
The Mucin Family of Proteins: Candidates as Potential Biomarkers for Colon Cancer

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
3. Results
3.1. Mucin 1
3.1.1. MUC1 Mouse Studies
3.1.2. Therapeutic Applications of MUC1
3.1.3. Prognostication with MUC1

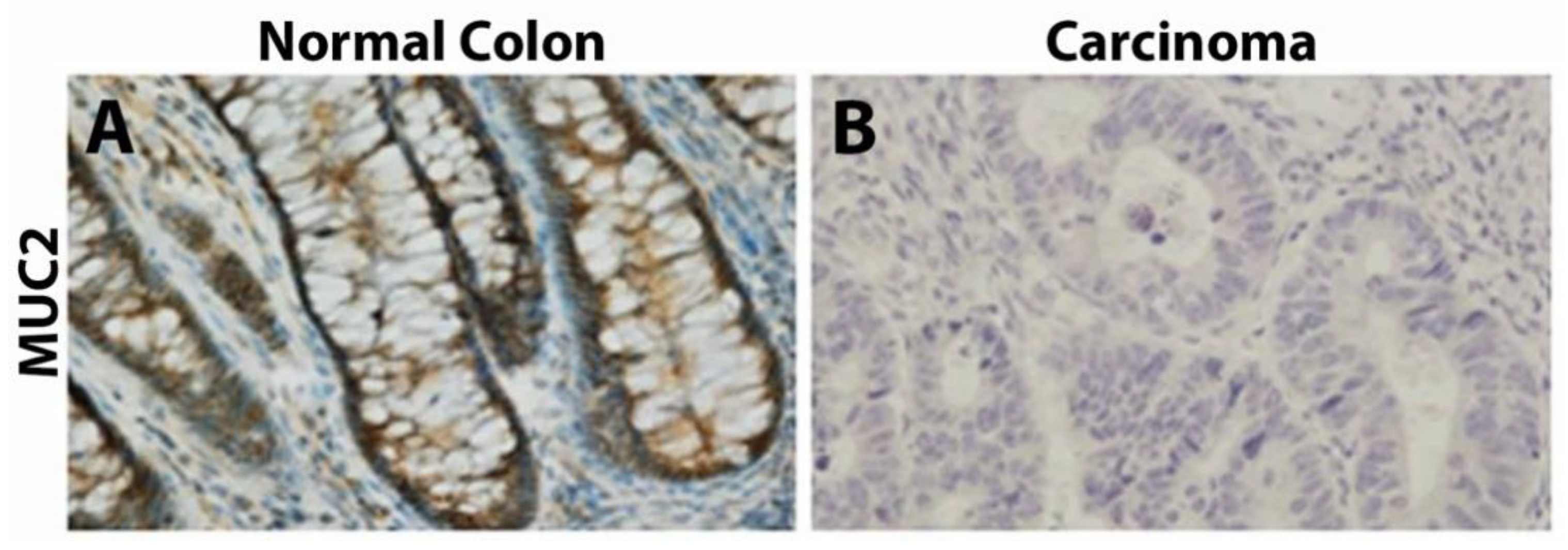
3.2. Mucin 2
3.2.1. MUC2 Expression within Polyps
3.2.2. MUC2 Mouse Studies
3.2.3. Prognostication with MUC2

3.3. Mucin 3

3.4. Mucin 4
3.4.1. MUC4 Expression within Polyps
3.4.2. MUC4 Mouse Studies
3.4.3. Prognostication with MUC4


3.5. Mucin 5
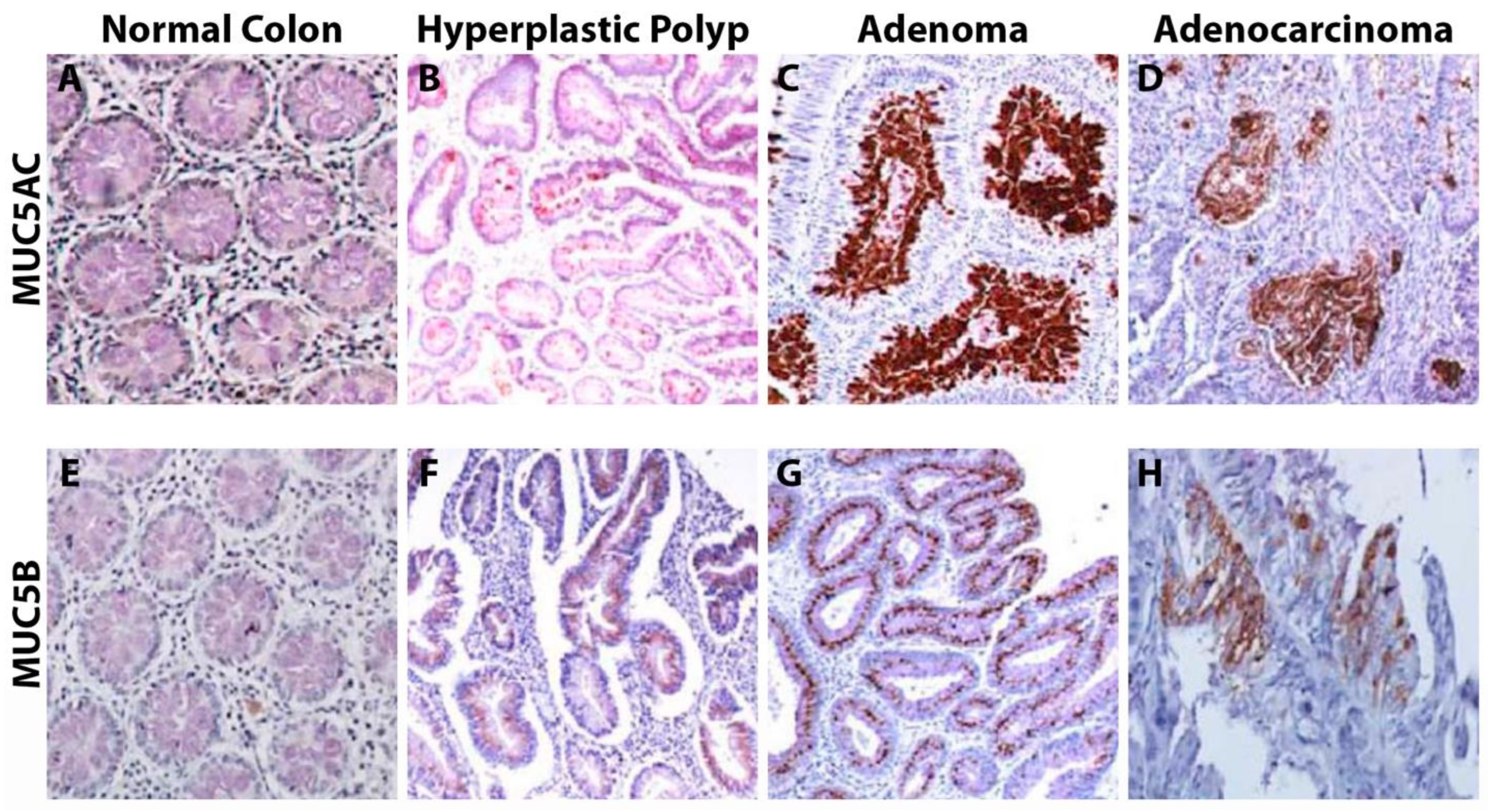
3.5.1. MUC5 Expression within Polyps
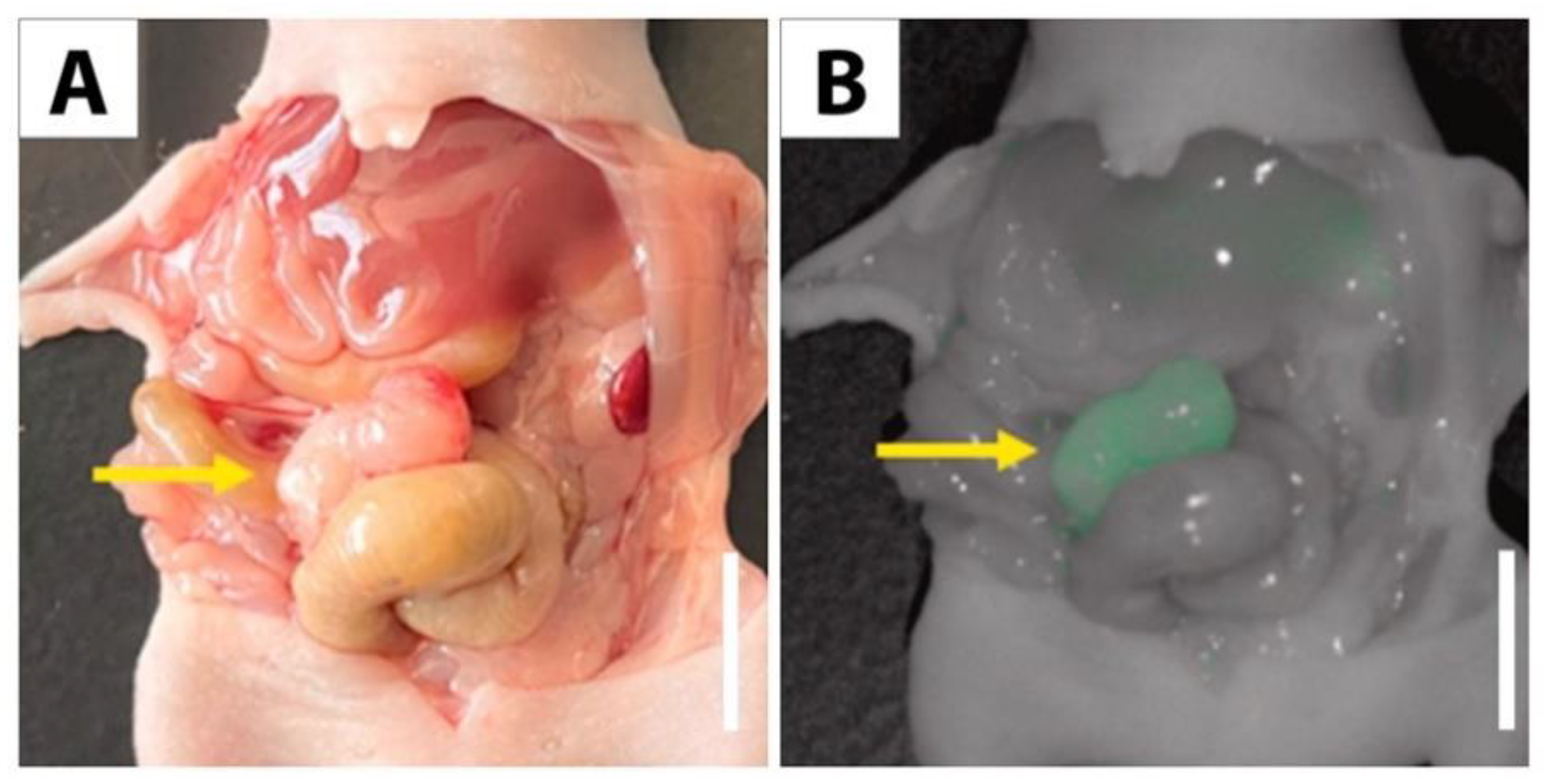
3.5.2. Tumor Imaging with MUC5AC
3.5.3. Prognostication with MUC5AC


