
Associations of Age and Sex with the Efficacy of Inpatient Cancer Rehabilitation: Results from a Longitudinal Observational Study Using Electronic Patient-Reported Outcomes

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample and Procedure
2.2. Outcome Assessments
2.2.1. EORTC QLQ-C30
2.2.2. Hospital Anxiety and Depression Scale (HADS)
2.2.3. Norton Scale
2.3. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Treatment Modalities
3.3. Internal Consistency
3.4. Differences in Treatment Needs at Baseline Regarding Age, Sex and Frailty
3.5. Improvements in HRQOL and Psychological Distress
3.5.1. Improvements by Age Group
3.5.2. Improvement by Norton Scale Risk Score
3.5.3. Improvements by Sex
4. Discussion
4.1. Patient Group Differences in HROQL at the Start of Rehabilitation
4.2. Improvements in HRQOL during Rehabilitation in All Groups and Similar Improvement in All Groups
4.3. Strenghts and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Code Availability (Software Application or Custom Code)
References
- De Angelis, R.; Sant, M.; Coleman, M.P.; Francisci, S.; Baili, P.; Pierannunzio, D.; Trama, A.; Visser, O.; Brenner, H.; Ardanaz, E.; et al. Cancer Survival in Europe 1999-2007 by Country and Age: Results of EUROCARE--5-a Population-Based Study. Lancet Oncol. 2014, 15, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Karim-Kos, H.E.; Vries, E.; Soerjomataram, I.; Lemmens, V.; Siesling, S.; Coebergh, J.W. Recent Trends of Cancer in Europe: A Combined Approach of Incidence, Survival and Mortality for 17 Cancer Sites since the 1990s. Eur. J. Cancer 2008, 44, 1345–1389. [Google Scholar] [CrossRef] [PubMed]
- Dong, S.T.; Butow, P.N.; Costa, D.S.; Lovell, M.R.; Agar, M. Symptom Clusters in Patients with Advanced Cancer: A Systematic Review of Observational Studies. J. Pain Symptom Manag. 2014, 48, 411–450. [Google Scholar] [CrossRef]
- Fialka-Moser, V.; Crevenna, R.; Korpan, M.; Quittan, M. Cancer Rehabilitation: Particularly with Aspects on Physical Impairments. J. Rehabil. Med. 2003, 35, 153–162. [Google Scholar] [CrossRef] [Green Version]
- Maehr, B.; Keilani, M.; Wiltschke, C.; Hassler, M.; Licht, T.; Marosi, C.; Huetterer, E.; Cenik, F.; Crevenna, R. Cancer Rehabilitation in Austria--Aspects of Physical Medicine and Rehabilitation. Wien. Med. Wochenschr. 2016, 166, 39–43. [Google Scholar] [CrossRef]
- Gudbergsson, S.B.; Dahl, A.A.; Loge, J.H. What Is Covered by ”cancer Rehabilitation” in PubMed? A Review of Randomized Controlled Trials 1990–2011. J. Rehabil. Med. 2015, 47, 97–106. [Google Scholar] [CrossRef] [Green Version]
- Lindbohm, M.L.; Kuosma, E.; Taskila, T.; Hietanen, P.; Carlsen, K.; Gudbergsson, S.; Gunnarsdottir, H. Early Retirement and Non-Employment after Breast Cancer. Psychooncology 2014, 23, 634–641. [Google Scholar] [CrossRef]
- Prince, M.J.; Wu, F.; Guo, Y.; Gutierrez Robledo, L.M.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The Burden of Disease in Older People and Implications for Health Policy and Practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef]
- Kim, J.; Hurria, A. Determining Chemotherapy Tolerance in Older Patients with Cancer. J. Natl. Compr. Canc. Netw. 2013, 11, 1494–1502. [Google Scholar] [CrossRef] [Green Version]
- Muhandiramge, J.; Orchard, S.G.; Warner, E.T.; Londen, G.J.; Zalcberg, J. Functional Decline in the Cancer Patient: A Review. Cancers 2022, 14, 1368. [Google Scholar] [CrossRef]
- Scheepers, E.R.M.; Vondeling, A.M.; Thielen, N.; Griend, R.; Stauder, R.; Hamaker, M.E. Geriatric Assessment in Older Patients with a Hematologic Malignancy: A Systematic Review. Haematologica 2020, 105, 1484–1493. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Garcia, A.D.; Thomas, D.R. Assessment and Management of Chronic Pressure Ulcers in the Elderly. Med. Clin. N. Am. 2006, 90, 925–944. [Google Scholar] [CrossRef] [PubMed]
- Norton, D.; McLaren, R.; Exton-Smith, A.N. An Investigation of Geriatric Nursing Problems in Hospital; Churchill Livingstone: London, UK, 1962; Volume 69. [Google Scholar]
- González-Expósito, J.; García-Román, J.C.; Prado-Amores, M.; Pardo-Fernández, L.; Pariente-Rodrigo, E. La Escala de Norton como predictor de la calidad de vida relacionada con la salud en el anciano institucionalizado [The Norton Scale as predictor of health-related quality of life in institutionalized elderly]. Enferm. Clin. 2015, 25, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Natanzon, S.S.; Maor, E.; Klempfner, R.; Goldenberg, I.; Shaviv, E.; Massalha, E.; Shlomo, N.; Goldanov, Y.; Mazin, I. Norton Score and Clinical Outcomes Following Acute Decompensated Heart Failure Hospitalization. J. Cardiol. 2020, 76, 335–341. [Google Scholar] [CrossRef]
- Leshem-Rubinow, E.; Vaknin, A.; Sherman, S.; Justo, D. Norton Scale, Hospitalization Length, Complications, and Mortality in Elderly Patients Admitted to Internal Medicine Departments. Gerontology 2013, 59, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Halperin, E.; Engel, T.; Sherman, S.; Justo, D. Low Admission Norton Scale Scores Are Associated with Falls Long after Rehabilitation in the Elderly with Hip Fractures. Clin. Interv. Aging 2012, 7, 431–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geue, K.; Mehnert-Theuerkauf, A.; Stroske, I.; Brock, H.; Friedrich, M.; Leuteritz, K. Psychosocial Long-Term Effects of Young Adult Cancer Survivors: Study Protocol of the Longitudinal AYA-LE Long-Term Effects Study. Front. Psychol. 2021, 12, 688142. [Google Scholar] [CrossRef]
