
Performance of Polydioxanone-Based Membrane in Association with 3D-Printed Bioceramic Scaffolds in Bone Regeneration
 ,
,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. PDO Membranes
2.2. Printing of Bioceramic Scaffolds
2.3. Animals
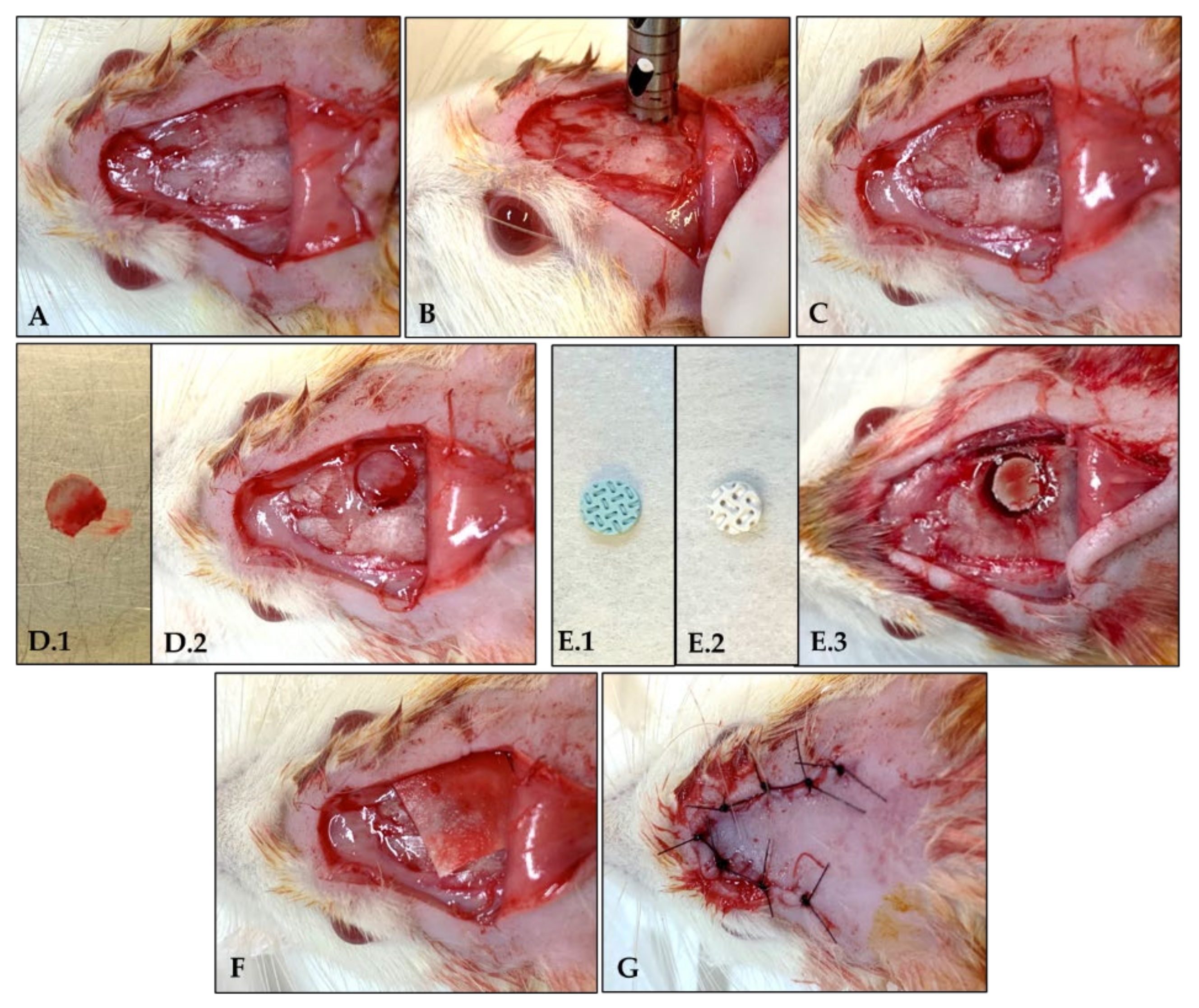
2.4. Surgical Procedure
2.5. Laboratorial Processing
2.6. Histological Analysis
2.7. Immunolabeling Analysis
2.8. Micro-Computed Tomographic (Micro-CT) Analysis
2.9. Statistical Analysis
3. Results
3.1. Histological Analysis
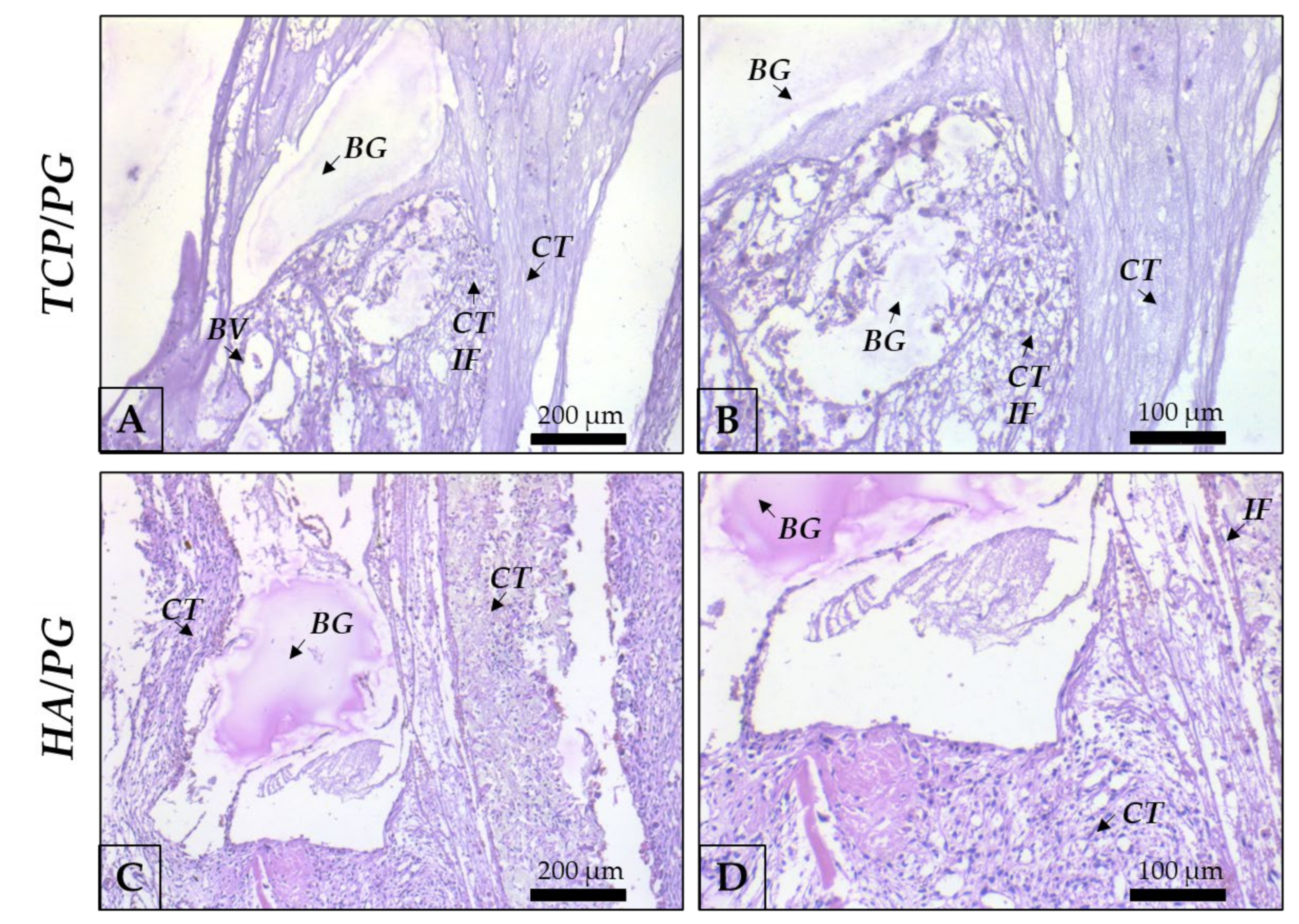
3.1.1. Histological Analysis at 7 Days of Bone Repair
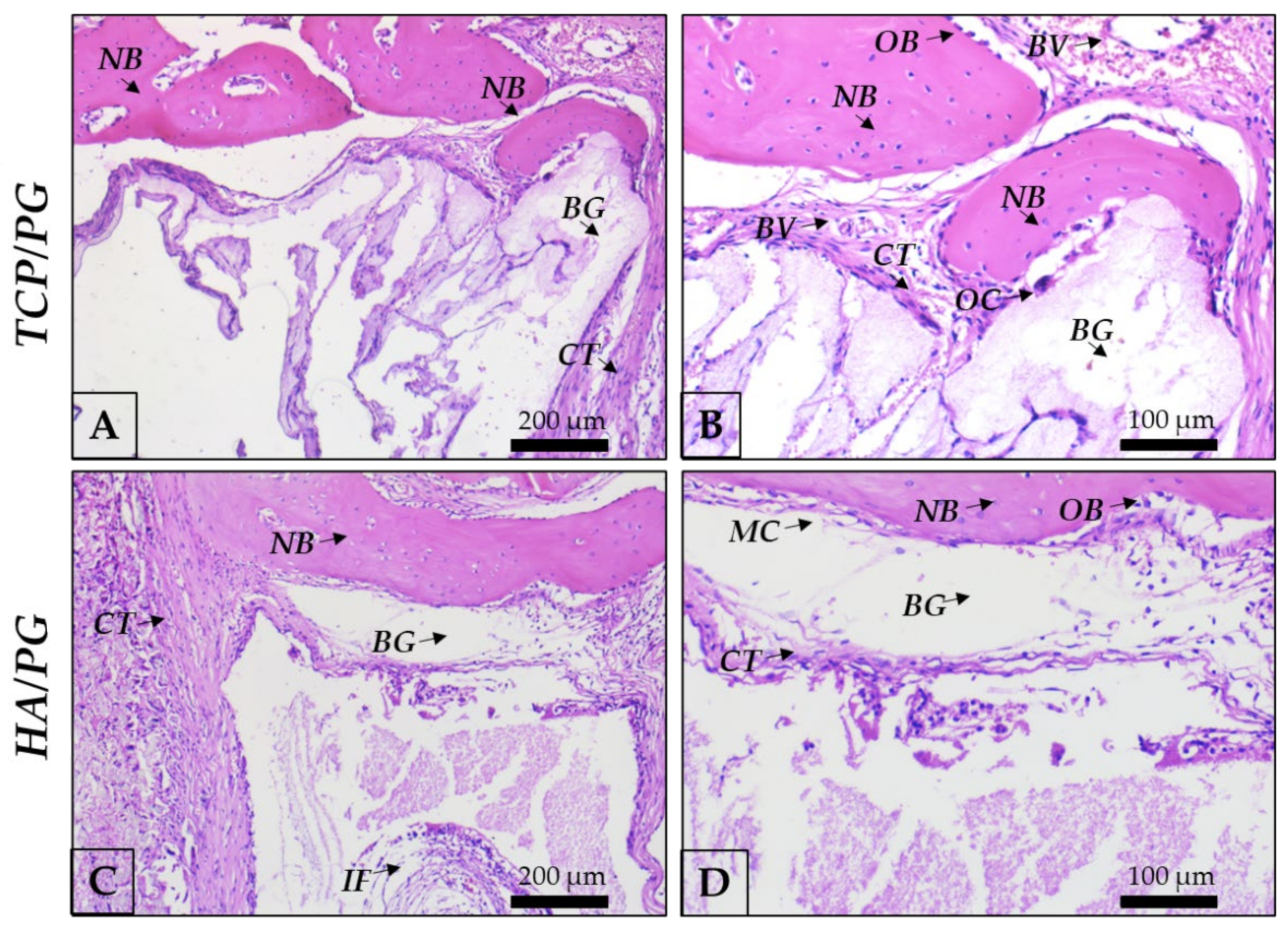
3.1.2. Histological Analysis at 30 Days of Bone Repair
3.2. Immunolabeling Analysis
Immunolabeling Analysis at 30 Days of Bone Repair
3.3. Micro-Computed Tomographic (Micro-CT) Analysis
3.3.1. Percentage of Bone Volume (BV/TV)
3.3.2. Trabecular Thickness (Tb.Th)
3.3.3. Trabecular Number (Tb.N)
3.3.4. Trabecular Separation (Tb.Sp)
3.3.5. Total Porosity (Po.Tot)
3.4. Clinical Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Retzepi, M.; Donos, N. Guided Bone Regeneration: Biological Principle and Therapeutic Applications. Clin. Oral Implants Res. 2010, 21, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Saska, S.; Pilatti, L.; Silva, E.; Nagasawa, M.; Câmara, D.; Lizier, N.; Finger, E.; Konwińska, M.D.; Kempisty, B.; Tunchel, S.; et al. Polydioxanone-Based Membranes for Bone Regeneration. Polymers 2021, 13, 1685. [Google Scholar] [CrossRef] [PubMed]
- Luvizuto, E.R.; Tangl, S.; Zanoni, G.; Okamoto, T.; Sonoda, C.K.; Gruber, R.; Okamoto, R. The Effect of BMP-2 on the Osteoconductive Properties of β-Tricalcium Phosphate in Rat Calvaria Defects. Biomaterials 2011, 32, 3855–3861. [Google Scholar] [CrossRef] [PubMed]
