
Real-World Impact of SABR on Stage I Non-Small-Cell Lung Cancer Outcomes at a Scottish Cancer Centre

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer Research UK. Lung Cancer Statistics. 2021. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/lung-cancer (accessed on 12 December 2022).
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Public Health Scotland. Cancer Statistics: Lung Cancer and Mesothelioma. Available online: https://www.opendata.nhs.scot/dataset/annual-cancer-incidence (accessed on 12 December 2022).
- Loganathan, R.S.; Stover, D.E.; Shi, W.; Venkatraman, E. Prevalence of COPD in Women Compared to Men Around the Time of Diagnosis of Primary Lung Cancer. Chest 2006, 129, 1305–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henson, L.A.; Chukwusa, E.; Ling, C.N.Y.; Khan, S.A.; Gao, W. Lung cancer deaths (England 2001–2017)—Comorbidities: A national population-based analysis. BMJ Support. Palliat. Care 2021. [Google Scholar] [CrossRef] [PubMed]
- Rowell, N.P.; Williams, C.J. Radical radiotherapy for stage I/II non-small cell lung cancer in patients not sufficiently fit for or declining surgery (medically inoperable): A systematic review. Thorax 2001, 56, 628–638. [Google Scholar] [CrossRef] [PubMed]
- Wisnivesky, J.P.; Halm, E.; Bonomi, M.; Powell, C.; Bagiella, E. Effectiveness of Radiation Therapy for Elderly Patients with Unresected Stage I and II Non–Small Cell Lung Cancer. Am. J. Respir. Crit. Care Med. 2010, 181, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S.; ESMO Guidelines Committee. Early and Locally Advanced Non-Small-Cell Lung Cancer (NSCLC): ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-up. Ann. Oncol. 2017, 28 (Suppl. 4), iv1–iv21. [Google Scholar] [CrossRef] [PubMed]
- Fakiris, A.J.; McGarry, R.C.; Yiannoutsos, C.T.; Papiez, L.; Williams, M.; Henderson, M.A.; Timmerman, R. Stereotactic Body Radiation Therapy for Early-Stage Non–Small-Cell Lung Carcinoma: Four-Year Results of a Prospective Phase II Study. Int. J. Radiat. Oncol. 2009, 75, 677–682. [Google Scholar] [CrossRef]
- Palma, D.; Lagerwaard, F.; Rodrigues, G.; Haasbeek, C.; Senan, S. Curative Treatment of Stage I Non-Small-Cell Lung Cancer in Patients with Severe COPD: Stereotactic Radiotherapy Outcomes and Systematic Review. Int. J. Radiat. Oncol. 2012, 82, 1149–1156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagerwaard, F.J.; Haasbeek, C.J.A.; Smit, E.F.; Slotman, B.J.; Senan, S. Outcomes of Risk-Adapted Fractionated Stereotactic Radiotherapy for Stage I Non–Small-Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Nanda, R.H.; Liu, Y.; Gillespie, T.W.; Mikell, J.L.; Ramalingam, S.S.; Fernandez, F.G.; Curran, W.J.; Lipscomb, J.; Higgins, K.A. Stereotactic body radiation therapy versus no treatment for early stage non-small cell lung cancer in medically inoperable elderly patients: A National Cancer Data Base analysis. Cancer 2015, 121, 4222–4230. [Google Scholar] [CrossRef]
- Ball, D.; Mai, G.T.; Vinod, S.; Babington, S.; Ruben, J.; Kron, T.; Chesson, B.; Herschtal, A.; Vanevski, M.; Rezo, A.; et al. Stereotactic ablative radiotherapy versus standard radiotherapy in stage 1 non-small-cell lung cancer (TROG 09.02 CHISEL): A phase 3, open-label, randomised controlled trial. Lancet Oncol. 2019, 20, 494–503. [Google Scholar] [CrossRef]
- Phillips, I.; Sandhu, S.; Lüchtenborg, M.; Harden, S.V. Stereotactic Ablative Body Radiotherapy Versus Radical Radiotherapy: Comparing Real-World Outcomes in Stage I Lung Cancer. Clin. Oncol. 2019, 31, 681–687. [Google Scholar] [CrossRef]