3.6. Mucin 6
MUC6 Expression within Polyps

3.7. Mucins 7 and 8

3.8. Mucin 11

3.9. Mucin 12
Prognostication with MUC12

3.10. Mucin 13
3.10.1. MUC13 Mouse Studies
3.10.2. Prognostication with MUC13

3.11. Mucin 14

3.12. Mucin 15
MUC15 Mouse Studies

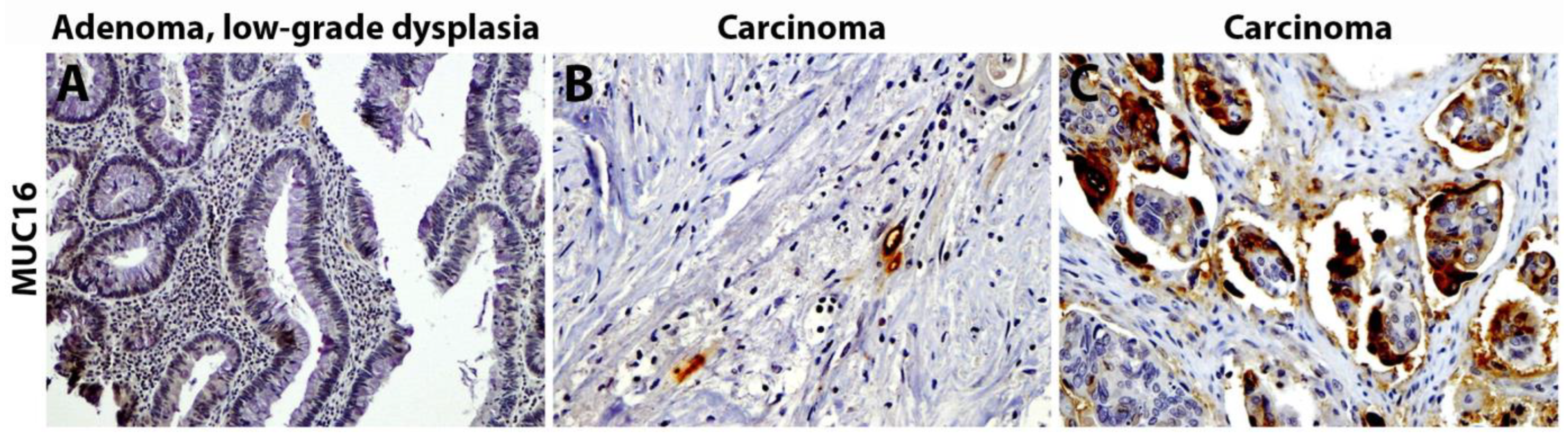
3.13. Mucin 16
Prognostication with MUC16

