
Role of Biomaterials Used for Periodontal Tissue Regeneration—A Concise Evidence-Based Review


Abstract
:1. Introduction
2. Calcium Phosphate Biomaterials
2.1. Tricalcium Phosphate (TCP)
2.2. Plaster of Paris/Calcium Sulfates
2.3. Bioactive Glass
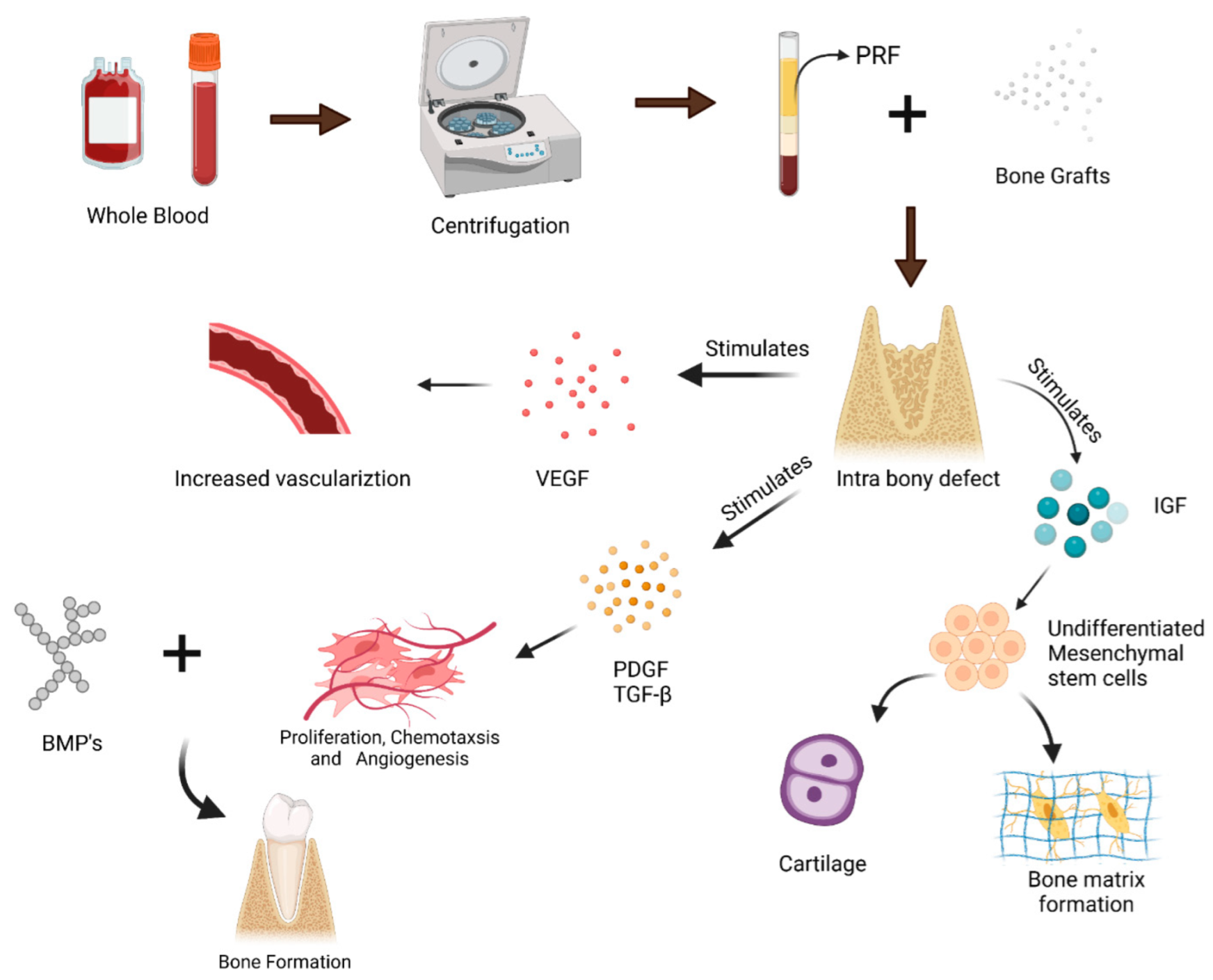
3. Autologous Materials as Regenerative Substitutes for Periodontal Regeneration
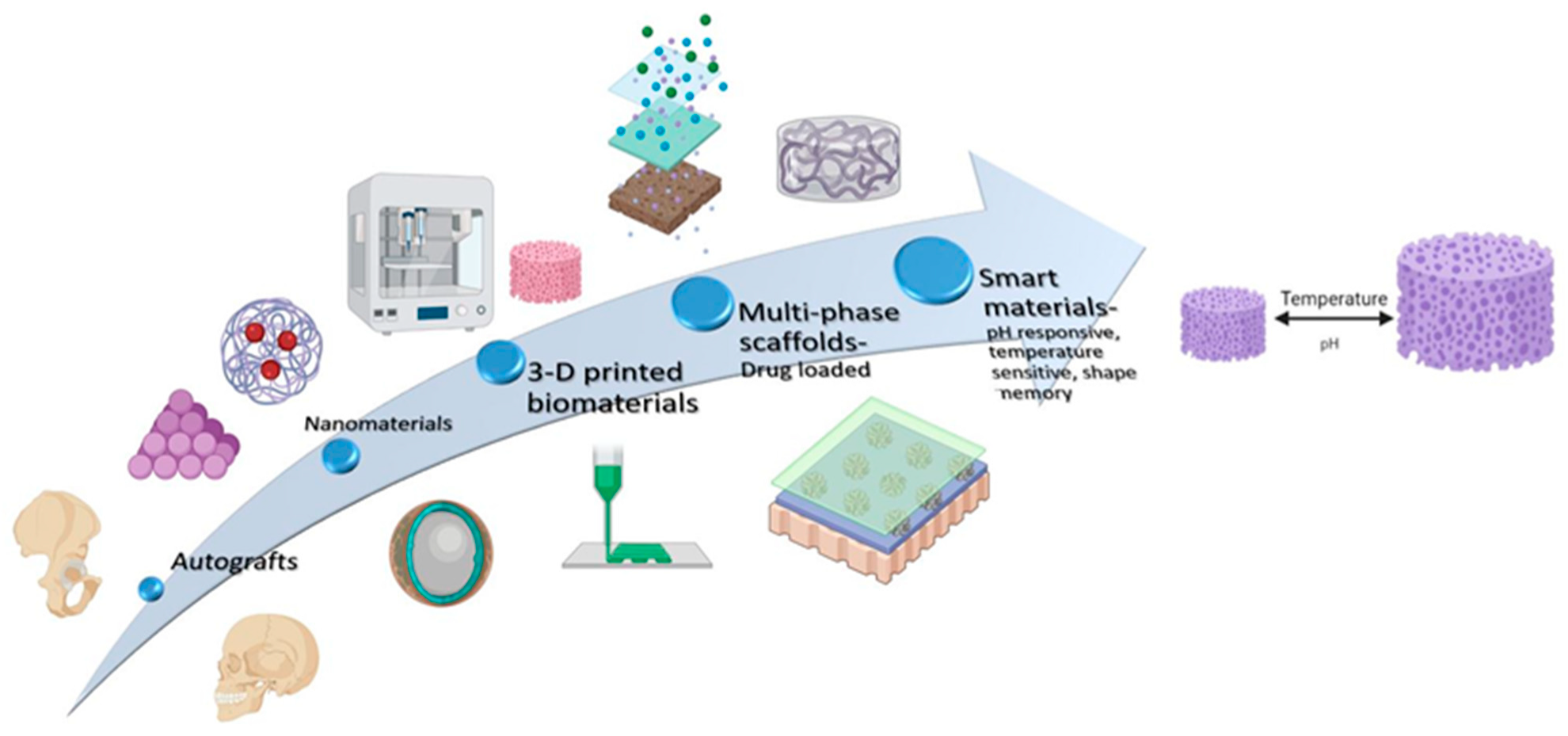
4. Recent Advances in Biomaterials for Periodontal Regeneration
4.1. Innovative Biomaterials Used as Bone Substitutes
4.1.1. Egg-Shell-Derived Nanohydroxyapatite
4.1.2. Metal-Ion-Doped Nanohydroxyapatite
- Silicon-doped hydroxyapatite showed significantly greater bone in-growth and bone implant coverage than undoped hydroxyapatite [96].
