
Applications of Electrospun Drug-Eluting Nanofibers in Wound Healing: Current and Future Perspectives



Abstract
:1. Introduction
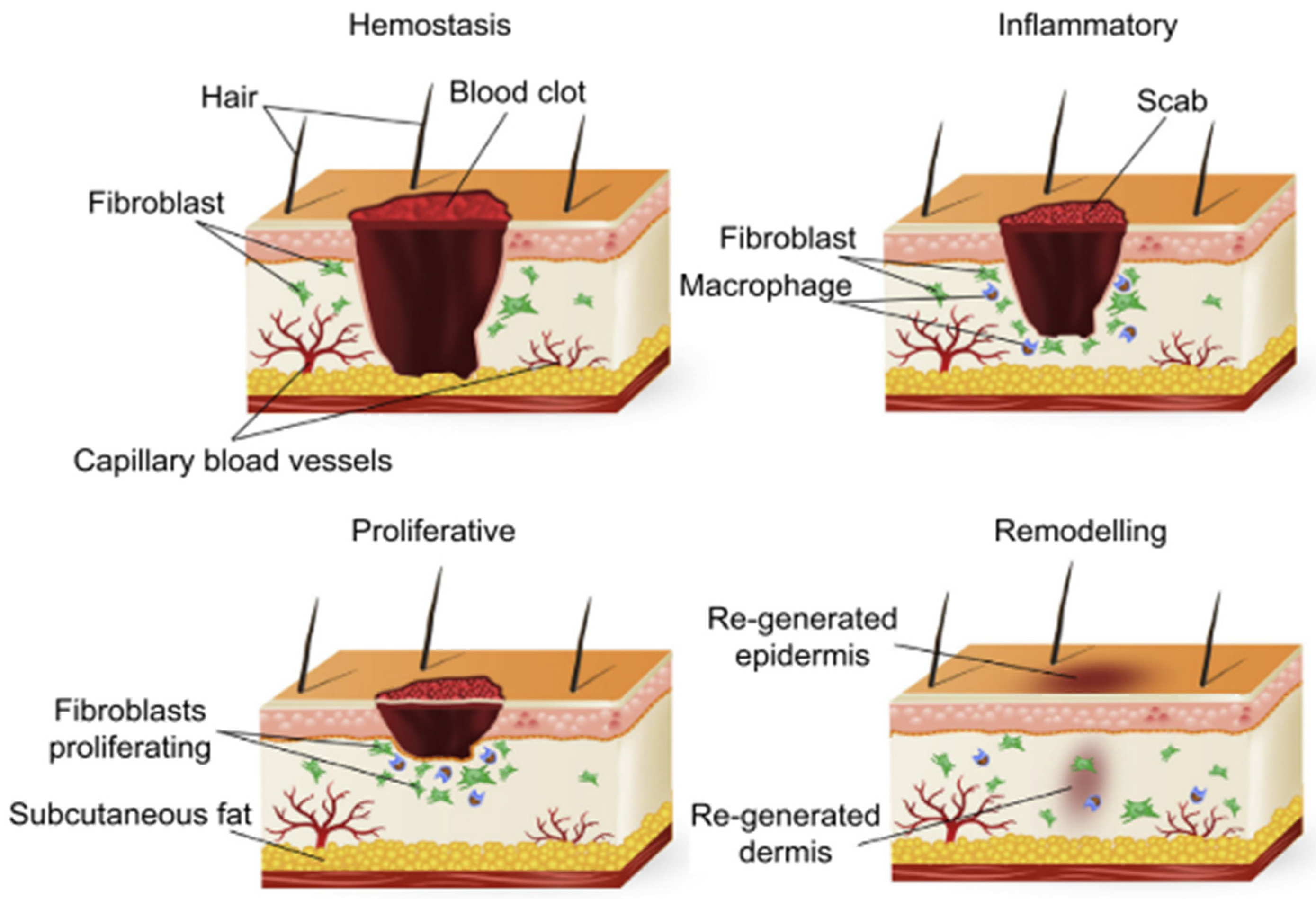
2. Process of Wound Healing
2.1. Hemostasis
2.2. Inflammation
2.3. Proliferation
2.4. Remodeling
3. Complications of Wound Healing
3.1. Factors Affecting Wound Healing
- Infection—Microbial colonization of the wound site is the most common barrier to wound healing. It is universally accepted that all wounds have some bacteria present on their surface; however, detrimental colonization of a host organism by foreign species defines wound infection [36]. Signs of wound infection generally present as a lack of friable granulation tissue, excessive exudate, and degraded wound beds, which are more or less a consequence of stimulation of inflammatory cells by invading bacteria [15].
- Necrosis—Necrosis is categorized by the presence of dead skin and foreign material at the wound site [15]. Necrotic cells are mortally harmed cells whose loss of function and cellular integrity could potentially evoke irritation in surrounding tissue, ultimately leading to a persistent inflammatory state and stalled wound healing [45].
- Nutrition—Wound healing involves several biological and molecular events that can be impaired by poor diet. Macronutrients like proteins, carbohydrates, and fats are necessary for the repair of lost tissue [46]. Inadequate dietary protein results in decreased wound tensile strength and a diminished ability of the body to defend the wound against infection. Furthermore, micronutrients such as vitamins and trace elements are essential components of cellular function and deficiencies in these molecules can impair the modulation of the healing phases [47].
- Moisture—Lack of moisture reduces tissue perfusion and slows down healing [15]. A moist environment is essential for the function of cells. Growth factors and other signalling molecules secreted following injury require a liquid medium for efficient intercellular communication. Epithelial cells also migrate and re-epithelialize more efficiently in a moist environment than in a dry one, saving tissue, time, and energy and reducing eschar formation [48].
- Individual physiologic variation–Patient conditions such as age and co-morbidities that restrict blood flow and hinder the activity of the immune system can cause non-healing of wounds [15]. Diabetes, obesity, hypothyroidism, and stress are associated with the development of chronic wounds. Conditions that present with impaired renal, hepatic, or respiratory function also hinder the wound healing process [33].
3.2. Wound and Scar Formation
4. Accelerating Healing of Surgical Wounds
“Class I/Clean: An uninfected operative wound in which no inflammation is encountered and the respiratory, alimentary, genital, or uninfected urinary tract is not entered. In addition, clean wounds are primarily closed and, if necessary, drained with closed drainage. Operative incisional wounds that follow nonpenetrating (blunt) trauma should be included in this category if they meet the criteria.