- Gomes-Ferreira, P.H.S.; Okamoto, R.; Ferreira, S.; De Oliveira, D.; Momesso, G.A.C.; Faverani, L.P. Scientific Evidence on the Use of Recombinant Human Bone Morphogenetic Protein-2 (RhBMP-2) in Oral and Maxillofacial Surgery. Oral Maxillofac. Surg. 2016, 20, 223–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva de Oliveira, J.C.; Okamoto, R.; Sonoda, C.K.; Poi, W.R.; Garcia Júnior, I.R.; Luvizuto, E.R. Evaluation of the Osteoinductive Effect of PDGF-BB Associated with Different Carriers in Bone Regeneration in Bone Surgical Defects in Rats. Implant Dent. 2017, 26, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Shibli, J.A.; Nagay, B.E.; Suárez, L.J.; Urdániga Hung, C.; Bertolini, M.; Barão, V.A.R.; Souza, J.G.S. Bone Tissue Engineering Using Osteogenic Cells: From the Bench to the Clinical Application. Tissue Eng. Part C Methods 2022, 28, 179–192. [Google Scholar] [CrossRef]
- Grossi-Oliveira, G.; Faverani, L.P.; Mendes, B.C.; Braga Polo, T.O.; Batista Mendes, G.C.; de Lima, V.N.; Ribeiro Júnior, P.D.; Okamoto, R.; Magro-Filho, O. Comparative Evaluation of Bone Repair with Four Different Bone Substitutes in Critical Size Defects. Int. J. Biomater. 2020, 2020, 5182845. [Google Scholar] [CrossRef]
- Moussa, N.T.; Dym, H. Maxillofacial Bone Grafting Materials. Dent. Clin. N. Am. 2020, 64, 473–490. [Google Scholar] [CrossRef]
- Cheah, C.W.; Al-Namnam, N.M.; Lau, M.N.; Lim, G.S.; Raman, R.; Fairbairn, P.; Ngeow, W.C. Synthetic Material for Bone, Periodontal, and Dental Tissue Regeneration: Where Are We Now, and Where Are We Heading Next? Materials 2021, 14, 6123. [Google Scholar] [CrossRef]
- Elgali, I.; Omar, O.; Dahlin, C.; Thomsen, P. Guided Bone Regeneration: Materials and Biological Mechanisms Revisited. Eur. J. Oral Sci. 2017, 125, 315–337. [Google Scholar] [CrossRef]