4.2. Magnesium Bone Substitutes
4.3. Carbon Nanomaterials
4.4. Titanium Bone Substitutes
5. Innovations in Biomaterials Used for Guided Tissue Regeneration
5.1. Electrospinning
5.1.1. Antibacterial GTR Membranes
5.1.2. Functionally Graded, Multilayered GTR Membranes
6. Innovations in Biomaterial Construction and Design for Tissue Engineering
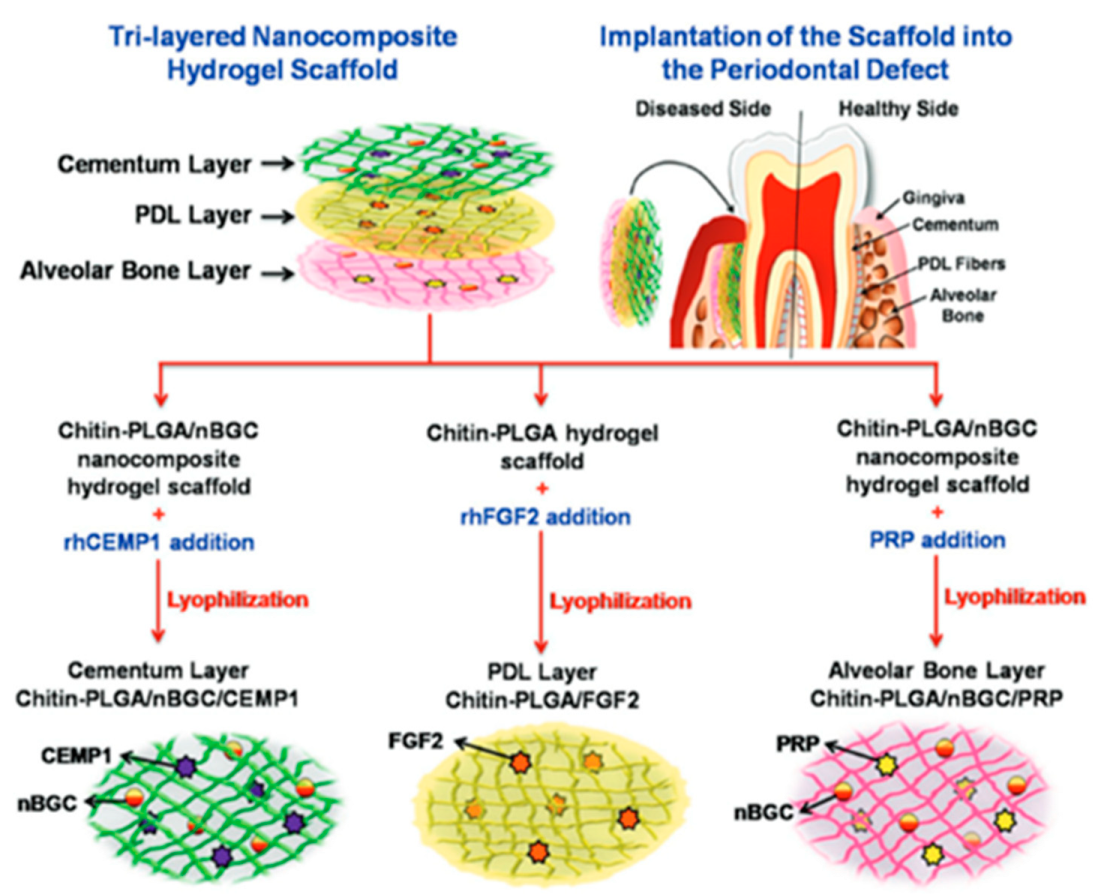
6.1. Trilayered Nanocomposite Hydrogel Scaffold
6.1.1. Sandwich Tissue-Engineered Complex
6.1.2. 3D-Printed Multiphase Scaffold
6.2. Temporal Control of Drug Release
6.3. An Injectable, Immunomodulatory Biomaterial
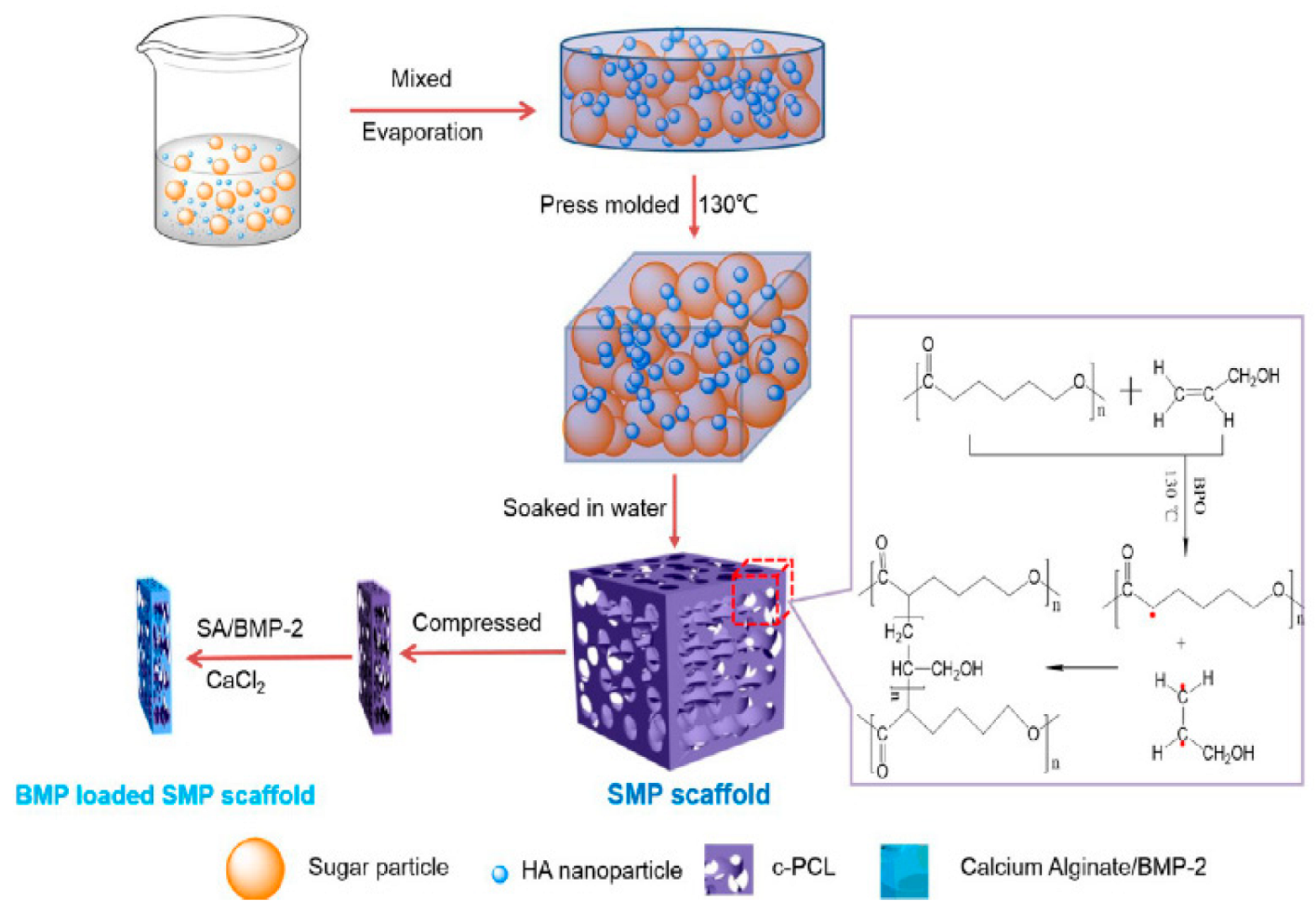
6.4. Smart Biomaterial with Shape Memory
7. Current Frontiers and Future Horizon
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Savage, A.; Eaton, K.A.; Moles, D.R.; Needleman, I. A systematic review of definitions of periodontitis and methods that have been used to identify this disease. J. Clin. Periodontol. 2009, 36, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Nanci, A.; Bosshardt, D.D. Structure of periodontal tissues in health and disease. Periodontology 2000, 40, 11–28. [Google Scholar] [CrossRef] [PubMed]
- McCauley, L.K.; Nohutcu, R.M. Mediators of Periodontal Osseous Destruction and Remodeling: Principles and Implications for Diagnosis and Therapy. J. Periodontol. 2002, 73, 1377–1391. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.J.A.; Trombelli, L.; Heitz, F.; Needleman, I.; Moles, D. A systematic review of the effect of surgical debridement vs. non-surgical debridement for the treatment of chronic periodontitis. J. Clin. Periodontol. 2002, 29 (Suppl. S3), 92–102. [Google Scholar] [CrossRef] [PubMed]
- Shue, L.; Yufeng, Z.; Mony, U. Biomaterials for periodontal regeneration: A review of ceramics and polymers. Biomatter 2012, 2, 271–277. [Google Scholar] [CrossRef] [Green Version]
- Hofmann, G.O.; Kirschner, M.H.; Wangemann, T.; Falk, C.; Mempel, W.; Hammer, C. Infections and immunological hazards of allogeneic bone transplantation. Arch. Orthop. Trauma. Surg. 1995, 114, 159–166. [Google Scholar] [CrossRef]
- Hulbert, S.F.; Hench, L.L.; Forbers, D.; Bowman, L.S. History of bioceramics. In Ceramics in Surgery; Vincenzini, P., Ed.; Elsevier: Amsterdam, The Netherlands, 1983; pp. 3–29. [Google Scholar]
- Hench, L.L. Bioceramics: From Concept to Clinic. J. Am. Ceram. Soc. 1991, 74, 1487–1510. [Google Scholar] [CrossRef]
- Kanazawa, T.; Umegaki, T.; Monma, H. Apatite, New inorganic materials. Ceram. Jpn. 1975, 10, 461–468. [Google Scholar]
- Müller, P.; Bulnheim, U.; Diener, A.; Lüthen, F.; Teller, M.; Klinkenberg, E.-D.; Neumann, H.-G.; Nebe, B.; Liebold, A.; Steinhoff, G.; et al. Calcium phosphate surfaces promote osteogenic differentiation of mesenchymal stem cells. J. Cell. Mol. Med. 2008, 12, 281–291. [Google Scholar] [CrossRef] [Green Version]
- Shih, Y.-R.V.; Hwang, Y.; Phadke, A.; Kang, H.; Hwang, N.S.; Caro, E.J.; Nguyen, S.; Siu, M.; Theodorakis, E.A.; Gianneschi, N.C.; et al. Calcium phosphate-bearing matrices induce osteogenic differentiation of stem cells through adenosine signaling. Proc. Natl. Acad. Sci. USA 2014, 111, 990–995. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Li, Y.; Zuo, Y.; Li, J.; Ma, S.; Cheng, L. Biocompatibility and osteogenesis of biomimetic nano-hydroxyapatite/polyamide composite scaffolds for bone tissue engineering. Biomaterials 2007, 28, 3338–3348. [Google Scholar] [CrossRef] [PubMed]
- Carson, J.S.; Bostrom, M.P. Synthetic bone scaffolds and fracture repair. Injury 2007, 38, S33–S37. [Google Scholar] [CrossRef] [PubMed]
- Martinetti, R.; Dolcini, L.; Mangano, C. Physical and chemical aspects of a new porous hydroxyapatite. Anal. Bioanal. Chem. 2005, 381, 634–638. [Google Scholar] [CrossRef]
- Ogilvie, A.; Frank, R.M.; Benque, E.P.; Gineste, M.; Heughebaert, M.; Hemmerle, J. The biocompatibility of hydroxyapatite implanted in the human periodontium. J. Periodontal Res. 1987, 22, 270–283. [Google Scholar] [CrossRef] [PubMed]
- Ghanaati, S.; Kirkpatrick, C.J.; Kovács, A.F.; Landes, C.; Lorenz, J.; Sader, R.A.; Seitz, O.; Stuebinger, S.; Barbeck, M. Synthetic bone substitute material comparable with xenogeneic material for bone tissue regeneration in oral cancer patients: First and preliminary histological, histomorphometrical and clinical results. Ann. Maxillofac. Surg. 2013, 3, 126–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bordea, I.R.; Candrea, S.; Alexescu, G.T.; Bran, S.; Băciuț, M.; Băciuț, G.; Lucaciu, O.; Dinu, C.M.; Todea, D.A. Nano-hydroxyapatite use in dentistry: A systematic review. Drug Metab. Rev. 2020, 52, 319–332. [Google Scholar] [CrossRef]
- Metsger, D.S.; Driskell, T.D.; Paulsrud, J.R. Tricalcium Phosphate Ceramic—A Resorbable Bone Implant: Review and Current Status. J. Am. Dent. Assoc. 1982, 105, 1035–1038. [Google Scholar] [CrossRef]
- Tosta, M.; Cortes, A.R.G.; Corrêa, L.; Pinto, D.D.S., Jr.; Tumenas, I.; Katchburian, E. Histologic and histomorphometric evaluation of a synthetic bone substitute for maxillary sinus grafting in humans. Clin. Oral Implant. Res. 2013, 24, 866–870. [Google Scholar] [CrossRef]
- Snyder, A.J.; Levin, M.P.; Cutright, D.E. Alloplastic Implants of Tricalcium Phosphate Ceramic in Human Periodontal Osseous Defects. J. Periodontol. 1984, 55, 273–277. [Google Scholar] [CrossRef]
- LeGeros, R.Z.; Lin, S.; Rohanizadeh, R.; Mijares, D.; LeGeros, J.P. Biphasic calcium phosphate bioceramics: Preparation, properties and applications. J. Mater. Sci. Mater. Med. 2003, 14, 201–209. [Google Scholar] [CrossRef]
