
Awake Craniotomy for Gliomas in the Non-Dominant Right Hemisphere: A Comprehensive Review
 , , , and
, , , and 
Abstract
:Simple Summary
Abstract
1. Introduction
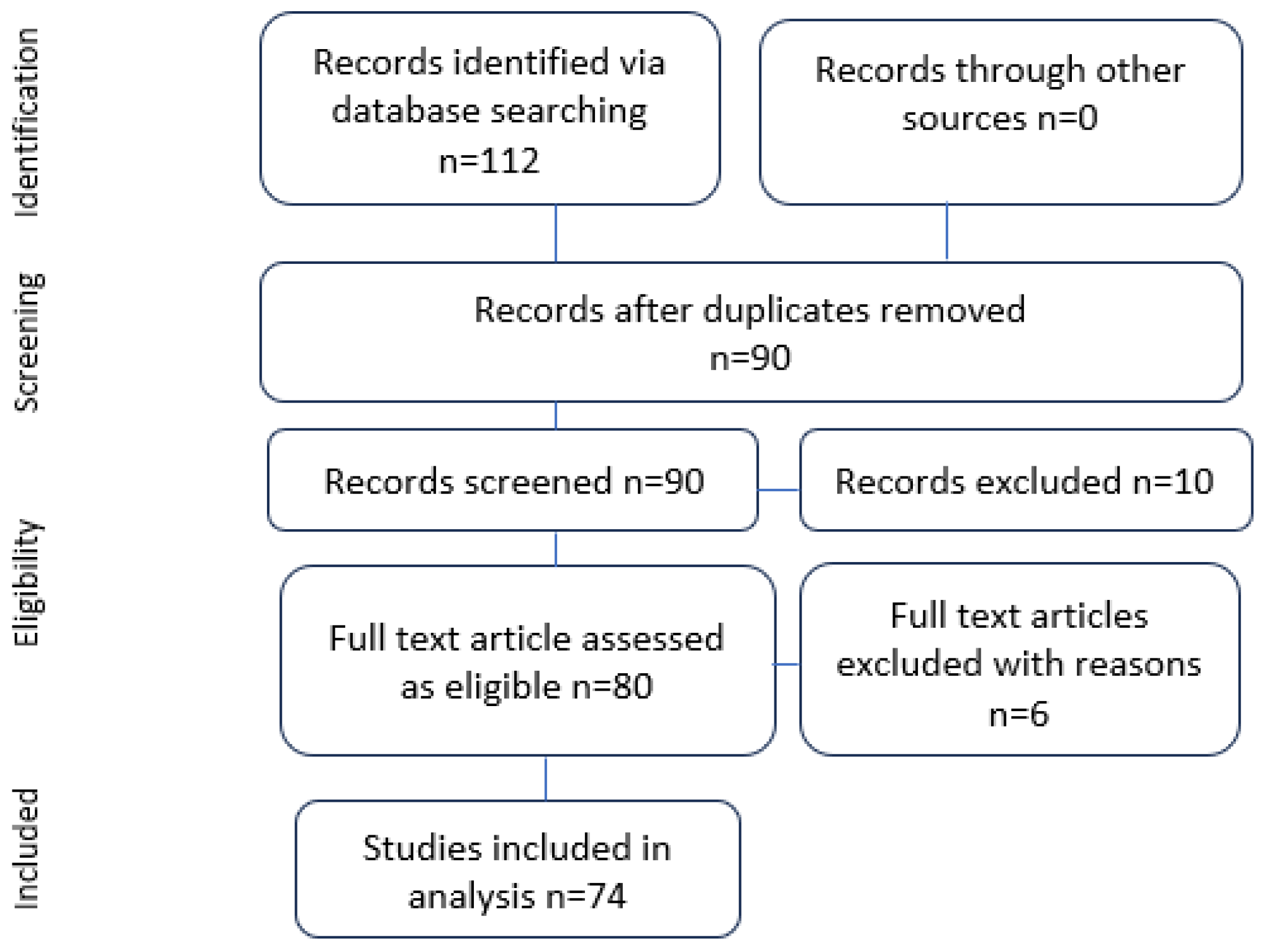
2. Materials and Methods
- Relevance to awake surgery in gliomas of the right cerebral hemisphere.
