Promising Drug Delivery Approaches to Treat Microbial Infections in the Vagina: A Recent Update

 , , , , and
, , , , and
Abstract
:
1. Introduction
2. Type and Treatment of Vaginal Infections
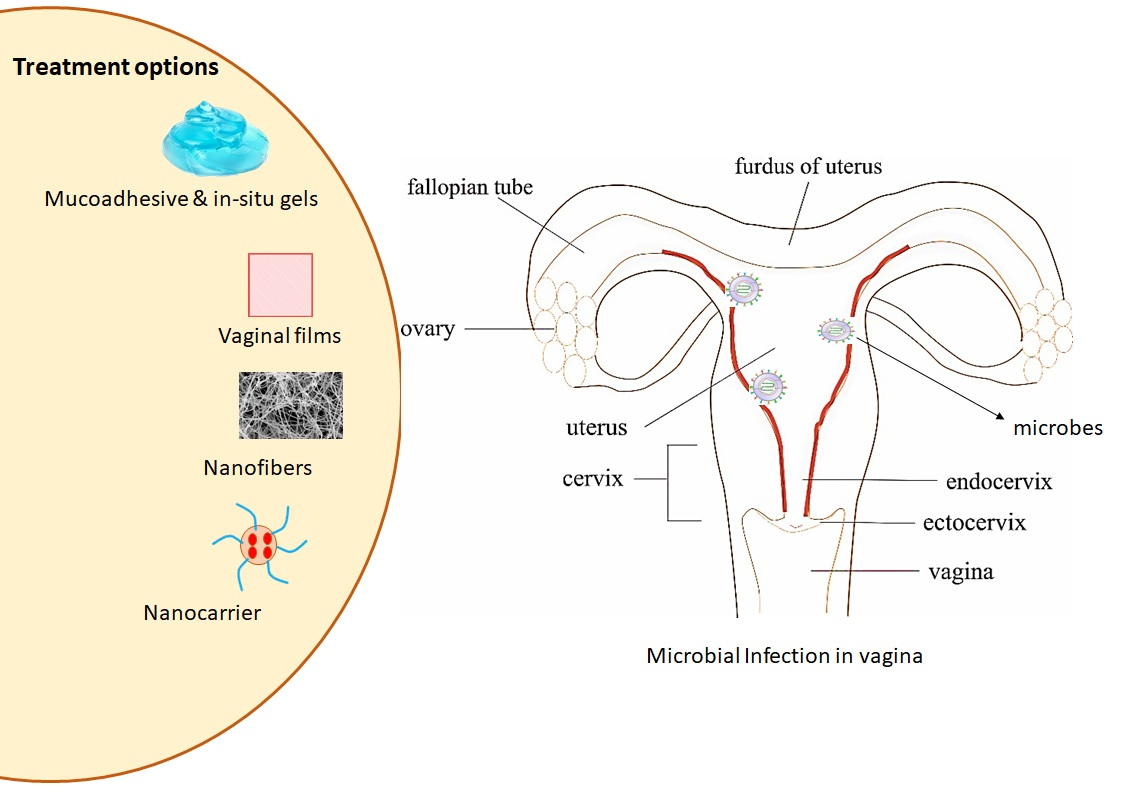
3. Novel Approaches for Vaginal Drug Delivery for Microbial Infections
3.1. Nanocarriers
3.2. Vaginal Gels with Nanocarriers
3.3. Vaginal Nanofibers
3.4. Vaginal Films
3.5. Mucoadhesive Polymeric Approaches
3.6. Stimuli-Responsive Approaches
3.6.1. Thermo-Responsive Systems
3.6.2. pH-Responsive Systems
3.6.3. Ion-Responsive Systems
3.6.4. Multi-Stimuli Responsive Systems
3.6.5. Other Responsive Systems
4. Progresses of Advanced Drug Delivery in Clinical Research
5. Expert Opinion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mulu, W.; Yimer, M.; Zenebe, Y.; Abera, B. Common causes of vaginal infections and antibiotic susceptibility of aerobic bacterial isolates in women of reproductive age attending at Felegehiwot referral Hospital, Ethiopia: A cross sectional study. BMC Womens Health 2015, 15, 42. [Google Scholar] [CrossRef] [Green Version]
- Balkus, J.E.; Srinivasan, S.; Anzala, O.; Kimani, J.; Andac, C.; Schwebke, J.; Fredricks, D.N.; McClelland, R.S. Impact of periodic presumptive treatment for bacterial vaginosis on the vaginal microbiome among women participating in the preventing vaginal infections trial. J. Infect. Dis. 2017, 215, 723–731. [Google Scholar] [CrossRef] [PubMed]
- Haahr, T.; Zacho, J.; Bräuner, M.; Shathmigha, K.; Skov Jensen, J.; Humaidan, P. Reproductive outcome of patients undergoing in vitro fertilisation treatment and diagnosed with bacterial vaginosis or abnormal vaginal microbiota: A systematic PRISMA review and meta-analysis. BJOG Int. J. Obstet. Gynaecol. 2019, 126, 200–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kairys, N.; Garg, M. Bacterial Vaginosis; StatPearls Publishing: Treasure Island, FL, USA, 2020; Available online: https://www.ncbi.nlm.nih.gov/books/NBK459216/ (accessed on 16 December 2020).
- Jain, J.P.; Bristow, C.C.; Pines, H.A.; Harvey-Vera, A.; Rangel, G.; Staines, H.; Patterson, T.L.; Strathdee, S.A. Factors in the HIV risk environment associated with bacterial vaginosis among HIV-negative female sex workers who inject drugs in the Mexico-United States border region. BMC Public Health 2018, 18, 1032–1042. [Google Scholar] [CrossRef] [PubMed]
- Eastment, M.C.; McClelland, R.S. Vaginal microbiota and susceptibility to HIV. AIDS 2018, 32, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Ranjit, E.; Raghubanshi, B.R.; Maskey, S.; Parajuli, P. Prevalence of bacterial vaginosis and its association with risk factors among nonpregnant women: A hospital based study. Int. J. Microbiol. 2018, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Palmeira-de-Oliveira, R.; Palmeira-de-Oliveira, A.; Martinez-de-Oliveira, J. New strategies for local treatment of vaginal infections. Adv. Drug Deliv. Rev. 2015, 92, 105–122. [Google Scholar] [CrossRef]
- Cook, M.T.; Brown, M.B. Polymeric gels for intravaginal drug delivery. J. Control. Release 2018, 270, 145–157. [Google Scholar] [CrossRef] [Green Version]
- Graziottin, A.; Gambini, D. Anatomy and Physiology of Genital Organs-Women, 1st ed.; Elsevier B.V.: Amsterdam, The Netherlands, 2015; Volume 130, ISBN 9780444632470. [Google Scholar]
- Łaniewski, P.; Herbst-Kralovetz, M. Vagina. Encycl. Reprod. 2018, 2, 353–359. [Google Scholar]
- Leyva-Gómez, G.; Del Prado-Audelo, M.L.; Ortega-Peña, S.; Mendoza-Muñoz, N.; Urbán-Morlán, Z.; González-Torres, M.; González-Del Carmen, M.; Figueroa-González, G.; Reyes-Hernández, O.D.; Cortés, H. Modifications in vaginal microbiota and their influence on drug release: Challenges and opportunities. Pharmaceutics 2019, 11, 217. [Google Scholar] [CrossRef] [Green Version]
- Rossi, S.; Vigani, B.; Sandri, G.; Bonferoni, M.C.; Caramella, C.M.; Ferrari, F. Recent advances in the mucus-interacting approach for vaginal drug delivery: From mucoadhesive to mucus-penetrating nanoparticles. Expert Opin. Drug Deliv. 2019, 16, 777–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leyva-Gómez, G.; Piñón-Segundo, E.; Mendoza-Muñoz, N.; Zambrano-Zaragoza, M.L.; Mendoza-Elvira, S.; Quintanar-Guerrero, D. Approaches in polymeric nanoparticles for vaginal drug delivery: A review of the state of the art. Int. J. Mol. Sci. 2018, 19, 1549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iqbal, Z.; Dilnawaz, F. Nanocarriers for vaginal drug delivery. Recent Pat. Drug Deliv. Formul. 2019, 13, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.; Cerca, N.; Jespers, V.; Vaneechoutte, M.; Crucitti, T. Bacterial biofilms in the vagina. Res. Microbiol. 2017, 168, 865–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jian, H.J.; Yu, J.; Li, Y.J.; Unnikrishnan, B.; Huang, Y.F.; Luo, L.J.; Hui-Kang Ma, D.; Harroun, S.G.; Chang, H.T.; Lin, H.J.; et al. Highly adhesive carbon quantum dots from biogenic amines for prevention of biofilm formation. Chem. Eng. J. 2020, 386, 123913. [Google Scholar] [CrossRef]
- Hamid Akash, M.S.; Rehman, K.; Chen, S. Natural and synthetic polymers as drug carriers for delivery of therapeutic proteins. Polym. Rev. 2015, 55, 371–406. [Google Scholar] [CrossRef]
- Veiga, M.-D.; Ruiz-Caro, R.; Martín-Illana, A.; Notario-Pérez, F.; Cazorla-Luna, R. Polymer gels in vaginal drug delivery systems. In Polymer Gels. Gels Horizons: From Science to Smart Materials; Thakur, V., Thakur, M., Eds.; Springer: Singapore, 2018; ISBN 9789811060830. [Google Scholar]
- Lalan, M.S.; Patel, V.N.; Misra, A. Polymers in vaginal drug delivery: Recent advancements. In Applications of Polymers in Drug Delivery; Elsevier: New York, NY, USA, 2021; pp. 281–303. [Google Scholar]
- Gupta, S.; Kakkar, V.; Bhushan, I. Crosstalk between vaginal microbiome and female health: A review. Microb. Pathog. 2019, 136, 103696. [Google Scholar] [CrossRef]
- Vazquez, F.; Fernández-Blázquez, A.; García, B. Vaginosis. Vaginal microbiota. Enferm. Infecc. Y Microbiol. Clin. 2019, 37, 592–601. [Google Scholar] [CrossRef]
- Pramanick, R.; Mayadeo, N.; Warke, H.; Begum, S.; Aich, P.; Aranha, C. Vaginal microbiota of asymptomatic bacterial vaginosis and vulvovaginal candidiasis: Are they different from normal microbiota? Microb. Pathog. 2019, 134, 103599. [Google Scholar] [CrossRef]
- Peebles, K.; Velloza, J.; Balkus, J.E.; McClelland, R.S.; Barnabas, R.V. High global burden and costs of bacterial vaginosis: A systematic review and meta-analysis. Sex. Transm. Dis. 2019, 46, 304–311. [Google Scholar] [CrossRef]
- Bagnall, P.; Rizzolo, D. Bacterial vaginosis: A practical review. J. Am. Acad. Physician Assist. 2017, 30, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Jones, A. Bacterial vaginosis: A review of treatment, recurrence, and disparities. J. Nurse Pract. 2019, 15, 420–423. [Google Scholar] [CrossRef] [Green Version]
- National Antimicrobial Guideline 2019; Ministry of Health Malaysia, Pharmaceutical Services Programme: Selangor, Malaysia, 2019; ISBN 9789675570780.
