
Prediction of Surgical Outcome in Advanced Ovarian Cancer by Imaging and Laparoscopy: A Narrative Review
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Prediction of Non-Resectability
2.1. Laparotomy
2.2. Laparoscopy
2.3. Imaging
2.3.1. Ultrasound
2.3.2. Computed Tomography
2.3.3. Magnetic Resonance Imaging
2.3.4. Positron Emission Tomography
3. Future Studies
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- International Agency for Research on Cancer, 2018, W. GLOBOCAN 2018. 2019. Available online: http://globocan.iarc.fr/ (accessed on 29 November 2022).
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.W.; Comber, H.; Forman, D.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer 2013, 49, 1374–1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menon, U.; Gentry-Maharaj, A.; Burnell, M.; Singh, N.; Ryan, A.; Karpinskyj, C.; Carlino, G.; Taylor, J.; Massingham, S.K.; Raikou, M.; et al. Ovarian cancer population screening and mortality after long-term follow-up in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): A randomised controlled trial. Lancet 2021, 397, 2182–2193. [Google Scholar] [CrossRef] [PubMed]
- Buys, S.S.; Partridge, E.; Black, A.; Johnson, C.C.; Lamerato, L.; Isaacs, C.; Reding, D.J.; Greenlee, R.T.; Yokochi, L.A.; Kessel, B.; et al. Effect of screening on ovarian cancer mortality: The Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Randomized Controlled Trial. JAMA 2011, 305, 2295–2303. [Google Scholar] [CrossRef] [Green Version]
- Pinsky, P.F.; Yu, K.; Kramer, B.S.; Black, A.; Buys, S.S.; Partridge, E.; Gohagan, J.; Berg, C.D.; Prorok, P.C. Extended mortality results for ovarian cancer screening in the PLCO trial with median 15 years follow-up. Gynecol. Oncol. 2016, 143, 270–275. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, I.J.; Menon, U.; Ryan, A.; Gentry-Maharaj, A.; Burnell, M.; Kalsi, J.K.; Amso, N.N.; Apostolidou, S.; Benjamin, E.; Cruickshank, D.; et al. Ovarian cancer screening and mortality in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): A randomised controlled trial. Lancet 2016, 387, 945–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du Bois, A.; Rochon, J.; Pfisterer, J.; Hoskins, W.J. Variations in institutional infrastructure, physician specialization and experience, and outcome in ovarian cancer: A systematic review. Gynecol. Oncol. 2009, 112, 422–436. [Google Scholar] [CrossRef]
- Vernooij, F.; Heintz, P.; Witteveen, E.; van der Graaf, Y. The outcomes of ovarian cancer treatment are better when provided by gynecologic oncologists and in specialized hospitals: A systematic review. Gynecol. Oncol. 2007, 105, 801–812. [Google Scholar] [CrossRef] [PubMed]
- Querleu, D.; Planchamp, F.; Chiva, L.; Fotopoulou, C.; Barton, D.; Cibula, D.; Aletti, G.; Carinelli, S.; Creutzberg, C.; Davidson, B.; et al. European Society of Gynaecological Oncology (ESGO) Guidelines for Ovarian Cancer Surgery. Int. J. Gynecol. Cancer 2017, 27, 1534–1542. [Google Scholar] [CrossRef] [PubMed]
- Fotopoulou, C.; Concin, N.; Planchamp, F.; Morice, P.; Vergote, I.; du Bois, A.; Querleu, D. Quality indicators for advanced ovarian cancer surgery from the European Society of Gynaecological Oncology (ESGO): 2020 update. Int. J. Gynecol. Cancer 2020, 30, 436–440. [Google Scholar] [CrossRef]
- Timmerman, D.; Planchamp, F.; Bourne, T.; Landolfo, C.; du Bois, A.; Chiva, L.; Cibula, D.; Concin, N.; Fischerova, D.; Froyman, W.; et al. ESGO/ISUOG/IOTA/ESGE Consensus Statement on pre-operative diagnosis of ovarian tumors. Int. J. Gynecol. Cancer 2021, 31, 961–982. [Google Scholar] [CrossRef]
- Froyman, W.; Wynants, L.; Landolfo, C.; Bourne, T.; Valentin, L.; Testa, A.; Sladkevicius, P.; Franchi, D.; Fischerova, D.; Savelli, L.; et al. Validation of the Performance of International Ovarian Tumor Analysis (IOTA) Methods in the Diagnosis of Early Stage Ovarian Cancer in a Non-Screening Population. Diagnostics 2017, 7, 32. [Google Scholar] [CrossRef]
- Du Bois, A.; Baert, T.; Vergote, I. Role of Neoadjuvant Chemotherapy in Advanced Epithelial Ovarian Cancer. J. Clin. Oncol. 2019, 37, 2398–2405. [Google Scholar] [CrossRef]
- Du Bois, A.; Reuss, A.; Pujade-Lauraine, E.; Harter, P.; Ray-Coquard, I.; Pfisterer, J. Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: A combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials: By the Arbeitsgemeinschaft Gynaekologische Onkologie Studiengruppe Ovarialkarzinom (AGO-OVAR) and the Groupe d’Investigateurs Nationaux Pour les Etudes des Cancers de l’Ovaire (GINECO). Cancer 2009, 115, 1234–1244. [Google Scholar]
- Miller, R.E.; Leary, A.; Scott, C.L.; Serra, V.; Lord, C.J.; Bowtell, D.; Chang, D.K.; Garsed, D.W.; Jonkers, J.; Ledermann, J.A.; et al. ESMO recommendations on predictive biomarker testing for homologous recombination deficiency and PARP inhibitor benefit in ovarian cancer. Ann. Oncol. 2020, 31, 1606–1622. [Google Scholar] [CrossRef]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef]
- Oza, A.M.; Cook, A.D.; Pfisterer, J.; Embleton, A.; Ledermann, J.A.; Pujade-Lauraine, E.; Kristensen, G.; Carey, M.S.; Beale, P.; Cervantes, A.; et al. Standard chemotherapy with or without bevacizumab for women with newly diagnosed ovarian cancer (ICON7): Overall survival results of a phase 3 randomised trial. Lancet Oncol. 2015, 16, 928–936. [Google Scholar] [CrossRef] [PubMed]
- Ray-Coquard, I.; Pautier, P.; Pignata, S.; Perol, D.; Gonzalez-Martin, A.; Berger, R.; Fujiwara, K.; Vergote, I.; Colombo, N.; Maenpaa, J.; et al. Olaparib plus Bevacizumab as First-Line Maintenance in Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2416–2428. [Google Scholar] [CrossRef]
- Tewari, K.S.; Burger, R.A.; Enserro, D.; Norquist, B.M.; Swisher, E.M.; Brady, M.F.; Bookman, M.A.; Fleming, G.F.; Huang, H.; Homesley, H.D.; et al. Final Overall Survival of a Randomized Trial of Bevacizumab for Primary Treatment of Ovarian Cancer. J. Clin. Oncol. 2019, 37, 2317–2328. [Google Scholar] [CrossRef]
- Bristow, R.E.; Tomacruz, R.S.; Armstrong, D.K.; Trimble, E.L.; Montz, F.J. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: A meta-analysis. J. Clin. Oncol. 2002, 20, 1248–1259. [Google Scholar] [CrossRef] [PubMed]
- Zapardiel, I.; Morrow, C.W. New terminology for cytoreduction in advanced ovarian cancer. Lancet Oncol. 2011, 12, 214. [Google Scholar] [CrossRef] [PubMed]
- Reuss, A.; du Bois, A.; Harter, P.; Fotopoulou, C.; Sehouli, J.; Aletti, G.; Guyon, F.; Greggi, S.; Mosgaard, B.J.; Reinthaller, A.; et al. TRUST: Trial of Radical Upfront Surgical Therapy in advanced ovarian cancer (ENGOT ov33/AGO-OVAR OP7). Int. J. Gynecol. Cancer 2019, 29, 1327–1331. [Google Scholar] [CrossRef] [PubMed]