- Gondos, A.; Hiripi, E.; Holleczek, B.; Luttmann, S.; Eberle, A.; Brenner, H.; GEKID Cancer Survival Working Group. Survival among Adolescents and Young Adults with Cancer in Germany and the United States: An International Comparison. Int. J. Cancer 2013, 133, 2207–2215. [Google Scholar] [CrossRef]
- Smith, S.R. Rehabilitation Strategies and Outcomes of the Sarcoma Patient. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Husson, O.; Huijgens, P.C.; Graaf, W.T.A. Psychosocial Challenges and Health-Related Quality of Life of Adolescents and Young Adults with Hematologic Malignancies. Blood 2018, 132, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Pulewka, K.; Strauss, B.; Hochhaus, A.; Hilgendorf, I. Clinical, Social, and Psycho-Oncological Needs of Adolescents and Young Adults (AYA) versus Older Patients Following Hematopoietic Stem Cell Transplantation. J. Cancer Res. Clin. Oncol. 2021, 147, 1239–1246. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.M.W.; Yi, J.C.; Jim, H.S.L.; Loren, A.W.; Majhail, N.S.; Uberti, J.; Whalen, V.; Leisenring, W.M.; Flowers, M.E.D.; Lee, S.J.; et al. Age and Gender Differences in Financial Distress among Hematopoietic Cell Transplant Survivors. Support Care Cancer 2020, 28, 4361–4371. [Google Scholar] [CrossRef]
- DeRouen, M.C.; Smith, A.W.; Tao, L.; Bellizzi, K.M.; Lynch, C.F.; Parsons, H.M.; Kent, E.E.; Keegan, T.H.; AYA HOPE Study Collaborative Group. Cancer-Related Information Needs and Cancer’s Impact on Control over Life Influence Health-Related Quality of Life among Adolescents and Young Adults with Cancer. Psychooncology 2015, 24, 1104–1115. [Google Scholar] [CrossRef] [Green Version]
- Sodergren, S.C.; Husson, O.; Rohde, G.E.; Tomaszewska, I.M.; Vivat, B.; Yarom, N.; Griffiths, H.; Darlington, A.-S. A Life Put on Pause: An Exploration of the Health-Related Quality of Life Issues Relevant to Adolescents and Young Adults with Cancer. J. Adolesc. Young Adult Oncol. 2018, 7, 453–464. [Google Scholar] [CrossRef]
- Sodergren, S.C.; Husson, O.; Rohde, G.E.; Tomaszewska, I.M.; Griffiths, H.; Pessing, A.; Yarom, N.; Hooker, L.; Din, A.; Darlington, A.S.; et al. Does Age Matter? A Comparison of Health-Related Quality of Life Issues of Adolescents and Young Adults with Cancer. Eur. J. Cancer Care 2018, 27, e12980. [Google Scholar] [CrossRef]
- Husson, O.; Reeve, B.B.; Darlington, A.-S.; Cheung, C.K.; Sodergren, S.; van der Graaf, W.T.A.; Salsman, J.M. Next Step for Global Adolescent and Young Adult Oncology: A Core Patient-Centered Outcome Set. J. Natl. Cancer Inst. 2022, 114, 496–502. [Google Scholar] [CrossRef]
- Husson, O.; Sodergren, S.C.; Darlington, A.-S. The Importance of a Collaborative Health-Related Quality of Life Measurement Strategy for Adolescents and Young Adults with Cancer. Cancer 2021, 127, 1712–1713. [Google Scholar] [CrossRef]
- Sodergren, S.C.; Husson, O.; Robinson, J.; Rohde, G.E.; Tomaszewska, I.M.; Vivat, B.; Dyar, R.; Darlington, A.-S.; EORTC Quality of Life Group. Systematic Review of the Health-Related Quality of Life Issues Facing Adolescents and Young Adults with Cancer. Qual. Life Res. 2017, 26, 1659–1672. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, C.H.; Rosner, B.; Chen, W.Y.; Kawachi, I.; Colditz, G.A.; Holmes, M.D. Functional Impact of Breast Cancer by Age at Diagnosis. J. Clin. Oncol. 2004, 22, 1849–1856. [Google Scholar] [CrossRef] [PubMed]
- Linden, W.; Vodermaier, A.; Mackenzie, R.; Greig, D. Anxiety and Depression after Cancer Diagnosis: Prevalence Rates by Cancer Type, Gender, and Age. J. Affect Disord. 2012, 141, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Hinz, A.; Singer, S.; Brähler, E. European Reference Values for the Quality of Life Questionnaire EORTC QLQ-C30: Results of a German Investigation and a Summarizing Analysis of Six European General Population Normative Studies. Acta Oncol. 2014, 53, 958–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehnert, A.; Vehling, S.; Scheffold, K.; Ladehoff, N.; Schön, G.; Wegscheider, K.; Heckl, U.; Weis, J.; Koch, U. Prävalenz von Anpassungsstörung, Akuter Und Posttraumatischer Belastungsstörung Sowie Somatoformen Störungen Bei Krebspatienten. PPmP-Psychother. Psychosom. Med. Psychol. 2013, 63, 466–472. [Google Scholar]
- Phipps, E.; Braitman, L.E.; Stites, S.; Leighton, J.C. Quality of Life and Symptom Attribution in Long-Term Colon Cancer Survivors. J. Eval. Clin. Pract. 2008, 14, 254–258. [Google Scholar] [CrossRef] [PubMed]
- Greimel, E.R.; Padilla, G.V.; Grant, M.M. Gender Differences in Outcomes among Patients with Cancer. Psychooncology 1998, 7, 9638781. [Google Scholar] [CrossRef]
- Sheth Bhutada, J.; Hwang, A.; Liu, L.; Deapen, D.; Freyer, D. Poor-Prognosis Metastatic Cancers in Adolescents and Young Adults: Incidence Patterns, Trends, and Disparities. JNCI Cancer Spectr. 2021, 5, pkab039. [Google Scholar] [CrossRef]
