
Multipurpose Prevention Technologies: Oral, Parenteral, and Vaginal Dosage Forms for Prevention of HIV/STIs and Unplanned Pregnancy

Abstract
:
1. Introduction
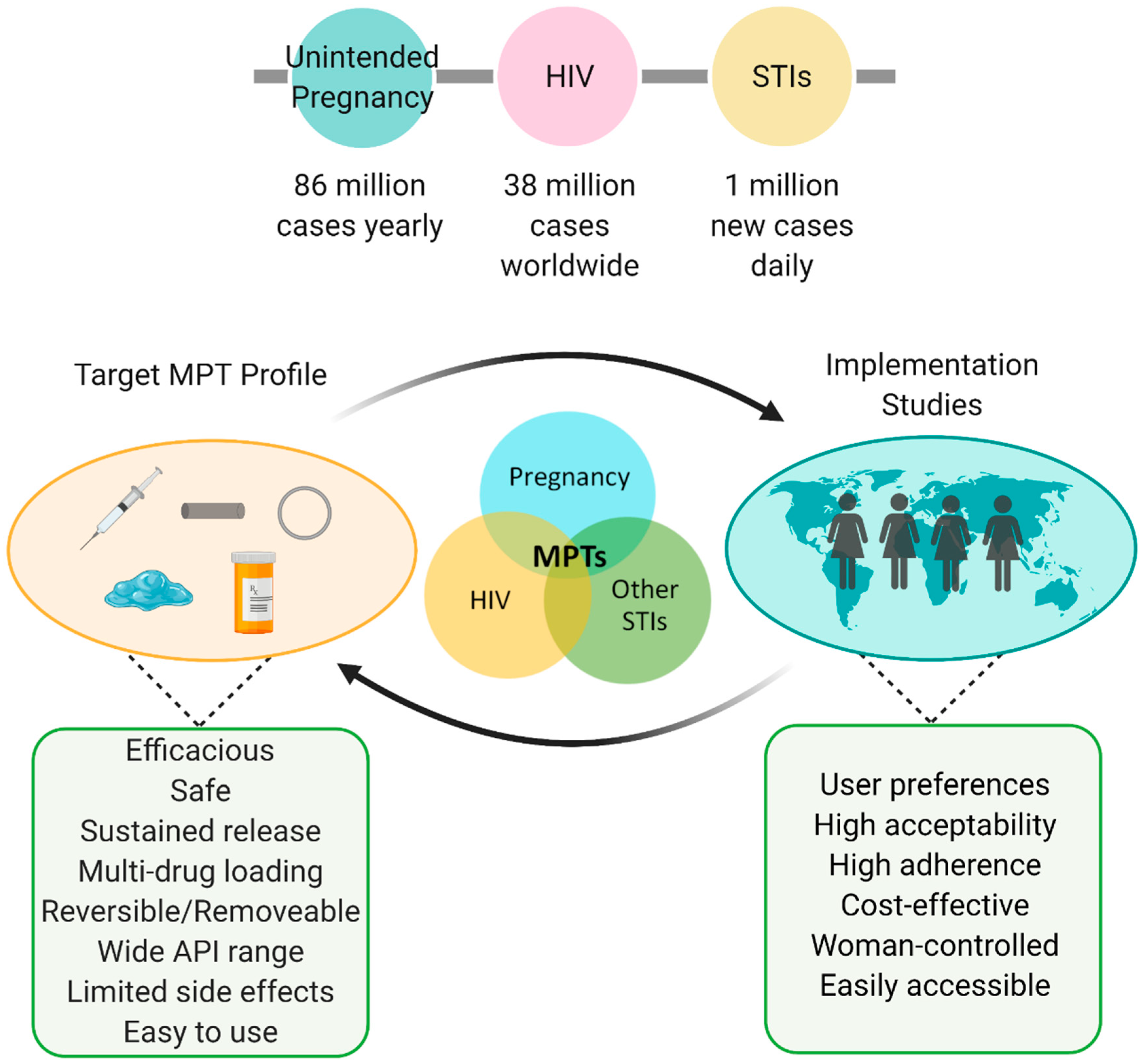
1.1. Prevalence of HIV, STIs, and Unplanned Pregnancy
1.2. Discontinuation of Current Treatments
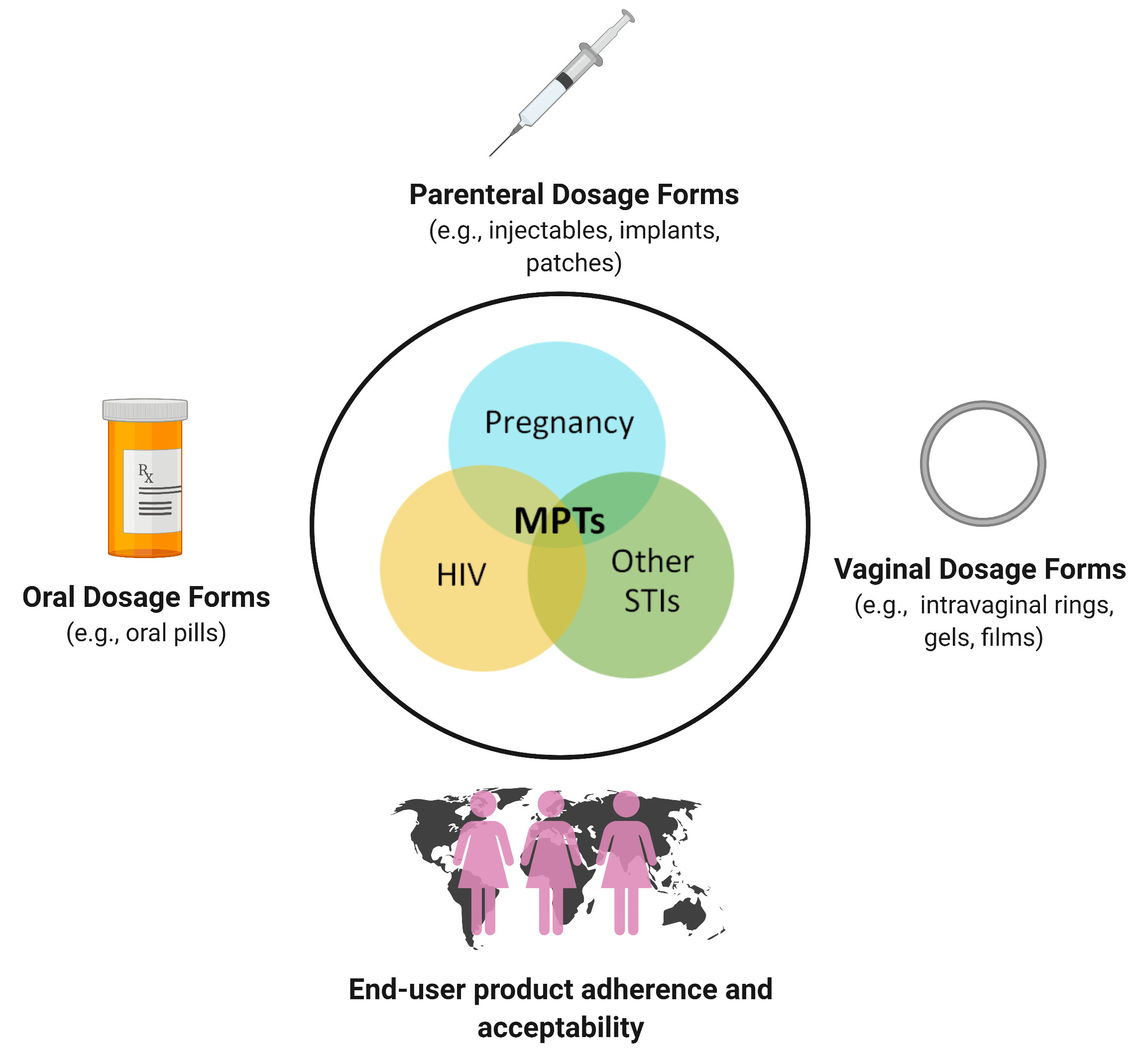
1.3. Sustained Release Systems and Multipurpose Prevention Technologies
2. Method for Literature Search and Collection of Articles
3. Orally Delivered MPTs
4. Parenterally Delivered MPTs
5. Vaginally Delivered MPTs
5.1. Vaginal Films, Gels, and Tablets
5.2.1. Intravaginal Rings
5.2.2. Manufacturing Limitations and Emerging IVR Technologies
6. MPT Implementation Studies
7. MPT Development Considerations, Challenges, and Limitations
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Disclosure Statement
References
- The Global HIV/AIDS Epidemic. Available online: https://www.hiv.gov/hiv-basics/overview/data-and-trends/global-statistics#:~:text=Number%20of%20People%20with%20HIV,(%3C15%20years%20old) (accessed on 31 May 2021).