- Haque, W.; Verma, V.; Polamraju, P.; Farach, A.; Butler, E.B.; Teh, B.S. Stereotactic body radiation therapy versus conventionally fractionated radiation therapy for early stage non-small cell lung cancer. Radiother. Oncol. 2018, 129, 264–269. [Google Scholar] [CrossRef]
- Nyman, J.; Hallqvist, A.; Lund, J.Å.; Brustugun, O.T.; Bergman, B.; Bergström, P.; Friesland, S.; Lewensohn, R.; Holmberg, E.; Lax, I. SPACE—A randomized study of SBRT vs conventional fractionated radiotherapy in medically inoperable stage I NSCLC. Radiother. Oncol. 2016, 121, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Franks, K.N.; McParland, L.; Webster, J.; Baldwin, D.R.; Sebag-Montefiore, D.; Evison, M.; Booton, R.; Faivre-Finn, C.; Naidu, B.; Ferguson, J.; et al. SABRTooth: A randomised controlled feasibility study of stereotactic ablative radiotherapy (SABR) with surgery in patients with peripheral stage I nonsmall cell lung cancer considered to be at higher risk of complications from surgical resection. Eur. Respir. J. 2020, 56, 2000118. [Google Scholar] [CrossRef]
- Chang, J.Y.; Senan, S.; Paul, M.A.; Mehran, R.J.; Louie, A.V.; Balter, P.; Groen, H.J.M.; McRae, S.E.; Widder, J.; Feng, L.; et al. Stereotactic ablative radiotherapy versus lobectomy for operable stage I non-small-cell lung cancer: A pooled analysis of two randomised trials. Lancet Oncol. 2015, 16, 630–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NICE. National Institute for Health and Care Excellence. Lung Cancer: Diagnosis and Management. 2019. Available online: https://www.nice.org.uk/guidance/NG122 (accessed on 12 December 2022).
- Vansteenkiste, J.; Crinò, L.; Dooms, C.; Douillard, J.Y.; Faivre-Finn, C.; Lim, E.; Rocco, G.; Senan, S.; Van Schil, P.; Veronesi, G.; et al. 2nd ESMO Consensus Conference on Lung Cancer: Early-stage non-small-cell lung cancer consensus on diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25, 1462–1474. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.Y.; Mehran, R.J.; Feng, L.; Verma, V.; Liao, Z.; Welsh, J.W.; Lin, S.H.; O’Reilly, M.S.; Jeter, M.D.; Balter, P.A.; et al. Stereotactic ablative radiotherapy for operable stage I non-small-cell lung cancer (revised STARS): Long-term results of a single-arm, prospective trial with prespecified comparison to surgery. Lancet Oncol. 2021, 22, 1448–1457. [Google Scholar] [CrossRef] [PubMed]
- Brooks, E.D.; Sun, B.; Zhao, L.; Komaki, R.; Liao, Z.; Jeter, M.; Welsh, J.W.; O’Reilly, M.S.; Gomez, D.R.; Hahn, S.M.; et al. Stereotactic Ablative Radiation Therapy is Highly Safe and Effective for Elderly Patients with Early-stage Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. 2017, 98, 900–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palma, D.; Visser, O.; Lagerwaard, F.J.; Belderbos, J.; Slotman, B.; Senan, S. Treatment of stage I NSCLC in elderly patients: A population-based matched-pair comparison of stereotactic radiotherapy versus surgery. Radiother. Oncol. 2011, 101, 240–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palma, D.; Visser, O.; Lagerwaard, F.J.; Belderbos, J.; Slotman, B.J.; Senan, S. Impact of Introducing Stereotactic Lung Radiotherapy for Elderly Patients with Stage I Non–Small-Cell Lung Cancer: A Population-Based Time-Trend Analysis. J. Clin. Oncol. 2010, 28, 5153–5159. [Google Scholar] [CrossRef] [PubMed]
- South East Scotland Cancer Network: SCAN—Tumour Specifjc Groups—Lung. Available online: https://www.scan.scot.nhs.uk/tumour-specific-groups/lung/ (accessed on 12 December 2022).