3.14. Mucin 17
3.14.1. MUC17 Expression within Polyps
3.14.2. MUC17 Mouse Studies

3.15. Mucin 18
MUC18 Mouse Studies

3.16. Mucin 19
3.17. Mucin 20
Prognostication with MUC20

3.18. Mucin 21
Prognostication with MUC21

4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer, J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Viale, P.H. The American Cancer Society’s Facts & Figures: 2020 Edition. J. Adv. Pract. Oncol. 2020, 11, 135–136. [Google Scholar] [PubMed]
- Carethers, J.M.; Jung, B.H. Genetics and Genetic Biomarkers in Sporadic Colorectal Cancer. Gastroenterology 2015, 149, 1177–1190 e1173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okugawa, Y.; Grady, W.M.; Goel, A. Epigenetic Alterations in Colorectal Cancer: Emerging Biomarkers. Gastroenterology 2015, 149, 1204–1225 e1212. [Google Scholar] [CrossRef] [Green Version]
- Pancione, M.; Remo, A.; Colantuoni, V. Genetic and epigenetic events generate multiple pathways in colorectal cancer progression. Pathol. Res. Int. 2012, 2012, 509348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buda, A.; De Bona, M.; Dotti, I.; Piselli, P.; Zabeo, E.; Barbazza, R.; Bellumat, A.; Valiante, F.; Nardon, E.; Probert, C.S.; et al. Prevalence of different subtypes of serrated polyps and risk of synchronous advanced colorectal neoplasia in average-risk population undergoing first-time colonoscopy. Clin. Transl. Gastroenterol. 2012, 3, e6. [Google Scholar] [CrossRef]
- Crockett, S.D.; Snover, D.C.; Ahnen, D.J.; Baron, J.A. Sessile serrated adenomas: An evidence-based guide to management. Clin. Gastroenterol. Hepatol. 2015, 13, 11–26 e11. [Google Scholar] [CrossRef]
- Hetzel, J.T.; Huang, C.S.; Coukos, J.A.; Omstead, K.; Cerda, S.R.; Yang, S.; O’Brien, M.J.; Farraye, F.A. Variation in the detection of serrated polyps in an average risk colorectal cancer screening cohort. Am. J. Gastroenterol. 2010, 105, 2656–2664. [Google Scholar] [CrossRef]
- Fearon, E.R. Molecular genetics of colorectal cancer. Annu. Rev. Pathol. 2011, 6, 479–507. [Google Scholar] [CrossRef]
- Johansson, M.E.; Sjövall, H.; Hansson, G.C. The gastrointestinal mucus system in health and disease. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 352–361. [Google Scholar] [CrossRef] [Green Version]
- Kufe, D.W. Mucins in cancer: Function, prognosis and therapy. Nat. Rev. Cancer 2009, 9, 874–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, S.; Kumar, S.; Momi, N.; Sasson, A.R.; Batra, S.K. Mucins in pancreatic cancer and its microenvironment. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 607–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatia, R.; Gautam, S.K.; Cannon, A.; Thompson, C.; Hall, B.R.; Aithal, A.; Banerjee, K.; Jain, M.; Solheim, J.C.; Kumar, S.; et al. Cancer-associated mucins: Role in immune modulation and metastasis. Cancer Metastasis Rev. 2019, 38, 223–236. [Google Scholar] [CrossRef]
- Breugelmans, T.; Oosterlinck, B.; Arras, W.; Ceuleers, H.; De Man, J.; Hold, G.L.; De Winter, B.Y.; Smet, A. The role of mucins in gastrointestinal barrier function during health and disease. Lancet Gastroenterol. Hepatol. 2022, 7, 455–471. [Google Scholar] [CrossRef] [PubMed]
- Pothuraju, R.; Krishn, S.R.; Gautam, S.K.; Pai, P.; Ganguly, K.; Chaudhary, S.; Rachagani, S.; Kaur, S.; Batra, S.K. Mechanistic and Functional Shades of Mucins and Associated Glycans in Colon Cancer. Cancers 2020, 12, 649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahan, R.; Kaur, S.; Macha, M.A.; Batra, S.K. Mucins (MUCs). In Encyclopedia of Signaling Molecules; Choi, S., Ed.; Springer: New York, NY, USA, 2016. [Google Scholar]
- Bafna, S.; Kaur, S.; Batra, S.K. Membrane-bound mucins: The mechanistic basis for alterations in the growth and survival of cancer cells. Oncogene 2010, 29, 2893–2904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coleman, O.I.; Haller, D. Microbe-Mucus Interface in the Pathogenesis of Colorectal Cancer. Cancers 2021, 13, 616. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Papadimitriou, J. Report on the first international workshop on carcinoma-associated mucins. Int. J. Cancer 1991, 49, 1–5. [Google Scholar] [CrossRef]
- Hollingsworth, M.A.; Swanson, B.J. Mucins in cancer: Protection and control of the cell surface. Nat. Rev. Cancer 2004, 4, 45–60. [Google Scholar] [CrossRef]
- Gendler, S.J. MUC1, the renaissance molecule. J. Mammary Gland Biol. Neoplasia 2001, 6, 339–353. [Google Scholar] [CrossRef]
- Spicer, A.P.; Duhig, T.; Chilton, B.S.; Gendler, S.J. Analysis of mammalian MUC1 genes reveals potential functionally important domains. Mamm. Genome 1995, 6, 885–888. [Google Scholar] [CrossRef] [PubMed]
- Patton, S.; Gendler, S.J.; Spicer, A.P. The epithelial mucin, MUC1, of milk, mammary gland and other tissues. Biochim. Biophys. Acta 1995, 1241, 407–423. [Google Scholar] [CrossRef] [PubMed]
- Girling, A.; Bartkova, J.; Burchell, J.; Gendler, S.; Gillett, C.; Taylor-Papadimitriou, J. A core protein epitope of the polymorphic epithelial mucin detected by the monoclonal antibody SM-3 is selectively exposed in a range of primary carcinomas. Int. J. Cancer 1989, 43, 1072–1076. [Google Scholar] [CrossRef] [PubMed]
- Pemberton, L.; Taylor-Papadimitriou, J.; Gendler, S.J. Antibodies to the cytoplasmic domain of the MUC1 mucin show conservation throughout mammals. Biochem. Biophys. Res. Commun. 1992, 185, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Bando, T.; Muguruma, N.; Ito, S.; Musashi, Y.; Inayama, K.; Kusaka, Y.; Tadatsu, M.; Kunio, I.; Irimura, T.; Shibamura, S.; et al. Basic studies on a labeled anti-mucin antibody detectable by infrared-fluorescence endoscopy. J. Gastroenterol. 2002, 37, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Nakamori, S.; Ota, D.M.; Cleary, K.R.; Shirotani, K.; Irimura, T. MUC1 mucin expression as a marker of progression and metastasis of human colorectal carcinoma. Gastroenterology 1994, 106, 353–361. [Google Scholar] [CrossRef]
- Wang, H.S.; Wang, L.H. The expression and significance of Gal-3 and MUC1 in colorectal cancer and colon cancer. OncoTargets Ther. 2015, 8, 1893–1898. [Google Scholar] [CrossRef] [Green Version]
- Gendler, S.J.; Spicer, A.P. Epithelial mucin genes. Annu. Rev. Physiol. 1995, 57, 607–634. [Google Scholar] [CrossRef]
