
Lung Cancer as a Leading Cause among Paraneoplastic Non-Bacterial Thrombotic Endocarditis: A Meta-Analysis of Individual Patients’ Data

 ,
,  , ,
, ,  , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Data Extraction and Quality Assessment
2.3. Outcomes of Interest
2.4. Follow-Up and Survival Analysis
2.5. Statistical Analysis
3. Results
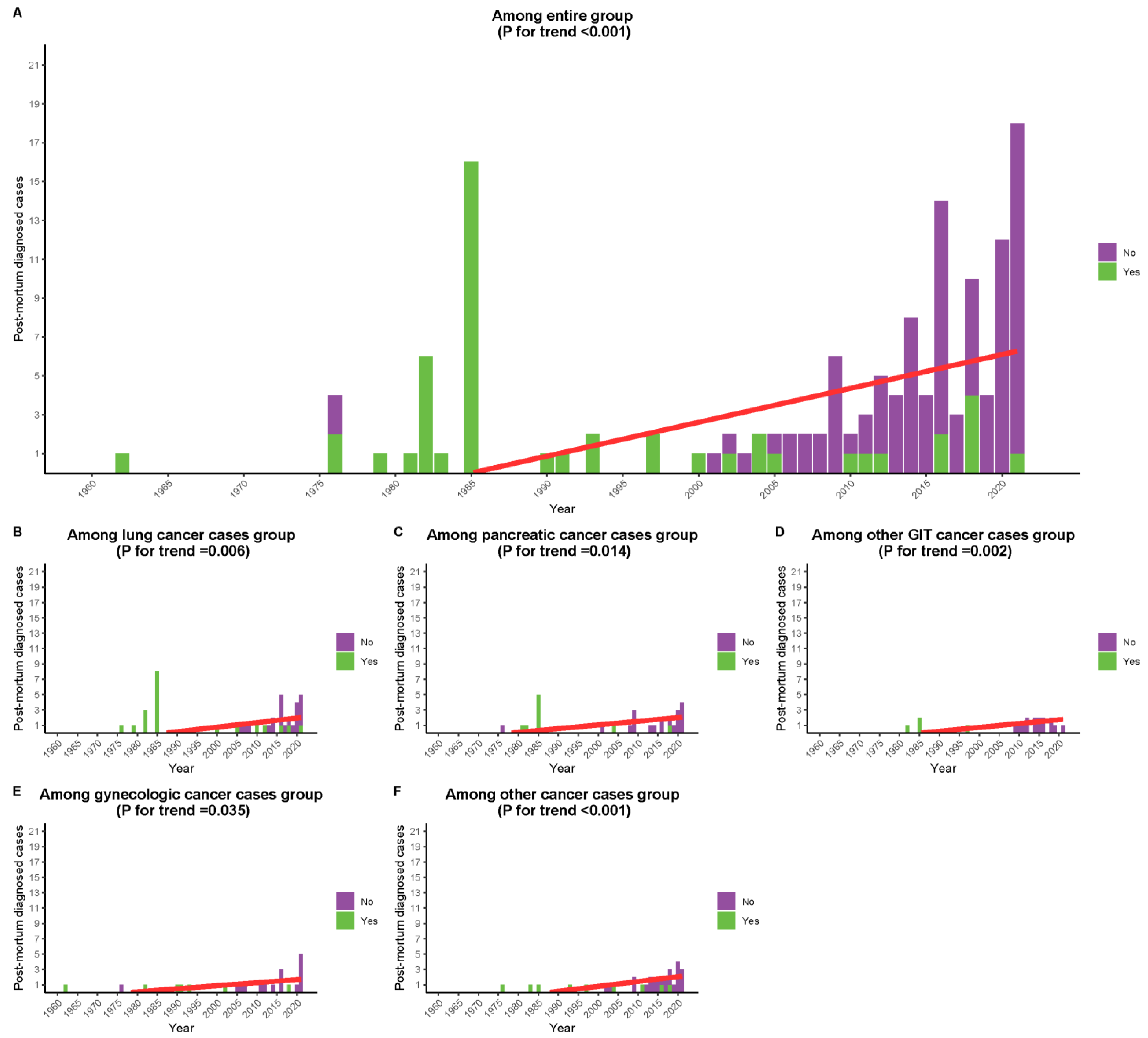
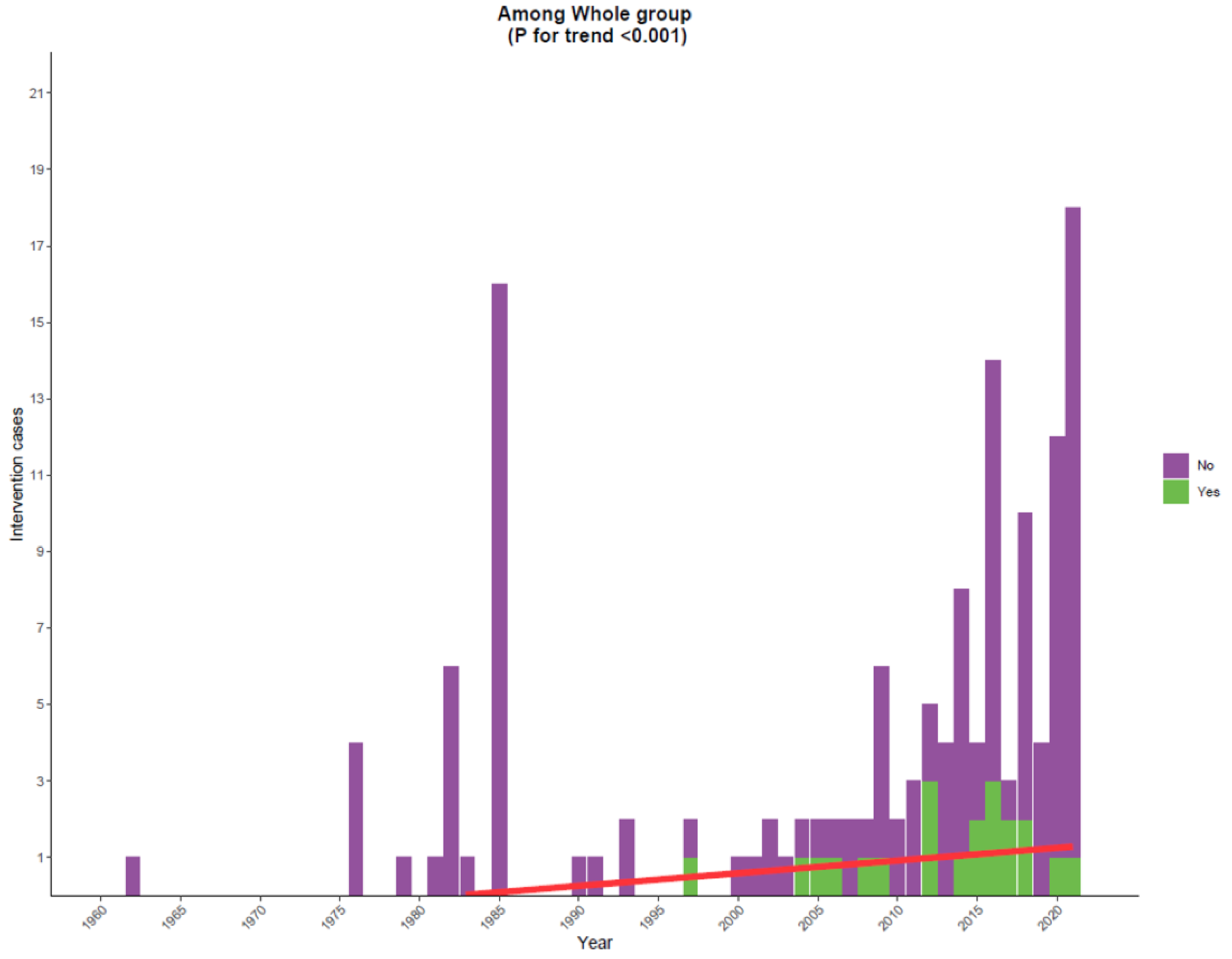
3.1. Trend Analysis
3.2. Survival Analysis
4. Discussion
4.1. Demographic, Clinical, and Pathologic Characteristics
4.2. Presentation and Diagnosis
4.3. Management
4.4. Prognosis
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Baron, J.A.; Gridley, G.; Weiderpass, E.; Nyren, O.; Linet, M. Venous thromboembolism and cancer. Lancet 1998, 351, 1077–1080. [Google Scholar] [CrossRef]
- Schmaier, A.A.; Ambesh, P.; Campia, U. Venous thromboembolism and cancer. Curr. Cardiol. Rep. 2018, 20, 1–10. [Google Scholar] [CrossRef]
- Trousseau, A. Lectures on Clinical Medicine; Lindsay & Blakiston: Pennsylvania, PA, USA, 1873; Volume 2. [Google Scholar]
- Ziegler, E. Ueber den Bau und die Entstehung der endocaridtis chen Efflorescenzen. Ver. Kong Inn. Med. 1888, 7, 339–343. [Google Scholar]
- Gross, L.; FRIEDBERG, C.K. Nonbacterial thrombotic endocarditis: Classification and general description. Arch. Intern. Med. 1936, 58, 620–640. [Google Scholar] [CrossRef] [Green Version]
- Libman, E. Characterization of various forms of endocarditis. J. Am. Med. Assoc. 1923, 80, 813–818. [Google Scholar] [CrossRef]
- Lopez, J.A.; Ross, R.S.; Fishbein, M.C.; Siegel, R.J. Nonbacterial thrombotic endocarditis: A review. Am. Heart J. 1987, 113, 773–784. [Google Scholar] [CrossRef]
- Bussani, R.; De-Giorgio, F.; Pesel, G.; Zandonà, L.; Sinagra, G.; Grassi, S.; Baldi, A.; Abbate, A.; Silvestri, F. Overview and comparison of infectious endocarditis and non-infectious endocarditis: A review of 814 autoptic cases. In Vivo 2019, 33, 1565–1572. [Google Scholar] [CrossRef] [Green Version]
- Joffe, I.I.; Jacobs, L.E.; Owen, A.N.; Ioli, A.; Kotler, M.N. Noninfective valvular masses: Review of the literature with emphasis on imaging techniques and management. Am. Heart J. 1996, 131, 1175–1183. [Google Scholar] [CrossRef]
- Deppisch, L.M.; Fayemi, A.O. Non-bacterial thrombotic endocarditis: Clinicopathologic correlations. Am. Heart J. 1976, 92, 723–729. [Google Scholar] [CrossRef] [Green Version]
- Llenas-García, J.; Guerra-Vales, J.M.; Montes-Moreno, S.; López-Ríos, F.; Castelbón-Fernández, F.J.; Chimeno-García, J. Nonbacterial thrombotic endocarditis: Clinicopathologic study of a necropsy series. Rev. Española De Cardiol. (Engl. Ed.) 2007, 60, 493–500. [Google Scholar] [CrossRef]
- Candela, M.; Vidal, C.; Roman, J.; Aramburo, P. Non-bacterial thrombotic endocarditis in cancer patients. Acta Cardiol. 1991, 46, 1–9. [Google Scholar]
- Edoute, Y.; Haim, N.; Rinkevich, D.; Brenner, B.; Reisner, S.A. Cardiac valvular vegetations in cancer patients: A prospective echocardiographic study of 200 patients. Am. J. Med. 1997, 102, 252–258. [Google Scholar] [CrossRef]
- Dutta, T.; Karas, M.G.; Segal, A.Z.; Kizer, J.R. Yield of transesophageal echocardiography for nonbacterial thrombotic endocarditis and other cardiac sources of embolism in cancer patients with cerebral ischemia. Am. J. Cardiol. 2006, 97, 894–898. [Google Scholar] [CrossRef]
- Zmaili, M.A.; Alzubi, J.M.; Kocyigit, D.; Bansal, A.; Samra, G.S.; Grimm, R.; Griffin, B.P.; Xu, B. A contemporary 20-year Cleveland Clinic experience of nonbacterial thrombotic endocarditis: Etiology, echocardiographic imaging, management, and outcomes. Am. J. Med. 2021, 134, 361–369. [Google Scholar] [CrossRef]
- Singhal, A.B.; Topcuoglu, M.A.; Buonanno, F.S. Acute ischemic stroke patterns in infective and nonbacterial thrombotic endocarditis: A diffusion-weighted magnetic resonance imaging study. Stroke 2002, 33, 1267–1273. [Google Scholar] [CrossRef] [Green Version]
- Mazokopakis, E.E.; Syros, P.K.; Starakis, I.K. Nonbacterial thrombotic endocarditis (marantic endocarditis) in cancer patients. Cardiovasc. Haematol. Disord.-Drug Targets (Former. Curr. Drug Targets-Cardiovasc. Hematol. Disord.) 2010, 10, 84–86. [Google Scholar] [CrossRef]
- Estevez, C.M.; Corya, B.C. Serial echocardiographic abnormalities in nonbacterial thrombotic endocarditis of the mitral valve. Chest 1976, 69, 801–804. [Google Scholar] [CrossRef] [Green Version]
- Patel, M.J.; Elzweig, J. Non-bacterial thrombotic endocarditis: A rare presentation and literature review. BMJ Case Rep. 2020, 13, e238585. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K. Chapter 7: Systematic reviews of etiology and risk. In Joanna Briggs Institute Reviewer’s Manual; The Joanna Briggs Institute: Adelaide, Australia, 2020; Volume 5, Available online: https://synthesismanual.jbi.global (accessed on 12 March 2023).
- Ahmed, S.; Jani, P.; Yamani, M.H.; Ailawadhi, S.; Alegria, V.R.; Ailawadhi, M. Marantic endocarditis associated with T-cell large granular lymphocytic leukemia: First report of its occurrence with a lymphoproliferative malignancy in adults. J. Oncol. Pract. 2018, 14, 625–627. [Google Scholar] [CrossRef]
- Alaiti, M.A.; Hoit, B.D. Nonbacterial thrombotic endocarditis. Echocardiography 2015, 32, 1051–1052. [Google Scholar] [CrossRef] [Green Version]
- Albright, B.B.; Black, J.D.; Vilardo, N.; Schwartz, P.E. Correction of coagulopathy associated with non-bacterial thrombotic endocarditis (NBTE) by surgical debulking in a case of ovarian clear cell carcinoma. Gynecol. Oncol. Rep. 2016, 17, 13. [Google Scholar] [CrossRef] [Green Version]