- British National Formulary (BNF)-Clindamycin. MedicinesComplete. 2020. Available online: https://www-medicinescomplete-com.ezp2.imu.edu.my/#/content/bnf/_673685021?hspl=clindamycin (accessed on 12 July 2020).
- British National Formulary (BNF)-Metronidazole. MedicinesComplete. 2020. Available online: https://www-medicinescomplete-com.ezp2.imu.edu.my/#/content/bnf/_555910287?hspl=metronidazole (accessed on 12 July 2020).
- Workowski, K. Bacterial Vaginosis-2015 STD Treatment Guidelines. 2015. Available online: https://www.cdc.gov/std/tg2015/bv.htm (accessed on 14 July 2020).
- Gonçalves, B.; Ferreira, C.; Alves, C.T.; Henriques, M.; Azeredo, J.; Silva, S. Vulvovaginal candidiasis: Epidemiology, microbiology and risk factors. Crit. Rev. Microbiol. 2016, 42, 905–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willems, H.M.; Ahmed, S.S.; Liu, J.; Xu, Z.; Peters, B.M. Vulvovaginal candidiasis: A current understanding and burning questions. J. Fungi 2020, 6, 27. [Google Scholar] [CrossRef] [Green Version]
- Denning, D.W.; Kneale, M.; Sobel, J.D.; Rautemaa-Richardson, R. Global burden of recurrent vulvovaginal candidiasis: A systematic review. Lancet Infect. Dis. 2018, 18, e339–e347. [Google Scholar] [CrossRef]
- Chatzivasileiou, P.; Vyzantiadis, T.A. Vaginal yeast colonisation: From a potential harmless condition to clinical implications and management approaches—A literature review. Mycoses 2019, 62, 638–650. [Google Scholar] [CrossRef]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef]
- Vulvovaginal Candidiasis—2015 STD Treatment Guidelines. 2015. Available online: https://www.cdc.gov/std/tg2015/candidiasis.htm (accessed on 18 July 2020).
- Kissinger, P. Trichomonas vaginalis: A review of epidemiologic, clinical and treatment issues. BMC Infect. Dis. 2015, 15, 307. [Google Scholar] [CrossRef] [Green Version]
- Rowley, J.; Vander Hoorn, S.; Korenromp, E.; Low, N.; Unemo, M.; Abu-Raddad, L.J.; Chico, R.M.; Smolak, A.; Newman, L.; Gottlieb, S.; et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: Global prevalence and incidence estimates, 2016. Bull. World Health Organ. 2019, 97, 548–562P. [Google Scholar] [CrossRef]
- Van Gerwen, O.T.; Muzny, C.A. Recent advances in the epidemiology, diagnosis, and management of Trichomonas vaginalis infection. F1000Research 2019, 8, 1666. [Google Scholar] [CrossRef]
- Workowski, K.A.; Bolan, G.A. Sexually transmitted diseases treatment guidelines, 2015. Mmwr Recomm. Rep. 2015, 64, 137. [Google Scholar]
- Trichomoniasis—2015 STD Treatment Guidelines. 2015. Available online: https://www.cdc.gov/std/tg2015/trichomoniasis.htm (accessed on 18 July 2020).
- World Health Organisation. HIV/AIDS. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/hiv-aids (accessed on 28 June 2020).
- Deeks, S.G.; Overbaugh, J.; Phillips, A.; Buchbinder, S. HIV Infection. Nat. Rev. Dis. Prim. 2015, 1, 1–22. [Google Scholar] [CrossRef]
- Torcia, M.G. Interplay among vaginal microbiome, immune response and sexually transmitted viral infections. Int. J. Mol. Sci. 2019, 20, 266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohapatra, A.; Sahoo, D. Review on HIV AIDS. Int. J. Psychosoc. Rehabil. 2019, 23, 521–527. [Google Scholar]
- Dubé, M.P.; Sattler, F.R. Inflammation and complications of HIV disease. J. Infect. Dis. 2010, 201, 1783–1785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malaysian Consensus Guidelines on Antiretroviral Therapy 2017; Ministry of Health Malaysia: Putrajaya, Malaysia, 2017.
- Fitzmaurice, C.; Dicker, D.; Pain, A.; Hamavid, H.; Moradi-Lakeh, M.; MacIntyre, M.F.; Allen, C.; Hansen, G.; Woodbrook, R.; Wolfe, C.; et al. The global burden of cancer 2013. JAMA Oncol. 2015, 1, 505–527. [Google Scholar] [CrossRef]
- Yarbrough, V.L.; Winkle, S.; Herbst-Kralovetz, M.M. Antimicrobial peptides in the female reproductive tract: A critical component of the mucosal immune barrier with physiological and clinical implications. Hum. Reprod. Update 2015, 21, 353–377. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Human papillomavirus (HPV) and cervical cancer. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/human-papillomavirus-(hpv)-and-cervical-cancer (accessed on 14 July 2020).
- HPV and Cancer. National Cancer Institute. 2020. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-and-cancer (accessed on 14 July 2020).
- Lírio, J.; Giraldo, P.C.; Amaral, R.L.; Sarmento, A.C.; Costa, A.P.; Goncalves, A.K. Antifungal (oral and vaginal) therapy for recurrent vulvovaginal candidiasis: A systematic review protocol. BMJ Open 2019, 9, e027489. [Google Scholar] [CrossRef] [Green Version]
- Bradshaw, C.S.; Sobel, J.D. Current treatment of bacterial vaginosis-limitations and need for innovation. J. Infect. Dis. 2016, 214, S14–S20. [Google Scholar] [CrossRef] [Green Version]
- Younus, N.K.; Gopinath, R.; Jegasothy, R.; Nordin, S.A.; van Belkum, A.; Mary, N.; Neela, V.K. An update on gardneralla vaginalis associated bacterial vaginosis in Malaysia. Asian Pac. J. Trop. Biomed. 2017, 7, 831–835. [Google Scholar] [CrossRef]
- Almomen, A.; Cho, S.; Yang, C.-H.; Li, Z.; Jarboe, E.A.; Peterson, C.M.; Huh, K.M.; Janát-Amsbury, M.M. Thermosensitive progesterone hydrogel: A safe and effective new formulation for vaginal application. Pharm. Res. 2015, 32, 2266–2279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srikrishna, S.; Cardozo, L. The vagina as a route for drug delivery: A review. Int. Urogynecol. J. Pelvic Floor Dysfunct. 2013, 24, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Sobel, J.D. Bacterial vaginosis: Treatment. UpToDate. 2020. Available online: https://www.uptodate.com/contents/bacterial-vaginosis-treatment (accessed on 28 June 2020).