- World Health Organization: Sexually Transmitted Infections (STIs). Available online: https://www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis) (accessed on 31 May 2021).
- Centers for Disease Control and Prevention: Unintended Pregnancy. Available online: https://www.cdc.gov/reproductivehealth/contraception/unintendedpregnancy/index.htm (accessed on 31 May 2021).
- HIV/AIDS: Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/hiv-aids (accessed on 31 May 2021).
- Global HIV & AIDS Statistics—2020 Fact Sheet. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 31 May 2021).
- Reported STDs Reach All-time High for 6th Consecutive Year. Available online: https://www.cdc.gov/media/releases/2021/p0413-stds.html (accessed on 31 May 2021).
- Chesson, H.W.; Dunne, E.F.; Hariri, S.; Markowitz, L.E. The estimated lifetime probability of acquiring human papillomavirus in the United States. Sex. Transm. Dis. 2014, 41, 660–664. [Google Scholar] [CrossRef]
- Saraiya, M.; Unger, E.R.; Thompson, T.D.; Lynch, C.F.; Hernandez, B.Y.; Lyu, C.W.; Steinau, M.; Watson, M.; Wilkinson, E.J.; Hopenhayn, C.; et al. US assessment of HPV types in cancers: Implications for current and 9-valent HPV vaccines. J. Natl. Cancer Inst. 2015, 107, djv086. [Google Scholar] [CrossRef] [Green Version]
- Bellizzi, S.; Mannava, P.; Nagai, M.; Sobel, H.L. Reasons for discontinuation of contraception among women with a current unintended pregnancy in 36 low and mid-dle-income countries. Contraception 2020, 101, 26–33. [Google Scholar] [CrossRef]
- Ganatra, B.; Gerdts, C.; Rossier, C.; Johnson, B.R., Jr.; Tuncalp, O.; Assifi, A.; Sedgh, G.; Singh, S.; Bankole, A.; Popinchalk, A.; et al. Global, regional, and subregional classification of abortions by safety, 2010–2014: Estimates from a Bayesian hierarchical model. Lancet 2017, 390, 2372–2381. [Google Scholar] [CrossRef] [Green Version]
- Gipson, J.D.; Koenig, M.A.; Hindin, M.J. The effects of unintended pregnancy on infant, child, and parental health: A review of the literature. Stud. Fam. Plann. 2008, 39, 18–38. [Google Scholar] [CrossRef]
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000-15: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef] [Green Version]
- Blencowe, H.; Cousens, S.; Jassir, F.B.; Say, L.; Chou, D.; Mathers, C.; Hogan, D.; Shiekh, S.; Qureshi, Z.U.; You, D.; et al. National, regional, and worldwide estimates of stillbirth rates in 2015, with trends from 2000: A systematic analysis. Lancet Glob. Health 2016, 4, e98–e108. [Google Scholar] [CrossRef] [Green Version]
- Garg, A.B.; Nuttall, J.; Romano, J. The future of HIV microbicides: Challenges and opportunities. Antivir. Chem. Chemother. 2009, 19, 143–150. [Google Scholar] [CrossRef]
- Senise, J.F.; Castelo, A.; Martinez, M. Current treatment strategies, complications and considerations for the use of HIV antiretroviral therapy during pregnancy. AIDS Rev. 2011, 13, 198–213. [Google Scholar]
- Nelson, A.G.; Zhang, X.; Ganapathi, U.; Szekely, Z.; Flexner, C.W.; Owen, A.; Sinko, P.J. Drug delivery strategies and systems for HIV/AIDS pre-exposure prophylaxis and treatment. J. Control. Release 2015, 219, 669–680. [Google Scholar] [CrossRef] [Green Version]
- Kirtane, A.R.; Abouzid, O.; Minahan, D.; Bensel, T.; Hill, A.L.; Selinger, C.; Bershteyn, A.; Craig, M.; Mo, S.S.; Mazdiyasni, H.; et al. Development of an oral once-weekly drug delivery system for HIV antiretroviral therapy. Nat. Commun. 2018, 9, 2. [Google Scholar] [CrossRef]
- Velloza, J.; Khoza, N.; Scorgie, F.; Chitukuta, M.; Mutero, P.; Mutiti, K.; Mangxilana, N.; Nobula, L.; Bulterys, M.A.; Atujuna, M.; et al. The influence of HIV-related stigma on PrEP disclosure and adherence among adolescent girls and young women in HPTN 082: A qualitative study. J. Int. AIDS Soc. 2020, 23, e25463. [Google Scholar] [CrossRef]
- Essien, T.; Mhlanga, N.; Hinson, K.; Mzizi, P.; Johnson, A.; Chasakara, C.; Yola, N.; Nobanda, S.; Delany-Moretlwe, S.; Celum, C.; et al. Engaging Adolescent Girls and Young Women in HPTN 082: Lessons Learned from an Oral PrEP Study. In Proceedings of the International AIDS Society (IAS), Mexico City, Mexico, 21–24 July 2019. [Google Scholar]
- Minnis, A.M.; Krogstad, E.; Shapley-Quinn, M.K.; Agot, K.; Ahmed, K.; Danielle Wagner, L.; van der Straten, A.; Team, T.S. Giving voice to the end-user: Input on multipurpose prevention technologies from the perspectives of young women in Kenya and South Africa. Sex. Reprod. Health Matters 2021, 29, 1927477. [Google Scholar] [CrossRef]
- Sullivan, P.S.; Mena, L.; Elopre, L.; Siegler, A.J. Implementation Strategies to Increase PrEP Uptake in the South. Curr. HIV/AIDS Rep. 2019, 16, 259–269. [Google Scholar] [CrossRef]
- Thurman, A.R.; Clark, M.R.; Hurlburt, J.A.; Doncel, G.F. Intravaginal rings as delivery systems for microbicides and multipurpose prevention technologies. Int. J. Womens Health 2013, 5, 695–708. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, T.; Baxi, K.; Sawarkar, S.; Sarmento, B.; das Neves, J. Vaginal multipurpose prevention technologies: Promising approaches for enhancing women’s sexual and reproductive health. Expert Opin. Drug Deliv. 2020, 17, 379–393. [Google Scholar] [CrossRef]
- Markowitz, M.; Gettie, A.; Bernard, L.; Blanchard, J.; Grasperge, B.; Fillgrove, K.; Xue, L.; Dube, N.; Hazuda, D. Weekly Oral Islatravir Provides Effective PEP Against IV Challenge with SIVMAC251. In Proceedings of the Conference on Retroviruses and Opportunistic Infections (CROI), Boston, MA, USA, 8–11 March 2020. [Google Scholar]
