
A Validated Methodological Approach to Prove the Safety of Clinical Electromagnetic Induction Systems in Magnetic Hyperthermia

 , , ,
, , ,  , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Coil Simulations
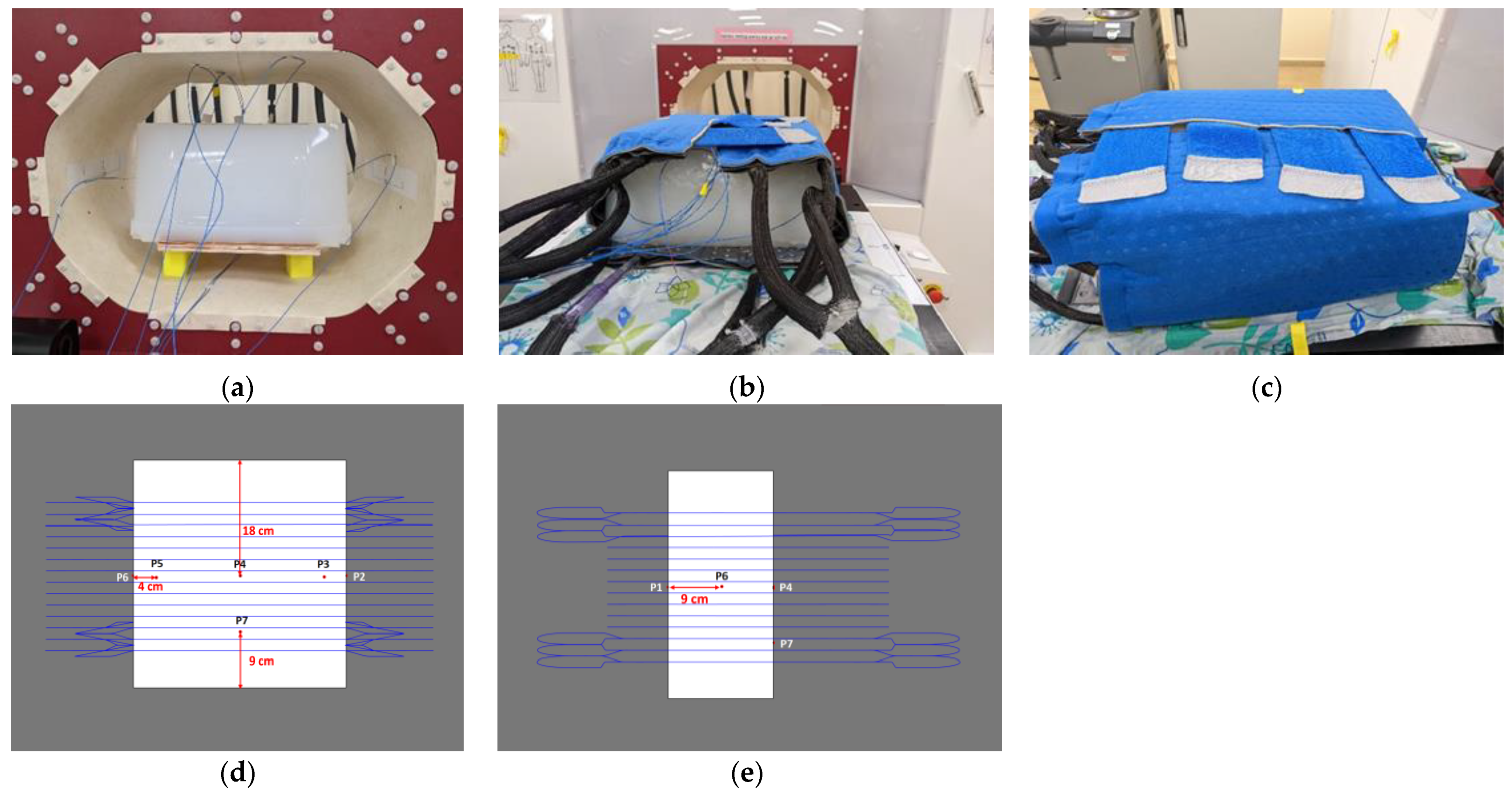
2.2. Agar Phantom Simulations
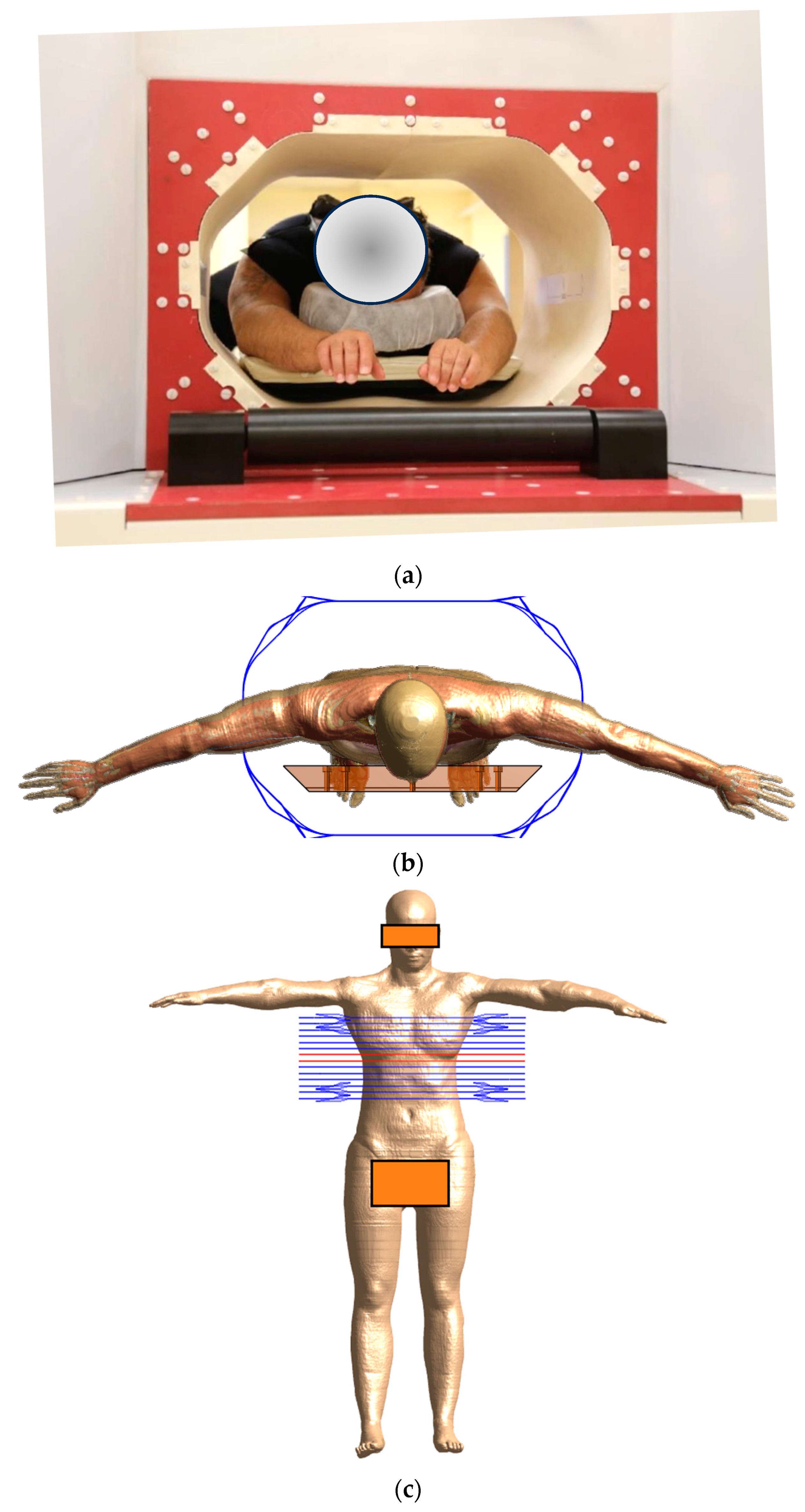
2.3. Human Phantom Simulations
3. Results
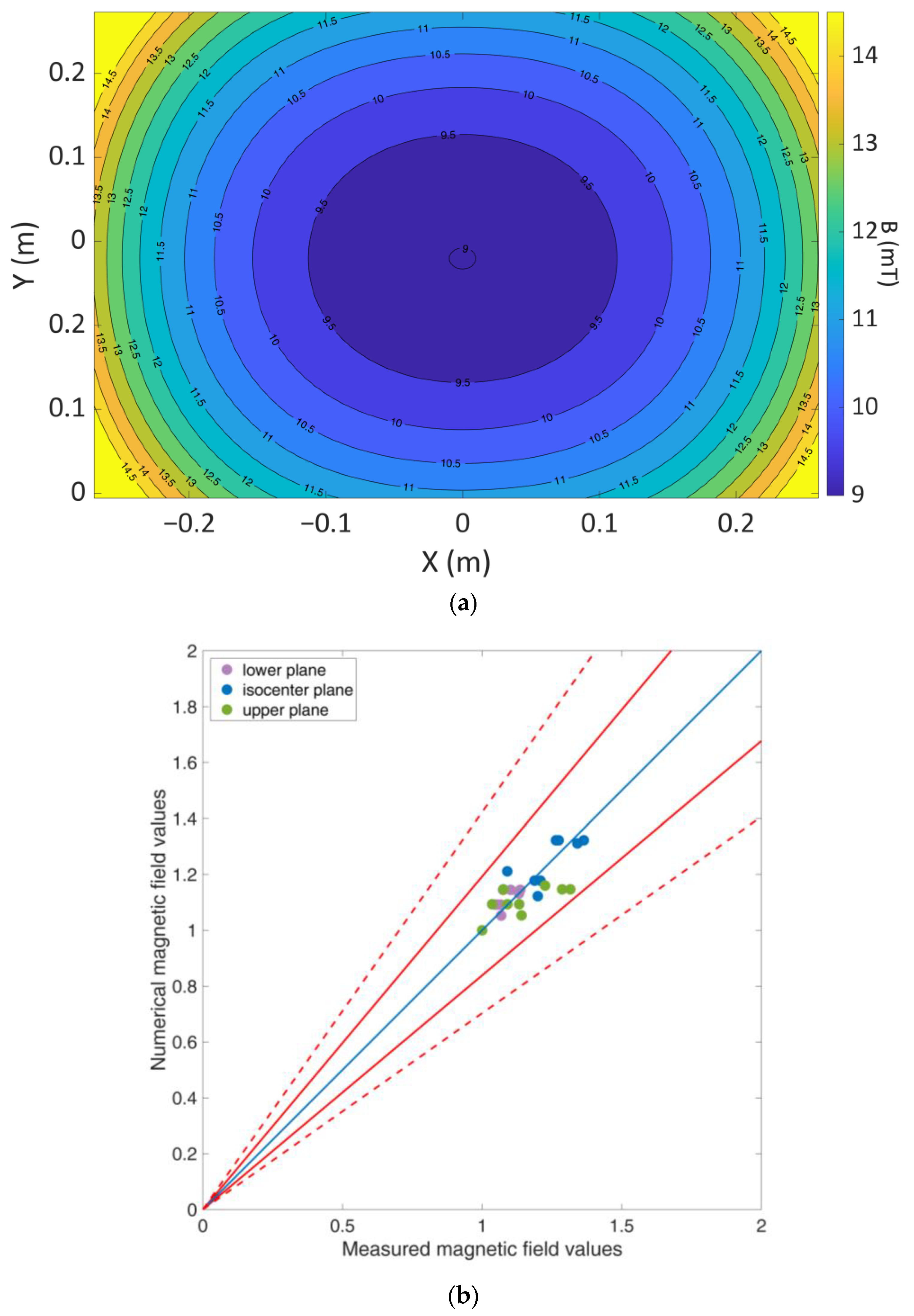
3.1. Coil Validation
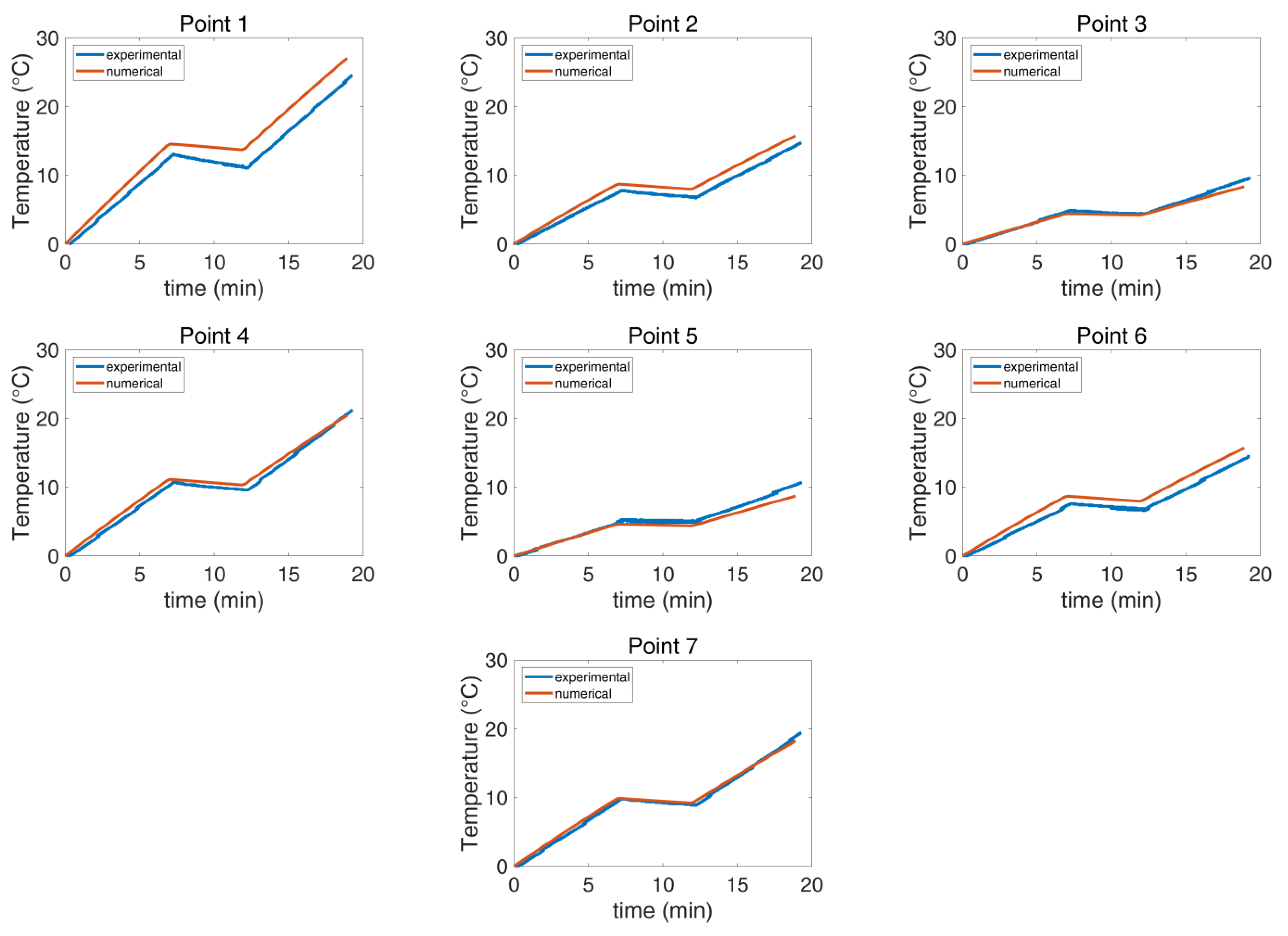
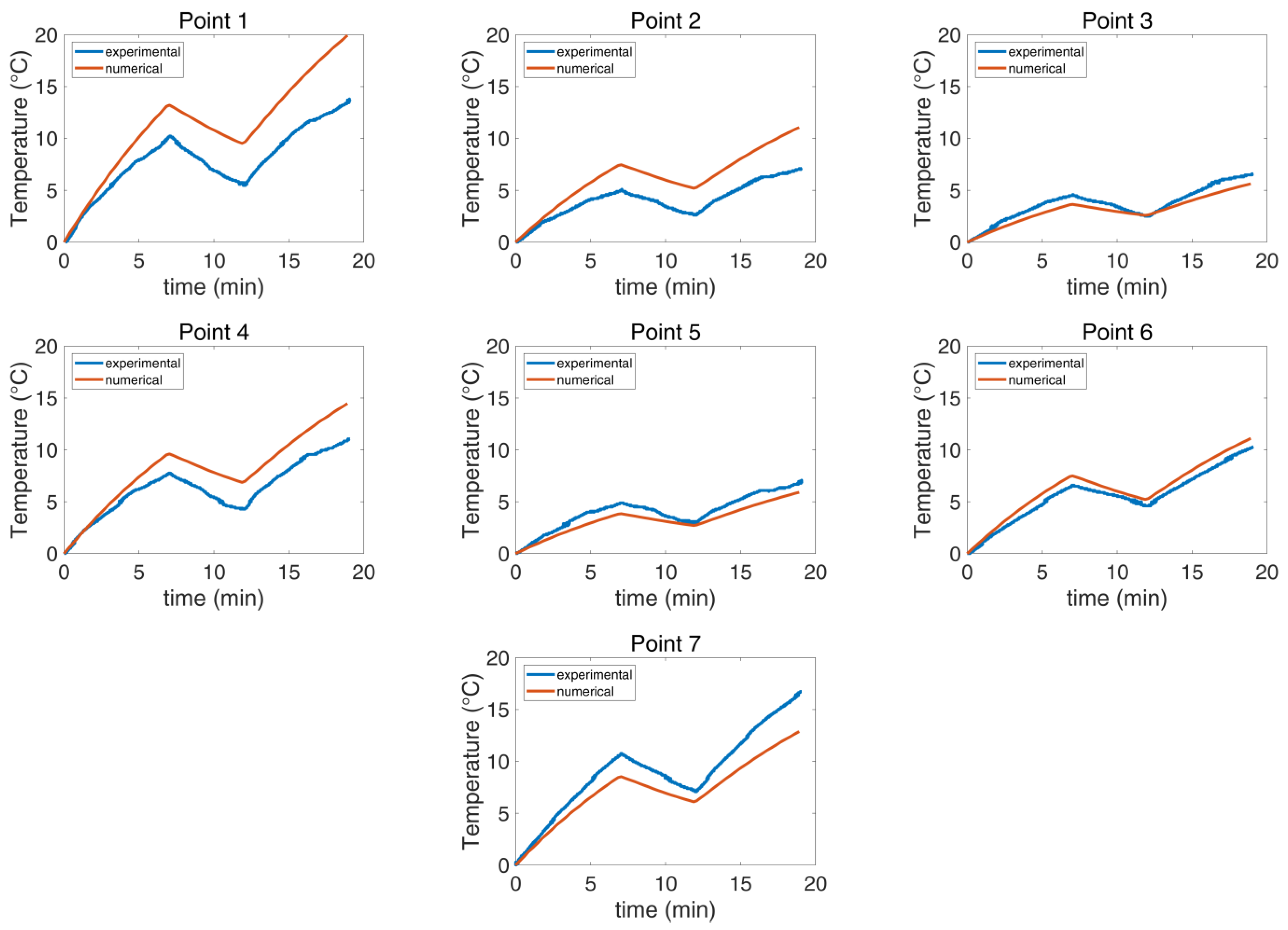
3.2. Cooling System Validation
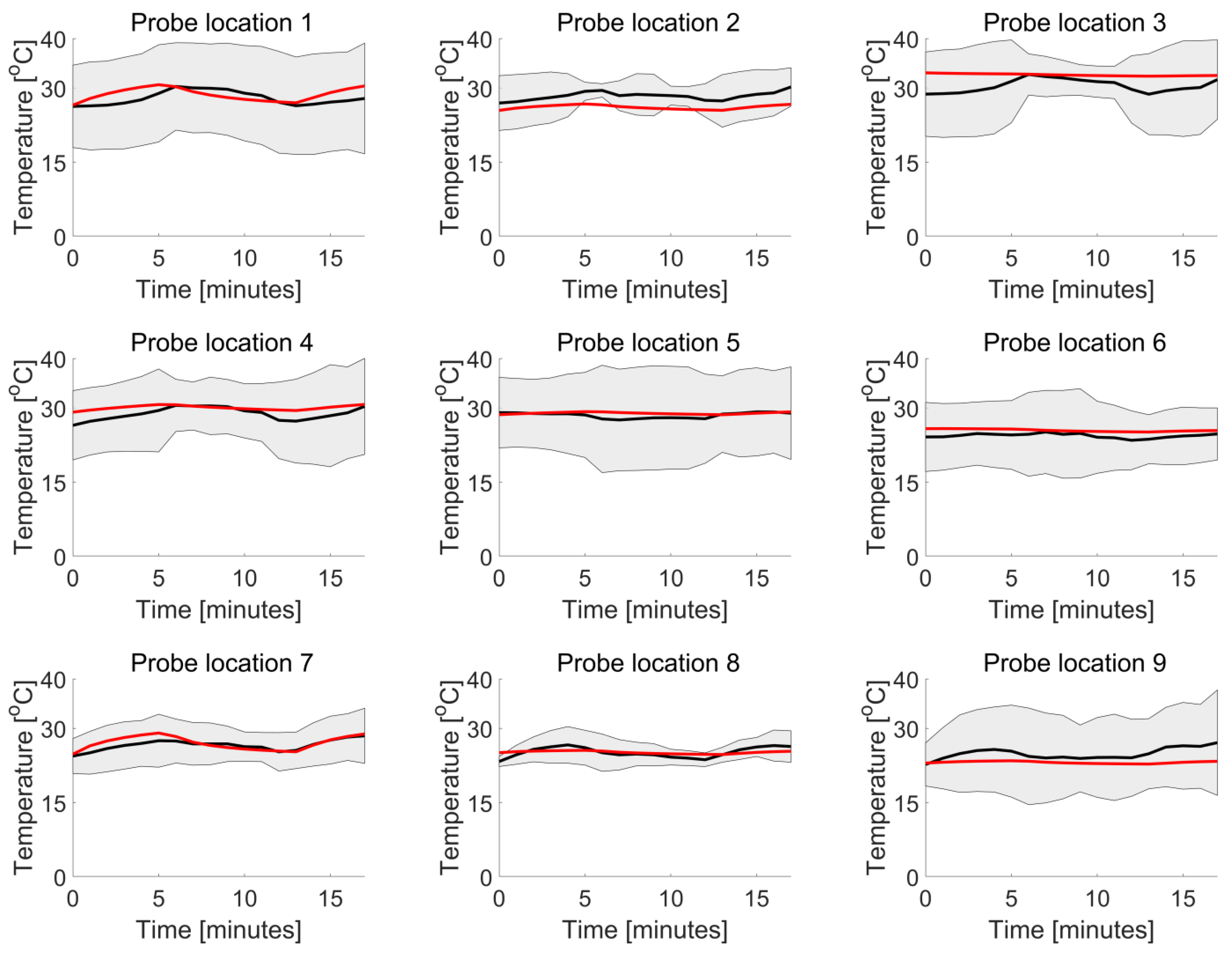
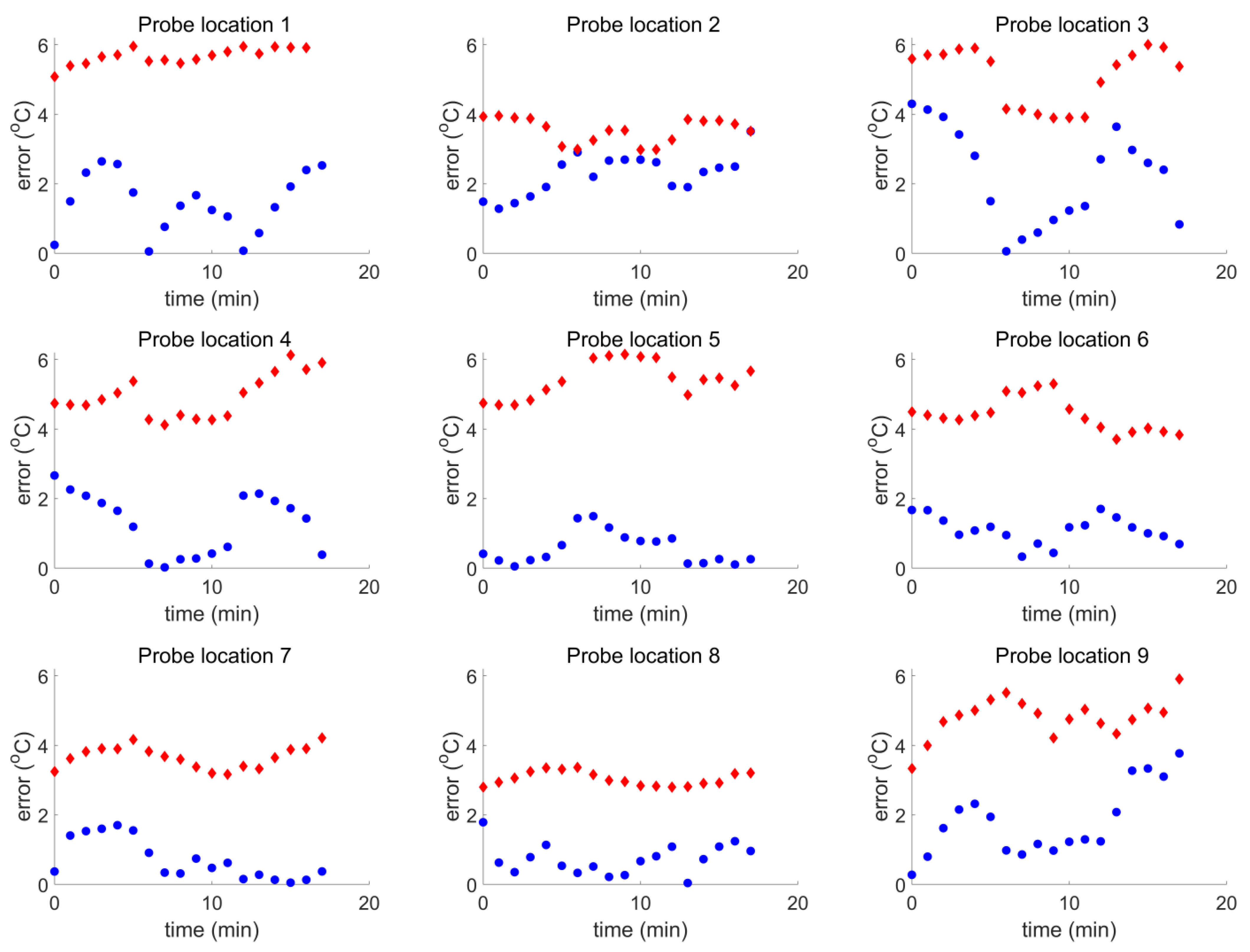
3.3. Human Model Validation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gilchrist, R.K.; Medal, R.; Shorey, W.D.; Hanselman, R.C.; Parrott, J.C.; Taylor, C.B. Selective Inductive Heating of Lymph Nodes. Ann. Surg. 1957, 146, 596–606. [Google Scholar] [CrossRef] [PubMed]
- Ortega, D.; Pankhurst, Q.A. Magnetic Hyperthermia. In Nanoscience: Volume 1: Nanostructures through Chemistry; The Royal Society of Chemistry: Cambridge, UK, 2012; pp. 60–88. [Google Scholar]