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and Validating the Charlson Comorbidity Index and Score for Risk Adjustment in Hospital Discharge Abstracts Using Data from 6 Countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Public Health Scotland. Scottish Morbidity Records (SMR) Datasets. Available online: https://www.ndc.scot.nhs.uk/Data-Dictionary/SMR-Datasets/Episode-Management/SMR-Record-Type/ (accessed on 12 December 2022).
- Damhuis, R.A.; Senan, S.; Khakwani, A.; Harden, S.; Helland, S.; Strand, T.-E. Age-related treatment patterns for stage I NSCLC in three European countries. J. Geriatr. Oncol. 2021, 12, 1214–1219. [Google Scholar] [CrossRef] [PubMed]
- Haasbeek, C.J.A.; Palma, D.; Visser, O.; Lagerwaard, F.J.; Slotman, B.; Senan, S. Early-stage lung cancer in elderly patients: A population-based study of changes in treatment patterns and survival in the Netherlands. Ann. Oncol. 2012, 23, 2743–2747. [Google Scholar] [CrossRef] [PubMed]
- Haasbeek, C.J.A.; Lagerwaard, F.J.; Antonisse, M.E.; Slotman, B.J.; Senan, S. Stage I nonsmall cell lung cancer in patients aged > or = 75 years: Outcomes after stereotactic radiotherapy. Cancer 2010, 116, 406–414. [Google Scholar] [CrossRef]