- Lehmann, J.; Rothmund, M.; Riedl, D.; Rumpold, G.; Grote, V.; Fischer, M.J.; Holzner, B. Clinical Outcome Assessment in Cancer Rehabilitation and the Central Role of Patient-Reported Outcomes. Cancers 2021, 14, 84. [Google Scholar] [CrossRef] [PubMed]
- Macquart-Moulin, G.; Viens, P.; Bouscary, M.L.; Genre, D.; Resbeut, M.; Gravis, G.; Camerlo, J.; Maraninchi, D.; Moatti, J.P. Discordance between Physicians’ Estimations and Breast Cancer Patients’ Self-Assessment of Side-Effects of Chemotherapy: An Issue for Quality of Care. Br. J. Cancer 1997, 76, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Pavlović Mavić, M.; Šeparović, R.; Tečić Vuger, A.; Vazdar, L. Difference in Estimation of Side Effects of Chemotherapy between Physicians and Patients with Early-Stage Breast Cancer: The Use of Patient Reported Outcomes (PROs) in the Evaluation of Toxicity in Everyday Clinical Practice. Cancers 2021, 13, 5922. [Google Scholar] [CrossRef]
- Atkinson, T.M.; Li, Y.; Coffey, C.W.; Sit, L.; Shaw, M.; Lavene, D.; Bennett, A.V.; Fruscione, M.; Rogak, L.; Hay, J.; et al. Reliability of Adverse Symptom Event Reporting by Clinicians. Qual. Life Res. 2012, 21, 1159–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkinson, T.M.; Schwartz, C.E.; Goldstein, L.; Garcia, I.; Storfer, D.F.; Li, Y.; Zhang, J.; Bochner, B.H.; Rapkin, B.D. Perceptions of Response Burden Associated with Completion of Patient-Reported Outcome Assessments in Oncology. Value Health 2019, 22, 225–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lampic, C.; Sjödén, P.O. Patient and Staff Perceptions of Cancer Patients’ Psychological Concerns and Needs. Acta Oncol. 2000, 39, 9–22. [Google Scholar] [CrossRef] [Green Version]
- Gouveia, L.; Lelorain, S.; Brédart, A.; Dolbeault, S.; Bonnaud-Antignac, A.; Cousson-Gélie, F.; Sultan, S. Oncologists’ Perception of Depressive Symptoms in Patients with Advanced Cancer: Accuracy and Relational Correlates. BMC Psychol. 2015, 3, 6. [Google Scholar] [CrossRef] [Green Version]
- Chandwani, K.D.; Zhao, F.; Morrow, G.R.; Deshields, T.L.; Minasian, L.M.; Manola, J.; Fisch, M.J. Lack of Patient-Clinician Concordance in Cancer Patients: Its Relation With Patient Variables. J. Pain Symptom Manag. 2017, 53, 988–998. [Google Scholar] [CrossRef] [Green Version]
- Gordon, B.E.; Chen, R.C. Patient-reported outcomes in cancer survivorship. Acta Oncol. 2017, 56, 166–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teichmann, J.V. Onkologische Rehabilitation: Evaluation der Effektivität stationärer onkologischer Rehabilitationsmassnahmen [Oncological rehabilitation: Evaluation of the efficiency of inpatient rehabilitation. Rehabilitation 2002, 41, 53–63. [Google Scholar] [CrossRef]
- Klocker, J.; Klocker-Kaiser, U.; Pipam, W.; Geissler, D. Long-Term Improvement of the Bio-Psycho-Social State of Cancer Patients after 3 Weeks of Inpatient Oncological Rehabilitation: A Long-Term Study at the Humanomed Zentrum Althofen. Wien. Med. Wochenschr. 2018, 168, 350–360. [Google Scholar] [CrossRef]
- Hartmann, U.; Kluge, A.; Ring, C.; Reuss-Borst, M. Verbesserung von Angst und Depression bei Brustkrebspatientinnen während stationärer onkologischer Rehabilitation—Ergebnisse einer prospektiven Studie [Improvement of anxiety and depression in women with breast cancer during inpatient oncological rehabilitation– results of a prospective study]. Rehabilitation 2006, 45, 88–94. [Google Scholar] [CrossRef]
- Leclerc, A.F.; Foidart-Dessalle, M.; Tomasella, M.; Coucke, P.; Devos, M.; Bruyère, O.; Bury, T.; Deflandre, D.; Jerusalem, G.; Lifrange, E.; et al. Multidisciplinary Rehabilitation Program after Breast Cancer: Benefits on Physical Function, Anthropometry and Quality of Life. Eur. J. Phys. Rehabil. Med. 2017, 53, 633–642. [Google Scholar] [CrossRef]
- Kirkham, A.A.; Klika, R.J.; Ballard, T.; Downey, P.; Campbell, K.L. Effective Translation of Research to Practice: Hospital-Based Rehabilitation Program Improves Health-Related Physical Fitness and Quality of Life of Cancer Survivors. J. Natl. Compr. Canc. Netw. 2016, 14, 1555–1562. [Google Scholar] [CrossRef] [PubMed]
- Wintner, L.M.; Sztankay, M.; Riedl, D.; Rumpold, G.; Nickels, A.; Licht, T.; Holzner, B. How to implement routine electronic patient-reported outcome monitoring in oncology rehabilitation. Int. J. Clin. Pract. 2021, 75, e13694. [Google Scholar] [CrossRef] [PubMed]
- Licht, T.; Nickels, A.; Rumpold, G.; Holzner, B.; Riedl, D. Evaluation by Electronic Patient-Reported Outcomes of Cancer Survivors’ Needs and the Efficacy of Inpatient Cancer Rehabilitation in Different Tumor Entities. Support Care Cancer 2021, 29, 5853–5864. [Google Scholar] [CrossRef]
- Holzner, B.; Giesinger, J.M.; Pinggera, J.; Zugal, S.; Schöpf, F.; Oberguggenberger, A.S.; Gamper, E.M.; Zabernigg, A.; Weber, B.; Rumpold, G. The Computer-Based Health Evaluation Software (CHES): A Software for Electronic Patient-Reported Outcome Monitoring. BMC Med. Inform. Decis. Mak. 2012, 12, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cocks, K.; King, M.T.; Velikova, G.; de Castro, G.; Martyn St-James, M.; Fayers, P.M.; Brown, J.M. Evidence-Based Guidelines for Interpreting Change Scores for the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. Eur. J. Cancer 2012, 48, 1713–1721. [Google Scholar] [CrossRef]
