
Current Treatment Practices and Prognostic Factors in Early-Stage Ovarian Cancer—An Analysis of the NOGGO/JAGO

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
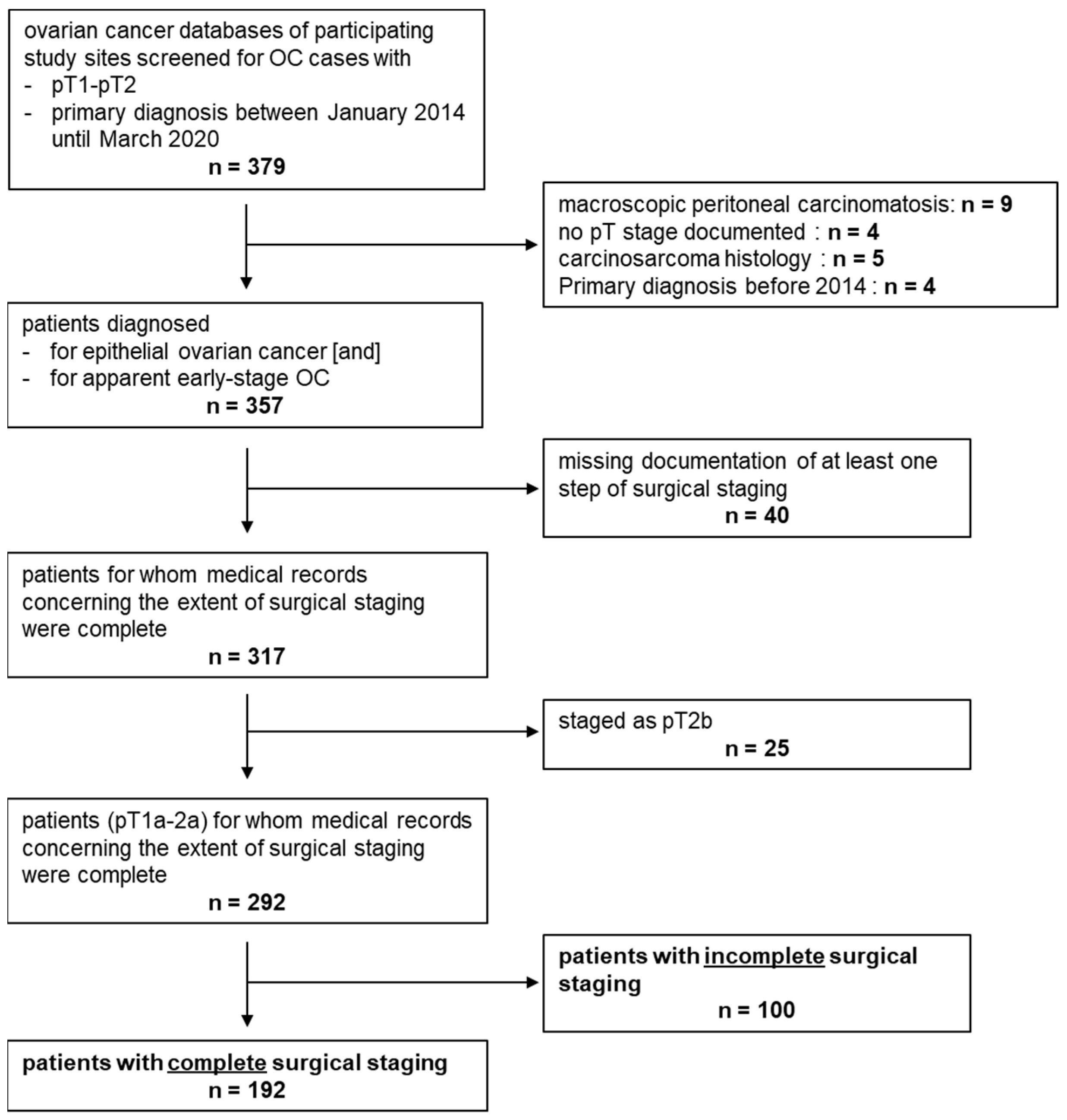
2.1. Characteristics of the Study Sample
2.2. Statistical Methods
3. Results
3.1. Study Sample Characteristics
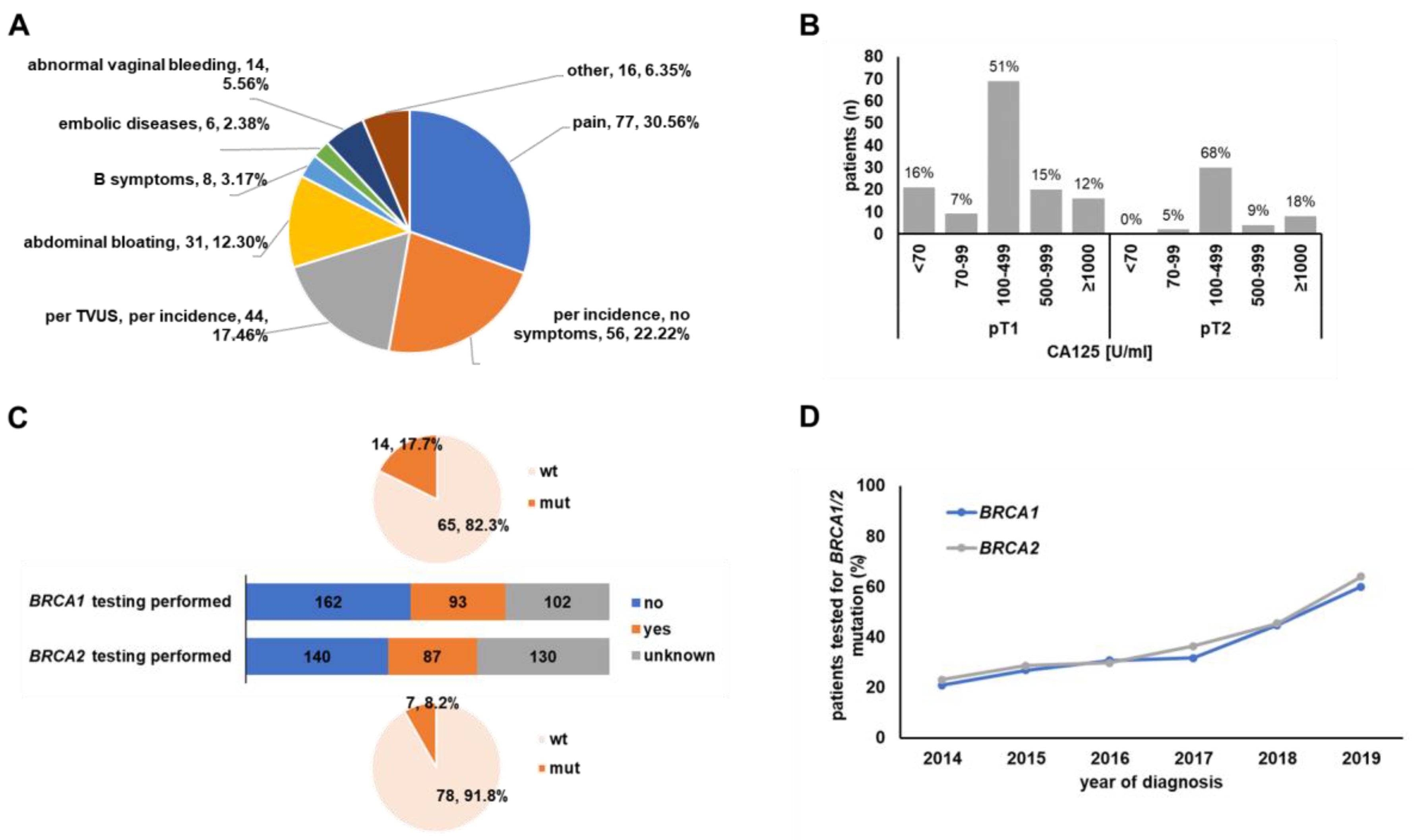
3.2. Symptoms, Clinical Setting and Diagnostic Procedures
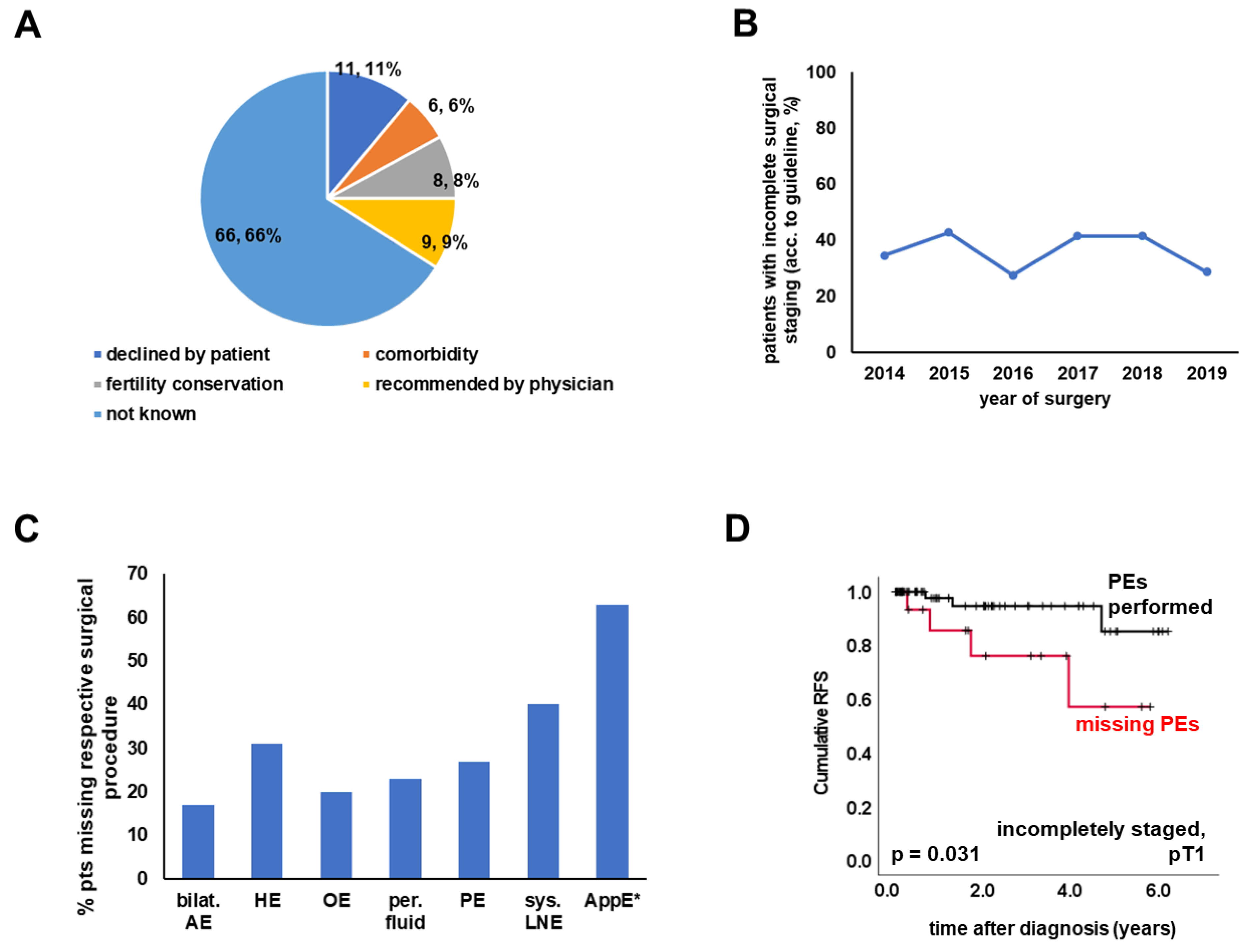
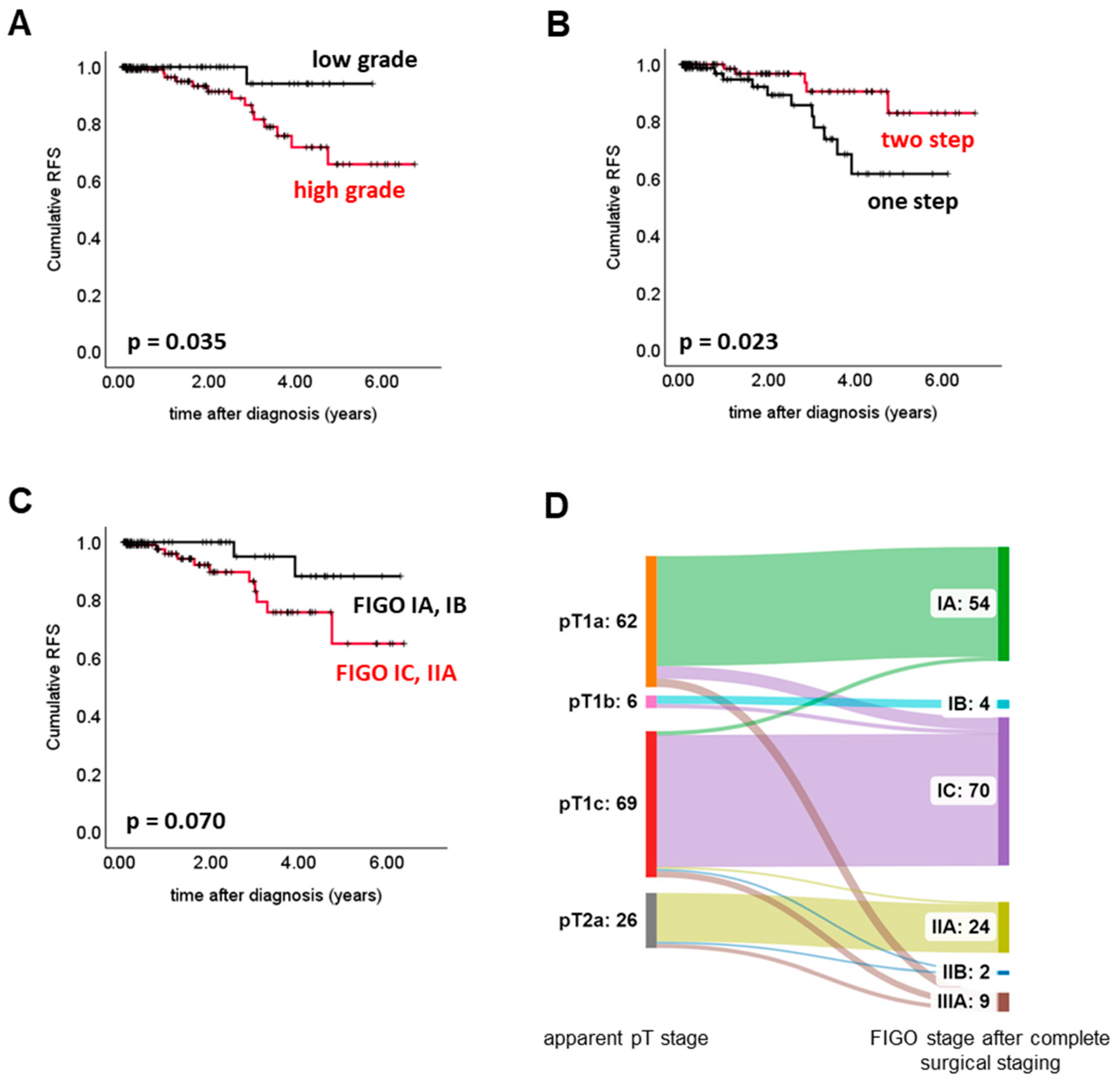
3.3. Surgery
3.4. Adjuvant Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Trimbos, J.B. Surgical treatment of early-stage ovarian cancer. Best Pract. Res. Clin. Obstet. Gynaecol. 2017, 41, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Filippova, O.; Straubhar, A.; Santiago, N.L.; Zivanovic, O.; Gardner, G.; Tew, W.; O’Cearbhaill, R.; Grisham, R.; Sonoda, Y.; Roche, K.L.; et al. 10-year survival in patients diagnosed with high-grade epithelial ovarian cancer: A new metric for a new millennium. Gynecol. Oncol. 2021, 162, S75. [Google Scholar] [CrossRef]
- Ushijima, K. Treatment for recurrent ovarian cancer-at first relapse. J. Oncol. 2010, 2010, 497429. [Google Scholar] [CrossRef] [PubMed]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): S3-Leitlinie Diagnostik, Therapie und Nachsorge maligner Ovarialtumoren, Langversion 5.0, 2021, AWMF-Registernummer: 032/035OL. Available online: https://www.leitlinienprogramm-onkologie.de/leitlinien/ovarialkarzinom/ (accessed on 4 March 2023).