- Feinstein, A.R.; Sosin, D.M.; Wells, C.K. The Will Rogers phenomenon. Stage migration and new diagnostic techniques as a source of misleading statistics for survival in cancer. N. Engl. J. Med. 1985, 312, 1604–1608. [Google Scholar] [CrossRef]
- Louie, A.V.; Tjong, M.C.; Siva, S. Surgery versus SABR for early-stage lung cancer-time to call it a draw? Lancet Oncol. 2021, 22, 1355–1357. [Google Scholar] [CrossRef]
- Kidane, B.; Spicer, J.; Kim, J.O.; Fiset, P.-O.; Abdulkarim, B.; Malthaner, R.; Palma, D. SABR-BRIDGE: Stereotactic Ablative Radiotherapy before Resection to Avoid Delay for Early-Stage Lung Cancer or Oligomets during the COVID-19 Pandemic. Front. Oncol. 2020, 10, 580189. [Google Scholar] [CrossRef]
- Chen, H.; Laba, J.M.; Boldt, R.G.; Goodman, C.D.; Palma, D.A.; Senan, S.; Louie, A.V. Stereotactic Ablative Radiation Therapy Versus Surgery in Early Lung Cancer: A Meta-analysis of Propensity Score Studies. Int. J. Radiat. Oncol. 2018, 101, 186–194. [Google Scholar] [CrossRef]