- Pontailler, M.; Illangakoon, E.; Williams, G.R.; Marijon, C.; Bellamy, V.; Balvay, D.; Autret, G.; Vanneaux, V.; Larghero, J.; Planat-Benard, V.; et al. Polymer-Based Reconstruction of the Inferior Vena Cava in Rat: Stem Cells or RGD Peptide? Tissue Eng. Part A 2015, 21, 1552–1564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chavda, S.; Levin, L. Human Studies of Vertical and Horizontal Alveolar Ridge Augmentation Comparing Different Types of Bone Graft Materials: A Systematic Review. J. Oral Implantol. 2018, 44, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments. Molecules 2021, 26, 3007. [Google Scholar] [CrossRef] [PubMed]
- Choy, C.S.; Lee, W.F.; Lin, P.Y.; Wu, Y.-F.; Huang, H.-M.; Teng, N.-C.; Pan, Y.-H.; Salamanca, E.; Chang, W.-J. Surface Modified β-Tricalcium Phosphate Enhanced Stem Cell Osteogenic Differentiation in Vitro and Bone Regeneration in Vivo. Sci. Rep. 2021, 11, 9234. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.K.; Ki, M.-R.; Kim, E.H.; Park, C.-J.; Ryu, J.J.; Jang, H.S.; Pack, S.P.; Jo, Y.K.; Jun, S.H. Biosilicated Collagen/β-Tricalcium Phosphate Composites as a BMP-2-Delivering Bone-Graft Substitute for Accelerated Craniofacial Bone Regeneration. Biomater. Res. 2021, 25, 13. [Google Scholar] [CrossRef] [PubMed]
- Montelongo, S.A.; Chiou, G.; Ong, J.L.; Bizios, R.; Guda, T. Development of Bioinks for 3D Printing Microporous, Sintered Calcium Phosphate Scaffolds. J. Mater. Sci. Mater. Med. 2021, 32, 94. [Google Scholar] [CrossRef] [PubMed]
- Pires, L.; da Silva, R.C.; Poli, P.P.; Ruas Esgalha, F.; Hadad, H.; Palin, L.P.; Piquera Santos, A.F.; Teixiera Colombo, L.; Kawamata de Jesus, L.; Bassi, A.P.F.; et al. Evaluation of Osteoconduction of a Synthetic Hydroxyapatite/β-Tricalcium Phosphate Block Fixed in Rabbit Mandibles. Materials 2020, 13, 4902. [Google Scholar] [CrossRef]