- Pankhurst, Q.A.; Thanh, N.T.K.; Jones, S.K.; Dobson, J. Progress in Applications of Magnetic Nanoparticles in Biomedicine. J. Phys. D Appl. Phys. 2009, 42, 224001. [Google Scholar] [CrossRef]
- Atkinson, W.J.; Brezovich, I.A.; Chakraborty, D.P. Usable Frequencies in Hyperthermia with Thermal Seeds. IEEE Trans. Biomed. Eng. 1984, BME-31, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Hergt, R.; Dutz, S. Magnetic Particle Hyperthermia—Biophysical Limitations of a Visionary Tumour Therapy. J. Magn. Magn. Mater. 2007, 311, 187–192. [Google Scholar] [CrossRef]
- Nadobny, J.; Szimtenings, M.; Diehl, D.; Stetter, E.; Brinker, G.; Wust, P. Evaluation of MR-Induced Hot Spots for Different Temporal SAR Modes Using a Time-Dependent Finite Difference Method With Explicit Temperature Gradient Treatment. IEEE Trans. Biomed. Eng. 2007, 54, 1837–1850. [Google Scholar] [CrossRef]
- Murbach, M.; Neufeld, E.; Capstick, M.; Kainz, W.; Brunner, D.O.; Samaras, T.; Pruessmann, K.P.; Kuster, N. Thermal Tissue Damage Model Analyzed for Different Whole-Body SAR and Scan Durations for Standard MR Body Coils. Magn. Reson. Med. 2014, 71, 421–431. [Google Scholar] [CrossRef]