Class Il/Clean-Contaminated: An operative wound in which the respiratory, alimentary, genital, or urinary tracts are entered under controlled conditions and without unusual contamination. Specifically, operations involving the biliary tract, appendix, vagina, and oropharynx are included in this category, provided no evidence of infection or major break in technique is encountered.
Class Ill/Contaminated: Open, fresh, accidental wounds. In addition, operations with major breaks in sterile technique (e.g., open cardiac massage) or gross spillage from the gastrointestinal tract and incisions in which acute, nonpurulent inflammation is encountered are included in this category.
Class IV/Dirty-Infected: Old traumatic wounds with retained devitalized tissue and those that involve existing clinical infection or perforated viscera. This definition suggests that the organisms causing postoperative infection were present in the operative field before the operation.” [56].
4.1. Cell Therapy
4.2. Bioactive Therapeutic Delivery
4.3. Scaffolds/Biomaterials
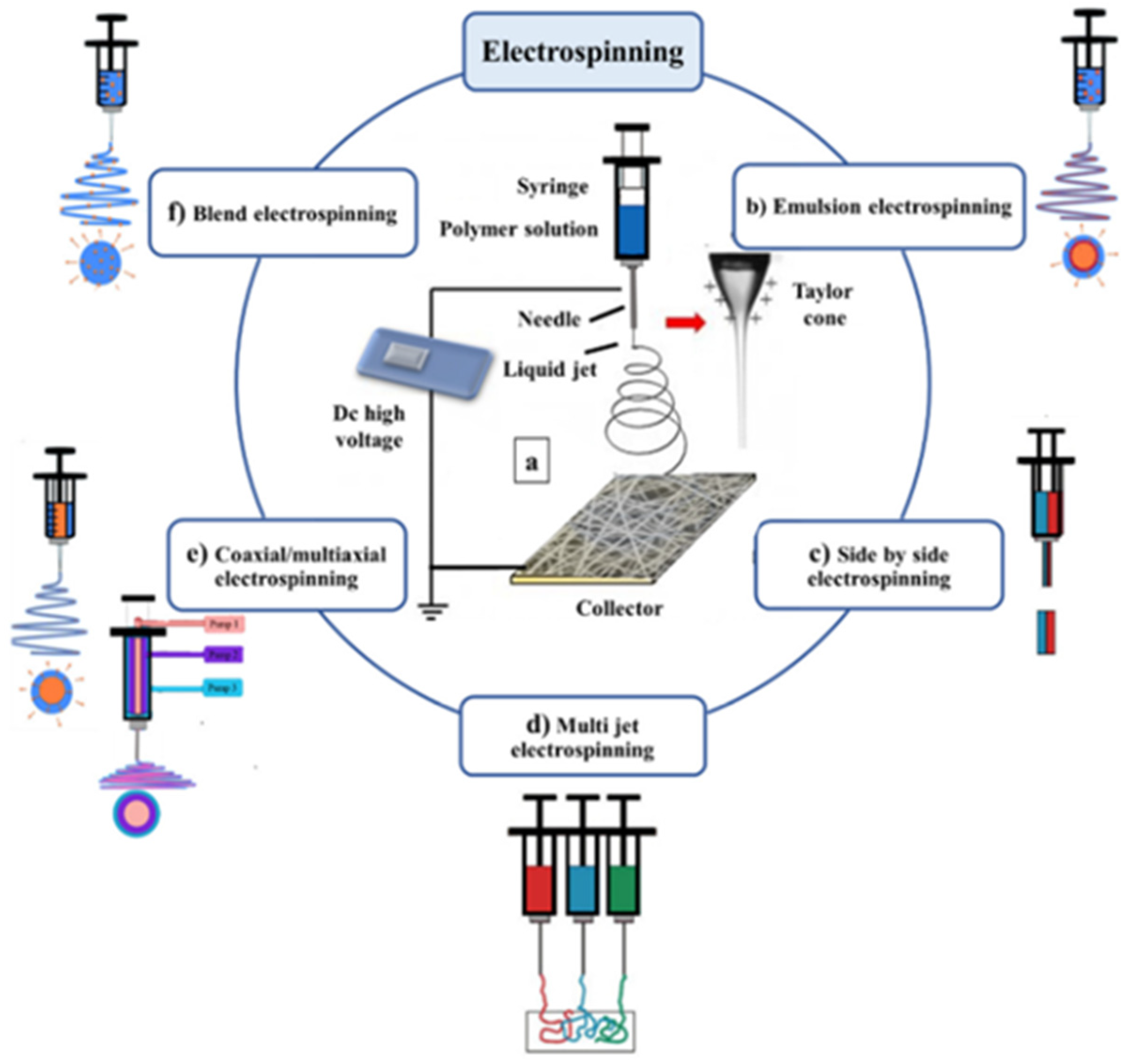
Nanofibers
5. Drug-Eluting Fibers
5.1. Antibacterial Agents
5.2. Anti-Inflammatory Agents
5.3. Proliferation Enhancers
5.4. Factors Impeding Industrialization of Drug-Eluting Fibers
6. Economic Considerations
7. Future Perspectives and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, X.; Xu, H.; Zhang, M.; Yu, D.G. Electrospun medicated nanofibers for wound healing: Review. Membranes 2021, 11, 770. [Google Scholar] [CrossRef] [PubMed]
- Gilaberte, Y.; Prieto-Torres, L.; Pastushenko, I.; Juarranz, Á. Anatomy and Function of the Skin; Elsevier Inc.: Amsterdam, The Netherlands, 2016; ISBN 9780128029459. [Google Scholar]
- Monteiro-Riviere, N.A. Structure and function of skin. In Toxicology of the Skin; CRC Press: Boca Raton, FL, USA, 2010; pp. 1–18. [Google Scholar] [CrossRef]
- Yang, J.; Wang, K.; Yu, D.G.; Yang, Y.; Bligh, S.W.A.; Williams, G.R. Electrospun Janus nanofibers loaded with a drug and inorganic nanoparticles as an effective antibacterial wound dressing. Mater. Sci. Eng. C 2020, 111, 110805. [Google Scholar] [CrossRef] [PubMed]
- Najafi, S.; Gholipour-Kanani, A.; Eslahi, N.; Bahrami, S.H. Study on release of cardamom extract as an antibacterial agent from electrospun scaffold based on sodium alginate. J. Text. Inst. 2021, 112, 1482–1490. [Google Scholar] [CrossRef]
- Schiff, B.A. Wound Healing. In Complications in Head and Neck Surgery, 2nd ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2009; pp. 39–45. ISBN 978-1-4160-4220-4. [Google Scholar]
- Peng, Y.; Ma, Y.; Bao, Y.; Liu, Z.; Chen, L.; Dai, F.; Li, Z. Electrospun PLGA/SF/artemisinin composite nanofibrous membranes for wound dressing. Int. J. Biol. Macromol. 2021, 183, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, H.P.; Longaker, M.T. Wounds: Biology, Pathology, and Management. In Essential Practice of Surgery; Springer: Berlin/Heidelberg, Germany, 2003. [Google Scholar] [CrossRef]
- Nussbaum, S.R.; Carter, M.J.; Fife, C.E.; DaVanzo, J.; Haught, R.; Nusgart, M.; Cartwright, D. An Economic Evaluation of the Impact, Cost, and Medicare Policy Implications of Chronic Nonhealing Wounds. Value Health 2018, 21, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Debas, H.T.; Gosselin, R.; Mccord, C. Surgery. In Disease Control Priorities in Developing Countries; Oxford University: New York, NY, USA, 2004; pp. 1245–1259. [Google Scholar]
- Yao, K.; Bae, L.; Yew, W.P. Post-operative wound management. Aust. Fam. Physician 2013, 42, 867–870. [Google Scholar]
- Singhal, H.; Kaur, K. Wound Infection. Medscape: General Surgery. Medscape, Manhattan, 2021. Available online: https://emedicine.medscape.com/article/188988-overview#a4 (accessed on 24 January 2022).