- Pons-Faudoa, F.P.; Sizovs, A.; Di Trani, N.; Paez-Mayorga, J.; Bruno, G.; Rhudy, J.; Manohar, M.; Gwenden, K.; Martini, C.; Chua, C.Y.X.; et al. 2-Hydroxypropyl-beta-cyclodextrin-enhanced pharmacokinetics of cabotegravir from a nanofluidic implant for HIV pre-exposure prophylaxis. J. Control. Release 2019, 306, 89–96. [Google Scholar] [CrossRef]
- Landovitz, R.J.; Li, S.; Grinsztejn, B.; Dawood, H.; Liu, A.Y.; Magnus, M.; Hosseinipour, M.C.; Panchia, R.; Cottle, L.; Chau, G.; et al. Safety, tolerability, and pharmacokinetics of long-acting injectable cabotegravir in low-risk HIV-uninfected individuals: HPTN 077, a phase 2a randomized controlled trial. PLoS Med. 2018, 15, e1002690. [Google Scholar] [CrossRef] [Green Version]
- Harrison, P.F.; Hemmerling, A.; Romano, J.; Whaley, K.J.; Young Holt, B. Developing multipurpose reproductive health technologies: An integrated strategy. AIDS Res. Treat. 2013, 2013, 790154. [Google Scholar] [CrossRef] [Green Version]
- Friend, D.R. An update on multipurpose prevention technologies for the prevention of HIV transmission and pregnancy. Expert Opin. Drug Deliv. 2016, 13, 533–545. [Google Scholar] [CrossRef]
- Fernandez-Romero, J.A.; Deal, C.; Herold, B.C.; Schiller, J.; Patton, D.; Zydowsky, T.; Romano, J.; Petro, C.D.; Narasimhan, M. Multipurpose prevention technologies: The future of HIV and STI protection. Trends Microbiol. 2015, 23, 429–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasserheit, J.N. Epidemiological synergy. Interrelationships between human immunodeficiency virus infection and other sexually transmitted diseases. Sex. Transm. Dis. 1992, 19, 61–77. [Google Scholar] [CrossRef]
- Looker, K.J.; Elmes, J.A.R.; Gottlieb, S.L.; Schiffer, J.T.; Vickerman, P.; Turner, K.M.E.; Boily, M.C. Effect of HSV-2 infection on subsequent HIV acquisition: An updated systematic review and meta-analysis. Lancet Infect Dis. 2017, 17, 1303–1316. [Google Scholar] [CrossRef] [Green Version]
- Giguere, R.; Carballo-Dieguez, A.; Ventuneac, A.; Mabragana, M.; Dolezal, C.; Chen, B.A.; Kahn, J.A.; Zimet, G.D.; McGowan, I. Variations in microbicide gel acceptability among young women in the USA and Puerto Rico. Cult. Health Sex. 2012, 14, 151–166. [Google Scholar] [CrossRef] [Green Version]
- Frezieres, R.G.; Walsh, T.; Kilbourne-Brook, M.; Coffey, P.S. Couples’ acceptability of the SILCS diaphragm for microbicide delivery. Contraception 2012, 85, 99–107. [Google Scholar] [CrossRef]
- Dallal Bashi, Y.H.; McCoy, C.F.; Murphy, D.J.; Boyd, P.; Spence, P.; Kleinbeck, K.; Devlin, B.; Malcolm, R.K. Towards a dapivirine and levonorgestrel multipurpose vaginal ring: Investigations into the reaction between levonorgestrel and addition-cure silicone elastomers. Int. J. Pharm. 2019, 569, 118574. [Google Scholar] [CrossRef]
- Fast Track to an MPT: Development of a Dual-Purpose Pill Containing Oral PrEP and an Oral Contraceptive. Available online: https://theimpt.org/blog/from-the-pipeline-fast-track-to-an-mpt-development-of-a-dual-purpose-pill-containing-oral-prep-and-an-oral-contraceptive/ (accessed on 31 May 2021).
- Calenda, G.; Villegas, G.; Barnable, P.; Litterst, C.; Levendosky, K.; Gettie, A.; Cooney, M.L.; Blanchard, J.; Fernandez-Romero, J.A.; Zydowsky, T.M.; et al. MZC Gel Inhibits SHIV-RT and HSV-2 in Macaque Vaginal Mucosa and SHIV-RT in Rectal Mucosa. J. Acquir. Immune Defic. Syndr. 2017, 74, e67–e74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenney, J.; Aravantinou, M.; Singer, R.; Hsu, M.; Rodriguez, A.; Kizima, L.; Abraham, C.J.; Menon, R.; Seidor, S.; Chudolij, A.; et al. An antiretroviral/zinc combination gel provides 24 hours of complete protection against vaginal SHIV infection in macaques. PLoS ONE 2011, 6, e15835. [Google Scholar] [CrossRef]
- Clark, J.T.; Clark, M.R.; Shelke, N.B.; Johnson, T.J.; Smith, E.M.; Andreasen, A.K.; Nebeker, J.S.; Fabian, J.; Friend, D.R.; Kiser, P.F. Engineering a segmented dual-reservoir polyurethane intravaginal ring for simultaneous prevention of HIV transmission and unwanted pregnancy. PLoS ONE 2014, 9, e88509. [Google Scholar] [CrossRef]
- Peet, M.M.; Agrahari, V.; Anderson, S.M.; Hanif, H.; Singh, O.N.; Thurman, A.R.; Doncel, G.F.; Clark, M.R. Topical Inserts: A Versatile Delivery Form for HIV Prevention. Pharmaceutics 2019, 11, 374. [Google Scholar] [CrossRef] [Green Version]
- Dobard, C.; Peet, M.M.; Nishiura, K.; Singh, O.N.; McCormick, T.; Mitchell, J.; Garcia-Lerma, G.; Agrahari, V.; Gupta, P.; Jonnalagadda, S.; et al. Protection against Vaginal SHIV Infection with an Insert Containing TAF and EVG. In Proceedings of the Conference on Retroviruses and Opportunisitc Infections (CROI), Seattle, WA, USA, 4–9 March 2019. [Google Scholar]
- Safety, PK, and PD Study of a Vaginal Insert Containing TAF and EVG. Available online: https://clinicaltrials.gov/ct2/show/NCT03762772 (accessed on 6 October 2020).
- Abdool Karim, Q.; Abdool Karim, S.S.; Frohlich, J.A.; Grobler, A.C.; Baxter, C.; Mansoor, L.E.; Kharsany, A.B.; Sibeko, S.; Mlisana, K.P.; Omar, Z.; et al. Effectiveness and safety of tenofovir gel, an antiretroviral microbicide, for the prevention of HIV infection in women. Science 2010, 329, 1168–1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Safety and Effectiveness of Tenofovir Gel in the Prevention of Human Immunodeficiency Virus (HIV-1) Infection in Women and the Effects of Tenofovir Gel on the Incidence of Herpes Simplex Virus (HSV-2) Infection. Available online: https://clinicaltrials.gov/ct2/show/NCT01386294 (accessed on 31 May 2021).