- Ajioka, Y.; Allison, L.J.; Jass, J.R. Significance of MUC1 and MUC2 mucin expression in colorectal cancer. J. Clin. Pathol. 1996, 49, 560–564. [Google Scholar] [CrossRef] [Green Version]
- Limburg, P.J.; Ahlquist, D.A.; Gilbert, J.A.; Harrington, J.J.; Klee, G.G.; Roche, P.C. Immunodiscrimination of colorectal neoplasia using MUC1 antibodies: Discrepant findings in tissue versus stool. Dig. Dis. Sci. 2000, 45, 494–499. [Google Scholar] [CrossRef]
- Terada, T. An immunohistochemical study of primary signet-ring cell carcinoma of the stomach and colorectum: II. Expression of MUC1, MUC2, MUC5AC, and MUC6 in normal mucosa and in 42 cases. Int. J. Clin. Exp. Pathol. 2013, 6, 613–621. [Google Scholar] [PubMed]
- Baeckström, D.; Nilsson, O.; Price, M.R.; Lindholm, L.; Hansson, G.C. Discrimination of MUC1 mucins from other sialyl-Le(a)-carrying glycoproteins produced by colon carcinoma cells using a novel monoclonal antibody. Cancer Res. 1993, 53, 755–761. [Google Scholar] [PubMed]
- Devine, P.L.; Layton, G.T.; Clark, B.A.; Birrell, G.W.; Ward, B.G.; Xing, P.X.; McKenzie, I.F. Production of MUC1 and MUC2 mucins by human tumor cell lines. Biochem. Biophys. Res. Commun. 1991, 178, 593–599. [Google Scholar] [CrossRef]
- van Bracht, E.; Stolle, S.; Hafmans, T.G.; Boerman, O.C.; Oosterwijk, E.; van Kuppevelt, T.H.; Daamen, W.F. Specific targeting of tumor cells by lyophilisomes functionalized with antibodies. Eur. J. Pharm. Biopharm. 2014, 87, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Blockzjil, A.; Nilsson, K.; Nilsson, O. Epitope characterization of MUC1 antibodies. Tumour. Biol. 1998, 19 (Suppl. 1), 46–56. [Google Scholar] [CrossRef] [PubMed]
- Saxena, A.; Baliga, M.S.; Ponemone, V.; Kaur, K.; Larsen, B.; Fletcher, E.; Greene, J.; Fayad, R. Mucus and adiponectin deficiency: Role in chronic inflammation-induced colon cancer. Int. J. Colorectal Dis. 2013, 28, 1267–1279. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, P.; Pathangey, L.B.; Bradley, J.B.; Tinder, T.L.; Basu, G.D.; Akporiaye, E.T.; Gendler, S.J. MUC1-specific immune therapy generates a strong anti-tumor response in a MUC1-tolerant colon cancer model. Vaccine 2007, 25, 1607–1618. [Google Scholar] [CrossRef] [Green Version]
- Supruniuk, K.; Czarnomysy, R.; Muszyńska, A.; Radziejewska, I. Anti-cancer effects of pyrazole-platinum(II) complexes combined with anti-MUC1 monoclonal antibody versus monotherapy in DLD-1 and HT-29 colon cancer cells. Transl. Oncol. 2022, 18, 101348. [Google Scholar] [CrossRef]
- Loveland, B.E.; Zhao, A.; White, S.; Gan, H.; Hamilton, K.; Xing, P.X.; Pietersz, G.A.; Apostolopoulos, V.; Vaughan, H.; Karanikas, V.; et al. Mannan-MUC1-pulsed dendritic cell immunotherapy: A phase I trial in patients with adenocarcinoma. Clin. Cancer Res. 2006, 12 Pt 1, 869–877. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, P.L.; Quinn, M.A.; Grant, P.T.; Allen, D.G.; Jobling, T.W.; White, S.C.; Zhao, A.; Karanikas, V.; Vaughan, H.; Pietersz, G.; et al. A phase 2, single-arm study of an autologous dendritic cell treatment against mucin 1 in patients with advanced epithelial ovarian cancer. J. Immunother. Cancer 2014, 2, 16. [Google Scholar] [CrossRef]
- Gray, H.J.; Benigno, B.; Berek, J.; Chang, J.; Mason, J.; Mileshkin, L.; Mitchell, P.; Moradi, M.; Recio, F.O.; Michener, C.M.; et al. Progression-free and overall survival in ovarian cancer patients treated with CVac, a mucin 1 dendritic cell therapy in a randomized phase 2 trial. J. Immunother. Cancer 2016, 4, 34. [Google Scholar] [CrossRef] [Green Version]
- Karanikas, V.; Hwang, L.A.; Pearson, J.; Ong, C.S.; Apostolopoulos, V.; Vaughan, H.; Xing, P.X.; Jamieson, G.; Pietersz, G.; Tait, B.; et al. Antibody and T cell responses of patients with adenocarcinoma immunized with mannan-MUC1 fusion protein. J. Clin. Investig. 1997, 100, 2783–2792. [Google Scholar] [CrossRef] [Green Version]
- Karanikas, V.; Thynne, G.; Mitchell, P.; Ong, C.S.; Gunawardana, D.; Blum, R.; Pearson, J.; Lodding, J.; Pietersz, G.; Broadbent, R.; et al. Mannan mucin-1 peptide immunization: Influence of cyclophosphamide and the route of injection. J. Immunother. 2001, 24, 172–183. [Google Scholar] [CrossRef] [PubMed]
- Fiedler, W.; DeDosso, S.; Cresta, S.; Weidmann, J.; Tessari, A.; Salzberg, M.; Dietrich, B.; Baumeister, H.; Goletz, S.; Gianni, L.; et al. A phase I study of PankoMab-GEX, a humanised glyco-optimised monoclonal antibody to a novel tumour-specific MUC1 glycopeptide epitope in patients with advanced carcinomas. Eur. J. Cancer 2016, 63, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ledermann, J.A.; Zurawski, B.; Raspagliesi, F.; De Giorgi, U.; Arranz Arija, J.; Romeo Marin, M.; Lisyanskaya, A.; Póka, R.L.; Markowska, J.; Cebotaru, C.; et al. Maintenance therapy of patients with recurrent epithelial ovarian carcinoma with the anti-tumor-associated-mucin-1 antibody gatipotuzumab: Results from a double-blind, placebo-controlled, randomized, phase II study. ESMO Open 2022, 7, 100311. [Google Scholar] [CrossRef]
- Schoen, R.E. Vaccine Therapy in Treating Patients with Newly Diagnosed Advanced Colon Polyps. Registry Number: NCT02134925. Available online: Clinicaltrials.gov (accessed on 28 January 2023).
- Bagheri, E.; Abnous, K.; Farzad, S.A.; Taghdisi, S.M.; Ramezani, M.; Alibolandi, M. Targeted doxorubicin-loaded mesenchymal stem cells-derived exosomes as a versatile platform for fighting against colorectal cancer. Life Sci. 2020, 261, 118369. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Liu, T.; Yin, L.; Zuo, D.; Lin, Y.; Wang, L. Prognostic and clinicopathological value of MUC1 expression in colorectal cancer: A meta-analysis. Medicine (Baltimore) 2019, 98, e14659. [Google Scholar] [CrossRef]
- Gum, J.R.; Byrd, J.C.; Hicks, J.W.; Toribara, N.W.; Lamport, D.T.; Kim, Y.S. Molecular cloning of human intestinal mucin cDNAs. Sequence analysis and evidence for genetic polymorphism. J. Biol. Chem. 1989, 264, 6480–6487. [Google Scholar] [CrossRef]
- Johansson, M.E.; Phillipson, M.; Petersson, J.; Velcich, A.; Holm, L.; Hansson, G.C. The inner of the two Muc2 mucin-dependent mucus layers in colon is devoid of bacteria. Proc. Natl. Acad. Sci. USA 2008, 105, 15064–15069. [Google Scholar] [CrossRef] [Green Version]