- Velnar, T.; Bailey, T.; Smrkolj, V. The wound healing process: An overview of the cellular and molecular mechanisms. J. Int. Med. Res. 2009, 37, 1528–1542. [Google Scholar] [CrossRef]
- Dhivya, S.; Padma, V.V.; Santhini, E. Wound dressings—A review. BioMedicine 2015, 5, 24–28. [Google Scholar] [CrossRef]
- Chaudhary, C.; Garg, T. Scaffolds: A novel carrier and potential wound healer. Crit. Rev. Ther. Drug Carr. Syst. 2015, 32, 277–321. [Google Scholar] [CrossRef]
- Wei, Z.; Wang, L.; Zhang, S.; Chen, T.; Yang, J.; Long, S.; Wang, X. Electrospun antibacterial nanofibers for wound dressings and tissue medicinal fields: A Review. J. Innov. Opt. Health Sci. 2020, 13, 2030012. [Google Scholar] [CrossRef]
- El Fawal, G.; Hong, H.; Mo, X.; Wang, H. Fabrication of scaffold based on gelatin and polycaprolactone (PCL) for wound dressing application. J. Drug Deliv. Sci. Technol. 2021, 63, 102501. [Google Scholar] [CrossRef]
- Ramazan, E. Advances in Fabric Structures for Wound Care, 2nd ed.; Elsevier Ltd.: Amsterdam, The Netherlands, 2019; ISBN 9780081021927. [Google Scholar]
- Senthamizhan, A.; Balusamy, B.; Uyar, T. Electrospinning: A Versatile Processing Technology for Producing Nanofibrous Materials for Biomedical and Tissue-Engineering Applications; Elsevier Ltd.: Amsterdam, The Netherlands, 2017; ISBN 9780081022221. [Google Scholar]
- Arora, A.; Aggarwal, G.; Chander, J.; Maman, P.; Nagpal, M. Drug eluting sutures: A recent update. J. Appl. Pharm. Sci. 2019, 9, 111–123. [Google Scholar] [CrossRef] [Green Version]
- Luk, A. Critical challenges to the design of drug-eluting medical devices. Ther. Deliv. 2013, 4, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, M.E.; Montoto, S.S. Routes of Drug Administration. In ADME Processes in Pharmaceutical Sciences; Talevi, A., Quiroga, P.A.M., Eds.; Springer: Cham, Germany, 2018; pp. 97–133. ISBN 9783319995939. [Google Scholar]
- Parikh, K.S. Nano-Structured, Drug Eluting Medical Devices For Improved Clinical Outcomes. Ph.D. Thesis, Johns Hopkins University, Baltimore, MD, USA, 2017; pp. 1–4. [Google Scholar]
- Anselmo, A.C.; Mitragotri, S. An overview of clinical and commercial impact of drug delivery systems. J. Control. Release 2014, 190, 15–28. [Google Scholar] [CrossRef] [Green Version]
- Guo, S.; DiPietro, L.A. Critical review in oral biology & medicine: Factors affecting wound healing. J. Dent. Res. 2010, 89, 219–229. [Google Scholar] [CrossRef]
- Schultz, G.S.; Chin, G.A.; Moldawer, L.; Diegelmann, R.F. Principles of wound healing. In Mechanisms of Vascular Disease: A Reference Book for Vascular Specialists; The University of Adelaide Press: Adelaide, Australia, 2011; pp. 423–450. [Google Scholar] [CrossRef]
- Rang, H.P.; Dale, M.M.; Ritter, J.M.; Flower, R.J.; Henderson, G. Rang and Dale’s Pharmacology, 7th ed.; Elsevier: Edinburgh, UK, 2012; pp. 294–307. ISBN 9780702034718. [Google Scholar]
- Maureane Hoffman Remodeling the Blood Coagulation Cascade. J. Thromb. Thrombolysis 2003, 16, 17–20. [CrossRef]
- Higgins, R.A. Coagulation Pathway and Physiology. In Hemostasis Physiology; Schematic Scholar: Washington, DC, USA, 2016; pp. 3–15. Available online: https://webapps.cap.org/apps/docs/store/algorithmic-approach-to-hemostasis-testing-sample-pages.pdf (accessed on 24 January 2022).
- Chaudhry, R.; Usama, S.M.; Babiker, H.M. Physiology, Coagulation Pathways; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK482253/ (accessed on 24 January 2022).