- Wang, L.; Shi, H.; Chen, Y.; Xue, J.; Chen, Y.; Liao, Y. Healing of acute alveolar bone dehiscence following treatment with porous biphasic calcium phosphate in beagle dogs. Clin. Oral Investig. 2011, 15, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Daculsi, G.; LeGeros, R.Z.; Nery, E.; Lynch, K.; Kerebel, B. Transformation of biphasic calcium phosphate ceramicsin vivo: Ultrastructural and physicochemical characterization. J. Biomed. Mater. Res. 1989, 23, 883–894. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Mahendra, J.; Samuel, S.; Govindraj, J.; Loganathan, T.; Vashum, Y.; Mahendra, L.; Krishnamoorthy, T. Platelet-rich fibrin/biphasic calcium phosphate impairs osteoclast differentiation and promotes apoptosis by the intrinsic mitochondrial pathway in chronic periodontitis. J. Periodontol. 2018, 90, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Dreesmann, H. Knochenplombierung Bei Hohlenforigen Defekten Des Knochens. Beitr. Klin. Chir. 1892, 9, 804–810. [Google Scholar]
- Peltier, L.F. The use of plaster of paris to fill large defects in bone: A preliminary report. Am. J. Surg. 1959, 97, 311–315. [Google Scholar] [CrossRef]
- Scarano, A.; Orsini, G.; Pecora, G.; Iezzi, G.; Perrotti, V.; Piattelli, A. Peri-Implant Bone Regeneration with Calcium Sulfate: A Light and Transmission Electron Microscopy Case Report. Implant Dent. 2007, 16, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Al Ruhaimi, K.A. Effect of adding resorbable calcium sulfate to grafting materials on early bone regeneration in osseous defects in rabbits. Int. J. Oral Maxillofac. Implant. 2000, 15, 801–810. [Google Scholar]
- Payne, J.M.; Cobb, C.M.; Rapley, J.W.; Killoy, W.J.; Spencer, P. Migration of Human Gingival Fibroblasts Over Guided Tissue Regeneration Barrier Materials. J. Periodontol. 1996, 67, 236–244. [Google Scholar] [CrossRef]
- Aichelmann-Reidy, M.E.; Heath, C.D.; Reynolds, M.A. Clinical Evaluation of Calcium Sulfate in Combination with Demineralized Freeze-Dried Bone Allograft for the Treatment of Human Intraosseous Defects. J. Periodontol. 2004, 75, 340–347. [Google Scholar] [CrossRef]
- Maragos, P.; Bissada, N.F.; Wang, R.; Cole, B.P. Comparison of three methods using calcium sulfate as a graft/barrier material for the treatment of Class II mandibular molar furcation defects. Int. J. Periodontics Restor. Dent. 2002, 22, 493–501. [Google Scholar]
- Mohammed, A.A.; Elsherbini, A.M.; Ibrahim, F.M.; El-Meadawy, S.M.; Youssef, J.M. Biological effect of the nanocrystalline calcium sulfate bone graft in the periodontal regeneration. J. Oral Biol. Craniofacial Res. 2020, 11, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Hench, L.L. The Story of Bioglass®. J. Mater. Sci. Mater. Med. 2006, 17, 967–978. [Google Scholar] [CrossRef] [PubMed]
- Sohrabi, K.; Saraiya, V.; Laage, T.A.; Harris, M.; Blieden, M.; Karimbux, N. An Evaluation of Bioactive Glass in the Treatment of Periodontal Defects: A Meta-Analysis of Randomized Controlled Clinical Trials. J. Periodontol. 2012, 83, 453–464. [Google Scholar] [CrossRef]
- Cannio, M.; Bellucci, D.; Roether, J.A.; Boccaccini, D.N.; Cannillo, V. Bioactive Glass Applications: A Literature Review of Human Clinical Trials. Materials 2021, 14, 5440. [Google Scholar] [CrossRef] [PubMed]
- Schepers, E.J.G.; Ducheyne, P. Bioactive glass particles of narrow size range for the treatment of oral bone defects: A 1–24 month experiment with several materials and particle sizes and size ranges. J. Oral Rehabil. 1997, 24, 171–181. [Google Scholar] [CrossRef]
- Villaça, J.H.; Novaes, A.B., Jr.; De Souza, S.L.S.; Taba, M., Jr.; Molina, G.O.; Carvalho, T.L.L.; Novaes, A.B.; Taba, M. Bioactive Glass Efficacy in the Periodontal Healing of Intrabony Defects in Monkeys. Braz. Dent. J. 2005, 16, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Lohmann, C.H.; Andreacchio, D.; Köster, G.; Carnes, D.L., Jr.; Cochran, D.L.; Dean, D.D.; Boyan, B.D.; Schwartz, Z. Tissue Response and Osteoinduction of Human Bone Grafts in Vivo. Arch. Orthop. Trauma. Surg. 2001, 121, 583–590. [Google Scholar] [CrossRef]
- Reynolds, M.A.; Aichelmann-Reidy, M.E.; Branch-Mays, G.L. Regeneration of Periodontal Tissue: Bone Replacement Grafts. Dent. Clin. N. Am. 2010, 54, 55–71. [Google Scholar] [CrossRef]
- Cortellini, P.; Labriola, A.; Tonetti, M.S. Regenerative periodontal therapy in intrabony defects: State of the art. Minerva Stomatol. 2007, 56, 519–539. [Google Scholar]
- Miron, R.J.; Choukroun, J. Uses of Platelet rich fibrin in Regenerative Dentistry: An Overview. In Platelet Rich Fibrin in Regenerative Dentistry: Biological Background and Clinical Indications; John, Wiley and Sons: Hoboken, NJ, USA, 2017. [Google Scholar] [CrossRef]
- Hollander, A.; Macchiarini, P.; Gordijn, B.; Birchall, M. The first stem cell-based tissue-engineered organ replacement: Implications for regenerative medicine and society. Regen. Med. 2009, 4, 147–148. [Google Scholar] [CrossRef] [Green Version]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2006, 101, e37–e44. [Google Scholar] [CrossRef] [PubMed]
- Christgau, M.; Moder, D.; Hiller, K.-A.; Dada, A.; Schmitz, G.; Schmalz, G. Growth factors and cytokines in autologous platelet concentrate and their correlation to periodontal regeneration outcomes. J. Clin. Periodontol. 2006, 33, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Song, J.S.; Kim, S.-O.; Kim, S.-H.; Choi, H.-J.; Son, H.-K.; Jung, H.-S.; Kim, C.-S.; Lee, J.-H. In Vitro and In Vivo Characteristics of Stem Cells Derived from the Periodontal Ligament of Human Deciduous and Permanent Teeth. Tissue Eng. Part A 2012, 18, 2040–2051. [Google Scholar] [CrossRef] [PubMed]
- Serroni, M.; Paolantonio, M.; Romano, L.; Santamaria, P.; Rexhepi, I.; Sinjari, B.; Paolantonio, G.; Secondi, L.; De Ninis, P.; Femminella, B. Added benefit of L-PRF to autogenous bone grafts in the treatment of degree II furcation involvement in mandibular molars. J. Periodontol. 2022, 1–14. [Google Scholar] [CrossRef]