- Cu-Uvin, S.; Moench, T.; Politch, J.; Tashima, K.; Guthrie, K.; Cabral, H.; Nyhuis, T.; Brenna, M.; Zeitlin, L.; Spiegal, H.; et al. Phase 1 Placebo-Controlled Safety, PK, and PD Study of MB66 Anti-HIV and Anti-HSV Film. In Proceedings of the Conference on Retroviruses and Opportunisitc Infections (CROI), Boston, MA, USA, 8–11 March 2020. [Google Scholar]
- Politch, J.A.; Cu-Uvin, S.; Moench, T.R.; Tashima, K.T.; Marathe, J.G.; Guthrie, K.M.; Cabral, H.; Nyhuis, T.; Brennan, M.; Zeitlin, L.; et al. Safety, acceptability, and pharmacokinetics of a monoclonal antibody-based vaginal multipurpose prevention film (MB66): A Phase I randomized trial. PLoS Med. 2021, 18, e1003495. [Google Scholar] [CrossRef]
- Tuyama, A.C.; Cheshenko, N.; Carlucci, M.J.; Li, J.H.; Goldberg, C.L.; Waller, D.P.; Anderson, R.A.; Profy, A.T.; Klotman, M.E.; Keller, M.J.; et al. ACIDFORM inactivates herpes simplex virus and prevents genital herpes in a mouse model: Optimal candidate for microbicide combinations. J. Infect. Dis. 2006, 194, 795–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, M.J.; Carpenter, C.A.; Lo, Y.; Einstein, M.H.; Liu, C.; Fredricks, D.N.; Herold, B.C. Phase I randomized safety study of twice daily dosing of acidform vaginal gel: Candidate antimicrobial contraceptive. PLoS ONE 2012, 7, e46901. [Google Scholar] [CrossRef] [Green Version]
- Rupp, R.; Rosenthal, S.L.; Stanberry, L.R. VivaGel (SPL7013 Gel): A candidate dendrimer--microbicide for the prevention of HIV and HSV infection. Int. J. Nanomed. 2007, 2, 561–566. [Google Scholar]
- Price, C.F.; Tyssen, D.; Sonza, S.; Davie, A.; Evans, S.; Lewis, G.R.; Xia, S.; Spelman, T.; Hodsman, P.; Moench, T.R.; et al. SPL7013 Gel (VivaGel(R)) retains potent HIV-1 and HSV-2 inhibitory activity following vaginal administration in humans. PLoS ONE 2011, 6, e24095. [Google Scholar] [CrossRef] [Green Version]
- Begg, L.; Brodsky, R.; Friedland, B.; Mathur, S.; Sailer, J.; Creasy, G. Estimating the market size for a dual prevention pill: Adding contraception to pre-exposure prophylaxis (PrEP) to increase uptake. BMJ Sex. Reprod. Health 2020, 47, 166–172. [Google Scholar] [CrossRef]
- Population Council: Developing an Oral Contraceptive and HIV-Prevention Method, in a Single Pill. Available online: https://www.popcouncil.org/research/developing-an-oral-contraceptive-and-hiv-prevention-method-in-a-single-pill (accessed on 5 October 2020).
- Markowitz, M.; Grobler, J.A. Islatravir for the treatment and prevention of infection with the human immunodeficiency virus type 1. Curr. Opin. HIV AIDS 2020, 15, 27–32. [Google Scholar] [CrossRef]
- Kawamoto, A.; Kodama, E.; Sarafianos, S.G.; Sakagami, Y.; Kohgo, S.; Kitano, K.; Ashida, N.; Iwai, Y.; Hayakawa, H.; Nakata, H.; et al. 2′-deoxy-4′-C-ethynyl-2-halo-adenosines active against drug-resistant human immunodeficiency virus type 1 variants. Int. J. Biochem. Cell Biol. 2008, 40, 2410–2420. [Google Scholar] [CrossRef] [PubMed]
- Ohrui, H.; Kohgo, S.; Hayakawa, H.; Kodama, E.; Matsuoka, M.; Nakata, T.; Mitsuya, H. 2′-deoxy-4′-C-ethynyl-2-fluoroadenosine: A nucleoside reverse transcriptase inhibitor with highly potent activity against wide spectrum of HIV-1 strains, favorable toxic profiles, and stability in plasma. Nucleosides Nucleotides Nucleic Acids 2007, 26, 1543–1546. [Google Scholar] [CrossRef]
- Murphey-Corb, M.; Rajakumar, P.; Michael, H.; Nyaundi, J.; Didier, P.J.; Reeve, A.B.; Mitsuya, H.; Sarafianos, S.G.; Parniak, M.A. Response of simian immunodeficiency virus to the novel nucleoside reverse transcriptase inhibitor 4’-ethynyl-2-fluoro-2’-deoxyadenosine in vitro and in vivo. Antimicrob. Agents Chemother. 2012, 56, 4707–4712. [Google Scholar] [CrossRef] [Green Version]
- Markowitz, M.; Gettie, A.; St Bernard, L.; Andrews, C.D.; Mohri, H.; Horowitz, A.; Grasperge, B.F.; Blanchard, J.L.; Niu, T.; Sun, L.; et al. Once-Weekly Oral Dosing of MK-8591 Protects Male Rhesus Macaques from Intrarectal Challenge with SHIV109CP3. J. Infect. Dis. 2020, 221, 1398–1406. [Google Scholar] [CrossRef]
- Kandala, B.; Fancourt, C.; Ananthula, H.; Cao, Y.; Vaddady, P.; Asante-Appiah, E.; Diamond, T.; Rhee, E.; Matthews, R.P.; Ankrom, W.; et al. Model-Informed Dose Selection for Islatravir/MK-8507 Oral Once-Weekly Phase 2B Study. In Proceedings of the Conferences on Retroviruses and Opportunistic Infections (CROI), Virtual, 6–10 March 2021. [Google Scholar]
- Patel, M.; Zang, X.; Cao, Y.; Matthews, R.P.; Plank, R.; Sklar, P.; Grobler, J.; Robertson, M.; Vargo, R. Islatravir PK Threshold & Dose Selection for Monthly Oral HIV-1 PrEP. In Proceedings of the Conference on Retroviruses and Opportunistic Infections (CROI), Virtual, 6–10 March 2021. [Google Scholar]
- Homayun, B.; Lin, X.; Choi, H.J. Challenges and Recent Progress in Oral Drug Delivery Systems for Biopharmaceuticals. Pharmaceutics 2019, 11, 129. [Google Scholar] [CrossRef] [Green Version]
- Tibaijuka, L.; Odongo, R.; Welikhe, E.; Mukisa, W.; Kugonza, L.; Busingye, I.; Nabukalu, P.; Ngonzi, J.; Asiimwe, S.B.; Bajunirwe, F. Factors influencing use of long-acting versus short-acting contraceptive methods among reproductive-age women in a resource-limited setting. BMC Women’s Health 2017, 17, 25. [Google Scholar] [CrossRef]
- Barrett, S.E.; Teller, R.S.; Forster, S.P.; Li, L.; Mackey, M.A.; Skomski, D.; Yang, Z.; Fillgrove, K.L.; Doto, G.J.; Wood, S.L.; et al. Extended-Duration MK-8591-Eluting Implant as a Candidate for HIV Treatment and Prevention. Antimicrob. Agents Chemother. 2018, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovarova, M.; Benhabbour, S.R.; Massud, I.; Spagnuolo, R.A.; Skinner, B.; Baker, C.E.; Sykes, C.; Mollan, K.R.; Kashuba, A.D.M.; Garcia-Lerma, J.G.; et al. Ultra-long-acting removable drug delivery system for HIV treatment and prevention. Nat. Commun. 2018, 9, 4156. [Google Scholar] [CrossRef] [Green Version]
