
Diagnosis, Prognosis, and Treatment of Canine Hemangiosarcoma: A Review Based on a Consensus Organized by the Brazilian Association of Veterinary Oncology, ABROVET
 , ,
, ,  , , , ,
, , , ,  , , , , , , add
Show full author list
, , , , , , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
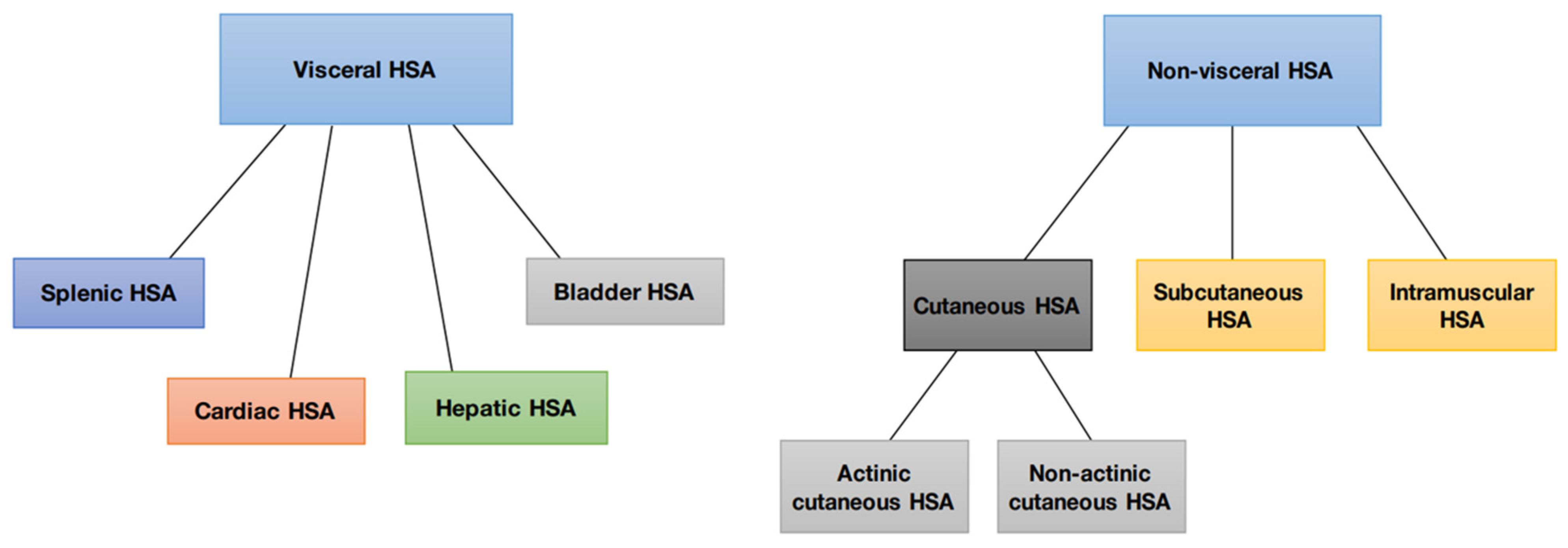
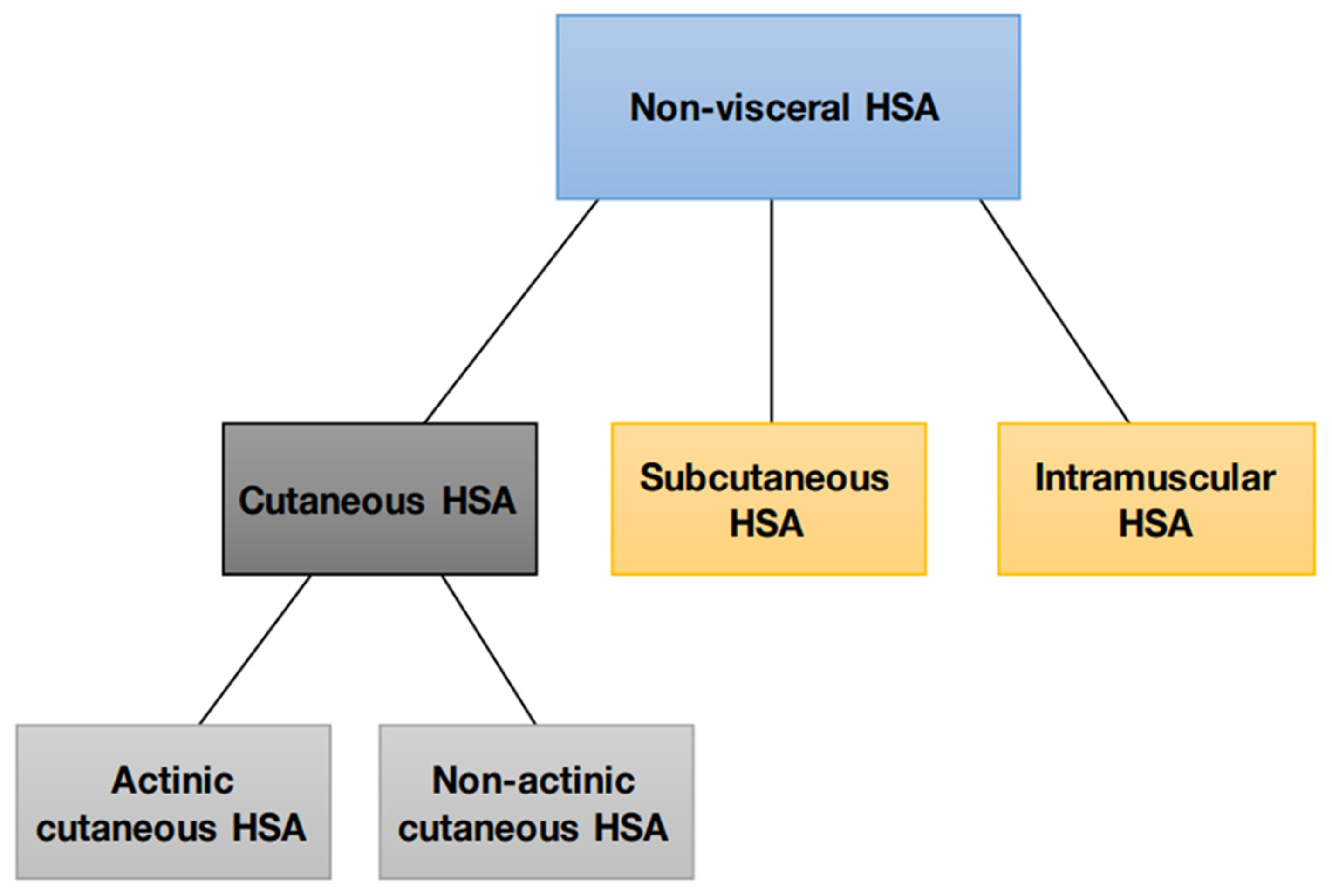
2. Canine Hemangiosarcoma and Its Different Forms
3. Cutaneous Hemangiosarcoma
4. Etiology and Epidemiology
4.1. Actinic and Non-Actinic Cutaneous HSA
Subcutaneous and Muscular HSA
5. Clinical Manifestation and Biological Behavior
Actinic and Non-Actinic Cutaneous HSA
6. Subcutaneous and Muscular HSA
7. Diagnosis and Staging
8. Treatment
Local Therapies
9. Systemic Therapies
9.1. Actinic and Non-Actinic Cutaneous HSA
9.2. HSA Subcutaneous and Muscular
9.3. Other Therapies
10. Prognostic
11. Prevention
12. Splenic Hemangiosarcoma
Etiology and Epidemiology
13. Clinical Manifestation and Biological Behavior
14. Diagnosis and Staging
15. Treatment
Prognosis
- Clinical staging: patients with TI and TII staging have a longer average survival time than patients with TIII staging; the possibility of administering a chemotherapy or adjuvant protocol increases the survival time of patients who are only subjected to splenectomy.
- Mitotic index (MI) of less than 11 is associated with a higher survival rate and is correlated with a slower tumor growth rate [176].
- Immunohistochemical evaluation: a low expression of Ki67 (below 16%) and PSMA is associated with better survival, while CLAUDIN 5 expression is associated with an increased risk of metastasis [175].
16. Cardiac Hemangiosarcoma
16.1. Etiology and Epidemiology
16.2. Clinical Manifestation and Biological Behavior
16.3. Diagnosis and Staging
16.4. Treatment
16.5. Prognosis
17. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mullin, C.; Clifford, C.A. Miscellaneous tumours: Hemangiosarcoma. In Withrow and MacEwen’s Small Animal Clinical Oncology, 5th ed.; Withrow, S.J., Vail, D.M., Page, R.L., Eds.; Elsevier Saunders: St. Louis, MO, USA, 2020; pp. 773–778. ISBN 978-0-323-59496-7. [Google Scholar]
- Nóbrega, D.F.; Sehaber, V.F.; Madureira, R.; Bracarense, A.P.F.R.L. Canine cutaneous haemangiosarcoma: Biomarkers and survival. J. Comp. Pathol. 2019, 166, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Ward, H.; Fox, L.E.; Calderwood-Mays, M.B.; Hammer, A.S.; Couto, C.G. Cutaneous hemangiosarcoma in 25 dogs: A retrospective study. Vet. Intern. Med. 1994, 8, 345–348. [Google Scholar] [CrossRef]
- Tinsley, A. Canine Hemangiosarcoma: A Certainly Less Than Ideal, Very Ugly Cancer. Preprints 2020, 1, 1–14. [Google Scholar] [CrossRef]
- Griffin, M.A.; Culp, W.T.N.; Rebhun, R.B. Canine and feline haemangiosarcoma. Vet. Rec. 2021, 585, e585. [Google Scholar] [CrossRef]
- Flores, M.M.; Panziera, W.; Kommers, G.D.; Irigoyen, L.F.; Barros, C.S.L.; Fighera, R.A. Aspectos epidemiológicos e anatomopatológicos do hemangiossarcoma em cães: 40 casos (1965–2012). Pesq. Vet. Bras. 2012, 32, 1319–1328. [Google Scholar] [CrossRef] [Green Version]
- Soares, N.P.; Medeiros, A.A.; Szabó, M.P.J.; Guimarães, E.C.; Fernandes, L.G.; dos Santos, T.R. Hemangiomas e Hemangiossarcomas em cães: Estudo retrospectivo de 192 casos (2002–2014). Ciênc. Anim. Bras. 2017, 18, 1–10. [Google Scholar] [CrossRef]
- Andrade, R.L.; Oliveira, D.M.; Dantas, A.F.M.; de Souza, A.P.; da Nóbrega, P.I.N.; Riet-Correa, F. Tumores de cães e gatos diagnosticados no semiárido da Paraíba. Pesq. Vet. Bras. 2012, 32, 1037–1040. [Google Scholar] [CrossRef] [Green Version]
- Alves, D.S.; Calvaca, M.B.; Fonseca-Alves, C.E. A Critical Review of the risk factors associated with Canine Squamous Cell Carcinoma development. Braz. J. Vet. Pathol. 2022, 15, 1–10. [Google Scholar] [CrossRef]
- DSA-INPE: Divisão de Satélites e Sistemas Ambientais, Instituto Nacional de Pesquisas Espaciais, Índice Ultravioleta Home page. Available online: http://satelite.cptec.inpe.br/uv (accessed on 20 March 2022).