- Perez-Pujol, S.; Aras, O.; Escolar, G. Factor V Leiden and Inflammation. Thrombosis 2012, 2012, 594986. [Google Scholar] [CrossRef] [Green Version]
- Marshall, C.D.; Hu, M.S.; Leavitt, T.; Barnes, L.A.; Lorenz, H.P.; Longaker, M.T. Cutaneous Scarring: Basic Science, Current Treatments, and Future Directions. Adv. Wound Care 2018, 7, 29–45. [Google Scholar] [CrossRef] [Green Version]
- Broughton, G.; Janis, J.E.; Attinger, C.E. Wound healing: An overview. Plast. Reconstr. Surg. 2006, 117, 1–32. [Google Scholar] [CrossRef]
- ben Amar, M.; Wu, M. Re-epithelialization: Advancing epithelium frontier during wound healing. J. R. Soc. Interface 2014, 11, 20131038. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, A.C.D.O.; Andrade, Z.D.A.; Costa, T.F.; Medrado, A.R.A.P. Wound healing—A literature review. An. Bras. Dermatol. 2016, 91, 614–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolcott, R.; Cutting, K.; Dowd, S.; Percival, S. Types of Wounds and Infections. In Microbiology Wounds; CRC Press: Boca Raton, FL, USA, 2010; pp. 219–232. [Google Scholar] [CrossRef]
- Emanuele, A.S.; Giada, M.; Alessio, F.; Ciprandi, G. From Tissue Repair To Tisse Regenetaion. In Wound Healing; IntechOpen: London UK, 2019; pp. 1–37. [Google Scholar] [CrossRef] [Green Version]
- Lipsky, B.A.; Hoey, C. Topical antimicrobial therapy for treating chronic wounds. Clin. Infect. Dis. 2009, 49, 1541–1549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathur, H.M.; Boulton, A.J.M. Recent advances in the diagnosis and management of diabetic neuropathy. J. Bone Jt. Sur. Ser. B 2005, 87, 1605–1610. [Google Scholar] [CrossRef] [PubMed]
- Webb, R. Pressure ulcer over pressure injury. Br. J. Nurs. 2017, 26, S4. [Google Scholar] [CrossRef]
- Stavrou, D.; Weissman, O.; Tessone, A.; Zilinsky, I.; Holloway, S.; Boyd, J.; Haik, J. Health Related Quality of Life in burn patients—A review of the literature. Burns 2014, 40, 788–796. [Google Scholar] [CrossRef]
- Gianfaldoni, S.; Wollina, U.; Lotti, J.; Gianfaldoni, R.; Lotti, T.; Fioranelli, M.; Roccia, M.G. History of venous leg ulcers. J. Biol. Regul. Homeost. Agents 2017, 31, 107–120. [Google Scholar]
- Kirkwood, M.L.; Arbique, G.M.; Guild, J.B.; Timaran, C.; Chung, J.; Modrall, G.; Anderson, J.A.; Valentine, R.J. Radiation Skin Injury: More Frequent After Complex Endovascular Procedures? J. Vasc. Surg. 2013, 58, 1725. [Google Scholar] [CrossRef] [Green Version]
- Coruh, A.; Yontar, Y. Application of split-thickness dermal grafts in deep partial- and full-thickness burns: A new source of auto-skin grafting. J. Burn Care Res. 2012, 33, 95–101. [Google Scholar] [CrossRef]
- Amala, C. Necrosis and Types of Necrosis. Trans. Med. 2020, 10, 210. [Google Scholar] [CrossRef]
- Williams, J.Z.; Barbul, A. Nutrition and wound healing. Surg. Clin. N. Am. 2003, 83, 571–596. [Google Scholar] [CrossRef]
- Barchitta, M.; Maugeri, A.; Favara, G.; San Lio, R.M.; Evola, G.; Agodi, A.; Basile, G. Nutrition and wound healing: An overview focusing on the beneficial effects of curcumin. Int. J. Mol. Sci. 2019, 20, 1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuutila, K.; Eriksson, E. Moist Wound Healing with Commonly Available Dressings. Adv. Wound Care 2021, 10, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Théorêt, C.; Stashak, T. Wound dressing. In Clinical Veterinary Advisor; WB Saunders: Philadelphia, PA, USA, 2011; ISBN 9781416099796. [Google Scholar] [CrossRef]
- Bayat, A.; McGrouther, D.A.; Ferguson, M.W.J. Skin scarring. Br. Med. J. 2003, 326, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Larson, B.J.; Longaker, M.T.; Lorenz, P.H. Scarless Fetal Wound Healing: A Basic Science Review. Plast. Reconstr. Surg. 2010, 126, 1172–1180. [Google Scholar] [CrossRef] [Green Version]
- Colwell, A.S.; Longaker, M.T.; Lorenze, P.H. Fetal Wound Healing. Front. Biosci. 2003, 84, 1240–1248. [Google Scholar] [CrossRef]
- Stöppler, M.C. Medterms Medical Dictionary a-z list/ Surgery Definition. Available online: https://www.medicinenet.com/surgery/definition.htm (accessed on 24 January 2022).