- Mahner, S.; du Bois, A.; Pfisterer, J.; Hilpert, F.; Sehouli, J.; Lamparter, C.; Kerkmann, M.; Harter, P. Behandlungsqualität des Ovarialkarzinoms in Deutschland: Aktuelle Ergebnisse des Qualitätssicherungsprogramms QS OVAR. Geburtshilfe Frauenheilkd 2019, 79, PD45. [Google Scholar]
- Hengeveld, E.M.; Zusterzeel, P.L.M.; Lajer, H.; Hogdall, C.K.; Rosendahl, M. The value of surgical staging in patients with apparent early stage epithelial ovarian carcinoma. Gynecol. Oncol. 2019, 154, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Hilpert, F.; du Bois, A.; Pfisterer, J.; Sehouli, J.; Lamparter, C.; Kerkmann, M.; Harter, P. Steigerung der Therapiequalität des Ovarialkarzinoms in Deutschland—Ergebnisse der eigenverantwortlichen QS Ovar. Geburtshilfe Frauenheilkd 2020, 80, P389. [Google Scholar]
- Available online: https://sankeymatic.com/ (accessed on 30 November 2022).
- Hsieh, S.-F.; Lau, H.-Y.; Wu, H.-H.; Hsu, H.-C.; Twu, N.-F.; Cheng, W.-F. Prognostic Factors of Early Stage Epithelial Ovarian Carcinoma. Int. J. Environ. Res. Public Health 2019, 16, 637. [Google Scholar] [CrossRef] [Green Version]