- Ferretti, F.; Boffito, M. Rilpivirine long-acting for the prevention and treatment of HIV infection. Curr. Opin. HIV AIDS 2018, 13, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.; McGowan, I. Long-acting rilpivirine for HIV prevention. Curr. Opin. HIV AIDS 2015, 10, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Gunawardana, M.; Remedios-Chan, M.; Miller, C.S.; Fanter, R.; Yang, F.; Marzinke, M.A.; Hendrix, C.W.; Beliveau, M.; Moss, J.A.; Smith, T.J.; et al. Pharmacokinetics of long-acting tenofovir alafenamide (GS-7340) subdermal implant for HIV prophylaxis. Antimicrob. Agents Chemother. 2015, 59, 3913–3919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, R.P.; Zang, X.; Barrett, S.; Goodey, A.; Heimbach, T.; Weissler, V.; Leyssens, C.; Reynders, T.; Vargo, R.; Liu, Y.; et al. Next-generation Islatravir Implants Projected to Provide Yearly HIV Prophylaxis. In Proceedings of the Conference on Retroviruses and Opportunistic Infections (CROI), Virtual, 8–11 March 2021. [Google Scholar]
- Grobler, J. Current status of the Merck LA/ER Pipline: Update on Islatravir (ISL, MK-8591). In Proceedings of the Long-acting/Extended Release Antiretroviral Resource Program (LEAP), Boston, MA, USA, 7 March 2020. [Google Scholar]
- Li, L.; Krovi, S.; Norton, C.; Luecke, E.; Demkovich, Z.; Johnson, P.; Areson, C.; Jimenez, G.; van der Straten, A.; Johnson, L. Biodegradable Implant for Sustained Delivery of Antiretroviral (ARV) and Hormonal Contraceptive. In Proceedings of the Conference on Retroviruses and Opportunistic Infections (CROI), Boston, MA, USA, 8–11 March 2020. [Google Scholar]
- Li, L.; Krovi, A.; Norton, C.; Johnson, P.; Jimenez, G.; Areson, C.; Van der Straten, A.; Johnson, L. Long-acting Co-formulated biodegradable implant for HIV Prevention and Contraception. In Proceedings of the Conference of Retroviruses and Opportunistic Infections (CROI), Virtual, 6–10 March 2021. [Google Scholar]
- Johnson, L.; Li, A.; Krovi, S.; Luecke, E.; Demokovich, Z.; Johnson, P.; Shapely-Quinn, M.; van der Straten, A. Biodegradable Implants for HIV Prevention and Contraception. In Proceedings of the Long-Acting/Extended Release Antiretrovial Resource Program (LEAP), Boston, MA, USA, 7 March 2020. [Google Scholar]
- Johnson, L.M.; Krovi, S.A.; Li, L.; Girouard, N.; Demkovich, Z.R.; Myers, D.; Creelman, B.; van der Straten, A. Characterization of a Reservoir-Style Implant for Sustained Release of Tenofovir Alafenamide (TAF) for HIV Pre-Exposure Prophylaxis (PrEP). Pharmaceutics 2019, 11, 315. [Google Scholar] [CrossRef] [Green Version]
- Rein-Weston, A.; Tekko, I.; Vora, L.; Jarrahian, C.; Spreen, B.; Scott, T.; Donnelly, R.; Zehrung, D. Microarray Patch Delivery of Long-Acting HIV PrEP and Contraception. In Proceedings of the IDWeek, Washington, DC, USA, 2–6 October 2019. [Google Scholar]
- Rein-Weston, A.; Kilbourne-Brook, M.; Creelman, B.; Saxon, G.; Frivold, C.; Delarosa, J.; Moyo, Y.; Mukabi, J.; Kariithi, E.; Katuntu, D.; et al. Microarray Patches (MAPs) for Delivery of Long-acting HIV PrEP and Contraception. In Proceedings of the HIV Research for Prevention (HIVR4P), Madrid, Spain, 21–25 October 2018. [Google Scholar]
- Ripolin, A.; Quinn, J.; Larraneta, E.; Vicente-Perez, E.M.; Barry, J.; Donnelly, R.F. Successful application of large microneedle patches by human volunteers. Int. J. Pharm. 2017, 521, 92–101. [Google Scholar] [CrossRef] [Green Version]
- Mc Crudden, M.T.C.; Larraneta, E.; Clark, A.; Jarrahian, C.; Rein-Weston, A.; Lachau-Durand, S.; Niemeijer, N.; Williams, P.; Haeck, C.; McCarthy, H.O.; et al. Design, formulation and evaluation of novel dissolving microarray patches containing a long-acting rilpivirine nanosuspension. J. Control. Release 2018, 292, 119–129. [Google Scholar] [CrossRef]
- Musmade, N.; Jadhav, A.; Moin, P.; Suvarna, P.; Gupta, A. An Overview of In Situ Gel Forming Implants: Current Approaches towards Alternative Drug Delivery Systems. J. Biol. Chem. Chron. 2019, 5, 14–21. [Google Scholar] [CrossRef]
- Kempe, S.; Mader, K. In situ forming implants-an attractive formulation principle for parenteral depot formulations. J. Control. Release 2012, 161, 668–679. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, P.; Rupenthal, I.D. Injectable implants for the sustained release of protein and peptide drugs. Drug Discov. Today 2013, 18, 337–349. [Google Scholar] [CrossRef]
- Solorio, L.; Olear, A.M.; Zhou, H.; Beiswenger, A.C.; Exner, A.A. Effect of cargo properties on in situ forming implant behavior determined by noninvasive ultrasound imaging. Drug Deliv. Transl. Res. 2012, 2, 45–55. [Google Scholar] [CrossRef] [Green Version]
- Southard, G.L.; Dunn, R.L.; Garrett, S. The drug delivery and biomaterial attributes of the ATRIGEL technology in the treatment of periodontal disease. Expert Opin. Investig. Drugs 1998, 7, 1483–1491. [Google Scholar] [CrossRef] [PubMed]
- Benhabbour, S.R.; Kovarova, M.; Jones, C.; Copeland, D.J.; Shrivastava, R.; Swanson, M.D.; Sykes, C.; Ho, P.T.; Cottrell, M.L.; Sridharan, A.; et al. Ultra-long-acting tunable biodegradable and removable controlled release implants for drug delivery. Nat. Commun. 2019, 10, 4324. [Google Scholar] [CrossRef] [PubMed]
- PDE for N-methylpyrrolidone (NMP). Available online: https://www.fda.gov/media/78985/download#:~:text=The%20EWG%20received%20new%20toxicity,by%20the%20NMP%20Producers%20Group.&text=The%20consensus%20was%20to%20remove,PDE%20of%20207%20mg%2Fday (accessed on 31 May 2021).