- Herrmann, C. International Experiences with the Hospital Anxiety and Depression Scale–a Review of Validation Data and Clinical Results. J. Psychosom. Res. 1997, 42, 17–41. [Google Scholar] [CrossRef]
- Puhan, M.A.; Frey, M.; Büchi, S.; Schünemann, H.J. The Minimal Important Difference of the Hospital Anxiety and Depression Scale in Patients with Chronic Obstructive Pulmonary Disease. Health Qual. Life Outcomes 2008, 6, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Goldstone, L.A.; Goldstone, J. The Norton Score: An Early Warning of Pressure Sores? J. Adv. Nurs. 1982, 7, 419–426. [Google Scholar] [CrossRef]
- Cathcart-Rake, E.J.; Ruddy, K.J.; Bleyer, A.; Johnson, R.H. Breast Cancer in Adolescent and Young Adult Women Under the Age of 40 Years. JCO Oncol. Pract. 2021, 17, 305–313. [Google Scholar] [CrossRef]
- Salkind, N.J. (Ed.) Encyclopedia of Research Design; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2010. [Google Scholar] [CrossRef]
- Hinz, A.; Brähler, E. Normative Values for the Hospital Anxiety and Depression Scale (HADS) in the General German Population. J. Psychosom. Res. 2011, 71, 74–78. [Google Scholar] [CrossRef]
- Holm, S. A Simple Sequentially Rejective Multiple Test Procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Lehmann, J.; Giesinger, J.M.; Nolte, S.; Sztankay, M.; Wintner, L.M.; Liegl, G.; Rose, M.; Holzner, B. EORTC Quality of Life Group Normative Data for the EORTC QLQ-C30 from the Austrian General Population. Health Qual. Life Outcomes 2020, 18, 275. [Google Scholar] [CrossRef] [PubMed]
- Stark, D.P.; House, A. Anxiety in Cancer Patients. Br. J. Cancer 2000, 83, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Oertelt-Prigione, S.; Rooij, B.H.; Mols, F.; Oerlemans, S.; Husson, O.; Schoormans, D.; Haanen, J.B.; Poll-Franse, L.V. Sex-Differences in Symptoms and Functioning in >5000 Cancer Survivors: Results from the PROFILES Registry. Eur. J. Cancer 2021, 156, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Hinz, A.; Mehnert, A.; Ernst, J.; Herschbach, P.; Schulte, T. Fear of progression in patients 6 months after cancer rehabilitation-a- validation study of the fear of progression questionnaire FoP-Q-12. Support Care Cancer 2015, 23, 1579–1587. [Google Scholar] [CrossRef]
- Lang, M.J.; Giese-Davis, J.; Patton, S.B.; Campbell, D.J.T. Does Age Matter? Comparing Post-Treatment Psychosocial Outcomes in Young Adult and Older Adult Cancer Survivors with Their Cancer-Free Peers. Psychooncology 2018, 27, 1404–1411. [Google Scholar] [CrossRef] [Green Version]
- Warner, E.L.; Kent, E.E.; Trevino, K.M.; Parsons, H.M.; Zebrack, B.J.; Kirchhoff, A.C. Social Well-Being among Adolescents and Young Adults with Cancer: A Systematic Review. Cancer 2016, 122, 1029–1037. [Google Scholar] [CrossRef] [Green Version]
- Riedl, D.; Licht, T.; Nickels, A.; Rothmund, M.; Rumpold, G.; Holzner, B.; Grote, V.; Fischer, M.J.; Fischmeister, G. Large Improvements in Health-Related Quality of Life and Physical Fitness during Multidisciplinary Inpatient Rehabilitation for Pediatric Cancer Survivors. Cancers 2022, 14, 4855. [Google Scholar] [CrossRef]
- Altice, C.K.; Banegas, M.P.; Tucker-Seeley, R.D.; Yabroff, K.R. Financial Hardships Experienced by Cancer Survivors: A Systematic Review. J. Natl. Cancer Inst. 2016, 109, djw205. [Google Scholar] [CrossRef]
- Bachner, F.; Bobek, J.; Habimana, K.; Ladurner, J.; Lepuschutz, L.; Ostermann, H.; Rainer, L.; Schmidt, A.E.; Zuba, M.; Quentin, W.; et al. Health System Review. Health Syst. Transit. 2018, 20, 1–254. [Google Scholar]
- Trostchansky, I.; Nimrod, A.; Tiberiu, E.; Vigorita, V.; Valiñas, R.; Karp, G. Is Norton Score a Useful Tool for Identifying High-Risk Patients Prior to Emergency Surgery? ANZ J. Surg. 2019, 89, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Guy, N.; Lerman, Y.; Justo, D. Admission Norton Scale Scores (ANSS) Correlate with Rehabilitation Outcome and Length in Elderly Patients with Deconditioning. Arch. Gerontol. Geriatr. 2012, 54, 381–384. [Google Scholar] [CrossRef] [PubMed]
- de Vries, J.; Bras, L.; Sidorenkov, G.; Festen, S.; Steenbakkers, R.J.H.M.; Langendijk, J.A.; Witjes, M.J.H.; van der Laan, B.F.A.M.; de Bock, G.H.; Halmos, G.B. Frailty Is Associated with Decline in Health-Related Quality of Life of Patients Treated for Head and Neck Cancer. Oral. Oncol. 2020, 111, 105020. [Google Scholar] [CrossRef] [PubMed]
- Su, M.; Yao, N.; Shang, M.; Shen, Y.; Qin, T.; Wang, J.; Sun, X. Frailty and Its Association with Health-Related Quality of Life among Older Cancer Patients: An Evidence-Based Study from China. Health Qual. Life Outcomes 2022, 20, 124. [Google Scholar] [CrossRef]
- Geessink, N.; Schoon, Y.; van Goor, H.; Rikkert, M.O.; Melis, R.; on behalf of the TOPICS-MDS consortium. Frailty and Quality of Life among Older People with and without a Cancer Diagnosis: Findings from TOPICS-MDS. PLoS ONE 2017, 12, e0189648. [Google Scholar] [CrossRef] [Green Version]