- Herrero de la Parte, B.; Rodrigo, I.; Gutiérrez-Basoa, J.; Iturrizaga Correcher, S.; Mar Medina, C.; Echevarría-Uraga, J.J.; Garcia, J.A.; Plazaola, F.; García-Alonso, I. Proposal of New Safety Limits for In Vivo Experiments of Magnetic Hyperthermia Antitumor Therapy. Cancers 2022, 14, 3084. [Google Scholar] [CrossRef]
- Stigliano, R.V.; Shubitidze, F.; Petryk, J.D.; Shoshiashvili, L.; Petryk, A.A.; Hoopes, P.J. Mitigation of Eddy Current Heating during Magnetic Nanoparticle Hyperthermia Therapy. Int. J. Hyperth. 2016, 32, 735–748. [Google Scholar] [CrossRef]
- Tsiapla, A.-R.; Kalimeri, A.-A.; Maniotis, N.; Myrovali, E.; Samaras, T.; Angelakeris, M.; Kalogirou, O. Mitigation of Magnetic Particle Hyperthermia Side Effects by Magnetic Field Controls. Int. J. Hyperth. 2021, 38, 511–522. [Google Scholar] [CrossRef]
- Balousis, A.; Maniotis, N.; Samaras, T. Improvement of Magnetic Particle Hyperthermia: Healthy Tissues Sparing by Reduction in Eddy Currents. Nanomaterials 2021, 11, 556. [Google Scholar] [CrossRef]
- Pefanis, G.; Maniotis, N.; Tsiapla, A.-R.; Makridis, A.; Samaras, T.; Angelakeris, M. Numerical Simulation of Temperature Variations during the Application of Safety Protocols in Magnetic Particle Hyperthermia. Nanomaterials 2022, 12, 554. [Google Scholar] [CrossRef]