- Ali, N.; Konstantinov, I.; Heath, J.A.; Bhagwat, K.; Cheung, M. Nonbacterial thrombotic endocarditis in a child with non-Hodgkin’s lymphoma. Pediatr. Cardiol. 2012, 33, 843–845. [Google Scholar] [CrossRef]
- Ali, M. Non-bacterial thrombotic endocarditis and subclinical myopericarditis in a patient with advanced rectal cancer. Case Rep. 2015, 2015, bcr2015212820. [Google Scholar]
- Arvold, N.D.; Hsu, L.; Chen, W.Y.; Benzaquen, L.R.; Weiss, S.E. Marantic endocarditis with cardioembolic strokes mimicking leptomeningeal metastases in breast cancer. J. Clin. Oncol. 2011, 29, e743–e746. [Google Scholar] [CrossRef]
- Ashenhurst, E.; Chertkow, G. Cerebral embolism from nonbacterial thrombotic endocarditis. Can. Med. Assoc. J. 1962, 86, 313. [Google Scholar]
- Bhardwaj, B.; Bajwa, A.; Sharma, A.; Towheed, A.; Sanghani, B.V.; McGhie, A.I. Nonbacterial thrombotic endocarditis involving both the tricuspid and aortic valves. Echocardiography 2016, 33, 1916–1918. [Google Scholar] [CrossRef]
- Binet, Q.; Goffinet, C.; Etogo-Asse, F.-E.; Shaza, L. Nonbacterial thrombotic endocarditis in a patient with gastric cancer and SARS-CoV-2 infection. Clin. J. Gastroenterol. 2021, 14, 1031–1035. [Google Scholar] [CrossRef]
- Borowski, A.; Ghodsizad, A.; Cohnen, M.; Gams, E. Recurrent embolism in the course of marantic endocarditis. Ann. Thorac. Surg. 2005, 79, 2145–2147. [Google Scholar] [CrossRef]
- Chen, L.; Li, Y.; Gebre, W.; Lin, J.H. Myocardial and cerebral infarction due to nonbacterial thrombotic endocarditis as an initial presentation of pancreatic adenocarcinoma. Arch. Pathol. Lab. Med. 2004, 128, 1307–1308. [Google Scholar] [CrossRef]
- Cheung, B.; Shivkumar, A.; Ahmed, A.S. Embolic showering from non-bacterial thrombotic endocarditis and adenocarcinoma of the lung. Eur. J. Case Rep. Intern. Med. 2020, 7, 001798. [Google Scholar]
- Chisholm, J.C., Jr.; Ireland, C.S.; Scott, R.N. Bronchogenic carcinoma, leukemoid reaction, marantic endocarditis, and consumptive thrombocytopathy. J. Natl. Med. Assoc. 1982, 74, 447. [Google Scholar]
- Clough, H.; George, J.; Duncan, A. Psychosis due to non-bacterial thrombotic endocarditis. Age Ageing 2010, 39, 276–277. [Google Scholar] [CrossRef] [Green Version]
- Detremerie, C.; Timmermans, F.; De Pauw, M.; Gheeraert, P.; Hemelsoet, D.; Toeback, J.; Bové, T.; Vandecasteele, E. Stroke due to non-bacterial thrombotic endocarditis as initial presentation of breast invasive ductal carcinoma. Acta Clin. Belg. 2017, 72, 268–273. [Google Scholar] [CrossRef]
- Dewey, N.; Mughal, L.H.; Houghton, A.R.; Khoo, J. Right ventricular marantic endocarditis. Echo Res. Pract. 2015, 2, I3. [Google Scholar] [CrossRef] [Green Version]
- Douin, C.; Marchetta, S.; Dulgheru, R.; Bruyère, P.-J.; Moonen, M.; Lancellotti, P. Case report: Aortic bioprosthesis marantic endocarditis. Acta Cardiol. 2021, 76, 1143–1144. [Google Scholar] [CrossRef]
- Elboudwarej, O.; Wei, J.; Siegel, R. Diagnosis of an aortic valvular lesion. Heart 2015, 101, 719. [Google Scholar] [CrossRef] [Green Version]
- Fanale, M.A.; Zeldenrust, S.R.; Moynihan, T.J. Case 2. Marantic endocarditis in advanced cancer. J. Clin. Oncol. 2002, 20, 4111–4114. [Google Scholar] [CrossRef]
- Farooqui, A.A.; Ashraf, R.; D’Ornellas, R.; Aslam, A.; Marcelin, M.; Shetty, V. Tricuspid Valve Vegetation Secondary to Ovarian Cancer Leading to Acute Stroke via Pulmonary Arteriovenous Malformation. Cureus 2021, 13, e17136. [Google Scholar] [CrossRef]
- Ferreira, T.L.; Alves, R.; Judas, T.; Delerue, M.F. Marantic endocarditis and paraneoplastic pulmonary embolism. Case Rep. 2017, 2017, bcr2017220217. [Google Scholar] [CrossRef]
- Fournier, J.B.; Testa, E.J. Nonbacterial thrombotic endocarditis. N. Engl. J. Med. 2019, 380, e48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frazer, G.; Laing, R.; Lamont, D. Non-bacterial thrombotic endocarditis with a negative transesophageal echocardiogram. N. Z. Med. J. (Online) 2005, 118, U1589. [Google Scholar]
- Fujimoto, D.; Mochizuki, Y.; Nakagiri, K.; Shite, J. Unusual rapid progression of non-bacterial thrombotic endocarditis in a patient with bladder cancer despite undergoing intensification treatment with rivaroxaban for acute venous thromboembolism. Eur. Heart J. 2018, 39, 3907. [Google Scholar] [CrossRef]
- Garcia, I.; Fainstein, V.; Rios, A.; Luna, M.; Mansell, P.; Reuben, J.; Hersh, E. Nonbacterial thrombotic endocarditis in a male homosexual with Kaposi’s sarcoma. Arch. Intern. Med. 1983, 143, 1243–1244. [Google Scholar] [CrossRef]
- Glass, J.P. The diagnosis and treatment of stroke in a patient with cancer: Nonbacterial thrombotic endocarditis (NBTE): A case report and review. Clin. Neurol. Neurosurg. 1993, 95, 315–318. [Google Scholar] [CrossRef]
- Gray, K.M.; Nguyen, B.; Baker, L.; Ahmad, M. Non-bacterial thrombotic endocarditis and coronary thrombectomy in a patient with metastatic small cell lung carcinoma. BMJ Case Rep. 2021, 14, e239893. [Google Scholar] [CrossRef]
- Green, S. Two unusual cardiac complications of gynaecological malignancy: Myocardial metastases and non-infective thrombotic endocarditis. Br. J. Clin. Pract. 1990, 44, 74–75. [Google Scholar]
- Gundersen, H.; Moynihan, B. An uncommon cause of stroke: Non-bacterial thrombotic endocarditis. J. Stroke Cerebrovasc. Dis. 2016, 25, e163–e164. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.Z.; Ternouth, I.; Lallu, B.D. Case report: Marantic endocarditis in renal cell carcinoma: Nephrectomy a treatment. Eur. Heart J.-Case Rep. 2021, 5, ytab437. [Google Scholar] [CrossRef]