- Rexhepi, I.; Paolantonio, M.; Romano, L.; Serroni, M.; Santamaria, P.; Secondi, L.; Paolantonio, G.; Sinjari, B.; De Ninis, P.; Femminella, B. Efficacy of inorganic bovine bone combined with leukocyte and platelet-rich fibrin or collagen membranes for treating unfavorable periodontal infrabony defects: Randomized non-inferiority trial. J. Periodontol. 2021, 92, 1576–1587. [Google Scholar] [CrossRef]
- Fujioka-Kobayashi, M.; Miron, R.J.; Hernandez, M.; Kandalam, U.; Zhang, Y.; Choukroun, J. Optimized Platelet-Rich Fibrin with the Low-Speed Concept: Growth Factor Release, Biocompatibility, and Cellular Response. J. Periodontol. 2017, 88, 112–121. [Google Scholar] [CrossRef]
- Suwondo, C.I.; Herawati, D.; Sudibyo, S. Effect of advanced platelet-rich fibrin applications on periodontal regeneration in infrabony pocket treatment. Maj. Kedokt. Gigi Indones. 2019, 4, 154–160. [Google Scholar] [CrossRef] [Green Version]
- Lei, L.; Yu, Y.; Han, J.; Shi, D.; Sun, W.; Zhang, D.; Chen, L. Quantification of growth factors in advanced platelet-rich fibrin and concentrated growth factors and their clinical efficacy as adjunctive to the GTR procedure in periodontal intrabony defects. J. Periodontol. 2020, 91, 462–472. [Google Scholar] [CrossRef]
- O’connell, S.M. Safety Issues Associated with Platelet-Rich Fibrin Method. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2007, 103, 587–593. [Google Scholar] [CrossRef]
- Tunalı, M.; Özdemir, H.; Küçükodacı, Z.; Akman, S.; Yaprak, E.; Toker, H.; Fıratlı, E. A novel platelet concentrate: Titanium-prepared platelet-rich fibrin. Biomed Res. Int. 2014, 2014, 209548. [Google Scholar] [CrossRef]
- Tunalı, M.; Özdemir, H.; Küçükodacı, Z.; Akman, S.; Fıratlı, E. In vivo evaluation of titanium-prepared platelet-rich fibrin (t-prf): A new platelet concentrate. Br. J. Oral. Maxillofac. Surg. 2013, 51, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Gummaluri, S.S.; Bhattacharya, H.S.; Astekar, M.; Cheruvu, S. Evaluation of titanium-prepared platelet-rich fibrin and leucocyteplatelet-rich fibrin in the treatment of intra-bony defects: Arandomized clinical trial. J. Dent. Res. Dent. Clin. Dent. Prospect. 2020, 14, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Lourenço, E.S.; Mourão, C.F.; Leite, P.E.; Granjeiro, J.; Calasans-Maia, M.D.; Alves, G.G. Thein vitrorelease of cytokines and growth factors from fibrin membranes produced through horizontal centrifugation: Characterization of l-prf-like fibrin membranes. J. Biomed. Mater. Res. Part A 2018, 106, 1373–1380. [Google Scholar] [CrossRef]
- Horváthy, D.B.; Simon, M.; Schwarz, C.M.; Masteling, M.; Vácz, G.; Hornyák, I.; Lacza, Z. Serum albumin as a local therapeutic agent in cell therapy and tissue engineering. BioFactors 2017, 43, 315–330. [Google Scholar] [CrossRef] [PubMed]
- De Almeida Barros Mourão, C.; Gheno, E.; Lourenço, E.S.; Barbosa, R.L.; Kurtzman, G.; Javid, K.; Mavropoulos, E.; Benedicenti, S.; Calasans-Maia, M.; de Mello Machado, R.C.; et al. Characterization of a new membrane from concentrated growth factors associated with denaturized Albumin (Alb-CGF) for clinical applications: A preliminary study. Int. J. Growth Factors Stem Cells Dent. 2018, 1, 64–69. [Google Scholar] [CrossRef]
- Fujioka-Kobayashi, M.; Schaller, B.; De Almeida Barros Mourão, C.F.; Zhang, Y.; Sculean, A.; Miron, R.J. Biological characterization of an injectable platelet-rich fibrin mixture consisting of autologous albumin gel and liquid platelet-rich fibrin (Alb-PRF). Platelets 2021, 32, 74–81. [Google Scholar] [CrossRef]
- Fujioka-Kobayashi, M.; Miron, R.J. Biological components of platelet rich fibrin: Growth factor release and cellular activity. In Platelet Rich Fibrin in Regenerative Dentistry: Biological Background and Clinical Indications; John, Wiley and Sons: Hoboken, NJ, USA, 2017; pp. 15–31. [Google Scholar]
- Turer, O.U.; Ozcan, M.; Alkaya, B.; Surmeli, S.; Seydaoglu, G.; Haytac, M.C. Clinical evaluation of injectable platelet-rich fibrin with connective tissue graft for the treatment of deep gingival recession defects: A controlled randomized clinical trial. J. Clin. Periodontol. 2020, 47, 72–80. [Google Scholar] [CrossRef]
- Aydinyurt, H.S.; Sancak, T.; Taskin, C.; Basbugan, Y.; Akinci, L. Effects of ınjectable platelet-rich fibrin in experimental periodontitis in rats. Odontology 2021, 109, 422–432. [Google Scholar] [CrossRef]
- Ozawa, Y.; Kubota, T.; Yamamoto, T.; Tsukune, N.; Koshi, R.; Nishida, T.; Asano, M.; Sato, S. Comparison of the bone augmentation ability of absorbable collagen sponge with that of hydroxyapatite/collagen composite. J. Oral Sci. 2018, 60, 514–518. [Google Scholar] [CrossRef]
- Leventis, M.; Agrogiannis, G.; Fairbairn, P.; Vasiliadis, O.; Papavasileiou, D.; Theodoropoulou, E.; Horowitz, R.; Kalyvas, D. Evaluation of an in situ hardening β-tricalcium phosphate graft material for alveolar ridge preservation. a histomorphometric animal study in pigs. J. Dent. 2018, 6, 27. [Google Scholar] [CrossRef] [Green Version]
- Kizildağ, A.; Arabaci, T.; Köse, O.; Çiçek, Y. The effect of leukocyte-platelet-rich fibrin on bone morphogenetic protein-2 and insulin-like growth factor-1 levels in patients with chronic periodontitis: A randomized split mouth clinical trail. Growth Factors 2018, 36, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Matsuura, T.; Akizuki, T.; Hoshi, S.; Shujaa Addin, A.; Fukuba, S.; Izumi, Y. Ridge preservation of extraction sockets with buccal bone deficiency using poly lactide-co-glycolide coated β-tricalcium phosphate bone grafts: An experimental study in dogs. J. Periodontol. 2019, 90, 1014–1022. [Google Scholar] [CrossRef] [PubMed]