- Bhatt, R.A.; Rozental, T.D. Bone graft substitutes. Hand Clin. 2012, 28, 457–468. [Google Scholar] [CrossRef]
- Kao, S.T.; Scott, D.D. A review of bone substitutes. Oral Maxillofac. Surg. Clin. N. Am. 2007, 19, 513–521. [Google Scholar] [CrossRef]
- Kattimani, V.S.; Chakravarthi, P.S.; Prasad, L.K. Biograft Block Hydroxyapatite: A Ray of Hope in the Reconstruction of Maxillofacial Defects. J. Craniofac. Surg. 2016, 27, 247–252. [Google Scholar] [CrossRef]
- Dewi, A.H.; Ana, I.D. The use of hydroxyapatite bone substitute grafting for alveolar ridge preservation, sinus augmentation, and periodontal bone defect: A systematic review. Heliyon 2018, 4, 884. [Google Scholar] [CrossRef] [Green Version]
- Abdul Halim, N.A.; Hussein, M.Z.; Kandar, M.K. Nanomaterials-Upconverted Hydroxyapatite for Bone Tissue Engineering and a Platform for Drug Delivery. Int. J. Nanomed. 2021, 16, 6477–6496. [Google Scholar] [CrossRef] [PubMed]
- Bajuri, M.Y.; Selvanathan, N.; Dzeidee Schaff, F.N.; Abdul Suki, M.H.; Ng, A.M.H. Tissue-Engineered Hydroxyapatite Bone Scaffold Impregnated with Osteoprogenitor Cells Promotes Bone Regeneration in Sheep Model. Tissue Eng. Regen. Med. 2021, 18, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Pittenger, M.F.; Mackay, A.M.; Beck, S.C.; Jaiswal, R.K.; Douglas, R.; Mosca, J.D.; Moorman, M.A.; Simonetti, D.W.; Craig, S.; Marshak, D.R. Multilineage Potential of Adult Human Mesenchymal Stem Cells. Science 1999, 284, 143–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, W.; Ma, X.; Gou, M.; Mei, D.; Zhang, K.; Chen, S. 3D printing of functional biomaterials for tissue engineering. Curr. Opin. Biotechnol. 2016, 40, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Louvrier, A.; Marty, P.; Barrabé, A.; Euvrard, E.; Chatelain, B.; Weber, E.; Meyer, C. How useful is 3D printing in maxillofacial surgery? J. Stomatol. Oral Maxillofac. Surg. 2017, 118, 206–212. [Google Scholar] [CrossRef]
