

A Mechanistic Insight into Beneficial Effects of Polyphenols in the Prevention and Treatment of Nephrolithiasis: Evidence from Recent In Vitro Studies
 , , and
, , and 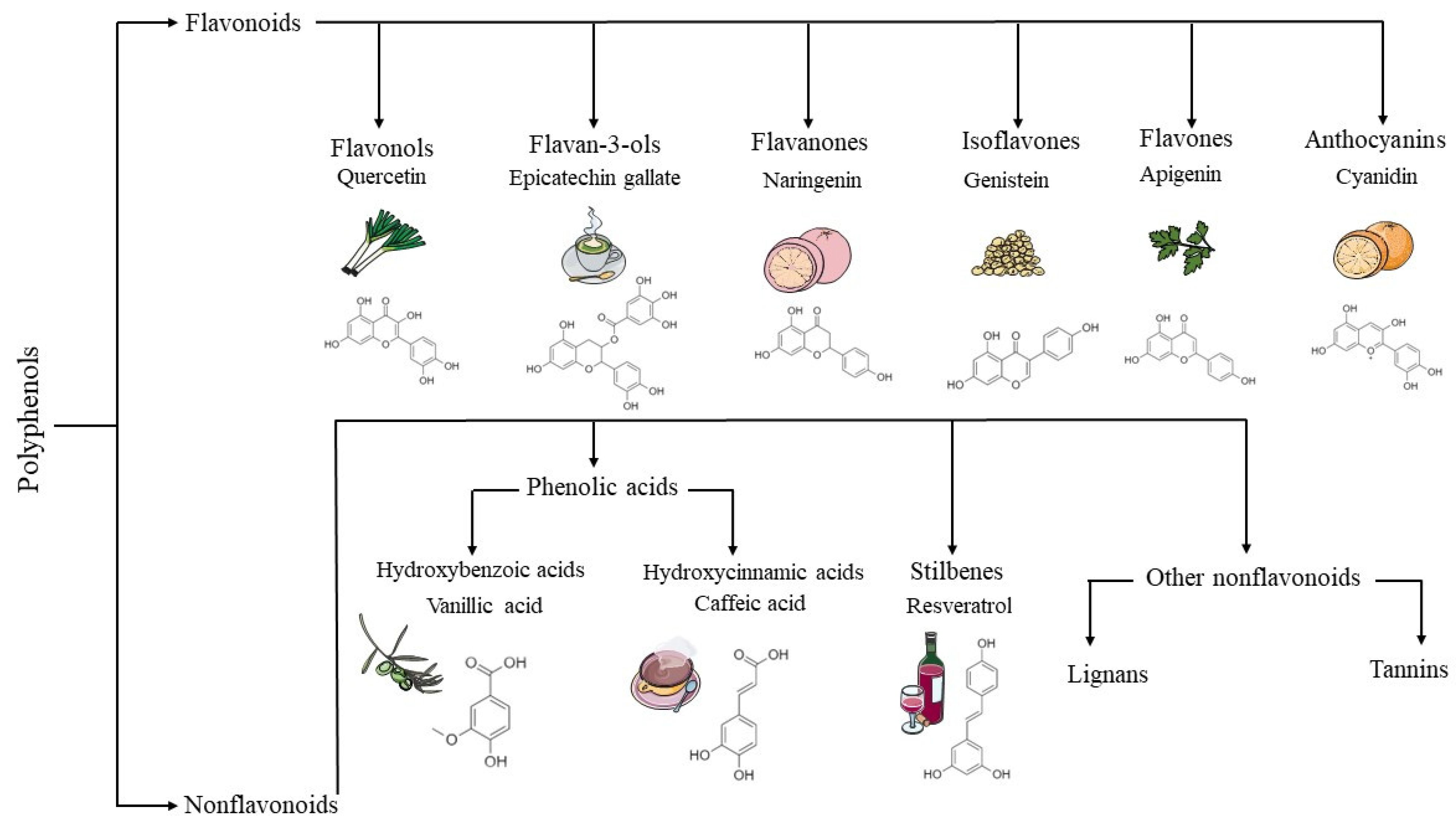{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
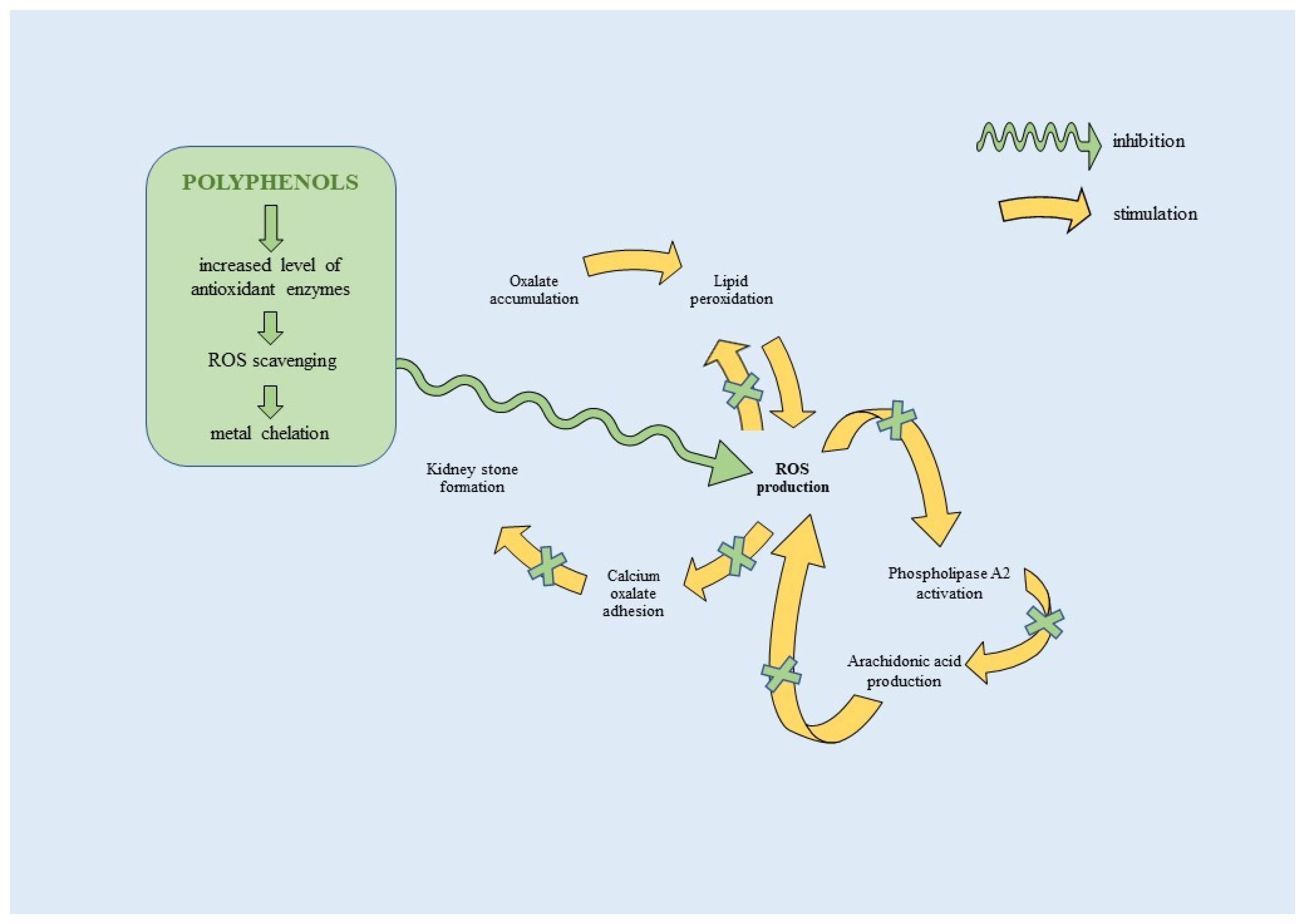
2. The Cellular Mechanisms of Beneficial Effects of Polyphenols in Nephrolithiasis
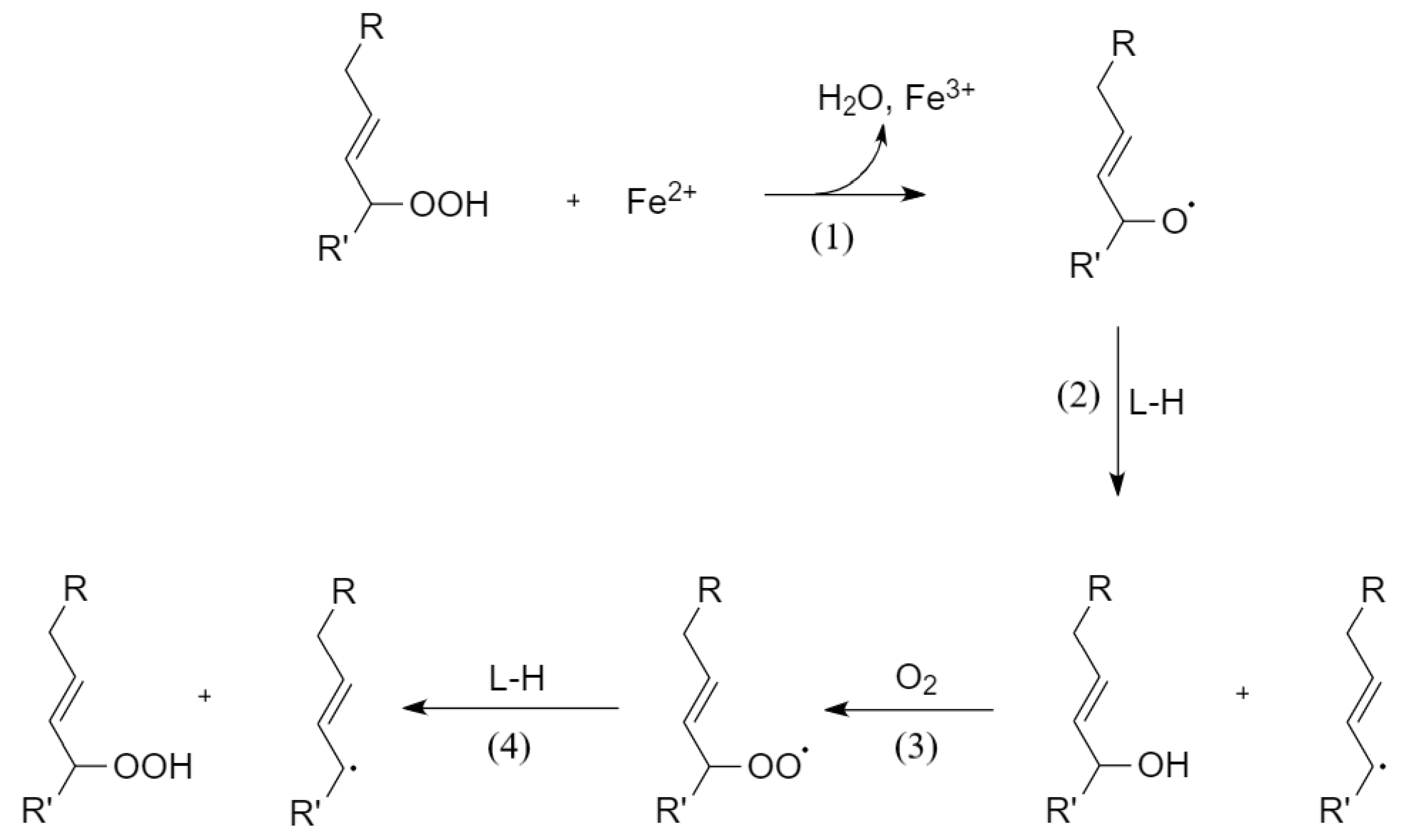
2.1. Lipid Peroxidation in Nephrolithiasis
2.2. Ferroptosis in Nephrolithiasis
2.3. Polyphenols Inhibit Lipid Peroxidation and Ferroptosis as Chelating Agents
3. Beneficial Effects of Polyphenols as Determined by Various In Vitro Models of Nephrolithiasis
3.1. Flavonoids
3.1.1. Quercetin
3.1.2. Catechins
3.1.3. Curcumin
3.1.4. Other Flavonoids
3.2. Phenolic Acids
3.3. Stilbenes (Resveratrol)
3.4. Various Polyphenol-Rich Plants and Compounds
4. Limitations of Current In Vitro Models of Nephrolithiasis Exploring Polyphenols
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Shah, J.; Whitfield, H.N. Urolithiasis through the ages. BJU Int. 2002, 89, 801–810. [Google Scholar] [CrossRef]
- Warli, S.M.; Mantiri, B.J.; Sihombing, B.; Siregar, G.P.; Prapiska, F.F. Nephrolithiasis-Associated Renal Cell Carcinoma in Patients Who Underwent Nephrectomy: A Single-Center Experience. World J. Oncol. 2023, 14, 94–100. [Google Scholar] [CrossRef]
- Chewcharat, A.; Curhan, G. Trends in the prevalence of kidney stones in the United States from 2007 to 2016. Urolithiasis 2021, 49, 27–39. [Google Scholar] [CrossRef]
- Skolarikos, A.; Neisius, J.H.; Petrik; Somani, B.; Tailly, T.; Gambaro, G.; Davis, N.F.; Geraghty, R.; Lombardo, R.; Tzelves, L. EAU Gidelines on Urolithiasis. 2023. Available online: https://uroweb.org/gidelines/urolithiasis (accessed on 20 April 2023).