- Sapata, V.M.; Llanos, A.H.; Neto, J.B.C.; Jung, R.E.; Thoma, D.S.; Ch, C.H.H.; Pannuti, C.M.; Romito, G.A.; Re, R.E.J. Deproteinized bovine bone mineral is non-inferior to deproteinized bovine bone mineral with 10% collagen in maintaining the soft tissue contour post-extraction: A randomized trial. Clin. Oral Implant. Res. 2020, 31, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Bodhare, G.H.; Kolte, A.P.; Kolte, R.A.; Shirke, P.Y. Clinical and radiographic evaluation and comparison of bioactive bone alloplast morsels when used alone and in combination with platelet-rich fibrin in the treatment of periodontal intrabony defects—A randomized controlled trial. J. Periodontol. 2019, 90, 584–594. [Google Scholar] [CrossRef]
- Atchuta, A.; Gooty, J.R.; Guntakandla, V.R.; Palakuru, S.K.; Durvasula, S.; Palaparthy, R. Clinical and radiographic evaluation of platelet-rich fibrin as an adjunct to bone grafting demineralized freeze-dried bone allograft in intrabony defects. J. Indian Soc. Periodontol. 2020, 24, 60. [Google Scholar] [CrossRef]
- Liu, K.-N.; Huang, Z.; Chen, Z.-B.; Han, B.; Ouyang, X.-Y. Treating periodontal intrabony defects using guided tissue regeneration and Bio-Oss® with platelet-rich fibrin: Study protocol for a self-controlled trial. Clin. Trials Orthop. Disord. 2020, 5, 9–13. [Google Scholar] [CrossRef]
- Thakkar, B.; Chandran, S.; Vishnoi, S.; Nadig, P.; Raval, R.; Doshi, P. Comparison of Regenerative Potential of Platelet-rich Fibrin Alone and in Combination with Bovine Bone Graft in Intraosseous Defect by Single Flap Approach: A Clinical and Radiographic Study. J. Int. Soc. Prev. Community Dent. 2020, 10, 743–751. [Google Scholar]
- Bahammam, M.A.; Attia, M.S. Expression of Vascular Endothelial Growth Factor Using Platelet Rich Fibrin (PRF) and Nanohydroxyapatite (nano-HA) in Treatment of Periodontal Intra-Bony Defects–A Randomized Controlled Trial. Saudi J. Biol. Sci. 2021, 28, 870–878. [Google Scholar] [CrossRef]
- Janardhanan, N.; Apine, A.A.; Bilichodmath, S. Comparison of Bioactive Glass Bone Graft (Putty) with Autologous Platelet-rich Fibrin in the Treatment of Intrabony Defects. J. Health Sci. Res. 2020, 11, 42–52. [Google Scholar] [CrossRef]
- Paolantonio, M.; Di Tullio, M.; Giraudi, M.; Romano, L.; Secondi, L.; Paolantonio, G.; Graziani, F.; Pilloni, A.; De Ninis, P.; Femminella, B. Periodontal regeneration by leukocyte and platelet-rich fibrin with autogenous bone graft versus enamel matrix derivative with autogenous bone graft in the treatment of periodontal intrabony defects: A randomized non-inferiority trial. J. Periodontol. 2020, 91, 1595–1608. [Google Scholar] [CrossRef]
- Lee, J.; Jeong, S. Long-term stability of adjunctive use of enamel matrix protein derivative on porcine-derived xenograft for the treatment of one-wall intrabony defects: A 4-year extended follow-up of a randomized controlled trial. J. Periodontol. 2021, 91, 880–889. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, S.; Debnath, S.; Siddeshappa, S.T.; Yeltiwar, R.K.; Dewan, V. Efficacy of Calcium Phosphate Composite Bone Graft in Treatment of Periodontal Intrabony Defects: Clinico-radiographic Study. J. Nepal. Soc. Periodontol. Oral Implant. 2021, 5, 39–44. [Google Scholar] [CrossRef]
- Pavani, M.P.; Reddy, K.R.K.M.; Reddy, B.H.; Biraggari, S.K.; Babu, C.H.C.; Chavan, V. Evaluation of platelet-rich fibrin and tricalcium phosphate bone graft in bone fill of intrabony defects using cone-beam computed tomography: A randomized clinical trial. J. Indian Soc. Periodontol. 2021, 25, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Razi, M.A.; Siddiqui, S.; Mahajan, A.; Qamar, S.; Kumari, P.; Kumari, S. Effectiveness of platelet-rich fibrin in the treatment of intrabony defects with or without bone graft: A clinical comparative study. J. Pharm. Bioallied Sci. 2021, 13 (Suppl. S2), S1350. [Google Scholar]
- Siegel, R.W.; Fougere, G.E. Mechanical properties of nanophase metals. Nanostruct. Mater. 1995, 6, 205–216. [Google Scholar] [CrossRef] [Green Version]
- Shi, Z.; Huang, X.; Cai, Y.; Tang, R.; Yang, D. Size effect of hydroxyapatite nanoparticles on proliferation and apoptosis of osteoblast-like cells. Acta Biomater. 2009, 5, 338–345. [Google Scholar] [CrossRef]
- Webster, T.J.; Siegel, R.W.; Bizios, R. Osteoblast adhesion on nanophase ceramics. Biomaterials 1999, 20, 1221–1227. [Google Scholar] [CrossRef]
- Sato, M.; Aslani, A.; Sambito, M.A.; Kalkhoran, N.M.; Slamovich, E.B.; Webster, T.J. Nanocrystalline hydroxyapatite/titania coatings on titanium improves osteoblast adhesion. J. Biomed. Mater. Res. Part A 2008, 84, 265–272. [Google Scholar] [CrossRef]
- Maxwell, T.H.; Hincke, M.T.; Nys, Y.; Gautron, J.; Mann, K.; Rodriguez-Navarro, A.B.; McKee, M.D. The eggshell: Structure, composition and mineralization. Front. Biosci. 2012, 17, 1266–1280. [Google Scholar] [CrossRef] [Green Version]
- Opris, H.; Bran, S.; Dinu, C.; Baciut, M.; Prodan, D.A.; Mester, A.; Baciut, G. Clinical applications of avian eggshell-derived hydroxyapatite. Bosn. J. Basic Med. Sci. 2020, 20, 430–437. [Google Scholar] [CrossRef]
- Al Anashar, A.; Daoud, A. Evaluation of the activity of hen eggshell graft in experimentally induced mandibular defects in rabbits: Pilot study. Int. J. Res. Med. Sci. 2019, 7, 1133–1135. [Google Scholar] [CrossRef]
- Salama, R.; Khashaba, M.; El Rouby, D. Histomorphometric evaluation of a nano-sized eggshell-containing supplement as a natural alloplast: An animal study. Saudi Dent. J. 2019, 31, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Kattimani, V.S.; Lingamaneni, K.P.; Kreedapathi, G.E.; Kattappagari, K.K. Socket preservation using eggshell-derived nanohydroxyapatite with platelet-rich fibrin as a barrier membrane: A new technique. J. Korean Assoc. Oral Maxillofac. Surg. 2019, 45, 332–342. [Google Scholar] [CrossRef] [PubMed]