- de Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A.; Lammers, J.W.J.; Weenink, C.; Yousaf-Khan, U.; Horeweg, N.; et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | All | No Radical Treatment | Radical Radiotherapy | Stereotactic Ablative Body Radiotherapy | Surgery | |
|---|---|---|---|---|---|---|
| n = 1143 | n = 361 | n = 182 | n = 132 | n = 468 | ||
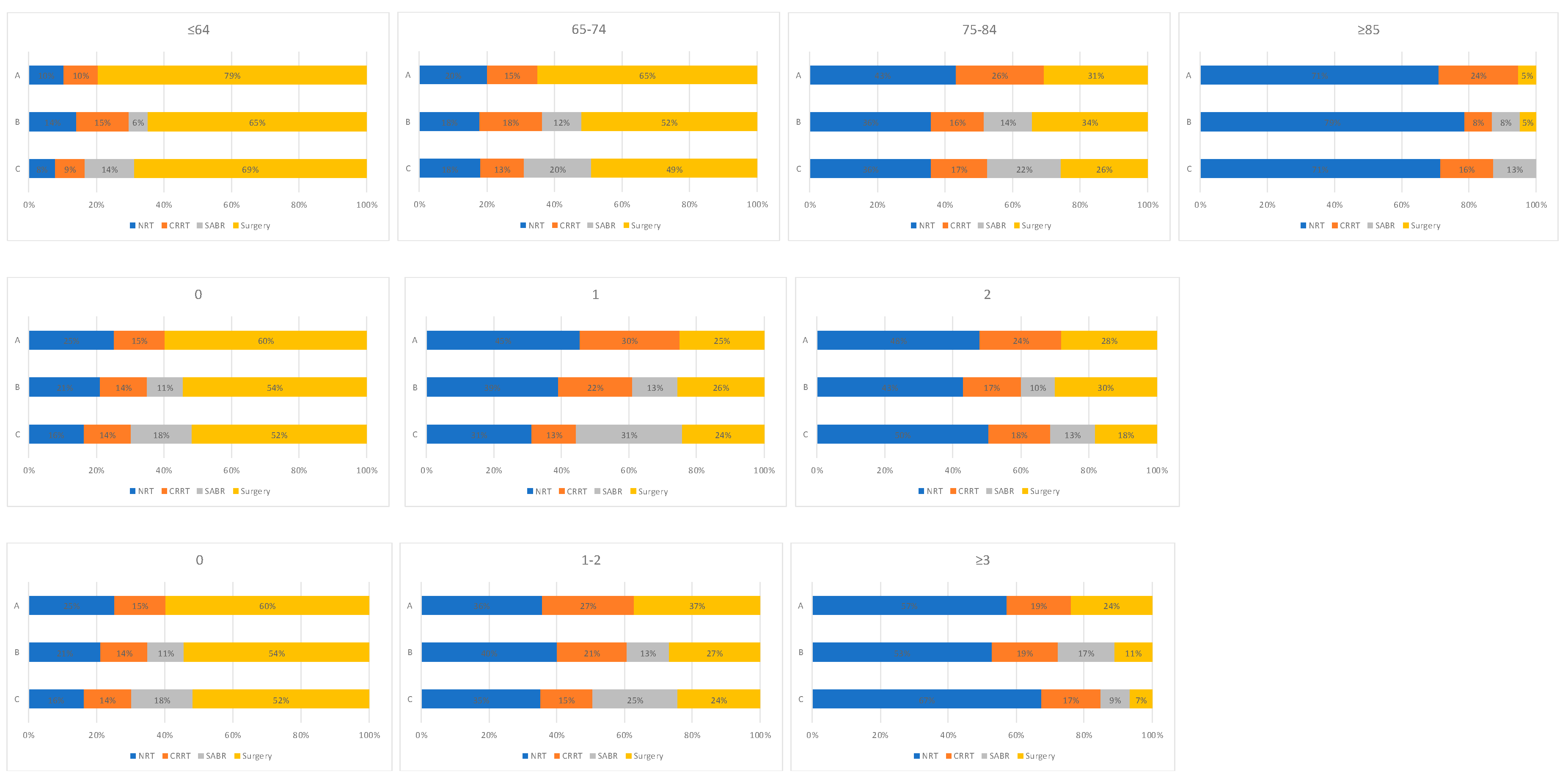
| Age | ≤64 | 200 (17) | 21 (6) | 23 (13) | 17 (13) | 139 (30) |
| 65–74 | 372 (33) | 66 (18) | 60 (33) | 44 (33) | 202 (43) | |
| 75–84 | 411 (36) | 154 (43) | 75 (41) | 58 (44) | 124 (26) | |
| ≥85 | 160 (14) | 120 (33) | 24 (13) | 13 (10) | 3 (1) | |
| Median (IQR) | 74 (68–81) | 82 (75–87) | 76 (70–81) | 75 (69–81) | 70 (63–75) | |
| Sex | Female | 628 (55) | 200 (55) | 95 (52) | 75 (57) | 258 (55) |
| Male | 515 (45) | 161 (45) | 87 (48) | 57 (43) | 210 (45) | |
| ECOG Performance Status | 0 | 244 (21) | 51 (14) | 21 (12) | 22 (17) | 150 (32) |
| 1 | 435 (38) | 87 (24) | 95 (52) | 61 (46) | 192 (41) | |
| 2 | 225 (20) | 66 (18) | 54 (30) | 42 (32) | 63 (14) | |
| 3+ | 76 (7) | 76 (21) | 0 (0) | 0 (0) | 0 (0) | |