- Presentation of anatomical and surgical considerations.
- Discussion of indications for awake surgery in the right hemisphere.
- Exploration of tools and techniques used during intraoperative assessment.
- Anatomical considerations specific to the right hemisphere.
- Surgical techniques employed during awake surgery for right-hemispheric gliomas.
- Indications for utilizing awake surgery in the right cerebral hemisphere.
- Evaluation methods and tools for intraoperative functional assessment.
3. Results
3.1. Understanding Syndromes and Symptoms of Right-Hemispheric Lesions and Their Intraoperative Tests
3.1.1. Lesions on the Frontal Lobe near the Superior Frontal Gyrus Involving the Supplementary Motor Area (SMA): Assessment of Supplementary Motor Functions
3.1.2. Deep Frontal Lobe Lesions Involving the FAT: Assessment of Executive Functions
3.1.3. Lesions of the Medial Part of the Frontal Lobe Involving the Cingulate Gyrus: Assessment of Social Cognition
3.1.4. Lesions of the Temporoparietal Region: Assessment of Visuospatial Function
3.1.5. Lesions Localized Deep in the Basal Surface of the Right Occipito-Temporal Area, Involving ILF, IFOF, and SLF: Assessment of Visuospatial Cognition
3.1.6. Lesions Localized in Temporal Lobe and Insula: Assessing Emotional Prosody

{kind=link}
{kind=link}
| Functional Area | Gyrus | Responsible Subcortical Tract | Function | Deficit | Testing Methods | Awake Intraoperative Assessment | |
|---|---|---|---|---|---|---|---|
| 1 | Ventral frontal cortex (vPFC) | MFG IFG | SLF III SLF II IFOF | Visuospatial cognition | Somatoparaphrenia Anosognosia Unilateral neglect Allochiria | Line bisection test Alberts test [67] Catherine Bergego Scale (CBS) [62] Target cancellation test Clock face drawing Butterfly drawing | Line bisection test Target cancellation test |
| 2 | Temporoparietal junction (TPJ) | SMG, both MTG STG (posterior part) | IFOF Right UF + corticolimbic system with bilateral mvPFC and orbitofrontal cortex and precuneus | Visuospatial Social cognition empathy, TOM | Somatoparaphrenia Anosognosia Unilateral neglect Constructional apraxia Emotional dysprosody Undermentalizing (autistic) Overmentalizing (schizophrenic) accentuation | Line bisection test Alberts test CBS Benton Visual Retention Test [68] “Reading the mind in the eyes” test [53]. False belief vs. photo | Line bisection test Target cancellation test |
| 3 | Medial ventral prefrontal cortex (mvPFC) | Ant.Cingulate gyrus Gyrus rectus Medial SFG | Social cognition (empathy TOM) | “Mind blindness” Undermentalizing (autistic) Overmentalizing (schizophrenic) accentuation | “Reading the mind in the eyes” test. Strategic game Trait judgement Social animations Rational actions | Reading the Mind in the Eyes | |
| 4 | Facial network, temporal part. SMG, left insular area. | Bilateral FFG posterior STS IFG, orbitofrontal gyrus mvPFC61 anterior cingulate gyrus, gyrus rectus medial SFG | UF | Facial emotion recognition | Ekman’s face test Japan, Caucasian brief affect recognition test | Ekman’s faces | |
| 5 | Emotional prosody | IFG SMG rt STG | AF | Emotional prosody | Emotional dysprosody | Storytelling with an intonation or listening to a prosodic text with emotional background. | No intraoperative test documented in literature |