- Polterauer, S.; Vergote, I.; Concin, N.; Braicu, I.; Chekerov, R.; Mahner, S.; Woelber, L.; Cadron, I.; Van Gorp, T.; Zeillinger, R.; et al. Prognostic value of residual tumor size in patients with epithelial ovarian cancer FIGO stages IIA-IV: Analysis of the OVCAD data. Int. J. Gynecol. Cancer 2012, 22, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Melamed, A.; Manning-Geist, B.; Bregar, A.J.; Diver, E.J.; Goodman, A.; Del Carmen, M.G.; Schorge, J.O.; Rauh-Hain, J.A. Associations between residual disease and survival in epithelial ovarian cancer by histologic type. Gynecol. Oncol. 2017, 147, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Takano, M.; Kikuchi, Y.; Yaegashi, N.; Kuzuya, K.; Ueki, M.; Tsuda, H.; Suzuki, M.; Kigawa, J.; Takeuchi, S.; Tsuda, H.; et al. Clear cell carcinoma of the ovary: A retrospective multicentre experience of 254 patients with complete surgical staging. Br. J. Cancer 2006, 94, 1369–1374. [Google Scholar] [CrossRef] [Green Version]
- Heitz, F.; Du Bois, A.; Reuss, A.; Pujade-Lauraine, E.; Mirza, M.R.; Greggi, S.; Colombo, N.; Marth, C.; Vergote, I.B.; Harter, P.; et al. 186 Surgical outcome as prognostic factor in different histologic subtypes of ovarian carcinoma-analysis of 7 phase III trials by AGO Studygroup + ENGOT. Int. J. Gynecol. Cancer 2021, 31 (Suppl. S3), A205–A206. [Google Scholar]
- Sioulas, V.D.; Schiavone, M.B.; Kadouri, D.; Zivanovic, O.; Roche, K.L.; O’Cearbhaill, R.; Abu-Rustum, N.R.; Levine, D.A.; Sonoda, Y.; Gardner, G.J.; et al. Optimal primary management of bulky stage IIIC ovarian, fallopian tube and peritoneal carcinoma: Are the only options complete gross resection at primary debulking surgery or neoadjuvant chemotherapy? Gynecol. Oncol. 2017, 145, 15–20. [Google Scholar] [CrossRef] [Green Version]
- Grabowski, J.P.; Harter, P.; Heitz, F.; Pujade-Lauraine, E.; Reuss, A.; Kristensen, G.; Ray-Coquard, I.; Heitz, J.; Traut, A.; Pfisterer, J.; et al. Operability and chemotherapy responsiveness in advanced low-grade serous ovarian cancer. An analysis of the AGO Study Group metadatabase. Gynecol. Oncol. 2016, 140, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Nickles, F.A.; Java, J.; Ueda, S.; Bristow, R.E.; Armstrong, D.K.; Bookman, M.A.; Gershenson, D.M.; Gynecologic Oncology Group. Survival in women with grade 1 serous ovarian carcinoma. Obstet. Gynecol. 2013, 122, 225–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, L.A.; He, W.; Sun, C.C.; Zhao, H.; Wright, A.A.; Suidan, R.S.; Dottino, J.; Alejandro Rauh-Hain, J.; Lu, K.H.; Giordano, S.H. Neoadjuvant chemotherapy in elderly women with ovarian cancer: Rates of use and effectiveness. Gynecol. Oncol. 2018, 150, 451–459. [Google Scholar] [CrossRef]
- Colombo, N.; Sessa, C.; Bois, A.D.; Ledermann, J.; McCluggage, W.G.; McNeish, I.; Morice, P.; Pignata, S.; Ray-Coquard, I.; Vergote, I.; et al. ESMO-ESGO consensus conference recommendations on ovarian cancer: Pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease. Int. J. Gynecol. Cancer 2019, 30, 672–705. [Google Scholar]
- Alessi, A.; Martinelli, F.; Padovano, B.; Serafini, G.; Lorusso, D.; Lorenzoni, A.; Ditto, A.; Lecce, F.; Mira, M.; Donfrancesco, C.; et al. FDG-PET/CT to predict optimal primary cytoreductive surgery in patients with advanced ovarian cancer: Preliminary results. Tumori 2016, 102, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Engbersen, M.P.; Sant, I.V.T.; Lok, C.; Lambregts, D.M.J.; Sonke, G.S.; Beets-Tan, R.G.H.; van Driel, W.J.; Lahaye, M.J. MRI with diffusion-weighted imaging to predict feasibility of complete cytoreduction with the peritoneal cancer index (PCI) in advanced stage ovarian cancer patients. Eur. J. Radiol. 2019, 114, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Espada, M.; Garcia-Flores, J.R.; Jimenez, M.; Alvarez-Moreno, E.; De Haro, M.; Gonzalez-Cortijo, L.; Hernandez-Cortes, G.; Martinez-Vega, V.; Sainz De La Cuesta, R. Diffusion-weighted magnetic resonance imaging evaluation of intra-abdominal sites of implants to predict likelihood of suboptimal cytoreductive surgery in patients with ovarian carcinoma. Eur. Radiol. 2013, 23, 2636–2642. [Google Scholar] [CrossRef] [PubMed]
- Fagotti, A.; Fanfani, F.; Ludovisi, M.; Lo Voi, R.; Bifulco, G.; Testa, A.C.; Scambia, G. Role of laparoscopy to assess the chance of optimal cytoreductive surgery in advanced ovarian cancer: A pilot study. Gynecol. Oncol. 2005, 96, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Michielsen, K.; Dresen, R.; Vanslembrouck, R.; De Keyzer, F.; Amant, F.; Mussen, E.; Leunen, K.; Berteloot, P.; Moerman, P.; Vergote, I. Diagnostic value of whole body diffusion-weighted MRI compared to computed tomography for pre-operative assessment of patients suspected for ovarian cancer. Eur. J. Cancer 2017, 83, 88–98. [Google Scholar] [CrossRef]
- Nasser, S.; Lazaridis, A.; Evangelou, M.; Jones, B.; Nixon, K.; Kyrgiou, M.; Gabra, H.; Rockall, A.; Fotopoulou, C. Correlation of pre-operative CT findings with surgical & histological tumor dissemination patterns at cytoreduction for primary advanced and relapsed epithelial ovarian cancer: A retrospective evaluation. Gynecol. Oncol. 2016, 143, 264–269. [Google Scholar]
- Nougaret, S.; Addley, H.C.; Colombo, P.E.; Fujii, S.; Al Sharif, S.S.; Tirumani, S.H.; Jardon, K.; Sala, E.; Reinhold, C. Ovarian carcinomatosis: How the radiologist can help plan the surgical approach. Radiographics 2012, 32, 1775–1800; discussion 1800-3. [Google Scholar] [CrossRef] [Green Version]
- Petrillo, M.; Vizzielli, G.; Fanfani, F.; Gallotta, V.; Cosentino, F.; Chiantera, V.; Legge, F.; Carbone, V.; Scambia, G.; Fagotti, A. Definition of a dynamic laparoscopic model for the prediction of incomplete cytoreduction in advanced epithelial ovarian cancer: Proof of a concept. Gynecol. Oncol. 2015, 139, 5–9. [Google Scholar] [CrossRef]
- Suidan, R.S.; Ramirez, P.T.; Sarasohn, D.M.; Teitcher, J.B.; Iyer, R.B.; Zhou, Q.; Iasonos, A.; Denesopolis, J.; Zivanovic, O.; Long Roche, K.C.; et al. A multicenter assessment of the ability of preoperative computed tomography scan and CA-125 to predict gross residual disease at primary debulking for advanced epithelial ovarian cancer. Gynecol. Oncol. 2017, 145, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Vergote, I.B.; Van Nieuwenhuysen, E.; Vanderstichele, A. How to Select Neoadjuvant Chemotherapy or Primary Debulking Surgery in Patients With Stage IIIC or IV Ovarian Carcinoma. J. Clin. Oncol. 2016, 34, 3827–3828. [Google Scholar] [CrossRef]
- Zhou, M.; Wang, D.; Long, Z.; Zhang, Y.; Liu, J. Role of Laparotomy-based Parameters in Assessment of Optimal Primary Debulking Surgery and Long-term Outcomes in Patients with Stage IIIC Epithelial Ovarian Cancer. J. Cancer 2020, 11, 983–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dowdy, S.C.; ullany, S.A.; Brandt, K.R.; Huppert, B.J.; Cliby, W.A. The utility of computed tomography scans in predicting suboptimal cytoreductive surgery in women with advanced ovarian carcinoma. Cancer 2004, 101, 346–352. [Google Scholar] [CrossRef]