- Reid, C.J.; Harris, A. Developmental expression of mucin genes in the human gastrointestinal system. Gut 1998, 42, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Ishizu, H.; Kumagai, J.; Eishi, Y.; Takizawa, T.; Koike, M. Mucin core protein expression by colorectal mucinous carcinomas with or without mucus hyperplasia. J. Gastroenterol. 2004, 39, 125–132. [Google Scholar] [CrossRef]
- Manne, U.; Weiss, H.L.; Grizzle, W.E. Racial differences in the prognostic usefulness of MUC1 and MUC2 in colorectal adenocarcinomas. Clin. Cancer Res. 2000, 6, 4017–4025. [Google Scholar] [PubMed]
- Chang, S.K.; Dohrman, A.F.; Basbaum, C.B.; Ho, S.B.; Tsuda, T.; Toribara, N.W.; Gum, J.R.; Kim, Y.S. Localization of mucin (MUC2 and MUC3) messenger RNA and peptide expression in human normal intestine and colon cancer. Gastroenterology 1994, 107, 28–36. [Google Scholar] [CrossRef]
- Wang, H.; Jin, S.; Lu, H.; Mi, S.; Shao, W.; Zuo, X.; Yin, H.; Zeng, S.; Shimamoto, F.; Qi, G. Expression of survivin, MUC2 and MUC5 in colorectal cancer and their association with clinicopathological characteristics. Oncol. Lett. 2017, 14, 1011–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blank, M.; Klussmann, E.; Krüger-Krasagakes, S.; Schmitt-Gräff, A.; Stolte, M.; Bornhoeft, G.; Stein, H.; Xing, P.X.; McKenzie, I.F.; Verstijnen, C.P. Expression of MUC2-mucin in colorectal adenomas and carcinomas of different histological types. Int. J. Cancer 1994, 59, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Walsh, M.D.; Clendenning, M.; Williamson, E.; Pearson, S.A.; Walters, R.J.; Nagler, B.; Packenas, D.; Win, A.K.; Hopper, J.L.; Jenkins, M.A.; et al. Expression of MUC2, MUC5AC, MUC5B, and MUC6 mucins in colorectal cancers and their association with the CpG island methylator phenotype. Mod. Pathol. 2013, 26, 1642–1656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bu, X.D.; Li, N.; Tian, X.Q.; Li, L.; Wang, J.S.; Yu, X.J.; Huang, P.L. Altered expression of MUC2 and MUC5AC in progression of colorectal carcinoma. World J. Gastroenterol. 2010, 16, 4089–4094. [Google Scholar] [CrossRef]
- Fujita, K.; Hirahashi, M.; Yamamoto, H.; Matsumoto, T.; Gushima, M.; Oda, Y.; Kishimoto, J.; Yao, T.; Iida, M.; Tsuneyoshi, M. Mucin core protein expression in serrated polyps of the large intestine. Virchows Arch. 2010, 457, 443–449. [Google Scholar] [CrossRef]
- Krishn, S.R.; Kaur, S.; Smith, L.M.; Johansson, S.L.; Jain, M.; Patel, A.; Gautam, S.K.; Hollingsworth, M.A.; Mandel, U.; Clausen, H.; et al. Mucins and associated glycan signatures in colon adenoma-carcinoma sequence: Prospective pathological implication(s) for early diagnosis of colon cancer. Cancer Lett. 2016, 374, 304–314. [Google Scholar] [CrossRef] [Green Version]
- Van der Sluis, M.; De Koning, B.A.; De Bruijn, A.C.; Velcich, A.; Meijerink, J.P.; Van Goudoever, J.B.; Büller, H.A.; Dekker, J.; Van Seuningen, I.; Renes, I.B.; et al. Muc2-deficient mice spontaneously develop colitis, indicating that MUC2 is critical for colonic protection. Gastroenterology 2006, 131, 117–129. [Google Scholar] [CrossRef]
- Velcich, A.; Yang, W.; Heyer, J.; Fragale, A.; Nicholas, C.; Viani, S.; Kucherlapati, R.; Lipkin, M.; Yang, K.; Augenlicht, L. Colorectal cancer in mice genetically deficient in the mucin Muc2. Science 2002, 295, 1726–1729. [Google Scholar] [CrossRef] [PubMed]
- Cecchini, M.J.; Walsh, J.C.; Parfitt, J.; Chakrabarti, S.; Correa, R.J.; MacKenzie, M.J.; Driman, D.K. CDX2 and Muc2 immunohistochemistry as prognostic markers in stage II colon cancer. Hum. Pathol. 2019, 90, 70–79. [Google Scholar] [CrossRef]
- Li, C.; Zuo, D.; Yin, L.; Lin, Y.; Li, C.; Liu, T.; Wang, L. Prognostic Value of MUC2 Expression in Colorectal Cancer: A Systematic Review and Meta-Analysis. Gastroenterol. Res. Pract. 2018, 2018, 6986870. [Google Scholar] [CrossRef] [Green Version]
- Pratt, W.S.; Crawley, S.; Hicks, J.; Ho, J.; Nash, M.; Kim, Y.S.; Gum, J.R.; Swallow, D.M. Multiple transcripts of MUC3: Evidence for two genes, MUC3A and MUC3B. Biochem. Biophys. Res. Commun. 2000, 275, 916–923. [Google Scholar] [CrossRef]
- Hattrup, C.L.; Gendler, S.J. Structure and function of the cell surface (tethered) mucins. Annu. Rev. Physiol. 2008, 70, 431–457. [Google Scholar] [CrossRef]
- Perçinel, S.; Savaş, B.; Ensari, A.; Kuzu, I.; Kuzu, M.A.; Bektaş, M.; Cetinkaya, H.; Kurşun, N. Mucins in the colorectal neoplastic spectrum with reference to conventional and serrated adenomas. Turk. J. Gastroenterol. 2007, 18, 230–238. [Google Scholar]
- Apostolopoulos, V.; Xing, P.X.; McKenzie, I.F. Anti-peptide monoclonal antibodies to intestinal mucin 3. J. Gastroenterol. Hepatol. 1995, 10, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Gum, J.R.; Crawley, S.C.; Hicks, J.W.; Szymkowski, D.E.; Kim, Y.S. MUC17, a novel membrane-tethered mucin. Biochem. Biophys. Res. Commun. 2002, 291, 466–475. [Google Scholar] [CrossRef]
- Williams, S.J.; Munster, D.J.; Quin, R.J.; Gotley, D.C.; McGuckin, M.A. The MUC3 gene encodes a transmembrane mucin and is alternatively spliced. Biochem. Biophys. Res. Commun. 1999, 261, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Xing, P.X.; Apostolopoulos, V.; Pietersz, G.; McKenzie, I.F. Anti-mucin monoclonal antibodies. Front. Biosci. 2001, 6, D1284–D1295. [Google Scholar] [CrossRef]
- Mukhopadhyay, P.; Chakraborty, S.; Ponnusamy, M.P.; Lakshmanan, I.; Jain, M.; Batra, S.K. Mucins in the pathogenesis of breast cancer: Implications in diagnosis, prognosis and therapy. Biochim. Biophys. Acta 2011, 1815, 224–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chauhan, S.C.; Singh, A.P.; Ruiz, F.; Johansson, S.L.; Jain, M.; Smith, L.M.; Moniaux, N.; Batra, S.K. Aberrant expression of MUC4 in ovarian carcinoma: Diagnostic significance alone and in combination with MUC1 and MUC16 (CA125). Mod. Pathol. 2006, 19, 1386–1394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majhi, P.D.; Lakshmanan, I.; Ponnusamy, M.P.; Jain, M.; Das, S.; Kaur, S.; Shimizu, S.T.; West, W.W.; Johansson, S.L.; Smith, L.M.; et al. Pathobiological implications of MUC4 in non-small-cell lung cancer. J. Thorac. Oncol. 2013, 8, 398–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyahara, N.; Shoda, J.; Ishige, K.; Kawamoto, T.; Ueda, T.; Taki, R.; Ohkohchi, N.; Hyodo, I.; Thomas, M.B.; Krishnamurthy, S.; et al. MUC4 interacts with ErbB2 in human gallbladder carcinoma: Potential pathobiological implications. Eur. J. Cancer 2008, 44, 1048–1056. [Google Scholar] [CrossRef]