- Bae, J.Y.; Groen, R.S.; Kushner, A.L. Surgery as a public health intervention: Common misconceptions versus the truth. Bull. World Health Organ. 2011, 89, 395. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Dumville, J.C.; Norman, G.; Westby, M.J.; Blazeby, J.; McFarlane, E.; Welton, N.J.; O’Connor, L.; Cawthorne, J.; George, R.P.; et al. Intraoperative interventions for preventing surgical site infection: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2018, 2018, CD012653. [Google Scholar] [CrossRef] [Green Version]
- Mangram, A.J.; Horan, T.C.; Pearson, M.L.; Christine Silver, L.; Jarvis, W.R.; The Hospital Infection Control Practices Advisory Committee. Guideline for Prevention of Surgical Site Infection, 1999. Infect. Control Hosp. Epidemiol. 1999, 20, 247–280. [Google Scholar] [CrossRef]
- Onyekwelu, I.; Yakkanti, R.; Protzer, L.; Pinkston, C.M.; Tucker, C.; Seligson, D. Surgical Wound Classification and Surgical Site Infections in the Orthopaedic Patient. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2017, 1, e022. [Google Scholar] [CrossRef]
- Gaynes, R.P.; Culver, D.H.; Horan, T.C.; Edwards, J.R.; Richards, C.; Tolson, J.S. Surgical Site Infection (SSI) rates in the United States, 1992-1998: The National Nosocomial Infections Surveillance system basic SSI risk index. Clin. Infect. Dis. 2001, 33, 1992–1998. [Google Scholar] [CrossRef]
- Goyal, R.; Sandhu, H.P.S.; Kumar, A.; Kosey, S. Surgical Site Infection in General Surgery. Int. J. Sci. Res. Knowl. 2015, 3, 198–203. [Google Scholar] [CrossRef]
- Gulacsi, L.; Tatar Kiss, Z.; Goldmann, D.A.; Huskins, W.C. Risk-adjusted infection rates in surgery: A model for outcome measurement in hospitals developing new quality improvement programmes. J. Hosp. Infect. 2000, 44, 43–52. [Google Scholar] [CrossRef]
- Raka, L.; Krasniqi, A.; Hoxha, F.; Musa, R.; Mulliqi, G.; Krasniqi, S.; Kurti, A.; Dervishaj, A.; Nuhiu, B.; Kelmendi, B.; et al. Surgical site infections in an abdominal surgical ward at Kosovo Teaching Hospital. J. Infect. Dev. Ctries. 2007, 1, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Atif, M.L.; Azouaou, A.; Bouadda, N.; Bezzaoucha, A.; Si-Ahmed, M.; Bellouni, R. Incidence and predictors of surgical site infection in a general surgery department in Algeria. Rev. d’Epidemiol. Sante Publique 2015, 63, 275–279. [Google Scholar] [CrossRef] [PubMed]
- van Walraven, C.; Musselman, R. The Surgical Site Infection Risk Score (SSIRS): A Model to Predict the Risk of Surgical Site Infections. PLoS ONE 2013, 8, 30–33. [Google Scholar] [CrossRef] [PubMed]
- Woldemicael, A.Y.; Bradley, S.; Pardy, C.; Richards, J.; Trerotoli, P.; Giuliani, S. Surgical Site Infection in a Tertiary Neonatal Surgery Centre. Eur. J. Pediatric Surg. 2019, 29, 260–265. [Google Scholar] [CrossRef]
- Zejnullahu, V.A.; Zejnullahu, V.A.; Isjanovska, R.; Sejfija, Z. Surgical site infections after cesarean sections at the University Clinical Center of Kosovo: Rates, microbiological profile and risk factors. BMC Infect. Dis. 2019, 19, 752. [Google Scholar] [CrossRef]
- Alkaaki, A.; Al-Radi, O.O.; Khoja, A.; Alnawawi, A.; Alnawawi, A.; Maghrabi, A.; Altaf, A.; Aljiffry, M. Surgical site infection following abdominal surgery: A prospective cohort study. Can. J. Surg. 2019, 62, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Shi, C.; Wang, C.; Liu, H.; Li, Q.; Li, R.; Zhang, Y.; Liu, Y.; Shao, Y.; Wang, J. Selection of Appropriate Wound Dressing for Various Wounds. Front. Bioeng. Biotechnol. 2020, 8, 182. [Google Scholar] [CrossRef] [Green Version]
- Nour, S.; Baheiraei, N.; Imani, R.; Khodaei, M.; Alizadeh, A.; Rabiee, N.; Moazzeni, S.M. A review of accelerated wound healing approaches: Biomaterial- assisted tissue remodeling. J. Mater. Sci. Mater Med. 2019, 30, 120. [Google Scholar] [CrossRef]
- Aronson, A.; Laageide, L.; Powers, J. Use of Stem Cells in Wound Healing. Curr. Dermatol. Rep. 2018, 7, 278–286. [Google Scholar] [CrossRef]
- Lee, D.E.; Ayoub, N.; Agrawal, D.K. Mesenchymal stem cells and cutaneous wound healing: Novel methods to increase cell delivery and therapeutic efficacy. Stem Cell Res. Ther. 2016, 7, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nourian Dehkordi, A.; Mirahmadi Babaheydari, F.; Chehelgerdi, M.; Raeisi Dehkordi, S. Skin tissue engineering: Wound healing based on stem-cell-based therapeutic strategies. Stem Cell Res. Ther. 2019, 10, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, S.; Baker, A.B. Biomaterials and nanotherapeutics for enhancing skin wound healing. Front. Bioeng. Biotechnol. 2016, 4, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grazul-Bilska, A.T.; Johnson, M.L.; Bilski, J.J.; Redmer, D.A.; Reynolds, L.P.; Abdullah, A.; Abdullah, K.M. Wound healing: The role of growth factors. Drugs Today 2003, 39, 787–800. [Google Scholar] [CrossRef]
- Eming, S.A.; Krieg, T.; Davidson, J.M. Gene Therapy and Wound Healing. Clin. Dermatol. 2007, 25, 79–92. [Google Scholar] [CrossRef] [Green Version]
- Punjataewakupt, A.; Napavichayanun, S.; Aramwit, P. The downside of antimicrobial agents for wound healing. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 39–54. [Google Scholar] [CrossRef]
- Krischak, G.D.; Augat, P.; Claes, L.; Kinzl, L.; Beck, A. The effects of non-steroidal anti-infl ammatory drug application on incisional wound healing in rats. J. Wound Care 2007, 16, 76–78. [Google Scholar] [CrossRef]