- Trimbos, J.B.; Vergote, I.; Bolis, G.; Vermorken, J.B.; Mangioni, C.; Madronal, C.; Franchi, M.; Tateo, S.; Zanetta, G.; Scarfone, G.; et al. Impact of adjuvant chemotherapy and surgical staging in early-stage ovarian carcinoma: European Organisation for Research and Treatment of Cancer-Adjuvant ChemoTherapy in Ovarian Neoplasm trial. J. Natl. Cancer Inst. 2003, 95, 113–125. [Google Scholar] [CrossRef] [Green Version]
- Patsner, B. Preoperative serum CA-125 levels in early stage ovarian cancer. Eur. J. Gynaecol. Oncol. 1990, 11, 319–321. [Google Scholar] [CrossRef]
- Trimbos, B.; Timmers, P.; Pecorelli, S.; Coens, C.; Ven, K.; van der Burg, M.; Casado, A. Surgical staging and treatment of early ovarian cancer: Long-term analysis from a randomized trial. J. Natl. Cancer Inst. 2010, 102, 982–987. [Google Scholar] [CrossRef] [Green Version]
- Harter, P.; Sehouli, J.; Lorusso, D.; Reuss, A.; Vergote, I.; Marth, C.; Kim, J.W.; Raspagliesi, F.; Lampe, B.; Landoni, F.; et al. LION: Lymphadenectomy in ovarian neoplasms—A prospective randomized AGO study group led gynecologic cancer intergroup trial. J. Clin. Oncol. 2017, 35, 5500. [Google Scholar] [CrossRef]