- Suidan, R.S.; Ramirez, P.T.; Sarasohn, D.M.; Teitcher, J.B.; Mironov, S.; Iyer, R.B.; Zhou, Q.; Iasonos, A.; Paul, H.; Hosaka, M.; et al. A multicenter prospective trial evaluating the ability of preoperative computed tomography scan and serum CA-125 to predict suboptimal cytoreduction at primary debulking surgery for advanced ovarian, fallopian tube, and peritoneal cancer. Gynecol. Oncol. 2014, 134, 455–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutten, M.J.; van Meurs, H.S.; van de Vrie, R.; Gaarenstroom, K.N.; Naaktgeboren, C.A.; van Gorp, T.; Ter Brugge, H.G.; Hofhuis, W.; Schreuder, H.W.; Arts, H.J.; et al. Laparoscopy to Predict the Result of Primary Cytoreductive Surgery in Patients With Advanced Ovarian Cancer: A Randomized Controlled Trial. J. Clin. Oncol. 2017, 35, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Borley, J.; Wilhelm-Benartzi, C.; Yazbek, J.; Williamson, R.; Bharwani, N.; Stewart, V.; Carson, I.; Hird, E.; McIndoe, A.; Farthing, A.; et al. Radiological predictors of cytoreductive outcomes in patients with advanced ovarian cancer. BJOG 2015, 122, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Bristow, R.E.; Duska, L.R.; Lambrou, N.C.; Fishman, E.K.; O’Neill, M.J.; Trimble, E.L.; Montz, F.J. A model for predicting surgical outcome in patients with advanced ovarian carcinoma using computed tomography. Cancer 2000, 89, 1532–1540. [Google Scholar] [CrossRef]
- Brun, J.L.; Rouzier, R.; Uzan, S.; Darai, E. External validation of a laparoscopic-based score to evaluate resectability of advanced ovarian cancers: Clues for a simplified score. Gynecol. Oncol. 2008, 110, 354–359. [Google Scholar] [CrossRef]
- Fagotti, A.; Ferrandina, G.; Fanfani, F.; Ercoli, A.; Lorusso, D.; Rossi, M.; Scambia, G. A laparoscopy-based score to predict surgical outcome in patients with advanced ovarian carcinoma: A pilot study. Ann. Surg. Oncol. 2006, 13, 1156–1161. [Google Scholar] [CrossRef]
- Forstner, R.; Sala, E.; Kinkel, K.; Spencer, J.A.; European Society of Urogenital, Radiology. ESUR guidelines: Ovarian cancer staging and follow-up. Eur. Radiol. 2010, 20, 2773–2780. [Google Scholar] [CrossRef]
- Fuso, L.; Ferrero, A.; Vietti, E.; Petracchini, M.; Mineccia, M.; Villa, M.; Menato, G. Development of a preoperative computed tomography score for the management of advanced epithelial ovarian cancer. Int. J. Gynecol. Cancer 2019, 29, 599–604. [Google Scholar] [CrossRef]
- Risum, S.; Hogdall, C.; Loft, A.; Berthelsen, A.K.; Hogdall, E.; Nedergaard, L.; Lundvall, L.; Engelholm, S.A. Prediction of suboptimal primary cytoreduction in primary ovarian cancer with combined positron emission tomography/computed tomography--a prospective study. Gynecol. Oncol. 2008, 108, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, S.; De Piano, F.; Buscarino, V.; Pagan, E.; Bagnardi, V.; Zanagnolo, V.; Colombo, N.; Maggioni, A.; Del Grande, M.; Del Grande, F.; et al. Pre-operative evaluation of epithelial ovarian cancer patients: Role of whole body diffusion weighted imaging MR and CT scans in the selection of patients suitable for primary debulking surgery. A single-centre study. Eur. J. Radiol. 2020, 123, 108786. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.; Meuli, R.A.; Achtari, C.; Prior, J.O. Peritoneal carcinomatosis in primary ovarian cancer staging: Comparison between MDCT, MRI, and 18F-FDG PET/CT. Clin. Nucl. Med. 2015, 40, 371–377. [Google Scholar] [CrossRef] [Green Version]
- Testa, A.C.; Ludovisi, M.; Mascilini, F.; Di Legge, A.; Malaggese, M.; Fagotti, A.; Fanfani, F.; Salerno, M.G.; Ercoli, A.; Scambia, G.; et al. Ultrasound evaluation of intra-abdominal sites of disease to predict likelihood of suboptimal cytoreduction in advanced ovarian cancer: A prospective study. Ultrasound Obstet. Gynecol. 2012, 39, 99–105. [Google Scholar] [CrossRef]
- Ferrandina, G.; Sallustio, G.; Fagotti, A.; Vizzielli, G.; Paglia, A.; Cucci, E.; Margariti, A.; Aquilani, L.; Garganese, G.; Scambia, G. Role of CT scan-based and clinical evaluation in the preoperative prediction of optimal cytoreduction in advanced ovarian cancer: A prospective trial. Br. J. Cancer. 2009, 101, 1066–1073. [Google Scholar] [CrossRef] [Green Version]
- Nelson, B.E.; Rosenfield, A.; Schwartz, P. Preoperative abdominopelvic computed tomographic prediction of optimal cytoreduction in epithelial ovarian carcinoma. J. Clin. Oncol. 1993, 11, 166–172. [Google Scholar] [CrossRef]
- Son, H.M.; Kim, S.H.; Kwon, B.R.; Kim, M.J.; Kim, C.S.; Cho, S.H. Preoperative prediction of suboptimal resection in advanced ovarian cancer based on clinical and CT parameters. Acta Radiol. 2017, 58, 498–504. [Google Scholar] [CrossRef]
- Shim, S.H.; Lee, S.J.; Kim, S.O.; Kim, S.N.; Kim, D.Y.; Lee, J.J.; Kim, J.H.; Kim, Y.M.; Kim, Y.T.; Nam, J.H. Nomogram for predicting incomplete cytoreduction in advanced ovarian cancer patients. Gynecol. Oncol. 2015, 136, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Kasper, S.M.; Dueholm, M.; Marinovskij, E.; Blaakaer, J. Imaging diagnostics in ovarian cancer: Magnetic resonance imaging and a scoring system guiding choice of primary treatment. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 210, 83–89. [Google Scholar] [CrossRef]
- Pinto, P.; Chiappa, V.; Alcazar, J.; Franchi, D.; Testa, A.C.; Cibula, D.; Valentin, L.; Fischerová, D. OC11.01: Preoperative assessment of non-resectability in patients with ovarian cancer using imaging (ISAAC study): An interim analysis. Ultrasound Obstet. Gynecol. 2022, 60, 31. [Google Scholar]
- Mert, I.; Kumar, A.; Sheedy, S.P.; Weaver, A.L.; McGree, M.E.; Kim, B.; Cliby, W.A. Clinical significance of enlarged cardiophrenic lymph nodes in advanced ovarian cancer: Implications for survival. Gynecol. Oncol. 2018, 148, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Shinagare, A.B.; Gujrathi, I.; Cochon, L.; Burk, K.S.; Sadowski, E.; Khorasani, R. Predictors of malignancy in incidental adnexal lesions identified on CT in patients with prior non-ovarian cancer. Abdom. Radiol. 2022, 47, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Heitz, F.; Harter, P.; Alesina, P.F.; Walz, M.K.; Lorenz, D.; Groeben, H.; Heikaus, S.; Fisseler-Eckhoff, A.; Schneider, S.; Ataseven, B. Pattern of and reason for postoperative residual disease in patients with advanced ovarian cancer following upfront radical debulking surgery. Gynecol. Oncol. 2016, 141, 264–270. [Google Scholar] [CrossRef]
- Vergote, I.; Coens, C.; Nankivell, M.; Kristensen, G.B.; Parmar, M.K.B.; Ehlen, T.; Jayson, G.C.; Johnson, N.; Swart, A.M.; Verheijen, R. Neoadjuvant chemotherapy versus debulking surgery in advanced tubo-ovarian cancers: Pooled analysis of individual patient data from the EORTC 55971 and CHORUS trials. Lancet Oncol. 2018, 19, 1680–1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vergote, I.; du Bois, A.; Amant, F.; Heitz, F.; Leunen, K.; Harter, P. Neoadjuvant chemotherapy in advanced ovarian cancer: On what do we agree and disagree? Gynecol. Oncol. 2013, 128, 6–11. [Google Scholar] [CrossRef]