- Schuyler, J.A.; Mordechai, E.; Adelson, M.E.; Sobel, J.D.; Gygax, S.E.; Hilbert, D.W. Identification of intrinsically metronidazole-resistant clades of Gardnerella vaginalis. Diagn. Microbiol. Infect. Dis. 2016, 84, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Kim, M.S.; Hayat, F.; Shin, D. Recent advances in the discovery of novel antiprotozoal agents. Molecules 2019, 24, 3886. [Google Scholar] [CrossRef] [Green Version]
- Bhatti, A.B.; Usman, M.; Kandi, V. Current scenario of HIV/AIDS, treatment options, and major challenges with compliance to antiretroviral therapy. Cureus 2016, 8, e515. [Google Scholar] [CrossRef] [Green Version]
- Wong, T.W.; Dhanawat, M.; Rathbone, M.J. Vaginal drug delivery: Strategies and concerns in polymeric nanoparticle development. Expert Opin. Drug Deliv. 2014, 11, 1419–1434. [Google Scholar] [CrossRef]
- Johal, H.S.; Garg, T.; Rath, G.; Goyal, A.K. Advanced topical drug delivery system for the management of vaginal candidiasis. Drug Deliv. 2016, 23, 550–563. [Google Scholar] [CrossRef]
- das Neves, J.; Nunes, R.; Machado, A.; Sarmento, B. Polymer-based nanocarriers for vaginal drug delivery. Adv. Drug Deliv. Rev. 2015, 92, 53–70. [Google Scholar] [CrossRef] [Green Version]
- Mirza, M.A.; Panda, A.K.; Asif, S.; Verma, D.; Talegaonkar, S.; Manzoor, N.; Khan, A.; Ahmed, F.J.; Dudeja, M.; Iqbal, Z. A vaginal drug delivery model. Drug Deliv. 2016, 23, 3123–3134. [Google Scholar] [CrossRef]
- Luo, L.J.; Lin, T.Y.; Yao, C.H.; Kuo, P.Y.; Matsusaki, M.; Harroun, S.G.; Huang, C.C.; Lai, J.Y. Dual-functional gelatin-capped silver nanoparticles for antibacterial and antiangiogenic treatment of bacterial keratitis. J. Colloid Interface Sci. 2019, 536, 112–126. [Google Scholar] [CrossRef]
- Gorain, B.; Choudhury, H.; Pandey, M.; Kesharwani, P. Paclitaxel loaded vitamin E-TPGS nanoparticles for cancer therapy. Mater. Sci. Eng. C 2018, 91, 868–880. [Google Scholar] [CrossRef] [PubMed]
- Gorain, B.; Choudhury, H.; Nair, A.B.; Dubey, S.K.; Kesharwani, P. Theranostic application of nanoemulsion in chemotherapy. Drug Discov. Today 2020, 25, 1174–1188. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.L.; Li, Y.J.; Jian, H.J.; Harroun, S.G.; Wei, S.C.; Ravindranath, R.; Lai, J.Y.; Huang, C.C.; Chang, H.T. Green synthesis of catalytic gold/bismuth oxyiodide nanocomposites with oxygen vacancies for treatment of bacterial infections. Nanoscale 2018, 10, 11808–11819. [Google Scholar] [CrossRef]
- Jian, H.J.; Wu, R.S.; Lin, T.Y.; Li, Y.J.; Lin, H.J.; Harroun, S.G.; Lai, J.Y.; Huang, C.C. Super-Cationic carbon quantum dots synthesized from spermidine as an eye drop formulation for topical treatment of bacterial keratitis. ACS Nano 2017, 11, 6703–6716. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, H.; Maheshwari, R.; Pandey, M.; Tekade, M.; Gorain, B.; Tekade, R.K. Advanced nanoscale carrier-based approaches to overcome biopharmaceutical issues associated with anticancer drug ‘Etoposide’. Mater. Sci. Eng. C 2020, 106, 110275. [Google Scholar] [CrossRef] [PubMed]
- Vanić, Ž.; Rukavina, Z.; Manner, S.; Fallarero, A.; Uzelac, L.; Kralj, M.; Klarić, D.A.; Bogdanov, A.; Raffai, T.; Virok, D.P.; et al. Azithromycin-liposomes as a novel approach for localized therapy of cervicovaginal bacterial infections. Int. J. Nanomed. 2019, 14, 5957–5976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jøraholmen, M.W.; Basnet, P.; Acharya, G.; Škalko-Basnet, N. PEGylated liposomes for topical vaginal therapy improve delivery of interferon alpha. Eur. J. Pharm. Biopharm. 2017, 113, 132–139. [Google Scholar] [CrossRef] [Green Version]
- Jøraholmen, M.W.; Škalko-Basnet, N.; Acharya, G.; Basnet, P. Resveratrol-loaded liposomes for topical treatment of the vaginal inflammation and infections. Eur. J. Pharm. Sci. 2015, 79, 112–121. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Pérez, B.; Quintanar-Guerrero, D.; Tapia-Tapia, M.; Cisneros-Tamayo, R.; Zambrano-Zaragoza, M.L.; Alcalá-Alcalá, S.; Mendoza-Muñoz, N.; Piñón-Segundo, E. Controlled-release biodegradable nanoparticles: From preparation to vaginal applications. Eur. J. Pharm. Sci. 2018, 115, 185–195. [Google Scholar] [CrossRef]
- Amaral, A.C.; Saavedra, P.H.V.; Oliveira Souza, A.C.; de Melo, M.T.; Tedesco, A.C.; Morais, P.C.; Soares Felipe, M.S.; Bocca, A.L. Miconazole loaded chitosan-based nanoparticles for local treatment of vulvovaginal candidiasis fungal infections. Colloids Surf. B Biointerfaces 2019, 174, 409–415. [Google Scholar] [CrossRef]
- Bhattacharya, D.S.; Svechkarev, D.; Souchek, J.J.; Hill, T.K.; Taylor, M.A.; Natarajan, A.; Mohs, A.M. Impact of structurally modifying hyaluronic acid on CD44 interaction. J. Mater. Chem. B 2017, 5, 8183–8192. [Google Scholar] [CrossRef]
- Melo, C.M.; Cardoso, J.F.; Perassoli, F.B.; de Oliveira Neto, A.S.; Pinto, L.M.; de Freitas Marques, M.B.; da Nova Mussel, W.; Magalhães, J.T.; de Lima Moura, S.A.; de Freitas Araújo, M.G.; et al. Amphotericin b-loaded eudragit RL100 nanoparticles coated with hyaluronic acid for the treatment of vulvovaginal candidiasis. Carbohydr. Polym. 2020, 230, 115608. [Google Scholar] [CrossRef]
- Calvo, N.L.; Sreekumar, S.; Svetaz, L.A.; Lamas, M.C.; Moerschbacher, B.M.; Leonardi, D. Design and characterization of chitosan nanoformulations for the delivery of antifungal agents. Int. J. Mol. Sci. 2019, 20, 3686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdellatif, M.M.; Khalil, I.A.; Elakkad, Y.E.; Eliwa, H.A.; Samir, T.M.; Al-Mokaddem, A.K. Formulation and characterization of sertaconazole nitrate mucoadhesive liposomes for vaginal candidiasis. Int. J. Nanomed. 2020, 15, 4079–4090. [Google Scholar] [CrossRef] [PubMed]
- Tuğcu-Demiröz, F. Vaginal delivery of benzydamine hydrochloride through liposomes dispersed in mucoadhesive gels. Chem. Pharm. Bull. 2017, 65, 660–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenechukwu, F.C.; Attama, A.A.; Ibezim, E.C.; Nnamani, P.O.; Umeyor, C.E.; Uronnachi, E.M.; Gugu, T.H.; Momoh, M.A.; Ofokansi, K.C.; Akpa, P.A. Surface-modified mucoadhesive microgels as a controlled release system for miconazole nitrate to improve localized treatment of vulvovaginal candidiasis. Eur. J. Pharm. Sci. 2018, 111, 358–375. [Google Scholar] [CrossRef] [PubMed]
- Rençber, S.; Karavana, S.Y.; Şenyiğit, Z.A.; Eraç, B.; Limoncu, M.H.; Baloğlu, E. Mucoadhesive in situ gel formulation for vaginal delivery of clotrimazole: Formulation, preparation, and in vitro/in vivo evaluation. Pharm. Dev. Technol. 2017, 22, 551–561. [Google Scholar] [CrossRef]
- Osmari, B.F.; Giuliani, L.M.; Reolon, J.B.; Rigo, G.V.; Tasca, T.; Cruz, L. Gellan gum-based hydrogel containing nanocapsules for vaginal indole-3-carbinol delivery in trichomoniasis treatment. Eur. J. Pharm. Sci. 2020, 151, 928–987. [Google Scholar] [CrossRef]
- Khattab, A.; Ismail, S. Formulation and evaluation of oxiconazole nitrate mucoadhesive nanoemulsion based gel for treatment of fungal vaginal infection. Int. J. Pharm. Pharm. Sci. 2016, 8, 33–40. [Google Scholar]
- Jeckson, T.A.; Neo, Y.P.; Sisinthy, S.P.; Gorain, B. Delivery of therapeutics from layer-by-layer electrospun nanofiber matrix for wound healing: An update. J. Pharm. Sci. 2020, S0022-3549, 30588-8. [Google Scholar] [CrossRef]
- Tuğcu-Demiröz, F.; Saar, S.; Tort, S.; Acartürk, F. Electrospun metronidazole-loaded nanofibers for vaginal drug delivery. Drug Dev. Ind. Pharm. 2020, 46, 1015–1025. [Google Scholar] [CrossRef] [PubMed]
- Nematpour, N.; Moradipour, P.; Zangeneh, M.M.; Arkan, E.; Abdoli, M.; Behbood, L. The application of nanomaterial science in the formulation a novel antibiotic: Assessment of the antifungal properties of mucoadhesive clotrimazole loaded nanofiber versus vaginal films. Mater. Sci. Eng. C 2020, 110, 110635. [Google Scholar] [CrossRef] [PubMed]
- Souza, R.O.; Henrique de Lima, T.; Oréfice, R.L.; de Freitas Araújo, M.G.; de Lima Moura, S.A.; Magalhães, J.T.; da Silva, G.R. Amphotericin B-Loaded poly(lactic-co-glycolic acid) nanofibers: An alternative therapy scheme for local treatment of vulvovaginal candidiasis. J. Pharm. Sci. 2018, 107, 2674–2685. [Google Scholar] [CrossRef]