- Szivek, A.; Burns, R.E.; Gericota, B.; Affolter, V.K.; Kent, M.S.; Rodriguez, C.O., Jr.; Skorupski, K.A. Clinical outcome in 94 cases of dermal haemangiosarcoma in dogs treated with surgical excision: 1993–2007. Vet. Comp. Oncol. 2012, 10, 65–73. [Google Scholar] [CrossRef]
- Vilar-Saavedra, P.; Kitchell, B.E. Sunlight-Induced Skin Cancer in Companion Animals. In Skin Cancer—A Practical Approach, 1st ed.; Baldi, A., Pasquali, P., Spugnini, E.P., Eds.; Humana Press: London, UK, 2014; pp. 499–514. ISBN 978-1-4614-7357-2. [Google Scholar]
- Hargis, A.M.; Ihrke, P.J.; Spangler, W.L.; Stannard, A.A. A retrospective clinicopathologic study of 212 dogs with cutaneous hemangiomas and hemangiosarcomas. Vet. Pathol. 1992, 29, 316–328. [Google Scholar] [CrossRef]
- Nikula, K.J.; Benjamin, S.A.; Angleton, G.M.; Saunders, W.J.; Lee, A.C. Ultraviolet radiation, solar dermatosis, and cutaneous neoplasia in beagle dogs. Radiat. Res. 1992, 129, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, S.C.; De Nardi, A.B. Hemangiossarcomas. In Oncologia de Cães e Gatos, 2nd ed.; Daleck, C.R., De Nardi, A.B., Eds.; Roca: Rio de Janeiro, RJ, Brazil, 2016; pp. 776–796. ISBN 9788527729918. [Google Scholar]
- Cezar, T.L.C.; Martinez, R.M.; da Rocha, C.; Melo, C.P.B.; Vale, D.L.; Borghi, S.M.; Fattori, V.; Vignoli, J.A.; Camilios-Neto, D.; Baracat, M.M.; et al. Treatment with maresin 1, a docoHSAexaenoic acid-derived pro-resolution lipid, protects skin from inflammation and oxidative stress caused by UVB irradiation. Sci. Rep. 2019, 9, 3062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nediani, C.; Dinu, M. Oxidative Stress and Inflammation as Targets for Novel Preventive and Therapeutic Approaches in Non-Communicable Diseases II. Antioxidants 2022, 11, 824. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Graef, A.J.; Dickerson, E.B.; Modiano, J.F. Pathobiology of hemangiosarcoma in dogs: Research advances and future perspectives. Vet. Sci. 2015, 2, 388–405. [Google Scholar] [CrossRef] [Green Version]
- Wong, K.; Ludwig, L.; Krijgsman, O.; Adams, D.J.; Wood, G.A.; van der Weyden, L. Comparison of the oncogenomic landscape of canine and feline hemangiosarcoma shows novel parallels with human angiosarcoma. Dis. Model. Mech. 2021, 14, dmm049044. [Google Scholar] [CrossRef]
- García-Iglesias, M.J.; Cuevas-Higuera, J.L.; Bastida-Sáenz, A.; de Garnica-García, M.G.; Polledo, L.; Perero, P.; González-Fernández, J.; Fernández-Martínez, B.; Pérez-Martínez, C. Immunohistochemical detection of p53 and pp53 Ser392 in canine hemangiomas and hemangiosarcomas located in the skin. BMC Vet. Res. 2020, 16, 239. [Google Scholar] [CrossRef]
- Rivera-Calderón, L.G.; Fonseca-Alves, C.E.; Kobayashi, P.E.; Carvalho, M.; Vasconcelos, R.O.; Laufer-Amorim, R. p-mTOR, p-4EBP-1 and eIF4E expression in canine prostatic carcinoma. Res. Vet. Sci. 2019, 122, 86–92. [Google Scholar] [CrossRef]
- Yonemaru, K.; Sakai, H.; Murakami, M.; Yanai, T.; Masegi, T. Expression of vascular endothelial growth factor, basic fibroblast growth factor, and their receptors (flt-1, flk-1, and flg-1) in canine vascular tumors. Vet. Pathol. 2006, 43, 971–980. [Google Scholar] [CrossRef]
- Sorenmo, K.U.; Jeglum, K.A.; Helfand, S.C. Chemotherapy of canine hemangiosarcoma with doxorubicin and cyclophosphamide. J. Vet. Int. Med. 1993, 7, 370–376. [Google Scholar] [CrossRef]
- Ogilvie, G.K.; Powers, B.E.; Mallinckrodt, C.H.; Withrow, S.J. Surgery and doxorubicin in dogs with hemangiosarcoma. J. Vet. Int. Med. 1996, 10, 379–384. [Google Scholar] [CrossRef]
- Bulakowski, E.J.; Philibert, J.C.; Siegel, S.; Clifford, C.A.; Risbon, R.; Zivin, K.; Cronin, K.L. Evaluation of outcome associated with subcutaneous and intramuscular hemangiosarcoma treated with adjuvant doxorubicin in dogs: 21 cases (2001–2006). J. Am. Vet. Med. Assoc. 2008, 233, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Shiu, K.B.; Flory, A.B.; Anderson, C.L.; Wypij, J.; Saba, C.; Wilson, H.; Kurzman, I.; Chun, R. Predictors of outcome in dogs with subcutaneous or intramuscular hemangiosarcoma. J. Am. Vet. Med. Assoc. 2011, 238, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Wiley, J.L.; Rook, K.A.; Clifford, C.A.; Gregor, T.P.; Sorenmo, K.U. Efficacy of doxorubicin-based chemotherapy for non-resectable canine subcutaneous haemangiosarcoma. Vet. Comp. Oncol. 2010, 8, 221–233. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.N. Hemangiosarcoma in dogs and cats. Vet. Clin. N. Am. Small Anim. Pract. 2003, 33, 533–552. [Google Scholar] [CrossRef]
- Schultheiss, P.C. A retrospective study of visceral and nonvisceral hemangiosarcoma and hemangiomas in domestic animals. J. Vet. Diagn. 2004, 16, 522–526. [Google Scholar] [CrossRef] [Green Version]
- Bertazzolo, W.; Dell’Orco, M.; Bonfanti, U.; Ghisleni, G.; Caniatti, M.; Masserdotti, C.; Antoniazzi, E.; Crippa, L.; Roccabianca, P. Canine angiosarcoma: Cytologic, histologic, and immunohistochemical correlations. Vet. Clin. Pathol. 2005, 34, 28–34. [Google Scholar] [CrossRef]
- Sabattini, S.; Bettini, G. An immunohistochemical analysis of canine haemangioma and haemangiosarcoma. J. Comp. Pathol. 2009, 140, 158–168. [Google Scholar] [CrossRef]
- Hammer, A.S.; Couto, C.G.; Filppi, J.; Getzt, D.; Shank, K. Efficacy and toxicity of VAC chemotherapy (vincristine doxorubicin, and cyclophosphamide) in dogs with hemangiosarcoma. J. Vet. Int. Med. 1991, 5, 160–166. [Google Scholar] [CrossRef]
- Wendelburg, K.M.; Price, L.L.; Burgess, K.E.; Lyons, J.A.; Lew, F.H.; Berg, J. Survival time of dogs with splenic hemangiosarcoma treated by splenectomy with or without adjuvant chemotherapy: 208 cases (2001–2012). J. Am. Vet. Met. Assoc. 2015, 247, 393–403. [Google Scholar] [CrossRef]
- Russel, W.O.; Cohen, J.; Enzinger, F.; Hajdu, S.I.; Heise, H.; Martin, R.G.; Meissner, W.; Miller, W.T.; Schmitz, R.L.; Suit, H.D. A clinical and pathological staging system for soft tissue sarcomas. Cancer 1997, 40, 1562–1570. [Google Scholar] [CrossRef]
- Von Beust, B.R.; Sutter, M.M.; Summers, B.A. Factor VIII-related antigen in canine endothelial neoplasms: An immunohistochemical study. Vet. Pathol. 1988, 25, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Jakab, C.S.; Halász, J.; Kiss, A.; Schaff, Z.; Rusvai, M.; Gálfi, P.; Abonyi, T.Z.; Kulka, J. Claudin-5 protein is a new differential marker for histopathological differential diagnosis of canine hemangiosarcoma. Histol. Histopathol. 2009, 24, 801–813. [Google Scholar] [CrossRef]
- Fukuda, S.; Kobayashi, T.; Robertson, I.D.; Oshima, F.; Fukazawa, R.; Nakano, Y.; Ono, S.; Thrall, D.E. Computed tomographic features of canine nonparenchymal hemangiosarcoma. Vet. Radiol. Ultrasound 2014, 55, 374–379. [Google Scholar] [CrossRef]
- Camboim, A.S.; Benvenutti, M.E.M.; de Oliveira, E.L.; Vaz, A.F.M.; da Silva, R.M.N.; Dantas, A.F.M.; de Souza, A.P. Manifestação de síndrome paraneoplásica em um cão com hemangiossarcoma cutâneo: Relato de caso. Braz. J. Vet. Res. 2017, 39, 126–132. [Google Scholar] [CrossRef] [Green Version]
- Vignoli, M.; Terragni, R.; Rossi, F.; Frühauf, L.; Bacci, B.; Ressel, L.; Capitani, O.; Marconato, L. Whole body computed tomographic characteristics of skeletal and cardiac muscular metastatic neoplasia in dogs and cats. Vet. Radiol. Ultrasound 2013, 54, 223–230. [Google Scholar] [CrossRef]
- Astudillo, R.M.W.; Contardo, C.M.I.; Merino, M.K.A.; Luna, J.I.L. Descripción clínica de hemangiosarcoma (HSA) cutáneo metastásico en un canino galgo: Estudio clínico de un caso. Rev. Med. Vet. 2015, 30, 107–116. [Google Scholar] [CrossRef]
- Nemanic, S.; London, C.A.; Wisner, E.R. Comparison of thoracic radiographs and single breath-hold helical CT for detection of pulmonary nodules in dogs with meta-static neoplasia. J. Vet. Intern. Med. 2006, 20, 508–515. [Google Scholar] [CrossRef]
- Oblak, M.L.; Boston, S.E.; Woods, J.P.; Nykamp, S. Comparison of concurrent imaging modalities for staging of dogs with appendicular primary bone tumours. Vet. Comp. Oncol. 2015, 13, 28–39. [Google Scholar] [CrossRef]