- Jacquet, P.; Sugarbaker, P. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer Treat. Res. 1996, 82, 359–374. [Google Scholar]
- Chereau, E.; Ballester, M.; Selle, F.; Cortez, A.; Darai, E.; Rouzier, R. Comparison of peritoneal carcinomatosis scoring methods in predicting resectability and prognosis in advanced ovarian cancer. Am. J. Obstet. Gynecol. 2010, 202, 178.e1–178.e10. [Google Scholar] [CrossRef]
- Gasimli, K.; Braicu, E.I.; Richter, R.; Chekerov, R.; Sehouli, J. Prognostic and Predictive Value of the Peritoneal Cancer Index in Primary Advanced Epithelial Ovarian Cancer Patients After Complete Cytoreductive Surgery: Study of Tumor Bank Ovarian Cancer. Ann. Surg. Oncol. 2015, 22, 2729–2737. [Google Scholar] [CrossRef] [PubMed]
- Lampe, B.; Kroll, N.; Piso, P.; Forner, D.M.; Mallmann, P. Prognostic significance of Sugarbaker’s peritoneal cancer index for the operability of ovarian carcinoma. Int. J. Gynecol. Cancer 2015, 25, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Gouy, S.; Belghiti, J.; Uzan, C.; Canlorbe, G.; Gauthier, T.; Morice, P. Accuracy and reproducibility of the peritoneal cancer index in advanced ovarian cancer during laparoscopy and laparotomy. Int. J. Gynecol. Cancer 2013, 23, 1699–1703. [Google Scholar] [CrossRef]
- Querleu, D.; Planchamp, F.; Chiva, L.; Fotopoulou, C.; Barton, D.; Cibula, D.; Aletti, G.; Carinelli, S.; Creutzberg, C.; Davidson, B.; et al. European Society of Gynaecologic Oncology Quality Indicators for Advanced Ovarian Cancer Surgery. Int. J. Gynecol. Cancer 2016, 26, 1354–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, S.A.; Abou-Taleb, H.; Yehia, A.; El Malek, N.A.A.; Siefeldein, G.S.; Badary, D.M.; Jabir, M.A. The accuracy of multi-detector computed tomography and laparoscopy in the prediction of peritoneal carcinomatosis index score in primary ovarian cancer. Acad. Radiol. 2019, 26, 1650–1658. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Wen, H.; Jiang, Z.; Liu, S.; Ju, X.; Chen, X.; Xia, L.; Xu, J.; Bi, R.; Wu, X. A triage strategy in advanced ovarian cancer management based on multiple predictive models for R0 resection: A prospective cohort study. J. Gynecol. Oncol. 2018, 29, e65. [Google Scholar] [CrossRef] [PubMed]
- Gu, B.; Xia, L.; Ge, H.; Liu, S. Preoperative PET/CT score can predict complete resection in advanced epithelial ovarian cancer: A prospective study. Quant. Imaging Med. Surg. 2020, 10, 743–753. [Google Scholar] [CrossRef]
- Jonsdottir, B.; Lomnytska, M.; Poromaa, I.S.; Silins, I.; Stalberg, K. The Peritoneal Cancer Index is a Strong Predictor of Incomplete Cytoreductive Surgery in Ovarian Cancer. Ann. Surg. Oncol. 2021, 28, 244–251. [Google Scholar] [CrossRef]
- Rosendahl, M.; Harter, P.; Bjorn, S.F.; Hogdall, C. Specific Regions, Rather than the Entire Peritoneal Carcinosis Index, are Predictive of Complete Resection and Survival in Advanced Epithelial Ovarian Cancer. Int. J. Gynecol. Cancer 2018, 28, 316–322. [Google Scholar] [CrossRef]
- Llueca, A.; Serra, A.; Rivadulla, I.; Gomez, L.; Escrig, J. Prediction of suboptimal cytoreductive surgery in patients with advanced ovarian cancer based on preoperative and intraoperative determination of the peritoneal carcinomatosis index. World J. Surg. Oncol. 2018, 16, 37. [Google Scholar] [CrossRef] [Green Version]
- Fischerova, D.; Pinto, P.; Burgetova, A.; Masek, M.; Slama, J.; Kocian, R.; Fruhauf, F.; Zikan, M.; Dusek, L.; Dundr, P.; et al. Preoperative staging of ovarian cancer: Comparison between ultrasound, CT and whole-body diffusion-weighted MRI (ISAAC study). Ultrasound Obstet. Gynecol. 2022, 59, 248–262. [Google Scholar] [CrossRef]
- Axtell, A.E.; Lee, M.H.; Bristow, R.E.; Dowdy, S.C.; Cliby, W.A.; Raman, S.; Weaver, J.P.; Gabbay, M.; Ngo, M.; Lentz, S.; et al. Multi-institutional reciprocal validation study of computed tomography predictors of suboptimal primary cytoreduction in patients with advanced ovarian cancer. J. Clin. Oncol. 2007, 25, 384–389. [Google Scholar] [CrossRef]
- Gerestein, C.G.; Eijkemans, M.J.; Bakker, J.; Elgersma, O.E.; van der Burg, M.E.; Kooi, G.S.; Burger, C.W. Nomogram for suboptimal cytoreduction at primary surgery for advanced stage ovarian cancer. Anticancer Res. 2011, 31, 4043–4049. [Google Scholar]
- Janco, J.M.; Glaser, G.; Kim, B.; McGree, M.E.; Weaver, A.L.; Cliby, W.A.; Dowdy, S.C.; Bakkum-Gamez, J.N. Development of a prediction model for residual disease in newly diagnosed advanced ovarian cancer. Gynecol. Oncol. 2015, 138, 70–77. [Google Scholar] [CrossRef]
- Kumar, A.; Sheedy, S.; Kim, B.; Suidan, R.; Sarasohn, D.M.; Nikolovski, I.; Lakhman, Y.; McGree, M.E.; Weaver, A.L.; Chi, D.; et al. Models to predict outcomes after primary debulking surgery: Independent validation of models to predict suboptimal cytoreduction and gross residual disease. Gynecol. Oncol. 2019, 154, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Avesani, G.; Arshad, M.; Lu, H.; Fotopoulou, C.; Cannone, F.; Melotti, R.; Aboagye, E.; Rockall, A. Radiological assessment of Peritoneal Cancer Index on preoperative CT in ovarian cancer is related to surgical outcome and survival. Radiol. Med. 2020, 125, 770–776. [Google Scholar] [CrossRef]
- Chong, G.O.; Jeong, S.Y.; Lee, Y.H.; Lee, H.J.; Lee, S.W.; Han, H.S.; Hong, D.G.; Lee, Y.S. The ability of whole-body SUVmax in F-18 FDG PET/CT to predict suboptimal cytoreduction during primary debulking surgery for advanced ovarian cancer. J. Ovarian Res. 2019, 12, 12. [Google Scholar] [CrossRef] [Green Version]
- Fagotti, A.; Ferrandina, G.; Fanfani, F.; Garganese, G.; Vizzielli, G.; Carone, V.; Salerno, M.G.; Scambia, G. Prospective validation of a laparoscopic predictive model for optimal cytoreduction in advanced ovarian carcinoma. Am. J. Obstet. Gynecol. 2008, 199, 642.e1–646.ei. [Google Scholar] [CrossRef] [PubMed]
- Varnoux, C.; Huchon, C.; Bats, A.S.; Bensaid, C.; Achouri, A.; Nos, C.; Lecuru, F. Diagnostic accuracy of hand-assisted laparoscopy in predicting resectability of peritoneal carcinomatosis from gynecological malignancies. Eur. J. Surg. Oncol. 2013, 39, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Tomar, T.S.; Nair, R.P.; Sambasivan, S.; Krishna, K.M.J.; Mathew, A.; Ahmed, I.M. Role of laparoscopy in predicting surgical outcomes in patients undergoing interval cytoreduction surgery for advanced ovarian carcinoma: A prospective validation study. Indian J. Cancer 2017, 54, 550–555. [Google Scholar]
- Ghisoni, E.; Katsaros, D.; Maggiorotto, F.; Aglietta, M.; Vaira, M.; De Simone, M.; Mittica, G.; Giannone, G.; Robella, M.; Genta, S.; et al. A predictive score for optimal cytoreduction at interval debulking surgery in epithelial ovarian cancer: A two- centers experience. J. Ovarian Res. 2018, 11, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, J.M.; Sood, A.K.; Coleman, R.L.; Westin, S.N.; Soliman, P.T.; Ramirez, P.T.; Fellman, B.M.; Schmeler, K.M.; Fleming, N.D. Concordance of a laparoscopic scoring algorithm with primary surgery findings in advanced stage ovarian cancer. Gynecol. Oncol. 2018, 151, 428–432. [Google Scholar] [CrossRef]