- Kalter, J.; Verdonck-de Leeuw, I.M.; Sweegers, M.G.; Aaronson, N.K.; Jacobsen, P.B.; Newton, R.U.; Courneya, K.S.; Aitken, J.F.; Armes, J.; Arving, C.; et al. Effects and Moderators of Psychosocial Interventions on Quality of Life, and Emotional and Social Function in Patients with Cancer: An Individual Patient Data Meta-Analysis of 22 RCTs. Psychooncology 2018, 27, 1150–1161. [Google Scholar] [CrossRef] [Green Version]
- Kangas, M.; Bovbjerg, D.H.; Montgomery, G.H. Cancer-Related Fatigue: A Systematic and Meta-Analytic Review of Non-Pharmacological Therapies for Cancer Patients. Psychol. Bull. 2008, 134, 700–741. [Google Scholar] [CrossRef] [Green Version]
- Berger, A.M.; Mooney, K.; Alvarez-Perez, A.; Breitbart, W.S.; Carpenter, K.M.; Cella, D.; Cleeland, C.; Dotan, E.; Eisenberger, M.A.; Escalante, C.P.; et al. Cancer-Related Fatigue, Version 2.2015. J. Natl. Compr. Canc. Netw. 2015, 13, 1012–1039. [Google Scholar] [CrossRef]
- Craft, L.L.; Vaniterson, E.H.; Helenowski, I.B.; Rademaker, A.W.; Courneya, K.S. Exercise Effects on Depressive Symptoms in Cancer Survivors: A Systematic Review and Meta-Analysis. Cancer Epidemiol. Biomark. Prev. 2012, 21, 3–19. [Google Scholar] [CrossRef] [Green Version]
- Anderson, E.; Shivakumar, G.; Mooney, K.; Alvarez-Perez, A.; Breitbart, W.S.; Carpenter, K.M.; Cella, D.; Cleeland, C.; Dotan, E.; Eisenberger, M.A.; et al. Effects of Exercise and Physical Activity on Anxiety. Front. Psychiatry 2013, 4, 27. [Google Scholar] [CrossRef] [Green Version]
- Pergolotti, M.; Deal, A.M.; Williams, G.R.; Bryant, A.L.; McCarthy, L.; Nyrop, K.A.; Covington, K.R.; Reeve, B.B.; Basch, E.; Muss, H.B. Older Adults with Cancer: A Randomized Controlled Trial of Occupational and Physical Therapy. J. Am. Geriatr. Soc. 2019, 67, 953–960. [Google Scholar] [CrossRef] [PubMed]
- Keilani, M.; Hasenoehrl, T.; Baumann, L.; Ristl, R.; Schwarz, M.; Marhold, M.; Sedghi Komandj, T.; Crevenna, R. Effects of resistance exercise in prostate cancer patients: A meta-analysis. Support Care Cancer 2017, 25, 2953–2968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caillet, P.; Laurent, M.; Bastuji-Garin, S.; Liuu, E.; Culine, S.; Lagrange, J.L.; Canoui-Poitrine, F.; Paillaud, E. Optimal Management of Elderly Cancer Patients: Usefulness of the Comprehensive Geriatric Assessment. Clin. Interv. Aging 2014, 9, 1645–1660. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Total Sample | >40 Years | 40–69 Years | ≥70 Years | |
|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | |
| Sample size (row %) | 5567 | 248 (4.5) | 3927 (70.5) | 1392 (25.0) |
| Sex | ||||
| Male | 2077 (37.3) | 87 (35.1) | 1363 (34.7) | 627 (45.0) |
| Female | 3490 (62.7) | 161 (64.9) | 2564 (65.3) | 765 (55.0) |
| Age | ||||
| Mean (SD) | 60.7 (12.0) | 33.1 (4.8) | 56.9 (7.0) | 76.2 (4.6) |
| Body mass index (BMI) | ||||
| Mean kg/m2 (SD) | 25.8 (5.2) | 24.4 (5.9) | 25.8 (5.3) | 26.0 (4.7) |
| Smoker | 936 (16.8) | 60 (24.2) | 760 (19.3) | 116 (8.3) |
| KPS | ||||
| High level of functioning (81–100%) | 1805 (32.7) | 109 (43.9) | 1337 (34.5) | 359 (26.0) |
| Medium level of functioning (51–80%) | 3675 (65.2) | 136 (54.8) | 2532 (65.3) | 1007 (72.9) |
| Low level of functioning (0–50%) | 111 (2.6) | 3 (1.2) | 12 (0.3) | 14 (1.0) |
| Missing information * | 58 | 0 | 46 | 12 |
| ECOG score | ||||
| Grade 0 | 417 (7.6) | 31 (12.6) | 324 (8.4) | 62 (4.5) |
| Grade 1 | 3219 (58.6) | 167 (67.6) | 2400 (62.1) | 652 (47.3) |
| Grade 2 | 1787 (32.5) | 45 (18.2) | 1115 (28.8) | 627 (45.5) |
| Grade 3 | 70 (1.3) | 4 (1.6) | 28 (0.7) | 38 (2.8) |
| Missing information * | 74 | 1 | 60 | 13 |
| Norton scale (n = 4791, 84.8%) | ||||
| Mean | 16.7 (1.9) | 18.2 (1.3) | 17.1 (1.6) | 15.4 (2.0) |
| <15 points (high risk) | 569 (12.1) | 4 (1.9) | 228 (6.8) | 337 (29.4) |
| ≥15 points (low risk) | 4150 (87.9) | 212 (98.1) | 3127 (93.2) | 811 (70.6) |
| Norton scale not assessed * | 848 | 32 | 572 | 244 |
| Cancer entities | ||||
| Head and neck cancers (C00–14; C30–C32) | 285 (5.1) | 3 (1.2) | 229 (5.8) | 53 (3.8) |
| Esophageal cancer (C15) | 75 (1.3) | 2 (0.8) | 50 (1.3) | 23 (1.7) |
| Gastric cancer (C16) | 149 (2.7) | 1 (0.4) | 89 (2.3) | 59 (4.2) |
| Colon cancer (C18–19) | 327 (5.9) | 3 (1.2) | 218 (5.6) | 106 (7.6) |
| Rectal cancer (C20–21) | 184 (3.3) | 1 (0.4) | 127 (3.2) | 56 (4.0) |
| Liver cancer(C22) | 38 (0.7) | 0 (0) | 16 (0.4) | 22 (1.6) |
| Pancreatic cancer (C25) | 118 (2.1) | 1 (0.4) | 67 (1.7) | 50 (3.6) |
| Lung cancer (C33–C34) | 273 (4.9) | 3 (1.2) | 164 (4.2) | 106 (7.6) |
| Skin cancer (C43–44) | 50 (0.9) | 2 (0.8) | 31 (0.8) | 17 (1.2) |
| Breast cancer (C50) | 1965 (35.3) | 66 (26.6) | 1565 (39.9) | 334 (24.0) |
| Uterine cancers (C51–55) | 182 (3.3) | 11 (4.4) | 134 (3.4) | 37 (2.7) |
| Ovarian cancer(C56) | 200 (3.6) | 7 (2.8) | 145 (3.7) | 48 (3.4) |
| Prostate cancer (C61) | 441 (7.9) | 0 (0) | 274 (7.0) | 167 (12.0) |
| Testicular cancer (C62) | 58 (1.0) | 23 (9.3) | 35 (0.9) | 0 (0) |
| Renal cancer (C64) | 115 (2.1) | 1 (0.4) | 80 (2.0) | 34 (2.4) |
| Bladder cancer (C67) | 122 (2.2) | 2 (0.8) | 67 (1.7) | 53 (3.8) |
| Brain cancers (C70–72) | 77 (1.4) | 13 (5.2) | 54 (1.4) | 10 (0.7) |
| Thyroid cancer (C73) | 52 (0.9) | 14 (5.6) | 35 (0.9) | 3 (0.2) |
| Malignant lymphomas (C81–C86; C88) | 369 (6.6) | 65 (26.2) | 234 (6.0) | 70 (5.0) |
