
Polymer-Based Bone Substitutes in Periodontal Infrabony Defects: A Systematic Evaluation of Clinical Studies

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Literature Search
2.3. Data Extraction
2.4. Statistical Analysis
2.5. Risk of Bias
3. Results
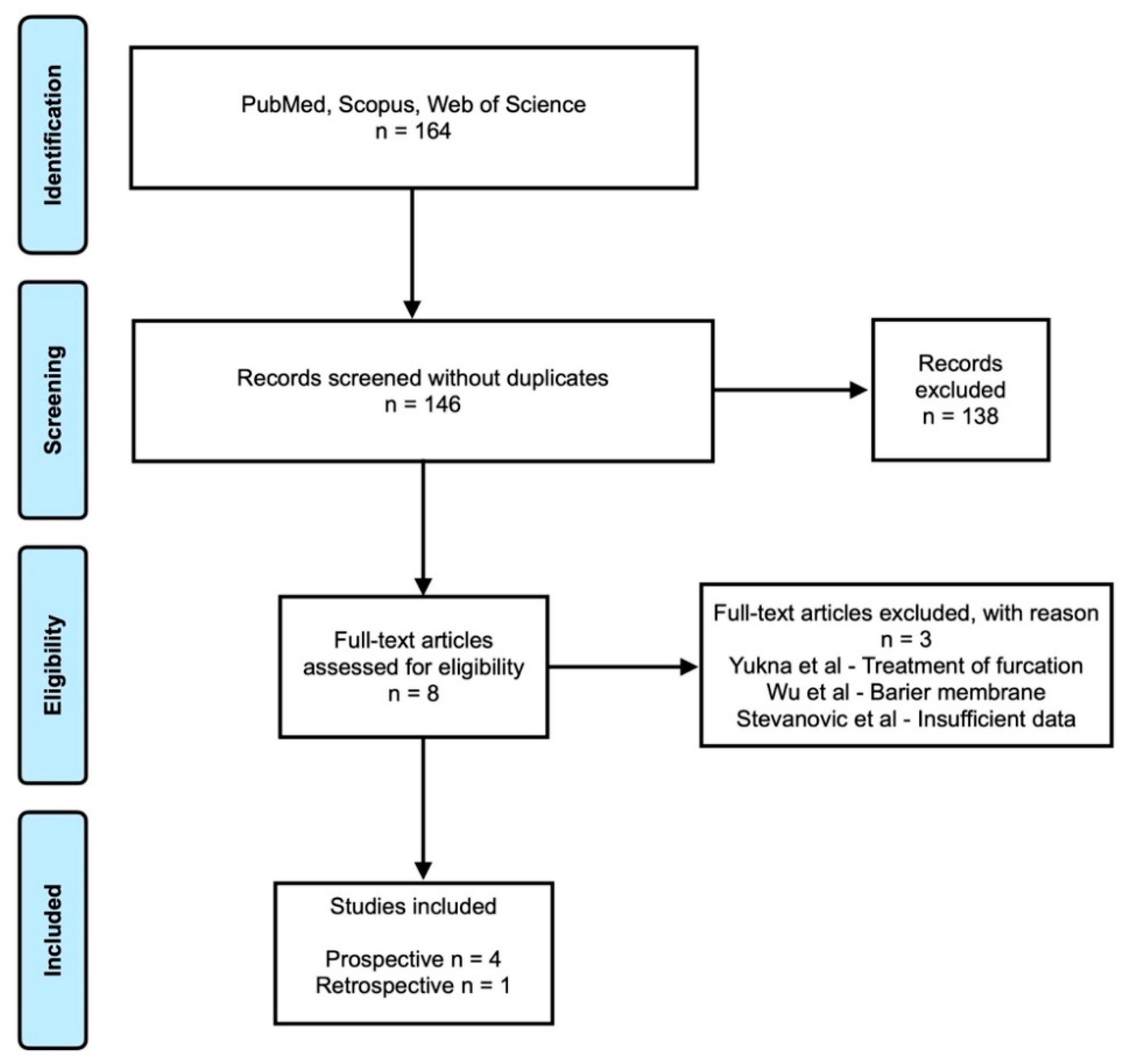
3.1. Search Results
3.2. General Characteristics
3.3. Clinical Assesment of Periodontal Disease and Infrabony Defects
3.4. Treatment of Infrabony Defect with Polymer Based Bone Substitute
3.5. Quality of the Included Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Costantini, E.; Sinjari, B.; Piscopo, F.; Porreca, A.; Reale, M.; Caputi, S.; Murmura, G. Evaluation of Salivary Cytokines and Vitamin D Levels in Periodontopathic Patients. Int. J. Mol. Sci. 2020, 21, 2269. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 45 (Suppl. S2), S149–S161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mester, A.; Ciobanu, L.; Taulescu, M.; Apostu, D.; Lucaciu, O.; Filip, G.A.; Feldrihan, V.; Licarete, E.; Ilea, A.; Piciu, A.; et al. Periodontal disease may induce liver fibrosis in an experimental study on Wistar rats. J. Periodontol. 2019, 90, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Rexhepi, I.; Paolantonio, M.; Romano, L.; Serroni, M.; Santamaria, P.; Secondi, L.; Paolantonio, G.; Sinjari, B.; De Ninis, P.; Femminella, B. Efficacy of inorganic bovine bone combined with leukocyte and platelet-rich fibrin or collagen membranes for treating unfavorable periodontal infrabony defects: Randomized non-inferiority trial. J. Periodontol. 2021, 92, 1576–1587. [Google Scholar] [CrossRef] [PubMed]
- Stefanini, M.; Bianchelli, D.; Sangiorgi, M. Porcine-derived acellular dermal collagen matrix and enamel matrix derivative for the treatment of infrabony defect in the esthetic area. Plast. Aesthetic Res. 2021, 2021, 2–11. [Google Scholar] [CrossRef]
- Solakoglu, Ö.; Heydecke, G.; Amiri, N.; Anitua, E. The use of plasma rich in growth factors (PRGF) in guided tissue regeneration and guided bone regeneration. A review of histological, immunohistochemical, histomorphometrical, radiological and clinical results in humans. Ann. Anat.-Anat. Anz. 2020, 231, 151528. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Yuan, Z.; Han, F.; Zhu, C.; Li, B. Polymeric biomaterials for bone regeneration. Ann. Jt. 2016, 1, 27. [Google Scholar] [CrossRef]
- Sanz, M.; Dahlin, C.; Apatzidou, D.; Artzi, Z.; Bozic, D.; Calciolari, E.; De Bruyn, H.; Dommisch, H.; Donos, N.; Eickholz, P.; et al. Biomaterials and regenerative technologies used in bone regeneration in the craniomaxillofacial region: Consensus report of group 2 of the 15th European Workshop on Periodontology on Bone Regeneration. J. Clin. Periodontol. 2019, 46 (Suppl. S2), 82–91. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Sun, X.; Yu, J.; Wang, J.; Zhai, P.; Chen, S.; Liu, M.; Zhou, Y. Platelet-Rich Fibrin as a Bone Graft Material in Oral and Maxillofacial Bone Regeneration: Classification and Summary for Better Application. Biomed. Res. Int. 2019, 2019, 3295756. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yukna, R.A. HTR polymer grafts in human periodontal osseous defects. I. 6-month clinical results. J. Periodontol. 1990, 61, 633–642. [Google Scholar] [CrossRef] [PubMed]