| 6 | Empathy | Bilateral mvPFC Bilateral TPJ STS paracingulate IFG, cingulate gyrus, and amygdala | UF | Showing empathy | Reading the Mind in the Eyes False belief vs. photograph Strategic game Trait judgement Social animations Rational actions | Reading the Mind in the Eyes Balanced Emotional Empathy Scale (BEES) | |
| 7 | Theory of mind | Bilateral mvPFC Bilateral TPJ STS Lat orbitofrontal gyrus MFG, cuneus precuneus, and STG | Corticolimbic system | Theory of mind | “Mind blindness” Undermentalizing (autistic) [53,55] Overmentalizing (schizophrenic) accentuation |
4. Discussion
4.1. Direct Electrical Stimulation (DES)
4.1.1. Stimulation Parameters
4.1.2. Site Selection Criteria
4.1.3. Protocols for Patient Safety
4.2. Limitations of Current Studies and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Witt Hamer, P.C.; Robles, S.G.; Zwinderman, A.H.; Duffau, H.; Berger, M.S. Impact of intraoperative stimulation brain mapping on glioma surgery outcome: A meta-analysis. J. Clin. Oncol. 2012, 30, 2559–2565. [Google Scholar] [CrossRef]
- Papagno, C.; Pisoni, A.; Mattavelli, G.; Casarotti, A.; Comi, A.; Fumagalli, F.; Vernice, M.; Fava, E.; Riva, M.; Bello, L. Specific disgust processing in the left insula: New evidence from direct electrical stimulation. Neuropsychologia 2016, 84, 29–35. [Google Scholar] [CrossRef]
- Duffau, H.; Denvil, D.; Capelle, L. Absence of movement disorders after surgical resection of glioma invading the right striatum. J. Neurosurg. 2002, 97, 363–369. [Google Scholar] [CrossRef]
- Keles, G.E.; Anderson, B.; Berger, M.S. The effect of extent of resection on time to tumor progression and survival in patients with glioblastoma multiforme of the cerebral hemisphere. Surg. Neurol. 1999, 52, 371–379. [Google Scholar] [CrossRef]
- Keles, G.E.; Chang, E.F.; Lamborn, K.R.; Tihan, T.; Chang, C.J.; Chang, S.M.; Berger, M.S. Volumetric extent of resection and residual contrast enhancement on initial surgery as predictors of outcome in adult patients with hemispheric anaplastic astrocytoma. J. Neurosurg. 2006, 105, 34–40. [Google Scholar] [CrossRef]
- McGirt, M.J.; Chaichana, K.L.; Gathinji, M.; Attenello, F.J.; Than, K.; Olivi, A.; Weingart, J.D.; Brem, H.; redo Quiñones-Hinojosa, A. Independent association of extent of resection with survival in patients with malignant brain astrocytoma: Clinical article. J. Neurosurg. 2009, 110, 156–162. [Google Scholar] [CrossRef]
- Lacroix, M.; Abi-Said, D.; Fourney, D.R.; Gokaslan, Z.L.; Shi, W.; DeMonte, F.; Lang, F.F.; McCutcheon, I.E.; Hassenbusch, S.J.; Holland, E.; et al. A multivariate analysis of 416 patients with glioblastoma multiforme: Prognosis, extent of resection, and survival. J. Neurosurg. 2001, 95, 190–198. [Google Scholar] [CrossRef]
- Lamborn, K.R.; Chang, S.M.; Prados, M.D. Prognostic factors for survival of patients with glioblastoma: Recursive partitioning analysis. Neuro Oncol. 2004, 6, 227–235. [Google Scholar] [CrossRef]
- Jeremić, B.; Grulicić, D.; Samardzić, M.; Antunović, V.; Joksimović, M.; Lj, D.; Milicić, B.; Nikolić, N. The effect of extent of tumor resection on the outcome of combined therapy in patients with glioblastoma multiforme. Srp. Arh. Celok. Lek. 1997, 125, 93–98. [Google Scholar]
- Sanai, N.; Polley, M.Y.; McDermott, M.W.; Parsa, A.T.; Berger, M.S. An extent of resection threshold for newly diagnosed glioblastomas: Clinical article. J. Neurosurg. 2011, 115, 3–8. [Google Scholar] [CrossRef]