- Stamatelou, K.; Goldfarb, D.S. Epidemiology of Kidney Stones. Healthcare 2023, 11, 424. [Google Scholar] [CrossRef]
- Ferraro, P.M.; Taylor, E.N.; Eisner, B.H.; Gambaro, G.; Rimm, E.B.; Mukamal, K.J.; Curhan, G.C. History of kidney stones and the risk of coronary heart disease. JAMA 2013, 310, 408–415. [Google Scholar] [CrossRef] [Green Version]
- Rule, A.D.; Roger, V.L.; Melton, L.J.I.; Bergstralh, E.J.; Li, X.; Peyser, P.A.; Krambeck, A.E.; Lieske, J.C. Kidney Stones Associate with Increased Risk for Myocardial Infarction. J. Am. Soc. Nephrol. 2010, 21, 1641–1644. [Google Scholar] [CrossRef] [Green Version]
- Rule, A.D.; Bergstralh, E.J.; Melton, L.J.I.; Li, X.; Weaver, A.L.; Lieske, J.C. Kidney Stones and the Risk for Chronic Kidney Disease. Clin. J. Am. Soc. Nephrol. 2009, 4, 804–811. [Google Scholar] [CrossRef] [Green Version]
- Taylor, E.N.; Feskanich, D.; Paik, J.M.; Curhan, G.C. Nephrolithiasis and Risk of Incident Bone Fracture. J. Urol. 2016, 195, 1482–1486. [Google Scholar] [CrossRef] [Green Version]
- Zeng, G.; Zhu, W.; Robertson, W.G.; Penniston, K.L.; Smith, D.; Pozdzik, A.; Tefik, T.; Prezioso, D.; Pearle, M.S.; Chew, B.H.; et al. International Alliance of Urolithiasis (IAU) guidelines on the metabolic evaluation and medical management of urolithiasis. Urolithiasis 2022, 51, 4. [Google Scholar] [CrossRef]
- Evan, A.P. Physiopathology and etiology of stone formation in the kidney and the urinary tract. Pediatr. Nephrol. 2010, 25, 831–841. [Google Scholar] [CrossRef] [Green Version]
- Petrović, A.; Kizivat, T.; Bilić Ćurčić, I.; Smolić, R.; Smolić, M. In Vitro Cell Culture Models of Hyperoxaluric States: Calcium Oxalate and Renal Epithelial Cell Interactions. Crystals 2021, 11, 735. [Google Scholar]
- Aggarwal, K.P.; Narula, S.; Kakkar, M.; Tandon, C. Nephrolithiasis: Molecular mechanism of renal stone formation and the critical role played by modulators. Biomed. Res. Int. 2013, 2013, 292953. [Google Scholar] [CrossRef] [Green Version]
- Mayans, L. Nephrolithiasis. Prim. Care Clin. Off. Pract. 2019, 46, 203–212. [Google Scholar] [CrossRef]
- Geraghty, R.M.; Davis, N.F.; Tzelves, L.; Lombardo, R.; Yuan, C.; Thomas, K.; Petrik, A.; Neisius, A.; Türk, C.; Gambaro, G.; et al. Best Practice in Interventional Management of Urolithiasis: An Update from the European Association of Urology Guidelines Panel for Urolithiasis 2022. Eur. Urol. Focus 2023, 9, 199–208. [Google Scholar] [CrossRef]
- Antonelli, J.A.; Maalouf, N.M.; Pearle, M.S.; Lotan, Y. Use of the National Health and Nutrition Examination Survey to calculate the impact of obesity and diabetes on cost and prevalence of urolithiasis in 2030. Eur. Urol. 2014, 66, 724–729. [Google Scholar] [CrossRef] [Green Version]
- Kizivat, T.; Smolić, M.; Marić, I.; Tolušić Levak, M.; Smolić, R.; Bilić Čurčić, I.; Kuna, L.; Mihaljević, I.; Včev, A.; Tucak-Zorić, S. Antioxidant Pre-Treatment Reduces the Toxic Effects of Oxalate on Renal Epithelial Cells in a Cell Culture Model of Urolithiasis. Int. J. Environ. Res. Public Health 2017, 14, 109. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.; Hasan, M.; Mahmood, Z. Antiurolithiatic plants: Multidimensional pharmacology. J. Pharmacogn. Phytochem. 2016, 5, 4–24. [Google Scholar]
- Yasir, F.; Wahab, A.-T.; Choudhary, M.I. Protective effect of dietary polyphenol caffeic acid on ethylene glycol-induced kidney stones in rats. Urolithiasis 2018, 46, 157–166. [Google Scholar] [CrossRef]
- Zhai, W.; Zheng, J.; Yao, X.; Peng, B.; Liu, M.; Huang, J.; Wang, G.; Xu, Y. Catechin prevents the calcium oxalate monohydrate induced renal calcium crystallization in NRK-52E cells and the ethylene glycol induced renal stone formation in rat. BMC Complement. Altern. Med. 2013, 13, 228. [Google Scholar] [CrossRef] [Green Version]
- Ghodasara, J.; Pawar, A.; Deshmukh, C.; Kuchekar, B. Inhibitory effect of rutin and curcumin on experimentally-induced calcium oxalate urolithiasis in rats. Pharmacogn. Res. 2010, 2, 388–392. [Google Scholar] [CrossRef] [Green Version]
- Noorafshan, A.; Karbalay-Doust, S.; Karimi, F. Diosmin Reduces Calcium Oxalate Deposition and Tissue Degeneration in Nephrolithiasis in Rats: A Stereological Study. Korean J. Urol. 2013, 54, 252–257. [Google Scholar]