- Powless, C.A.; Aletti, G.D.; Bakkum-Gamez, J.N.; Cliby, W.A. Risk factors for lymph node metastasis in apparent early-stage epithelial ovarian cancer: Implications for surgical staging. Gynecol. Oncol. 2011, 122, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Le, T.; Adolph, A.; Krepart, G.V.; Lotocki, R.; Heywood, M.S. The benefits of comprehensive surgical staging in the management of early-stage epithelial ovarian carcinoma. Gynecol. Oncol. 2002, 85, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Huang, Y.; Matsuzaki, S.; Klar, M.; Roman, L.D.; Sood, A.K.; Wright, J.D. Minimally Invasive Surgery and Risk of Capsule Rupture for Women With Early-Stage Ovarian Cancer. JAMA Oncol. 2020, 6, 1110–1113. [Google Scholar] [CrossRef]
- Konstantinopoulos, P.A.; Ceccaldi, R.; Shapiro, G.I.; D’Andrea, A.D. Homologous Recombination Deficiency: Exploiting the Fundamental Vulnerability of Ovarian Cancer. Cancer Discov. 2015, 5, 1137–1154. [Google Scholar] [CrossRef] [Green Version]
- Lavie, O.; Narod, S.; Lejbkowicz, F.; Dishon, S.; Goldberg, Y.; Gemer, O.; Rennert, G. Double heterozygosity in the BRCA1 and BRCA2 genes in the Jewish population. Ann. Oncol. 2011, 22, 964–966. [Google Scholar] [CrossRef] [PubMed]
- You, Y.; Li, L.; Lu, J.; Wu, H.; Wang, J.; Gao, J.; Wu, M.; Liang, Z. Germline and Somatic BRCA1/2 Mutations in 172 Chinese Women With Epithelial Ovarian Cancer. Front. Oncol. 2020, 10, 295. [Google Scholar] [CrossRef] [PubMed]