- Su, W.H.; Cheng, M.H.; Lee, W.L.; Tsou, T.S.; Chang, W.H.; Chen, C.-S.; Wang, P.H. Nonsteroidal anti-inflammatory drugs for wounds: Pain relief or excessive scar formation? Mediat. Inflamm. 2010, 2010, 413238. [Google Scholar] [CrossRef]
- Tarafder, S.; Park, G.Y.; Felix, J.; Lee, C.H. Bioadhesives for musculoskeletal tissue regeneration. Acta Biomater. 2020, 117, 77–92. [Google Scholar] [CrossRef]
- Duan, W.; Bian, X.; Bu, Y. Applications of Bioadhesives: A Mini Review. Front. Bioeng. Biotechnol. 2021, 9, 716035. [Google Scholar] [CrossRef] [PubMed]
- Ge, L.; Chen, S. Recent advances in tissue adhesives for clinical medicine. Polymers 2020, 12, 939. [Google Scholar] [CrossRef] [PubMed]
- Duarte, A.P.; Coelho, J.F.; Bordado, J.C.; Cidade, M.T.; Gil, M.H. Surgical adhesives: Systematic review of the main types and development forecast. Prog. Polym. Sci. 2012, 37, 1031–1050. [Google Scholar] [CrossRef]
- Boateng, J.S.; Matthews, K.H.; Stevens, H.N.E.; Eccleston, G.M. Wound healing dressings and drug delivery systems: A review. J. Pharm. Sci. 2008, 97, 2892–2923. [Google Scholar] [CrossRef]
- Agarwal, Y.; Rajinikanth, P.S.; Ranjan, S.; Tiwari, U.; Balasubramnaiam, J.; Pandey, P.; Arya, D.K.; Anand, S.; Deepak, P. Curcumin loaded polycaprolactone-/polyvinyl alcohol-silk fibroin based electrospun nanofibrous mat for rapid healing of diabetic wound: An in-vitro and in-vivo studies. Int. J. Biol. Macromol. 2021, 176, 376–386. [Google Scholar] [CrossRef]
- Nagar, H.K.; Srivastava, A.K.; Srivastava, R.; Kurmi, M.L.; Chandel, H.S.; Ranawat, M.S. Pharmacological Investigation of the Wound Healing Activity of Cestrum nocturnum (L.) Ointment in Wistar Albino Rats. J. Pharm. 2016, 2016, 9249040. [Google Scholar] [CrossRef] [Green Version]
- Su, C.; Menon, N.V.; Xu, X.; Teo, Y.R.; Cao, H.; Dalan, R.; Tay, C.Y.; Hou, H.W. A novel human arterial wall-on-a-chip to study endothelial inflammation and vascular smooth muscle cell migration in early atherosclerosis. Lab Chip 2021, 21, 2359–2371. [Google Scholar] [CrossRef]
- Nugud, A.; Sandeep, D.; El-Serafi, A.T. Two faces of the coin: Minireview for dissecting the role of reactive oxygen species in stem cell potency and lineage commitment. J. Adv. Res. 2018, 14, 73–79. [Google Scholar] [CrossRef]
- Cao, H.; Yang, L.; Tian, R.; Wu, H.; Gu, Z.; Li, Y. Versatile polyphenolic platforms in regulating cell biology. Chem. Soc. Rev. 2022, 51, 4175–4198. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Z.; Yang, P.; Duan, G.; Liu, X.; Gu, Z.; Li, Y. Polyphenol scaffolds in tissue engineering. Mater. Horiz. 2021, 8, 145–167. [Google Scholar] [CrossRef]
- Hu, J.; Yang, L.; Yang, P.; Jiang, S.; Liu, X.; Li, Y. Polydopamine free radical scavengers. Biomater. Sci. 2020, 8, 4940–4950. [Google Scholar] [CrossRef]
- Ou, Q.; Zhang, S.; Fu, C.; Yu, L.; Xin, P.; Gu, Z.; Cao, Z.; Wu, J.; Wang, Y. More natural more better: Triple natural anti-oxidant puerarin/ferulic acid/polydopamine incorporated hydrogel for wound healing. J. Nanobiotechnol. 2021, 19, 237. [Google Scholar] [CrossRef] [PubMed]
- Gathani, K.M.; Raghavendra, S.S. Scaffolds in regenerative endodontics: A review. Dent. Res. J. 2016, 13, 379–386. [Google Scholar] [CrossRef]
- Samadian, H.; Zamiri, S.; Ehterami, A.; Farzamfar, S.; Vaez, A.; Khastar, H.; Alam, M.; Ai, A.; Derakhshankhah, H.; Allahyari, Z.; et al. Electrospun cellulose acetate/gelatin nanofibrous wound dressing containing berberine for diabetic foot ulcer healing: In vitro and in vivo studies. Sci. Rep. 2020, 10, 8312. [Google Scholar] [CrossRef] [PubMed]
- Sabbagh, F.; Kim, B.S. Recent advances in polymeric transdermal drug delivery systems. J. Control. Release 2022, 341, 132–146. [Google Scholar] [CrossRef]
- Vyas, S.; Zhang, X.; Goli, E.; Geubelle, P.H. Frontal vs. bulk polymerization of fiber-reinforced polymer-matrix composites. Compos. Sci. Technol. 2020, 198, 108303. [Google Scholar] [CrossRef]
- Ghaemi, N.; Safari, P. Nano-porous SAPO-34 enhanced thin-film nanocomposite polymeric membrane: Simultaneously high water permeation and complete removal of cationic/anionic dyes from water. J. Hazard. Mater. 2018, 358, 376–388. [Google Scholar] [CrossRef]
- Çaykara, T.; Akçakaya, İ. Synthesis and network structure of ionic poly(N,N-dimethylacrylamide-co-acrylamide) hydrogels: Comparison of swelling degree with theory. Eur. Polym. J. 2006, 42, 1437–1445. [Google Scholar] [CrossRef]
- Buyukgoz, G.G.; Castro, J.N.; Atalla, A.E.; Pentangelo, J.G.; Tripathi, S.; Davé, R.N. Impact of Mixing on Content Uniformity of Thin Polymer Films Containing Drug Micro-Doses. Pharmaceutics 2021, 13, 812. [Google Scholar] [CrossRef]
- Guillen, G.R.; Pan, Y.; Li, M.; Hoek, E.M. Preparation and Characterization of Membranes Formed by Nonsolvent Induced Phase Separation: A Review. Ind. Eng. Chem. Res. 2011, 50, 3798–3817. [Google Scholar] [CrossRef]
- Lee, W.R.; Im, C.; Park, H.-Y.; Seo, J.-M.; Kim, J.-M. Fabrication of Convex PDMS–Parylene Microstructures for Conformal Contact of Planar Micro-Electrode Array. Polymers 2019, 11, 1436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richard, A.S.; Verma, R.S. Bioactive nano yarns as surgical sutures for wound healing. Mater. Sci. Eng. C 2021, 128, 112334. [Google Scholar] [CrossRef] [PubMed]