- Lamb, C.R.; Whitlock, J.; Foster-Yeow, A.T. Prevalence of pulmonary nodules in dogs with malignant neoplasia as determined by CT. Vet. Radiol. Ultrasound 2019, 60, 300–305. [Google Scholar] [CrossRef]
- Carloni, A.; Terragni, R.; Morselli-Labate, A.M.; Paninarova, M.; Graham, J.; Valenti, P.; Alberti, M.; Albarello, G.; Millanta, F.; Vignoli, M. Prevalence, distribution, and clinical characteristics of hemangiosarcoma-associated skeletal muscle metastases in 61 dogs: A whole body computed tomographic study. J. Vet. Intern. Med. 2019, 33, 812–819. [Google Scholar] [CrossRef]
- Chu, M.L.; Hayes, G.M.; Henry, J.G.; Oblak, M.L. Comparison of lateral surgical margins of up to two centimeters with margins of three centimeters for achieving tumor-free histologic margins following excision of grade I or II cutaneous mast cell tumors in dogs. J. Am. Vet. Med. Assoc. 2020, 256, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Saunders, H.; Thomson, M.J.; O’Connell, K.; Bridges, J.P.; Chau, L. Evaluation of a modified proportional margin approach for complete surgical excision of canine cutaneous mast cell tumours and its association with clinical outcome. Vet. Comp. Oncol. 2020, 19, 604–615. [Google Scholar] [CrossRef] [PubMed]
- Whitehair, J.G.; Griffey, S.M.; Olander, H.J.; Vasseur, P.B.; Naydan, D. The Accuracy of Intraoperative Diagnoses Based on Examination of Frozen Sections A Prospective Comparison with Paraffin-Embedded Sections. Vet. Surg. 1993, 22, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, A.A.; Riaz, R.; Zia, S.; Shahid, H.; Malik, U.A.; Khan, R.; Irfan, M.; Shamail, F.; Zia, F.; Asif, M.G. Impact of Histological Type and Grade on the Diagnostic Accuracy of Intraoperative Frozen Section for Detecting Breast Cancer Metastasis to Axillary Sentinel Lymph Nodes. Cureus 2021, 13, e16146. [Google Scholar] [CrossRef]
- Tozon, N.; Sersa, G.; Cemazar, M. Electrochemotherapy: Potentiation of local antitumor effectiveness of cisplatin in dogs and cats. Anticancer Res. 2001, 21, 2483–2488. [Google Scholar]
- Hillers, K.R.; Lana, S.E.; Fuller, C.R.; LaRue, S.M. Effects of palliative radiation therapy on nonsplenic hemangiosarcoma in dogs. J. Am. Anim. Hosp. Assoc. 2007, 43, 187–192. [Google Scholar] [CrossRef]
- Mir, L.M.; Gehl, J.; Sersa, G.; Collins, C.G.; Garbay, J.R.; Billard, V.; Geertsen, P.F.; Rudolf, Z.; O’Sullivan, G.C.; Marty, M. Standard operating procedures of the electrochemotherapy: Instructions for the use of bleomycin or cisplatin administered either systemically or locally and electric pulses delivered by the CliniporatorTM by means of invasive or non-invasive electrodes. EJC Suppl. 2006, 4, 14–25. [Google Scholar] [CrossRef]
- Rangel, M.M.; Luz, J.; Oliveira, K.D.; Ojeda, J.; Freytag, J.O.; Suzuki, D.O. Electrochemotherapy in the treatment of neoplasms in dogs and cats. Austral J. Vet. Sci. 2019, 51, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Spugnini, E.P.; Baldi, A. Electrochemotherapy in veterinary oncology: State-of-the-art and perspectives. Vet. Clin. N. Am. Small Anim. Pract. 2019, 49, 967–979. [Google Scholar] [CrossRef]
- Mir, L.M. Bases and rationale of the electrochemotherapy. EJC Suppl. 2006, 4, 38–44. [Google Scholar] [CrossRef]
- Escoffre, J.M.; Rols, M.P. Electrochemotherapy: Progress and prospects. Curr. Pharm. Des. 2012, 18, 3406–3415. [Google Scholar] [CrossRef]
- Mir, L.M.; Orlowski, S.; Belehradek, J.J.; Paoletti, C. Electrochemotherapy potentiation of antitumour effect of bleomycin by local electric pulses. Eur. J. Cancer 1991, 27, 68–72. [Google Scholar] [CrossRef]
- Tounekti, O.; Pron, G.; Belehradek, J.; Mir, L.M. Bleomycin, an apoptosis-mimetic drug that induces two types of cell death depending on the number of molecules internalized. Cancer Res. 1993, 53, 5462–5496. [Google Scholar]
- Sersa, G.; Jarm, T.; Kotnik, T.; Coer, A.; Podkrajesk, M.; Sentjurc, M.; Miklavcic, D.; Kadivec, M.; Kranjc, S.; Secerov, A.; et al. Vascular disrupting action of electroporation and electrochemotherapy with bleomycin in murine sarcoma. Br. J. Cancer 2008, 98, 388–398. [Google Scholar] [CrossRef] [Green Version]
- Campana, L.G.; Kis, E.; Bottyán, K.; Orlando, A.; de Terlizzi, F.; Mitsala, G.; Careri, R.; Curatolo, P.; Snoj, M.; Sersa, G.; et al. Electrochemotherapy for advanced cutaneous angiosarcoma: A European register-based cohort study from the International Network for Sharing Practices of electrochemotherapy (InspECT). Int. J. Surg. 2019, 72, 34–42. [Google Scholar] [CrossRef]
- Spugnini, E.P.; Porrello, A. Potentiation of chemotherapy in companion animals with spontaneous large neoplasms by application of biphasic electric pulses. J. Exp. Clin. Cancer Res. 2003, 22, 571–580. [Google Scholar]
- Spugnini, E.P.; Citro, G.; D’Avino, A.; Baldi, A. Potential role of electrochemotherapy for the treatment of soft tissue sarcoma: First insights from preclinical studies in animals. Int. J. Biochem. Cell Biol. 2008, 40, 159–163. [Google Scholar] [CrossRef]
- Spugnini, E.P.; Vincenzi, B.; Betti, G.; Cordahi, F.; Dotsinsky, I.; Mudrov, N.; Citro, G.; Baldi, A. Surgery and electrochemotherapy of a high-grade soft tissue sarcoma in a dog. Vet. Rec. 2008, 162, 186–188. [Google Scholar] [CrossRef]
- Spugnini, E.P.; Vincenzi, B.; Amadio, B.; Baldi, A. Adjuvant electrochemotherapy with bleomycin and cisplatin combination for canine soft tissue sarcomas: A study of 30 cases. Open Vet. J. 2019, 9, 88–93. [Google Scholar] [CrossRef] [Green Version]
- Torrigiani, F.; Pierini, A.; Lowe, R.; Simčič, P.; Lubas, G. Soft tissue sarcoma in dogs: A treatment review and a novel approach using electrochemotherapy in a case series. Vet. Comp. Oncol. 2019, 17, 234–241. [Google Scholar] [CrossRef]
- Spugnini, E.P.; Vincenzi, B.; Citro, G.; Santini, D.; Dotsinsky, I.; Mudrov, N.; Montersarchio, V.; Laieta, M.T.; Esposito, V.; Baldi, A. Adjuvant electrochemotherapy for the treatment of incompletely excised spontaneous canine sarcomas. Vivo 2007, 21, 819–822. [Google Scholar]
- Groselj, A.; Bosnjak, M.; Krzan, M.; Kosjek, T.; Bottyán, K.; Plesnik, H.; Jamsek, C.; Cemazar, M.; Kis, E.; Sersa, G. Bleomycin Concentration in Patients’ Plasma and Tumors after Electrochemotherapy. A Study from InspECT Group. Pharmaceutics 2021, 13, 1324. [Google Scholar] [CrossRef] [PubMed]
- de Queiroz, G.F.; Matera, J.M.; Dagli, M.L.Z. Clinical study of cryosurgery efficacy in the treatment of skin and subcutaneous tumors in dogs and cats. Vet. Surg. 2008, 37, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Laus, J.L.; Ortiz, J.P.D.; Brito, F.L.C.; Lisbão, C.B.S.; Silva, V.A., Jr.; Maia, F.C.L. Hemangiosarcoma of the nictitant membrane in a Brazilian Fila dog: Case report. Arq. Bras. Med. Vet. Zootec. 2008, 60, 1413–1417. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, F.J.; Hosoya, K.; Lara-Garcia, A.; Kisseberth, W.; Couto, G. VAC Protocol for Treatment of Dogs with Stage III Hemangiosarcoma. J. Am. Anim. Hosp. Assoc. 2013, 49, 370–377. [Google Scholar] [CrossRef]
- Finotello, R.; Henriques, J.; Sabattini, S.; Stefanello, D.; Felisberto, R.; Pizzoni, S.; Ferrari, R.; Marconato, L. A retrospective analysis of chemotherapy switch suggests improved outcome in surgically removed, biologically aggressive canine haemangiosarcoma. Vet. Comp. Oncol. 2017, 15, 493–503. [Google Scholar] [CrossRef]
- Treggiari, E.; Borrego, J.F.; Gramer, I.; Valenti, P.; Harper, A.; Finotello, R.; Toni, C.; Laomedonte, P.; Romanelli, G. Retrospective comparison of first-line adjuvant anthracycline vs metronomic-based chemotherapy protocols in the treatment of stage I and II canine splenic haemangiosarcoma. Vet. Comp. Oncol. 2020, 18, 43–51. [Google Scholar] [CrossRef]
- Rocha, M.S.T.; Lucci, C.M.; dos Santos, J.A.; Longo, J.P.F.; Muehlmann, L.A.; Azevedo, R.B. Photodynamic therapy for cutaneous hemangiosarcoma in dogs. Photodiagnosis Photodyn. Ther. 2019, 27, 39–43. [Google Scholar] [CrossRef]