- Dinnimath, B.M.; Jalalpure, S.S.; Patil, U.K. Antiurolithiatic activity of natural constituents isolated from Aerva lanata. J. Ayurveda Integr. Med. 2017, 8, 226–232. [Google Scholar] [CrossRef]
- Hong, S.H.; Lee, H.J.; Sohn, E.J.; Ko, H.S.; Shim, B.S.; Ahn, K.S.; Kim, S.H. Anti-nephrolithic potential of resveratrol via inhibition of ROS, MCP-1, hyaluronan and osteopontin in vitro and in vivo. Pharm. Rep. 2013, 65, 970–979. [Google Scholar] [CrossRef]
- Shakoor, H.; Feehan, J.; Apostolopoulos, V.; Platat, C.; Al Dhaheri, A.S.; Ali, H.I.; Ismail, L.C.; Bosevski, M.; Stojanovska, L. Immunomodulatory Effects of Dietary Polyphenols. Nutrients 2021, 13, 728. [Google Scholar] [CrossRef]
- Fraga, C.G.; Croft, K.D.; Kennedy, D.O.; Tomás-Barberán, F.A. The effects of polyphenols and other bioactives on human health. Food Funct 2019, 10, 514–528. [Google Scholar] [CrossRef] [Green Version]
- Di Lorenzo, C.; Colombo, F.; Biella, S.; Stockley, C.; Restani, P. Polyphenols and Human Health: The Role of Bioavailability. Nutrients 2021, 13, 273. [Google Scholar] [CrossRef]
- Yahfoufi, N.; Alsadi, N.; Jambi, M.; Matar, C. The Immunomodulatory and Anti-Inflammatory Role of Polyphenols. Nutrients 2018, 10, 1618. [Google Scholar] [CrossRef] [Green Version]
- Luca, S.V.; Macovei, I.; Bujor, A.; Miron, A.; Skalicka-Woźniak, K.; Aprotosoaie, A.C.; Trifan, A. Bioactivity of dietary polyphenols: The role of metabolites. Crit. Rev. Food Sci. Nutr. 2020, 60, 626–659. [Google Scholar] [CrossRef]
- Xiao, J. Stability of dietary polyphenols: It’s never too late to mend? Food Chem. Toxicol. 2018, 119, 3–5. [Google Scholar] [CrossRef]
- Shen, N.; Wang, T.; Gan, Q.; Liu, S.; Wang, L.; Jin, B. Plant flavonoids: Classification, distribution, biosynthesis, and antioxidant activity. Food Chem. 2022, 383, 132531. [Google Scholar] [CrossRef]
- Santos-Buelga, C.; González-Paramás, A.M.; Oludemi, T.; Ayuda-Durán, B.; González-Manzano, S. Plant phenolics as functional food ingredients. Adv. Food Nutr. Res. 2019, 90, 183–257. [Google Scholar] [CrossRef]
- Wang, Y.; Qi, H.; Liu, Y.; Duan, C.; Liu, X.; Xia, T.; Chen, D.; Piao, H.L.; Liu, H.X. The double-edged roles of ROS in cancer prevention and therapy. Theranostics 2021, 11, 4839–4857. [Google Scholar] [CrossRef]
- Aneklaphakij, C.; Saigo, T.; Watanabe, M.; Naake, T.; Fernie, A.R.; Bunsupa, S.; Satitpatipan, V.; Tohge, T. Diversity of Chemical Structures and Biosynthesis of Polyphenols in Nut-Bearing Species. Front. Plant Sci. 2021, 12, 642581. [Google Scholar] [CrossRef]
- Rudrapal, M.; Khairnar, S.J.; Khan, J.; Dukhyil, A.B.; Ansari, M.A.; Alomary, M.N.; Alshabrmi, F.M.; Palai, S.; Deb, P.K.; Devi, R. Dietary Polyphenols and Their Role in Oxidative Stress-Induced Human Diseases: Insights into Protective Effects, Antioxidant Potentials and Mechanism(s) of Action. Front. Pharmacol. 2022, 13, 806470. [Google Scholar] [CrossRef]
- Peerapen, P.; Thongboonkerd, V. Kidney Stone Prevention. Adv. Nutr. 2023, 14, 555–569. [Google Scholar] [CrossRef]
- Peerapen, P.; Thongboonkerd, V. Kidney stone proteomics: An update and perspectives. Expert Rev. Proteom. 2021, 18, 557–569. [Google Scholar] [CrossRef]
- Den Hartogh, D.J.; Tsiani, E. Health Benefits of Resveratrol in Kidney Disease: Evidence from In Vitro and In Vivo Studies. Nutrients 2019, 11, 1624. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Zhao, M.; Zhou, Y.; Wang, C.; Yuan, Y.; Li, L.; Bresette, W.; Chen, Y.; Cheng, J.; Lu, Y.; et al. Resveratrol exerts dose-dependent anti-fibrotic or pro-fibrotic effects in kidneys: A potential risk to individuals with impaired kidney function. Phytomedicine 2019, 57, 223–235. [Google Scholar] [CrossRef]
- Su, L.J.; Zhang, J.H.; Gomez, H.; Murugan, R.; Hong, X.; Xu, D.; Jiang, F.; Peng, Z.Y. Reactive Oxygen Species-Induced Lipid Peroxidation in Apoptosis, Autophagy, and Ferroptosis. Oxid. Med. Cell Longev. 2019, 2019, 5080843. [Google Scholar] [CrossRef] [Green Version]