| Multiple myeloma (C90) | 88 (1.6) | 0 (0) | 60 (1.5) | 28 (2.0) |
| Leukemias (C91–C95) | 108 (1.9) | 17 (6.9) | 64 (1.6) | 27 (1.9) |
| Other cancer types | 291 (5.2) | 13 (5.2) | 189 (4.8) | 89 (6.4) |
| Total Sample | >40 Years | 40–69 Years | ≥70 Years | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | mdn | IQR | N | % | mdn | IQR | N | % | mdn | IQR | N | % | mdn | IQR | |
| Guidance and treatment by physician | 5567 | 100.0 | 6 | 5–7 | 248 | 100.0 | 6 | 5–7 | 3927 | 100.0 | 6 | 5–7 | 1392 | 100.0 | 6 | 5–7 |
| Psycho-oncological counseling (group) | 5567 | 100.0 | 1 | 1–1 | 248 | 100.0 | 1 | 1–1 | 3927 | 100.0 | 1 | 1–1 | 1392 | 100.0 | 1 | 1–1 |
| Relaxation therapies | 5566 | 99.9 | 3 | 3–5 | 248 | 100.0 | 4 | 3–5 | 3927 | 100.0 | 3 | 3–5 | 1391 | 99.9 | 4 | 3–5 |
| Physiotherapy (individual treatment) | 5565 | 99.9 | 6 | 5–8 | 248 | 100.0 | 6 | 5–8 | 3926 | 100.0 | 6 | 5–8 | 1391 | 99.9 | 6 | 5–8 |
| Nutritional advice | 5563 | 99.9 | 4 | 3–4 | 248 | 100.0 | 3 | 3–4 | 3925 | 99.9 | 4 | 3–4 | 1390 | 99.9 | 4 | 3–4 |
| Psycho-educative lectures | 5558 | 99.8 | 3 | 2–3 | 247 | 99.6 | 3 | 2–4 | 3921 | 99.8 | 3 | 2–3 | 1390 | 99.9 | 3 | 2–3 |
| Nursing procedures | 5555 | 99.8 | 2 | 2–2 | 248 | 100.0 | 2 | 2–2 | 3917 | 99.7 | 2 | 2–2 | 1390 | 99.9 | 2 | 2–2 |
| Physiotherapy (groups) | 5534 | 99.4 | 7 | 5–10 | 244 | 98.4 | 6 | 5–8 | 3910 | 99.6 | 7 | 5–9 | 1380 | 99.1 | 8 | 6–11 |
| Medical training therapy—aerobic training | 5506 | 98.9 | 7 | 5–9 | 246 | 99.2 | 7 | 6–9 | 3894 | 99.2 | 7 | 5–9 | 1366 | 98.1 | 6 | 5–9 |
| Psycho-oncology (individual counseling) including biofeedback | 5361 | 96.3 | 5 | 4–7 | 239 | 96.4 | 6 | 5–7 | 3769 | 96.0 | 5 | 4–7 | 1353 | 97.2 | 5 | 4–6 |
| Remedial massages | 5350 | 96.1 | 3 | 3–4 | 245 | 98.8 | 3 | 3–4 | 3785 | 96.4 | 3 | 3–4 | 1320 | 94.8 | 3 | 3–4 |
| Functional occupational therapies (groups) | 5307 | 95.3 | 5 | 4–7 | 240 | 96.8 | 5 | 4–7 | 3760 | 95.7 | 6 | 4–7 | 1307 | 93.9 | 5 | 3–7 |
| Educational presentations—motivation and lifestyle modification | 5229 | 93.9 | 2 | 1–3 | 230 | 92.7 | 2 | 1–2 | 3692 | 94.0 | 2 | 1–3 | 1307 | 93.9 | 2 | 1–3 |
| Medical training therapy—resistance training | 5168 | 92.8 | 5 | 4–7 | 244 | 98.4 | 6 | 4–7 | 3746 | 95.4 | 5 | 4–7 | 1178 | 84.6 | 5 | 4–6 |
| Social counseling | 4870 | 87.5 | 2 | 1–2 | 233 | 94.0 | 2 | 2–3 | 3559 | 90.6 | 2 | 1–3 | 1078 | 77.4 | 2 | 1–2 |
| Educational lectures | 4674 | 84.0 | 1 | 1–2 | 206 | 83.1 | 1 | 1–1 | 3269 | 83.2 | 1 | 1–1 | 1199 | 86.1 | 1 | 1–2 |
| Occupational therapy (individual treatment) | 4666 | 83.8 | 2 | 2–3 | 201 | 81.0 | 2 | 2–3 | 3292 | 83.8 | 2 | 2–3 | 1173 | 84.3 | 3 | 2–3 |
| Thermotherapy | 4248 | 76.3 | 4 | 3–7 | 180 | 72.6 | 4 | 3–6 | 3026 | 77.1 | 4 | 3–7 | 1042 | 74.9 | 5 | 3–7 |
| Electrotherapy | 2863 | 51.4 | 4 | 3–6 | 123 | 49.6 | 4 | 3–6 | 2067 | 52.6 | 4 | 3–6 | 673 | 48.3 | 5 | 3–6 |
| Hydrogymnastics | 2554 | 45.9 | 3 | 2–4 | 156 | 62.9 | 3 | 2–4 | 1905 | 48.5 | 3 | 2–4 | 493 | 35.4 | 3 | 2–4 |
| Manual lymphatic drainage | 1422 | 25.5 | 4 | 3–6 | 38 | 15.3 | 3 | 2–5 | 1075 | 27.4 | 4 | 3–6 | 309 | 22.2 | 4 | 3–6 |
| Cognitive and perception training | 1370 | 24.6 | 2 | 2–4 | 44 | 17.7 | 2 | 1–2 | 825 | 21.0 | 2 | 1–4 | 501 | 36.0 | 2 | 2–4 |
| Psychological counseling: sexual therapy | 1098 | 19.7 | 1 | 1–4 | 63 | 25.4 | 1 | 1–3 | 865 | 22.0 | 1 | 1–4 | 170 | 12.2 | 2 | 1–4 |
| Inhalation therapies | 887 | 15.9 | 5 | 4–7 | 24 | 9.7 | 4 | 3–6 | 596 | 15.2 | 5 | 4–7 | 267 | 19.2 | 5 | 4–7 |
| Creative therapies | 597 | 10.7 | 2 | 2–4 | 33 | 13.3 | 4 | 2–4 | 439 | 11.2 | 2 | 2–4 | 125 | 9.0 | 2 | 2–4 |
| Speech therapy | 402 | 7.2 | 4 | 2–6 | 14 | 5.6 | 4 | 1–6 | 291 | 7.4 | 4 | 2–6 | 97 | 7.0 | 4 | 2–5 |
| Therapeutic ultrasound | 313 | 5.6 | 3 | 2–4 | 4 | 1.6 | 2 | 2–3 | 228 | 5.8 | 3 | 2–5 | 81 | 5.8 | 3 | 2–4 |
| Age Group | N | T1 | T2 | Delta | d | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | (SD) | p a | Mean | (SD) | p b | |||||
| Functioning scales (higher scores indicate better functioning) | ||||||||||
| Physical functioning | <40 years | 248 | 77.4 | (17.6) | n.s. | 84.8 | 16.1 | 7.3 | 0.43 | <0.001 |
| 40–69 years | 3927 | 76.0 | (19.8) | - | 81.8 | 18.6 | 5.7 | 0.30 | ||
| ≥70 years | 1392 | 65.4 | (22.7) | ** | 73.9 | 20.4 | 8.5 | 0.40 | ||
| Role functioning | <40 years | 248 | 57.1 | (29.8) | n.s. | 69.8 | 27.5 | 12.8 | 0.45 | n.s. |
| 40–69 years | 3927 | 59.0 | (29.8) | - | 72.1 | 26.5 | 13.1 | 0.47 | ||
| ≥70 years | 1392 | 55.6 | (31.1) | n.s. | 70.7 | 27.0 | 15.1 | 0.52 | ||
| Social functioning | <40 years | 248 | 55.1 | (30.4) | n.s. | 69.4 | 29.8 | 14.2 | 0.47 | 0.036 |
| 40–69 years | 3927 | 59.7 | (29.5) | - | 74.4 | 26.2 | 14.8 | 0.53 | ||
| ≥70 years | 1392 | 58.7 | (31.3) | n.s. | 76.5 | 26.0 | 17.8 | 0.62 | ||
| Emotional functioning | <40 years | 248 | 54.9 | (25.6) | n.s. | 74.7 | 22.6 | 19.8 | 0.82 | n.s. |
| 40–69 years | 3927 | 57.8 | (25.0) | - | 77.3 | 22.2 | 19.4 | 0.82 | ||
| ≥70 years | 1392 | 59.4 | (24.7) | n.s. | 78.2 | 21.2 | 18.9 | 0.82 | ||
| Cognitive functioning | <40 years | 248 | 70.2 | (28.7) | n.s. | 77.2 | 23.8 | 7.1 | 0.27 | n.s. |