- Notario-Pérez, F.; Cazorla-Luna, R.; Martín-Illana, A.; Galante, J.; Ruiz-Caro, R.; das Neves, J.; Veiga, M.D. Design, fabrication and characterisation of drug-loaded vaginal films: State-of-the-art. J. Control. Release 2020, 327, 477–499. [Google Scholar] [CrossRef] [PubMed]
- Gahlot, N.; Maheshwari, R.K. Formulation and development of vaginal films of poorly water soluble drug, metronidazole, using mixed solvency concept and their evaluations. J. Drug Deliv. Ther. 2018, 8, 41–48. [Google Scholar] [CrossRef]
- Cazorla-Luna, R.; Notario-Pérez, F.; Martín-Illana, A.; Bedoya, L.M.; Tamayo, A.; Rubio, J.; Ruiz-Caro, R.; Veiga, M.D. Development and in vitro/ ex vivo characterization of vaginal mucoadhesive bilayer films based on ethylcellulose and biopolymers for vaginal sustained release of tenofovir. Biomacromolecules 2020, 21, 2309–2319. [Google Scholar] [CrossRef] [PubMed]
- Kumar, L.; Reddy, M.S.; Shirodkar, R.K.; Pai, G.K.; Krishna, V.T.; Verma, R. Preparation and characterisation of fluconazole vaginal films for the treatment of vaginal Candidiasis. Indian J. Pharm. Sci. 2013, 75, 585–590. [Google Scholar]
- Abilova, G.K.; Kaldybekov, D.B.; Irmukhametova, G.S.; Kazybayeva, D.S.; Iskakbayeva, Z.A.; Kudaibergenov, S.E.; Khutoryanskiy, V.V. Chitosan/poly(2-ethyl-2-oxazoline) films with ciprofloxacin for application in vaginal drug delivery. Materials 2020, 13, 1709. [Google Scholar] [CrossRef] [Green Version]
- Tentor, F.; Siccardi, G.; Sacco, P.; Demarchi, D.; Marsich, E.; Almdal, K.; Bose Goswami, S.; Boisen, A. Long lasting mucoadhesive membrane based on alginate and chitosan for intravaginal drug delivery. J. Mater. Sci. Mater. Med. 2020, 31, 25. [Google Scholar] [CrossRef]
- Jalil, A.; Asim, M.H.; Le, N.N.; Laffleur, F.; Matuszczak, B.; Tribus, M.; Bernkop-Schnürch, A. S-protected gellan gum: Decisive approach towards mucoadhesive antimicrobial vaginal films. Int. J. Biol. Macromol. 2019, 130, 148–157. [Google Scholar] [CrossRef]
- Calvo, N.L.; Svetaz, L.A.; Alvarez, V.A.; Quiroga, A.D.; Lamas, M.C.; Leonardi, D. Chitosan-hydroxypropyl methylcellulose tioconazole films: A promising alternative dosage form for the treatment of vaginal candidiasis. Int. J. Pharm. 2019, 556, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Mishra, R.; Joshi, P.; Mehta, T. Formulation, development and characterization of mucoadhesive film for treatment of vaginal candidiasis. Int. J. Pharm. Investig. 2016, 6, 47. [Google Scholar] [CrossRef] [Green Version]
- Cunha-Reis, C.; Machado, A.; Barreiros, L.; Araújo, F.; Nunes, R.; Seabra, V.; Ferreira, D.; Segundo, M.A.; Sarmento, B.; das Neves, J. Nanoparticles-in-film for the combined vaginal delivery of anti-HIV microbicide drugs. J. Control. Release 2016, 243, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.J.; Marathe, J.; Pudney, J.; Anderson, D. The structure of the human vaginal stratum corneum and its role in immune defense HHS public access. Am. J. Reprod. Immunol. 2014, 71, 618–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ways, T.M.M.; Lau, W.M.; Khutoryanskiy, V.V. Chitosan and its derivatives for application in mucoadhesive drug delivery systems. Polymers 2018, 10, 267. [Google Scholar] [CrossRef] [Green Version]
- Gu, J.; Yang, S.; Ho, E.A. Biodegradable film for the targeted delivery of siRNA-loaded nanoparticles to vaginal immune cells. Mol. Pharm. 2015, 12, 2889–2903. [Google Scholar] [CrossRef]
- Bhat, S.R.; Shivakumar, H.G. Bioadhesive controlled release clotrimazole vaginal tablets. Trop. J. Pharm. Res. 2010, 9, 339–346. [Google Scholar] [CrossRef] [Green Version]
- Meng, J.; Agrahari, V.; Ezoulin, M.J.; Purohit, S.S.; Zhang, T.; Molteni, A.; Dim, D.; Oyler, N.A.; Youan, B.B. Spray-dried thiolated chitosan-coated sodium alginate multilayer microparticles for vaginal HIV microbicide delivery. AAPS J. 2017, 19, 692–702. [Google Scholar] [CrossRef]
- Yang, T.-T.; Cheng, Y.-Z.; Qin, M.; Wang, Y.-H.; Yu, H.-L.; Wang, A.-L.; Zhang, W.-F. Thermosensitive chitosan hydrogels containing polymeric microspheres for vaginal drug delivery. Biomed. Res. Int. 2017, 2017, 12. [Google Scholar] [CrossRef] [Green Version]
- Malli, S.; Bories, C.; Pradines, B.; Loiseau, P.M.; Ponchel, G.; Bouchemal, K. In situ forming pluronic® F127/chitosan hydrogel limits metronidazole transmucosal absorption. Eur. J. Pharm. Biopharm. 2017, 112, 143–147. [Google Scholar] [CrossRef]
- Chatterjee, S.; Hui, P.C. Review of stimuli-responsive polymers in drug delivery and textile application. Molecules 2019, 24, 2547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabane, E.; Zhang, X.; Langowska, K.; Palivan, C.G.; Meier, W. Stimuli-responsive polymers and their applications in nanomedicine. Biointerphases 2012, 7, 1–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, A.S. Stimuli-responsive polymers: Biomedical applications and challenges for clinical translation. Adv. Drug Deliv. Rev. 2013, 65, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Sood, N.; Bhardwaj, A.; Mehta, S.; Mehta, A. Stimuli-responsive hydrogels in drug delivery and tissue engineering. Drug Deliv. 2016, 23, 748–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, D.D.; Lai, J.Y. Advancing the stimuli response of polymer-based drug delivery systems for ocular disease treatment. Polym. Chem. 2020, 11, 6988–7008. [Google Scholar] [CrossRef]
- Mei, L.; Chen, J.; Yu, S.; Huang, Y.; Xie, Y.; Wang, H.; Pan, X.; Wu, C. Expansible thermal gelling foam aerosol for vaginal drug delivery. Drug Deliv. 2017, 24, 1325–1337. [Google Scholar] [CrossRef] [Green Version]
- Tuğcu-Demiröz, F. Development of in situ poloxamer-chitosan hydrogels for vaginal drug delivery of benzydamine hydrochloride: Textural, mucoadhesive and in vitro release properties. Marmara Pharm. J. 2017, 21, 762–770. [Google Scholar] [CrossRef] [Green Version]
- Jelvehgari, M.; Montazam, H. Evaluation of mechanical and rheological properties of metronidazole gel as local delivery system. Arch. Pharm. Res. 2011, 34, 931–940. [Google Scholar] [CrossRef]
- Cevher, E.; Taha, M.A.M.; Orlu, M.; Araman, A. Evaluation of mechanical and mucoadhesive properties of clomiphene citrate gel formulations containing carbomers and their thiolated derivatives. Drug Deliv. 2008, 15, 57–67. [Google Scholar] [CrossRef] [Green Version]
- Nikhar, S.; Bansode, D.A.; Mahadik, K.R. Thermosensitive in situ gel of tinidazole in treatment of bacterial vaginosis: Formulation and evaluation. Int. J. Ayurveda Pharma Res. 2020, 8, 1–12. [Google Scholar]
- Patil, M.V.; Jadhav, R.L.; Shaikh, S.N.; Belhekar, S.N. Formulation and evaluation thermoreversible gel of antifungal agent for treatment of vaginal infection. J. Pharm. Res. Int. 2020, 32, 58–66. [Google Scholar] [CrossRef]
- Sosa, L.; Calpena, A.C.; Silva-Abreu, M.; Espinoza, L.C.; Rincón, M.; Bozal, N.; Domenech, O.; Rodríguez-Lagunas, M.J.; Clares, B. Thermoreversible gel-loaded amphotericin B for the treatment of dermal and vaginal candidiasis. Pharmaceutics 2019, 11, 312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, R.; Kumar, S.; Das Gupta, G. Preparation and evaluation of in situ gelling miconazole nitrate liquid suppository. Drug Invent. Today 2018, 10, 1556–1563. [Google Scholar]
- Zhang, Y.; Miyamoto, Y.; Ihara, S.; Yang, J.Z.; Zuill, D.E.; Angsantikul, P.; Zhang, Q.; Gao, W.; Zhang, L.; Eckmann, L. Composite thermoresponsive hydrogel with auranofin-loaded nanoparticles for topical treatment of vaginal trichomonad infection. Adv. Ther. 2019, 2, 1900157. [Google Scholar] [CrossRef] [PubMed]
- Timur, S.S.; Şahin, A.; Aytekin, E.; Öztürk, N.; Polat, K.H.; Tezel, N.; Gürsoy, R.N.; Çalış, S. Design and in vitro evaluation of tenofovir-loaded vaginal gels for the prevention of HIV infections. Pharm. Dev. Technol. 2018, 23, 301–310. [Google Scholar] [CrossRef]
- Alves, T.; Souza, J.; Rebelo, M.; Pontes, K.; Santos, C.; Lima, R.; Jozala, A.; Grotto, D.; Severino, P.; Rai, M.; et al. Formulation and evaluation of thermoresponsive polymeric blend as a vaginal controlled delivery system. J. Sol. Gel Sci. Technol. 2018, 86, 536–552. [Google Scholar] [CrossRef]