- Tamada, S.; Shibahara, H.; Higashi, M.; Goto, M.; Batra, S.K.; Imai, K.; Yonezawa, S. MUC4 is a novel prognostic factor of extrahepatic bile duct carcinoma. Clin. Cancer Res. 2006, 12 Pt 1, 4257–4264. [Google Scholar] [CrossRef] [Green Version]
- Shanmugam, C.; Jhala, N.C.; Katkoori, V.R.; Wan, W.; Meleth, S.; Grizzle, W.E.; Manne, U. Prognostic value of mucin 4 expression in colorectal adenocarcinomas. Cancer 2010, 116, 3577–3586. [Google Scholar] [CrossRef] [Green Version]
- Biemer-Hüttmann, A.E.; Walsh, M.D.; McGuckin, M.A.; Ajioka, Y.; Watanabe, H.; Leggett, B.A.; Jass, J.R. Immunohistochemical staining patterns of MUC1, MUC2, MUC4, and MUC5AC mucins in hyperplastic polyps, serrated adenomas, and traditional adenomas of the colorectum. J. Histochem. Cytochem. 1999, 47, 1039–1048. [Google Scholar] [CrossRef]
- Das, S.; Rachagani, S.; Sheinin, Y.; Smith, L.M.; Gurumurthy, C.B.; Roy, H.K.; Batra, S.K. Mice deficient in Muc4 are resistant to experimental colitis and colitis-associated colorectal cancer. Oncogene 2016, 35, 2645–2654. [Google Scholar] [CrossRef] [Green Version]
- Turner, M.A.; Hollandsworth, H.M.; Amirfakhri, S.; Lwin, T.M.; Nishino, H.; Neel, N.C.; Natarajan, G.; Kaur, S.; Mallya, K.; Hoffman, R.M.; et al. Anti-mucin 4 fluorescent antibody brightly targets colon cancer in patient-derived orthotopic xenograft mouse models: A proof-of-concept study for future clinical applications. Am. J. Surg. 2022, 224, 1081–1085. [Google Scholar] [CrossRef]
- Peng, L.; Li, Y.; Gu, H.; Xiang, L.; Xiong, Y.; Wang, R.; Zhou, H.; Wang, J. Mucin 4 mutation is associated with tumor mutation burden and promotes antitumor immunity in colon cancer patients. Aging (Albany NY) 2021, 13, 9043–9055. [Google Scholar] [CrossRef]
- Lu, S.; Catalano, C.; Huhn, S.; Pardini, B.; Partu, L.; Vymetalkova, V.; Vodickova, L.; Levy, M.; Buchler, T.; Hemminki, K.; et al. Single nucleotide polymorphisms within MUC4 are associated with colorectal cancer survival. PLoS ONE 2019, 14, e0216666. [Google Scholar]
- Bartman, A.E.; Sanderson, J.; Ewing, S.L.; Niehans, G.A.; Wiehr, C.L.; Evans, M.K.; Ho, S.B. Aberrant expression of MUC5AC and MUC6 gastric mucin genes in colorectal polyps. Int. J. Cancer 1999, 80, 210–218. [Google Scholar] [CrossRef]
- Zhu, X.; Long, X.; Luo, X.; Song, Z.; Li, S.; Wang, H. Abrogation of MUC5AC Expression Contributes to the Apoptosis and Cell Cycle Arrest of Colon Cancer Cells. Cancer Biother. Radiopharm. 2016, 31, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Imai, Y.; Yamagishi, H.; Fukuda, K.; Ono, Y.; Inoue, T.; Ueda, Y. Differential mucin phenotypes and their significance in a variation of colorectal carcinoma. World J. Gastroenterol. 2013, 19, 3957–3968. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, K.J.; Rhee, Y.Y.; Bae, J.M.; Cho, N.Y.; Lee, H.S.; Kang, G.H. Gastric-type expression signature in serrated pathway-associated colorectal tumors. Hum. Pathol. 2015, 46, 643–656. [Google Scholar] [CrossRef] [PubMed]
- Krishn, S.R.; Kaur, S.; Sheinin, Y.M.; Smith, L.M.; Gautam, S.K.; Patel, A.; Jain, M.; Juvvigunta, V.; Pai, P.; Lazenby, A.J.; et al. Mucins and associated O-glycans based immunoprofile for stratification of colorectal polyps: Clinical implication for improved colon surveillance. Oncotarget 2017, 8, 7025–7038. [Google Scholar] [CrossRef] [Green Version]
- Rossez, Y.; Burtea, C.; Laurent, S.; Gosset, P.; Léonard, R.; Gonzalez, W.; Ballet, S.; Raynal, I.; Rousseaux, O.; Dugué, T.; et al. Early detection of colonic dysplasia by magnetic resonance molecular imaging with a contrast agent raised against the colon cancer marker MUC5AC. Contrast Media Mol. Imaging 2016, 11, 211–221. [Google Scholar] [CrossRef]
- Toribara, N.W.; Roberton, A.M.; Ho, S.B.; Kuo, W.L.; Gum, E.; Hicks, J.W.; Gum, J.R.; Byrd, J.C.; Siddiki, B.; Kim, Y.S. Human gastric mucin. Identification of a unique species by expression cloning. J. Biol. Chem. 1993, 268, 5879–5885. [Google Scholar] [CrossRef]
- Chik, J.H.; Zhou, J.; Moh, E.S.; Christopherson, R.; Clarke, S.J.; Molloy, M.P.; Packer, N.H. Comprehensive glycomics comparison between colon cancer cell cultures and tumours: Implications for biomarker studies. J. Proteom. 2014, 108, 146–162. [Google Scholar] [CrossRef]
- Owens, S.R.; Chiosea, S.I.; Kuan, S.F. Selective expression of gastric mucin MUC6 in colonic sessile serrated adenoma but not in hyperplastic polyp aids in morphological diagnosis of serrated polyps. Mod. Pathol. 2008, 21, 660–669. [Google Scholar] [CrossRef] [Green Version]
- Bartley, A.N.; Thompson, P.A.; Buckmeier, J.A.; Kepler, C.Y.; Hsu, C.H.; Snyder, M.S.; Lance, P.; Bhattacharyya, A.; Hamilton, S.R. Expression of gastric pyloric mucin, MUC6, in colorectal serrated polyps. Mod. Pathol. 2010, 23, 169–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, S.J.; McGuckin, M.A.; Gotley, D.C.; Eyre, H.J.; Sutherland, G.R.; Antalis, T.M. Two novel mucin genes down-regulated in colorectal cancer identified by differential display. Cancer Res. 1999, 59, 4083–4089. [Google Scholar] [PubMed]
- Packer, L.M.; Williams, S.J.; Callaghan, S.; Gotley, D.C.; McGuckin, M.A. Expression of the cell surface mucin gene family in adenocarcinomas. Int. J. Oncol. 2004, 25, 1119–1126. [Google Scholar] [PubMed]
- Aziz, M.A.; AlOtaibi, M.; AlAbdulrahman, A.; AlDrees, M.; AlAbdulkarim, I. Mucin Family Genes are Downregulated in Colorectal Cancer Patients. J. Carcinog. Mutagen. 2014, S10, 009. [Google Scholar] [CrossRef] [Green Version]
- Iranmanesh, H.; Majd, A.; Nazemalhosseini Mojarad, E.; Zali, M.R.; Hashemi, M. Investigating the Relationship between the Expression Level of Membrane-Bound Mucin (MUC12) and Clinicopathological Characterization of Colorectal Cancer. Arch. Adv. Biosci. 2021, 12, 31–36. [Google Scholar]
- Pham, E.; Friedrich, M.; Aeffner, F.; Lutteropp, M.; Mariano, N.F.; Deegen, P.; Dahlhoff, C.; Vogel, F.; Bluemel, C.; Harrold, J.M.; et al. Preclinical Assessment of a MUC12-Targeted BiTE (Bispecific T-cell Engager) Molecule. Mol. Cancer Ther. 2021, 20, 1977–1987. [Google Scholar] [CrossRef]