- Hofstra, J.; Timmer, J.; Breeman, A.; Havenith, M. Non-bacterial thrombotic endocarditis in metastatic caecal adenocarcinoma. Neth. Heart J. 2009, 17, 349–350. [Google Scholar] [CrossRef] [Green Version]
- Holt, J.N. A case of multifocal stroke—The first presentation of underlying ovarian malignancy. J. Surg. Case Rep. 2021, 2021, rjaa550. [Google Scholar] [CrossRef]
- Ilyas, S.; Lang, W.; Belani, N.; Philip Stockwell, M. Non-bacterial thrombotic endocarditis as a Cause of Cryptogenic Stroke in Malignancy. Rhode Isl. Med. J. 2021, 104, 63–66. [Google Scholar]
- Iranpour, A.; Mahmoodian, R.; Haghighi, A.; Vakili, M.; Shahriari-Ahmadi, A.; Hajsadeghi, S.; Arabi, M. A 34 Year Old Man with Purple Discoloration and Paresthesia. Int. J. Hematol.-Oncol. Stem Cell Res. 2014, 8, 41. [Google Scholar] [PubMed]
- Ito, S.; Yoshitomi, H.; Pak, M.; Kawahara, H.; Oshima, T.; Ito, S.; Watanabe, N.; Sato, H.; Adachi, T.; Takeda, M. Trousseau syndrome with nonbacterial thrombotic endocarditis in a patient with uterine cancer. Intern. Med. 2013, 52, 1353–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jameson, G.S.; Ramanathan, R.K.; Borad, M.J.; Downhour, M.; Korn, R.; Von Hoff, D. Marantic endocarditis associated with pancreatic cancer: A case series. Case Rep. Gastroenterol. 2009, 3, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.B.; Richards, M.J.; Holt, D.Q.; Yan, B.P.; Aggarwal, A. Marantic endocarditis presenting as recurrent arterial embolisation. Int. J. Cardiol. 2009, 132, e14–e16. [Google Scholar] [CrossRef]
- Julson, J.R.; Weiland, T.; Kemp, W.L. Acute subdural hemorrhage associated with both metastatic adenocarcinoma of the dura and minor head trauma: A case report and review of the literature. Acad. Forensic Pathol. 2018, 8, 769–776. [Google Scholar] [CrossRef]
- Kalangos, A.; Pretre, R.; Girardet, C.; Ricou, F.; Faidutti, B. An atypical aortic valve non-bacterial thrombotic endocarditis in the course of multiple myeloma. Eur. Heart J. 1997, 18, 351–352. [Google Scholar] [CrossRef] [Green Version]
- Kaneyuki, D.; Matsuura, K.; Ueda, H.; Kohno, H.; Kanbe, M.; Matsumiya, G. Surgical management of nonbacterial thrombotic endocarditis in malignancy. Surg. Case Rep. 2017, 3, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Kanthasamy, V.; Natarajan, I. Rare and challenging case of stroke as a manifestation of non bacterial thrombotic endocarditis in an underlying ovarian clear cell carcinoma. JRSM Open 2016, 7, 2054270416669304. [Google Scholar] [CrossRef] [Green Version]
- Kaufmann, C.C.; Wessely, E.; Huber, K. Non-bacterial thrombotic endocarditis in the context of pulmonary adenocarcinoma: A case report. Eur. Heart J. Case Rep. 2020, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Kearsley, J.H.; Tattersall, M.H. Cerebral embolism in cancer patients. Q. J. Med. 1982, 51, 279–291. [Google Scholar]
- Khan, O.A.; Rogers, V.; Sharma, R.; Ohri, S.K. Lung cancer masquerading as prosthetic valve endocarditis. Heart Lung Circ. 2008, 17, 161–163. [Google Scholar] [CrossRef]
- Khan, K.A.; Wahid, K.; Qureshi, S.U. Nonbacterial thrombotic endocarditis as the initial presentation of prostate cancer- a case report. J. Pak. Med. Assoc. 2019, 69, 1737–1740. [Google Scholar] [CrossRef]
- Kijpaisalratana, N.; Chutinet, A.; Travanichakul, S.; Kitjawijit, T.; Yokumporn, P.; Duangjino, K.; Suwanwela, N.C. Nonbacterial thrombotic endocarditis related to adenocarcinoma of the uterine cervix. Case Rep. Neurol. 2020, 12, 183–188. [Google Scholar] [CrossRef]
- Kimyai-Asadi, A.; Usman, A.; Milani, F. Cutaneous manifestations of marantic endocarditis. Int. J. Dermatol. 2000, 39, 290–292. [Google Scholar] [CrossRef]
- Kooiker, J.C.; MacLean, J.M.; Sumi, S.M. Cerebral embolism, marantic endocarditis, and cancer. Arch. Neurol. 1976, 33, 260–264. [Google Scholar] [CrossRef]
- Kuipers, R.S.; Berghuis, M.A.; Ogilvie, A.C.; van Wissen, S.A.; Riezebos, R.K. Non-bacterial thrombotic endocarditis manifested by ventricular fibrillation in a patient with low grade ovarian carcinoma: Case report and literature review. Eur. Heart J.-Case Rep. 2021, 5, ytab120. [Google Scholar] [CrossRef]
- Kurdi, M.; Beanlands, D.S.; Chan, K.L.; Veinot, J.P. Nonbacterial thrombotic endocarditis presenting as aortic stenosis with suspected infective endocarditis: Clinicopathological correlation. Can. J. Cardiol. 2004, 20, 549–552. [Google Scholar]
- Kwon, S.; Jeon, J.; Kim, J.; Kim, M.-J.; Yoon, J.S. Neoplastic non-bacterial endocarditis of the aortic valve. Eur. Heart J.–Cardiovasc. Imaging 2017, 18, 605. [Google Scholar] [CrossRef]
- Lal, G.; Brennan, T.V.; Hambleton, J.; Clark, O.H. Coagulopathy, marantic endocarditis, and cerebrovascular accidents as paraneoplastic features in medullary thyroid cancer—Case report and review of the literature. Thyroid 2003, 13, 601–605. [Google Scholar] [CrossRef]
- Lee, V.; Gilbert, J.D.; Byard, R.W. Marantic endocarditis–a not so benign entity. J. Forensic Leg. Med. 2012, 19, 312–315. [Google Scholar] [CrossRef]
- Lee, J.M.; Lim, J.H.; Kim, J.-S.; Park, J.S.; Memon, A.; Lee, S.-K.; Nam, H.-S.; Cho, J.-H.; Kwak, S.-M.; Lee, H.L. Multiple hypercoagulability disorders at presentation of non-small-cell lung cancer. Tuberc. Respir. Dis. 2014, 77, 34–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makhdumi, M.; Meyer, D.M.; Roberts, W.C. Malignancy-Associated Non-Bacterial Thrombotic Endocarditis Causing Aortic Regurgitation and Leading to Aortic Valve Replacement. Am. J. Cardiol. 2021, 154, 120–122. [Google Scholar] [CrossRef]