- Smith, J.S.; Chang, E.F.; Lamborn, K.R.; Chang, S.M.; Prados, M.D.; Cha, S.; Tihan, T.; VandenBerg, S.; McDermott, M.W.; Berger, M.S. Role of extent of resection in the long-term outcome of low-grade hemispheric gliomas. J. Clin. Oncol. 2008, 26, 1338–1345. [Google Scholar] [CrossRef]
- Stummer, W.; Reulen, H.J.; Meinel, T.; Pichlmeier, U.; Schumacher, W.; Tonn, J.C.; Rohde, V.; Oppel, F.; Turowski, B.; Woiciechowsky, C.; et al. Extent of resection and survival in glioblastoma multiforme: Identification of and adjustment for bias. Neurosurgery 2008, 62, 564–576. [Google Scholar] [CrossRef]
- Ushio, Y.; Kochi, M.; Hamada, J.I.; Kai, Y.; Nakamura, H. Effect of surgical removal on survival and quality of life in patients with supratentorial glioblastoma. Neurol. Med. Chir. 2005, 45, 454. [Google Scholar] [CrossRef]
- Vecht, C.J.; Avezaat, C.J.J.; Van Putten, W.L.J.; Eijkenbom, W.M.H.; Stefanko, S.Z. The influence of the extent of surgery on the neurological function and survival in malignant glioma. A retrospective analysis in 243 patients. J. Neurol. Neurosurg. Psychiatry 1990, 53, 466. [Google Scholar] [CrossRef]
- Charras, P.; Herbet, G.; Deverdun, J.; De Champfleur, N.M.; Duffau, H.; Bartolomeo, P.; Bonnetblanc, F. Functional reorganization of the attentional networks in low-grade glioma patients: A longitudinal study. Cortex 2015, 63, 27–41. [Google Scholar] [CrossRef]
- Conner, A.K.; Glenn, C.; Burks, J.D.; McCoy, T.; Bonney, P.A.; Chema, A.A.; Case, J.L.; Brunner, S.; Baker, C.; Sughrue, M.; et al. The use of the target cancellation task to identify eloquent visuospatial regions in awake craniotomies: Technical note. Cureus 2016, 8, e883. [Google Scholar] [CrossRef]
- Fried, I.; Mateer, C.; Ojemann, G.; Wohns, R.; Fedio, P. Organization of visuospatial functions in human cortex. Evidence from electrical stimulation. Brain J. Neurol. 1982, 105 Pt 2, 349–371. [Google Scholar] [CrossRef]
- Giussani, C.; Pirillo, D.; Roux, F.E. Mirror of the soul: A cortical stimulation study on recognition of facial emotions. J. Neurosurg. 2010, 112, 520–527. [Google Scholar] [CrossRef]
- Kitabayashi, T.; Nakada, M.; Kinoshita, M.; Sakurai, H.; Kobayashi, S.; Okita, H.; Nanbu, Y.; Hayashi, Y.; Hamada, J. Awake surgery with line bisection task for two cases of parietal glioma in the non-dominant hemisphere. No Shinkei Geka 2012, 40, 1087–1093. (In Japanese) [Google Scholar]
- Kleinman, J.T.; Sepkuty, J.P.; Hillis, A.E.; Lenz, F.A.; Heidler-Gary, J.; Gingis, L.; Crone, N.E. Spatial neglect during electrocortical stimulation mapping in the right hemisphere. Epilepsia 2007, 48, 2365–2368. [Google Scholar] [CrossRef]
- Manning, L.; Halligan, P.W.; Marshall, J.C. Individual variation in line bisection: A study of normal subjects with application to the interpretation of visual neglect. Neuropsychologia 1990, 28, 647–655. [Google Scholar] [CrossRef]
- Mazerand, E.; Le Renard, M.; Hue, S.; Lemée, J.M.; Klinger, E.; Menei, P. Intraoperative subcortical electrical mapping of the optic tract in awake surgery using a virtual reality headset. World Neurosurg. 2017, 97, 424–430. [Google Scholar] [CrossRef]
- Plummer, P.; Morris, M.E.; Dunai, J. Assessment of unilateral neglect. Phys. Ther. 2003, 83, 732–740. [Google Scholar] [CrossRef]