- Wu, Z.; Liu, Z.; Ge, W.; Shou, J.; You, L.; Pan, H.; Han, W. Analysis of potential genes and pathways associated with the colorectal normal mucosa-adenoma-carcinoma sequence. Cancer Med. 2018, 7, 2555–2566. [Google Scholar] [CrossRef]
- Matsuyama, T.; Ishikawa, T.; Mogushi, K.; Yoshida, T.; Iida, S.; Uetake, H.; Mizushima, H.; Tanaka, H.; Sugihara, K. MUC12 mRNA expression is an independent marker of prognosis in stage II and stage III colorectal cancer. Int. J. Cancer 2010, 127, 2292–2299. [Google Scholar] [CrossRef]
- Williams, S.J.; Wreschner, D.H.; Tran, M.; Eyre, H.J.; Sutherland, G.R.; McGuckin, M.A. Muc13, a novel human cell surface mucin expressed by epithelial and hemopoietic cells. J. Biol. Chem. 2001, 276, 18327–18336. [Google Scholar] [CrossRef] [Green Version]
- Walsh, M.D.; Young, J.P.; Leggett, B.A.; Williams, S.H.; Jass, J.R.; McGuckin, M.A. The MUC13 cell surface mucin is highly expressed by human colorectal carcinomas. Hum. Pathol. 2007, 38, 883–892. [Google Scholar] [CrossRef]
- Gupta, B.K.; Maher, D.M.; Ebeling, M.C.; Sundram, V.; Koch, M.D.; Lynch, D.W.; Bohlmeyer, T.; Watanabe, A.; Aburatani, H.; Puumala, S.E.; et al. Increased expression and aberrant localization of mucin 13 in metastatic colon cancer. J. Histochem. Cytochem. 2012, 60, 822–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, B.K.; Maher, D.M.; Ebeling, M.C.; Stephenson, P.D.; Puumala, S.E.; Koch, M.R.; Aburatani, H.; Jaggi, M.; Chauhan, S.C. Functions and regulation of MUC13 mucin in colon cancer cells. J. Gastroenterol. 2014, 49, 1378–1391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheng, Y.H.; Wong, K.Y.; Seim, I.; Wang, R.; He, Y.; Wu, A.; Patrick, M.; Lourie, R.; Schreiber, V.; Giri, R.; et al. MUC13 promotes the development of colitis-associated colorectal tumors via β-catenin activity. Oncogene 2019, 38, 7294–7310. [Google Scholar] [CrossRef] [PubMed]
- Sojka, L.; Opattova, A.; Bartu, L.; Horak, J.; Korenkova, V.; Novosadova, V.; Krizkova, V.; Bruha, J.; Liska, V.; Schneiderova, M.; et al. MUC13-miRNA-4647 axis in colorectal cancer: Prospects to identifications of risk factors and clinical outcomes. Oncol. Lett. 2023, 25, 72. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, I.S.; O’Connell, E.; Fichtner, M.; McNamara, D.A.; Kay, E.W.; Prehn, J.H.M.; Furney, S.J.; Burke, J.P. Mucinous adenocarcinoma of the colon and rectum: A genomic analysis. J. Surg. Oncol. 2019, 120, 1427–1435. [Google Scholar] [CrossRef] [PubMed]
- Pallesen, L.T.; Berglund, L.; Rasmussen, L.K.; Petersen, T.E.; Rasmussen, J.T. Isolation and characterization of MUC15, a novel cell membrane-associated mucin. Eur. J. Biochem. 2002, 269, 2755–2763. [Google Scholar] [CrossRef]
- Huang, J.; Che, M.I.; Huang, Y.T.; Shyu, M.K.; Huang, Y.M.; Wu, Y.M.; Lin, W.C.; Huang, P.H.; Liang, J.T.; Lee, P.H.; et al. Overexpression of MUC15 activates extracellular signal-regulated kinase 1/2 and promotes the oncogenic potential of human colon cancer cells. Carcinogenesis 2009, 30, 1452–1458. [Google Scholar] [CrossRef] [Green Version]
- Iranmanesh, H.; Entezari, M.; Rejali, L.; Nazemalhosseini-Mojarad, E.; Maghsoudloo, M.; Aghdaei, H.A.; Zali, M.R.; Hushmandi, K.; Rabiee, N.; Makvandi, P.; et al. The association of clinicopathological characterizations of colorectal cancer with membrane-bound mucins genes and LncRNAs. Pathol.-Res. Pract. 2022, 233, 153883. [Google Scholar] [CrossRef]
- Streppel, M.M.; Vincent, A.; Mukherjee, R.; Campbell, N.R.; Chen, S.H.; Konstantopoulos, K.; Goggins, M.G.; Van Seuningen, I.; Maitra, A.; Montgomery, E.A. Mucin 16 (cancer antigen 125) expression in human tissues and cell lines and correlation with clinical outcome in adenocarcinomas of the pancreas, esophagus, stomach, and colon. Hum. Pathol. 2012, 43, 1755–1763. [Google Scholar] [CrossRef] [Green Version]
- Ward, T.M.; Cauley, C.E.; Stafford, C.E.; Goldstone, R.N.; Bordeianou, L.G.; Kunitake, H.; Berger, D.L.; Ricciardi, R. Tumour genotypes account for survival differences in right- and left-sided colon cancers. Colorectal Dis 2022, 24, 601–610. [Google Scholar] [CrossRef]
- Björkman, K.; Mustonen, H.; Kaprio, T.; Haglund, C.; Böckelman, C. Mucin 16 and kallikrein 13 as potential prognostic factors in colon cancer: Results of an oncological 92-multiplex immunoassay. Tumour. Biol. 2019, 41, 1010428319860728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Gu, Y.; Li, X.; Zhou, L.; Cheng, X.; Jiang, H.; Huang, Y.; Zhang, Y.; Xu, T.; Yang, W.; et al. Mucin 16 Promotes Colorectal Cancer Development and Progression Through Activation of Janus Kinase 2. Dig. Dis. Sci. 2022, 67, 2195–2208. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.J.; Jiang, J.K.; Chang, S.C.; Lin, J.K.; Yang, S.H. Serum CA125 concentration as a predictor of peritoneal dissemination of colorectal cancer in men and women. Medicine (Baltimore) 2016, 95, e5177. [Google Scholar] [CrossRef]
- Giessen-Jung, C.; Nagel, D.; Glas, M.; Spelsberg, F.; Lau-Werner, U.; Modest, D.P.; Schulz, C.; Heinemann, V.; Di Gioia, D.; Stieber, P. Preoperative serum markers for individual patient prognosis in stage I-III colon cancer. Tumour Biol. 2015, 36, 7897–7906. [Google Scholar] [CrossRef]
- Björkman, K.; Mustonen, H.; Kaprio, T.; Kekki, H.; Pettersson, K.; Haglund, C.; Böckelman, C. CA125: A superior prognostic biomarker for colorectal cancer compared to CEA, CA19-9 or CA242. Tumour Biol. 2021, 43, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Senapati, S.; Ho, S.B.; Sharma, P.; Das, S.; Chakraborty, S.; Kaur, S.; Niehans, G.; Batra, S.K. Expression of intestinal MUC17 membrane-bound mucin in inflammatory and neoplastic diseases of the colon. J. Clin. Pathol. 2010, 63, 702–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolff, R.K.; Hoffman, M.D.; Wolff, E.C.; Herrick, J.S.; Sakoda, L.C.; Samowitz, W.S.; Slattery, M.L. Mutation analysis of adenomas and carcinomas of the colon: Early and late drivers. Genes Chromosomes Cancer 2018, 57, 366–376. [Google Scholar] [CrossRef]
- Luu, Y.; Junker, W.; Rachagani, S.; Das, S.; Batra, S.K.; Heinrikson, R.L.; Shekels, L.L.; Ho, S.B. Human intestinal MUC17 mucin augments intestinal cell restitution and enhances healing of experimental colitis. Int. J. Biochem. Cell Biol. 2010, 42, 996–1006. [Google Scholar] [CrossRef] [Green Version]