- Mantovani, F.; Navazio, A.; Barbieri, A.; Boriani, G. A first described case of cancer-associated non-bacterial thrombotic endocarditis in the era of direct oral anticoagulants. Thromb. Res. 2017, 149, 45–47. [Google Scholar] [CrossRef]
- Marglani, O.; Al-Herabi, A.; Odell, P. Marantic endocarditis as an unusual paraneoplastic syndrome of head and neck squamous cell carcinoma. J. Otolaryngol.-Head Neck Surg. 2009, 38, E76. [Google Scholar]
- Markides, V.; Nihoyannopoulos, P. Non-bacterial thrombotic endocarditis. Eur. J. Echocardiogr. 2000, 1, 291–294. [Google Scholar] [CrossRef] [Green Version]
- Martín-Martorell, P.; Insa-Molla, A.; Chirivella-González, M.I.; Cervera-Miguel, J.I. Nonbacterial thrombotic endocarditis associated with lung adenocarcinoma. Clin Transl Oncol 2007, 9, 744–746. [Google Scholar] [CrossRef] [PubMed]
- Mitma, A.A.; Varghese, J.G.; Witt, D.; Zarich, S.W. Stroke and a valvular lesion in a patient with stage IV non-small cell lung cancer. Case Rep. 2016, 2016, bcr2016215317. [Google Scholar] [CrossRef]
- Morimoto, S.; Tanaka, J.; Saito, Y.; Tsuyama, N.; Nishimura, T.; Komiya, T.; Kyo, S.; Arai, T.; Kanemaru, A.; Kanemaru, K.; et al. Non-bacterial thrombotic endocarditis in a Trousseau syndrome patient with stomach cancer: A case report. Geriatr. Gerontol. Int. 2016, 16, 1171–1172. [Google Scholar] [CrossRef] [PubMed]
- Moţăţăianu, A.; Maier, S.; Gothard, A.; Bajkó, Z.; Bălaşa, R. Severe Fatal Systemic Embolism Due to Non-Bacterial Thrombotic Endocarditis as the Initial Manifestation of Gastric Adenocarcinoma: Case Report. J. Crit. Care Med. (Targu Mures) 2018, 4, 68–73. [Google Scholar] [CrossRef] [Green Version]
- Nadkarni, N.; Lee, Y.J.; Hoefen, R.; Alweis, R. Cholangiocarcinoma manifesting as non-bacterial thrombotic endocarditis in a young patient. Am. J. Med. 2020, 133, e396–e398. [Google Scholar] [CrossRef]
- Nakashima, K.; Mori, M.; Haraki, T.; Hirase, H.; Yoshimuta, T.; Ichida, F.; Okeie, K.; Konno, T.; Hayashi, K.; Ino, H.; et al. Non-bacterial thrombotic endocarditis associated with Trousseau’s syndrome. J. Echocardiogr. 2012, 10, 115–116. [Google Scholar] [CrossRef] [PubMed]
- Neilan, T.G.; Price, M.C.; Sanborn, D.Y.; Gainor, J.F.; Chen, A. Case 33-2018: A 57-Year-Old Man with Confusion, Fever, Malaise, and Weight Loss. N. Engl. J. Med. 2018, 379, 1658–1669. [Google Scholar] [CrossRef]
- Al Nidawi, F.; Mohamed, M.W.; Taha, F.; Alarab, D.; Hussein, A.E.M. Recurrent Strokes as the First Presentation of Occult Pancreatic Cancer; Trousseau Syndrome: A Case Report. Case Rep. Oncol. 2021, 14, 1741–1747. [Google Scholar] [CrossRef]
- Numnum, T.M.; Leath III, C.A.; Straughn Jr, M.J. Synchronous primary endometrial and ovarian carcinoma in a patient with marantic endocarditis. Obstet. Gynecol. 2006, 108, 748–750. [Google Scholar] [CrossRef]
- O’Boyle, C.P.; Dempsey, J.; Otridge, B.; Barniville, H. Malignant islet-cell tumour of the pancreas presenting with non-bacterial thrombotic endocarditis and eosinophilia. Postgrad. Med. J. 1981, 57, 457–458. [Google Scholar] [CrossRef] [Green Version]
- Ojeda, V.J.; Frost, F.; Mastaglia, F.L. Non-bacterial thrombotic endocarditis associated with malignant disease: A clinicopathological study of 16 cases. Med. J. Aust. 1985, 142, 629–631. [Google Scholar] [CrossRef]
- Okuchi, K.; Fujioka, M.; Iwanaga, H.; Koshimae, N.; Sakaki, T. Fulminant cerebral infarctions caused by nonbacterial thrombotic endocarditis due to gallbladder cancer. Acta Neurochir. 1997, 139, 995–996. [Google Scholar] [CrossRef] [PubMed]
- Olney, B.A.; Schattenberg, T.T.; Campbell, J.K.; Okazaki, H.; Lie, J. The consequences of the inconsequential: Marantic (nonbacterial thrombotic) endocarditis. Am. Heart J. 1979, 98, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Orfanelli, T.; Sultanik, E.; Shell, R.; Gibbon, D. Nonbacterial thrombotic endocarditis: A rare manifestation of gynecologic cancer. Gynecol. Oncol. Rep. 2016, 17, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oueida, Z.; Scola, M. Ovarian clear cell carcinoma presenting as non-bacterial thrombotic endocarditis and systemic embolization. World J. Oncol. 2011, 2, 270. [Google Scholar] [CrossRef] [PubMed]
- Panicucci, E.; Bruno, C.; Ferrari, V.; Suissa, L. Recurrence of ischemic stroke on direct oral anticoagulant therapy in a patient with marantic endocarditis related to lung cancer. J. Cardiol. Cases 2021, 23, 242–245. [Google Scholar] [CrossRef]
- Perrone, F.; Biagi, A.; Facchinetti, F.; Bozzetti, F.; Ramelli, A.; Vezzani, A.; Manca, T.; Gnetti, L.; Majori, M.; Alfieri, V.; et al. Systemic thromboembolism from a misdiagnosed non-bacterial thrombotic endocarditis in a patient with lung cancer: A case report. Oncol. Lett. 2020, 20, 194. [Google Scholar] [CrossRef] [PubMed]
- Piovanelli, B.; Rovetta, R.; Bonadei, I.; Vizzardi, E.; D’Aloia, A.; Metra, M. Nonbacterial thrombotic endocarditis in pancreatic cancer. Monaldi Arch. Chest Dis. 2013, 80, 189–192. [Google Scholar] [CrossRef] [Green Version]
- Polo, J.; Raufast, D.; Cornand, D.; Elias, A. Acute ischaemia of the lower limb due to non-bacterial thrombotic endocarditis with recent venous thrombo-embolic disease as the initial manifestation of lung adenocarcinoma: A case report. Eur. Heart J. Case Rep. 2021, 5, ytab426. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Escudero Ugalde, G.; Codina Prat, M.; Candina Urizar, R.; Garcia Ibarrondo, N.; Manzanal Rey, A.; Ruiz Gomez, L.; Ugedo Alzaga, K.; Castellanos Alcalde, M.; Lambarri Izaguirre, A.; Asla Ormaza, C. P691 New onset severe mitral regurgitation in oncological patient: When the disease progresses. Eur. Heart J.-Cardiovasc. Imaging 2020, 21, jez319.366. [Google Scholar] [CrossRef]