- Rorden, C.; Fruhmann Berger, M.; Karnath, H.O. Disturbed line bisection is associated with posterior brain lesions. Brain Res. 2006, 1080, 17–25. [Google Scholar] [CrossRef]
- Roux, F.E.; Dufor, O.; Lauwers-Cances, V.; Boukhatem, L.; Brauge, D.; Draper, L.; Lotterie, J.A.; Démonet, J.F. Electrostimulation mapping of spatial neglect. Neurosurgery 2011, 69, 1218–1231. [Google Scholar] [CrossRef]
- Sallard, E.; Duffau, H.; Bonnetblanc, F. Ultra-fast recovery from right neglect after “awake surgery” for slow-growing tumor invading the left parietal area. Neurocase 2012, 18, 80–90. [Google Scholar] [CrossRef]
- Schenkenberg, T.; Bradford, D.C.; Ajax, E.T. Line bisection and unilateral visual neglect in patients with neurologic impairment. Neurology 1980, 30, 509–517. [Google Scholar] [CrossRef]
- Talacchi, A.; Squintani, G.M.; Emanuele, B.; Tramontano, V.; Santini, B.; Savazzi, S. Intraoperative cortical mapping of visuospatial functions in parietal low-grade tumors: Changing perspectives of neurophysiological mapping. Neurosurg. Focus 2013, 34, E4. [Google Scholar] [CrossRef]
- Vallar, G.; Bello, L.; Bricolo, E.; Castellano, A.; Casarotti, A.; Falini, A.; Riva, M.; Fava, E.; Papagno, C. Cerebral correlates of visuospatial neglect: A direct cerebral stimulation study. Hum. Brain Mapp. 2014, 35, 1334–1350. [Google Scholar] [CrossRef]
- Vilasboas, T.; Herbet, G.; Duffau, H. Challenging the myth of right nondominant hemisphere: Lessons from corticosubcortical stimulation mapping in awake surgery and surgical implications. World Neurosurg. 2017, 103, 449–456. [Google Scholar] [CrossRef]
- Yagmurlu, K.; Middlebrooks, E.H.; Tanriover, N.; Rhoton, A.L. Fiber tracts of the dorsal language stream in the human brain. J. Neurosurg. 2016, 124, 1396–1405. [Google Scholar] [CrossRef]
- Hartwigsen, G.; Saur, D. Neuroimaging of stroke recovery from aphasia-insights into plasticity of the human language network. NeuroImage 2019, 190, 14–31. [Google Scholar] [CrossRef]
- Dick, A.S.; Bernal, B.; Tremblay, P. The Language Connectome: New Pathways, New Concepts. Neurosci. 2014, 20, 453–467. [Google Scholar] [CrossRef]
- Duffau, H. Lessons from brain mapping in surgery for low-grade glioma: Insights into associations between tumor and brain plasticity. Lancet Neurol. 2005, 4, 476–486. [Google Scholar] [CrossRef]
- Duffau, H.; Sichez, J.P.; Lehéricy, S. Intraoperative unmasking of brain redundant motor sites during resection of a precentral angioma: Evidence using direct cortical stimulation. Ann. Neurol. 2000, 47, 132–135. [Google Scholar] [CrossRef]
- Krainik, A.; Duffau, H.; Capelle, L.; Cornu, P.; Boch, A.L.; Mangin, J.F.; Le Bihan, D.; Marsault, C.; Chiras, J.; Lehéricy, S. Role of the healthy hemisphere in recovery after resection of the supplementary motor area. Neurology 2004, 62, 1323–1332. [Google Scholar] [CrossRef]
- Blanshard, H.J.; Chung, F.; Manninen, P.H.; Taylor, M.D.; Bernstein, M. Awake craniotomy for removal of intracranial tumor: Considerations for early discharge. Anesth Analg 2001, 92, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Beez, T.; Boge, K.; Wager, M.; Whittle, I.; Fontaine, D.; Spena, G.; Braun, S.; Szelényi, A.; Bello, L.; Duffau, H.; et al. Tolerance of awake surgery for glioma: A prospective European low-grade glioma network multicenter study. Acta Neurochir. 2013, 155, 1301–1308. [Google Scholar] [CrossRef] [PubMed]