- Delker, D.A.; McGettigan, B.M.; Kanth, P.; Pop, S.; Neklason, D.W.; Bronner, M.P.; Burt, R.W.; Hagedorn, C.H. RNA sequencing of sessile serrated colon polyps identifies differentially expressed genes and immunohistochemical markers. PLoS ONE 2014, 9, e88367. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.; Du, L.; Chen, D.; Ye, Z.; Duan, H.; Tu, T.; Feng, J.; Yang, Y.; Chen, Q.; Yan, X. Reduced CD146 expression promotes tumorigenesis and cancer stemness in colorectal cancer through activating Wnt/β-catenin signaling. Oncotarget 2016, 7, 40704–40718. [Google Scholar] [CrossRef]
- Tian, B.; Xhang, Y.; Li, N. CD146 Protein as a Marker to Predict Postoperative Liver Metastasis in Colorectal Cancer. Cancer Biother. Radiopharm. 2013, 28, 466–470. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Di, J.; Wang, Z.; Gao, P.; Jiang, B.; Su, X. Genomic profiling of colorectal cancer with isolated lung metastasis. Cancer Cell Int. 2020, 20, 281. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; Wang, L.; Wei, P.; Chi, Y.; Li, D.; Wang, Q.; Ni, S.; Tan, C.; Sheng, W.; Sun, M.; et al. Role of MUC20 overexpression as a predictor of recurrence and poor outcome in colorectal cancer. J. Transl. Med. 2013, 11, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itoh, Y.; Kamata-Sakurai, M.; Denda-Nagai, K.; Nagai, S.; Tsuiji, M.; Ishii-Schrade, K.; Okada, K.; Goto, A.; Fukayama, M.; Irimura, T. Identification and expression of human epiglycanin/MUC21: A novel transmembrane mucin. Glycobiology 2008, 18, 74–83. [Google Scholar] [CrossRef] [PubMed]
- King, R.J.; Yu, F.; Singh, P.K. Genomic alterations in mucins across cancers. Oncotarget 2017, 8, 67152–67168. [Google Scholar] [CrossRef] [Green Version]
- Vymetalkova, V.; Pardini, B.; Rosa, F.; Jiraskova, K.; Di Gaetano, C.; Bendova, P.; Levy, M.; Veskrnova, V.; Buchler, T.; Vodickova, L.; et al. Polymorphisms in microRNA binding sites of mucin genes as predictors of clinical outcome in colorectal cancer patients. Carcinogenesis 2017, 38, 28–39. [Google Scholar] [CrossRef]
- Kim, D.H.; Shin, N.; Kim, G.H.; Song, G.A.; Jeon, T.Y.; Kim, D.H.; Lauwers, G.Y.; Park, D.Y. Mucin expression in gastric cancer: Reappraisal of its clinicopathologic and prognostic significance. Arch. Pathol. Lab. Med. 2013, 137, 1047–1053. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Cytogenetic Band | Form |
|---|---|---|
| MUC1 | 1q22 | Membrane-bound mucin |
| MUC2 | 11p15.5 | Secreted |
| MUC3 | 7q22 | Membrane-bound mucin |
| MUC4 | 3q29 | Membrane-bound mucin |
| MUC5AC | 11p15.5 | Secreted |
| MUC5B | 11p15.5 | Secreted |
| MUC6 | 11p15.5 | Secreted |
| MUC7 | 4q13.3 | Secreted |
| MUC8 | 12q24.33 | Secreted |
| MUC9 | 1p13.2 | Secreted |
| MUC12 | 7q22.1 | Membrane-bound mucin |
| MUC13 | 3q21.2 | Membrane-bound mucin |
| MUC14 | 4q24 | Membrane-bound mucin |
| MUC15 | 11p14.2 | Membrane-bound mucin |
| MUC16 | 19p13.2 | Membrane-bound mucin |
| MUC17 | 7q22.1 | Membrane-bound mucin |
| MUC18 | 11q23.3 | Membrane-bound mucin |
| MUC19 | 12q12 | Secreted |
| MUC20 | 3q29 | Membrane-bound mucin |
| MUC21 | 6p21.33 | Membrane-bound mucin |
| MUC22 | 6p21.33 | Membrane-bound mucin |
| MUC24 | 6q21 | Membrane-bound mucin |
| Normal Colon | HP | Adenoma | TSA | SSA | Study |
|---|---|---|---|---|---|
| - | 75.4% (49/65) | - | 43.1% (31/72) | 80.4% (41/51) | Fujita et al. [60] |
| 0% (0/9) | 20% (2/10) | 27% (8/30) | - | - | Krishn et al. [61] |
| 10.7% (3/28) | 100% (8/8) | 100% (19/19) | - | 100% (10/10) | Perçinel et al. [68] |
| 0% (0/26) | 11% (1/9) | 24% (6/25) | - | - | Bartman et al. [84] |
| 0% (0/18) | 43.4% (23/53) | - | 31% (5/16) | 61% (19/31) | Kim et al. [87] |
| - | 15.2% (5/33) | 8.3% (3/36) | - | 61.5% (24/39) | Krishn et al. [88] |
| HP | Adenoma | SSA | Study |
|---|---|---|---|
| 16.9% (11/65) | - | 39.2% (20/51) | Fujita et al. [60] |
| - | 10% (1/10) | - | Krishn et al. [61] |
| - | 15.8% (3/19) | 20% (2/10) | Perçinel et al. [68] |
| 0% (0/9) | 16% (4/25) | - | Bartman et al. [84] |
| 4.3% (1/23) | 0% (0/63) | 51.6% (16/31) | Kim et al. [87] |
| 0% (0/48) | - | 100% (26/26) | Owens et al. [92] |
| 17.4% (16/92) | 0% (0/87) | 53.5% (23/43) | Bartley et al. [93] |
| Study | Sample Size | 5-Year Survival | p-Value |
|---|---|---|---|
| Björkman et al. 2019 [113] | 148 | 75.3% (low expression) vs. 50.7% (high expression) | <0.001 |
| Giessen-Jung et al. [116] | 472 | 87.1% (elevated MUC16) vs. 84.9% (overall) | 0.3114 |
| Björkman et al. 2020 [117] | 282 | 66.7% (low expression) vs. 41.1% (high expression) | <0.001 |
| Study | Sample Size | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|---|
| Ward et al. [112] | 420 | 2.06 | 1.51–8.14 | 0.011 |
| Björkman et al. 2019 [113] | 148 | 1.91 | 1.45–2.53 | <0.001 |
| Björkman et al. 2020 [117] | 282 | 2.48 | 1.68–3.65 | <0.001 |
| Mucin and Level | Subset of CRC | HR | 95% CI | p-Value | Study |
|---|---|---|---|---|---|
| High MUC1 | 1.51 | 1.30–1.75 | <0.00001 | Li et al. [49] | |
| Loss of MUC2 | Stage II | 3.32 | 1.20–9.20 | 0.021 | Cecchini et al. [64] |
| Low MUC2 | 1.67 | 1.43–1.94 | <0.00001 | Li et al. [65] | |
| High MUC4 | 2.07 | 1.14–3.75 | 0.017 | Shanmugam et al. [78] | |
| High MUC4 | Stage I and II | 3.77 | 1.46–9.73 | 0.006 | Shanmugam et al. [78] |
| High MUC16 | 2.06 | 1.51–8.14 | 0.011 | Ward et al. [112] | |
| High MUC16 | 1.91 | 1.45–2.53 | <0.001 | Björkman et al. [113] | |
| High MUC16 | 2.48 | 1.68–3.65 | <0.001 | Björkman et al. [117] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cox, K.E.; Liu, S.; Lwin, T.M.; Hoffman, R.M.; Batra, S.K.; Bouvet, M. The Mucin Family of Proteins: Candidates as Potential Biomarkers for Colon Cancer. Cancers 2023, 15, 1491. https://doi.org/10.3390/cancers15051491
Cox KE, Liu S, Lwin TM, Hoffman RM, Batra SK, Bouvet M. The Mucin Family of Proteins: Candidates as Potential Biomarkers for Colon Cancer. Cancers. 2023; 15(5):1491. https://doi.org/10.3390/cancers15051491
Chicago/Turabian StyleCox, Kristin E., Shanglei Liu, Thinzar M. Lwin, Robert M. Hoffman, Surinder K. Batra, and Michael Bouvet. 2023. "The Mucin Family of Proteins: Candidates as Potential Biomarkers for Colon Cancer" Cancers 15, no. 5: 1491. https://doi.org/10.3390/cancers15051491