, 17, 284–297. [Google Scholar] [CrossRef]
- He, M.; Yang, G.; Zhang, S.; Zhao, X.; Gao, Y. Dissolving microneedles loaded with etonogestrel microcrystal particles for intradermal sustained delivery. J. Pharm. Sci. 2017, 107, 1037–1045. [Google Scholar] [CrossRef]
- Ho, M.J.; Jeong, H.T.; Im, S.H.; Kim, H.T.; Lee, J.E.; Park, J.S.; Cho, H.R.; Kim, D.Y.; Choi, Y.W.; Lee, J.W.; et al. Design and in vivo pharmacokinetic evaluation of triamcinolone acetonide microcrystals-loaded PLGA microsphere for increased drug retention in knees after intra-articular injection. Pharmaceutics 2019, 11, 419. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Zhang, S.; Zhao, X.; Lian, J.; Gao, Y. Preparation, characterization, and in vivo evaluation of levonorgestrel-loaded thermostable microneedles. Drug Deliv. Transl. Res. 2021, 12, 944–956. [Google Scholar] [CrossRef]
- Cao, S.; Wang, Y.; Wang, M.; Yang, X.; Tang, Y.; Pang, M.; Wang, W.; Chen, L.; Wu, C.; Xu, Y. Microneedles mediated bioinspired lipid nanocarriers for targeted treatment of alopecia. J. Control. Release 2021, 329, 1–15. [Google Scholar] [CrossRef]
- Xing, M.; Yang, G.; Zhang, S.; Gao, Y. Acid-base combination principles for preparation of anti-acne dissolving microneedles loaded with azelaic acid and matrine. Eur. J. Pharm. Sci. 2021, 165, 105935. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Zhang, S.; Zhou, Z.; Xing, M.; Gao, Y. Two-layer sustained-release microneedles encapsulating exenatide for type 2 diabetes treatment. Pharmaceutics 2022, 14, 1255. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Zhang, S.; Yang, G.; Zhou, Z.; Xing, M.; Liu, H.; Cheng, A.; Gao, Y. Dissolvable polymeric microneedles loaded with aspirin for antiplatelet aggregation. Asian J. Pharm. Sci. 2023, 18, 100776. [Google Scholar] [CrossRef]
- Cahill, E.M.; Keaveney, S.; Stuettgen, V.; Eberts, P.; Ramos-Luna, P.; Zhang, N.; Dangol, M.; O’Cearbhaill, E.D. Metallic microneedles with interconnected porosity: A scalable platform for biosensing and drug delivery. Acta Biomater. 2018, 80, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Resnik, D.; Mozek, M.; Pecar, B.; Janez, A.; Urbancic, V.; Iliescu, C.; Vrtacnik, D. In vivo experimental study of noninvasive insulin microinjection through hollow Si microneedle array. Micromachines 2018, 9, 40. [Google Scholar] [CrossRef] [Green Version]
- Hinz, B.; Lagares, D. Evasion of apoptosis by myofibroblasts: A hallmark of fibrotic diseases. Nat. Rev. Rheumatol. 2020, 16, 11–31. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Encoding Gene Name | Forward Primer (3′–5′) | Reverse Primer (3′–5′) | Fragment Length (bp) |
|---|---|---|---|
| GAPDH | CTGGTCATCAACGGGAAGGC | CTCCATGGTGGTGAAGACGC | 120 |
| α-SMA | GCACTGTCAGGAATCCCGTG | CGGAGCCATTGTCACACACA | 83 |
| TGF-β1 | GCGGCAGCTGTACATTGACT | TTGTACAGGGCCAGGACCTT | 147 |
| Collagen I | GGCCGAACTGGAGAAACAGG | AGCAGTACCAGCCTCTCCAG | 81 |
| Collagen III | CCGAACCGTGCCAAATATGC | AACAGTGCGGGGAGTAGTTG | 158 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, B.; Zhang, S.; Cheng, A.; Yan, J.; Gao, Y. Soluble Polymer Microneedles Loaded with Interferon Alpha 1b for Treatment of Hyperplastic Scar. Polymers 2023, 15, 2621. https://doi.org/10.3390/polym15122621
Wang B, Zhang S, Cheng A, Yan J, Gao Y. Soluble Polymer Microneedles Loaded with Interferon Alpha 1b for Treatment of Hyperplastic Scar. Polymers. 2023; 15(12):2621. https://doi.org/10.3390/polym15122621
Chicago/Turabian StyleWang, Baorui, Suohui Zhang, Aguo Cheng, Juan Yan, and Yunhua Gao. 2023. "Soluble Polymer Microneedles Loaded with Interferon Alpha 1b for Treatment of Hyperplastic Scar" Polymers 15, no. 12: 2621. https://doi.org/10.3390/polym15122621