- Martín-Illana, A.; Notario-Pérez, F.; Cazorla-Luna, R.; Ruiz-Caro, R.; Veiga, M.D. Smart freeze-dried bigels for the prevention of the sexual transmission of HIV by accelerating the vaginal release of tenofovir during intercourse. Pharmaceutics 2019, 11, 232. [Google Scholar] [CrossRef] [Green Version]
- Cazorla-Luna, R.; Martín-Illana, A.; Notario-Pérez, F.; Bedoya, L.M.; Tamayo, A.; Ruiz-Caro, R.; Rubio, J.; Veiga, M.-D. Vaginal polyelectrolyte layer-by-layer films based on chitosan derivatives and Eudragit® S100 for pH responsive release of tenofovir. Mar. Drugs 2020, 18, 44. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Traore, Y.L.; Chen, Y.; Ho, E.A.; Liu, S. Switchable on-demand release of a nanocarrier from a segmented reservoir type intravaginal ring filled with a ph-responsive supramolecular polyurethane hydrogel. ACS Appl. Biol. Mater. 2018, 1, 652–662. [Google Scholar] [CrossRef]
- Kim, S.; Traore, Y.L.; Ho, E.A.; Shafiq, M.; Kim, S.H.; Liu, S. Design and development of pH-responsive polyurethane membranes for intravaginal release of nanomedicines. Acta Biomater. 2018, 82, 12–23. [Google Scholar] [CrossRef]
- Mahalingam, A.; Jay, J.I.; Langheinrich, K.; Shukair, S.; McRaven, M.D.; Rohan, L.C.; Herold, B.C.; Hope, T.J.; Kiser, P.F. Inhibition of the transport of HIV in vitro using a pH-responsive synthetic mucin-like polymer system. Biomaterials 2011, 32, 8343–8355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, H.; Sharma, A. Ion activated bioadhesive in situ gel of clindamycin for vaginal application. Int. J. Drug Deliv. 2011, 1, 32–40. [Google Scholar] [CrossRef]
- Bhardwaj, A.; Kumar, L.; Mehta, S.; Mehta, A. Stimuli-sensitive Systems-an emerging delivery system for drugs. Artif. Cells, Nanomed. Biotechnol. 2015, 43, 299–310. [Google Scholar] [CrossRef]
- Wagner, G.; Levin, R.J. Electrolytes in vaginal fluid during the menstrual cycle of coitally active and inactive women. J. Reprod. Fertil. 1980, 60, 17–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, P.; Patel, P. Formulation and evaluation of clindamycin HCL in situ gel for vaginal application. Int. J. Pharm. Investig. 2015, 5, 50–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harish, N.M.; Prabhu, P.; Charyulu, R.N.; Gulzar, M.A.; Subrahmanyam, E.V.S. Formulation and in vitro evaluation of in situ gels containing secnidazole for vaginitis. Indian J. Pharm. Sci. 2009, 71, 421–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agrawal, A.K.; Das, M.; Jain, S. In situ gel systems as “smart” carriers for sustained ocular drug delivery. Expert Opin. Drug Deliv. 2012, 9, 383–402. [Google Scholar] [CrossRef]
- Yenkar, P.; Mayee, R.; Nawale, R.; Chavan, R.; Salunke, T.; Bhoyar, V. Bio responsive in situ gel of clindamycin for vaginal application. Res. Rev. J. Pharm. Pharm. Sci. 2013, 2, 26–32. [Google Scholar]
- Abd Ellah, N.H.; Abouelmagd, S.A.; Abbas, A.M.; Shaaban, O.M.; Hassanein, K.M. Dual-responsive lidocaine in situ gel reduces pain of intrauterine device insertion. Int. J. Pharm. 2018, 538, 279–286. [Google Scholar] [CrossRef]
- Karimi, M.; Ghasemi, A.; Zangabad, P.S.; Rahighi, R.; Moosavi Basri, S.M.; Mirshekari, H.; Amiri, M.; Pishabad, Z.S.; Aslani, A.; Bozorgomid, M.; et al. Smart micro/nanoparticles in stimulus-responsive drug/gene delivery systems. Chem. Soc. Rev. 2016, 45, 1457–1501. [Google Scholar] [CrossRef] [Green Version]
- Guragain, S.; Bastakoti, B.P.; Malgras, V.; Nakashima, K.; Yamauchi, Y. Multi-stimuli-responsive polymeric materials. Chem. A Eur. J. 2015, 21, 13164–13174. [Google Scholar] [CrossRef] [PubMed]
- Schattling, P.; Jochum, F.D.; Theato, P. Multi-stimuli responsive polymers-the all-in-one talents. Polym. Chem. 2014, 5, 25–36. [Google Scholar] [CrossRef]
- Cheaburu-Yilmaz, C.N.; Yilmaz, O.; Kose, F.A.; Bibire, N. Chitosan-graft-poly(N-isopropylacrylamide)/PVA cryogels as carriers for mucosal delivery of voriconazole. Polymers 2019, 11, 1432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yermak, I.M.; Davydova, V.N.; Kravchenko, A.O.; Chistyulin, D.A.; Pimenova, E.A.; Glazunov, V.P. Mucoadhesive properties of sulphated polysaccharides carrageenans from red seaweed families Gigartinaceae and Tichocarpaceae. Int. J. Biol. Macromol. 2020, 142, 634–642. [Google Scholar] [CrossRef]
- Lin, X.; Ma, Q.; Su, J.; Wang, C.; Kankala, R.K.; Zeng, M.; Lin, H.; Zhou, S.F. Dual-responsive alginate hydrogels for controlled release of therapeutics. Molecules 2019, 24, 2089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, M.J.; Yao, M.; Gao, S.; Zhang, A.P.; Tam, H.Y.; Wai, P.K. Rapid 3D patterning of poly(acrylic acid) ionic hydrogel for miniature pH sensors. Adv. Mater. 2016, 28, 1394–1399. [Google Scholar] [CrossRef]
- Thakur, G.; Singh, A.; Singh, I. Formulation and evaluation of transdermal composite films of chitosan-montmorillonite for the delivery of curcumin. Int. J. Pharm. Investig. 2016, 6, 31. [Google Scholar]
- Abd Ellah, N.H.; Abdel-Aleem, J.A.; Abdo, M.N.; Abou-Ghadir, O.F.; Zahran, K.M.; Hetta, H.F. Efficacy of ketoconazole gel-flakes in treatment of vaginal candidiasis: Formulation, in vitro and clinical evaluation. Int. J. Pharm. 2019, 567, 118472. [Google Scholar] [CrossRef]
- Kaur, L.; Abhijeet, A.; Jain, S.K. Safe and effective delivery of amphotericin B: A survey of patents. Recent Pat. Nanotechnol. 2017, 11, 214–234. [Google Scholar] [CrossRef]
- Kang, J.Y.; Gao, J.; Shin, D.H.; Alvarez, C.; Zhong, W.; Kwon, G.S. Pharmacokinetics and renal toxicity of monomeric amphotericin B in rats after a multiple dose regimen. Pharm. Nanotechnol. 2016, 4, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.T.; Shin, B.K.; Garripelli, V.K.; Kim, J.K.; Davaa, E.; Jo, S.; Park, J.S. A thermosensitive vaginal gel formulation with HPγCD for the pH-dependent release and solubilization of amphotericin B. Eur. J. Pharm. Sci. 2010, 41, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Garripelli, V.K.; Kim, J.K.; Namgung, R.; Kim, W.J.; Repka, M.A.; Jo, S. A novel thermosensitive polymer with pH-dependent degradation for drug delivery. Acta Biomater. 2010, 6, 477–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swift, T.; Swanson, L.; Geoghegan, M.; Rimmer, S. The pH-responsive behaviour of poly(acrylic acid) in aqueous solution is dependent on molar mass. Soft Matter 2016, 12, 2542–2549. [Google Scholar] [CrossRef] [Green Version]
- Carbomer—Inactive Ingredient Search for Approved Drug Products. Available online: https://www.accessdata.fda.gov/scripts/cder/iig/index.cfm?event=browseByLetter.page&Letter=C (accessed on 18 July 2020).
- Gupta, K.M.; Barnes, S.R.; Tangaro, R.A.; Roberts, M.C.; Owen, D.H.; Katz, D.F.; Kiser, P.F. Temperature and pH sensitive hydrogels: An approach towards smart semen-triggered vaginal microbicidal vehicles. J. Pharm. Sci. 2007, 96, 670–681. [Google Scholar] [CrossRef] [PubMed]
- Ilomuanya, M.O.; Elesho, R.F.; Amenaghawon, A.N.; Adetuyi, A.O.; Velusamy, V.; Akanmu, A.S. Development of trigger sensitive hyaluronic acid/palm oil-based organogel for in vitro release of HIV/AIDS microbicides using artificial neural networks. Futur. J. Pharm. Sci. 2020, 6, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Esposito, C.L.; Kirilov, P.; Roullin, V.G. Organogels, promising drug delivery systems: An update of state-of-the-art and recent applications. J. Control. Release 2018, 271, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, A.M.; Faisal, W.; Saleh, K.I.; Osman, S.K. Self-assembling organogels based on pluronic and lecithin for sustained release of etodolac: In Vitro and in vivo correlation. Curr. Drug Deliv. 2017, 14, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Valcarcel, J.; García, M.R.; Varela, U.R.; Vázquez, J.A. Hyaluronic acid of tailored molecular weight by enzymatic and acid depolymerization. Int. J. Biol. Macromol. 2020, 145, 788–794. [Google Scholar] [CrossRef]
- Buhren, B.A.; Schrumpf, H.; Hoff, N.P.; Bölke, E.; Hilton, S.; Gerber, P.A. Hyaluronidase: From clinical applications to molecular and cellular mechanisms. Eur. J. Med. Res. 2016, 21, 5. [Google Scholar] [CrossRef] [Green Version]
- Guidance for Industry Vaginal Microbicides: Development for the Prevention of HIV Infection; FDA: Silver Spring, MD, USA, 2014.