- Young, R.C.; Walton, L.A.; Ellenberg, S.S.; Homesley, H.D.; Wilbanks, G.D.; Decker, D.G.; Miller, A.; Park, R.; Major, F., Jr. Adjuvant therapy in stage I and stage II epithelial ovarian cancer. Results of two prospective randomized trials. N. Engl. J. Med. 1990, 322, 1021–1027. [Google Scholar] [CrossRef]
- Bolis, G.; Colombo, N.; Pecorelli, S.; Torri, V.; Marsoni, S.; Bonazzi, C.; Chiari, S.; Favalli, G.; Mangili, G.; Presti, M.; et al. Adjuvant treatment for early epithelial ovarian cancer: Results of two randomised clinical trials comparing cisplatin to no further treatment or chromic phosphate (32P). G.I.C.O.G.: Gruppo Interregionale Collaborativo in Ginecologia Oncologica. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 1995, 6, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, M.; Tamauchi, S.; Iyoshi, S.; Kitami, K.; Uno, K.; Mogi, K.; Kajiyama, H. Impact of incomplete surgery and adjuvant chemotherapy for the intraoperative rupture of capsulated stage I epithelial ovarian cancer: A multi-institutional study with an in-depth subgroup analysis. J. Gynecol. Oncol. 2021, 32, e66. [Google Scholar] [CrossRef]
- Collinson, F.; Qian, W.; Fossati, R.; Lissoni, A.; Williams, C.; Parmar, M.; Ledermann, J.; Colombo, N.; Swart, A. Optimal treatment of early-stage ovarian cancer. Ann. Oncol. 