- Attaluri, A.; Jackowski, J.; Sharma, A.; Kandala, S.K.; Nemkov, V.; Yakey, C.; DeWeese, T.L.; Kumar, A.; Goldstein, R.C.; Ivkov, R. Design and Construction of a Maxwell-Type Induction Coil for Magnetic Nanoparticle Hyperthermia. Int. J. Hyperth. 2020, 37, 1–14. [Google Scholar] [CrossRef]
- Shoshiashvili, L.; Shamatava, I.; Kakulia, D.; Shubitidze, F. Design and Assessment of a Novel Biconical Human-Sized Alternating Magnetic Field Coil for MNP Hyperthermia Treatment of Deep-Seated Cancer. Cancers 2023, 15, 1672. [Google Scholar] [CrossRef]
- Bellizzi, G.; Bucci, O.M.; Chirico, G. Numerical Assessment of a Criterion for the Optimal Choice of the Operative Conditions in Magnetic Nanoparticle Hyperthermia on a Realistic Model of the Human Head. Int. J. Hyperth. 2016, 32, 688–703. [Google Scholar] [CrossRef] [PubMed]
- Kandala, S.K.; Sharma, A.; Mirpour, S.; Liapi, E.; Ivkov, R.; Attaluri, A. Validation of a Coupled Electromagnetic and Thermal Model for Estimating Temperatures during Magnetic Nanoparticle Hyperthermia. Int. J. Hyperth. 