- Kullavanijaya, P.; Lim, H.W. Photoprotection. J. Am. Acad. Dermatol. 2005, 52, 937–958. [Google Scholar] [CrossRef]
- Souyoul, S.A.; Saussy, K.P.; Lupo, M.P. Nutraceuticals: A Review. Dermatol. Ther. 2018, 8, 5–16. [Google Scholar] [CrossRef] [Green Version]
- Sawada, Y.; Saito-Sasaki, N.; Nakamura, M. Omega 3 Fatty Acid and Skin Diseases. Front. Immunol. 2020, 11, 623052. [Google Scholar] [CrossRef]
- Sulciner, M.L.; Serhan, C.N.; Gilligan, M.M.; Mudge, D.K.; Chang, J.; Gartung, A.; Lehner, K.A.; Bielenberg, D.R.; Schmidt, B.; Dalli, J.; et al. Resolvins suppress tumor growth and enhance cancer therapy. J. Exp. Med. 2018, 215, 115–140. [Google Scholar] [CrossRef] [Green Version]
- Takamiya, R.; Fukunaga, K.; Arita, M.; Miyata, J.; Seki, H.; Minematsu, N.; Suematsu, M.; Asano, K. Resolvin E1 maintains macrophage function under cigarette smoke-induced oxidative stress. FEBS Open Bio 2012, 2, 328–333. [Google Scholar] [CrossRef] [Green Version]
- Ye, Y.; Scheff, N.N.; Bernabé, D.; Salvo, E.; Ono, K.; Liu, C.; Veeramachaneni, R.; Viet, C.T.; Viet, D.T.; Dolan, J.C.; et al. Anti-cancer and analgesic effects of resolvin D2 in oral squamous cell carcinoma. Neuropharmacology 2018, 139, 182–193. [Google Scholar] [CrossRef]
- Fania, L.; Mazzanti, C.; Campione, E.; Candi, E.; Abeni, D.; Dellambra, E. Role of Nicotinamide in Genomic Stability and Skin Cancer Chemoprevention. Int. J. Mol. Sci. 2019, 20, 5946. [Google Scholar] [CrossRef] [Green Version]
- Jastrząb, A.; Jarocka-Karpowicz, J.; Markowska, A.; Wroński, A.; Gęgotek, A.; Skrzydlewska, E. Antioxidant and Anti-inflammatory Effect of Cannabidiol Contributes to the Decreased Lipid Peroxidation of Keratinocytes of Rat Skin Exposed to UV Radiation. Antioxidants 2020, 9, 21. [Google Scholar] [CrossRef]
- Wang, K.; Jiang, H.; Li, W.; Qiang, M.; Dong, T.; Li, H. Role of Vitamin C in Skin Diseases. Front. Physiol. 2018, 9, 819. [Google Scholar] [CrossRef] [Green Version]
- Milovancev, M.; Russell, D.S. Surgical margins in the veterinary cancer patient. Vet. Comp. Oncol. 2018, 15, 1136–1157. [Google Scholar] [CrossRef] [Green Version]
- Mark, R.J.; Tran, L.M.; Sercarz, J.; Fu, Y.S.; Calcaterra, T.C.; Juillard, G.F. Angiosarcoma of the Head and Neck. The UCLA Experience 1955 Through 1990. Arch. Otolaryngol. Head Neck Surg. 1993, 119, 973–978. [Google Scholar] [CrossRef]
- Pawlik, T.M.; Paulino, A.F.; McGinn, C.J.; Baker, L.H.; Cohen, D.S.; Morris, J.S.; Rees, R.; Sondak, V.K. Cutaneous angiosarcoma of the scalp: A multidisciplinary approach. Cancer 2003, 98, 1716–1726. [Google Scholar] [CrossRef] [Green Version]
- Clifford, C.A.; Hughes, D.; Beal, M.W.; Mackin, A.J.; Henry, C.J.; Shofer, F.S.; Sorenmo, K.U. Plasma vascular endothelial growth factor concentrations in healthy dogs and dogs with hemangiosarcoma. J. Vet. Intern. Med. 2001, 15, 131–135. [Google Scholar] [CrossRef]
- Clifford, C.A.; de Loirimier, L.P. Hemangiosarcoma. In Textbook of Veterinary Internal Medicine, 8th ed.; Ettinger, S.J., Feldman, E.C., Côté, E., Eds.; Elsevier Saunders: St. Louis, MO, USA, 2017; pp. 5062–5084. ISBN 978-0-323-46214-3. [Google Scholar]
- Valli, V.E.; Bienzle, D.; Meuten, D.J.; Linder, K.E. Tumors of the Hemolymphactic System—Tumors of the Spleen. In Tumors in Domestic Animals, 5th ed.; Meuten, D.J., Ed.; Wiley Blackwell: Ames, IA, USA, 2017; pp. 307–313. ISBN 978-1-119-18119-4. [Google Scholar]
- Johnson, K.A.; Powers, B.E.; Withrow, J.S.; Sheetz, M.J.; Curtis, C.R.; Wrigley, R.H. Splenomegaly in dogs. Predictors of neoplasia and survival after splenectomy. J. Vet. Intern. Med. 1989, 3, 160–166. [Google Scholar] [CrossRef]
- Hammond, T.N.; Persillo-Crosby, S.A. Prevalence of hemangiosarcoma in anemic dogs with a splenic mass and hemoperitoneum requiring a transfusion: 71 cases (2003–2005). J. Am. Vet. Med. Assoc. 2008, 232, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Corbin, E.E.; Cavanaugh, R.P.; Schwartz, P.; Zawadski, K.I.; Donovan, T. Splenomegaly in small-breed dogs: 45 cases (2005–2011). J. Am. Vet. Med. Assoc. 2017, 250, 1148–1154. [Google Scholar] [CrossRef]
- Leyva, F.J.; Loughin, C.A.; Dewey, C.W.; Marino, D.J.; Akerman, M.; Lesser, M.L. Histopathologic characteristics of biopsies from dogs undergoing surgery with concurrent gross splenic and hepatic masses: 125 cases (2012–2016). BMC Res. Notes 2018, 11, 122. [Google Scholar] [CrossRef] [Green Version]
- Davies, O.; Taylor, A.J. Refining the “double two-thirds” rule: Genotype-based breed grouping and clinical presentation help predict the diagnosis of canine splenic mass lesions in 288 dogs. Vet. Comp. Oncol. 2020, 18, 548–558. [Google Scholar] [CrossRef]
- Story, A.L.; Wavreille, V.; Abrams, B.; Egan, A.; Cray, M.; Selmic, L.E. Outcomes of 43 small breed dogs treated for splenic hemangiosarcoma. Vet. Surg. 2020, 49, 1154–1163. [Google Scholar] [CrossRef]
- Giuffrida, M.A.; Bacon, N.J.; Kamstock, D.A. Use of routine histopathology and factor VIII-related antigen/von Willebrand factor immunohistochemistry to differentiate primary hemangiosarcoma of bone from telangiectatic osteosarcoma in 54 dogs. Vet. Comp. Oncol. 2017, 15, 1232–1239. [Google Scholar] [CrossRef]
- Movilla, R.; Altet, L.; Serrano, L.; Tabar, M.D.; Roura, X. Molecular detection of vector-borne pathogens in blood and splenic samples from dogs with splenic disease. Parasit. Vectors 2017, 10, 131. [Google Scholar] [CrossRef] [Green Version]
- Lashnits, E.; Neupane, P.; Bradley, J.M.; Richardson, T.; Thomas, R.; Linder, K.E.; Breen, M.; Maggi, R.G.; Breitschwerdt, E.B. Molecular prevalence of Bartonella, Babesia, and hemotropic Mycoplasma species in dogs with hemangiosarcoma from across the United States. PLoS ONE 2020, 15, e0227234. [Google Scholar] [CrossRef] [Green Version]
- Lashnits, E.; Neupane, P.; Bradley, J.M.; Richardson, T.; Maggi, R.G.; Bretischwerdt, E.B. Comparison of Serological and Molecular Assays for Bartonella Species in Dogs with Hemangiosarcoma. Pathogens 2021, 10, 794. [Google Scholar] [CrossRef] [PubMed]
- Carnio, A.; Eleni, C.; Cocumelli, C.; Del Pino, L.E.B.; Simeoni, S.; Spallucci, V.; Scaramozzino, P. Evaluation of intrinsic and extrinsic risk factors for dog visceral hemangiosarcoma: A retrospective case-control study register-based in Lazio region, Italy. Prev. Vet. Med. 2020, 181, 105074. [Google Scholar] [CrossRef] [PubMed]
- Pinello, K.; Pires, I.; Castro, A.F.; Carvalho, P.T.; Santos, A.; de Matos, A.; Queiroga, F.; Canadas-Sousa, A.; Dias-Pereira, P.; Catarino, J.; et al. Cross Species Analysis and Comparison of Tumors in Dogs and Cats, by Age, Sex, Topography and Main Morphologies. Data from Vet-OncoNet. Vet. Sci. 2022, 9, 167. [Google Scholar] [CrossRef] [PubMed]
- Cleveland, M.H.; Casale, S. Incidence of malignancy and outcomes for dogs undergoing splenectomy for incidentally detected nonruptured splenic nodules or mass-es: 105 cases (2009–2013). J. Am. Vet. Med. Assoc. 2016, 248, 1267–1273. [Google Scholar] [CrossRef]
- Linden, D.; Liptak, J.M.; Vinayak, A.; Grimes, J.A.; Sandey, M.; Smiley, W.; Matz, B.M. Outcomes and prognostic variables associated with primary abdominal visceral soft tissue sarcomas in dogs: A Veterinary Society of Surgical Oncology retrospective study. Vet. Comp. Oncol. 2019, 17, 265–270. [Google Scholar] [CrossRef]
- Robinson, K.L.; Bryan, M.E.; Atkinson, E.S.; Keeler, M.R.; Hahn, A.W.; Bryan, J.N. Neutering is associated with developing hemangiosarcoma in dogs in the Veterinary Medical Database: An age and time-period matched case-control study (1964–2003). Can. Vet. J. 2020, 61, 499–504. [Google Scholar]
- Aronsohn, M.G.; Dubiel, B.; Roberts, B.; Powers, B.E. Prognosis for Acute Non-traumatic Hemoperitoneum in the Dog: A retrospective Analysis of 60 Cases (2003–2006). J. Am. Anim. Hosp. Assoc. 2009, 45, 72–77. [Google Scholar] [CrossRef]
- Sherwood, J.M.; Haynes, A.M.; Klocke, E.; Higginbotham, M.L.; Thmson, E.M.; Weng, H.Y.; Millard, H.A.T. Ocurrence and Clinicopathologic Features of Splenic Neoplasia Based on Body Weight: (2003–2013). J. Am. Anim. Hosp. Assoc. 2016, 52, 220–226. [Google Scholar] [CrossRef]