- Boybeyi, Ö.; Kaçmaz, B.; Günal, Y.D.; Gül, S.; Yörübulut, S.; Aslan, M.K. Bacterial adhesion to braided surgical sutures: An in vitro study. Eur. J. Plast. Surg. 2016, 39, 1–6. [Google Scholar] [CrossRef]
- Keshvardoostchokami, M.; Majidi, S.S.; Huo, P.; Ramachandran, R.; Chen, M.; Liu, B. Electrospun nanofibers of natural and synthetic polymers as artificial extracellular matrix for tissue engineering. Nanomaterials 2021, 11, 21. [Google Scholar] [CrossRef]
- Alghoraibi, I.; Alomari, S. Different Methods for Nanofiber Design and Fabrication; Springer International Publishing: Damascus, Syria, 2020; ISBN 9783319427898. [Google Scholar]
- Hu, W.; Huang, Z.M.; Liu, X.Y. Development of braided drug-loaded nanofiber sutures. Nanotechnology 2010, 21, 315104. [Google Scholar] [CrossRef]
- Lee, J.E.; Park, S.; Park, M.; Kim, M.H.; Park, C.G.; Lee, S.H.; Choi, S.Y.; Kim, B.H.; Park, H.J.; Park, J.H.; et al. Surgical suture assembled with polymeric drug-delivery sheet for sustained, local pain relief. Acta Biomater. 2013, 9, 8318–8327. [Google Scholar] [CrossRef]
- Zare, M.; Dziemidowicz, K.; Williams, G.R.; Ramakrishna, S. Encapsulation of pharmaceutical and nutraceutical active ingredients using electrospinning processes. Nanomaterials 2021, 11, 1968. [Google Scholar] [CrossRef]
- Amarjargal, A.; Brunelli, M.; Fortunato, G.; Spano, F.; Kim, C.-S.; Rossi, R.M. On-demand drug release from tailored blended electrospun nanofibers. J. Drug Deliv. Sci. Technol. 2019, 52, 8–14. [Google Scholar] [CrossRef]
- Mousavi, S.M.; Nejad, Z.M.; Hashemi, S.A.; Salari, M.; Gholami, A.; Ramakrishna, S.; Chiang, W.H.; Lai, C.W. Bioactive agent-loaded electrospun nanofiber membranes for accelerating healing process: A review. Membranes 2021, 11, 702. [Google Scholar] [CrossRef]
- Boonkaew, B.; Kempf, M.; Kimble, R.; Supaphol, P.; Cuttle, L. Antimicrobial efficacy of a novel silver hydrogel dressing compared to two common silver burn wound dressings: ActicoatTM and PolyMem Silver®. Burns 2014, 40, 89–96. [Google Scholar] [CrossRef]
- Fahimirad, S.; Abtahi, H.; Satei, P.; Ghaznavi-Rad, E.; Moslehi, M.; Ganji, A. Wound healing performance of PCL/chitosan based electrospun nanofiber electrosprayed with curcumin loaded chitosan nanoparticles. Carbohydr. Polym. 2021, 259, 117640. [Google Scholar] [CrossRef] [PubMed]
- Alshomer, F.; Madhavan, A.; Pathan, O.; Song, W. Bioactive Sutures: A Review of Advances in Surgical Suture Functionalisation. Curr. Med. Chem. 2017, 24, 215–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, X.; Qasim, M.; Ali, A. Engineering and polymeric composition of drug-eluting suture: A review. J. Biomed. Mater. Res. Part A 2021, 109, 2065–2081. [Google Scholar] [CrossRef] [PubMed]
- Gallo, A.L.; Paladini, F.; Romano, A.; Verri, T.; Quattrini, A.; Sannino, A.; Pollini, M. Efficacy of silver coated surgical sutures on bacterial contamination, cellular response and wound healing. Mater. Sci. Eng. C 2016, 69, 884–893. [Google Scholar] [CrossRef] [PubMed]
- Deliaert, A.E.; van den Kerckhove, E.; Tuinder, S.; Fieuws, S.; Sawor, J.H.; Meesters-Caberg, M.A.; van der Hulst, R.R. The effect of triclosan-coated sutures in wound healing. A double blind randomised prospective pilot study. J. Plast. Reconstr. Aesthetic Surg. 2009, 62, 771–773. [Google Scholar] [CrossRef] [PubMed]
- Obermeier, A.; Schneider, J.; Föhr, P.; Wehner, S.; Kühn, K.D.; Stemberger, A.; Schieker, M.; Burgkart, R. In vitro evaluation of novel antimicrobial coatings for surgical sutures using octenidine. BMC Microbiol. 2015, 15, 168. [Google Scholar] [CrossRef] [Green Version]
- Viju, S.; Thilagavathi, G. Effect of chitosan coating on the characteristics of silk-braided sutures. J. Ind. Text. 2013, 42, 256–268. [Google Scholar] [CrossRef]
- Zurita, R.; Puiggalí, J.; Rodríguez-Galán, A. Loading and release of ibuprofen in multi- and monofilament surgical sutures. Macromol. Biosci. 2006, 6, 767–775. [Google Scholar] [CrossRef]
- Huh, B.K.; Kim, B.H.; Kim, S.N.; Park, C.G.; Lee, S.H.; Kim, K.R.; Heo, C.Y.; Choy, Y. bin Surgical suture braided with a diclofenac-loaded strand of poly(lactic-co-glycolic acid) for local, sustained pain mitigation. Mater. Sci. Eng. C 2017, 79, 209–215. [Google Scholar] [CrossRef]
- Kopf, S.; Birkenfeld, F.; Becker, R.; Petersen, W.; Stärke, C.; Wruck, C.J.; Tohidnezhad, M.; Varoga, D.; Pufe, T. Local treatment of meniscal lesions with vascular endothelial growth factor. J. Bone Jt. Surg. Ser. A 2010, 92, 2682–2691. [Google Scholar] [CrossRef]
- Bigalke, C.; Luderer, F.; Wulf, K.; Storm, T.; Lobler, M.; Arbeiter, D.; Rau, B.M.; Nizze, H.; Vollmar, B.; Schmitz, K.P.; et al. VEGF-releasing suture material for enhancement of vascularization: Development, in vitro and in vivo study. Acta Biomater. 2014, 10, 5081–5089. [Google Scholar] [CrossRef] [PubMed]
- Dhand, C.; Ong, S.T.; Dwivedi, N.; Diaz, S.M.; Venugopal, J.R.; Navaneethan, B.; Fazil, M.H.U.T.; Liu, S.; Seitz, V.; Wintermantel, E.; et al. Bio-inspired in situ crosslinking and mineralization of electrospun collagen scaffolds for bone tissue engineering. Biomaterials 2016, 104, 323–338. [Google Scholar] [CrossRef] [PubMed]
- Uttarwar, M.; Aswath, P. Fabrication of porous, drug-releasing, biodegradable, polymer scaffolds for sustained drug release. J. Biomed. Mater. Res. Part B Appl. Biomater. 2008, 87, 121–131. [Google Scholar] [CrossRef]