- Gharabaghi, A.; Kunath, F.; Erb, M.; Saur, R.; Heckl, S.; Tatagiba, M.; Grodd, W.; Karnath, H.O. Perisylvian white matter connectivity in the human right hemisphere. BMC Neurosci. 2009, 10, 15. [Google Scholar] [CrossRef] [PubMed]
- Ruis, C. Monitoring cognition during awake brain surgery in adults: A systematic review. J. Clin. Exp. Neuropsychol. 2018, 40, 1081–1104. [Google Scholar] [CrossRef] [PubMed]
- Duffau, H.; Lopes, M.; Arthuis, F.; Bitar, A.; Sichez, J.P.; Van Effenterre, R.; Capelle, L. Contribution of intraoperative electrical stimulations in surgery of low-grade gliomas: A comparative study between two series without (1985–96) and with (1996–2003) functional mapping in the same institution. J. Neurol. Neurosurg. Psychiatry 2005, 76, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Kourtidou, E.; Kasselimis, D.; Angelopoulou, G.; Karavasilis, E.; Velonakis, G.; Kelekis, N.; Zalonis, I.; Evdokimidis, I.; Potagas, C.; Petrides, M. The Role of the Right Hemisphere White Matter Tracts in Chronic Aphasic Patients After Damage of the Language Tracts in the Left Hemisphere. Front. Hum. Neurosci. 2021, 15, 635750. [Google Scholar] [CrossRef]
- Gallet, C.; Clavreul, A.; Bernard, F.; Menei, P.; Lemée, J.M. Frontal aslant tract in the non-dominant hemisphere: A systematic review of anatomy, functions, and surgical applications. Front. Neuroanat. 2022, 16, 1025866. [Google Scholar] [CrossRef]
- Rech, F.; Herbet, G.; Moritz-Gasser, S.; Duffau, H. Disruption of bimanual movement by unilateral subcortical stimulation. Hum. Brain Mapp. 2014, 35, 3439–3445. [Google Scholar] [CrossRef]
- Kinoshita, M.; de Champfleur, N.M.; Deverdun, J.; Moritz-Gasser, S.; Herbet, G.; Duffau, H. Role of fronto-striatal tract and frontal aslant tract in movement and speech: An axonal mapping study. Brain Struct. Funct. 2015, 220, 3399–3412. [Google Scholar] [CrossRef]
- Budisavljevic, S.; Dell’Acqua, F.; Djordjilovic, V.; Miotto, D.; Motta, R.; Castiello, U. The role of the frontal aslant tract and premotor connections in visually guided hand movements. Neuroimage 2017, 146, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Rech, F.; Herbet, G.; Moritz-Gasser, S.; Duffau, H. Somatotopic organization of the white matter tracts underpinning motor control in humans: An electrical stimulation study. Brain Struct. Funct. 2016, 221, 3743–3753. [Google Scholar] [CrossRef] [PubMed]
- Godefroy, O.; Azouvi, P.; Robert, P.; Roussel, M.; LeGall, D.; Meulemans, T. Dysexecutive syndrome: Diagnostic criteria and validation study. Ann. Neurol. 2010, 68, 855–864. [Google Scholar] [CrossRef]
- Bernard, F.; Lemée, J.M.; Minassian, A.T.; Menei, P. Right Hemisphere Cognitive Functions: From Clinical and Anatomic Bases to Brain Mapping During Awake Craniotomy Part I: Clinical and Functional Anatomy. World Neurosurg. 2018, 118, 348–359. [Google Scholar] [CrossRef]
- Herbet, G.; Lafargue, G.; Duffau, H. The dorsal cingulate cortex as a critical gateway in the network supporting conscious awareness. Brain 2016, 139, e23. [Google Scholar] [CrossRef]
- Della Puppa, A.; De Pellegrin, S.; d’Avella, E.; Gioffrè, G.; Munari, M.; Saladini, M.; Salillas, E.; Scienza, R.; Semenza, C. Right parietal cortex and calculation processing: Intraoperative functional mapping of multiplication and addition in patients affected by a brain tumor. J. Neurosurg. 2013, 119, 1107–1111. [Google Scholar] [CrossRef] [PubMed]