- Rastogi, R.; Teller, R.S.; Mesquita, P.M.; Herold, B.C.; Kiser, P.F. Osmotic pump tablets for delivery of antiretrovirals to the vaginal mucosa. Antivir. Res. 2013, 100, 255–258. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.F.; Afrooz, H.; Hampel, R.; Mohamed, E.M.; Bhattacharya, R.; Cook, P.; Khan, M.A.; Rahman, Z. Blend of cellulose ester and enteric polymers for delayed and enteric coating of core tablets of hydrophilic and hydrophobic drugs. Int. J. Pharm. 2019, 567, 118462. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Sun, K.; Mu, H.; Tang, M.; Liang, R.; Wang, A.; Zhou, S.; Sun, H.; Zhao, F.; Yao, J.; et al. pH and temperature dual-sensitive liposome gel based on novel cleavable mPEG-Hz-CHEMS polymeric vaginal delivery system. Int. J. Nanomed. 2012, 7, 2621–2630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, D.; Liu, W.; Shen, Y.; Mu, H.; Zhang, Y.; Liang, R.; Wang, A.; Sun, K.; Fu, F. Effects of a novel pH-sensitive liposome with cleavable esterase-catalyzed and pH-responsive double smart mPEG lipid derivative on ABC phenomenon. Int J. Nanomed. 2011, 6, 2053–2061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, D.; Jiang, X.; Liu, J.; Jin, X.; Zhang, C.; Ping, Q. In vivo evaluation of novel pH-sensitive mPEG-Hz-chol conjugate in liposomes: Pharmacokinetics, tissue distribution, efficacy assessment. Artif. Cells Blood Substit. Immob. Biotechnol 2010, 38, 136–142. [Google Scholar] [CrossRef]
- dos Santos Ramos, M.A.; Calixto, G.; de Toledo, L.G.; Bonifácio, B.V.; dos Santos, L.C.; de Almeida, M.T.; Chorilli, M.; Bauab, T.M. Liquid crystal precursor mucoadhesive system as a strategy to improve the prophylactic action of Syngonanthus nitens (Bong.) Ruhland against infection by Candida krusei. Int. J. Nanomed. 2015, 10, 7455–7466. [Google Scholar] [CrossRef]
- dos Santos Ramos, M.A.; de Toledo, L.G.; Calixto, G.M.; Bonifácio, B.V.; de Freitas Araújo, M.G.; dos Santos, L.C.; de Almeida, M.T.; Chorilli, M.; Bauab, T.M. Syngonanthus nitens Bong. (Rhul.)-loaded nanostructured system for vulvovaginal candidiasis treatment. Int. J. Mol. Sci. 2016, 17, 1368. [Google Scholar] [CrossRef]
- Huang, J.; Liu, L.; Gui, S.; Wang, X.; Hu, R.; Zhang, Y.; Tian, C.; Xia, M.; Chu, X. A novel phytantriol-based in situ liquid crystal gel for vaginal delivery. AAPS Pharmscitech 2019, 20, 185. [Google Scholar]
- de Araújo, P.R.; Calixto, G.M.; da Silva, I.C.; de Paula Zago, L.H.; Oshiro, J.A.J.; Pavan, F.R.; Ribeiro, A.O.; Fontana, C.R.; Chorilli, M. Mucoadhesive in situ gelling liquid crystalline precursor system to improve the vaginal administration of drugs. AAPS Pharmscitech 2019, 20, 225. [Google Scholar] [CrossRef]
- Chavoustie, S.E.; Carter, B.A.; Waldbaum, A.S.; Donders, G.G.G.; Peters, K.H.; Schwebke, J.R.; Paull, J.R.A.; Price, C.F.; Castellarnau, A.; McCloud, P.; et al. Two phase 3, double-blind, placebo-controlled studies of the efficacy and safety of Astodrimer 1% Gel for the treatment of bacterial vaginosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 245, 13–18. [Google Scholar] [CrossRef]
- Borgman, R.J. Multi-Center Study of New Medications to Treat Vaginal Infections. Available online: https://www.clinicaltrials.gov/ct2/show/NCT02308046?cond=Vaginal+Infection&draw=1&rank=4 (accessed on 18 July 2020).
- Mcgowan, I.; Gomez, K.; Bruder, K.; Febo, I.; Chen, B.A.; Richardson, B.A.; Husnik, M.; Livant, E.; Price, C. Phase 1 randomized trial of the vaginal safety and acceptability of SPL7013 Gel (VivaGel® ) in sexually active young women. AIDS 2012, 25, 1057–1064. [Google Scholar] [CrossRef] [Green Version]
- Khazaeian, S.; Navidian, A.; Navabi-Rigi, S.D.; Araban, M.; Mojab, F.; Khazaeian, S. Comparing the effect of sucrose gel and metronidazole gel in treatment of clinical symptoms of bacterial vaginosis: A randomized controlled trial 11 Medical and Health Sciences 1103 Clinical Sciences. Trials 2018, 19, 4–11. [Google Scholar]
- Marrazzo, J.M.; Dombrowski, J.C.; Wierzbicki, M.R.; Perlowski, C.; Pontius, A.; Dithmer, D.; Schwebke, J. Safety and efficacy of a novel vaginal anti-infective, TOL-463, in the treatment of bacterial vaginosis and vulvovaginal candidiasis: A randomized, single-blind, phase 2, controlled trial. Clin. Infect. Dis. 2019, 68, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Acarturk, F. Mucoadhesive vaginal drug delivery systems. Recent Pat. Drug Deliv. Formul. 2009, 3, 193–205. [Google Scholar] [CrossRef] [PubMed]
- Abbas, A.M.; Shabaan, S.O. Once daily in-situ forming versus twice-daily conventional metronidazole vaginal gels for treatment of bacterial vaginosis: A randomized controlled trial. J. Genit. Syst. Disord. 2015, 4, 1–5. [Google Scholar] [CrossRef]
- Chavoustie, S.E.; Jacobs, M.; Reisman, H.A.; Waldbaum, A.S.; Levy, S.F.; Hillier, S.L.; Nyirjesy, P. Metronidazole vaginal gel 1.3% in the treatment of bacterial vaginosis. J. Low. Genit. Tract Dis. 2015, 19, 129–134. [Google Scholar] [CrossRef] [Green Version]
- Darwesh, B.; Aldawsari, H.M.; Badr-Eldin, S.M. Optimized chitosan/anion polyelectrolyte complex based inserts for vaginal delivery of fluconazole: In vitro/in vivo evaluation. Pharmaceutics 2018, 10, 227. [Google Scholar] [CrossRef] [Green Version]
- Qin, H.; Wang, J.; Wang, T.; Gao, X.; Wan, Q.; Pei, X. Preparation and characterization of chitosan/β-glycerophosphate thermal-sensitive hydrogel reinforced by graphene oxide. Front. Chem. 2018, 6, 565. [Google Scholar] [CrossRef]
- Modrzejewska, Z.; Skwarczyńska, A.; Maniukiewicz, W.; Douglas, T.E.L. Mechanism of formation of thermosensitive chitosan chloride gels. Prog. Chem. Appl. Chitin Deriv. 2014, 19, 125–134. [Google Scholar] [CrossRef] [Green Version]
- Szymańska, E.; Sosnowska, K.; Miltyk, W.; Rusak, M.; Basa, A.; Winnicka, K. The effect of β-glycerophosphate crosslinking on chitosan cytotoxicity and properties of hydrogels for vaginal application. Polymers 2015, 7, 2223–2244. [Google Scholar] [CrossRef] [Green Version]
- Andany, N.; Kennedy, V.L.; Aden, M.; Loutfy, M. Perspectives on menopause and women with HIV. Int. J. Womens Health 2016, 8, 1–22. [Google Scholar]
- Muthukumar, T.; Song, J.E.; Khang, G. Biological role of gellan gum in improving scaffold drug delivery, cell adhesion properties for tissue engineering applications. Molecules 2019, 24, 4514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García, M.C. Ionic-Strength-Responsive Polymers for Drug Delivery Applications; Elsevier Ltd.: Cambridge, UK, 2018; ISBN 9780081019955. [Google Scholar]
- Salunke, S.R.; Patil, S.B. Ion activated in situ gel of gellan gum containing salbutamol sulphate for nasal administration. Int. J. Biol. Macromol. 2016, 87, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Yang, F.; Feng, L.; Yang, L.; Chen, L.; Wei, G.; Lu, W. In vivo retention of poloxamer-based in situ hydrogels for vaginal application in mouse and rat models. Acta Pharm. Sin. B 2017, 7, 502–509. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Vaginal Infections | Causes | Risk Factors | Symptoms | Diagnosis | Treatment |
|---|---|---|---|---|---|
| Bacterial vaginosis (BV) | Caused by overgrowth of anaerobic and microaerophilic bacteria such as Gardnerella vaginalis, Atopobium vaginae, Bacteroides spp., etc. | Douching, sexual intercourse, and poor personal hygiene | Vaginal discharge with fishy odour, itchiness, and irritation | Nugent criteria, Amsel criteria, or Hay–Ison criteria | Oral metronidazole, oral clindamycin, oral tinidazole, metronidazole gel, clindamycin cream and clindamycin ovules |
| Vulvovaginal candidiasis (VVC) | Caused primarily by Candida albicans | Patient’s sexual and hygienic habits, the use of hormones and antibiotics, pregnancy, and immunosuppression | Abnormal vaginal discharge, dysuria, dyspareunia, and vaginal soreness | Positive wet-mount method, microscopic examination of vaginal swab culture, vaginal yeast count | Oral and topical azole therapies such as fluconazole, clotrimazole, miconazole, tioconazole, butoconazole and terconazole |
| Trichomoniasis | Trichomonas vaginalis | Infertility, poor pregnancy outcomes and sexually transmitted infections (STIs) acquisition | Yellow-green vaginal discharge, lower abdominal pain, dysuria, and vulvar irritation | Microscopic examination of vaginal fluid smear | Oral metronidazole and tinidazole, along with this topical formulation for metronidazole |