- Kotta, S.; Nair, A.; Alsabeelah, N. 3D Printing Technology in Drug Delivery: Recent Progress and Application. Curr. Pharm. Des. 2018, 24, 5039–5048. [Google Scholar] [CrossRef]
- Prasad, L.K.; Smyth, H. 3D Printing technologies for drug delivery: A review. Drug Dev. Ind. Pharm. 2016, 42, 1019–1031. [Google Scholar] [CrossRef]
- Dubrov, V.E.; Klimashina, E.S.; Shcherbakov, I.M.; Shipunov, G.A.; Putlyaev, V.I.; Evdokimov, P.V.; Tikhonov, A.A.; Zyuzin, D.A.; Danilova, N.V.; Mal’kov, P.G. Experimental Evaluation of the Properties of 3D Porous Bone Substitute Based on Calcium Phosphate on the Model of Monocortical Diaphysial Femur Defect in Rats. Bull. Exp. Biol. Med. 2019, 167, 400–403. [Google Scholar] [CrossRef]
- Franch, J.; Barba, A.; Rappe, K.; Maazouz, Y.; Ginebra, M.-P. Use of three-dimensionally printed β-tricalcium phosphate synthetic bone graft combined with recombinant human bone morphogenic protein-2 to treat a severe radial atrophic nonunion in a Yorkshire terrier. Vet. Surg. 2020, 49, 1626–1631. [Google Scholar] [CrossRef]
- Wang, M.M.; Flores, R.L.; Witek, L.; Torroni, A.; Ibrahim, A.; Wang, Z.; Liss, H.A.; Cronstein, B.N.; Lopez, C.D.; Maliha, S.G.; et al. Dipyridamole-loaded 3D-printed bioceramic scaffolds stimulate pediatric bone regeneration in vivo without disruption of craniofacial growth through facial maturity. Sci. Rep. 2019, 9, 18439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.