- Kattimani, V.S.; Lingamaneni, K.P. Natural bioceramics: Our experience with changing perspectives in the reconstruction of maxillofacial skeleton. J. Korean Assoc. Oral Maxillofac. Surg. 2019, 45, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Kattimani, V.; Lingamaneni, K.P.; Yalamanchili, S.; Mupparapu, M. Use of eggshell-derived nano-hydroxyapatite as novel bone graft substitute–A randomized controlled clinical study. J. Biomater. Appl. 2019, 34, 597–614. [Google Scholar] [CrossRef]
- Aina, V.; Bergandi, L.; Lusvardi, G.; Malavasi, G.; Imrie, F.E.; Gibson, I.R.; Cerrato, G.; Ghigo, D. Sr-containing hydroxyapatite: Morphologies of HA crystals and bioactivity on osteoblast cells. Mater. Sci. Eng. C 2013, 33, 1132–1142. [Google Scholar] [CrossRef]
- Wang, Q.; Li, P.; Tang, P.; Ge, X.; Ren, F.; Zhao, C.; Fang, J.; Wang, K.; Fang, L.; Li, Y.; et al. Experimental and simulation studies of strontium/fluoride-codoped hydroxyapatite nanoparticles with osteogenic and antibacterial activities. Colloids Surf. B Biointerfaces 2019, 182, 110359. [Google Scholar] [CrossRef]
- Chopra, V.; Thomas, J.; Sharma, A.; Panwar, V.; Kaushik, S.; Sharma, S.; Porwal, K.; Kulkarni, C.; Rajput, S.; Singh, H.; et al. Synthesis and Evaluation of a Zinc Eluting rGO/Hydroxyapatite Nanocomposite Optimized for Bone Augmentation. ACS Biomater. Sci. Eng. 2020, 6, 6710–6725. [Google Scholar] [CrossRef]
- Maleki-Ghaleh, H.; Siadati, M.H.; Fallah, A.; Koc, B.; Kavanlouei, M.; Khademi-Azandehi, P.; Moradpur-Tari, E.; Omidi, Y.; Barar, J.; Beygi-Khosrowshahi, Y.; et al. Antibacterial and Cellular Behaviors of Novel Zinc-Doped Hydroxyapatite/Graphene Nanocomposite for Bone Tissue Engineering. Int. J. Mol. Sci. 2021, 22, 9564. [Google Scholar] [CrossRef]
- Yuan, Q.; Xu, A.; Zhang, Z.; Chen, Z.; Wan, L.; Shi, X.; Lin, S.; Yuan, Z.; Deng, L. Bioactive silver doped hydroxyapatite composite coatings on metal substrates: Synthesis and characterization. Mater. Chem. Phys. 2018, 218, 130–139. [Google Scholar] [CrossRef]
- Bai, X.; Sandukas, S.; Appleford, M.; Ong, J.L.; Rabiei, A. Antibacterial effect and cytotoxicity of Ag-doped functionally graded hydroxyapatite coatings. J. Biomed. Mater. Res. Part B Appl. Biomater. 2012, 100, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Sandukas, S.; Yamamoto, A.; Rabiei, A. Osteoblast adhesion to functionally graded hydroxyapatite coatings doped with silver. J. Biomed. Mater. Res. Part A 2011, 97, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Best, S.M.; Bonfield, W.; Gibson, I.; Hing, K.A.; Damien, E.; Revell, P.A. A comparative study on the in vivo behavior of hydroxyapatite and silicon substituted hydroxyapatite granules. J. Mater. Sci. Mater. Med. 2002, 13, 1199–1206. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Wan, P.; Tan, L.L.; Wang, K.; Yang, K. Preclinical investigation of an innovative magnesium-based bone graft substitute for potential orthopaedic applications. J. Orthop. Transl. 2014, 2, 139–148. [Google Scholar] [CrossRef] [Green Version]
- Eivazzadeh-Keihan, R.; Maleki, A.; de la Guardia, M.; Bani, M.S.; Chenab, K.K.; Pashazadeh-Panahi, P.; Baradaran, B.; Mokhtarzadeh, A.; Hamblin, M.R. Carbon based nanomaterials for tissue engineering of bone: Building new bone on small black scaffolds: A review. J. Adv. Res. 2019, 18, 185–201. [Google Scholar] [CrossRef] [PubMed]
- Khalid, P.; Suman, V.B. Carbon Nanotube-Hydroxyapatite Composite for Bone Tissue Engineering and Their Interaction with Mouse Fibroblast L929 In Vitro. J. Bionanosci. 2017, 11, 233–240. [Google Scholar] [CrossRef]
- Tutak, W.; Chhowalla, M.; Sesti, F. The chemical and physical characteristics of single-walled carbon nanotube film impact on osteoblastic cell response. Nanotechnology 2010, 21, 315102. [Google Scholar] [CrossRef]
- Pei, B.; Wang, W.; Dunne, N.; Li, X. Applications of Carbon Nanotubes in Bone Tissue Regeneration and Engineering: Superiority, Concerns, Current Advancements, and Prospects. Nanomaterials 2019, 9, 1501. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Zhu, Z.; Xiao, W.; Li, L. Multi-Walled Carbon Nanotubes Promote Cementoblast Differentiation and Mineralization through the TGF-β/Smad Signaling Pathway. Int. J. Mol. Sci. 2015, 16, 3188–3201. [Google Scholar] [CrossRef] [Green Version]
- Haroun, A.A.; Zaki, B.M.; Shalash, M.; Morsy, R.A.A. Preparation and Histological Study of Multi-Walled Carbon Nanotubes Bone Graft in Management of Class II Furcation Defects in Dogs. Open Access Maced. J. Med. Sci. 2019, 7, 3634–3641. [Google Scholar] [CrossRef] [Green Version]
- Hong, J.; Azens, A.; Ekdahl, K.N.; Granqvist, C.G.; Nilsson, B. Material-specific thrombin generation following contact between metal surfaces and whole blood. Biomaterials 2005, 26, 1397–1403. [Google Scholar] [CrossRef] [PubMed]
- Gorbet, M.B.; Sefton, M.V. Biomaterial-associated thrombosis: Roles of coagulation factors, complement, platelets and leukocytes. Biomaterials 2004, 25, 5681–5703. [Google Scholar] [CrossRef] [PubMed]
- Wohlfahrt, J.C.; Aass, A.M.; Rønold, H.J.; Heijl, L.; Haugen, H.J.; Lyngstadaas, S.P. Microcomputed Tomographic and Histologic Analysis of Animal Experimental Degree II Furcation Defects Treated with Porous Titanium Granules or Deproteinized Bovine Bone. J. Periodontol. 2012, 83, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Wohlfahrt, J.C.; Lyngstadaas, S.P.; Heijl, L.; Aass, A.M. Porous Titanium Granules in the Treatment of Mandibular Class II Furcation Defects: A Consecutive Case Series. J. Periodontol. 2012, 83, 61–69. [Google Scholar] [CrossRef]