- Randhawa, G.; Aslam, A.; Suarez, M.J.; Lin, Y.S.; Kuhn-Basti, M. Non-Bacterial Thrombotic Endocarditis: A Case of Metastatic Pancreatic Cancer Masquerading as Infective Endocarditis. Cureus 2020, 12, e9103. [Google Scholar] [CrossRef]
- Royter, V.; Cohen, S.N. Recurrent embolic strokes and cardiac valvular disease in a patient with non-small cell adenocarcinoma of lung. J. Neurol. Sci. 2006, 241, 99–101. [Google Scholar] [CrossRef]
- Sakima, H.; Isa, K.; Kokuba, K.; Nakachi, K.; Ikemiyagi, H.; Shiroma, K.; Ishihara, S.; Tokashiki, T.; Yasu, T.; Ohya, Y. Recurrent embolic stroke due to nonbacterial thrombotic endocarditis followed by transesophageal echocardiography. Arch. Neurol. 2011, 68, 1604–1605. [Google Scholar] [CrossRef]
- Sánchez Quirós, B.; Ruiz López, N.; López Herrero, R.; Bartolomé Bartolomé, C. Marantic endocarditis. Rev. Esp. Anestesiol. Reanim. 2020, 67, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Enrique, C.; Vilacosta, I.; Moreno, H.G.; Delgado-Bolton, R.; Pérez-Alonso, P.; Martínez, A.; Vivas, D.; Ferrera, C.; Olmos, C. Infected marantic endocarditis with leukemoid reaction. Circ. J. 2014, 78, 2325–2327. [Google Scholar] [CrossRef] [Green Version]
- Savarapu, P.; Abdelazeem, B.; Isa, S.; Baral, N.; Hassan, M. Cancer-Related Non-Bacterial Thrombotic Endocarditis Presenting as Acute Ischemic Stroke. Cureus 2021, 13, e14953. [Google Scholar] [CrossRef] [PubMed]
- Sawai, T.; Ikezawa, M.; Hirota, A.; Yamamoto, S.; Nakajima, H.; Makino, K.; Takase, K.; Ito, M. Large Non-Bacterial Vegetation Causing Acute Aortic Regurgitation—Unexpected Finding at Autopsy. Circ. J. 2018, 82, 2378–2379. [Google Scholar] [CrossRef] [Green Version]
- Scalia, G.M.; Tandon, A.K.; Robertson, J.A. Stroke, aortic vegetations and disseminated adenocarcinoma—A case of marantic endocarditis. Heart Lung Circ. 2012, 21, 234–236. [Google Scholar] [CrossRef] [PubMed]
- Sekulic, M.; Gupta, A.; Patterson, A.; Oliveira, G.; Rajagopalan, S. Chemotherapy-associated nonbacterial thrombotic endocarditis: A radiological mimicker of cardiac amyloidosis requiring histopathologic examination for definitive diagnosis. Cardiovasc. Pathol. 2020, 47, 107210. [Google Scholar] [CrossRef]
- Shatila, W.; Rizkallah, A.; Aldin, E.S.; Tfayli, A. Nonbacterial thrombotic endocarditis as the sole manifestation of stage IV gastric cancer: A case report. J. Med. Case Rep. 2014, 8, 267. [Google Scholar] [CrossRef] [Green Version]
- Shibata, N.; Matsumoto, K.; Kitamura, S.; Sakashita, A.; Kizawa, Y.; Hirata, K.I. Nonbacterial Thrombotic Endocarditis Concomitant with Repeated Systemic Embolization That Received Palliative Care Based on the Antemortem Diagnosis. Intern. Med. 2018, 57, 3559–3563. [Google Scholar] [CrossRef] [Green Version]
- Shoji, M.K.; Kim, J.-H.; Bakshi, S.; Govea, N.; Marukian, N.; Wang, S.J. Nonbacterial thrombotic endocarditis due to primary gallbladder malignancy with recurrent stroke despite anticoagulation: Case report and literature review. J. Gen. Intern. Med. 2019, 34, 1934–1940. [Google Scholar] [CrossRef]
- Shuaib, A. Stroke from other etiologies masquerading as migraine-stroke. Stroke 1991, 22, 1068–1074. [Google Scholar] [CrossRef] [Green Version]
- Sia, C.H.; Lim, J.S.; Poh, K.K.; Chin, T.M. A classical case of non-bacterial thrombotic endocarditis from pancreatic adenocarcinoma presenting as multiple strokes, myocardial infarction and acute limb ischaemia. Oxf. Med. Case Rep. 2016, 2016, omw084. [Google Scholar] [CrossRef] [Green Version]
- Singh, V.; Bhat, I.; Havlin, K. Marantic endocarditis (NBTE) with systemic emboli and paraneoplastic cerebellar degeneration: Uncommon presentation of ovarian cancer. J. Neuro-Oncol. 2007, 83, 81–83. [Google Scholar] [CrossRef]
- Smeglin, A.; Ansari, M.; Skali, H.; Oo, T.H.; Maysky, M. Marantic endocarditis and disseminated intravascular coagulation with systemic emboli in presentation of pancreatic cancer. J. Clin. Oncol. 2008, 26, 1383–1385. [Google Scholar] [CrossRef]
- Soga, Y.; Taira, K.; Sugimoto, A.; Kurosawa, M.; Kira, H.; Su, T.; Doi, K.; Nakano, A.; Himura, Y. Mitral valve nonbacterial thrombotic endocarditis: A rare multi-surgery-tolerant survivor of Trousseau’s syndrome. Surg Case Rep. 2018, 4, 104. [Google Scholar] [CrossRef]
- Spurgeon, L.; Ispoglou, S. Non-bacterial thrombotic endocarditis in pancreatic cancer and other high-risk malignancies: The case for prophylactic treatment. Oxf. Med. Case Rep. 2021, 2021, omab110. [Google Scholar] [CrossRef]
- Starobinska, E.; Robinson, E.A.; Brucks, E.; Scott, S. Marantic endocarditis: Incidental infarcts leading to diagnosis of pancreatic cancer. Case Rep. 2018, 2018, bcr2018224529. [Google Scholar] [CrossRef]
- Studdy, P.; Willoughby, J.M. Non-bacterial thrombotic endocarditis in early cancer. Br. Med. J. 1976, 1, 752. [Google Scholar] [CrossRef] [Green Version]
- Sugawara, M.; Nakao, T.; Yatomi, Y.; Daimon, M. Development of aortic regurgitation due to non-bacterial thrombotic endocarditis. J. Med. Ultrason. 2021, 48, 363–364. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Tanaka, K.; Nogawa, S.; Umezawa, A.; Hata, J.; Fukuuchi, Y. Expression of interleukin-6 in cerebral neurons and ovarian cancer tissue in Trousseau syndrome. Clin. Neuropathol. 2002, 21, 232–235. [Google Scholar] [PubMed]