- Meadows, C.L.; Gher, M.E.; Quintero, G.; Lafferty, T.A. A comparison of polylactic acid granules and decalcified freeze-dried bone allograft in human periodontal osseous defects. J. Periodontol. 1993, 64, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Prakash, S.; Sunitha, J.; Abid, S. Evaluation of HTR polymer (Bioplant HTR) as a bone graft material in the treatment of interproximal vertical bony defects: A clinical and radiological study. Indian J. Dent. Res. 2010, 21, 179–184. [Google Scholar] [CrossRef]
- Chhabra, V.; Gill, A.S.; Sikri, P.; Bhaskar, N. Evaluation of the relative efficacy of copolymerized polylactic-polyglycolic acids alone and in conjunction with polyglactin 910 membrane in the treatment of human periodontal infrabony defects: A clinical and radiological study. Indian J. Dent. Res. 2011, 22, 83–89. [Google Scholar] [CrossRef]
- Verardi, S.; Lombardi, T.; Stacchi, C. Clinical and Radiographic Evaluation of Nanohydroxyapatite Powder in Combination with Polylactic Acid/Polyglycolic Acid Copolymer as Bone Replacement Graft in the Surgical Treatment of Intrabony Periodontal Defects: A Retrospective Case Series Study. Materials 2020, 13, 269. [Google Scholar] [CrossRef] [Green Version]
- Yukna, R.A.; Yukna, C.N. Six-year clinical evaluation of HTR synthetic bone grafts in human grade II molar furcations. J. Periodontal Res. 1997, 32, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-Y.; Chen, Y.-T.; Chen, C.-W.; Chi, L.-Y.; Hsu, N.-Y.; Hung, S.-L.; Ling, L.-J. Comparison of clinical outcomes following guided tissue regeneration treatment with a polylactic acid barrier or a collagen membrane. Int. J. Periodontics Restor. Dent. 2010, 30, 173–179. [Google Scholar]
- Stevanović, M.; Biočanin, V.; Nedkić, M.; Ignjatović, N. Efficacy of nanocrystalline bone substitute biphasic calcium phosphate/poly-DL-lactide-co-glycolide for periodontal intrabony defects filling. Vojnosanit. Pregl. 2015, 72, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Fernandez de Grado, G.; Keller, L.; Idoux-Gillet, Y.; Wagner, Q.; Musset, A.-M.; Benkirane-Jessel, N.; Bornert, F.; Offner, D. Bone substitutes: A review of their characteristics, clinical use, and perspectives for large bone defects management. J. Tissue Eng. 2018, 9, 2041731418776819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campana, V.; Milano, G.; Pagano, E.; Barba, M.; Cicione, C.; Salonna, G.; Lattanzi, W.; Logroscino, G. Bone substitutes in orthopaedic surgery: From basic science to clinical practice. J. Mater. Sci. Mater. Med. 2014, 25, 2445–2461. [Google Scholar] [CrossRef] [PubMed]
- Lopes, M.S.; Jardini, A.L.; Filho, R.M. Poly (Lactic Acid) Production for Tissue Engineering Applications. Procedia Eng. 2012, 42, 1402–1413. [Google Scholar] [CrossRef] [Green Version]