- Gainotti, G. The Role of the Right Hemisphere in Emotional and Behavioral Disorders of Patients With Fronto-temporal Lobar Degeneration: An Updated Review. Front. Aging Neurosci. 2019, 11, 55. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Wheelwright, S.; Hill, J.; Raste, Y. The “Reading the Mind in the Eyes’’ test revised version: A study with normal adults, and adults with Asperger syndrome or high-functioning autism. J. Child Psychol. Psychiatry 2001, 42, 241–251. [Google Scholar] [CrossRef]
- Prat-Acín, R. Intraoperative brain mapping of language, cognitive functions, and social cognition in awake surgery of low-grade gliomas located in the right non-dominant hemisphere. Clin. Neurol. Neurosurg. 2020, 200, 106363. [Google Scholar] [CrossRef]
- Chenausky, K.; Kernbach, J.; Norton, A.; Schlaug, G. White matter integrity and treatment-based change in speech performance in minimally verbal children with autism spectrum disorder. Front. Hum. Neurosci. 2017, 11, 175. [Google Scholar] [CrossRef]
- Gras-Combes, G.; Moritz-Gasser, S.; Herbet, G.; Duffau, H. Intraoperative subcortical electrical mapping of optic radiations in awake surgery for glioma involving visual pathways. J. Neurosurg. 2012, 117, 466–473. [Google Scholar] [CrossRef]
- Geng, J.J.; Vossel, S. Re-evaluating the role of TPJ in attentional control: Contextual updating? Neurosci. Biobehav. Rev. 2013, 37, 2608–2620. [Google Scholar] [CrossRef]
- Snell, R.S. Clinical Neuroanatomy, 7th ed.; Wolter-Kluwer: Hong Kong, China; Lippincott William and Wilkins: Philadephia, PA, USA, 2010. [Google Scholar]
- Martino, J.; De Witt Hamer, P.C.; Berger, M.S.; Lawton, M.T.; Arnold, C.M.; de Lucas, E.M.; Duffau, H. Analysis of the subcomponents and cortical terminations of the perisylvian superior longitudinal fasciculus: A fiber dissection and DTI tractography study. Brain Struct. Funct. 2013, 218, 105–121. [Google Scholar] [CrossRef] [PubMed]
- Rech, F.; Duffau, H. Beyond Avoiding Hemiplegia after Glioma Surgery: The Need to Map Complex Movement in Awake Patient to Preserve Conation. Cancers 2023, 15, 1528. [Google Scholar] [CrossRef]
- Marques, C.L.S.; Souza, J.T.D.; Gonçalves, M.G.; Silva, T.R.D.; Costa, R.D.M.D.; Modolo, G.P.; Corrente, J.E.; Bazan, R.; Luvizutto, G.J. Validation of the Catherine Bergego Scale in patients with unilateral spatial neglect after stroke. Dement. Neuropsychol. 2019, 13, 82–88. [Google Scholar] [CrossRef]
- Arena, R.; Gainotti, G. Constructional apraxia and Visuoperceptive Disabilities in Relation to Laterality of Cerebral Lesions. Cortex 1978, 14, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Duffau, H.; Leroy, M.; Gatignol, P. Cortico-subcortical organization of language networks in the right hemisphere: An electrostimulation study in left-handers. Neuropsychologia 2008, 46, 3197–3209. [Google Scholar] [CrossRef]
- Sarubbo, S.; de Benedictis, A.; Merler, S.; Mandonnet, E.; Balbi, S.; Granieri, E.; Duffau, H. Towards a functional atlas of human white matter. Hum. Brain Mapp. 2015, 36, 3117–3136. [Google Scholar] [CrossRef] [PubMed]
- Herbet, G.; Moritz-Gasser, S.; Duffau, H. Direct evidence for the contributive role of the right inferior fronto-occipital fasciculus in non-verbal semantic cognition. Brain Struct. Funct. 2016, 222, 1597–1610. [Google Scholar] [CrossRef]