2021, 38, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Stigliano, R.V.; Shubitidze, F.; Petryk, A.A.; Tate, J.A.; Hoopes, P.J. Magnetic Nanoparticle Hyperthermia: Predictive Model for Temperature Distribution; Ryan, T.P., Ed.; SPIE: Bellingham, WA, USA, 2013; p. 858410. [Google Scholar]
- The Open-Label Programming Study of Increasing Dose to Test the Safety of Nanoparticles with Electromagnetic Field Radiation in Patients with Metastatic Solid Tumor Type Cancer. Available online: https://my.health.gov.il/CliniTrials/Pages/MOH_2022-09-18_012060.aspx (accessed on 12 January 2024).
- Kraus, S.; Rabinovitz, R.; Sigalov, E.; Eltanani, M.; Khandadash, R.; Tal, C.; Rivlin, O.; Sharaga, E.; Rukenstein, P.; Cohen-Erner, M.; et al. Self-Regulating Novel Iron Oxide Nanoparticle-Based Magnetic Hyperthermia in Swine: Biocompatibility, Biodistribution, and Safety Assessments. Arch. Toxicol. 2022, 96, 2447–2464. [Google Scholar] [CrossRef] [PubMed]
- Kraus, S.; Khandadash, R.; Hof, R.; Nyska, A.; Sigalov, E.; Eltanani, M.; Rukenstein, P.; Rabinovitz, R.; Kassem, R.; Antebi, A.; et al. Novel Nanoparticle-Based Cancer Treatment, Effectively Inhibits Lung Metastases and Improves Survival in a Murine Breast Cancer Model. Front. Oncol. 