- Schreiber, R.; Buchholz, B.; Kraus, A.; Schley, G.; Scholz, J.; Ousingsawat, J.; Kunzelmann, K. Lipid Peroxidation Drives Renal Cyst Growth. J. Am. Soc. Nephrol. 2019, 30, 228–242. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.; Hasan, M.M.; Khan, H.; Mahmood, Z.A.; Patel, S. The mechanistic insight of polyphenols in calcium oxalate urolithiasis mitigation. Biomed. Pharmacother. 2018, 106, 1292–1299. [Google Scholar] [CrossRef]
- Gasmi, A.; Mujawdiya, P.K.; Noor, S.; Lysiuk, R.; Darmohray, R.; Piscopo, S.; Lenchyk, L.; Antonyak, H.; Dehtiarova, K.; Shanaida, M.; et al. Polyphenols in Metabolic Diseases. Molecules 2022, 27, 6280. [Google Scholar] [CrossRef]
- Fan, X.; Fan, Z.; Yang, Z.; Huang, T.; Tong, Y.; Yang, D.; Mao, X.; Yang, M. Flavonoids-Natural Gifts to Promote Health and Longevity. Int. J. Mol. Sci. 2022, 23, 2176. [Google Scholar] [CrossRef]
- Li, J.; Cao, F.; Yin, H.L.; Huang, Z.J.; Lin, Z.T.; Mao, N.; Sun, B.; Wang, G. Ferroptosis: Past, present and future. Cell Death Dis. 2020, 11, 88. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Wang, B.; Yuan, S.; He, Q.; Jin, J. The Role of Ferroptosis in Acute Kidney Injury. Front. Mol. Biosci. 2022, 9, 951275. [Google Scholar] [CrossRef]
- Tang, D.; Chen, X.; Kang, R.; Kroemer, G. Ferroptosis: Molecular mechanisms and health implications. Cell Res. 2021, 31, 107–125. [Google Scholar] [CrossRef]
- Messerer, D.A.C.; Halbgebauer, R.; Nilsson, B.; Pavenstädt, H.; Radermacher, P.; Huber-Lang, M. Immunopathophysiology of trauma-related acute kidney injury. Nat. Rev. Nephrol 2021, 17, 91–111. [Google Scholar] [CrossRef]
- Lesjak, M.; Simin, N.; Srai, S.K.S. Can Polyphenols Inhibit Ferroptosis? Antioxidants 2022, 11, 150. [Google Scholar] [CrossRef]
- Hu, W.; Liang, K.; Zhu, H.; Zhao, C.; Hu, H.; Yin, S. Ferroptosis and Its Role in Chronic Diseases. Cells 2022, 11, 2040. [Google Scholar] [CrossRef]
- Xu, S.; Wu, B.; Zhong, B.; Lin, L.; Ding, Y.; Jin, X.; Huang, Z.; Lin, M.; Wu, H.; Xu, D. Naringenin alleviates myocardial ischemia/reperfusion injury by regulating the nuclear factor-erythroid factor 2-related factor 2 (Nrf2) /System xc-/ glutathione peroxidase 4 (GPX4) axis to inhibit ferroptosis. Bioengineered 2021, 12, 10924–10934. [Google Scholar] [CrossRef]
- Lin, C.H.; Tseng, H.F.; Hsieh, P.C.; Chiu, V.; Lin, T.Y.; Lan, C.C.; Tzeng, I.S.; Chao, H.N.; Hsu, C.C.; Kuo, C.Y. Nephroprotective Role of Chrysophanol in Hypoxia/Reoxygenation-Induced Renal Cell Damage via Apoptosis, ER Stress, and Ferroptosis. Biomedicines 2021, 9, 1283. [Google Scholar] [CrossRef]
- Liu, Y.; Wan, Y.; Jiang, Y.; Zhang, L.; Cheng, W. GPX4: The hub of lipid oxidation, ferroptosis, disease and treatment. Biochim. Et Biophys. Acta (BBA)-Rev. Cancer 2023, 1878, 188890. [Google Scholar] [CrossRef]
- He, Z.; Liao, W.; Song, Q.; Li, B.; Liu, J.; Xiong, Y.; Song, C.; Yang, S. Role of ferroptosis induced by a high concentration of calcium oxalate in the formation and development of urolithiasis. Int. J. Mol. Med. 2021, 47, 289–301. [Google Scholar] [CrossRef]
- Sanz, A.B.; Sanchez-Niño, M.D.; Ramos, A.M.; Ortiz, A. Regulated cell death pathways in kidney disease. Nat. Rev. Nephrol 2023, 19, 281–299. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, J. Ferroptosis, a Rising Force against Renal Fibrosis. Oxid. Med. Cell. Longev. 2022, 2022, 7686956. [Google Scholar] [CrossRef]
- Su, Y.; Liu, Z.; Xie, K.; Ren, Y.; Li, C.; Chen, W. Ferroptosis: A Novel Type of Cell Death in Male Reproduction. Genes 2022, 14, 43. [Google Scholar] [CrossRef]
- Stepanić, V.; Kučerová-Chlupáčová, M. Review and Chemoinformatic Analysis of Ferroptosis Modulators with a Focus on Natural Plant Products. Molecules 2023, 28, 475. [Google Scholar] [CrossRef]
- Singh, P.; Arif, Y.; Bajguz, A.; Hayat, S. The role of quercetin in plants. Plant. Physiol. Biochem. 2021, 166, 10–19. [Google Scholar] [CrossRef]
- Tao, H.; Zhao, Y.; Li, L.; He, Y.; Zhang, X.; Zhu, Y.; Hong, G. Comparative metabolomics of flavonoids in twenty vegetables reveal their nutritional diversity and potential health benefits. Food Res. Int. 2023, 164, 112384. [Google Scholar] [CrossRef]
- Oh, W.Y.; Ambigaipalan, P.; Shahidi, F. Quercetin and its ester derivatives inhibit oxidation of food, LDL and DNA. Food Chem. 2021, 364, 130394. [Google Scholar] [CrossRef]