| 40–69 years | 3927 | 73.3 | (26.4) | - | 77.5 | 24.1 | 4.3 | 0.17 | ||
| ≥70 years | 1392 | 74.1 | (24.9) | n.s. | 78.8 | 22.6 | 4.7 | 0.20 | ||
| Global health/QOL | <40 years | 248 | 61.4 | (17.0) | n.s. | 74.4 | 16.5 | 13.0 | 0.78 | n.s. |
| 40–69 years | 3927 | 59.3 | (19.1) | - | 74.3 | 16.9 | 15.0 | 0.83 | ||
| ≥70 years | 1392 | 54.7 | (19.9) | ** | 70.7 | 17.7 | 16.1 | 0.85 | ||
| Symptom scales (higher scores indicate higher impairment) | ||||||||||
| Fatigue | <40 years | 248 | 54.4 | (26.8) | n.s. | 38.8 | (23.0) | 15.5 | 0.62 | n.s. |
| 40–69 years | 3927 | 50.8 | (25.8) | - | 35.6 | (23.9) | 15.1 | 0.61 | ||
| ≥70 years | 1392 | 56.1 | (26.5) | ** | 39.3 | (24.1) | 16.9 | 0.67 | ||
| Pain | <40 years | 248 | 34.9 | (27.7) | n.s. | 24.9 | (23.2) | 10.0 | 0.39 | <0.001 |
| 40–69 years | 3927 | 39.1 | (28.6) | - | 29.4 | (25.9) | 9.7 | 0.35 | ||
| ≥70 years | 1392 | 42.7 | (30.4) | n.s. | 29.7 | (28.0) | 13.0 | 0.44 | ||
| Nausea/vomiting | <40 years | 248 | 11.8 | (20.7) | n.s. | 8.1 | (19.7) | 3.7 | 0.18 | n.s. |
| 40–69 years | 3927 | 10.9 | (19.7) | - | 5.4 | (14.1) | 5.5 | 0.32 | ||
| ≥70 years | 1392 | 12.7 | (22.1) | n.s. | 7.0 | (17.1) | 5.7 | 0.29 | ||
| Sleep disturbances | <40 years | 248 | 39.7 | (34.7) | n.s. | 34.7 | (32.8) | 5.0 | 0.15 | <0.001 |
| 40–69 years | 3927 | 46.3 | (33.4) | - | 38.9 | (32.6) | 7.4 | 0.22 | ||
| ≥70 years | 1392 | 46.7 | (34.8) | n.s. | 35.8 | (32.7) | 10.9 | 0.32 | ||
| Dyspnea | <40 years | 248 | 32.3 | (32.8) | n.s. | 24.6 | (25.8) | 7.7 | 0.26 | n.s. |
| 40–69 years | 3927 | 30.7 | (30.9) | - | 28.7 | (28.3) | 2.0 | 0.07 | ||
| ≥70 years | 1392 | 36.7 | (33.6) | ** | 33.3 | (31.0) | 3.4 | 0.10 | ||
| Appetite loss | <40 years | 248 | 21.2 | (29.9) | n.s. | 12.8 | (25.3) | 8.5 | 0.31 | <0.001 |
| 40–69 years | 3927 | 19.9 | (29.3) | - | 11.5 | (23.1) | 8.4 | 0.32 | ||
| ≥70 years | 1392 | 28.9 | (35.2) | ** | 17.1 | (29.2) | 11.9 | 0.37 | ||
| Constipation | <40 years | 248 | 15.9 | (28.4) | n.s. | 7.8 | (20.8) | 8.1 | 0.32 | n.s. |
| 40–69 years | 3927 | 17.2 | (28.2) | - | 10.1 | (22.3) | 7.2 | 0.28 | ||
| ≥70 years | 1392 | 22.9 | (32.0) | ** | 15.3 | (27.6) | 7.7 | 0.26 | ||
| Diarrhea | <40 years | 248 | 15.1 | (25.0) | n.s. | 12.9 | (23.7) | 2.2 | 0.09 | n.s. |
| 40–69 years | 3927 | 14.4 | (26.1) | - | 10.1 | (21.6) | 4.2 | 0.18 | ||
| ≥70 years | 1392 | 18.6 | (29.2) | ** | 12.8 | (24.9) | 5.8 | 0.21 | ||
| Financial impact | <40 years | 248 | 37.8 | (33.4) | ** | 28.8 | (32.3) | 9.0 | 0.27 | n.s. |
| 40–69 years | 3927 | 29.6 | (34.0) | - | 21.6 | (29.9) | 8.0 | 0.25 | ||
| ≥70 years | 1392 | 19.5 | (29.0) | ** | 13.5 | (24.5) | 6.0 | 0.23 | ||
| HADS (higher scores indicate higher psychological distress) | ||||||||||
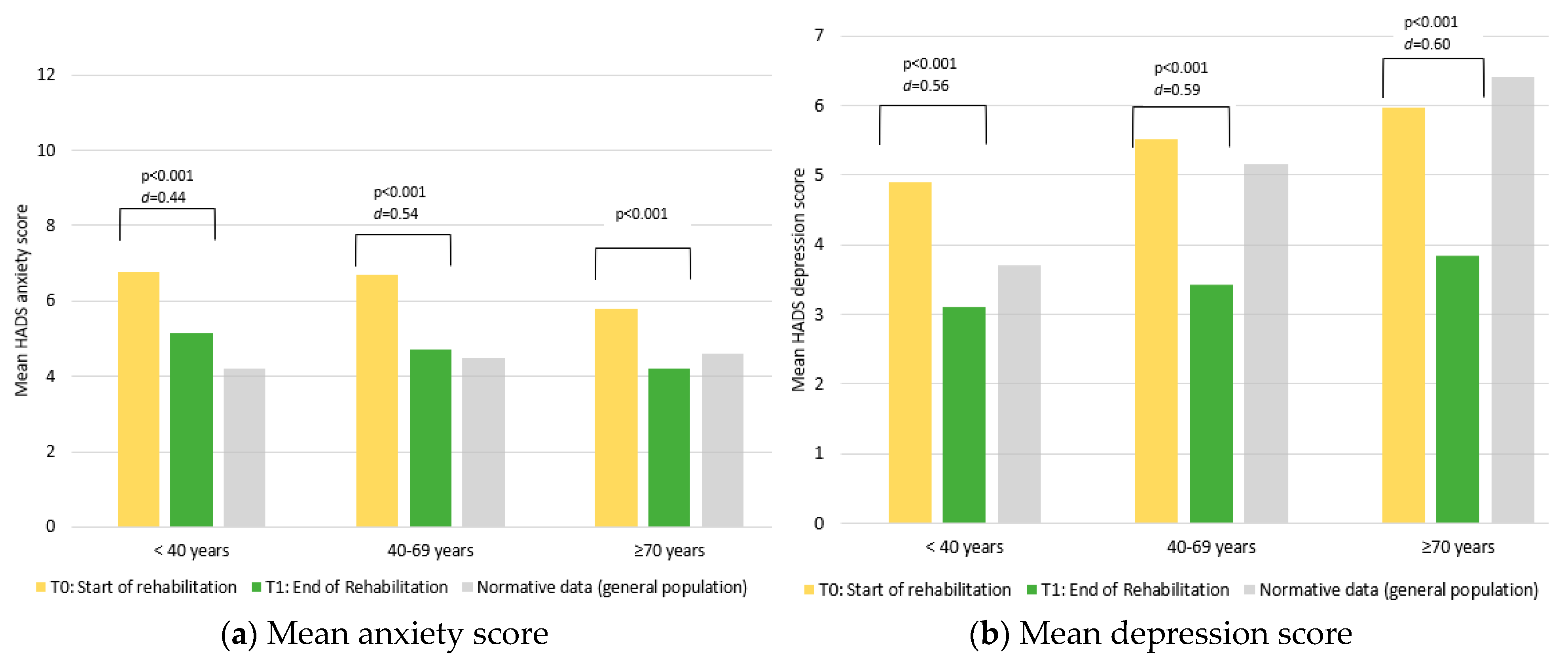
| Anxiety | <40 years | 248 | 6.8 | (4.0) | n.s. | 5.1 | (3.5) | 1.6 | 0.44 | <0.001 |
| 40–69 years | 3927 | 6.7 | (3.9) | - | 4.7 | (3.4) | 2.0 | 0.54 | ||
| ≥70 years | 1392 | 5.8 | (3.6) | ** | 4.2 | (3.2) | 1.6 | 0.47 | ||
| Depression | <40 years | 248 | 4.9 | (3.4) | n.s. | 3.1 | (2.9) | 1.8 | 0.56 | n.s. |
| 40–69 years | 3927 | 5.5 | (3.9) | - | 3.4 | (3.3) | 2.1 | 0.59 | ||
| ≥70 years | 1392 | 6.0 | (3.8) | ** | 3.9 | (3.2) | 2.1 | 0.60 | ||
| T1 | T2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Norton Score | N | Mean | (SD) | p a | Mean | (SD) | Delta | d | p b | |
| Functioning scales (higher scores indicate better functioning) | ||||||||||
| Physical functioning | Low risk | 4140 | 76.6 | 18.8 | ** | 82.5 | (17.4) | 5.9 | 0.33 | <0.001 |
| High risk | 566 | 53.4 | 23.1 | 63.0 | (22.8) | 9.6 | 0.42 | |||
| Role functioning | Low risk | 4140 | 60.5 | 29.3 | ** | 73.7 | (25.6) | 13.2 | 0.48 | n.s. |
| High risk | 566 | 44.4 | 31.6 | 58.0 | (30.1) | 13.6 | 0.44 | |||
| Social functioning | Low risk | 4140 | 61.2 | 29.2 | ** | 75.8 | (25.6) | 14.5 | 0.53 | <0.001 |
| High risk | 566 | 48.2 | 32.0 | 67.7 | (29.3) | 19.5 | 0.64 | |||
| Emotional functioning | Low risk | 4140 | 59.2 | 24.7 | ** | 78.3 | (21.4) | 19.1 | 0.83 | n.s. |
| High risk | 566 | 52.0 | 25.4 | 71.9 | (24.2) | 19.9 | 0.80 | |||
| Cognitive functioning | Low risk | 4140 | 74.3 | 25.9 | ** | 78.9 | (23.2) | 4.6 | 0.19 | n.s. |
| High risk | 566 | 68.1 | 27.2 | 72.3 | (26.1) | 4.2 | 0.16 | |||
| Global health/QOL | Low risk | 4140 | 60.1 | 18.7 | ** | 74.8 | (16.5) | 14.7 | 0.83 | n.s. |
| High risk | 566 | 47.7 | 19.9 | 64.4 | (18.4) | 16.8 | 0.87 | |||
| Symptom scales (higher scores indicate higher impairment) | ||||||||||
| Fatigue | Low risk | 4140 | 50.0 | 25.7 | ** | 34.8 | (23.2) | −15.2 | 0.62 | n.s. |
| High risk | 566 | 65.8 | 24.0 | 48.9 | (24.5) | −16.8 | 0.69 | |||
| Pain | Low risk | 4140 | 37.7 | 28.2 | ** | 27.7 | (25.2) | −10.0 | 0.37 | n.s. |
| High risk | 566 | 51.3 | 31.5 | 38.1 | (30.7) | −13.2 | 0.42 | |||
| Nausea/vomiting | Low risk | 4140 | 10.3 | 19.2 | ** | 5.3 | (14.2) | −5.1 | 0.30 | 0.042 |
| High risk | 566 | 17.8 | 26.0 | 10.1 | (19.9) | −7.8 | 0.34 | |||
| Sleep disturbances | Low risk | 4140 | 45.0 | 33.7 | ** | 37.7 | (32.7) | −7.3 | 0.22 | n.s. |
| High risk | 566 | 51.3 | 34.7 | 39.9 | (34.0) | −11.3 | 0.33 | |||
| Dyspnea | Low risk | 4140 | 30.2 | 30.7 | ** | 28.3 | (28.0) | −2.0 | 0.07 | 0.015 |