- He, C.L.; Huang, Z.M.; Han, X.J. Fabrication of drug-loaded electrospun aligned fibrous threads for suture applications. J. Biomed. Mater. Res. Part A 2009, 89, 80–95. [Google Scholar] [CrossRef] [PubMed]
- Fife, C.E.; Carter, M.J.; Walker, D.; Thomson, B. Wound Care Outcomes and Associated Cost Among Patients Treated in US Outpatient Centers: Data from the US Wound Registry. Wound Care Learn. Netw. 2012, 24, 10–17. [Google Scholar]
- Hurd, T.; Zuiliani, N.; Posnett, J. Evaluation of the impact of restructuring wound management practices in a community care provider in Niagara, Canada. Int. Wound J. 2008, 5, 296–304. [Google Scholar] [CrossRef]
- El-aassar, M.R.; Ibrahim, O.M.; Al-oanzi, Z.H. Biotechnological applications of polymeric nanofiber platforms loaded with diverse bioactive materials. Polymers 2021, 13, 3734. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Overall Infection Rate * | SSI Detection (%) | Ref | |||
|---|---|---|---|---|---|---|
| a | b | c | x | |||
| United States | 6.8 | 51.9 | 44.4 | 3.7 | [57] | |
| United States | 16 | 78 | 9 | 13 | [58] | |
| Hungary | 2.9 | 24 | 6 | 70 | [60] | |
| Kosovo | 12 | 40.7 | 3.7 | 55.6 | [61] | |
| Algeria | 5.4 | 62 | 38 | [62] | ||
| Canada | 3.9 | 15.8 | 29.2 | 57.5 | [63] | |
| United Kingdom | 15.6 | 14 | 86 | [64] | ||
| Kosovo | 9.8 | 6.3 | 93.7 | [65] | ||
| Saudi Arabia | 16.3 | 9 | 45 | 45 | [66] | |
| Therapeutic Agent/Class | Drug Carrier | Treatment Method | Therapeutic Activity Assessment Method | General Findings |
|---|---|---|---|---|
| Silver particles/antibacterial | Silver solution on 910 PGLA suture | Silver deposition technology | In vitro | Modified sutures demonstrated long-term antibacterial capability on Gram-positive and Gram-negative bacteria [113] |
| Triclosan/antibacterial | Vicryl Plus ® (Ethicon, Cincinnati, Ohio, USA) | Coating | Double-blind randomized prospective pilot study | Toxic byproducts of triclosan possibly adversely affected wound healing [114] |
| Chlorohexidine/Octenidine (antibacterial) | PA80/LA80 on Gunze PGA suture (Gunze Limited, Tokyo, Japan) | Dip coating | In vitro | Coated sutures were effective against multiple species within 48 h [115] |
| Cefotaxime & Chitosan (antibacterial) | PLLA | Electrospinning (cefotaxime: core-sheath or blend), braiding and dipping in chitosan solution | In vitro | Constant drug release was observed for core-sheath. Mild tissue reactivity [104] |
| Chitosan (antibacterial) | Braided silk sutures | Coating | In vitro | Increased knot strength of suture, both E. coli and S aureus were inhibited [116] |
| Curcumin hydrochloride (antibacterial/anti-inflammatory) | PLLA | Electrospinning (curcumin hydrochloride blend) | Preclinical | Curcumin-loaded sutures exhibited superior mechanical strength. Optimized suture released the drug in a controlled manner. Improved antibacterial properties, marked antiplatelet performance, and good biocompatibility were observed [100] |
| Ibuprofen (anti-inflammatory) | Braided polyglycolide thread/Poly(p-dioxanone) monofilaments | Coating | N/A | Drug release began with initial burst followed by then sustained release [117] |
| Ibuprofen (anti-inflammatory) | PLGA sheets braided on VICRYL™W9114 suture (Ethicon, Cincinnati, Ohio, USA ) | Electrospinning (single/multiple layered sheets) | Preclinical | Drug loading was reproducible, multiple layers prolonged drug release. Pain relief efficacy similar to oral drug administration. Fabrication method is not scalable [105] |
| Diclofenac (anti-inflammatory) | PLGA sheets braided on 3-0 VICRYL™W9114 suture (Ethicon, Cincinnati, Ohio, USA ) | Electrospinning | Preclinical | Sustained drug release was attained. Pain was mitigated throughout the wound healing period. Recruitment of inflammatory cells was suppressed [118]. |
| VEGF (Proliferation enhancer) | PDLLA (VEGF blend) on Ethibond™ suture (Ethicon, Cincinnati, Ohio, USA ) | Coating | Preclinical | Meniscal healing did not improve, and angiogenesis did not increase [119] |
| VEGF (Proliferation enhancer) | PLLA (VEGF blend) on EthiconPDS™ suture (Ethicon, Cincinnati, Ohio, USA ) | Coating | Preclinical | Biological activity and cellular viability increased [120] |
| Norepinephrine/dopamine (bioadhesive) | Collagen-CaCO3 PNE composite scaffold | Electrospinning & complexation | In vitro | Satisfactory cellular adhesion, proliferation and differentiation of human fetal osteoblasts. Potential osteoconductive scaffolds for bone tissue engineering [121] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akombaetwa, N.; Bwanga, A.; Makoni, P.A.; Witika, B.A. Applications of Electrospun Drug-Eluting Nanofibers in Wound Healing: Current and Future Perspectives. Polymers 2022, 14, 2931. https://doi.org/10.3390/polym14142931
Akombaetwa N, Bwanga A, Makoni PA, Witika BA. Applications of Electrospun Drug-Eluting Nanofibers in Wound Healing: Current and Future Perspectives. Polymers. 2022; 14(14):2931. https://doi.org/10.3390/polym14142931
Chicago/Turabian StyleAkombaetwa, Nakamwi, Alick Bwanga, Pedzisai Anotida Makoni, and Bwalya A. Witika. 2022. "Applications of Electrospun Drug-Eluting Nanofibers in Wound Healing: Current and Future Perspectives" Polymers 14, no. 14: 2931. https://doi.org/10.3390/polym14142931