- Angeles, M.A.; Migliorelli, F.; Del, M.; Martinez-Gomez, C.; Daix, M.; Betrian, S.; Gabiache, E.; Balague, G.; Leclerc, S.; Mery, E.; et al. Concordance of laparoscopic and laparotomic peritoneal cancer index using a two-step surgical protocol to select patients for cytoreductive surgery in advanced ovarian cancer. Arch. Gynecol. Obstet. 2021, 303, 1295–1304. [Google Scholar] [CrossRef]
- Climent, M.T.; Serra, A.; Gilabert-Estelles, J.; Gilabert-Aguilar, J.; Llueca, A. Comparison of Peritoneal Carcinomatosis Scoring Methods in Predicting Resectability and Prognosis in Gynecologic Malignancies. J. Clin. Med. 2021, 10, 2553. [Google Scholar] [CrossRef]
- Llueca, A.; Climent, M.T.; Escrig, J.; Carrasco, P.; Serra, A.; MUAPOS working group (Multidisciplinary Unit of Abdominal Pelvic Oncology Surgery). Validation of three predictive models for suboptimal cytoreductive surgery in advanced ovarian cancer. Sci. Rep. 2021, 11, 8111. [Google Scholar] [CrossRef] [PubMed]
- Fagotti, A.; Perelli, F.; Pedone, L.; Scambia, G. Current Recommendations for Minimally Invasive Surgical Staging in Ovarian Cancer. Curr. Treat. Options Oncol. 2016, 17, 3. [Google Scholar] [CrossRef] [PubMed]
- Vergote, I.; De Wever, I.; Tjalma, W.; Van Gramberen, M.; Decloedt, J.; van Dam, P. Neoadjuvant chemotherapy or primary debulking surgery in advanced ovarian carcinoma: A retrospective analysis of 285 patients. Gynecol. Oncol. 1998, 71, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Fagotti, A.; Vizzielli, G.; De Iaco, P.; Surico, D.; Buda, A.; Mandato, V.D.; Petruzzelli, F.; Ghezzi, F.; Garzarelli, S.; Mereu, L.; et al. A multicentric trial (Olympia-MITO 13) on the accuracy of laparoscopy to assess peritoneal spread in ovarian cancer. Am. J. Obstet. Gynecol. 2013, 209, 462.e1–462.e11. [Google Scholar] [CrossRef]
- Van de Vrie, R.; Rutten, M.J.; Asseler, J.D.; Leeflang, M.M.; Kenter, G.G.; Mol, B.W.J.; Buist, M. Laparoscopy for diagnosing resectability of disease in women with advanced ovarian cancer. Cochrane Database Syst. Rev. 2019, 3, CD009786. [Google Scholar] [CrossRef]
- Lomnytska, M.; Karlsson, E.; Jonsdottir, B.; Lejon, A.M.; Stalberg, K.; Poromaa, I.S.; Silins, I.; Graf, W. Peritoneal cancer index predicts severe complications after ovarian cancer surgery. Eur. J. Surg. Oncol. 2021, 47, 2915–2924. [Google Scholar] [CrossRef]
- Llueca, A.; Escrig, J.; MUAPOS working group (Multidisciplinary Unit of Abdominal Pelvic Oncology Surgery). Prognostic value of peritoneal cancer index in primary advanced ovarian cancer. Eur. J. Surg. Oncol. 2018, 44, 163–169. [Google Scholar] [CrossRef]
- Diaz-Gil, D.; Fintelmann, F.J.; Molaei, S.; Elmi, A.; Hedgire, S.S.; Harisinghani, M.G. Prediction of 5-year survival in advanced-stage ovarian cancer patients based on computed tomography peritoneal carcinomatosis index. Abdom. Radiol. 2016, 41, 2196–2202. [Google Scholar] [CrossRef]
- Sartor, H.; Bjurberg, M.; Asp, M.; Kahn, A.; Brandstedt, J.; Kannisto, P.; Jirstrom, K. Ovarian cancer subtypes and survival in relation to three comprehensive imaging parameters. J. Ovarian. Res. 2020, 13, 26. [Google Scholar] [CrossRef] [Green Version]
- Alcazar, J.L.; Caparros, M.; Arraiza, M.; Minguez, J.A.; Guerriero, S.; Chiva, L.; Jurado, M. Pre-operative assessment of intra-abdominal disease spread in epithelial ovarian cancer: A comparative study between ultrasound and computed tomography. Int. J. Gynecol. Cancer 2019, 29, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Fischerova, D.; Zikan, M.; Semeradova, I.; Slama, J.; Kocian, R.; Dundr, P.; Nemejcova, K.; Burgetova, A.; Dusek, L.; Cibula, D. Ultrasound in preoperative assessment of pelvic and abdominal spread in patients with ovarian cancer: A prospective study. Ultrasound Obstet. Gynecol. 2017, 49, 263–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tempany, C.M.; Zou, K.H.; Silverman, S.G.; Brown, D.L.; Kurtz, A.B.; McNeil, B.J. Staging of advanced ovarian cancer: Comparison of imaging modalities--report from the Radiological Diagnostic Oncology Group. Radiology 2000, 215, 761–767. [Google Scholar] [CrossRef]
- Epstein, E.; Van Calster, B.; Timmerman, D.; Nikman, S. Subjective ultrasound assessment, the ADNEX model and ultrasound-guided tru-cut biopsy to differentiate disseminated primary ovarian cancer from metastatic non-ovarian cancer. Ultrasound Obstet. Gynecol. 2016, 47, 110–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischerova, D.; Cibula, D.; Dundr, P.; Zikan, M.; Calda, P.; Freitag, P.; Slama, J. Ultrasound-guided tru-cut biopsy in the management of advanced abdomino-pelvic tumors. Int. J. Gynecol. Cancer 2008, 18, 833–837. [Google Scholar] [CrossRef]
- Zikan, M.; Fischerova, D.; Pinkavova, I.; Dundr, P.; Cibula, D. Ultrasound-guided tru-cut biopsy of abdominal and pelvic tumors in gynecology. Ultrasound Obstet. Gynecol. 2010, 36, 767–772. [Google Scholar] [CrossRef]
- Expert Panel on Women’s Imaging; Kang, S.K.; Reinhold, C.; Atri, M.; Benson, C.B.; Bhosale, P.R.; Jhingran, A.; Lakhman, Y.; Maturen, K.E.; Nicola, R.; et al. ACR Appropriateness Criteria((R)) Staging and Follow-Up of Ovarian Cancer. J. Am. Coll. Radiol. 2018, 15, S198–S207. [Google Scholar] [CrossRef]
- Michielsen, K.; Vergote, I.; Op de Beeck, K.; Amant, F.; Leunen, K.; Moerman, P.; Deroose, C.; Souverijns, G.; Dymarkowski, S.; De Keyzer, F.; et al. Whole-body MRI with diffusion-weighted sequence for staging of patients with suspected ovarian cancer: A clinical feasibility study in comparison to CT and FDG-PET/CT. Eur. Radiol. 2014, 24, 889–901. [Google Scholar] [CrossRef]
- Bharwani, N.; Reznek, R.; Rockall, A. Ovarian Cancer Management: The role of imaging and diagnostic challenges. Eur. J. Radiol. 2011, 78, 41–51. [Google Scholar] [CrossRef]
- Garcia Prado, J.; Gonzalez Hernando, C.; Varillas Delgado, D.; Saiz Martinez, R.; Bhosale, P.; Blazquez Sanchez, J.; Chiva, L. Diffusion-weighted magnetic resonance imaging in peritoneal carcinomatosis from suspected ovarian cancer: Diagnostic performance in correlation with surgical findings. Eur. J. Radiol. 2019, 121, 108696. [Google Scholar] [CrossRef]
- Kitajima, K.; Murakami, K.; Yamasaki, E.; Kaji, Y.; Fukasawa, I.; Inaba, N.; Sugimura, K. Diagnostic accuracy of integrated FDG-PET/contrast-enhanced CT in staging ovarian cancer: Comparison with enhanced CT. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 1912–1920. [Google Scholar] [CrossRef] [PubMed]