- Panissidi, A.A.; DeSandre-Robinson, D.M. Development of perioperative premature ventricular contractions as an indicator of splenic hemangiosarcoma and me-dian survival times. Vet. Surg. 2020, 50, 1609–1616. [Google Scholar] [CrossRef]
- Masyr, A.R.; Rendahl, A.K.; Winter, A.L.; Borgatti, A.; Modiano, J.F. Retrospective evaluation of thrombocytopenia and tumor stage as prognostic indicators in dogs with splenic heman-giosarcoma. J. Am. Vet. Med. Assoc. 2021, 258, 630–637. [Google Scholar] [CrossRef]
- Mullin, C.M.; Arkans, M.A.; Samarco, C.D.; Vail, D.M.; Britton, B.M.; Vickery, K.R.; Risbon, R.E.; Lachowicz, J.; Burgess, K.E.; Manley, C.A.; et al. Doxorubicin chemotherapy for presumptive cardiac hemangiosarcoma in dogs. Vet. Comp. Oncol. 2016, 14, 171–183. [Google Scholar] [CrossRef]
- Boston, S.E.; Higginson, G.; Monteith, G. Concurrent Splenic and Right Atrial Mass at Presentation in Dogs with HAS: A Retrospective Study. J. Am. Anim. Hosp. Assoc. 2011, 47, 336–341. [Google Scholar] [CrossRef]
- Yankin, I.; Nemanic, S.; Funes, S.; de Morais, H.; Gorman, E.; Ruaux, G. Clinical relevance of splenic nodules or heterogeneous splenic parenchyma assessed by cytologic evaluation of fine-needle samples in 125 dogs (2011–2015). J. Vet. Intern. Med. 2020, 34, 125–131. [Google Scholar] [CrossRef]
- Hammer, A.S.; Bailey, M.Q.; Sagartz, J.E. Retrospective assessment of thoracic radiographic findings in metastatic canine hemangiosarcoma. Vet. Radiol. Ultrasound 1993, 34, 235–238. [Google Scholar] [CrossRef]
- Hristov, T. Ultrasound findings in dogs with splenic hemangiosarcoma. Tradit. Mod. Vet. Med. 2020, 5, 15–20. [Google Scholar] [CrossRef]
- Maronezi, M.C.; Carneiro, R.K.; da Cruz, I.C.K.; de Oliveira, A.P.L.; De Nardi, A.B.; Pavan, L.; Del’Aguila-Silva, P.; Uscategui, R.A.R.; Feliciano, M.A.R. Accuracy of B-mode ultrasound and ARFI elastography in predicting malignancy of canine splenic lesions. Sci. Rep. 2022, 12, 4252. [Google Scholar] [CrossRef]
- Levinson, J.G.; Bouma, J.L.; Althouse, G.C.; Rieser, T.M. Prevalence of malignancy when solitary versus multiple lesions are detected during abdominal ultrasonographic examination of dogs with spontaneous hemoperitoneum: 31 cases (2003–2008). J. Vet. Emerg. Crit. Care 2009, 19, 496–500. [Google Scholar] [CrossRef]
- Patten, S.G.; Boston, S.E.; Monteith, G.J. Outcome and prognostic factors for dogs with a histological diagnosis of splenic hematoma following splenectomy: 35 cases (2001–2013). Can. Vet. J. 2016, 57, 842–846. [Google Scholar]
- Lacreta, A.C.C., Jr.; Guimarães, B.L.L. Fígado. In Ultrassonografia em Cães e Gatos, 1st ed.; Feliciano, M.A.R., Assis., A.R., Vicente, W.R.R., Eds.; MedVet: São Paulo, SP, Brazil, 2019; pp. 265–328. ISBN 978-8-562-45158-4. [Google Scholar]
- Lacreta, A.C.C., Jr.; Guimarães, B.L.L. Baço. In Ultrassonografia em Cães e Gatos, 1st ed.; Feliciano, M.A.R., Assis., A.R., Vicente, W.R.R., Eds.; MedVet: São Paulo, SP, Brazil, 2019; pp. 329–367. ISBN 978-8-562-45158-4. [Google Scholar]
- Watson, A.T.; Penninck, D.; Knoll, J.S.; Keating, J.H.; Sutherland-Smith, J. Safety and correlation of test results of combined ultrasound-guided fine-needle aspiration and needle core biopsy of the canine spleen. Vet. Radiol. Ultrasound 2011, 52, 317–322. [Google Scholar] [CrossRef]
- Ohlerth, S.; Dennler, M.; Rüefli, E.; Hauser, B.; Poirier, V.; Siebeck, N.; Roos, M.; Kaser-Hotz, B. Contrast harmonic imaging characterization of canine splenic lesions. J. Vet. Intern. Med. 2008, 22, 1095–1102. [Google Scholar] [CrossRef]
- Nakamura, K.; Takagi, S.; Sasaki, N.; Kumara, W.R.B.; Murakami, M.; Ohta, H.; Yamasaki, M.; Takiguchi, M. Contrast-enhanced ultrasonography for characterization of canine focal liver lesions. Vet. Radiol. Ultrasound. 2010, 51, 79–85. [Google Scholar] [CrossRef]
- Canejo-Teixeira, R.; Lima, A.; Santana, A. Applications of contrast-enhanced ultrasound in splenic studies of dogs and cats. Animals 2022, 12, 2104. [Google Scholar] [CrossRef]
- Kutara, K.; Seki, M.; Ishigaki, K.; Teshima, K.; Ishikawa, C.; Kagawa, Y.; Edamura, K.; Nakayama, T.; Asano, K. Triple-Phase Helical Computed Tomography in Dogs with Solid Splenic Masses. J. Vet. Med. Sci. 2017, 79, 1870–1877. [Google Scholar] [CrossRef] [Green Version]
- Jones, I.D.; Lamb, C.R.; Drees, R.; Priestnall, S.L.; Mantis, P. Associations between dual phase computed tomography features and histopathologic diagnoses in 52 dogs with hepatic or splenic masses. Vet. Radiol. Ultrasound. 2016, 57, 144–153. [Google Scholar] [CrossRef]
- Tanaka, T.; Akiyoshi, H.; Nishida, H.; Mie, K.; Lin, L.S.; Iimori, Y.; Okamonto, M. Contrast-enhanced computed tomography findings of canine primary renal tumors including renal cell carcinoma, lymphoma, and hemangiosarcoma. PLoS ONE 2019, 14, e0225211. [Google Scholar] [CrossRef] [Green Version]
- Pickhardt, P.J.; Kitchin, D.; Lubner, M.G.; Ganeshan, D.M.; Bhalla, S.; Covey, A.M. Primary hepatic angiosarcoma: Multi-institutional comprehensive cancer centre review of multiphasic CT and MR imaging in 35 patients. Eur. Radiol. 2015, 25, 315–322. [Google Scholar] [CrossRef]
- Gaballah, A.H.; Jensen, C.T.; Palmquist, S.; Pickhardt, P.J.; Duran, A.; Broering, G.; Elsayes, K.M. Angiosarcoma: Clinical and imaging features from head to toe. Br. J. Radiol. 2017, 90, 20170039. [Google Scholar] [CrossRef]
- Fife, W.D.; Samii, V.F.; Drost, W.T.; Mattoon, J.S.; Hoshaw-Woodard, S. Comparison between malignant and non-malignant splenic masses in dogs using contrast enhanced computed tomography. Vet. Radiol. Ultrasound 2004, 45, 289–297. [Google Scholar] [CrossRef]
- Kim, M.; Choi, S.; Choi, H.; Lee, Y.; Lee, K. Diagnosis of a large splenic tumor in a dog: Computed tomography versus magnetic resonance imaging. J. Vet. Med. Sci. 2016, 77, 1685–1687. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Park, J.; Choi, H.; Lee, H.; Jeong, S.M. Presurgical assessment of splenic tumors in dogs: A retrospective study of 57 cases (2012–2017). J. Vet. Sci. 2018, 19, 827–834. [Google Scholar] [CrossRef]
- Borgatti, A.; Winter, A.L.; Stuebner, K.; Scott, R.; Ober, C.P.; Anderson, K.L.; Feeney, D.A.; Vallera, D.A.; Koopmeiners, J.S.; Modiano, J.F.; et al. Evaluation of 18-F-fluoro-2-deoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) as a staging and monitoring tool for dogs with stage-2 splenic hemangiosarcoma—A pilot study. PLoS ONE 2017, 12, e0172651. [Google Scholar] [CrossRef] [Green Version]
- Waters, D.J.; Hayden, D.W.; Walter, P.A. Intracranial lesions in dogs with hemangiosarcoma. J. Vet. Int. Med. 1989, 3, 222–230. [Google Scholar] [CrossRef]
- Clendaniel, D.C.; Sivacolundhu, R.K.; Sorenmo, K.U.; Donovan, T.A.; Turner, A.; Arteaga, T.; Bergman, P.J. Association between macroscopic appearance of liver lesions and liver histology in dogs with splenic hemangiosarcoma: 79 Cases (2004–2009). J. Am. Anim. Hosp. Assoc. 2014, 50, 6–10. [Google Scholar] [CrossRef] [Green Version]
- Clarke, E.; Levien, A.S.; Bennett, R.A.; Perry, S.; Daniel, G. Clinical utility of liver biopsies in dogs undergoing splenectomy. J. Small Anim. Pract. 2020, 61, 684–688. [Google Scholar] [CrossRef]
- Herman, E.J.; Stern, A.W.; Fox, R.J.; Dark, M.J. Understanding the Efficiency of Splenic Hemangiosarcoma Diagnosis Using Monte Carlo Simulations. Vet. Pathol. 2019, 56, 856–859. [Google Scholar] [CrossRef]
- Spangler, W.L.; Kass, P.H. Pathologic Factors Affecting Postsplenectomy Survival in Dogs. J. Vet. Intern. Med. 1997, 11, 166–171. [Google Scholar] [CrossRef]
- Frenz, M.; Kaup, F.J.; Neumann, S. Serum vascular endothelial Growth factor in dogs with haemangiosarcoma and haematoma. Res. Vet. Sci. 2014, 97, 257–262. [Google Scholar] [CrossRef]
- Grimes, J.A.; Prasad, N.; Levy, S.; Cattley, R.; Lindley, S.; Boothe, H.W.; Henderson, R.A.; Smith, B.F. A comparison of microRNA expression. Profiles from splenic hemangiosarcoma, splenic nodular hyperplasia, and normal spleen of dogs. BMC Vet. Res. 2016, 12, 272. [Google Scholar] [CrossRef] [Green Version]