-H.; Ghayor, C.; Siegenthaler, B.; Schuler, F.; Rüegg, J.; De Wild, M.; Weber, F.E. Lattice Microarchitecture for Bone Tissue Engineering from Calcium Phosphate Compared to Titanium. Tissue Eng. Part A 2018, 24, 1554–1561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tovar, N.; Witek, L.; Atria, P.; Sobieraj, M.; Bowers, M.; Lopez, C.D.; Cronstein, B.N.; Coelho, P.G. Form and functional repair of long bone using 3D-printed bioactive scaffolds. J. Tissue Eng. Regen. Med. 2018, 12, 1986–1999. [Google Scholar] [CrossRef] [PubMed]
- Diao, J.; OuYang, J.; Deng, T.; Liu, X.; Feng, Y.; Zhao, N.; Mao, C.; Wang, Y. 3D-Plotted Beta-Tricalcium Phosphate Scaffolds with Smaller Pore Sizes Improve In Vivo Bone Regeneration and Biomechanical Properties in a Critical-Sized Calvarial Defect Rat Model. Adv. Healthc. Mater. 2018, 7, 1800441. [Google Scholar] [CrossRef]
- Nandi, S.K.; Fielding, G.; Banerjee, D.; Bandyopadhyay, A.; Bose, S. 3D-printed β-TCP bone tissue engineering scaffolds: Effects of chemistry on in vivo biological properties in a rabbit tibia model. J. Mater. Res. 2018, 33, 1939–1947. [Google Scholar] [CrossRef]
- Lopez, C.D.; Diaz-Siso, J.R.; Witek, L.; Bekisz, J.M.; Cronstein, B.N.; Torroni, A.; Flores, R.L.; Rodriguez, E.D.; Coelho, P.G. Three dimensionally printed bioactive ceramic scaffold osseoconduction across critical-sized mandibular defects. J. Surg. Res. 2018, 223, 115–122. [Google Scholar] [CrossRef] [Green Version]
- Atala, A. Introduction: 3D Printing for Biomaterials. Chem. Rev. 2020, 120, 10545–10546. [Google Scholar] [CrossRef]
- ISO 13175-3; Implants for Surgery—Calcium Phosphates Part 3: Hydroxyapatite and Beta-Tricalcium Phosphate Bone Substitutes. The International Organization for Standardization: Geneva, Switzerland, 2012.
- ASTM C1421-15; Standard Test Methods for Determination of Fracture Toughness of Advanced Ceramics at Ambient Temperature. American Society for Testing and Materials International: West Conshohocken, PA, USA, 2015.