- Hynninen, J.; Kemppainen, J.; Lavonius, M.; Virtanen, J.; Matomaki, J.; Oksa, S.; Carpen, O.; Grenman, S.; Seppanen, M.; Auranen, A. A prospective comparison of integrated FDG-PET/contrast-enhanced CT and contrast-enhanced CT for pretreatment imaging of advanced epithelial ovarian cancer. Gynecol. Oncol. 2013, 131, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Liu, S.; Ju, X.; Chen, X.; Li, R.; Bi, R.; Wu, X. Diagnostic accuracy of (18)F-FDG PET/CT scan for peritoneal metastases in advanced ovarian cancer. Quant. Imaging Med. Surg. 2021, 11, 3392–3398. [Google Scholar] [CrossRef] [PubMed]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- American Society of Anesthesiologists. ASA Physical Status Classification System. Available online: https://www.asahq.org/standards-and-guidelines/asa-physical-status-classification-system (accessed on 29 November 2022).
- Forstner, R.; Meissnitzer, M.; Cunha, T. Update on Imaging of Ovarian Cancer. Curr. Radiol. Rep. 2016, 4, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pichler, B.J.; Wehrl, H.F.; Kolb, A.; Judenhofer, M.S. Positron emission tomography/magnetic resonance imaging: The next generation of multimodality imaging? Semin. Nucl. Med. 2008, 38, 199–208. [Google Scholar] [CrossRef] [Green Version]
- Satoh, Y.; Ichikawa, T.; Motosugi, U.; Kimura, K.; Sou, H.; Sano, K.; Araki, T. Diagnosis of peritoneal dissemination: Comparison of 18F-FDG PET/CT, diffusion-weighted MRI, and contrast-enhanced MDCT. AJR Am. J. Roentgenol. 2011, 196, 447–453. [Google Scholar] [CrossRef]
- Thomassin-Naggara, I.; Toussaint, I.; Perrot, N.; Rouzier, R.; Cuenod, C.A.; Bazot, M.; Darai, E. Characterization of complex adnexal masses: Value of adding perfusion- and diffusion-weighted MR imaging to conventional MR imaging. Radiology 2011, 258, 793–803. [Google Scholar] [CrossRef]
- Vandecaveye, V.; Dresen, R.; De Keyzer, F. Novel imaging techniques in gynaecological cancer. Curr. Opin. Oncol. 2017, 29, 335–342. [Google Scholar] [CrossRef]
- Dai, G.; Liang, K.; Xiao, Z.; Yang, Q.; Yang, S. A meta-analysis on the diagnostic value of diffusion-weighted imaging on ovarian cancer. J. BUON 2019, 24, 2333–2340. [Google Scholar]
- Vandecaveye, V.D.R. Whole Body Diffusion-Weighted MRI in Ovarian Cancer Staging. J. Belg. Soc. Radiol. 2019, 103, 70. [Google Scholar] [CrossRef] [Green Version]
- Fischerova, D.; Burgetova, A. Imaging techniques for the evaluation of ovarian cancer. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 697–720. [Google Scholar] [CrossRef]
- Kurokawa, T.; Yoshida, Y.; Kawahara, K.; Tsuchida, T.; Okazawa, H.; Fujibayashi, Y.; Yonekura, Y.; Kotsuji, F. Expression of GLUT-1 glucose transfer, cellular proliferation activity and grade of tumor correlate with [F-18]-fluorodeoxyglucose uptake by positron emission tomography in epithelial tumors of the ovary. Int. J. Cancer 2004, 109, 926–932. [Google Scholar] [CrossRef] [PubMed]
- Tanizaki, Y.; Kobayashi, A.; Shiro, M.; Ota, N.; Takano, R.; Mabuchi, Y.; Yagi, S.; Minami, S.; Terada, M.; Ino, K. Diagnostic value of preoperative SUVmax on FDG-PET/CT for the detection of ovarian cancer. Int. J. Gynecol. Cancer 2014, 24, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Dauwen, H.; Van Calster, B.; Deroose, C.M.; Op de Beeck, K.; Amant, F.; Neven, P.; Berteloot, P.; Leunen, K.; Timmerman, D.; Vergote, I. PET/CT in the staging of patients with a pelvic mass suspicious for ovarian cancer. Gynecol. Oncol. 2013, 131, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Nam, E.J.; Yun, M.J.; Oh, Y.T.; Kim, J.W.; Kim, J.H.; Kim, S.; Jung, Y.W.; Kim, S.W.; Kim, Y.T. Diagnosis and staging of primary ovarian cancer: Correlation between PET/CT, Doppler US, and CT or MRI. Gynecol. Oncol. 2010, 116, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Castellucci, P.; Perrone, A.M.; Picchio, M.; Ghi, T.; Farsad, M.; Nanni, C.; Messa, C.; Meriggiola, M.C.; Pelusi, G.; Al-Nahhas, A.; et al. Diagnostic accuracy of 18F-FDG PET/CT in characterizing ovarian lesions and staging ovarian cancer: Correlation with transvaginal ultrasonography, computed tomography, and histology. Nucl. Med. Commun. 2007, 28, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Khiewvan, B.; Torigian, D.A.; Emamzadehfard, S.; Paydary, K.; Salavati, A.; Houshmand, S.; Werner, T.J.; Alavi, A. An update on the role of PET/CT and PET/MRI in ovarian cancer. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1079–1091. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
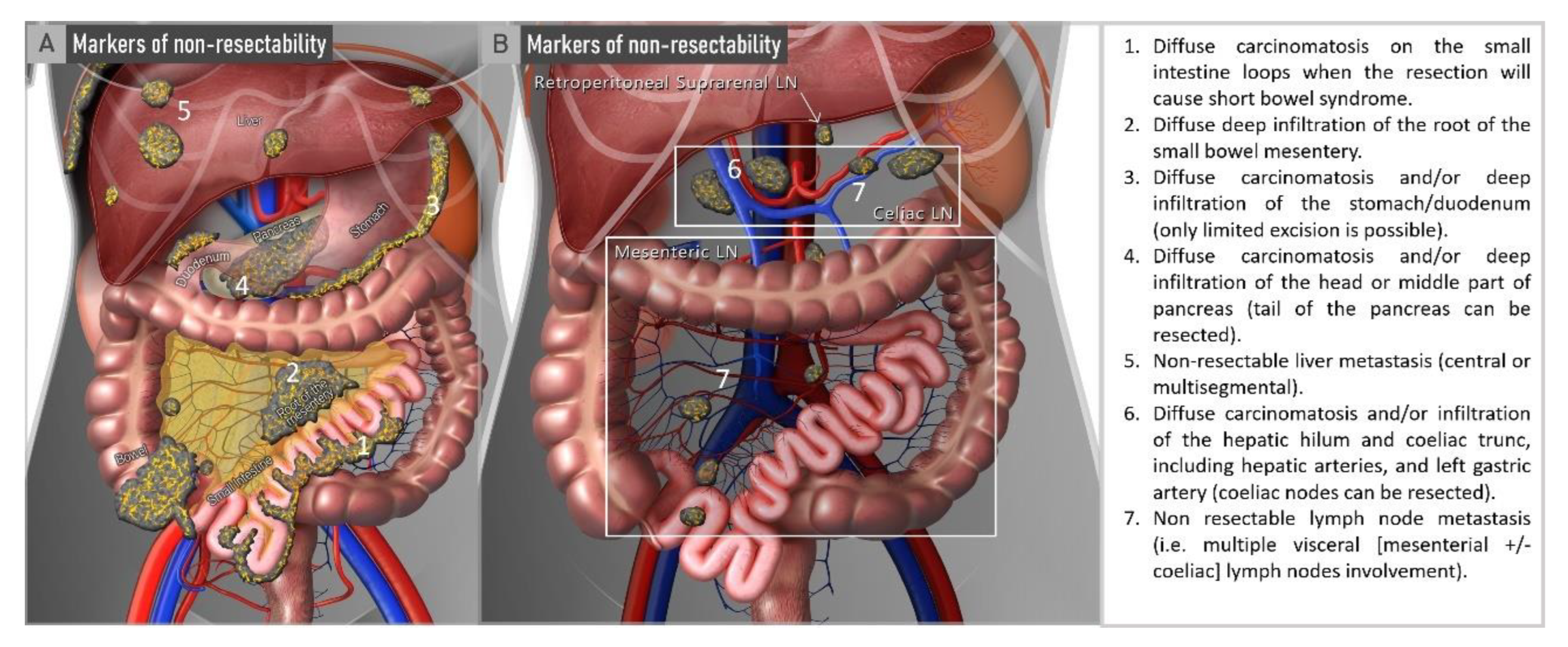
| ESMO-ESGO Markers of Non-Resectability | References (n = 29) | % (n) |
|---|---|---|
| Diffuse carcinomatosis of the small bowel involving such large parts that resection would lead to short bowel syndrome (remaining bowel < 1.5 m) | [32,33,34,35,36,37,38,39,40,41,42,43,44,45] | 48 (14/29) |
| Diffuse deep infiltration of the root of small bowel mesentery | [32,33,34,35,36,37,38,39,40,41,42,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60] | 97 (28/29) |
| Diffuse involvement/deep infiltration of: Stomach/duodenum; Head or middle part of pancreas. | [32,33,36,39,41,42,48,49,51] | 31 (9/29) |
| Central or multisegmental parenchymal liver metastases | [32,33,34,38,39,41,42,48,49,50,51,57,60] | 45 (13/29) |
| Involvement of coeliac trunk, hepatic arteries or left gastric artery | [32,34,36,37,38,40,41,47,50,51,57,60] | 41 (12/29) |
| Non-resectable lymph node metastases | [34,36,38,40,41,42,47,50,51,52,56,57,58] | 45 (13/29) |
| Multiple parenchymal lung metastases (preferably histologically proven) | [35,36,41,43,46,57] | 17 (5/29) |
| Brain metastases | [35,36] | 7 (2/29) |
| Date | Study Type | Patients (n) | Type of Model | Imaging Modality (Cut-Off 1) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Accuracy (%) | AUC | Outcome | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ULTRASOUND | ||||||||||||
| Testa et al. [55] | 2012 | Prospective | 147 | Scoring system | >5 | 31 | 92 | 83 | 51 | 58 | - | >1 cm residual disease |
| Fischerova et al. [79] * | 2022 | Prospective | 67 | Multivariable analysis | - | 63 | 98 | 91 | 89 | 90 | 0.80 | >1 cm residual disease |
| CT | ||||||||||||
| Nelson et al. [57] | 1993 | Retrospective | 42 | Multivariable analysis | - | 92 | 79 | 67 | 96 | - | - | ≥2 cm residual disease |
| Bristow et al. [47] | 2000 | Retrospective | 41 | Scoring system | ≥4 | 100 | 85 | 88 | 100 | 93 | 0.97 | >1 cm residual disease |
| Dowdy et al. [43] | 2004 | Retrospective | 87 | Multivariable logistic regression | - | 52 | 90 | 68 | 82 | 79 | - | >1 cm residual disease |
| Axtell et al. [80] | 2007 | Retrospective | 65 | Multivariable logistic regression | - | 79 | 75 | 46 | 93 | 77 | - | >1 cm residual disease |
| Axtell et al. [80] | 2007 | Retrospective | 87 | External validation Axtell et al. | - | 72 | 56 | 48 | 78 | 64 | - | >1 cm residual disease |
| Ferrandina et al. [56] | 2009 | Prospective | 195 | Scoring system | - | 24 | 98 | 93 | 50 | 56 | 0.82 | >1 cm residual disease |
| Gerestein et al. [81] | 2011 | Multicentric prospective | 115 | Nomogram | - | - | - | - | - | 74 | 0.67 | >1 cm residual disease |
| Suidan et al. [44] | 2014 | Multicentric prospective | 350 | Scoring system | - | - | - | - | - | - | 0.76 | >1 cm residual disease |