- Tai, M.L.; Tan, E.C.; Ang, C.C.; Liam, C.K. Recurrent cerebral infarcts secondary to marantic endocarditis in a patient with adenocarcinoma of the lung. Singap. Med. J. 2016, 57, 524–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeshita, S.; Ogata, T.; Mera, H.; Tsugawa, J.; Aoki, M.; Takeshita, M.; Tsuboi, Y. Multiple Thrombi in the Heart in Trousseau Syndrome Caused by Pancreatic Carcinoma. J. Stroke Cereb. Dis. 2018, 27, e75–e77. [Google Scholar] [CrossRef]
- Tamura, Y.; Sakata, K.; Terada, K.; Usui, S.; Kawashiri, M.A.; Takamura, M. Treatment with a Direct Oral Anticoagulant for Nonbacterial Thrombotic Endocarditis. Intern. Med. 2021, 60, 1881–1885. [Google Scholar] [CrossRef]
- Tiong, I.S.; Williams, M.J.; Perez, D.J. Nonbacterial thrombotic endocarditis with ST-elevation myocardial infarction treated with percutaneous coronary aspiration thrombectomy. Heart Lung Circ. 2013, 22, 386–389. [Google Scholar] [CrossRef]
- Tsai, C.C.; Wu, M.N. Frequent Ischemic Stroke as First Manifestation of Occult Colon Cancer: A Rare Case. Am. J. Case Rep. 2015, 16, 723–727. [Google Scholar] [CrossRef] [Green Version]
- Umeojiako, W.I.; Kasouridis, I.; Sargent, R.; Ghani, S. Atypical marantic endocarditis. BMJ Case Rep. 2019, 12, e232057. [Google Scholar] [CrossRef] [PubMed]
- Vaideeswar, P.; Pandit, M.J.; Deshpande, J.R.; Sivaraman, A.; Vora, I.M. Fibrolamellar carcinoma of the liver--an unusual presentation. J. Postgrad. Med. 1993, 39, 159–161. [Google Scholar]
- Van Herck, J.; Thoen, H.; Delens, C.; Voet, J. Multi-territory stroke preceded by pulmonary embolism with asymptomatic coronavirus disease 2019: A case report. Eur. Heart J. Case Rep. 2021, 5, ytab471. [Google Scholar] [CrossRef]
- Vlachostergios, P.J.; Daliani, D.D.; Dimopoulos, V.; Patrikidou, A.; Voutsadakis, I.A.; Papandreou, C.N. Nonbacterial thrombotic (marantic) endocarditis in a patient with colorectal cancer. Onkologie 2010, 33, 456–459. [Google Scholar] [CrossRef]
- Wang, J.; Monga, N.; Mopala, P.; Husnain, M. Development of nonbacterial thrombotic endocarditis while on systemic anticoagulation in pancreatic cancer: A case report. Cureus 2020, 12, e10967. [Google Scholar] [CrossRef] [PubMed]
- Washburn, E.R.; Weyant, G.W.; Yang, X.J.; Yang, Z. A rare case of prostatic ductal adenocarcinoma presenting as papillary metastatic carcinoma of unknown primary: A case report and review of the literature. Hum. Pathol. Case Rep. 2016, 6, 26–31. [Google Scholar] [CrossRef] [Green Version]
- Wigger, O.; Windecker, S.; Bloechlinger, S. Nonbacterial thrombotic endocarditis presenting as intracerebral hemorrhage. Wien. Klin. Wochenschr. 2016, 128, 922–924. [Google Scholar] [CrossRef]
- Wild, J.; Distelmeier, S.; Keil, P.; Weinmann, A.; Münzel, T.; Weinmann-Menke, J.; Kraus, D. Non-bacterial thrombotic endocarditis in a patient with pancreatic carcinoma. Echocardiography 2021, 38, 1455–1458. [Google Scholar] [CrossRef]
- Wong, S.F.; Seow, J.; Profitis, K.; Johns, J.; Barnett, S.; John, T. Marantic endocarditis presenting with multifocal neurological symptoms. Intern. Med. J. 2013, 43, 211–214. [Google Scholar] [CrossRef]
- Woo, P.; Chan, D.; Cheung, T.; Zhu, X.; Poon, W. Middle cerebral artery infarction in a cancer patient: A fatal case of Trousseau’s syndrome. Hong Kong Med. J. 2014, 20, 74–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagi, T.; Takahashi, K.; Tanikawa, M.; Seki, M.; Abe, T.; Suzuki, N. Fatal intracranial hemorrhage after intravenous thrombolytic therapy for acute ischemic stroke associated with cancer-related nonbacterial thrombotic endocarditis. J. Stroke Cereb. Dis. 2014, 23, e413–e416. [Google Scholar] [CrossRef] [PubMed]
- Yamane, A.; Sadahiro, H.; Goto, H.; Inamura, A.; Ishihara, H.; Oka, F.; Oku, T.; Kondo, T.; Suzuki, M. Multiple ischemic strokes caused by nonbacterial thrombotic endocarditis because of gallbladder cancer: A case report. J. Stroke Cereb. Dis. 2014, 23, 1727–1729. [Google Scholar] [CrossRef]
- Yasutake, H.; Sugano, Y.; Ikeda, Y.; Ohara, T.; Hasegawa, T.; Kanzaki, H.; Anzai, T. First Case Report of the Antemortem Diagnosis of Nonbacterial Thrombotic Endocarditis of a Mechanical Prosthetic Valve. Intern. Med. 2016, 55, 255–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshii, Y.; Numata, T.; Ishitobi, W.; Takahashi, N.; Wakui, H.; Kojima, J.; Shimizu, K.; Hara, H.; Ishikawa, T.; Kawaishi, M.; et al. Lung adenocarcinoma complicated by Trousseau’s syndrome successfully treated by a combination of anticoagulant therapy and chemotherapy. Intern. Med. 2014, 53, 1835–1839. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Yee, Y.; Qin, Y. Non-bacterial thrombotic endocarditis and metastatic lung adenocarcinoma. BMJ Case Rep. 2021, 14, e242948. [Google Scholar] [CrossRef]
- Schlittler, L.A.; Dallagasperina, V.W.; Schavinski, C.; Baggio, A.P.; Lazaretti, N.S.; Villaroel, R.U. Marantic endocarditis and adenocarcinoma of unknown primary site. Arq. Bras. De Cardiol. 2011, 96, e73–e75. [Google Scholar]
- Glancy, D.L.; Roberts, W.C. The heart in malignant melanoma: A study of 70 autopsy cases. Am. J. Cardiol. 1968, 21, 555–571. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.L.; Naguwa, S.M.; Cheema, G.S.; Gershwin, M.E. Revisiting Libman–Sacks endocarditis: A historical review and update. Clin. Rev. Allergy Immunol. 2009, 36, 126–130. [Google Scholar] [CrossRef]
- Eiken, P.W.; Edwards, W.D.; Tazelaar, H.D.; McBane, R.D.; Zehr, K.J. Surgical pathology of nonbacterial thrombotic endocarditis in 30 patients, 1985–2000. Mayo Clin. Proc. 2001, 76, 1204–1212. [Google Scholar] [CrossRef]