- Percie du Sert, N.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The ARRIVE Guidelines 2.0: Updated Guidelines for Reporting Animal Research. PLoS Biol. 2020, 18, e3000410. [Google Scholar] [CrossRef]
- de Siqueira, N.B.; da Silva, A.C.E.; Pereira, R.D.S.; Hochuli-Vieira, E.; Lisboa-Filho, P.N.; de Deus, C.B.D.; Okamoto, R. Different Responses of Heterogeneous Graft Presentations in Bone Reconstructions during Sinus Lift Elevation Surgery: An Immunolabeling and Histomorphometric Study Performed in Rabbits. Front. Oral Maxillofac. Med. 2022, 4, 1. [Google Scholar] [CrossRef]
- Pitol-Palin, L.; de Souza Batista, F.R.; Gomes-Ferreira, P.H.S.; Mulinari-Santos, G.; Ervolino, E.; Souza, F.Á.; Matsushita, D.H.; Okamoto, R. Different Stages of Alveolar Bone Repair Process Are Compromised in the Type 2 Diabetes Condition: An Experimental Study in Rats. Biology 2020, 9, 471. [Google Scholar] [CrossRef]
- Pedrosa, W.F.; Okamoto, R.; Faria, P.E.P.; Arnez, M.F.M.; Xavier, S.P.; Salata, L.A. Immunohistochemical, Tomographic and Histological Study on Onlay Bone Graft Remodeling. Part II: Calvarial Bone. Clin. Oral Implants Res. 2009, 20, 1254–1264. [Google Scholar] [CrossRef]
- Manrique, N.; Pereira, C.C.S.; Luvizuto, E.R.; Sánchez, M.D.P.R.; Okamoto, T.; Okamoto, R.; Sumida, D.H.; Antoniali, C. Hypertension Modifies OPG, RANK, and RANKL Expression during the Dental Socket Bone Healing Process in Spontaneously Hypertensive Rats. Clin. Oral Investig. 2015, 19, 1319–1327. [Google Scholar] [CrossRef] [PubMed]
- Bouxsein, M.L.; Boyd, S.K.; Christiansen, B.A.; Guldberg, R.E.; Jepsen, K.J.; Müller, R. Guidelines for assessment of bone microstructure in rodents using micro-computed tomography. J. Bone Miner. Res. 2010, 25, 1468–1486. [Google Scholar] [CrossRef] [PubMed]
- Langer, R.; Vacanti, J.P. Tissue Engineering. Science 1993, 260, 920–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fatkhudinov, T.; Tsedik, L.; Arutyunyan, I.; Lokhonina, A.; Makarov, A.; Korshunov, A.; Elchaninov, A.; Kananykhina, E.; Vasyukova, O.; Usman, N.; et al. Evaluation of resorbable polydioxanone and polyglycolic acid meshes in a rat model of ventral hernia repair. J. Biomed. Mater. Res. Part B Appl. Biomater. 2019, 107, 652–663. [Google Scholar] [CrossRef]
- Rowland, D.C.; Aquilina, T.; Klein, A.; Hakimi, O.; Alexis-Mouthuy, P.; Carr, A.J.; Snelling, S.J. A comparative evaluation of the effect of polymer chemistry and fiber orientation on mesenchymal stem cell differentiation. J. Biomed. Mater. Res. A 2016, 104, 2843–2853. [Google Scholar] [CrossRef] [Green Version]
- Saska, S.; Pilatti, L.; Blay, A.; Shibli, J.A. Bioresorbable Polymers: Advanced Materials and 4D Printing for Tissue Engineering. Polymers 2021, 13, 563. [Google Scholar] [CrossRef]
- Ai-Aql, Z.S.; Alagl, A.S.; Graves, D.T.; Gerstenfeld, L.C.; Einhorn, T.A. Molecular Mechanisms Controlling Bone Formation during Fracture Healing and Distraction Osteogenesis. J. Dent. Res. 2008, 87, 107–118. [Google Scholar] [CrossRef]
- Batoon, L.; Millard, S.M.; Raggatt, L.J.; Pettit, A.R. Osteomacs and Bone Regeneration. Curr. Osteoporos. Rep. 2017, 15, 385–395. [Google Scholar] [CrossRef]
- Kendal, A.; Snelling, S.; Dakin, S.; Stace, E.; Mouthuy, P.A.; Carr, A. Resorbable electrospun polydioxanone fibers modify the behaviour of cells from both healthy and diseased human tendons. Eur. Cells Mater. 2017, 33, 169–182. [Google Scholar] [CrossRef]