| Janco et al. [82] | 2015 | Retrospective | 279 | Nomogram | - | - | - | - | - | - | 0.75 | Any visible disease |
| Borley et al. [46] | 2015 | Retrospective | 111 | Scoring system | - | 69 | 71 | 75 | 65 | - | 0.75 | >1 cm residual disease |
| Borley et al. [46] | 2015 | Retrospective | 70 | External validation Borley et al. | - | 65 | 68 | - | - | - | 0.72 | >1 cm residual disease |
| Son et al. [58] | 2016 | Retrospective | 220 | Scoring system | - | 71 | 74 | - | - | - | 0.79 | >1 cm residual disease |
| Son et al. [58] | 2016 | Prospective | 107 | External validation Son et al. | - | 69 | 73 | - | - | - | 0.76 | >1 cm residual disease |
| Suidan et al. [40] | 2017 | Multicentric prospective | 350 | Scoring system (same population of Suidan 2014 [44]) | ≥3 | 68 | 76 | 68 | 76 | 72 | 0.72 | Any visible disease |
| Michielsen et al. [36] * | 2017 | Prospective | 161 | Multivariable analysis | - | 66 | 77 | 77 | 67 | 71 | 0.72 | Any visible disease |
| Feng et al. [74] | 2018 | Prospective | 100 | External validation Suidan et al. [40] | ≥3 | - | - | - | - | - | 0.55 | Any visible disease |
| Llueca et al. [78] | 2018 | Retrospective | 49 | External validation PCI score | >20 | 27 | 91 | 33 | 89 | - | - | >1 cm residual disease |
| Fuso et al. [51] | 2019 | Retrospective | 61 | Scoring system | >8 | 85 | 100 | 100 | 60 | 92 | 0.95 | Any visible disease |
| Ahmed et al. [73] | 2019 | Prospective | 80 | External validation PCI score | <20 | 90 | 39 | 75 | 70 | 69 | - | ≥1 cm residual disease |
| Kumar et al. [83] | 2019 | Retrospective | 276 | External validation Suidan et al. [44] | - | - | - | - | - | - | 0.65 | >1 cm residual disease |
| Kumar et al. [83] | 2019 | Retrospective | 276 | External validation Suidan et al. [40] | - | - | - | - | - | - | 0.76 | Any visible disease |
| Avesani et al. [84] | 2020 | Retrospective | 297 | External validation PCI score | - | - | - | - | - | - | 0.64 | Any visible di-sease |
| Fischerova et al. [79] * | 2022 | Prospective | 67 | Multivariable analysis | - | 56 | 94 | 75 | 87 | 85 | 0.75 | >1 cm residual disease |
| WB-DWI/MRI | ||||||||||||
| Michielsen et al. [36] * | 2017 | Prospective | 161 | Multivariableanalysis | - | 94 | 98 | 98 | 94 | 96 | 0.96 | Any visible disease |
| Engbersen et al. [33] | 2019 | Prospective | 25 | External validation PCI score | <15 | 100 | 88 | - | - | - | 0.98 | Any visible di-sease |
| Rizzo et al. [53] | 2020 | Prospective | 92 | Nomogram | - | - | - | - | - | - | 0.88 | >1 cm residual disease |
| Fischerova et al. [79] * | 2022 | Prospective | 67 | Multivariableanalysis | - | 50 | 98 | 89 | 86 | 87 | 0.74 | >1 cm residual disease |
| PET/CT | ||||||||||||
| Shim et al. [59] | 2015 | Retrospective | 240 | Nomogram | - | 66 | 88 | - | - | - | 0.88 | Any visible disease |
| Shim et al. [59] | 2015 | Retrospective | 103 | External validation Shim et al. | - | - | - | - | - | - | 0.86 | Any visible disease |
| Alessi et al. [32] | 2016 | Prospective | 23 | Multivariable analysis | - | 100 | 100 | - | - | - | - | Any visible disease |
| Chong et al. [85] | 2019 | Retrospective | 51 | Scoring system | >10 | 82 | 65 | - | - | - | 0.78 | >1 cm residual disease |
| Chong et al. [85] | 2019 | Retrospective | 51 | External validation PCI score | - | - | - | - | - | - | 0.56 | >1 cm residual disease |
| Gu et al. [75] | 2020 | Prospective | 31 | External validation Suidan et al. [40] | - | - | - | - | - | - | 0.80 | Any visible disease |
| LAPAROSCOPY | ||||||||||||
| Fagotti et al. [49] | 2006 | Prospective | 64 | Fagottic score | ≥8 | 30 | 100 | 70 | 100 | 75 | - | >1 cm residual disease |
| Fagotti et al. [86] | 2008 | Prospective | 113 | External validation Fagotti score | ≥8 | 70 | 100 | 100 | 60 | - | - | >1 cm residual disease |
| Brun et al. [48] | 2008 | Retrospective | 55 | External validation Fagotti score | ≥8 | 46 | 89 | 89 | 44 | 60 | 0.74 | >1 cm residual disease |
| Brun et al. [48] | 2008 | Retrospective | 55 | Scoring system | ≥4 | 35 | 100 | 100 | 43 | 56 | 0.68 | >1 cm residual disease |
| Chéreau et al. [68] | 2010 | Retrospective | 61 | External validation Fagotti score | <8 | - | - | - | - | - | 0.66 | Any visible disease |
| Chéreau et al. [68] | 2010 | Retrospective | 61 | External validation Brun et al. [48] | <4 | - | - | - | - | - | 0.76 | Any visible disease |
| Varnoux et al. [87] | 2013 | Prospective | 29 | Multivariable analysis | - | 100 | 40 | 61 | 100 | - | 0.70 | Any visible disease |
| Varnoux et al. [87] | 2013 | Prospective | 29 | External validation Brun et al. [48] | ≥4 | 100 | 47 | 64 | 100 | 73 | - | Any visible disease |
| Varnoux et al. [87] | 2013 | Prospective | 29 | External validation Fagotti score | ≥8 | 100 | 47 | 64 | 100 | 73 | - | Any visible disease |
| Varnoux et al. [87] | 2013 | Prospective | 29 | External validation PCI score | ≥10 | 64 | 93 | 90 | 74 | 79 | - | Any visible disease |
| Petrillo et al. [39] | 2015 | Prospective | 135 | Scoring system | ≥10 | 47 | 97 | 100 | 67 | - | 0.89 | >1 cm residual disease |
| Rutten et al. [45] | 2017 | Multicentric prospective | 63 | Multivariable analysis | - | - | - | - | 84 | 84 | - | >1 cm residual disease |
| Tomar et al. [88] | 2017 | Prospective | 73 | External validation Fagotti score | ≥8 | 85 | 100 | 100 | 96 | 97 | 0.98 | >1 cm residual disease |
| Feng et al. [74] | 2018 | Prospective | 39 | External validation Fagotti score | <8 | - | - | - | - | - | 0.71 | Any visible disease |
| Ghisoni et al. [89] | 2018 | Multicentre retrospective | 65 | External validation PCI score | >16 | 63 | 90 | 71 | 86 | 82 | - | Any visible disease |
| Hansen et al. [90] | 2018 | Prospective | 226 | External validation Fagotti score | ≥8 | 71 | 49 | 85 | 29 | 67 | - | Any visible disease |
| Llueca et al. [78] | 2018 | Retrospective | 80 | External validation PCI score | >20 | 38 | 88 | 33 | 90 | - | - | >1 cm residual disease |
| Ahmed et al. [73] | 2019 | Prospective | 80 | External validation PCI score | <20 | 89 | 42 | 76 | 71 | 71 | - | ≥1 cm residual disease |
| Angeles et al. [91] | 2021 | Retrospective | 43 | External validation PCI score | - | - | - | - | - | - | 0.90 | Any visible disease |
| Climent et al. [92] | 2021 | Retrospective | 34 | External validation Fagotti score | ≥8 | 14 | 81 | 16 | 78 | 68 | 0.66 | >1 cm residual disease |
| Climent et al. [92] | 2021 | Retrospective | 34 | External validation PCI score | ≥20 | 43 | 88 | 50 | 78 | 79 | - | >1 cm residual disease |
| Llueca et al. [93] | 2021 | Retrospective | 103 | External validation Fagotti score | <4 | 86 | 74 | - | - | - | 0.83 | >1 cm residual disease |
| LAPAROTOMY | ||||||||||||
| Chéreau et al. [68] | 2010 | Prospective | 61 | External validation PCI score | <10 | - | - | - | - | - | 0.69 | Any visible disease |
| Espada et al. [34] | 2013 | Prospective | 34 | Scoring system | ≥4 | 88 | 89 | 70 | 96 | 88 | 0.95 | >1 cm residual disease |