- Grimes, J.A.; Robinson, K.R.; Bullington, A.C.M.; Schmiedt, J.M. Identification of serum microRNAs with differential expression between dogs with splenic masses and healthy dogs with histologically normal spleens. Am. J. Vet. Res. 2021, 82, 659–666. [Google Scholar] [CrossRef]
- Favaro, P.F.; Stewart, S.D.; McDonald, B.R.; Cawley, J.; Contente-Cuomo, T.; Wong, S.; Hendricks, W.P.D.; Trent, J.M.; Khanna, C.; Murtaza, M. Feasibility of circulating tumor DNA analysis in dogs with naturally occurring malignant and benign splenic lesions. Sci. Rep. 2022, 12, 6337. [Google Scholar] [CrossRef]
- Kim, J.H. PIK3CA mutations matter for cancer in dogs. Res. Vet. Sci. 2020, 133, 39–41. [Google Scholar] [CrossRef]
- Wang, G.; Wu, M.; Durham, A.C.; Radaelli, E.; Mason, N.J.; Xu, X.; Roth, D.B. Molecular subtypes in canine hemangiosarcoma reveal similarities with human angiosarcoma. PLoS ONE 2020, 15, e0229728. [Google Scholar] [CrossRef]
- Megquier, K.; Turner-Maier, J.; Swofford, R.; Kim, J.H.; Sarver, A.L.; Wang, C.; Sakthikumar, S.; Johnson, J.; Koltookian, M.; Lewellen, M.; et al. Comparative genomics reveals shared mutational landscape in canine hemangiosarcoma and human angiosarcoma. Mol. Cancer Res. 2019, 17, 2410–2421. [Google Scholar] [CrossRef] [Green Version]
- Alsaihati, B.A.; Ho, K.L.; Watson, J.; Feng, Y.; Wang, T.; Dobbin, K.K.; Zhao, S. Canine tumor mutational burden is correlated with TP53 mutation across tumor types and breeds. Nat. Commun. 2021, 12, 4670. [Google Scholar] [CrossRef]
- Bray, J.P.; Orbell, G.; Cave, N.; Munday, J.S. Does thalidomide prolong survival in dogs with splenic haemangiosarcoma? J. Small Anim. Pract. 2018, 59, 85–91. [Google Scholar] [CrossRef]
- Mallinckrodt, M.J.; Gottfried, S.D. Mass-to-splenic volume ration and splenic weight as a percentage of body weight in dogs with malignant and benign splenic masses: 65 cases (2007–2008). J. Am. Vet. Med. Assoc. 2011, 239, 1325–1327. [Google Scholar] [CrossRef]
- Lynch, A.M.; O’Toole, T.E.; Hamilton, J. Transfusion practices for treatment of dogs undergoing splenectomy for splenic masses: 542 cases (2001–2012). J. Am. Vet. Med. Assoc. 2015, 247, 636–642. [Google Scholar] [CrossRef]
- Batschinski, K.; Nobre, A.; Vargaz-Mendez, E.; Tedardi, M.V.; Cirillo, J.; Cstari, G.; Ubukata, R.; Dagli, M.L.Z. Canine visceral hemangiosarcoma treated with surgery alone or surgery and doxorubicin: 37 cases (2005–2014). Can. Vet. J. 2018, 59, 967–972. [Google Scholar]
- Barker, D.A.; Foale, R.D.; Holmes, M.A.; Demetriou, J.L. Survey of UK-based veterinary surgeons’ opinions on the use of surgery and chemotherapy in the treatment of canine high-grade mast cell tumour, splenic haemangiosarcoma and appendicular osteosarcoma. Vet. Rec. 2016, 179, 572–579. [Google Scholar] [CrossRef]
- Payne, S.E.; Rassnick, K.M.; Northrup, N.C.; Kristal, O.; Chretinm, J.D.; Cotter, S.M.; Kintzer, P.; Frimberger, A.E.; Morrison-Collister, K.E.; Wood, C.A.; et al. Treatment of vascular and soft-tissue sarcomas in dogs using an alternating protocol of ifosfamide and doxorubicin. Vet. Comp. Oncol. 2003, 1, 171–179. [Google Scholar] [CrossRef]
- Teske, E.; Rutteman, G.R.; Kirpenstein, J.; Hirschberger, J. A randomized controlled study into the efficacy and toxicity of pegylated liposome encapsulated doxorubicin as an adjuvant therapy in dogs with splenic haemangiosarcoma. Vet. Cop. Oncol. 2011, 9, 283–289. [Google Scholar] [CrossRef]
- Kim, S.E.; Liptak, J.M.; Gall, T.T.; Monteith, G.J.; Woods, J.P. Epirubicin in the adjuvant treatment of splenic hemangiosarcoma in dogs: 59 cases (1997–2004). J. Am. Vet. Med. Assoc. 2007, 231, 1550–1557. [Google Scholar] [CrossRef] [Green Version]
- Matsuyama, A.; Poirier, V.J.; Mantovani, F.; Foster, R.A.; Mutsaers, A.J. Adjuvant Doxorubicin with or without Metronomic Cyclophosphamide for Canine Splenic Hemangiosarcoma. J. Am. Anim. Hosp. Assoc. 2017, 53, 304–312. [Google Scholar] [CrossRef]
- Marconato, L.; Chalfon, C.; Finotello, R.; Polton, G.; Vasconi, M.E.; Annoni, M.; Stefanello, D.; Mesto, P.; Capitani, O.; Agnoli, C.; et al. Adjuvant anthracycline-based vs. metronomic chemotherapy vs. no medical treatment for dogs with metastatic splenic hemangiosarcoma: A multi-institutional retrospective study of the Italian Society of Veterinary Oncology. Vet. Comp. Oncol. 2019, 17, 537–544. [Google Scholar] [CrossRef]
- Faulhaber, E.A.; Janik, E.; Thamm, D.H. Adjuvant carboplatin for treatment of splenic hemangiosarcoma in dogs: Retrospective evaluation of 18 cases (2011–2016) and comparison with doxorubicin-based chemotherapy. J. Vet. Intern. Med. 2021, 35, 1929–1934. [Google Scholar] [CrossRef]
- Lana, S.; U’ren, L.; Plaza, S.; Elmslie, R.; Gustafson, D.; Morley, P.; Dow, S. Continuous Low-Dose Oral Chemotherapy for Adjuvant Therapy of Splenic Hemangiosarcoma in Dogs. J. Vet. Intern. Med. 2007, 21, 764–769. [Google Scholar] [CrossRef]
- Gardner, H.L.; London, C.A.; Portela, R.A.; Nguyen, S.; Rosengerb, M.P.; Klein, M.K.; Clifford, C.; Thamm, D.H.; Vail, D.; Bergman, P.; et al. Maintenance therapy with toceranib following doxorubicin-based chemotherapy for canine splenic hemangiosarcoma. BMC Vet. Res. 2015, 11, 131. [Google Scholar] [CrossRef] [Green Version]
- Borgatti, A.; Koopmeiners, J.S.; Sarver, A.L.; Winter, A.L.; Stuebner, K.; Todhunter, D.; Rizzardi, A.E.; Henriksen, J.C.; Schmechel, S.; Forster, C.L.; et al. Safe and Effective Sarcoma Therapy through Bispecific Targeting of EGFR and uPAR. Mol. Cancer Ther. 2017, 16, 956–965. [Google Scholar] [CrossRef] [Green Version]
- Borgatti, A.; Fieberg, A.; Winter, A.L.; Stuebner, K.; Taras, E.; Todhunter, D.; Masyr, A.; Rendhal, A.; Vallera, D.A.; Koopmeiners, J.S.; et al. Impact of Repeated Cycles of EGF Bispecific Angiotoxin (eBAT) Administered at a Reduced Interval from Doxorubicin Chemotherapy in Dogs with Splenic Hemangiosarcoma. Vet. Comp. Oncol. 2020, 18, 664–674. [Google Scholar] [CrossRef]
- Bray, J.P.; Munday, J.S. Thalidomide Reduces Vascular Endothelial Growth Factor Immunostaining in Canine Splenic Hemangiosarcoma. Vet. Sci. 2020, 7, 67. [Google Scholar] [CrossRef]
- Dickerson, E.B.; Bryan, B.A. Beta Adrenergic Signaling: A Targetable Regulator of Angiosarcoma and Hemangiosarcoma. Vet. Sci. 2015, 2, 270–292. [Google Scholar] [CrossRef] [Green Version]
- Rains, S.L.; Amaya, C.N.; Bryan, B.A. Beta-adrenergic receptors are expressed across diverse cancers. Oncoscience 2017, 4, 95–105. [Google Scholar] [CrossRef] [Green Version]
- Fjaestad, K.Y.; Romer, A.M.A.; Goitea, V.; Johansen, A.Z.; Thorseth, M.L.; Carretta, M.; Engelhol, L.H.; Grontved, L.; Junker, N.; Madsen, D.H. Blockade of beta-adrenergic receptors reduces cancer growth and enhances the response to anti-CTLA4 therapy by modulating the tumor microenvironment. Oncogene 2022, 41, 1364–1375. [Google Scholar] [CrossRef]
- Amaya, C.N.; Perkins, M.; Belmont, A.; Herrera, C.; Nasrazadani, A.; Vargas, A.; Khayou, T.; Montoya, A.; Ballou, Y.; Galvan, D.; et al. Non-selective beta blockers inhibit angiosarcoma cell viability and increase progression free- and overall-survival in patients diagnosed with metastatic angiosarcoma. Oncoscience 2018, 5, 109–119. [Google Scholar] [CrossRef] [Green Version]
- Galván, D.C.; Ayyappan, A.P.; Bryan, B.A. Regression of primary cardiac angiosarcoma and metastatic nodules following propanolol as a single agent treatment. Oncoscience 2018, 5, 264–268. [Google Scholar] [CrossRef] [Green Version]
- Wagner, M.J.; Cranmer, L.D.; Loggers, E.T.; Pollack, S.M. Propanolol for the treatment of vascular sarcomas. J. Exp. Pharmacol. 2018, 10, 51–58. [Google Scholar] [CrossRef] [Green Version]
- HSAa, J.; Kim, J.H.; Amaya, C.N.; Witcher, C.; Khammanivong, A.; Korpela, D.M.; Brown, D.R.; Taylor, J.; Bryan, B.A.; Dickerson, E.B. Propanolol Sensitizes Vascular Sar-coma Cells to Doxorubicin by Altering Lysosomal Drug Sequestration and Drug Efflux. Front. Oncol. 2021, 10, 614288. [Google Scholar] [CrossRef]