- Xue, J.; Wu, T.; Dai, Y.; Xia, Y. Electrospinning and Electrospun Nanofibers: Methods, Materials, and Applications. Chem. Rev. 2019, 119, 5298–5415. [Google Scholar] [CrossRef]
- Sun, B.; Long, Y.Z.; Zhang, H.D.; Li, M.; Duvail, J.-L.; Jiang, X.Y.; Yin, H.L. Advances in three-dimensional nanofibrous macrostructures via electrospinning. Prog. Polym. Sci. 2014, 39, 862–890. [Google Scholar] [CrossRef]
- Xue, J.; Xie, J.; Liu, W.; Xia, Y. Electrospun Nanofibers: New Concepts, Materials, and Applications. Acc. Chem. Res. 2017, 50, 1976–1987. [Google Scholar] [CrossRef]
- Zhuang, Y.; Lin, K.; Yu, H. Advance of Nano-Composite Electrospun Fibers in Periodontal Regeneration. Front. Chem. 2019, 7, 495. [Google Scholar] [CrossRef]
- Li, D.; Wang, Y.; Xia, Y. Electrospinning of Polymeric and Ceramic Nanofibers as Uniaxially Aligned Arrays. Nano Lett. 2003, 3, 1167–1171. [Google Scholar] [CrossRef]
- Zhang, E.; Zhu, C.; Yang, J.; Sun, H.; Zhang, X.; Li, S.; Wang, Y.; Sun, L.; Yao, F. Electrospun PDLLA/PLGA composite membranes for potential application in guided tissue regeneration. Mater. Sci. Eng. C 2016, 58, 278–285. [Google Scholar] [CrossRef]
- Sunandhakumari, V.J.; Vidhyadharan, A.K.; Alim, A.; Kumar, D.; Ravindran, J.; Krishna, A.; Prasad, M. Fabrication and In Vitro Characterization of Bioactive Glass/Nano Hydroxyapatite Reinforced Electrospun Poly(ε-Caprolactone) Composite Membranes for Guided Tissue Regeneration. Bioengineering 2018, 5, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdelaziz, D.; Hefnawy, A.; Al-Wakeel, E.; El-Fallal, A.; El-Sherbiny, I.M. New biodegradable nanoparticles-in-nanofibers based membranes for guided periodontal tissue and bone regeneration with enhanced antibacterial activity. J. Adv. Res. 2020, 28, 51–62. [Google Scholar] [CrossRef]
- Liu, X.; He, X.; Jin, D.; Wu, S.; Wang, H.; Yin, M.; Aldalbahi, A.; El-Newehy, M.; Mo, X.; Wu, J. A biodegradable multifunctional nanofibrous membrane for periodontal tissue regeneration. Acta Biomater. 2020, 108, 207–222. [Google Scholar] [CrossRef]
- Ou, Q.; Miao, Y.; Yang, F.; Lin, X.; Zhang, L.-M.; Wang, Y. Zein/gelatin/nanohydroxyapatite nanofibrous scaffolds are biocompatible and promote osteogenic differentiation of human periodontal ligament stem cells. Biomater. Sci. 2019, 7, 1973–1983. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.-F.; Lee, Y.-Y.; Chi, L.-Y.; Chen, Y.-T.; Hung, S.-L.; Ling, L.-J. Bacterial Penetration Through Antibiotic-Loaded Guided Tissue Regeneration Membranes. J. Periodontol. 2009, 80, 1471–1478. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.-F.; Wu, K.-M.; Chen, Y.-T.; Hung, S.-L. Bacterial adhesion to antibiotic-loaded guided tissue regeneration membranes–A scanning electron microscopy study. J. Formos. Med. Assoc. 2015, 114, 35–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, H.; Wang, Q.; Li, G.; Qiu, Y.; Wei, Q. Electrospun water-stable zein/ethyl cellulose composite nanofiber and its drug release properties. Mater. Sci. Eng. C 2017, 74, 86–93. [Google Scholar] [CrossRef]
- Jia, L.-N.; Zhang, X.; Xu, H.-Y.; Hua, F.; Hu, X.-G.; Xie, Q.; Wang, W.; Jia, J. Development of a Doxycycline Hydrochloride-Loaded Electrospun Nanofibrous Membrane for GTR/GBR Applications. J. Nanomater. 2016, 2016, 6507459. [Google Scholar] [CrossRef]
- Ho, M.; Claudia, J.C.; Tai, W.; Huang, K.; Lai, C.; Chang, C.; Chang, Y.; Wu, Y.; Kuo, M.Y.; Chang, P. The treatment response of barrier membrane with amoxicillin-loaded nanofibers in experimental periodontitis. J. Periodontol. 2021, 92, 886–895. [Google Scholar] [CrossRef]
- Shah, A.T.; Zahid, S.; Ikram, F.; Maqbool, M.; Chaudhry, A.A.; Rahim, M.I.; Schmidt, F.; Goerke, O.; Khan, A.S.; Rehman, I.U. Tri-layered functionally graded membrane for potential application in periodontal regeneration. Mater. Sci. Eng. C 2019, 103, 109812. [Google Scholar] [CrossRef]
- Zhou, T.; Chen, S.; Ding, X.; Hu, Z.; Cen, L.; Zhang, X. Fabrication and Characterization of Collagen/PVA Dual-Layer Membranes for Periodontal Bone Regeneration. Front. Bioeng. Biotechnol. 2021, 9, 437. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Dong, Y.; Zhang, N.; Shi, J.; Zhang, X.; Qi, C.; Midgley, A.C.; Wang, S. Potentials of sandwich-like chitosan/polycaprolactone/gelatin scaffolds for guided tissue regeneration membrane. Mater. Sci. Eng. C-Mater. Biol. Appl. 2020, 109, 110618. [Google Scholar] [CrossRef] [PubMed]
- Sowmya, S.; Mony, U.; Jayachandran, P.; Reshma, S.; Kumar, R.A.; Arzate, H.; Nair, S.V.; Jayakumar, R. Tri-Layered Nanocomposite Hydrogel Scaffold for the Concurrent Regeneration of Cementum, Periodontal Ligament, and Alveolar Bone. Adv. Healthc. Mater. 2017, 6, 1601251. [Google Scholar] [CrossRef]
- Wu, M.; Wang, J.; Zhang, Y.; Liu, H.; Dong, F. Mineralization Induction of Gingival Fibroblasts and Construction of a Sandwich Tissue-Engineered Complex for Repairing Periodontal Defects. Med. Sci. Monit. 2018, 24, 1112–1123. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Hajibandeh, J.; Suzuki, T.; Fan, A.; Shang, P.; Mao, J.J. Three-Dimensional Printed Multiphase Scaffolds for Regeneration of Periodontium Complex. Tissue Eng. Part A 2014, 20, 1342–1351. [Google Scholar] [CrossRef] [PubMed]
- Duruel, T.; Çakmak, A.S.; Akman, A.; Nohutcu, R.M.; Gümüşderelioğlu, M. Sequential IGF-1 and BMP-6 releasing chitosan/alginate/PLGA hybrid scaffolds for periodontal regeneration. Int. J. Biol. Macromol. 2017, 104, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Jing, Y.; Sun, H.; Liu, X. Hierarchical Nanofibrous Microspheres with Controlled Growth Factor Delivery for Bone Regeneration. Adv. Healthc. Mater. 2015, 4, 2699–2708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Z.; Ma, C.; Rong, X.; Zou, S.; Liu, X. Immunomodulatory ECM-like Microspheres for Accelerated Bone Regeneration in Diabetes Mellitus. ACS Appl. Mater. Interfaces 2018, 10, 2377–2390. [Google Scholar] [CrossRef]