2014, 25, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- Nasioudis, D.; Mastroyannis, S.; Ko, E.; Haggerty, A.; Cory, L.; Giuntoli, R.; Kim, S.; Morgan, M.; Latif, N. Delay in adjuvant chemotherapy administration for patients with FIGO stage I epithelial ovarian carcinoma is associated with worse survival. Gynecol. Oncol. 2021, 162, S124. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n (Data Available) | n | % or Range | |
|---|---|---|---|
| Patient age (median) | (55.8) | 19.1–88.1 | |
| pT | 357 | ||
| 1a | 145 | 40.6 | |
| 1b | 14 | 3.9 | |
| 1c | 126 | 35.3 | |
| 2a | 42 | 11.8 | |
| 2b | 30 | 8.4 | |
| Grading | 335 | ||
| HGSOC | 117 | 34.9 | |
| LGSOC | 21 | 6.3 | |
| G1 | 60 | 17.9 | |
| G2 | 65 | 19.4 | |
| G3 | 72 | 21.5 | |
| Histology | 353 | ||
| serous | 141 | 39.9 | |
| endometrioid | 93 | 26.3 | |
| mucinous | 54 | 15.3 | |
| clear cell | 46 | 13.0 | |
| mixed | 10 | 2.8 | |
| other | 9 | 2.5 |
| Surgical Staging | ||||
|---|---|---|---|---|
| Data Available (n) | Complete | Incomplete | p | |
| pT | ||||
| pT1 | 292 | 165 | 91 | ns |
| pT2 | 27 | 9 | ||
| Histology | ||||
| other | 291 | 110 | 71 | 0.016 |
| serous | 82 | 28 | ||
| Grade | ||||
| low | 281 | 68 | 48 | 0.013 |
| high | 120 | 45 | ||
| (Primary) Surgery | ||||
| regular care hospital | 291 | 130 | 58 | ns |
| maximal care hospital | 62 | 41 | ||