- Caine, G.J.; Stonelake, P.S.; Lip, G.Y.; Kehoe, S.T. The hypercoagulable state of malignancy: Pathogenesis and current debate. Neoplasia 2002, 4, 465–473. [Google Scholar] [CrossRef]
- Rosen, P.; Armstrong, D. Nonbacterial thrombotic endocarditis in patients with malignant neoplastic diseases. Am. J. Med. 1973, 54, 23–29. [Google Scholar] [CrossRef]
- Bryan, C.S. Nonbacterial thrombotic endocarditis with malignant tumors. Am. J. Med. 1969, 46, 787–793. [Google Scholar] [CrossRef]
- MACDONALD, R.A.; ROBBINS, S.L. The significance of nonbacterial thrombotic endocarditis: An autopsy and clinical study of 78 cases. Ann. Intern. Med. 1957, 46, 255–273. [Google Scholar]
- Rohner, R.F.; Prior, J.T.; Sipple, J.H. Mucinous malignancies, venous thrombosis and terminal endocarditis with emboli: A syndrome. Cancer 1966, 19, 1805–1812. [Google Scholar] [CrossRef]
- Eliakim, M.; Pinchas, S. Degenerative verrucous endocardiosis. A clinical-pathological study of 45 cases with reference to a protracted form of the disease. Isr. J. Med. Sci. 1966, 2, 42–51. [Google Scholar] [PubMed]
- Mügge, A.; Daniel, W.G.; Frank, G.; Lichtlen, P.R. Echocardiography in infective endocarditis: Reassessment of prognostic implications of vegetation size determined by the transthoracic and the transesophageal approach. J. Am. Coll. Cardiol. 1989, 14, 631–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sack, G.H., Jr.; Levin, J.; Bell, W.R. Trousseau’s syndrome and other manifestations of chronic disseminated coagulopathy in patients with neoplasms: Clinical, pathophysiologic, and therapeutic features. Medicine 1977, 56, 1–37. [Google Scholar] [CrossRef] [PubMed]
- Rogers, L.R.; Cho, E.-s.; Kempin, S.; Posner, J.B. Cerebral infarction from non-bacterial thrombotic endocarditis: Clinical and pathological study including the effects of anticoagulation. Am. J. Med. 1987, 83, 746–756. [Google Scholar] [CrossRef] [PubMed]
- Mosesson, M.W.; Colman, R.W.; Sherry, S. Chronic intravascular coagulation syndrome: Report of a case with special studies of an associated plasma cryoprecipitate (cryofibrinogen). N. Engl. J. Med. 1968, 278, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Owen, C.A.; Bowie, E.W. Chronic intravascular coagulation and fibrinolysis (ICF) syndromes (DIC). Semin. Thromb. Hemost. 1977, 3, 268–290. [Google Scholar] [CrossRef]
- Quintero-Martinez, J.A.; Hindy, J.-R.; El Zein, S.; Michelena, H.I.; Nkomo, V.T.; DeSimone, D.C.; Baddour, L.M. Contemporary demographics, diagnostics and outcomes in non-bacterial thrombotic endocarditis. Heart 2022, 108. [Google Scholar] [CrossRef]
- Marin, G.; Margineanu, C.; Penes, D.; Maresiu, C.; Boiangiu, S.; Stoica, E.; Radu, R.; Antohi, E.; Chioncel, O. P1243 Nonbacterial thrombotic endocarditis (NBTE) of the aortic valve: Incidental finding in hospitalized patients with advanced heart failure. Eur. Heart J.-Cardiovasc. Imaging 2020, 21, jez319.697. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Level | Overall | |
|---|---|---|
| n | 144 | |
| Antiphospholipid antibodies (%) | No | 141 (97.9) |
| Yes | 3 (2.1) | |
| Primary cancer organ (%) | Gynecological | 23 (16.0) |
| Lung | 41 (28.5) | |
| Other GIT cancers | 19 (13.2) | |
| Others | 33 (22.9) | |
| Pancreas | 28 (19.4) | |
| Lung vs. other cancers (%) | Others | 103 (71.5) |
| Lung cancer | 41 (28.5) | |
| Pathology (%) | Adenocarcinoma | 93 (64.6) |
| Hematopoietic | 6 (4.2) | |
| Others | 38 (26.4) | |
| Sarcoma | 1 (0.7) | |
| SCC | 6 (4.2) | |
| Adenocarcinoma vs. other pathologies (%) | Other pathologies | 51 (35.4) |
| Adenocarcinoma | 93 (64.6) | |
| Organ of metastasis (n = 97) (%) | Bone | 5 (5.2) |
| Brain | 3 (3.1) | |
| Liver | 23 (23.7) | |
| Lung | 7 (7.2) | |
| Lymph nodes | 22 (22.7) | |
| Multiple | 25 (25.8) | |
| Others | 12 (12.4) | |
| Metastasis (n = 141) (%) | Non-metastatic | 43 (30.7) |
| Metastatic | 97 (69.3) | |
| Marantic presentation before diagnosis of cancer (n = 125) (%) | Known cancer case | 42 (33.6) |
| Marantic as first presentation | 83 (66.4) | |
| Interval diagnosis (months) (mean (SD) | 6.24 (25.51) | |
| Age (median (IQR)) | 60.00 (49.75, 66.00) | |
| Sex (%) | Females | 81 (56.25) |
| Males | 63 (43.75) | |
| COPD (n = 52) (%) | No | 49 (94.2) |
| Yes | 3 (5.8) | |
| Smoking (n = 56) (%) | No | 43 (76.8) |
| Yes | 13 (23.2) | |
| Diabetes (n = 52) (%) | No | 43 (82.7) |
| Yes | 9 (17.3) | |
| Obesity (n = 53) (%) | No | 52 (98.1) |
| Yes | 1 (1.9) | |
| Dyslipidemia (n = 54) (%) | No | 46 (85.2) |
| Yes | 8 (14.8) | |
| Hypertension (n = 56) (%) | No | 36 (64.3) |
| Yes | 20 (35.7) | |
| Embolization event at presentation (n = 132) (%) | No | 15 (11.4) |
| Yes | 117 (88.6) | |
| Embolic event after diagnosis (n = 125) (%) | No | 76 (60.8) |
| Yes | 49 (39.2) | |
| Incidental finding of NBTE (%) | No | 132 (91.7) |
| Yes | 12 (8.3) | |
| Postmortem diagnosis of NBTE (%) | No | 95 (66.0) |
| Yes | 49 (34.0) | |
| Position of vegetation (n = 132) (%) | Aortic | 48 (36.4) |
| Left atrium | 1 (0.8) | |
| Mitral | 62 (47.0) | |
| Multiple | 21 (15.9) | |
| Valve insufficiency (n = 89) (%) | No | 28 (31.5) |
| Yes | 61 (68.5) | |
| Valve stenosis (n = 90) (%) | No | 81 (90.0) |
| Yes | 9 (10.0) | |
| Underwent intervention (%) | No | 123 (85.4) |
| Yes | 21 (14.6) | |
| Type of surgery (%) | Excision of vegetation | 5 (3.5) |
| None | 123 (85.4) | |
| Replacement | 16 (11.1) | |
| Presenting symptoms (n = 139) (%) | Cardiological | 6 (4.5) |
| Neurological | 96 (72.7) | |
| Others | 7 (5.3) | |