2021, 11, 761045. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Erner, M.; Khandadash, R.; Hof, R.; Shalev, O.; Antebi, A.; Cyjon, A.; Kanakov, D.; Nyska, A.; Goss, G.; Hilton, J.; et al. Fe3O4 Nanoparticles and Paraffin Wax as Phase Change Materials Embedded in Polymer Matrixes for Temperature-Controlled Magnetic Hyperthermia. ACS Appl. Nano Mater. 2021, 4, 11187–11198. [Google Scholar] [CrossRef]
- Fang, J.; Nakamura, H.; Maeda, H. The EPR Effect: Unique Features of Tumor Blood Vessels for Drug Delivery, Factors Involved, and Limitations and Augmentation of the Effect. Adv. Drug Deliv. Rev. 2011, 63, 136–151. [Google Scholar] [CrossRef] [PubMed]
- Pennes, H.H. Analysis of Tissue and Arterial Blood Temperatures in the Resting Human Forearm. J. Appl. Physiol. 1948, 1, 93–122. [Google Scholar] [CrossRef]
- Gabriel, C. Compilation of the Dielectric Properties of Body Tissues at RF and Microwave Frequencies; Occupational and Environmental Health Directorate: San Antonio, TX, USA, 1996. [Google Scholar]
- Shah, R.K.; London, A.L. Laminar Flow Forced Convection in Ducts; Academic Press: Cambridge, MA, USA, 1978. [Google Scholar]