- Patel, R.B.; Solorio, L.; Wu, H.; Krupka, T.; Exner, A.A. Effect of injection site on in situ implant formation and drug release in vivo. J. Control. Release 2010, 147, 350–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parent, M.; Nouvel, C.; Koerber, M.; Sapin, A.; Maincent, P.; Boudier, A. PLGA in situ implants formed by phase inversion: Critical physicochemical parameters to modulate drug release. J. Control. Release 2013, 172, 292–304. [Google Scholar] [CrossRef] [PubMed]
- Trezza, C.; Ford, S.L.; Spreen, W.; Pan, R.; Piscitelli, S. Formulation and pharmacology of long-acting cabotegravir. Curr. Opin. HIV AIDS 2015, 10, 239–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malcolm, R.K.; Boyd, P.; McCoy, C.F.; Murphy, D.J. Beyond HIV microbicides: Multipurpose prevention technology products. BJOG 2014, 121 (Suppl. 5), 62–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acarturk, F. Mucoadhesive vaginal drug delivery systems. Recent Pat. Drug Deliv. Formul. 2009, 3, 193–205. [Google Scholar] [CrossRef]
- D’Cruz, O.J.; Uckun, F.M. Vaginal microbicides and their delivery platforms. Expert Opin. Drug Deliv. 2014, 11, 723–740. [Google Scholar] [CrossRef] [PubMed]
- Marrazzo, J.M.; Rabe, L.; Kelly, C.; Richardson, B.; Deal, C.; Schwartz, J.L.; Chirenje, Z.M.; Piper, J.; Morrow, R.A.; Hendrix, C.W.; et al. Tenofovir Gel for Prevention of Herpes Simplex Virus Type 2 Acquisition: Findings From the VOICE Trial. J. Infect. Dis. 2019, 219, 1940–1947. [Google Scholar] [CrossRef] [PubMed]
- Abdool Karim, S.S.; Abdool Karim, Q.; Kharsany, A.B.; Baxter, C.; Grobler, A.C.; Werner, L.; Kashuba, A.; Mansoor, L.E.; Samsunder, N.; Mindel, A.; et al. Tenofovir Gel for the Prevention of Herpes Simplex Virus Type 2 Infection. N. Engl. J. Med. 2015, 373, 530–539. [Google Scholar] [CrossRef]
- McConville, C.; Major, I.; Devlin, B.; Brimer, A. Development of a multi-layered vaginal tablet containing dapivirine, levonorgestrel and acyclovir for use as a multipurpose prevention technology. Eur. J. Pharm. Biopharm. 2016, 104, 171–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Regev, G.; Patel, S.K.; Patton, D.; Sweeney, Y.; Graebing, P.; Grab, S.; Wang, L.; Sant, V.; Rohan, L.C. Rational Design of a Multipurpose Bioadhesive Vaginal Film for Co-Delivery of Dapivirine and Levonorgestrel. Pharmaceutics 2019, 12, 1. [Google Scholar] [CrossRef] [Green Version]
- Bunge, K.E.; Dezzutti, C.S.; Rohan, L.C.; Hendrix, C.W.; Marzinke, M.A.; Richardson-Harman, N.; Moncla, B.J.; Devlin, B.; Meyn, L.A.; Spiegel, H.M.; et al. A Phase 1 Trial to Assess the Safety, Acceptability, Pharmacokinetics, and Pharmacodynamics of a Novel Dapivirine Vaginal Film. J. Acquir. Immune Defic. Syndr. 2016, 71, 498–505. [Google Scholar] [CrossRef] [Green Version]
- Hombach, J.; Palmberger, T.F.; Bernkop-Schnurch, A. Development and in vitro evaluation of a mucoadhesive vaginal delivery system for nystatin. J. Pharm. Sci. 2009, 98, 555–564. [Google Scholar] [CrossRef] [PubMed]
- Baloglu, E.; Ay Senyigit, Z.; Karavana, S.Y.; Vetter, A.; Metin, D.Y.; Hilmioglu Polat, S.; Guneri, T.; Bernkop-Schnurch, A. In vitro evaluation of mucoadhesive vaginal tablets of antifungal drugs prepared with thiolated polymer and development of a new dissolution technique for vaginal formulations. Chem. Pharm. Bull. 2011, 59, 952–958. [Google Scholar] [CrossRef] [Green Version]
- Hornof, M.; Weyenberg, W.; Ludwig, A.; Bernkop-Schnurch, A. Mucoadhesive ocular insert based on thiolated poly(acrylic acid): Development and in vivo evaluation in humans. J. Control. Release 2003, 89, 419–428. [Google Scholar] [CrossRef]
- Weitzel, M.; North, B.B.; Waller, D. Development of multipurpose technologies products for pregnancy and STI prevention: Update on polyphenylene carboxymethylene MPT gel developmentdagger. Biol. Reprod. 2020, 103, 299–309. [Google Scholar] [CrossRef]
- Cheshenko, N.; Keller, M.J.; MasCasullo, V.; Jarvis, G.A.; Cheng, H.; John, M.; Li, J.H.; Hogarty, K.; Anderson, R.A.; Waller, D.P.; et al. Candidate topical microbicides bind herpes simplex virus glycoprotein B and prevent viral entry and cell-to-cell spread. Antimicrob. Agents Chemother. 2004, 48, 2025–2036. [Google Scholar] [CrossRef] [Green Version]
- Herold, B.C.; Scordi-Bello, I.; Cheshenko, N.; Marcellino, D.; Dzuzelewski, M.; Francois, F.; Morin, R.; Casullo, V.M.; Anderson, R.A.; Chany, C., 2nd; et al. Mandelic acid condensation polymer: Novel candidate microbicide for prevention of human immunodeficiency virus and herpes simplex virus entry. J. Virol. 2002, 76, 11236–11244. [Google Scholar] [CrossRef] [Green Version]
- Zaneveld, L.J.; Anderson, R.A.; Diao, X.H.; Waller, D.P.; Chany, C.; Feathergill, K.; Doncel, G.; Cooper, M.D.; Herold, B. Use of mandelic acid condensation polymer (SAMMA), a new antimicrobial contraceptive agent, for vaginal prophylaxis. Fertil. Steril. 2002, 78, 1107–1115. [Google Scholar] [CrossRef]
- Mesquita, P.M.; Cheshenko, N.; Wilson, S.S.; Mhatre, M.; Guzman, E.; Fakioglu, E.; Keller, M.J.; Herold, B.C. Disruption of tight junctions by cellulose sulfate facilitates HIV infection: Model of microbicide safety. J. Infect. Dis. 2009, 200, 599–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ball, C.; Krogstad, E.; Chaowanachan, T.; Woodrow, K.A. Drug-eluting fibers for HIV-1 inhibition and contraception. PLoS ONE 2012, 7, e49792. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.J.; Politch, J.A.; Cone, R.A.; Zeitlin, L.; Lai, S.K.; Santangelo, P.J.; Moench, T.R.; Whaley, K.J. Engineering monoclonal antibody-based contraception and multipurpose prevention technologiesdagger. Biol. Reprod. 2020, 103, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Kiser, P.F.; Johnson, T.J.; Clark, J.T. State of the art in intravaginal ring technology for topical prophylaxis of HIV infection. AIDS Rev. 2012, 14, 62–77. [Google Scholar] [PubMed]
- Morrow Guthrie, K.; Vargas, S.; Shaw, J.G.; Rosen, R.K.; van den Berg, J.J.; Kiser, P.F.; Buckheit, K.; Bregman, D.; Thompson, L.; Jensen, K.; et al. The Promise of Intravaginal Rings for Prevention: User Perceptions of Biomechanical Properties and Implications for Prevention Product Development. PLoS ONE 2015, 10, e0145642. [Google Scholar] [CrossRef] [PubMed]
- Malcolm, R.K.; Edwards, K.L.; Kiser, P.; Romano, J.; Smith, T.J. Advances in microbicide vaginal rings. Antivir. Res. 2010, 88 (Suppl. 1), S30–S39. [Google Scholar] [CrossRef]
- Friend, D.R. Intravaginal rings: Controlled release systems for contraception and prevention of transmission of sexually transmitted infections. Drug Deliv. Transl. Res. 2011, 1, 185–193. [Google Scholar] [CrossRef]
- Malcolm, R.K.; Woolfson, A.D.; Toner, C.F.; Morrow, R.J.; McCullagh, S.D. Long-term, controlled release of the HIV microbicide TMC120 from silicone elastomer vaginal rings. J. Antimicrob. Chemother. 2005, 56, 954–956. [Google Scholar] [CrossRef] [Green Version]
- Romano, J.; Variano, B.; Coplan, P.; Van Roey, J.; Douville, K.; Rosenberg, Z.; Temmerman, M.; Verstraelen, H.; Van Bortel, L.; Weyers, S.; et al. Safety and availability of dapivirine (TMC120) delivered from an intravaginal ring. AIDS Res. Hum. Retrovir. 2009, 25, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.M.; Pearce, S.M.; Poursaid, A.E.; Aliyar, H.A.; Tresco, P.A.; Mitchnik, M.A.; Kiser, P.F. Polyurethane intravaginal ring for controlled delivery of dapivirine, a nonnucleoside reverse transcriptase inhibitor of HIV-1. J. Pharm. Sci. 2008, 97, 4228–4239. [Google Scholar] [CrossRef] [PubMed]
- Woolfson, A.D.; Malcolm, R.K.; Morrow, R.J.; Toner, C.F.; McCullagh, S.D. Intravaginal ring delivery of the reverse transcriptase inhibitor TMC 120 as an HIV microbicide. Int. J. Pharm. 2006, 325, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Malcolm, K.; Woolfson, D.; Russell, J.; Andrews, C. In vitro release of nonoxynol-9 from silicone matrix intravaginal rings. J. Control. Release 2003, 91, 355–364. [Google Scholar] [CrossRef]
- Dahiya, P.; Dalal, M.; Yadav, A.; Dahiya, K.; Jain, S.; Silan, V. Efficacy of combined hormonal vaginal ring in comparison to combined hormonal pills in heavy menstrual bleeding. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 203, 147–151. [Google Scholar] [CrossRef]
- Mulders, T.M.; Dieben, T.O. Use of the novel combined contraceptive vaginal ring NuvaRing for ovulation inhibition. Fertil. Steril. 2001, 75, 865–870. [Google Scholar] [CrossRef]
- Phelps, R. Choosing a Birth Control Method; Association of Reproductive Health Professionals: Washington, DC, USA, 2011. [Google Scholar]
- NuvaRing (Etonogestrel/Ethinyl Estradiol Vaginal Ring). Available online: https://www.nuvaring.com/ (accessed on 31 May 2021).