- Brown, D.C.; Reetz, J. Single Agent Polysaccharopeptide Delays Metastases and Improves Survival in Naturally Occurring Hemangiosarcoma. Evid.-Based Complement. Altern. Med. 2012, 1, 384301. [Google Scholar] [CrossRef]
- Wirth, K.A.; Kow, K.; Salute, M.E.; Bacon, N.J.; Milner, R.J. In vitro effects of Yunnan Baiyao on canine hemangiosarcoma cell lines. Vet. Comp. Oncol. 2014, 14, 281–294. [Google Scholar] [CrossRef]
- Ciepluch, B.J.; Wilson-Robles, H.M.; Pashmakova, M.B.; Budke, C.M.; Ellison, G.W.; Manjin, K.M.T. Long-term postoperative effects of administration of allogeneic blood products in 104 dogs with hemangiosarcoma. Vet. Surg. 2018, 47, 1039–1045. [Google Scholar] [CrossRef]
- Gedney, A.; Salah, P.; Mahoney, J.A.; Kirck, E.; Martins, R.; Scavello, H.; Lenz, J.A.; Atherton, M.J. Evaluation of the anti-tumour activity of Coriolus versicolor polysaccharopeptide (I’m-Yunity) alone or in combination with doxorubicin for canine splenic hemangiosarcoma. Vet. Comp. Oncol. 2022, 20, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Andersen, N.J.; Nickoloff, B.J.; Dykema, K.J.; Bogulawski, E.A.; Krivochenitser, R.I.; Froman, R.E.; Dawes, M.J.; Baker, L.H.; Thomas, D.G.; Kamstock, D.A.; et al. Pharmacologic inhibition of MEK signaling prevents growth of canine hemangiosarcoma. Mol. Cancer Ther. 2013, 12, 1701–1714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyuen, A.A.; Meuten, T.; Rose, B.J.; Thamm, D.H. In vitro effects of PI3K/mTOR inhibition in canine hemangiosarcoma. PLoS ONE 2018, 13, e0200634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahl, K.; Gamlem, H.; Tverdal, A.; Glattre, E.; Moe, L. Canine vascular neoplasia—A population-based study of prognosis. APMIIS Suppl. 2008, 125, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Göritz, M.; Müller, K.; Krastel, D.; Staudacher, G.; Schmidt, P.; Kühn, M.; Nickel, R.; Schoon, H.A. Canine Splenic Haemangiosarcoma: Influence of Metastases, Chemotherapy and Growth Pattern on Post-splenectomy Survival and Expression of Angiogenic Factors. J. Comp. Pathol. 2013, 149, 30–39. [Google Scholar] [CrossRef]
- Teng, K.T.Y.; Devleesschauwer, B.; De Noordhout, C.M.; Bennett, P.; McGreevy, P.D.; Chiu, P.Y.; Toribio, J.A.L.M.L.; Dhand, N.K. Welfare-Adjusted Life Years (WALY): A novel metric of animal welfare that combines the im-pacts of impaired welfare and abbreviated lifespan. PLoS ONE 2018, 13, e0202580. [Google Scholar] [CrossRef] [Green Version]
- Rozolen, J.M.; Teodoro, T.G.W.; Sobral, R.A.; Sueiro, F.A.R.; Laufer-Amorim, R.; Elias, F.; Fonseca-Alves, C.E. Investigation of Prognostic Value of Claudin-5, PSMA, and Ki67 Expression in Canine Splenic Hemangiosarcoma. Animals 2021, 11, 2406. [Google Scholar] [CrossRef]
- Moore, A.S.; Rassnick, K.M.; Frimberger, A.E. Evaluation of clinical and histologic factors associated with survival time in dogs with stage II splenic hemangiosarcoma treated by splenectomy and adjuvant chemotherapy: 30 cases (2011–2014). J. Am. Vet. Med. Assoc. 2017, 251, 559–565. [Google Scholar] [CrossRef]
- Ware, W.A.; Hopper, D.L. Cardiac tumors in dogs: 1982–1995. J. Vet. Intern. Med. 1999, 13, 95–103. [Google Scholar] [CrossRef]
- Treggiari, E.; Pedro, B.; Dukes-McEwan, J.; Gelzer, A.R.; Blackwood, L. A descriptive review of cardiac tumours in dogs and cats. Vet. Comp. Oncol. 2017, 15, 273–288. [Google Scholar] [CrossRef] [Green Version]
- Weisse, C.; Soares, N.; Beal, M.W.; Steffey, M.A.; Drobatz, K.J.; Henry, C.J. Survival times in dogs with right atrial hemangiosarcoma treated by means of surgical resection with or without adjuvant chemotherapy: 23 cases (1986–2000). J. Am. Vet. Med. Assoc. 2005, 226, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Hoshi, K.; Hirakawa, A.; Chimura, S.; Kbayashi, M.; Machida, N. Epidemiological, clinical and pathological features of primary cardiac hemangiosarcoma in dogs: A review of 51 cases. J. Vet. Med. Sci. 2013, 75, 1433–1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cagle, L.A.; Epstein, S.E.; Owens, S.D.; Mellema, M.S.; Hopper, K.; Burton, A.G. Diagnostic yield of cytologic analysis of pericardial effusion in dogs. J. Vet. Intern. Med. 2014, 28, 66–71. [Google Scholar] [CrossRef] [Green Version]
- Fernández-del Palacio, M.J.; López, J.T.; del Río, A.B.; Alcaraz, J.S.; Pallarés, F.J.; Martinez, C.M. Left ventricular outflow tract obstruction secondary to hemangiosarcoma in a dog. J. Vet. Intern. Med. 2006, 20, 687–690. [Google Scholar] [CrossRef]
- Thompson, D.J.; Cave, N.J.; Scrimgeour, A.B.; Thompson, K.G. Haemangiosarcoma of the interventricular septum in a dog. N. Z. Vet. J. 2011, 59, 332–336. [Google Scholar] [CrossRef]
- Osuga, T.; Nakamura, K.; Morita, T.; Kaagawa, Y.; Ohta, H.; Takiguchi, M. Diastolic heart failure associated with hemangiosarcoma infiltrating left ventricular walls in a dog. Can. Vet. J. 2017, 58, 1167–1170. [Google Scholar] [PubMed]
- Maneval, K.L.; Karlin, E.T.; Dos Santos, L.; Priest, K. Third-degree atrioventricular block secondary to infiltrative cardiac hemangiosarcoma in a dog. J. Vet. Cardiol. 2022, 42, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Bunn, T.A.; Robveille, C.; Irwin, P.J.; Langner, K.F.A. A neurological presentation caused by brain metastases in a dog with interventricular septal hemangiosarcoma. Aust. Vet. J. 2021, 99, 119–123. [Google Scholar] [CrossRef]
- Scheuermann, L.M.; Gordon-Evans, W.J.; Nault, A.J. Systematic review of the treatment options for pericardial effusions in dogs. Vet. Surg. 2021, 50, 20–28. [Google Scholar] [CrossRef]
- Smiderle, A.P.; Endo, V.T.; Almagro, L.D.; Montagni, K.C.P.; Panini, B.M.; Paula, C.G.; Viott, A.M.; Jojima, F.S. Tamponamento cardíaco secundário ao hemangiossarcoma em cães. Acta Sci. Vet. 2021, 49, 1–5. [Google Scholar] [CrossRef]
- Johnson, M.S.; Martin, M.; Binns, S.; Day, M.J. A retrospective study of clinical findings, treatment and outcome in 143 dogs with pericardial effusion. J. Small. Anim. Pract. 2004, 45, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Robinson, D.M.; Quina, M.T.; Lurie, D.M. Pericardial hemangiosarcoma in a 10-year-old papillon. J. Am. Anim. Hosp. Assoc. 2018, 54, e545-04. [Google Scholar] [CrossRef]
- Arai, S.; Milley, E.P.; Lichtenberger, J.; Savidge, C.; Lawrence, J.; Côté, E. Metastatic cardiac hemangiosarcoma in a 6 year old wheaten terrier mix. Vet. Sci. 2019, 6, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pharr, J.W.; Holmberg, D.L.; Clark, E.G. Hemangiosarcoma in the main pulmonary artery of a dog. Vet. Radiol. Ultrasound 1992, 33, 78–82. [Google Scholar] [CrossRef]
- Girard, C.; Helie, P.; Odin, M. Intrapericardial neoplasia in dogs. J. Vet. Diagn. Investig. 1999, 11, 73–78. [Google Scholar] [CrossRef]
- Rutherford, L.; Stell, A.; Smith, K.; Kulendra, N. Hemothorax in three dogs with intrathoracic extracardiac hemangiosarcoma. J. Am. Anim. Osp. Assoc. 2016, 52, 325–329. [Google Scholar] [CrossRef] [Green Version]
- Gunasekaran, T.; Olivier, N.B.; Smedley, R.C.; Sanders, R.A. Pericardial effusion in a dog with pericardial hemangiosarcoma. J. Vet. Cardiol. 2019, 23, 81–87. [Google Scholar] [CrossRef]
- Laforcade, A.M.; Freeman, L.M.; Rozanski, E.A.; Rush, J.E. Biochemical analysis of pericardial fluid and whole blood in dogs with pericardial effusion. J. Vet. Intern. Med. 2005, 19, 833–836. [Google Scholar] [CrossRef]
- MacDonald, K.A.; Cagney, O.; Magne, M.L. Echocardiographic and clinicopathologic characterization of pericardial effusion in dogs: 107 cases (1985–2006). J. Am. Vet. Med. Assoc. 2009, 235, 1456–1461. [Google Scholar] [CrossRef]
- Rajagopalan, V.; Jesty, S.A.; Craig, L.E.; Gompf, R. Comparison of presumptive echocardiographic and definitive diagnoses of cardiac tumors in dogs. J. Vet. Intern. Med. 2013, 27, 1092–1096. [Google Scholar] [CrossRef] [Green Version]