| Human immunodeficiency virus (HIV) infection | Human immunodeficiency virus | Risk of infection are associated with intravenous drug users, sex workers, transgender people, and, gay | Fever, myalgias, and swollen lymph nodes. Additionally liver dysfunction, tuberculosis, and acquired immunodeficiency syndrome (AIDS) | Detection of antibody | Antiretroviral drugs such as tenofovir, nevirapine, ritonavir, enfuvirtide, maraviroc etc. |
| Human papillomavirus (HPV) infection | Human papillomavirus | lower socioeconomic status, oral contraceptive use, history of multiple sexual partners, high parity, immunosuppression | Genital warts | Pap smear, biopsy | Prophylaxis by vaccine, treatment of wart by Salicylic acid, Trichloroacetic acid etc. |
| Type of Formulation | Objective of Research | Polymer Used | Disease Type/Drug | Cell Line/Animal Model | Outcomes | Source |
|---|---|---|---|---|---|---|
| Conventional liposomes | To develop azithromycin liposomes and evaluate their ability for the treatment of cervicovaginal infections | Phosphatidylcholine Hydrogenated phosphatidylcholine | Escherichia coli-related vaginal infections/azithromycin | HeLa cells |
| [71] |
| Deformable propylene glycol liposomes | To develop azithromycin liposomes and explore their potentials for treating cervicovaginal infections | Phosphatidylcholine Monoacyl phosphatidylcholine Propylene glycol | Escherichia coli-related vaginal infections/azithromycin | HeLa cells |
| [71] |
| Mucus-penetrating liposomes | To deliver the drug for local therapy for HPV vaginal infections | Cholesterol Methoxy poly (ethylene glycol)-modified lipids Phosphatidylcholine | HPV vaginal infections | - |
| [72] |
| Chitosan-coated liposomes | To prepare and optimize vaginal formulation of Resveratrol for effective treatment of vaginal infection and inflammation | Phosphatidylcholine Chitosan | Vaginal inflammation and infection/Resveratrol | - |
| [73] |
| Chitosan-surface modified PLGA nanoparticles | To vectorize clotrimazole with polymeric nanoparticles to treat vaginitis | Poly(lactic-co-glycolic acid) (PLGA) (lactide: glycolide 50:50) Low molecular weight chitosan | Candida albicans vaginal infections/Clotrimazole | Porcine cell culture |
| [74] |
| Chitosan-based nanoparticles | To evaluate the therapeutic efficacy of the developed miconazole nitrate-chitosan-based nanoparticles against murine vulvovaginal candidiasis | Chitosan | Vulvovaginal candidiasis/Miconazole | Mice bone marrow cells |
| [75] |
| Eudragit RL100 nanoparticles coated with HA | To overcome the drawbacks of the conventional formulations with the developed AmB-loaded Eudragit RL100 nanoparticles coated with HA | Eudragit RL100 HA | Vulvovaginal candidiasis/AmB | - |
| [77] |
| Nanocapsules | To develop chitosan nanocapsules loaded with antifungal drug suitable for vaginal application | Chitosan Lecithin | Vaginal candidiasis/Tioconazole, Econazole | Human keratinocyte cell line |
| [78] |
| Mucoadhesive liposomal gel | To fabricate sertaconazole nitrate-loaded liposomes for the effective treatment of vaginal candidiasis | Soy phosphatidylcholine Cholesterol Dimethyldidodecylammonium bromide (DDAB) Pectin | Vaginal Candidiasis/Sertaconazole | Sprague-Dawley rats |
| [79] |
| Vaginal lipogel | To disperse drug-loaded liposomes into mucoadhesive gel for vaginal drug delivery | Carbopol® 974P NF, HPMC K100M | Vaginitis/Benzydamide hydrochloride | - |
| [80] |
| Vaginal in situ gel | To combine poloxamer and different types of HPMC to improve the mucoadhesive and mechanical properties of the in situ gels to prolong the residence time in vaginal cavity. | HPMC K100M, E50 | Vaginal candidiasis/ Clotrimazole | - |
| [82] |
| Microgel | To formulate and evaluate mucoadhesive microgels for enhanced antifungal activity of miconazole nitrate. | Polycarbophil | Vulvovaginal candidiasis/Miconazole nitrate | Female rabbits |
| [81] |
| Nanocapsules in hydrogel | To design polymeric nanocapsules containing hydrogel to increase the drug residence time in the vaginal epithelium. | Eudragit® RS100 nanocapsules, gellan gum | Vaginal trichomoniasis/Indole-3-carbinol (I3C) | - |
| [83] |
| Nanoemulsion gel | To formulate mucoadhesive nanoemulsion-based vaginal gel for vaginal candidiasis. | Carbopol 934, HPMC, NaCMC, xanthan gum | Vaginal candidiasis/Oxiconazole nitrate | - |
| [84] |
| Electrospun nanofibers | To develop and characterize innovative vaginal dosage forms for the treatment of bacterial vaginosis | PVP | Bacterial vaginosis/Metronidazole | - |
| [86] |
| Electrospun mucoadhesive nanofibers | To assess the antifungal properties of mucoadhesive clotrimazole loaded nanofiber versus vaginal film | Dextran Sodium alginate Polyvinyl alcohol | Vaginal candidiasis/Clotrimazole | Human gingival fibroblast cells |
| [87] |
| PLGA nanofibers | To develop AmB-loaded PLGA nanofibers as alternative drug delivery systems | PLGA (75:25) | Vulvovaginal candidiasis/AmB | Female Wistar rats (Rattus novergicus) |
| [88] |
| Vaginal film | To develop a mucoadhesive vaginal film based on a mixture of chitosan (CHI) and poly(2-ethyl-2-oxazoline) (POZ). | Chitosan | Bacterial vaginosis/ Ciprofloxacin | - |
| [93] |
| Vaginal membrane | To develop an alginate/chitosan (AC) membrane with bactericide effect and controlled release property. | Alginate, chitosan | Bacterial vaginosis/Metronidazole | Cervix epithelial cells Ect1/E6E7 |
| [94] |
| Vaginal film | To combine the advantages of in situ gelling polymers and thiomers to enhance vaginal residence time. | S-protected gellan gum (S-GG 81, S-GG 174) | Bacterial vaginosis/Metronidazole | Caco-2 cells |
| [95] |
| Vaginal film | To develop a vaginal film using of two polymers to enhance the therapeutic efficacy for vaginal candidiasis. | Chitosan, HPMC | Vaginal candidiasis/Ticonazole | Human HCC cell lines Huh7 |
| [96] |
| Vaginal film | To develop vaginal films with a different combination of polymers and plasticizers for vaginal candidiasis. | HPC, sodium alginate | Vaginal candidiasis/Clotrimazole | - |
| [97] |
| Type of Formulation | Objective of Research | Stimuli Type and Polymer Used | Disease Type/Drug/Formulation | Cell Line/Animal Model | Outcomes | Source |
|---|---|---|---|---|---|---|
| Thermal gelling foam aerosol | To combine the advantages of gel and foam for retention and drug penetration in vagina | Temperature Polymers: P407 P188 Carbopol | Vaginitis and cervical erosion/silver nanoparticle | Sprague Dawley (SD) rats |
| [111] |
| In situ poloxamer-chitosan hydrogel | To develop a vaginal delivery system for benzydamine hydrochloride (BNZ) using poloxamer-chitosan in situ hydrogels. | Temperature Polymers: P407 Chitosan H | Vaginitis/benzydamine hydrochloride | Cow vaginal mucosa |
| [112] |
| In situ gel of tinidazole | To avoid hepatic first-pass metabolism, a reduction in the incidence and severity of gastrointestinal side-effects. | Temperature Polymers: P407 HPMC E100 | Bacterial vaginosis/Tinidazole | - |
| [115] |
| Clotrimazole-loaded vaginal gel | To formulate and evaluate thermoreversible gel of antifungal agent Clotrimazole for treatment of vaginal infection. | Temperature Polymers: Pluronic F127 Pluronic F68 Polycarbophil | Candidiasis/ Clotrimazole | - |
| [116] |
| Thermoreversible gel-loaded AmB | To achieve an improved release of amphotericin B for skin and vaginal treatment against Candida spp. | Temperature Polymer: P407 | Candidiasis/AmB | Vaginal porcine mucosae |
| [117] |
| Miconazole nitrate liquid vaginal suppository | To prepare and evaluate of in situ gelling miconazole nitrate liquid vaginal suppository for fungal infection. | Temperature Polymers: P188 P407 HPMC | Candidiasis/Miconazole nitrate | - |
| [118] |
| Auranofin-nanoparticle composite hydrogel | To address the challenges of vaginal drug delivery with a novel thermo-responsive nanoparticle (NP)-hydrogel composite for the effective topical treatment of trichomoniasis. | Temperature Polymers: Chitosan Pluronic F127 (P407) | Trichomoniasis/Auranofin | Bagg Albino (BALB/c) mice |
| [119] |
| Tenofovir-loaded vaginal gel | To design a thermogelling system which releases the antiretroviral agent in a controlled fashion while patient compliance will be increased with both prolonged contact time and ease of application. | Temperature Polymers: Pluronic F127 Chitosan | HIV infection Drug: Tenofovir | L929 cell line |