- Liu, X.; Zhao, K.; Gong, T.; Song, J.; Bao, C.; Luo, E.; Weng, J.; Zhou, S. Delivery of Growth Factors Using a Smart Porous Nanocomposite Scaffold to Repair a Mandibular Bone Defect. Biomacromolecules 2014, 15, 1019–1030. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Biomaterial | Model Used | Observation Period | Outcomes |
|---|---|---|---|---|
| Ozawa et al. (2018) [62] | Collagen sponge (ACS) hydroxyapatite/collagen composite (HAP/Col) | Rats (male) | 12 weeks | Results suggested that application of HAP/Col increased outgrowth of new bone much more prominently than collagen group |
| Leventis et al. (2018) [63] | β-TCP + poly(lactic-co-glycolic) acid (PGLA) + Biolinker® (N-methyl-2-pyrrolidone solution) | Landrace (female) pigs | 12 weeks | Experimental sites showed less mean horizontal dimensional reduction of alveolar bridge but not statistically significant, with more new bone in experimental group |
| Kizildağ et al. (2018) [64] | Leukocyte-platelet-rich fibrin (L-PRF) + (OFD)/OFD alone | 16 humans with 32 sites | baseline and 6 months | (L-PRF) + (OFD) group showed significant PD reduction and CAL gain than OFD alone group |
| Okada et al. (2019) [65] | Group 1: β-TCP Group 2: β-TCP + PGLA | Beagle (male) dogs | 12 weeks | β-TCP + PGLA seems to be more effective than conventional β-TCP for ridge preservation |
| Sapata et al. (2019) [66] | Deproteinized bovine bone mineral (DBBM) DBBM with 10% collagen–collagen matrix (CM) | 65 patients | 4 months | DBBM demonstrated a noninferiority status compared to DBBM-CM group |
| Bodhare et al. (2019) [67] | Control: OFD + BioGide Test: OFD + BioGide + PRF | 40 human sites | 6 months | BioGide when used in combination with PRF is found to be more effective in gain in CAL, reduction in PD and achieving greater bone fill as compared to treatment with BG alone |
| Atchuta A et al. (2020) [68] | Group I: open-flap debridement; Group II: DFDBA alone; Group III: DFDBA + PRF | 39 human sites | Baseline, 3 months and 6 months | DFDBA + PRF group yielded better reduction of PPD and Relative attachment level (RAL) at 6 months interval |
| Kai-Ning Liu et al. (2020) [69] | Control group, GTR and Bio-Oss® Test group, GTR, Bio-Oss® and PRF | 14 patients | 6, 12 and 24 months | GTR and Bio-Oss® with PRF is more effective in treatment of periodontal intrabony defects than GTR and Bio-Oss® without PRF (CAL, PD) at all time intervals |
| Thakkar B et al. (2020) [70] | Group I: PRF and GTR Group II: PRF + bovine bone graft + GTR | 32 human sites | Baseline, 3 months and 6 months | Group II showed statistically significant changes in reduction in pocket depth and defect depth resolution |
| Bahammam MA et al. (2020) [71] | Group I: PRF + OFD Group II: nano-HA bone graft + OFD. Group III: OFD + PRF + nano-HA bone graft. Group IV: OFD alone | 60 human patients | Baseline and 6 months | Most significant increase in bone density and fill was observed for IBD depth in group III |
| Apine AA et al. (2020) [72] | Group I: NovaBone® putty. Group II: autologous platelet-rich fibrin | 30 intrabony defects were treated in 11 patients | Baseline, 3, 6 and 9 months | Improvement of clinical and radiographic parameters at sites treated with NovaBone® putty was better compared to that of sites treated with PRF, but differences were statistically not significant |
| Paolantonio M et al. (2020) [73] | Test group: L-PRF associated with autogenous bone graft (ABG) Control group: EMD + ABG | 44 patients | Baseline and 12 months | L-PRF + ABG produces noninferior results for CAL gain, PPD reduction, GR increase and DBL gain in comparison with EMD + ABG when treating noncontained IBDs. |
| Jae-Hong Lee et al. (2021) [74] | Test group: demineralized porcine bone matrix (DPBM) with EMD Control group: DPBM alone | 34 patients | Baseline, 2 years and 4 years | clinical, radiographic and patient-reported outcomes were significantly improved when DPBM no additional clinical and radiographic benefits were observed with adjunctive use of EMD |
| Bhatnagar S et al. (2021) [75] | Control sites: OFD alone Test sites: Calcium Phosphate ceramic GUIDOR® easy-graft Crystal, Sunstar Group, Etoy, Switzerland) and OFD. | 15 patients; 30 intrabony periodontal defects | Baseline, 3 and 6 months | Significant increase in Defect Fill and Percentage of Defect fill in both groups with better bone fill in test sites |
| Pavani MP et al. (2021) [76] | Group A: open-flap debridement (OFD) Group B: OFD with β TCP with PRF Group C: β TCP | 30 human sites | 6 months | Bone fill achieved in β TCP with PRF was more compared to β TCP alone and OFD at 6 months follow-up |
| Razi MA et al. (2021) [77] | Group I: PRF with demineralized bone matrix Group II: PRF alone Group III: open-flap debridement (OFD) | 30 patients | 9 months | PRF group had significant reduction in PD, RAL and Gingival recession (GR) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varghese, J.; Rajagopal, A.; Shanmugasundaram, S. Role of Biomaterials Used for Periodontal Tissue Regeneration—A Concise Evidence-Based Review. Polymers 2022, 14, 3038. https://doi.org/10.3390/polym14153038
Varghese J, Rajagopal A, Shanmugasundaram S. Role of Biomaterials Used for Periodontal Tissue Regeneration—A Concise Evidence-Based Review. Polymers. 2022; 14(15):3038. https://doi.org/10.3390/polym14153038
Chicago/Turabian StyleVarghese, Jothi, Anjale Rajagopal, and Shashikiran Shanmugasundaram. 2022. "Role of Biomaterials Used for Periodontal Tissue Regeneration—A Concise Evidence-Based Review" Polymers 14, no. 15: 3038. https://doi.org/10.3390/polym14153038