| High risk | 566 | 44.4 | 35.6 | 38.7 | (33.9) | −5.7 | 0.16 | |||
| Appetite loss | Low risk | 4140 | 20.2 | 29.7 | ** | 11.8 | (23.8) | −8.4 | 0.31 | n.s. |
| High risk | 566 | 33.5 | 35.8 | 21.5 | (31.5) | −11.9 | 0.35 | |||
| Constipation | Low risk | 4140 | 17.0 | 28.1 | ** | 10.3 | (22.6) | −6.8 | 0.27 | n.s. |
| High risk | 566 | 27.1 | 34.1 | 17.6 | (30.0) | −9.5 | 0.30 | |||
| Diarrhea | Low risk | 4140 | 14.5 | 26.2 | ** | 10.2 | (21.7) | −4.3 | 0.18 | n.s. |
| High risk | 566 | 21.7 | 30.3 | 13.8 | (25.7) | −7.9 | 0.28 | |||
| Financial impact | Low risk | 4140 | 27.0 | 33.0 | ** | 19.6 | (28.7) | −7.3 | 0.24 | n.s. |
| High risk | 566 | 29.9 | 33.7 | 23.3 | (32.2) | −6.6 | 0.20 | |||
| HADS (higher scores indicate higher psychological distress) | ||||||||||
| Anxiety | Low risk | 4140 | 6.4 | (3.8) | ** | 4.5 | (3.4) | 1.9 | 0.53 | n.s. |
| High risk | 566 | 6.6 | (3.9) | 5.0 | (3.6) | 1.7 | 0.44 | |||
| Depression | Low risk | 4140 | 5.3 | (3.7) | ** | 3.3 | (3.1) | 2.1 | 0.60 | n.s. |
| High risk | 566 | 7.1 | (4.2) | 4.9 | (3.7) | 2.2 | 0.57 | |||
| T1 | T2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sex | N | Mean | SD | p a | Mean | SD | Delta | d | p b | |
| Functioning scales (higher scores indicate better functioning) | ||||||||||
| Physical functioning | Male | 2077 | 73.4. | 21.7 | n.s. | 80.6 | (19.8) | 7.2 | 0.35 | n.s. |
| Female | 3490 | 73.5 | 20.6 | 79.6 | (19.0) | 6.1 | 0.31 | |||
| Role functioning | Male | 2077 | 58.3. | 31.4 | n.s. | 71.3 | (26.7) | 13.0 | 0.45 | n.s. |
| Female | 3490 | 57.9 | 29.5 | 71.9 | (26.7) | 13.9 | 0.50 | |||
| Social functioning | Male | 2077 | 57.6 | 30.6 | * | 73.3 | (26.4) | 15.7 | 0.55 | n.s. |
| Female | 3490 | 60.2 | 29.7 | 75.6 | (26.3) | 15.4 | 0.55 | |||
| Emotional functioning | Male | 2077 | 61.0 | 24.5 | ** | 78.3 | (21.4) | 17.3 | 0.75 | <.001 |
| Female | 3490 | 56.3 | 25.1 | 76.9 | (22.2) | 20.5 | 0.87 | |||
| Cognitive functioning | Male | 2077 | 76.1 | 25.1 | ** | 79.6 | (23.0) | 3.5 | 0.15 | n.s. |
| Female | 3490 | 71.7 | 26.6 | 76.8 | (24.1) | 5.1 | 0.20 | |||
| Global health/QOL | Male | 2077 | 56.9 | 19.9 | ** | 71.5 | (17.6) | 14.6 | 0.78 | n.s. |
| Female | 3490 | 59.1 | 19.0 | 74.6 | (16.8) | 15.5 | 0.87 | |||
| Symptom scales (higher scores indicate higher impairment) | ||||||||||
| Fatigue | Male | 2077 | 49.7 | 26.5 | ** | 34.8 | (23.7) | −14.9 | 0.59 | n.s. |
| Female | 3490 | 53.8 | 25.8 | 37.8 | (24.0) | −16.0 | 0.64 | |||
| Pain | Male | 2077 | 37.1 | 29.1 | ** | 26.5 | (25.9) | −10.6 | 0.39 | n.s. |
| Female | 3490 | 41.4 | 29.0 | 30.9 | (26.4) | −10.5 | 0.38 | |||
| Nausea/vomiting | Male | 2077 | 10.7 | 19.9 | n.s. | 5.8 | (14.7) | −4.9 | 0.28 | n.s. |
| Female | 3490 | 11.8 | 20.6 | 6.0 | (15.4) | −5.7 | 0.31 | |||
| Sleep disturbances | Male | 2077 | 40.5 | 33.8 | ** | 32.2 | (31.9) | −8.3 | 0.25 | n.s. |
| Female | 3490 | 49.4 | 33.5 | 41.3 | (32.7) | −8.1 | 0.24 | |||
| Dyspnea | Male | 2077 | 30.7 | 31.7 | * | 27.3 | (29.0) | −3.4 | 0.11 | n.s. |
| Female | 3490 | 33.2 | 31.8 | 31.0 | (28.9) | −2.1 | 0.07 | |||
| Appetite loss | Male | 2077 | 24.8 | 32.6 | ** | 14.8 | (26.4) | −10.0 | 0.34 | n.s. |
| Female | 3490 | 20.7 | 30.1 | 11.9 | (24.0) | −8.8 | 0.32 | |||
| Constipation | Male | 2077 | 16.9 | 27.4 | ** | 10.1 | (22.1) | −6.8 | 0.27 | n.s. |
| Female | 3490 | 19.6 | 30.3 | 12.0 | (24.7) | −7.6 | 0.28 | |||
| Diarrhea | Male | 2077 | 17.7 | 27.6 | ** | 12.3 | (23.3) | −5.3 | 0.21 | n.s. |
| Female | 3490 | 14.1 | 26.3 | 10.1 | (22.1) | −4.0 | 0.17 | |||
| Financial impact | Male | 2077 | 26.1 | 32.4 | n.s. | 19.4 | (28.5) | −6.8 | 0.22 | n.s. |
| Female | 3490 | 28.3 | 33.5 | 20.2 | (29.3) | −8.0 | 0.26 | |||
| HADS (higher scores indicate higher psychological distress) | ||||||||||
| Anxiety | Male | 2077 | 5.9 | (3.7) | ** | 4.3 | (3.4) | 1.6 | 0.46 | <0.001 |
| Female | 3490 | 6.8 | (3.8) | 4.8 | (3.4) | 2.0 | 0.56 | |||
| Depression | Male | 2077 | 5.7 | (3.9) | n.s. | 3.7 | (3.3) | 2.0 | 0.55 | n.s. |
| Female | 3490 | 5.5 | (3.8) | 3.4 | (3.2) | 2.1 | 0.61 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lehmann, J.; Riedl, D.; Nickels, A.; Sanio, G.; Hassler, M.; Rumpold, G.; Holzner, B.; Licht, T. Associations of Age and Sex with the Efficacy of Inpatient Cancer Rehabilitation: Results from a Longitudinal Observational Study Using Electronic Patient-Reported Outcomes. Cancers 2023, 15, 1637. https://doi.org/10.3390/cancers15061637
Lehmann J, Riedl D, Nickels A, Sanio G, Hassler M, Rumpold G, Holzner B, Licht T. Associations of Age and Sex with the Efficacy of Inpatient Cancer Rehabilitation: Results from a Longitudinal Observational Study Using Electronic Patient-Reported Outcomes. Cancers. 2023; 15(6):1637. https://doi.org/10.3390/cancers15061637
Chicago/Turabian StyleLehmann, Jens, David Riedl, Alain Nickels, Gabriele Sanio, Marco Hassler, Gerhard Rumpold, Bernhard Holzner, and Thomas Licht. 2023. "Associations of Age and Sex with the Efficacy of Inpatient Cancer Rehabilitation: Results from a Longitudinal Observational Study Using Electronic Patient-Reported Outcomes" Cancers 15, no. 6: 1637. https://doi.org/10.3390/cancers15061637