- Teparat, T.; Solt, C.W.; Claman, L.J.; Beck, F.M. Clinical comparison of bioabsorbable barriers with non-resorbable barriers in guided tissue regeneration in the treatment of human intrabony defects. J. Periodontol. 1998, 69, 632–641. [Google Scholar] [CrossRef]
- Budak, K.; Sogut, O.; Aydemir Sezer, U. A review on synthesis and biomedical applications of polyglycolic acid. J. Polym. Res. 2020, 27, 1–19. [Google Scholar] [CrossRef]
- Stavropoulos, A.; Sculean, A.; Karring, T. GTR treatment of intrabony defects with PLA/PGA copolymer or collagen bioresorbable membranes in combination with deproteinized bovine bone (Bio-Oss). Clin. Oral Investig. 2004, 8, 226–232. [Google Scholar] [CrossRef]
- Osathanon, T.; Chanjavanakul, P.; Kongdecha, P.; Clayhan, P.; Huynh, N.C.-N. Polycaprolactone-Based Biomaterials for Guided Tissue Regeneration Membrane. In Periodontitis—A Useful Ref; IntechOpen: London, UK, 2017. [Google Scholar]
- Park, J.; Park, S.; Kim, J.E.; Jang, K.-J.; Seonwoo, H.; Chung, J.H. Enhanced Osteogenic Differentiation of Periodontal Ligament Stem Cells Using a Graphene Oxide-Coated Poly(ε-caprolactone) Scaffold. Polymers 2021, 13, 797. [Google Scholar] [CrossRef] [PubMed]
- Terzopoulou, Z.; Baciu, D.; Gounari, E.; Steriotis, T.; Charalambopoulou, G.; Tzetzis, D.; Bikiaris, D. Composite Membranes of Poly(ε-caprolactone) with Bisphosphonate-Loaded Bioactive Glasses for Potential Bone Tissue Engineering Applications. Molecules 2019, 24, 3067. [Google Scholar] [CrossRef] [Green Version]
- Toledano, M.; Toledano-Osorio, M.; Carrasco-Carmona, Á.; Vallecillo, C.; Toledano, R.; Medina-Castillo, A.L.; Osorio, R. State of the Art on Biomaterials for Soft Tissue Augmentation in the Oral Cavity. Part II: Synthetic Polymers-Based Biomaterials. Polymers 2020, 12, 1845. [Google Scholar] [CrossRef]
- Haugen, H.J.; Lyngstadaas, S.P.; Rossi, F.; Perale, G. Bone grafts: Which is the ideal biomaterial? J. Clin. Periodontol. 2019, 46 (Suppl. S2), 92–102. [Google Scholar] [CrossRef]
- Amini, A.R.; Laurencin, C.T.; Nukavarapu, S.P. Bone tissue engineering: Recent advances and challenges. Crit. Rev. Biomed. Eng. 2012, 40, 363–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukuba, S.; Okada, M.; Nohara, K.; Iwata, T. Alloplastic Bone Substitutes for Periodontal and Bone Regeneration in Dentistry: Current Status and Prospects. Materials 2021, 14, 1096. [Google Scholar] [CrossRef]
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments. Molecules 2021, 26, 3007. [Google Scholar] [CrossRef] [PubMed]
- Ai, C.; Sheng, D.; Chen, J.; Cai, J.; Wang, S.; Jiang, J.; Chen, S. Surface modification of vascular endothelial growth factor-loaded silk fibroin to improve biological performance of ultra-high-molecular-weight polyethylene via promoting angiogenesis. Int. J. Nanomed. 2017, 12, 7737–7750. [Google Scholar] [CrossRef] [Green Version]
- Kashirina, A.; Yao, Y.; Liu, Y.; Leng, J. Biopolymers as bone substitutes: A review. Biomater. Sci. 2019, 7, 3961–3983. [Google Scholar] [CrossRef] [PubMed]