- Boddy, K.N.; Sleeper, M.M.; Sammarco, C.D.; Weisse, C.; Ghods, S.; Litt, H.I. Cardiac magnetic resonance in the differentiation of neoplastic and nonneoplastic pericardial effusion. J. Vet. Intern. Med. 2011, 25, 1003–1009. [Google Scholar] [CrossRef]
- Boz, E.; Papa, M.; Claretti, M.; Bussadori, R.; Lopez, B.S.; Rossii, C.; Mazzoni, L.; Pradelli, D.; Bussadori, C.M. Real-time three-dimensional echocardiographic study of a cardiac hemangiosarcoma in a dog. J. Vet. Cardiol. 2020, 28, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Pedro, B.; Linney, C.; Navarro-Cubas, X.; Stephenson, H.; Dukes-McEwann, J.; Gelzer, A.R.; Kraus, M.S. Cytological diagnosis of cardiac masses with ultrasound guided fine needle aspirates. J. Vet. Cardiol. 2016, 18, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Shaw, S.P.; Rozanski, E.A.; Rush, J.E. Cardiac troponins I and T in dogs with pericardial effusion. J. Vet. Intern. Med. 2016, 18, 322–324. [Google Scholar] [CrossRef]
- Linde, A.; Summerfield, N.J.; Sleeper, M.M.; Wrightm, F.B.; Clifford, C.A.; Melgarejo, T.; Knight, D.H. Pilot study on cardiac troponin I levels in dogs with pericardial effusion. J. Vet. Cardiol. 2006, 8, 19–23. [Google Scholar] [CrossRef]
- Langhorn, R.; Willesen, J.L. Cardiac troponins in dogs and cats. J. Vet. Intern. Med. 2016, 30, 36–50. [Google Scholar] [CrossRef]
- Chun, R.; Kellihan, H.B.; Henik, R.A.; Stepien, R.L. Comparison of plasma cardiac troponin I concentrations among dogs with cardiac hemangiosarcoma, noncardiac hemangiosarcoma, other neoplasms, and pericardial effusion of nonhemangiosarcoma origin. J. Am. Et. Med. Assoc. 2010, 237, 806–811. [Google Scholar] [CrossRef]
- Clifford, C.A.; Mackin, A.J.; Henry, C.J. Treatment of canine hemangiosarcoma: 2000 and beyond. J. Vet. Intern. Med. 2000, 14, 479–485. [Google Scholar] [CrossRef]
- Crumbaker, D.M.; Rooney, M.B.; Case, J.B. Thoracoscopic subtotal pericardiectomy and right atrial mass resection in a dog. J. Am. Vet. Med. Assoc. 2010, 237, 551–554. [Google Scholar] [CrossRef]
- Ployart, S.; Libermann, S.; Doran, I.; Bomassi, E.; Monnet, E. Thoracoscopic resection of right auricular masses in dogs: 9 cases (2003–2011). J. Am. Vet. Med. Assoc. 2013, 242, 237–241. [Google Scholar] [CrossRef]
- Verbeke, F.; Binst, D.; Stegen, L.; Waelbers, R.; de Rooster, H.; Van Goethem, B. Total venous inflow occlusion and pericardial auto-graft reconstruction for right atrial hemangiosarcoma resection in a dog. Can. Vet. J. 2012, 53, 1114–1118. [Google Scholar]
- Jackson, J.; Richter, K.P.; Launer, D.P. Thoracoscopic partial pericardiectomy in 13 dogs. J. Vet. Intern. Med. 1999, 13, 529–533. [Google Scholar] [CrossRef]
- Nolan, M.W.; Arkans, M.M.; LaVine, D.; DeFrancesco, T.; Myers, J.A.; Friffth, E.H.; Posner, L.P.; Keene, B.W.; Tou, S.P.; Gieger, T.L. Pilot study to determine the fea-sibility of radiation therapy for dogs with right atrial masses and hemorrhagic pericardial effusion. J. Vet. Cardiol. 2017, 19, 132–143. [Google Scholar] [CrossRef]
- Murphy, L.A.; Panek, C.M.; Bianco, D.; Nakamura, R.K. Use of Yunnan Baiyao and epsilon aminocaproic acid in dogs with right atrial masses and pericardial effusion. J. Vet. Emerg. Crit. Care 2017, 27, 121–126. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primary tumor (T) | |
| T0 | No evidence of tumor |
| T1 | Primary tumor confined to the dermis |
| T2 | Primary tumor involving the hypodermis, with or without concomitant dermal involvement. No muscle involvement |
| T3 | Any primary tumor with muscle involvement |
| Regional Lymph Nodes (N) | |
| N0 | No involvement of regional lymph nodes |
| N1 | Involvement of regional lymph nodes |
| N2 | Distant lymph node involvement |
| Distant Metastasis (M) | |
| M0 | No evidence of distant metastases |
| M1 | Presence of distant metastases |
| Staging | |
| I | T0 or T1; N0; M0 |
| II | T2; N0, N1 or N2; M0 |
| III | T1, T2 or T3; N0, N1 or N2; M1 |
| Chemotherapy Protocol | N | HSA Type | Surgery | Mean Survival Time (Days) |
|---|---|---|---|---|
| VAC Protocol (Hammer et al., 1991) [32] | 4 | Subcutaneous | Incomplete resection (n = 4) | 436 |
| AC Protocol (Sorenmo et al., 1993) [23] | 5 | Subcutaneous | Complete resection (n = 2); Incomplete resection (n = 3) | 240 |
| Doxorrubicin +/− Cyclofosfamide (Bulakowski et al., 2008) [25] | 21 | Subcutaneous (n = 17) Intramuscular (n = 4) | Complete resection (in the first surgery—n = 11; in the second surgery—n = 5); Adjuvant radiotherapy after incomplete resection (n = 5) a | 1189 (subcutaneous) 272 (intramuscular) b |
| Doxorrubicin +/− ciclofosfamide, vincristine or lomustine (Shiu et al., 2011) [26] | 36 | Subcutaneous (n = 55) Intramuscular (n = 16) | Complete resection (n = 18); Incomplete resection (n = 18) | 212 (subcutaneous) 136 (intramuscular) c |
| Positive | Negative | |
|---|---|---|
| Tissue of origin | Dermis (stage I) | Subcutaneous and muscle (stage II and III) |
| Subcutaneous or muscular invasion | Absent | Present |
| Actinic lesions | Present | Absent |
| Breeds | Predisposed breeds | Non-predisposed breeds |
| Surgical margins | Complete | Incomplete |
| Tumor size | <4 cm | >4 cm |
| Primary Tumor (T) | |
| T0 | No evidence of tumor |
| T1 | Tumor less than 5 cm in diameter, confined to one organ |
| T2 | Tumor greater than or equal to 5 cm in diameter, ruptured |
| T3 | Tumor with invasion of adjacent structures |
| Regional Lymph Nodes (N) | |
| N0 | No involvement of regional lymph nodes |
| N1 | Involvement of regional lymph nodes |
| N2 | Distant lymph node involvement |
| Distant Metastasis (M) | |
| M0 | No evidence of distant metastases |
| M1 | Presence of distant metastases |
| Staging | |
| I | T0 or T1; N0; M0 |
| II | T2; N0, N1 or N2; M0 |
| III | T1, T2 or T3; N0, N1 or N2; M1 |
| Primary Tumor (T) | |
| T0 | No evidence of tumor |
| T1 | Tumor confined to one organ, without evidence of rupture |
| T2 | Tumor with evidence of rupture |
| Regional Lymph Nodes (N) | |
| N0 | No involvement of regional lymph nodes |
| N1 | Confirmed lymph node metastasis |
| Metástases distantes (M) | |
| M0 | No evidence of distant metastases |
| M1 | Presence of distant metastases |
| Staging | |
| I | T0 or T1; N0; M0 |
| II | T1; N1; M0; or T2; N0; M0 |
| III | T1, T2 or T3; N0, N1 or N2; M1 |
| Clinical Staging | Median Survival Time (Days) | |||||
|---|---|---|---|---|---|---|
| Sorenmo et al. 1993 [23] | Kim et al. 2007 [150] | Wendelburg et al. 2015 [33] | Matsuyama et al. 2017 [151] | Batschinski et al. 2018 [146] | Ciepluch et al. 2018 [168] | |
| I | 250 | 345 | 160 | 259 | 196 | 193 |
| II | 186 | 93 | 60 | 125 | 117 | 105 |
| III | 87 | 68 | 30 | 62 | 23 | 63 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Nardi, A.B.; de Oliveira Massoco Salles Gomes, C.; Fonseca-Alves, C.E.; de Paiva, F.N.; Linhares, L.C.M.; Carra, G.J.U.; dos Santos Horta, R.; Ruiz Sueiro, F.A.; Jark, P.C.; Nishiya, A.T.; et al. Diagnosis, Prognosis, and Treatment of Canine Hemangiosarcoma: A Review Based on a Consensus Organized by the Brazilian Association of Veterinary Oncology, ABROVET. Cancers 2023, 15, 2025. https://doi.org/10.3390/cancers15072025
De Nardi AB, de Oliveira Massoco Salles Gomes C, Fonseca-Alves CE, de Paiva FN, Linhares LCM, Carra GJU, dos Santos Horta R, Ruiz Sueiro FA, Jark PC, Nishiya AT, et al. Diagnosis, Prognosis, and Treatment of Canine Hemangiosarcoma: A Review Based on a Consensus Organized by the Brazilian Association of Veterinary Oncology, ABROVET. Cancers. 2023; 15(7):2025. https://doi.org/10.3390/cancers15072025
Chicago/Turabian StyleDe Nardi, Andrigo Barboza, Cristina de Oliveira Massoco Salles Gomes, Carlos Eduardo Fonseca-Alves, Felipe Noleto de Paiva, Laís Calazans Menescal Linhares, Gabriel João Unger Carra, Rodrigo dos Santos Horta, Felipe Augusto Ruiz Sueiro, Paulo Cesar Jark, Adriana Tomoko Nishiya, and et al. 2023. "Diagnosis, Prognosis, and Treatment of Canine Hemangiosarcoma: A Review Based on a Consensus Organized by the Brazilian Association of Veterinary Oncology, ABROVET" Cancers 15, no. 7: 2025. https://doi.org/10.3390/cancers15072025