- Lisboa-Filho, P.N.; Gomes-Ferreira, P.H.S.; Batista, F.R.S.; Momesso, G.A.C.; Faverani, L.P.; Okamoto, R. Bone Repair with Raloxifene and Bioglass Nanoceramic Composite in Animal Experiment. Connect. Tissue Res. 2018, 59, 97–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fillingham, Y.; Jacobs, J. Bone grafts and their substitutes. Bone Jt. J. 2016, 98, 6–9. [Google Scholar] [CrossRef]
- Ripamonti, U. Functionalized Surface Geometries Induce: “Bone: Formation by Autoinduction”. Front. Physiol. 2018, 8, 1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levi, B.; Longaker, M.T. Concise review: Adipose-derived stromal cells for skeletal regenerative medicine. Stem Cells 2011, 29, 576–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trávníčková, M.; Bačáková, L. Application of adult mesenchymal stem cells in bone and vascular tissue engineering. Physiol. Res. 2018, 67, 831–850. [Google Scholar] [CrossRef]
- Wessing, B.; Lettner, S.; Zechner, W. Guided Bone Regeneration with Collagen Membranes and Particulate Graft Materials: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implants 2018, 33, 87–100. [Google Scholar] [CrossRef]
- Thrivikraman, G.; Athirasala, A.; Twohig, C.; Boda, S.K.; Bertassoni, L.E. Biomaterials for Craniofacial Bone Regeneration. Dent. Clin. N. Am. 2017, 61, 835–856. [Google Scholar] [CrossRef]
- Suneelkumar, C.; Datta, K.; Srinivasan, M.R.; Kumar, S.T. Biphasic calcium phosphate in periapical surgery. J. Conserv. Dent. 2008, 11, 92–96. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Auto/PG | TCP/PG | HA/PG | |
|---|---|---|---|
| Runx2 | ++ | + | +++ |
| OPN | ++ | ++ | + |
| OCN | ++ | ++ | ++ |
| Trap | + | + | + |
| Auto/PG | TCP/PG | HA/PG | Statistical Difference | |
|---|---|---|---|---|
| BV/TV (%) | 82.710 ± 6.757 | 87.950 ± 1.732 | 84.360 ± 6.323 | no |
| Tb.Th (mm) | 0.2504 ± 0.027 | 0.3318 ± 0.008 | 0.3144 ± 0.049 | Auto/PG vs. TCP/PG = 0.0027 Auto/PG vs. HA/PG = 0.0189 |
| Tb.N (1/mm) | 2.945 ± 0.184 | 2.533 ± 0.247 | 2.700 ± 0.167 | Auto/PG vs. TCP/PG = 0.0351 |
| Tb.Sp (mm) | 0.226 ± 0.043 | 0.170 ± 0.021 | 0.182 ± 0.020 | Auto/PG vs. TCP/PG = 0.0442 |
| Po.Tot (%) | 23.960 ± 7.294 | 12.050 ± 1.732 | 16.120 ± 6.452 | Auto/PG vs. TCP/PG = 0.0214 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pitol-Palin, L.; Frigério, P.B.; Moura, J.; Pilatti, L.; de Oliveira, L.M.J.; Matsubara, E.Y.; Tunchel, S.; Shibli, J.A.; Blay, A.; Saska, S.; et al. Performance of Polydioxanone-Based Membrane in Association with 3D-Printed Bioceramic Scaffolds in Bone Regeneration. Polymers 2023, 15, 31. https://doi.org/10.3390/polym15010031
Pitol-Palin L, Frigério PB, Moura J, Pilatti L, de Oliveira LMJ, Matsubara EY, Tunchel S, Shibli JA, Blay A, Saska S, et al. Performance of Polydioxanone-Based Membrane in Association with 3D-Printed Bioceramic Scaffolds in Bone Regeneration. Polymers. 2023; 15(1):31. https://doi.org/10.3390/polym15010031
Chicago/Turabian StylePitol-Palin, Letícia, Paula Buzo Frigério, Juliana Moura, Livia Pilatti, Letícia Marques Jordão de Oliveira, Elaine Yoshiko Matsubara, Samy Tunchel, Jamil Awad Shibli, Alberto Blay, Sybele Saska, and et al. 2023. "Performance of Polydioxanone-Based Membrane in Association with 3D-Printed Bioceramic Scaffolds in Bone Regeneration" Polymers 15, no. 1: 31. https://doi.org/10.3390/polym15010031