- IT’IS Foundation. Ella cViP3.1; IT’IS Foundation: Zürich, Switzerland, 2016. [Google Scholar] [CrossRef]
- Drizdal, T.; Togni, P.; Visek, L.; Vrba, J. Comparison of Constant and Temperature Dependent Blood Perfusion in Temperature Prediction for Superficial Hyperthermia. Radioengineering 2010, 19, 281–289. [Google Scholar]
- Cabot, E.; Lloyd, T.; Christ, A.; Kainz, W.; Douglas, M.; Stenzel, G.; Wedan, S.; Kuster, N. Evaluation of the RF heating of a generic deep brain stimulator exposed in 1.5 T magnetic resonance scanners. Bioelectromagnetics 2013, 34, 104–113. [Google Scholar] [CrossRef]
- Neufeld, E.; Kühn, S.; Szekely, G.; Kuster, N. Measurement, simulation and uncertainty assessment of implant heating during MRI. Phys. Med. Biol. 2009, 54, 4151–4169. [Google Scholar] [CrossRef]
- Joint Committee for Guides in Metrology/Working Group 1. Evaluation of Measurement Data—Guide to the Expression of Uncertainty in Measurement. 2008. Available online: https://www.bipm.org/documents/20126/2071204/JCGM_100_2008_E.pdf/cb0ef43f-baa5-11cf-3f85-4dcd86f77bd6 (accessed on 20 December 2023).