- Wang, Y.; Quan, F.; Cao, Q.; Lin, Y.; Yue, C.; Bi, R.; Cui, X.; Yang, H.; Yang, Y.; Birnbaumer, L.; et al. Quercetin alleviates acute kidney injury by inhibiting ferroptosis. J. Adv. Res. 2021, 28, 231–243. [Google Scholar] [CrossRef]
- Linkermann, A.; Chen, G.; Dong, G.; Kunzendorf, U.; Krautwald, S.; Dong, Z. Regulated Cell Death in AKI. J. Am. Soc. Nephrol. 2014, 25, 2689–2701. [Google Scholar]
- Wu, X.; Wang, J.; Li, B.; Gong, M.; Cao, C.; Song, L.; Qin, L.; Wang, Y.; Zhang, Y.; Li, Y. Chlorogenic acid, rutin, and quercetin from Lysimachia christinae alleviate triptolide-induced multi-organ injury in vivo by modulating immunity and AKT/mTOR signal pathway to inhibit ferroptosis and apoptosis. Toxicol. Appl. Pharmacol. 2023, 467, 116479. [Google Scholar] [CrossRef]
- Martin-Sanchez, D.; Poveda, J.; Fontecha-Barriuso, M.; Ruiz-Andres, O.; Sanchez-Niño, M.D.; Ruiz-Ortega, M.; Ortiz, A.; Sanz, A.B. Targeting of regulated necrosis in kidney disease. Nefrología 2018, 38, 125–135. [Google Scholar] [CrossRef]
- Zhang, H.; Qi, R.; Mine, Y. The impact of oolong and black tea polyphenols on human health. Food Biosci. 2019, 29, 55–61. [Google Scholar] [CrossRef]
- Heber, D.; Zhang, Y.; Yang, J.; Ma, J.E.; Henning, S.M.; Li, Z. Green Tea, Black Tea, and Oolong Tea Polyphenols Reduce Visceral Fat and Inflammation in Mice Fed High-Fat, High-Sucrose Obesogenic Diets. J. Nutr. 2014, 144, 1385–1393. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.; Chen, Y.; Cheng, M.; Zhang, X.; Zheng, X.; Zhang, Z. The modulatory effect of polyphenols from green tea, oolong tea and black tea on human intestinal microbiota in vitro. J. Food Sci. Technol 2018, 55, 399–407. [Google Scholar] [CrossRef]
- Jeong, B.C.; Kim, B.S.; Kim, J.I.; Kim, H.H. Effects of green tea on urinary stone formation: An in vivo and in vitro study. J. Endourol. 2006, 20, 356–361. [Google Scholar] [CrossRef]
- Chacko, S.M.; Thambi, P.T.; Kuttan, R.; Nishigaki, I. Beneficial effects of green tea: A literature review. Chin. Med. 2010, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Nasrul, S.I.; Sehgal, A. Antilithogenic potential of green tea, oolong tea, and black tea. Pharmacogn. Res. 2020, 12, 92. [Google Scholar] [CrossRef]
- Higdon, J.V.; Frei, B. Tea catechins and polyphenols: Health effects, metabolism, and antioxidant functions. Crit. Rev. Food Sci. Nutr. 2003, 43, 89–143. [Google Scholar] [CrossRef]
- Kanlaya, R.; Thongboonkerd, V. Protective Effects of Epigallocatechin-3-Gallate from Green Tea in Various Kidney Diseases. Adv. Nutr. 2019, 10, 112–121. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Liang, Y.; Zhou, L. Natural products for kidney disease treatment: Focus on targeting mitochondrial dysfunction. Front. Pharmacol. 2023, 14, 1142001. [Google Scholar] [CrossRef]
- Liu, Y.; Bi, S.; Li, H.; Shi, J.; Xia, Y.; Niu, K.; Bai, S. Association between tea intake and hospitalized nephrolithiasis in Chinese adults: A case-control study. Front. Nutr. 2022, 9, 1014491. [Google Scholar] [CrossRef]
- Yunna, C.; Mengru, H.; Lei, W.; Weidong, C. Macrophage M1/M2 polarization. Eur. J. Pharmacol. 2020, 877, 173090. [Google Scholar] [CrossRef]
- Liu, Q.; Liu, Y.; Guan, X.; Wu, J.; He, Z.; Kang, J.; Tao, Z.; Deng, Y. Effect of M2 Macrophages on Injury and Apoptosis of Renal Tubular Epithelial Cells Induced by Calcium Oxalate Crystals. Kidney Blood Press Res. 2019, 44, 777–791. [Google Scholar] [CrossRef]
- Taguchi, K.; Okada, A.; Unno, R.; Hamamoto, S.; Yasui, T. Macrophage Function in Calcium Oxalate Kidney Stone Formation: A Systematic Review of Literature. Front. Immunol. 2021, 12, 673690. [Google Scholar] [CrossRef]
- Hu, Y.; Gu, J.; Lin, J.; Wang, Y.; Yang, F.; Yin, J.; Yu, Z.; Wu, S.; Lv, H.; Ji, X.; et al. (-)-Epigallocatechin-3-gallate (EGCG) modulates polarized macrophages to suppress M1 phenotype and promote M2 polarization in vitro and in vivo. J. Funct. Foods 2021, 87, 104743. [Google Scholar] [CrossRef]
- Kotha, R.R.; Luthria, D.L. Curcumin: Biological, Pharmaceutical, Nutraceutical, and Analytical Aspects. Molecules 2019, 24, 2930. [Google Scholar] [CrossRef] [Green Version]