| Respiratory | 13 (9.8) | |
| Vascular | 10 (7.6) | |
| Death (%) | No | 47 (32.6) |
| Yes | 97 (67.4) | |
| Time to death (days) (median (IQR)) | 15.40 (2.73, 56.00) |
| Level | Non-Lung Cancers | Lung Cancer | p | |
|---|---|---|---|---|
| n | 103 | 41 | ||
| Antiphospholipid antibodies (%) | No | 100 (97.1) | 41 (100.0) | 0.647 |
| Yes | 3 (2.9) | 0 (0.0) | ||
| Primary cancer organ (%) | Gynecological | 23 (22.3) | 0 (0.0) | <0.001 |
| Lung | 0 (0.0) | 41 (100.0) | ||
| Other GIT cancers | 19 (18.4) | 0 (0.0) | ||
| Others | 33 (32.0) | 0 (0.0) | ||
| Pancreas | 28 (27.2) | 0 (0.0) | ||
| Pathology (%) | Adenocarcinoma | 60 (58.3) | 33 (80.5) | 0.004 |
| Hematopoietic | 6 (5.8) | 0 (0.0) | ||
| Others | 34 (33.0) | 4 (9.8) | ||
| Sarcoma | 1 (1.0) | 0 (0.0) | ||
| SCC | 2 (1.9) | 4 (9.8) | ||
| Adenocarcinoma vs. other pathologies (%) | Other pathologies | 43 (41.7) | 8 (19.5) | 0.02 |
| Adenocarcinoma | 60 (58.3) | 33 (80.5) | ||
| Organ of metastasis (n = 97) (%) | Bone | 3 (4.8) | 2 (5.9) | 0.258 |
| Brain | 2 (3.2) | 1 (2.9) | ||
| Liver | 20 (31.7) | 3 (8.8) | ||
| Lung | 5 (7.9) | 2 (5.9) | ||
| Lymph nodes | 11 (17.5) | 11 (32.4) | ||
| Multiple | 15 (23.8) | 10 (29.4) | ||
| Others | 7 (11.1) | 5 (14.7) | ||
| Metastasis (n = 141) (%) | Non-metastatic | 38 (37.6) | 5 (12.8) | 0.008 |
| Metastatic | 63 (62.4) | 34 (87.2) | ||
| Marantic presentation before diagnosis of cancer (n = 125) (%) | Known cancer case | 34 (36.2) | 8 (25.8) | 0.401 |
| Marantic as a first presentation | 60 (63.8) | 23 (74.2) | ||
| Interval diagnosis (months) (mean (SD)) | 7.95 (29.56) | 1.54 (3.81) | 0.257 | |
| Age (median (IQR)) | 59.00 (49.00, 65.00) | 61.00 (55.00, 67.00) | 0.389 | |
| Sex (%) | F | 63 (61.2) | 18 (45.0) | 0.118 |
| M | 40 (38.8) | 22 (55.0) | ||
| COPD (n = 52) (%) | No | 39 (97.5) | 10 (83.3) | 0.254 |
| Yes | 1 (2.5) | 2 (16.7) | ||
| Smoke (n = 56) (%) | No | 37 (92.5) | 6 (37.5) | <0.001 |
| Yes | 3 (7.5) | 10 (62.5) | ||
| Diabetes (n = 52) (%) | No | 31 (77.5) | 12 (100.0) | 0.17 |
| Yes | 9 (22.5) | 0 (0.0) | ||
| Obesity (n = 53) (%) | No | 40 (97.6) | 12 (100.0) | 1 |
| Yes | 1 (2.4) | 0 (0.0) | ||
| Dyslipidemia (n = 54) (%) | No | 35 (85.4) | 11 (84.6) | 1 |
| Yes | 6 (14.6) | 2 (15.4) | ||
| Hypertension (n = 56) (%) | No | 27 (64.3) | 9 (64.3) | 1 |
| Yes | 15 (35.7) | 5 (35.7) | ||
| Embolization event at presentation (n = 132) (%) | No | 12 (12.4) | 3 (8.6) | 0.767 |
| Yes | 85 (87.6) | 32 (91.4) | ||
| Embolic event after diagnosis (n = 125) (%) | No | 55 (59.1) | 21 (65.6) | 0.661 |
| Yes | 38 (40.9) | 11 (34.4) | ||
| Incidental finding of NBTE (%) | No | 95 (92.2) | 37 (90.2) | 0.956 |
| Yes | 8 (7.8) | 4 (9.8) | ||
| Postmortem diagnosis of NBTE (%) | No | 74 (71.8) | 21 (51.2) | 0.031 |
| Yes | 29 (28.2) | 20 (48.8) | ||
| Position of vegetation (n = 132) (%) | Aortic | 29 (31.2) | 19 (48.7) | 0.008 |
| Left atrium | 1 (1.1) | 0 (0.0) | ||
| Mitral | 42 (45.2) | 20 (51.3) | ||
| Multiple | 21 (22.6) | 0 (0.0) | ||
| Valve insufficiency (n = 89) (%) | No | 23 (35.4) | 5 (20.8) | 0.292 |
| yes | 42 (64.6) | 19 (79.2) | ||
| Valve stenosis (n = 90) (%) | No | 57 (86.4) | 24 (100.0) | 0.131 |
| Yes | 9 (13.6) | 0 (0.0) | ||
| Underwent intervention (%) | No | 84 (81.6) | 39 (95.1) | 0.069 |
| Yes | 19 (18.4) | 2 (4.9) | ||
| Type of surgery (%) | Excision of vegetation | 4 (3.9) | 1 (2.4) | 0.096 |
| None | 84 (81.6) | 39 (95.1) | ||
| Replacement | 15 (14.6) | 1 (2.4) | ||
| Presenting symptoms (n = 139) (%) | Cardiological | 4 (4.2) | 2 (5.6) | 0.467 |
| Neurological | 68 (70.8) | 28 (77.8) | ||
| Others | 4 (4.2) | 3 (8.3) | ||
| Respiratory | 11 (11.5) | 2 (5.6) | ||
| Vascular | 9 (9.4) | 1 (2.8) | ||
| Death (144) (%) | No | 37 (36.3) | 8 (20.0) | 0.094 |
| Yes | 65 (63.7) | 32 (80.0) | ||
| Time to death (days) (median (IQR)) | 19.60 (1.05, 56.00) | 10.99 (3.50, 35.28) | 0.64 |
| Variables | Hazard Ratio, 95% CI, p Value |
|---|---|
| Age | 1.021 [0.999; 1.043], 0.06157 |
| Year | 0.975 [0.959; 0.991], 0.00289 |
| Underwent intervention | 1.235 [0.472; 3.229], 0.66705 |
| Pathology (adenocarcinoma vs. others) | 0.994 [0.560; 1.764], 0.98430 |
| Cancer organ (ref: lung) | |
| 0.928 [0.477; 1.806], 0.82582 |
| 0.555 [0.210; 1.463], 0.23369 |
| 0.578 [0.180; 1.855], 0.35703 |
| 0.724 [0.338; 1.548], 0.40459 |
| Organ affected by metastasis (liver vs. others) | 1.235 [0.644; 2.368], 0.52555 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahouma, M.; Khairallah, S.; Dabsha, A.; Elkharbotly, I.A.M.H.; Baudo, M.; Ismail, A.; Korani, O.M.; Hossny, M.; Dimagli, A.; Girardi, L.N.; et al. Lung Cancer as a Leading Cause among Paraneoplastic Non-Bacterial Thrombotic Endocarditis: A Meta-Analysis of Individual Patients’ Data. Cancers 2023, 15, 1848. https://doi.org/10.3390/cancers15061848
Rahouma M, Khairallah S, Dabsha A, Elkharbotly IAMH, Baudo M, Ismail A, Korani OM, Hossny M, Dimagli A, Girardi LN, et al. Lung Cancer as a Leading Cause among Paraneoplastic Non-Bacterial Thrombotic Endocarditis: A Meta-Analysis of Individual Patients’ Data. Cancers. 2023; 15(6):1848. https://doi.org/10.3390/cancers15061848
Chicago/Turabian StyleRahouma, Mohamed, Sherif Khairallah, Anas Dabsha, Ismail A. M. H. Elkharbotly, Massimo Baudo, Amr Ismail, Omnia M. Korani, Mohamed Hossny, Arnaldo Dimagli, Leonard N. Girardi, and et al. 2023. "Lung Cancer as a Leading Cause among Paraneoplastic Non-Bacterial Thrombotic Endocarditis: A Meta-Analysis of Individual Patients’ Data" Cancers 15, no. 6: 1848. https://doi.org/10.3390/cancers15061848