| Unknown | 163 (14) | 81 (22) | 12 (7) | 7 (5) | 63 (14) | |
| Charlson Comorbidity Index | 0 | 564 (49) | 113 (31) | 80 (44) | 64 (48) | 307 (66) |
| 1–2 | 301 (26) | 114 (32) | 60 (33) | 44 (33) | 83 (18) | |
| ≥3 | 103 (9) | 62 (17) | 19 (10) | 10 (8) | 12 (3) | |
| Unknown | 175 (15) | 72 (20) | 23 (13) | 14 (11) | 66 (14) | |
| Pathological Confirmation | Yes | 660 (58) | 85 (23) | 86 (47) | 21 (16) | 468 (100) |
| No | 483 (42) | 276 (77) | 96 (53) | 111 (84) | 0 (0) | |
| T-stage | IA | 783 (69) | 247 (68) | 99 (54) | 112 (85) | 325 (69) |
| IB | 360 (31) | 114 (32) | 83 (46) | 20 (15) | 143 (31) | |
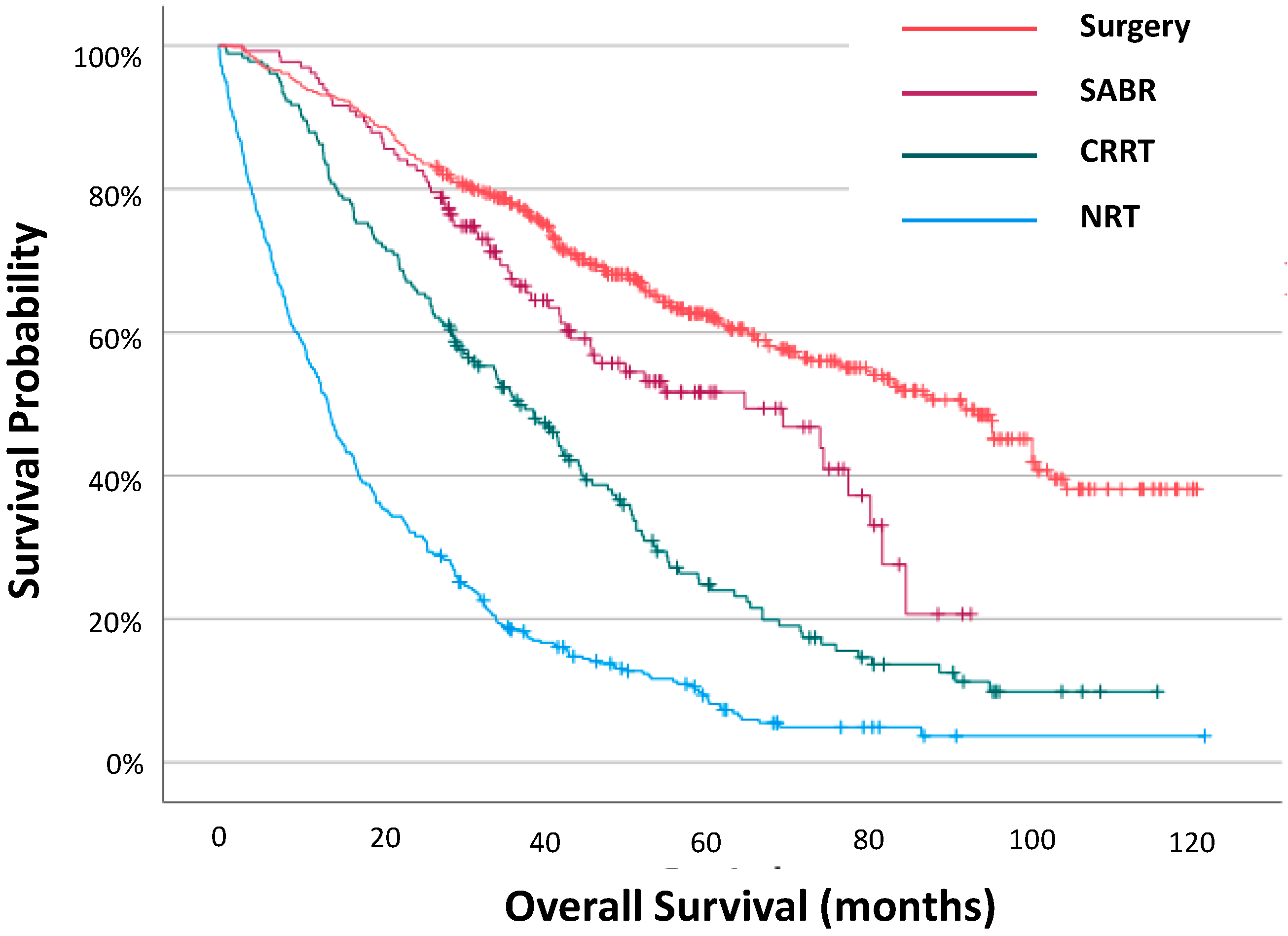
| Overall survival | Median (IQR) | 41.6 (15.4–95.8) | 13.5 (5.3–30.3) | 37.1 (18.5–59.6) | 65.3 (29.1–85.3) | 92.3 (40.6-NR) |
| 2-year survival | n (%) | 744 (65) | 116 (32) | 121 (66) | 110 (83) | 397 (85) |
| Censored | n (%) | 407 (36) | 30 (8) | 40 (22) | 69 (52) | 268 (57) |
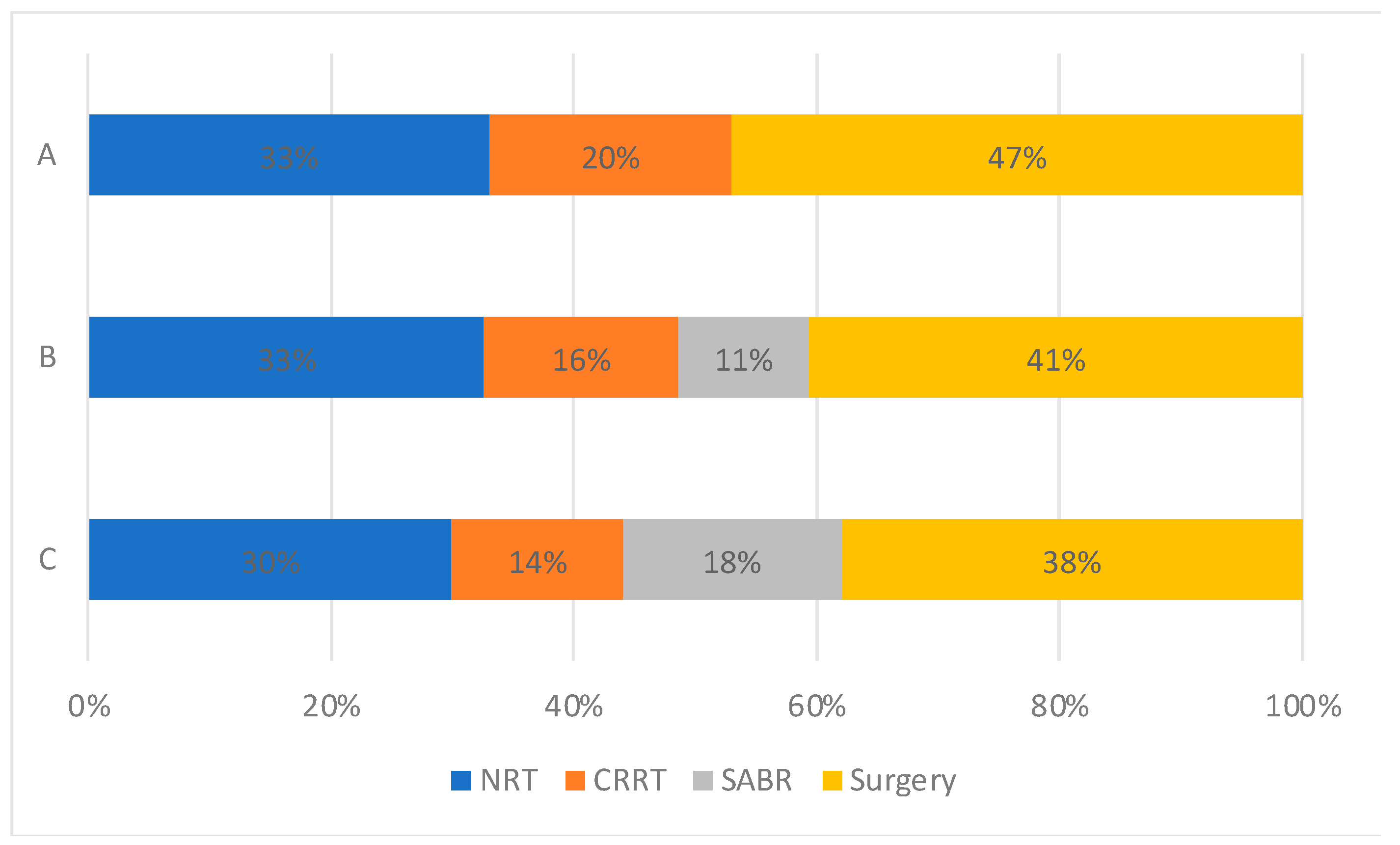
| Period of Diagnosis | A (2012–2013) | 252 (22) | 83 (23) | 51 (28) | 0 (0) | 118 (25) |