| Lampe et al. [70] | 2015 | Retrospective | 98 | External validation PCI score | - | - | - | - | - | - | 0.84 | Any visible disease |
| Kasper et al. [60] | 2016 | Prospective | 99 | Scoring system | ≥14 | 70 | 94 | 83 | 88 | - | 91 | >1 cm residual disease |
| LLueca et al. [78] | 2018 | Retrospective | 80 | External validation PCI score | >20 | 73 | 81 | 38 | 95 | - | - | >1 cm residual disease |
| Rosendahl et al. [77] | 2018 | Prospective | 507 | External validation PCI score | - | - | - | - | - | - | 0.75 | Any visible disease |
| Rosendahl et al. [77] | 2018 | Prospective | 507 | Score (PCI-2 + 9–12) | 4 | 78 | 70 | - | - | - | 0.79 | Any visible disease |
| Ahmed et al. [73] | 2019 | Prospective | 80 | External validation PCI score | <20 | 91 | 83 | 88 | 90 | 89 | - | ≥1 cm residual disease |
| Engbersen et al. [33] | 2019 | Prospective | 25 | External validation PCI score | - | - | - | - | - | - | 0.92 | Any visible disease |
| Feng et al. [74] | 2018 | Prospective | 109 | External validation PCI score | - | - | - | - | - | - | 0.80 | Any visible disease |
| Gu et al. [75] | 2020 | Prospective | 31 | External validation PCI score | - | - | - | - | - | - | 0.81 | Any visible disease |
| Zhou et al. [42] | 2020 | Retrospective | 400 | Scoring system | - | - | - | - | - | - | 0.75 | >1 cm residual disease |
| Zhou et al. [42] | 2020 | Retrospective | 400 | External validation PCI score | - | - | - | - | - | - | 0.79 | >1 cm residual disease |
| Zhou et al. [42] | 2020 | Retrospective | 400 | External validation Petrillo et al. [39] | - | - | - | - | - | - | 0.74 | >1 cm residual disease |
| Jónsdóttir et al. [76] | 2021 | Prospective | 167 | External validation PCI score | ≥24 | - | - | - | - | - | 0.94 | Any visible disease |
| Parameters | Score 2 If: |
|---|---|
| Omental disease | Tumour infiltration of the greater omentum up to the large curvature of the stomach (infiltration of supracolic omentum) |
| Liver metastases | Any surface lesion larger than 2 cm |
| Lesser omentum and/or stomach and/or spleen involvement | Presence of obvious neoplastic involvement of the stomach and/or lesser omentum and/or spleen |
| Parietal peritoneal carcinomatosis | Massive peritoneal involvement and/or a miliaric pattern of distribution for parietal peritoneal carcinomatosis |
| Diaphragmatic disease | Widespread infiltrating carcinomatosis and/or confluent nodules to the most part of the diaphragmatic surface |
| Bowel infiltration | Large/small bowel infiltration (excluding recto-sigmoid involvement) * |
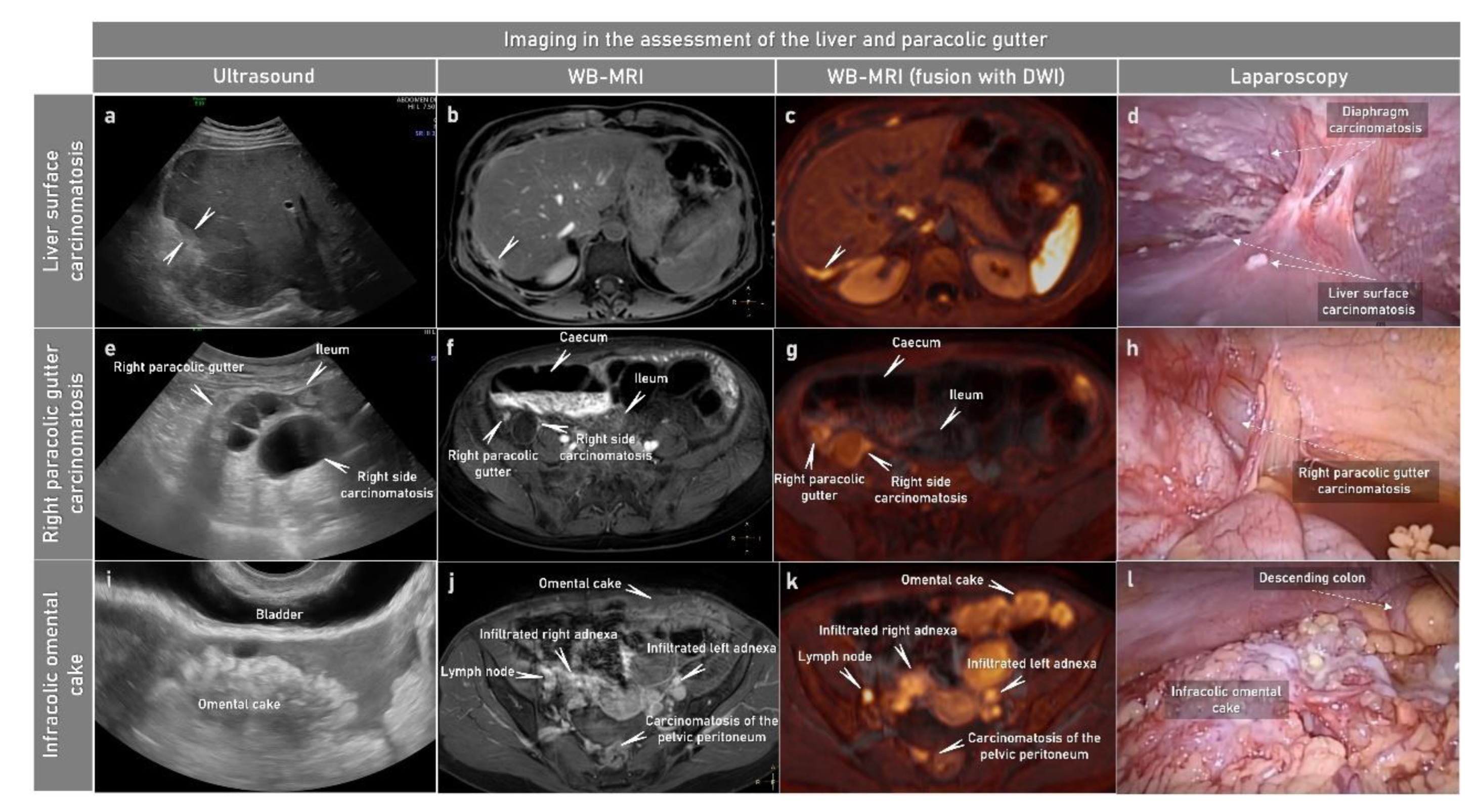
| Transvaginal and Transabdominal US | CE-CT | Whole-Body Diffusion-Weighted Imaging (DWI)/MRI | PET-CT | |
|---|---|---|---|---|
| Advantages | Low cost High availability Exam duration~15–20 min Dynamic examination No radiation exposure No patient preparation No contraindications Ultrasound-guided tru-cut biopsy | High availability Exam duration < 5 min No patient preparation CT-guided tru-cut biopsy of less accessible abdominal sites | Detection of small-volume disease (bowel serosa and mesentery) Differentiation of distant metastases and metastatic retroperitoneal-and supradiaphragmatic lymph nodes from benign processes No radiation exposure | Differentiation of distant metastases and metastatic retroperitoneal and supradiaphragmatic lymph nodes from benign processes |
| Disadvantages | Limited visualization of chest and bones Insufficient detection of small-volume disease (bowel serosa and mesentery) Low image quality for retroperitoneum in obese patients | Radiation exposure Insufficient detection of small-volume disease (bowel serosa and mesentery) Iodine-based contrast: Contraindicated if previous severe allergy to contrast | Low availability Low experience in acquisition and interpretation High cost Antiperistaltic agent Exam duration > 45 min MRI-guided tru-cut biopsy limited by cost and availability of non-magnetic biopsy equipment Contraindicated by non-MRI-conditional implants, cardiac pacemaker, cochlear implants or severe claustrophobia Gd-based contrast: contraindicated if previous severe allergy to contrast | High cost Radiation exposure Exam duration ~30–40 min Insufficient detection of small-volume disease (bowel serosa and mesentery) |
| Date | Study Type | Patients (n) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Accuracy (%) | |
|---|---|---|---|---|---|---|---|---|
| ULTRASOUND | ||||||||
| Tempany et al. [104] * | 2000 | Multicentric prospective | 280 | 61 | 95 | 61 | 95 | 91 |
| Testa et al. [55] | 2012 | Prospective | 147 | 90 | 96 | 94 | 92 | 93 |
| Fischerova et al. [103] | 2017 | Prospective | 394 | 70 | 98 | 89 | 93 | 92 |
| Alcázar et al. [102] * | 2019 | Prospective | 93 | 70 | 98 | 91 | 91 | 91 |
| Fischerova et al. [79] * | 2022 | Prospective | 67 | 86 | 88 | 93 | 78 | 87 |
| CT | ||||||||
| Tempany et al. [104] * | 2000 | Prospective | 280 | 78 | 89 | 48 | 97 | 88 |
| Michielsen et al. [109] * | 2014 | Prospective | 32 | 61 | 86 | 72 | 78 | 76 |
| Schmidt et al. [54] * | 2015 | Prospective | 15 | 90 | 91 | 91 | 90 | 90 |
| Alcazar et al. [102] * | 2019 | Prospective | 93 | 60 | 94 | 76 | 88 | 86 |
| Rizzo et al. [53] | 2020 | Prospective | 92 | 58 | 88 | 78 | 75 | 76 |
| Fischerova et al. [79] * | 2022 | Prospective | 67 | 80 | 58 | 80 | 88 | 82 |
| WB-DWI/MRI | ||||||||
| Michielsen et al. [109] * | 2014 | Prospective | 32 | 89 | 92 | 88 | 93 | 91 |
| Garcia Prado et al. [111] | 2019 | Prospective | 50 | 84 | 89 | 72 | 92 | 89 |
| Rizzo et al. [53] | 2020 | Prospective | 92 | 76 | 87 | 80 | 83 | 82 |
| Fischerova et al. [79] * | 2022 | Prospective | 67 | 89 | 79 | 89 | 86 | 88 |
| PET/CT | ||||||||
| Kitajima et al. [112] | 2008 | Prospective | 40 | 69 | 97 | 80 | 96 | 94 |
| Hynninen et al. [113] | 2013 | Prospective | 41 | 57 | 89 | 91 | 50 | 64 |
| Michielsen et al. [109] * | 2014 | Prospective | 32 | 48 | 89 | 73 | 74 | 73 |
| Schmidt et al. [54]* | 2015 | Prospective | 15 | 93 | 96 | 96 | 94 | 95 |
| Feng et al. [114] | 2021 | Prospective | 43 | 73 | 85 | 84 | 75 | 79 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinto, P.; Burgetova, A.; Cibula, D.; Haldorsen, I.S.; Indrielle-Kelly, T.; Fischerova, D. Prediction of Surgical Outcome in Advanced Ovarian Cancer by Imaging and Laparoscopy: A Narrative Review. Cancers 2023, 15, 1904. https://doi.org/10.3390/cancers15061904
Pinto P, Burgetova A, Cibula D, Haldorsen IS, Indrielle-Kelly T, Fischerova D. Prediction of Surgical Outcome in Advanced Ovarian Cancer by Imaging and Laparoscopy: A Narrative Review. Cancers. 2023; 15(6):1904. https://doi.org/10.3390/cancers15061904
Chicago/Turabian StylePinto, Patrícia, Andrea Burgetova, David Cibula, Ingfrid S. Haldorsen, Tereza Indrielle-Kelly, and Daniela Fischerova. 2023. "Prediction of Surgical Outcome in Advanced Ovarian Cancer by Imaging and Laparoscopy: A Narrative Review" Cancers 15, no. 6: 1904. https://doi.org/10.3390/cancers15061904