| Surgical Setup | ||||
| one-step | 291 | 85 | 43 | ns |
| two-step | 107 | 56 | ||
| Received CHT | ||||
| no | 243 | 135 | 54 | ns |
| yes | 36 | 18 | ||
| Patient Age | ||||
| ≤56 years | 288 | 104 | 46 | ns |
| >56 years | 87 | 51 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heublein, S.; Baum, J.; Jaeger, A.; Grimm-Glang, D.; Olthoff, J.; Braicu, E.I.; Azzam Nieto, O.; Hassdenteufel, K.; Schmalfeldt, B.; Hanker, L.; et al. Current Treatment Practices and Prognostic Factors in Early-Stage Ovarian Cancer—An Analysis of the NOGGO/JAGO. Cancers 2023, 15, 2038. https://doi.org/10.3390/cancers15072038
Heublein S, Baum J, Jaeger A, Grimm-Glang D, Olthoff J, Braicu EI, Azzam Nieto O, Hassdenteufel K, Schmalfeldt B, Hanker L, et al. Current Treatment Practices and Prognostic Factors in Early-Stage Ovarian Cancer—An Analysis of the NOGGO/JAGO. Cancers. 2023; 15(7):2038. https://doi.org/10.3390/cancers15072038
Chicago/Turabian StyleHeublein, Sabine, Joanna Baum, Anna Jaeger, Donata Grimm-Glang, Julia Olthoff, Elena Ioana Braicu, Osama Azzam Nieto, Kathrin Hassdenteufel, Barbara Schmalfeldt, Lars Hanker, and et al. 2023. "Current Treatment Practices and Prognostic Factors in Early-Stage Ovarian Cancer—An Analysis of the NOGGO/JAGO" Cancers 15, no. 7: 2038. https://doi.org/10.3390/cancers15072038