- Carolina Alves, R.; Perosa Fernandes, R.; Fonseca-Santos, B.; Damiani Victorelli, F.; Chorilli, M. A Critical Review of the Properties and Analytical Methods for the Determination of Curcumin in Biological and Pharmaceutical Matrices. Crit. Rev. Anal. Chem. 2019, 49, 138–149. [Google Scholar] [CrossRef]
- Amalraj, A.; Pius, A.; Gopi, S.; Gopi, S. Biological activities of curcuminoids, other biomolecules from turmeric and their derivatives—A review. J. Tradit. Complement. Med. 2017, 7, 205–233. [Google Scholar] [CrossRef] [Green Version]
- Deng, L.; He, S.; Guo, N.; Tian, W.; Zhang, W.; Luo, L. Molecular mechanisms of ferroptosis and relevance to inflammation. Inflamm. Res. 2023, 72, 281–299. [Google Scholar] [CrossRef]
- Guerrero-Hue, M.; García-Caballero, C.; Palomino-Antolín, A.; Rubio-Navarro, A.; Vázquez-Carballo, C.; Herencia, C.; Martín-Sanchez, D.; Farré-Alins, V.; Egea, J.; Cannata, P.; et al. Curcumin reduces renal damage associated with rhabdomyolysis by decreasing ferroptosis-mediated cell death. FASEB J. 2019, 33, 8961–8975. [Google Scholar] [CrossRef]
- Abbas, S. Green Synthesis, Characterization and In-Vitro Bioactivities of Gold Nanoparticles Mediated by Turmeric Crude Extract and Curcumin. Ph.D. Thesis, Universiti Tun Hussein Onn Malaysia, Parit Raja, Malaysia, 2021. [Google Scholar]
- Jing, G.H.; Liu, Y.D.; Liu, J.N.; Jin, Y.S.; Yu, S.L.; An, R.H. Puerarin prevents calcium oxalate crystal-induced renal epithelial cell autophagy by activating the SIRT1-mediated signaling pathway. Urolithiasis 2022, 50, 545–556. [Google Scholar] [CrossRef]
- Hadar, A.; Gozes, I.; Gurwitz, D. Chapter 12-RGS2 and SIRT1 Link Renin Angiotensin Aldosterone System to Alzheimer’s Disease. In Neuroprotection in Alzheimer’s Disease; Illana, G., Ed.; Academic Press: Cambridge, MA, USA, 2017; pp. 239–251. [Google Scholar]
- Ding, T.; Zhao, T.; Li, Y.; Liu, Z.; Ding, J.; Ji, B.; Wang, Y.; Guo, Z. Vitexin exerts protective effects against calcium oxalate crystal-induced kidney pyroptosis in vivo and in vitro. Phytomedicine 2021, 86, 153562. [Google Scholar] [CrossRef]
- Alam, W.; Khan, H.; Shah, M.A.; Cauli, O.; Saso, L. Kaempferol as a Dietary Anti-Inflammatory Agent: Current Therapeutic Standing. Molecules 2020, 25, 4073. [Google Scholar] [CrossRef]
- Sharma, D.; Gondaliya, P.; Tiwari, V.; Kalia, K. Kaempferol attenuates diabetic nephropathy by inhibiting RhoA/Rho-kinase mediated inflammatory signalling. Biomed. Pharm. 2019, 109, 1610–1619. [Google Scholar] [CrossRef]
- Hyun, S.K.; Jung, H.A.; Chung, H.Y.; Choi, J.S. In vitro peroxynitrite scavenging activity of 6-hydroxykynurenic acid and other flavonoids fromGingko biloba yellow leaves. Arch. Pharmacal Res. 2006, 29, 1074–1079. [Google Scholar] [CrossRef]
- Lin, C.W.; Chen, P.N.; Chen, M.K.; Yang, W.E.; Tang, C.H.; Yang, S.F.; Hsieh, Y.S. Kaempferol reduces matrix metalloproteinase-2 expression by down-regulating ERK1/2 and the activator protein-1 signaling pathways in oral cancer cells. PLoS ONE 2013, 8, e80883. [Google Scholar] [CrossRef] [Green Version]
- Yuan, P.; Sun, X.; Liu, X.; Hutterer, G.; Pummer, K.; Hager, B.; Ye, Z.; Chen, Z. Kaempferol alleviates calcium oxalate crystal-induced renal injury and crystal deposition via regulation of the AR/NOX2 signaling pathway. Phytomedicine 2021, 86, 153555. [Google Scholar] [CrossRef]
- Ambursa, M.B.; Rahman, M.N.G.; Sulaiman, S.A.; Zakaria, A.D.; Mohamed Daud, M.A.; Zakaria, Z.; Zahari, Z.; Wong, M.P. An In vitro Study of Orthosiphon stamineus (Misai Kucing) Standardized Water Extract as a Chemolytic Agent in Urolithiasis. J. Pharm. Bioallied Sci. 2021, 13, 373–379. [Google Scholar] [CrossRef]
- Zhou, D.; Wu, Y.; Yan, H.; Shen, T.; Li, S.; Gong, J.; Li, G.; Mai, H.; Wang, D.; Tan, X. Gallic acid ameliorates calcium oxalate crystal-induced renal injury via upregulation of Nrf2/HO-1 in the mouse model of stone formation. Phytomedicine 2022, 106, 154429. [Google Scholar] [CrossRef]
- Sohgaura, A.K.; Bigoniya, P.; Shrivastava, B. In Vitro Antilithiatic Potential of Kalanchoe pinnata, Emblica officinalis, Bambusa nutans, and Cynodon dactylon. J. Pharm. Bioallied Sci. 2018, 10, 83–89. [Google Scholar] [CrossRef]