- Baeten, J.M.; Palanee-Phillips, T.; Brown, E.R.; Schwartz, K.; Soto-Torres, L.E.; Govender, V.; Mgodi, N.M.; Matovu Kiweewa, F.; Nair, G.; Mhlanga, F.; et al. Use of a Vaginal Ring Containing Dapivirine for HIV-1 Prevention in Women. N. Engl. J. Med. 2016, 375, 2121–2132. [Google Scholar] [CrossRef] [PubMed]
- Murphy, D.J.; Desjardins, D.; Boyd, P.; Dereuddre-Bosquet, N.; Stimmer, L.; Caldwell, A.; Le Grand, R.; Kelly, C.; van Roey, J.; Malcolm, R.K. Impact of ring size and drug loading on the pharmacokinetics of a combination dapivirine-darunavir vaginal ring in cynomolgus macaques. Int. J. Pharm. 2018, 550, 300–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, T.J.; Gupta, K.M.; Fabian, J.; Albright, T.H.; Kiser, P.F. Segmented polyurethane intravaginal rings for the sustained combined delivery of antiretroviral agents dapivirine and tenofovir. Eur. J. Pharm. Sci. 2010, 39, 203–212. [Google Scholar] [CrossRef]
- Morrow, R.J.; Woolfson, A.D.; Donnelly, L.; Curran, R.; Andrews, G.; Katinger, D.; Malcolm, R.K. Sustained release of proteins from a modified vaginal ring device. Eur. J. Pharm. Biopharm. 2011, 77, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Moss, J.; Smith, J.; Malone, A. In vitro and in vivo release of tenofovir from silicone intravaginal rings. In Proceedings of the Microbicides 2010: Building Bridges in HIV Prevention, Pittsburgh, PA, USA, 22–25 May 2010. [Google Scholar]
- Baum, M.M.; Butkyavichene, I.; Gilman, J.; Kennedy, S.; Kopin, E.; Malone, A.M.; Nguyen, C.; Smith, T.J.; Friend, D.R.; Clark, M.R.; et al. An intravaginal ring for the simultaneous delivery of multiple drugs. J. Pharm. Sci. 2012, 101, 2833–2843. [Google Scholar] [CrossRef] [Green Version]
- Moss, J.A.; Malone, A.M.; Smith, T.J.; Kennedy, S.; Kopin, E.; Nguyen, C.; Gilman, J.; Butkyavichene, I.; Vincent, K.L.; Motamedi, M.; et al. Simultaneous delivery of tenofovir and acyclovir via an intravaginal ring. Antimicrob. Agents Chemother. 2012, 56, 875–882. [Google Scholar] [CrossRef] [Green Version]
- Moss, J.A.; Malone, A.M.; Smith, T.J.; Kennedy, S.; Nguyen, C.; Vincent, K.L.; Motamedi, M.; Baum, M.M. Pharmacokinetics of a multipurpose pod-intravaginal ring simultaneously delivering five drugs in an ovine model. Antimicrob. Agents Chemother. 2013, 57, 3994–3997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moss, J.A.; Srinivasan, P.; Smith, T.J.; Butkyavichene, I.; Lopez, G.; Brooks, A.A.; Martin, A.; Dinh, C.T.; Smith, J.M.; Baum, M.M. Pharmacokinetics and preliminary safety study of pod-intravaginal rings delivering antiretroviral combinations for HIV prophylaxis in a macaque model. Antimicrob. Agents Chemother. 2014, 58, 5125–5135. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.M.; Moss, J.A.; Srinivasan, P.; Butkyavichene, I.; Gunawardana, M.; Fanter, R.; Miller, C.S.; Sanchez, D.; Yang, F.; Ellis, S.; et al. Novel multipurpose pod-intravaginal ring for the prevention of HIV, HSV, and unintended pregnancy: Pharmacokinetic evaluation in a macaque model. PLoS ONE 2017, 12, e0185946. [Google Scholar] [CrossRef] [Green Version]
- Fu, J.; Yu, X.; Jin, Y. 3D printing of vaginal rings with personalized shapes for controlled release of progesterone. Int. J. Pharm. 2018, 539, 75–82. [Google Scholar] [CrossRef]
- Welsh, N.R.; Malcolm, R.K.; Devlin, B.; Boyd, P. Dapivirine-releasing vaginal rings produced by plastic freeforming additive manufacturing. Int. J. Pharm. 2019, 572, 118725. [Google Scholar] [CrossRef] [PubMed]
- Janusziewicz, R.; Mecham, S.J.; Olson, K.R.; Benhabbour, S.R. Design and Characterization of a Novel Series of Geometrically Complex Intravaginal Rings with Digital Light Synthesis. Adv. Mater. Technol. 2020, 5, 2000261. [Google Scholar] [CrossRef]
- Tumbleston, J.R.; Shirvanyants, D.; Ermoshkin, N.; Janusziewicz, R.; Johnson, A.R.; Kelly, D.; Chen, K.; Pinschmidt, R.; Rolland, J.P.; Ermoshkin, A.; et al. Additive manufacturing. Continuous liquid interface production of 3D objects. Science 2015, 347, 1349–1352. [Google Scholar] [CrossRef]
- Bloomquist, C.J.; Mecham, M.B.; Paradzinsky, M.D.; Janusziewicz, R.; Warner, S.B.; Luft, J.C.; Mecham, S.J.; Wang, A.Z.; DeSimone, J.M. Controlling release from 3D printed medical devices using CLIP and drug-loaded liquid resins. J. Control. Release 2018, 278, 9–23. [Google Scholar] [CrossRef]
- Weinrib, R.; Minnis, A.; Agot, K.; Ahmed, K.; Owino, F.; Manenzhe, K.; Cheng, H.; van der Straten, A. End-Users’ Product Preference Across Three Multipurpose Prevention Technology Delivery Forms: Baseline Results from Young Women in Kenya and South Africa. AIDS Behav. 2018, 22, 133–145. [Google Scholar] [CrossRef] [Green Version]
- Minnis, A.M.; Roberts, S.T.; Agot, K.; Weinrib, R.; Ahmed, K.; Manenzhe, K.; Owino, F.; van der Straten, A.; Team, T.S. Young Women’s Ratings of Three Placebo Multipurpose Prevention Technologies for HIV and Pregnancy Prevention in a Randomized, Cross-Over Study in Kenya and South Africa. AIDS Behav. 2018, 22, 2662–2673. [Google Scholar] [CrossRef]
- Minnis, A.M.; Montgomery, E.T.; Napierala, S.; Browne, E.N.; van der Straten, A. Insights for Implementation Science from 2 Multiphased Studies With End-Users of Potential Multipurpose Prevention Technology and HIV Prevention Products. J. Acquir. Immune Defic. Syndr. 2019, 82 (Suppl. 3), S222–S229. [Google Scholar] [CrossRef] [PubMed]
- Mensch, B.S.; van der Straten, A.; Katzen, L.L. Acceptability in microbicide and PrEP trials: Current status and a reconceptualization. Curr. Opin. HIV AIDS 2012, 7, 534–541. [Google Scholar] [CrossRef] [Green Version]