- Guduric, V.; Metz, C.; Siadous, R.; Bareille, R.; Levato, R.; Engel, E.; Fricain, J.-C.; Devillard, R.; Luzanin, O.; Catros, S. Layer-by-layer bioassembly of cellularized polylactic acid porous membranes for bone tissue engineering. J. Mater. Sci. Mater. Med. 2017, 28, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedberg, E.L.; Kroese-Deutman, H.C.; Shih, C.K.; Crowther, R.S.; Carney, D.H.; Mikos, A.G.; Jansen, J.A. In vivo degradation of porous poly(propylene fumarate)/poly(DL-lactic-co-glycolic acid) composite scaffolds. Biomaterials 2005, 26, 4616–4623. [Google Scholar] [CrossRef] [PubMed]
- Miron, R.J.; Zucchelli, G.; Pikos, M.A.; Salama, M.; Lee, S.; Guillemette, V.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Wang, H.-L.; et al. Use of platelet-rich fibrin in regenerative dentistry: A systematic review. Clin. Oral Investig. 2017, 21, 1913–1927. [Google Scholar] [CrossRef]


{kind=link}
| Author. Year. Country | Study Type | Patients’ Characteristics | Measurements | Results | Conclusion | |
|---|---|---|---|---|---|---|
| Pre-Operative | Post-Operative | |||||
| Yukna. 1990. USA [12] | Prospective | n = 21 Male: 14 Female: 7 Age: 29–69 years (mean age 40.6 years) Control: OFD Experimental: polymer bone | O’Leary index PD Periapical radiographs | (a) PD (mm) Control: 6.00 ± 1.3 Experimental: 6.4 ± 1.3 | (a) PD (mm)–6 months Control: 3.7 ± 0.6 Experimental: 3.3 ± 0.8 (b) Gain clinical attachment (mm)–6 months Control: 1.0 ± 0.9 Experimental: 1.9 ± 1.1 (c) % Defect fill–6 months Control: 9% Experimental: 76% | Polymer bone substitute showed better results for the repair of periodontal osseous defect compared to OFD. |
| Meadows. 1993. USA [13] | Prospective | n = 10 Male: 6 Female: 4 Age: 28–58 years (mean age 42 years) | Modified O’Leary index BOP PD Defect depth Tooth mobility Periapical radiographs Photomicrographs | (a) PD (mm) FPD: 6.30 ± 1.70 DFDBA: 7.45 ± 2.25 PLA: 6.85 ± 1.63 (b) Defect depth (mm) FPD: 3.55 ± 1.34 DFDBA: 4.65 ± 0.94 PLA: 4.50 ± 1.43 | (a) PD (mm)–6 months FPD: 2.90 ± 1.28 DFDBA: 3.30 ± 1.13 PLA: 5.05 ± 1.72 (b) Defect depth (mm)–6 months FPD: 1.85 ± 1.65 DFDBA: 1.05 ± 0.82 PLA: 2.85 1.31 (c) % Defect fill–6 months FPD: 11.2% DFDBA: 65% PLA: 2.2% | DFDBA showed the greatest amount of osseous defect fill. PLA did not show comparable results compared to FPD. |
| Prakash. 2010. India [14] | Prospective | n = 5 Age: 33- 55 years Control: OFD Experimental: polymer bone | Plaque index Gingival index PD CAL Periapical radiographs | (a) PD (mm) Control: 7.13 ± 1.25 Experimental: 7.88 ± 1.46 (b) CAL (mm) Control: 7.38 ± 2.33 Experimental: 8.00 ± 1.41 (c) Initial defect fill Control: 14.10 ± 5.0 Experimental: 18.56 ± 7.95 | (a) PD (mm)–3 months Control: 5.38 ± 0.92 Experimental: 4.38 ± 1.06 PD (mm)–6 months Control: 5.38 ± 0.74 Experimental: 4.75 ± 0.89 (b) CAL (mm)–3 months Control: 6.50 ± 2.27 Experimental: 5.75 ± 1.28 CAL (mm)–6 months Control: 6.00 ± 2.20 Experimental: 5.50 ± 1.20 (c) Defect fill–6 months Control: 11.30 ± 7.7 Experimental: 9.50 ± 4.80 % Defect fill–6 months Control: 26.7% Experimental: 44% | Polymer bone substitute showed better results than OFD in terms of both clinical and radiographic analysis. |