| B (2014–2016) | 443 (39) | 144 (40) | 69 (38) | 50 (38) | 180 (39) | |
| C (2017–2019) | 448 (39) | 134 (37) | 62 (34) | 82 (62) | 170 (36) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stares, M.; Lewis, G.; Vallet, M.; Killean, A.; Tramonti, G.; Patrizio, A.; Mackean, M.; Harrow, S.; Barrie, C.; MacLennan, K.; et al. Real-World Impact of SABR on Stage I Non-Small-Cell Lung Cancer Outcomes at a Scottish Cancer Centre. Cancers 2023, 15, 1431. https://doi.org/10.3390/cancers15051431
Stares M, Lewis G, Vallet M, Killean A, Tramonti G, Patrizio A, Mackean M, Harrow S, Barrie C, MacLennan K, et al. Real-World Impact of SABR on Stage I Non-Small-Cell Lung Cancer Outcomes at a Scottish Cancer Centre. Cancers. 2023; 15(5):1431. https://doi.org/10.3390/cancers15051431
Chicago/Turabian StyleStares, Mark, Georgina Lewis, Maheva Vallet, Angus Killean, Giovanni Tramonti, Ailsa Patrizio, Melanie Mackean, Stephen Harrow, Colin Barrie, Kirsty MacLennan, and et al. 2023. "Real-World Impact of SABR on Stage I Non-Small-Cell Lung Cancer Outcomes at a Scottish Cancer Centre" Cancers 15, no. 5: 1431. https://doi.org/10.3390/cancers15051431