- van der Straten, A.; Agot, K.; Ahmed, K.; Weinrib, R.; Browne, E.N.; Manenzhe, K.; Owino, F.; Schwartz, J.; Minnis, A.; TRIO Study Team. The Tablets, Ring, Injections as Options (TRIO) study: What young African women chose and used for future HIV and pregnancy prevention. J. Int. AIDS Soc. 2018, 21, e25094. [Google Scholar] [CrossRef] [PubMed]
- Luecke, E.H.; Cheng, H.; Woeber, K.; Nakyanzi, T.; Mudekunye-Mahaka, I.C.; van der Straten, A.; MTN-003D Study Team. Stated product formulation preferences for HIV pre-exposure prophylaxis among women in the VOICE-D (MTN-003D) study. J. Int. AIDS Soc. 2016, 19, 20875. [Google Scholar] [CrossRef]
- Quaife, M.; Terris-Prestholt, F.; Eakle, R.; Cabrera Escobar, M.A.; Kilbourne-Brook, M.; Mvundura, M.; Meyer-Rath, G.; Delany-Moretlwe, S.; Vickerman, P. The cost-effectiveness of multi-purpose HIV and pregnancy prevention technologies in South Africa. J. Int. AIDS Soc. 2018, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiebe, E.; Kaczorowski, J.; Mackay, J. Mood and sexual side effects of hormonal contraception: Physicians’ and residents’ knowledge, attitudes, and practices. Can. Fam. Physician 2012, 58, e677–e683. [Google Scholar] [PubMed]
- Smith, J.S.; Green, J.; Berrington de Gonzalez, A.; Appleby, P.; Peto, J.; Plummer, M.; Franceschi, S.; Beral, V. Cervical cancer and use of hormonal contraceptives: A systematic review. Lancet 2003, 361, 1159–1167. [Google Scholar] [CrossRef]
- Hemmerling, A.; Christopher, E.; Young Holt, B. Towards a roadmap to advance non-hormonal contraceptive multipurpose prevention technologies: Strategic insights from key stakeholdersdagger. Biol. Reprod. 2020, 103, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Scarsi, K.K.; Darin, K.M.; Nakalema, S.; Back, D.J.; Byakika-Kibwika, P.; Else, L.J.; Dilly Penchala, S.; Buzibye, A.; Cohn, S.E.; Merry, C.; et al. Unintended Pregnancies Observed With Combined Use of the Levonorgestrel Contraceptive Implant and Efavirenz-based Antiretroviral Therapy: A Three-Arm Pharmacokinetic Evaluation Over 48 Weeks. Clin. Infect. Dis. 2016, 62, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Vieira, C.S.; Bahamondes, M.V.; de Souza, R.M.; Brito, M.B.; Rocha Prandini, T.R.; Amaral, E.; Bahamondes, L.; Duarte, G.; Quintana, S.M.; Scaranari, C.; et al. Effect of antiretroviral therapy including lopinavir/ritonavir or efavirenz on etonogestrel-releasing implant pharmacokinetics in HIV-positive women. J. Acquir. Immune Defic. Syndr. 2014, 66, 378–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarsi, K.K.; Cramer, Y.; Gingrich, D.; Rosekranz, S.; Aweeka, F.; Coombs, R.; Zorrilla, C.; Coughlin, K.; Moran, L.; Berzins, B.; et al. Vaginal Contraceptive Hormone Exposure Profoundly Altered by EFV- and ATV/R-Based ART. In Proceedings of the Conference on Retroviruses and Opportunisitc Infections (CROI), Boston, MA, USA, 4–7 March 2018. [Google Scholar]
- Tietz, K.; Klein, S. In Vitro Methods for Evaluating Drug Release of Vaginal Ring Formulations—A Critical Review. Pharmaceutics 2019, 11, 538. [Google Scholar] [CrossRef] [Green Version]
- Young Holt, B.; Kiarie, J.; Kopf, G.S.; Nanda, K.; Hemmerling, A.; Achilles, S.L. Bridging the gap: Advancing multipurpose prevention technologies from the lab into the hands of womendagger. Biol. Reprod. 2020, 103, 286–288. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product Name/Developer | Indication | Delivery Platform | Development Stage | Active Pharmaceutical Ingredients | Duration of Action | Reference |
|---|---|---|---|---|---|---|
| International Partnership for Microbicides (originally developed by Karl Malcolm at Belfast University) | HIV, Pregnancy | Intravaginal ring | Clinical—Phase 1 | Dapivirine, levonorgestrel | 90 days | [34] |
| Population Council | HIV, Pregnancy | Oral capsule | Clinical—Phase 3 | Tenofovir, emtricitabine, levonorgestrel, ethinyl estradiol | 24 h | [35] |
| HIV, HSV-2, HPV | Vaginal gel | Clinical—Phase 1 | carrageenan, MIV-150, zinc acetate | 24 h | [36,37] | |
| CONRAD Program (originally developed by Patrick Kiser at University of Utah and Northwestern) | HIV, Pregnancy | Intravaginal ring (Segmented) | Clinical—Phase 1 | levonorgestrel, tenofovir | 90 days | [38] |
| CONRAD Program | HIV, HSV-2 | Vaginal insert | Clinical—Phase 1 | tenofovir, elvitegravir | 4–72 h | [39,40,41] |
| HIV, HSV-2 | Vaginal gel | Clinical—Phase 3 | 1% tenofovir | 12 h | [42,43] | |
| MAPP Biopharmaceutical (originally developed by Deborah Anderson at Boston University) | HIV, HSV-2, Pregnancy | Vaginal film | Clinical—Phase 1 | MB66 (monoclonal antibody) | 24 h | [44,45] |
| Evofem Inc. | Chlamydia, Gonorrhea, Pregnancy | Vaginal gel | Clinical—Phase 2 | Amphora® gel (L-lactic acid, citric acid, Potassium bitartrate) | Pre-coital | [46,47] |
| StarPharma | HIV, HSV-2 | Vaginal gel | Clinical—Phase 1 | SPL7013- VivaGel™ | 24 h | [48,49] |
| Delivery Route | Formulations | Advantages | Limitations | Considerations |
|---|---|---|---|---|
| Oral | Tablets |
|
|
|
| Parenteral | Implants Injectables |
|
|
|
| Vaginal | Films Gels Tablets/Inserts |
|
|
|
| Intravaginal rings |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Young, I.C.; Benhabbour, S.R. Multipurpose Prevention Technologies: Oral, Parenteral, and Vaginal Dosage Forms for Prevention of HIV/STIs and Unplanned Pregnancy. Polymers 2021, 13, 2450. https://doi.org/10.3390/polym13152450
Young IC, Benhabbour SR. Multipurpose Prevention Technologies: Oral, Parenteral, and Vaginal Dosage Forms for Prevention of HIV/STIs and Unplanned Pregnancy. Polymers. 2021; 13(15):2450. https://doi.org/10.3390/polym13152450
Chicago/Turabian StyleYoung, Isabella C., and Soumya Rahima Benhabbour. 2021. "Multipurpose Prevention Technologies: Oral, Parenteral, and Vaginal Dosage Forms for Prevention of HIV/STIs and Unplanned Pregnancy" Polymers 13, no. 15: 2450. https://doi.org/10.3390/polym13152450