| Chhabra. 2011. India [15] | Prospective | n = 40 Group A: copolymerized polylactic-polyglycolic acids alone Group B: copolymerized polylactic-polyglycolic acids in conjunction with polyglactin 910 membrane | PD CAL Periapical radiographs | (a) PD (mm) Group A: 6.40 ± 0.32 Group B: 7.25 ± 0.40 (b) CAL (mm) Group A: 6.30 ± 0.40 Group B: 6.50 ± 0.43 (c) Initial defect fill (mm) Group A: 10.73 ± 0.48 Group B: 11.75 ± 0.56 | (a) PD (mm)–3 months Group A: 3.75 ± 0.24 Group B: 4.25 ± 0.37 PD (mm)–6 months Group A: 3.05 ± 0.25 Group B: 3.10 ± 0.25 (b) CAL (mm)–3 months Group A: 3.75 ± 0.26 Group B: 3.95 ± 0.47 CAL (mm)–6 months Group A: 2.95 ± 0.23 Group B: 3.20 ± 0.40 (c) Defect fill–3 months (mm) Group A: 8.71 ± 0.44 Group B: 9.41 ± 0.32 Defect fill–6 months (mm) Group A: 8.05 ± 0.44 Group B: 8.68 ± 0.34 | Both methods are beneficial for the treatment of infrabony defects. |
| Veradi. 2019. USA [16] | Retrospective | n = 25 Male: 13 Female: 12 Age: 28–58 years (mean age 55.1 ± 10.5 years) NHA in combination with PLGA copolymer | Full mouth plaque score PD CAL Periapical radiographs | (a) PD (mm) 8.32 ± 1.41 (b) CAL (mm) 9.96 ± 1.69 | (a) PD–12 months (mm) 4.04 ± 0.84 (b) CAL–12 months (mm) 6.24 ± 1.71 (c) Defect fill–12 months (mm) 4.06 ± 1.66 % Defect fill–12 months 73.3% | NHA in combination with PLGA may give significant improvements for infrabony defects. This case series should not be generalized to larger population. |
| Reference | Study Design | Participants | Sample Size | Variable Description | Potential Confounders | Outcome Measurements | Statistical Analysis | Total Score |
|---|---|---|---|---|---|---|---|---|
| Yukna [12] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Meadows [13] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Prakash [14] | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 5 |
| Chhabra [15] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Veradi [16] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onisor, F.; Bran, S.; Mitre, I.; Mester, A.; Voina-Tonea, A.; Armencea, G.; Baciut, M. Polymer-Based Bone Substitutes in Periodontal Infrabony Defects: A Systematic Evaluation of Clinical Studies. Polymers 2021, 13, 4445. https://doi.org/10.3390/polym13244445
Onisor F, Bran S, Mitre I, Mester A, Voina-Tonea A, Armencea G, Baciut M. Polymer-Based Bone Substitutes in Periodontal Infrabony Defects: A Systematic Evaluation of Clinical Studies. Polymers. 2021; 13(24):4445. https://doi.org/10.3390/polym13244445
Chicago/Turabian StyleOnisor, Florin, Simion Bran, Ileana Mitre, Alexandru Mester, Andrada Voina-Tonea, Gabriel Armencea, and Mihaela Baciut. 2021. "Polymer-Based Bone Substitutes in Periodontal Infrabony Defects: A Systematic Evaluation of Clinical Studies" Polymers 13, no. 24: 4445. https://doi.org/10.3390/polym13244445