- MagForce NT GmbH. Available online: https://magforce.de/ (accessed on 12 January 2024).
- Kraus, S. Novel Approach for Magnetic Nanoparticle-Based Hyperthermia for Metastatic Cancer Treatment. Biomed. J. Sci. Tech. Res. 2020, 32. [Google Scholar] [CrossRef]
- Paulides, M.M.; Stauffer, P.R.; Neufeld, E.; Maccarini, P.F.; Kyriakou, A.; Canters, R.A.M.; Diederich, C.J.; Bakker, J.F.; Van Rhoon, G.C. Simulation Techniques in Hyperthermia Treatment Planning. Int. J. Hyperth. 2013, 29, 346–357. [Google Scholar] [CrossRef]
- Verhaart, R.F.; Fortunati, V.; Verduijn, G.M.; van der Lugt, A.; van Walsum, T.; Veenland, J.F.; Paulides, M.M. The Relevance of MRI for Patient Modeling in Head and Neck Hyperthermia Treatment Planning: A Comparison of CT and CT-MRI Based Tissue Segmentation on Simulated Temperature. Med. Phys. 2014, 41, 123302. [Google Scholar] [CrossRef] [PubMed]
- Beck, M.; Ghadjar, P.; Weihrauch, M.; Burock, S.; Budach, V.; Nadobny, J.; Sehouli, J.; Wust, P. Regional Hyperthermia of the Abdomen, a Pilot Study towards the Treatment of Peritoneal Carcinomatosis. Radiat. Oncol. 2015, 10, 157. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Rioux, T.P.; Castellani, M.P. Three Dimensional Models of Human Thermoregulation: A Review. J. Therm. Biol. 2023, 112, 103491. [Google Scholar] [CrossRef]
- Oh, S.; Ryu, Y.-C.; Carluccio, G.; Sica, C.T.; Collins, C.M. Measurement of SAR-Induced Temperature Increase in a Phantom and in Vivo with Comparison to Numerical Simulation. Magn. Reson. Med. 2014, 71, 1923–1931. [Google Scholar] [CrossRef]
- Rossmanna, C.; Haemmerich, D. Review of Temperature Dependence of Thermal Properties, Dielectric Properties, and Perfusion of Biological Tissues at Hyperthermic and Ablation Temperatures. Crit. Rev. Biomed. Eng. 2014, 42, 467–492. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age [Years] | Weight [kg] | Height [cm] | BMI [kg/m2] | Back Width [cm] | Chest Height [cm] | Circumference [cm] | Gender | |
|---|---|---|---|---|---|---|---|---|
| P01 | 55 | 52.0 | 160 | 20.3 | 26.0 | 17.0 | 82.0 | F |
| P02 | 63 | 53.7 | 163 | 20.2 | 30.5 | 22.0 | 86.0 | F |
| P03 | 64 | 61.0 | 160 | 23.8 | 38.0 | 17.0 | 86.5 | F |
| P04 | 70 | 64.4 | 165 | 23.7 | 35.0 | 20.0 | 92.0 | F |
| P05 | 56 | 47.2 | 155 | 19.6 | N/A | N/A | 93.0 | F |
| P06 | 67 | 86.6 | 193 | 23.2 | 35.0 | 21.0 | 105.0 | M |
| Ella | 26 | 57.3 | 163 | 21.6 | 27.0 | 17.7 | 89.9 | F |
| Deviation | |||||||
|---|---|---|---|---|---|---|---|
| Point 1 | Point 2 | Point 3 | Point 4 | Point 5 | Point 6 | Point 7 | |
| CBS OFF | −10% | −7% | 14% | 4% | 18% | −9% | 6% |
| CBS ON | −46% | −56% | 15% | −31% | 13% | −8% | 23% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rouni, M.A.; Shalev, B.; Tsanidis, G.; Markakis, I.; Kraus, S.; Rukenstein, P.; Suchi, D.; Shalev, O.; Samaras, T. A Validated Methodological Approach to Prove the Safety of Clinical Electromagnetic Induction Systems in Magnetic Hyperthermia. Cancers 2024, 16, 621. https://doi.org/10.3390/cancers16030621
Rouni MA, Shalev B, Tsanidis G, Markakis I, Kraus S, Rukenstein P, Suchi D, Shalev O, Samaras T. A Validated Methodological Approach to Prove the Safety of Clinical Electromagnetic Induction Systems in Magnetic Hyperthermia. Cancers. 2024; 16(3):621. https://doi.org/10.3390/cancers16030621
Chicago/Turabian StyleRouni, Maria Anastasia, Boaz Shalev, George Tsanidis, Ioannis Markakis, Sarah Kraus, Pazit Rukenstein, Doron Suchi, Ofer Shalev, and Theodoros Samaras. 2024. "A Validated Methodological Approach to Prove the Safety of Clinical Electromagnetic Induction Systems in Magnetic Hyperthermia" Cancers 16, no. 3: 621. https://doi.org/10.3390/cancers16030621