| [120] |
| Polymeric blend hydrogel | To fabricate and optimize different thermo-responsive and mucoadhesive hydrogel for improving the vaginal delivery of CUR. | Temperature Polymers: P407 Chitosan HPMC K4M | Vaginal mucosal inflammation and infectious diseases, including HPV infection/Curcumin | HeLa cells |
| [121] |
| Type of Formulation | Objective of Research | Stimuli Type and Polymer Used | Disease Type/Drug | Cell Line/Animal Model | Outcomes | Source |
|---|---|---|---|---|---|---|
| Freeze-dried bigels | To obtain freeze-dried bigels for the controlled release of Tenofovir (TFV) in the vaginal environment. | pH Polymers: Pectin | HIV infection/Tenofovir | - |
| [122] |
| Vaginal polyelectrolyte layer-by-layer film | To develop polyelectrolyte multilayers vaginal films based on optimized chitosan derivatives and Eudragit® S100 using the layer-by-layer technique. | pH Polymers: Chitosan citrate Methyl polymethacrylate (Eudragit® S100) | HIV infection/Tenofovir | Lymphoblastic cell line (MT-2) Macrophage-monocyte derived cell line (THP-1) Uterine/endometrial epithelial cell line (HEC-1A) |
| [123] |
| Polyurethane hydrogel in intravaginal ring | To synthesise supramolecular pH-responsive hydrogel to filled in the lumen of reservoir-IVRs for the on-demand release of nanocarriers. | pH Polymers: 2,2-dimethylolpropionic acid (DMPA) Hexamethylene diisocyanate (HDI) PEG | HIV infection/siRNA | VK2/E6E7 cell lines |
| [124] |
| Polyurethane membrane in intravaginal ring | To develop a pH-responsive membrane for vaginal delivery of nanoparticles to achieve site specific delivery. | pH Polymers: 1,4-Bis(2-hydroxyethyl) piperazine (HEP) 4,40-Methylenebis (phenyl isocyanate) (MDI) PEG | HIV infection/siRNA | Human vaginal epithelial cell line (VK2/E6E7) Human T-cell line (Sup-T1) |
| [125] |
| Synthetic mucin-like polymer system | To design a biologically inspired synthetic mucin-like polymer system to prevent transport of virions in the vagina. | pH Polymers: Phenylboronic acid (PBA)-salicylhyldroxamic acid (SHA) crosslinked polymers | HIV infection | VK2/E6E7 cell lines/ VEC-100 tissues BALB/c mice |
| [126] |
| Type of Formulation | Objective of Research | Stimuli Type and Polymer Used | Disease Type/Drug | Cell Line/Animal Model | Outcomes | Source |
|---|---|---|---|---|---|---|
| Vaginal in situ gel | To develop an in situ gel of clindamycin with prolonged retention time in the vaginal cavity. | Ion-responsive Polymer: Gellan gum | Bacterial vaginosis/Clindamycin | - |
| [127] |
| Vaginal in situ gel | To combine advantages of both gels and solution for vaginal application. | Ion-responsive Polymer: Gellan gum (Gelrite®) | Vaginitis/Clindamycin | - |
| [130] |
| Vaginal in situ gel | To formulate an in situ vaginal gel based on ion-activated systems to prolong the drug release. | Ion-responsive Polymer: Gellan gum | Vaginal trichomoniasis/Secnidazole | - |
| [131] |
| Type of Formulation | Objective of Research | Stimuli Type and Polymer Used | Disease Type/Drug | Cell Line/Animal Model | Outcomes | Source |
|---|---|---|---|---|---|---|
| In situ gel | To develop in situ gel formulation for prolonged drug release for vaginal application. | Temperature and ion Polymer: PF-127/68 and gellan gum | Bacterial vaginosis/Clindamycin | - |
| [133] |
| Hydrogel | To develop biocompatible hydrogel-based formulations for sustained drug release. | Temperature and pH Polymer: SA/pNIPAAm | Bacterial vaginosis/Oxytetracycline (OTC) | Human umbilical vein endothelial cells (HUVEC) cells |
| [140] |
| Flakes-loaded in situ gel | To design and develop a multifunctional ketoconazole (KTZ) carrier to provide efficient spreading and coating of the vagina due to free-flowing properties during application, flakes entanglement within folded vaginal epithelia, and sustained release for the treatment of VVC. | Temperature and ion Polymer: PF-127 and chitosan/gellan gum | Vulvovaginal candidiasis/KTZ (in the form of KTZ/β-CD complex) | - |
| [143] |
| In situ gel | To design a vaginal gel formulation with thermosensitive and mucoadhesive properties to ensure longer residence at the infection site, thereby providing a pH-dependent sustained release profile for AmB. | Temperature and pH Polymer: MBCP-2 copolymer | Vulvovaginal candidiasis/AmB (in the form of AmB-HPγCD complex) | HEK 293 cells and female ICR mice |
| [146] |
| In situ hydrogel | To prepare and characterise physically crosslinked gel formulations of chitosan-graft-PNIPAAm and PVA for smart delivery of voriconazole for mucosal applications. | Temperature and pH Polymer: CS-g-PNIPAAm/PVA grafted copolymer (75/25 ratio) | Drug: Voriconazole | HK-2 and NIH-3T3 cell lines |
| [138] |
| In situ hydrogel | To design a smart bio-responsive microbicide that is able to coat vaginal tissue and provide a burst release of entrapped antiviral agents when exposed to semen. | Temperature and pH Polymer: Poly(NiPAAm-co-BM-co-AA) | HIV infection (Pre-exposure prophylaxis) | Immortalised L-929 mouse fibroblasts cell line |
| [150] |
| Organogel | To develop and evaluate HA/palm oil-based organogel loaded with MRV which would be released using hyaluronidase as the trigger for pre-exposure prophylaxis of HIV. | Temperature and hyaluronidase enzyme Polymer: HA | HIV infection (Pre-exposure prophylaxis)/Maraviroc | TZM-bl cell lines and HeLa cell lines |
| [151] |
| pH-sensitive vaginal osmotic pump | To develop an osmotic pump tablet that can deliver antiretrovirals for several days. | pH and osmotic pressure Polymer: CAP | HIV infection (Pre-exposure prophylaxis)/ IQP-0528 | Adult female sheep |
| [157] |
| In situ liposome gel | To prepare a dual temperature- and pH-sensitive cleavable liposome gel loaded with arctigenin. | Temperature and pH Polymer: P407/188 and mPEG-Hz-CHEMS | Arctigenin | HEK 293 cells |
| [159] |
| Type of Formulation | Objective of Research | Stimuli Type and Polymer Used | Disease Type/Drug | Cell Line/Animal Model | Outcomes | Source |
|---|---|---|---|---|---|---|
| Liquid crystal precursor mucoadhesive systems | To evaluate the potential of the methanolic extract of scapes of Syngonanthus nitens (S. nitens) and a S. nitens-loaded liquid crystal precursor system | Water Carbopol 974P Polycarbophil | Vulvovaginal candidiasis with Candida krusei Drug: Syngonanthus nitens | Wistar female rats (Rattus norvegicus) |
| [162] |
| Liquid crystal precursor mucoadhesive systems | To evaluate the antifungal activity of S. nitens extract that was not loaded or loaded into a liquid crystal precursor system | Water Carbopol 974P Polycarbophil | Vulvovaginal candidiasis with Candida albicans Drug: Syngonanthus nitens | Wistar female rats (Rattus norvegicus) |
| [163] |
| Phytantriol-Based in situ liquid crystal gel | To evaluate the potential of in situ liquid crystal gels based on phytantriol for vaginal delivery | Water Phytantriol 64% w/w Ethanol 16% w/w Water 20% w/w | Cervical cancer Drug: Sinomenine hydrochloride | Sprague Dawley (SD) rats |
| [164] |
| Mucoadhesive in situ gelling liquid crystalline precursor system | To improve the vaginal administration of drugs | Water P407 | Vaginal bacterial infection and gynaecological cancers. Drug: Hypericin | L-929 cell line |
| [165] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pandey, M.; Choudhury, H.; Abdul-Aziz, A.; Bhattamisra, S.K.; Gorain, B.; Carine, T.; Wee Toong, T.; Yi, N.J.; Win Yi, L. Promising Drug Delivery Approaches to Treat Microbial Infections in the Vagina: A Recent Update. Polymers 2021, 13, 26. https://doi.org/10.3390/polym13010026
Pandey M, Choudhury H, Abdul-Aziz A, Bhattamisra SK, Gorain B, Carine T, Wee Toong T, Yi NJ, Win Yi L. Promising Drug Delivery Approaches to Treat Microbial Infections in the Vagina: A Recent Update. Polymers. 2021; 13(1):26. https://doi.org/10.3390/polym13010026
Chicago/Turabian StylePandey, Manisha, Hira Choudhury, Azila Abdul-Aziz, Subrat Kumar Bhattamisra, Bapi Gorain, Teng Carine, Tan Wee Toong, Ngiam Jing Yi, and Lim Win Yi. 2021. "Promising Drug Delivery Approaches to Treat Microbial Infections in the Vagina: A Recent Update" Polymers 13, no. 1: 26. https://doi.org/10.3390/polym13010026