- Salehi, B.; Mishra, A.P.; Nigam, M.; Sener, B.; Kilic, M.; Sharifi-Rad, M.; Fokou, P.V.T.; Martins, N.; Sharifi-Rad, J. Resveratrol: A Double-Edged Sword in Health Benefits. Biomedicines 2018, 6, 91. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Xun, Y.; Zhang, J.; Hu, H.; Qin, B.; Wang, T.; Wang, S.; Li, C.; Lu, Y. Resveratrol Attenuates Oxalate-Induced Renal Oxidative Injury and Calcium Oxalate Crystal Deposition by Regulating TFEB-Induced Autophagy Pathway. Front. Cell Dev. Biol. 2021, 9, 638759. [Google Scholar] [CrossRef]
- Ye, Q.L.; Wang, D.M.; Wang, X.; Zhang, Z.Q.; Tian, Q.X.; Feng, S.Y.; Zhang, Z.H.; Yu, D.X.; Ding, D.M.; Xie, D.D. Sirt1 inhibits kidney stones formation by attenuating calcium oxalate-induced cell injury. Chem. Biol. Interact. 2021, 347, 109605. [Google Scholar] [CrossRef]
- Hewagama, S.P.; Hewawasam, R.P. Antiurolithiatic Potential of Three Sri Lankan Medicinal Plants by the Inhibition of Nucleation, Growth, and Aggregation of Calcium Oxalate Crystals In Vitro. Sci. World J. 2022, 2022, 8657249. [Google Scholar] [CrossRef]
- Guillén-Meléndez, G.A.; Soto-Domínguez, A.; Loera-Arias, M.J.; Castillo-Velázquez, U.; Villa-Cedillo, S.A.; Piña-Mendoza, E.I.; Estrada-Castillón, E.; Chávez-Montes, A.; González-Alcocer, A.; Becerra-Verdín, E.M.; et al. Effect of methanolic extract of Mimosa malacophylla A.Gray in vero and HEK-293 cell lines, and in the morphology of kidney and bladder of rats with induced urolithiasis. J. Ethnopharmacol. 2022, 297, 115552. [Google Scholar] [CrossRef]
- Li, S.; Macaringue, E.G.J.; Zhou, D.; Shi, P.; Tang, W.; Gong, J. Discovering inhibitor molecules for pathological crystallization of CaOx kidney stones from natural extracts of medical herbs. J. Ethnopharmacol. 2022, 284, 114733. [Google Scholar] [CrossRef]
- Moreno, K.G.T.; Gasparotto Junior, A.; Dos Santos, A.C.; Palozi, R.A.C.; Guarnier, L.P.; Marques, A.A.M.; Romão, P.V.M.; Lorençone, B.R.; Cassemiro, N.S.; Silva, D.B.; et al. Nephroprotective and antilithiatic activities of Costus spicatus (Jacq.) Sw.: Ethnopharmacological investigation of a species from the Dourados region, Mato Grosso do Sul State, Brazil. J. Ethnopharmacol. 2021, 266, 113409. [Google Scholar] [CrossRef]
- Ye, T.; Yang, X.; Liu, H.; Lv, P.; Lu, H.; Jiang, K.; Peng, E.; Ye, Z.; Chen, Z.; Tang, K. Theaflavin protects against oxalate calcium-induced kidney oxidative stress injury via upregulation of SIRT1. Int. J. Biol. Sci. 2021, 17, 1050–1060. [Google Scholar] [CrossRef]
- Yachi, L.; Bennis, S.; Aliat, Z.; Cheikh, A.; Idrissi, M.O.B.; Draoui, M.; Bouatia, M. In vitro litholytic activity of some medicinal plants on urinary stones. Afr. J. Urol. 2018, 24, 197–201. [Google Scholar] [CrossRef]
- Khan, S.R.; Canales, B.K. Unified theory on the pathogenesis of Randall’s plaques and plugs. Urolithiasis 2015, 43 (Suppl. S1), 109–123. [Google Scholar] [CrossRef] [Green Version]
- Pandey, K.B.; Rizvi, S.I. Plant polyphenols as dietary antioxidants in human health and disease. Oxid. Med. Cell. Longev. 2009, 2, 270–278. [Google Scholar] [CrossRef] [Green Version]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hefer, M.; Huskic, I.M.; Petrovic, A.; Raguz-Lucic, N.; Kizivat, T.; Gjoni, D.; Horvatic, E.; Udiljak, Z.; Smolic, R.; Vcev, A.; et al. A Mechanistic Insight into Beneficial Effects of Polyphenols in the Prevention and Treatment of Nephrolithiasis: Evidence from Recent In Vitro Studies. Crystals 2023, 13, 1070. https://doi.org/10.3390/cryst13071070
Hefer M, Huskic IM, Petrovic A, Raguz-Lucic N, Kizivat T, Gjoni D, Horvatic E, Udiljak Z, Smolic R, Vcev A, et al. A Mechanistic Insight into Beneficial Effects of Polyphenols in the Prevention and Treatment of Nephrolithiasis: Evidence from Recent In Vitro Studies. Crystals. 2023; 13(7):1070. https://doi.org/10.3390/cryst13071070
Chicago/Turabian StyleHefer, Marija, Ivana Mihin Huskic, Ana Petrovic, Nikola Raguz-Lucic, Tomislav Kizivat, Dominik Gjoni, Elizabeta Horvatic, Zarko Udiljak, Robert Smolic, Aleksandar Vcev, and et al. 2023. "A Mechanistic Insight into Beneficial Effects of Polyphenols in the Prevention and Treatment of Nephrolithiasis: Evidence from Recent In Vitro Studies" Crystals 13, no. 7: 1070. https://doi.org/10.3390/cryst13071070