- Fernandez Coello, A.; Moritz-Gasser, S.; Martino, J.; Matsuda, A.; Duffau, H. Selection of intraoperative tasks for awake mapping based on relationships between tumor location and functional networks. J. Neurosurg. 2013, 119, 1380–1394. [Google Scholar] [CrossRef]
- Oliveira, F.F.; Marin SM, C.; Bertolucci, P.H.F. Communicating with the non-dominant hemisphere: Implications for neurological rehabilitation. Neural Regen. Res. 2013, 8, 1236–1246. [Google Scholar] [CrossRef]
- Albert, M.L. A simple test of visual neglect. Neurology 1973, 23, 658. [Google Scholar] [CrossRef]
- Wiedemayer, H.; Sandalcioglu, I.E.; Armbruster, W.; Regel, J.; Schaefer, H.; Stolke, D. False negative findings in intraoperative SEP monitoring: Analysis of 658 consecutive neurosurgical cases and review of published reports. J. Neurol. Neurosurg. Psychiatry 2004, 75, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Duffau, H. A two-level model of interindividual anatomo-functional variability of the brain and its implications for neurosurgery. Cortex 2017, 86, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Krainik, A.; Lehéricy, S.; Duffau, H.; Vlaicu, M.; Poupon, F.; Capelle, L.; Cornu, P.; Clemenceau, S.; Sahel, M.; Valery, C.; et al. Role of the supplementary motor area in motor deficit following medial frontal lobe surgery. Neurology 2001, 57, 871–878. [Google Scholar] [CrossRef]
- Magnani, M.; Rustici, A.; Zoli, M.; Tuleasca, C.; Chaurasia, B.; Franceschi, E.; Tonon, C.; Lodi, R.; Conti, A. Connectome-Based Neurosurgery in Primary Intra-Axial Neoplasms: Beyond the Traditional Modular Conception of Brain Architecture for the Preservation of Major Neurological Domains and Higher-Order Cognitive Functions. Life 2024, 14, 136. [Google Scholar] [CrossRef]
- De Witte, E.; Satoer, D.; Robert, E.; Colle, H.; Verheyen, S.; Visch-Brink, E.; Mariën, P. The Dutch linguistic intraoperative protocol: A valid linguistic approach to awake brain surgery. Brain Lang. 2015, 140, 35–48. [Google Scholar] [CrossRef] [PubMed]
- Peng, G.; Wang, W.S. Hemisphere lateralization is influenced by bilingual status and composition of words. Neuropsychologia 2011, 49, 1981–1986. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Relkin, N.R.; Lee, K.M.; Hirsch, J. Distinct cortical areas associated with native and second languages. Nature 1997, 388, 171–174. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mamadaliev, D.M.; Saito, R.; Motomura, K.; Ohka, F.; Scalia, G.; Umana, G.E.; Conti, A.; Chaurasia, B. Awake Craniotomy for Gliomas in the Non-Dominant Right Hemisphere: A Comprehensive Review. Cancers 2024, 16, 1161. https://doi.org/10.3390/cancers16061161
Mamadaliev DM, Saito R, Motomura K, Ohka F, Scalia G, Umana GE, Conti A, Chaurasia B. Awake Craniotomy for Gliomas in the Non-Dominant Right Hemisphere: A Comprehensive Review. Cancers. 2024; 16(6):1161. https://doi.org/10.3390/cancers16061161
Chicago/Turabian StyleMamadaliev, Dilshod Muhammadvalievich, Ryuta Saito, Kazuya Motomura, Fumiharu Ohka, Gianluca Scalia, Giuseppe Emmanuele Umana, Alfredo Conti, and Bipin Chaurasia. 2024. "Awake Craniotomy for Gliomas in the Non-Dominant Right Hemisphere: A Comprehensive Review" Cancers 16, no. 6: 1161. https://doi.org/10.3390/cancers16061161