
Pediatric Myeloid Sarcoma, More than Just a Chloroma: A Review of Clinical Presentations, Significance, and Biology

Abstract
:Simple Summary
Abstract
1. Introduction
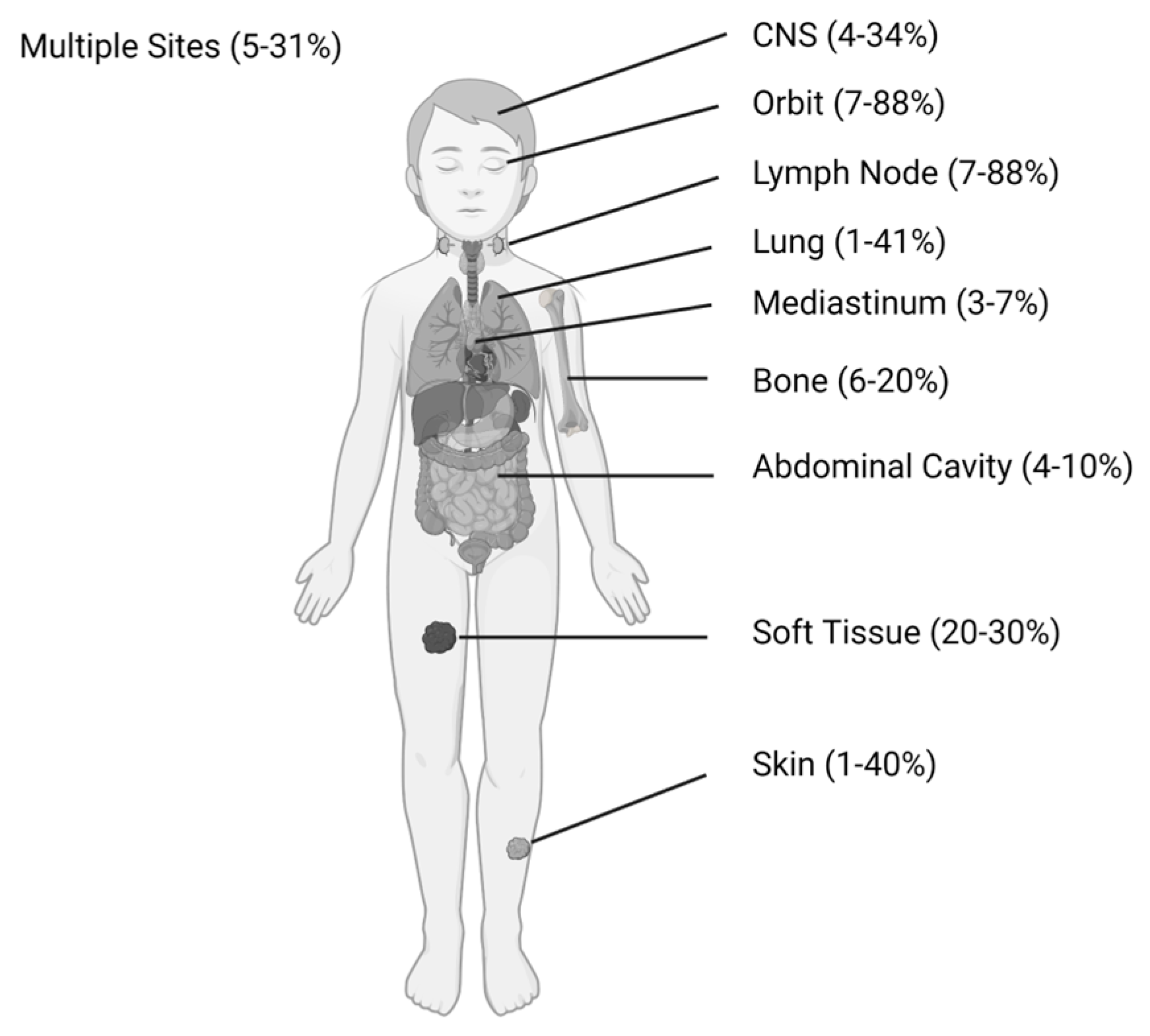
2. Pediatric Clinical Presentation, Incidence, and Outcomes
2.1. Incidence
2.2. Clinical Associations
2.3. Outcomes
3. Significance of Extramedullary Disease and Myeloid Sarcomas Post-Allogeneic Hematopoietic Stem Cell Transplant
4. Imaging Evaluation of Myeloid Sarcomas
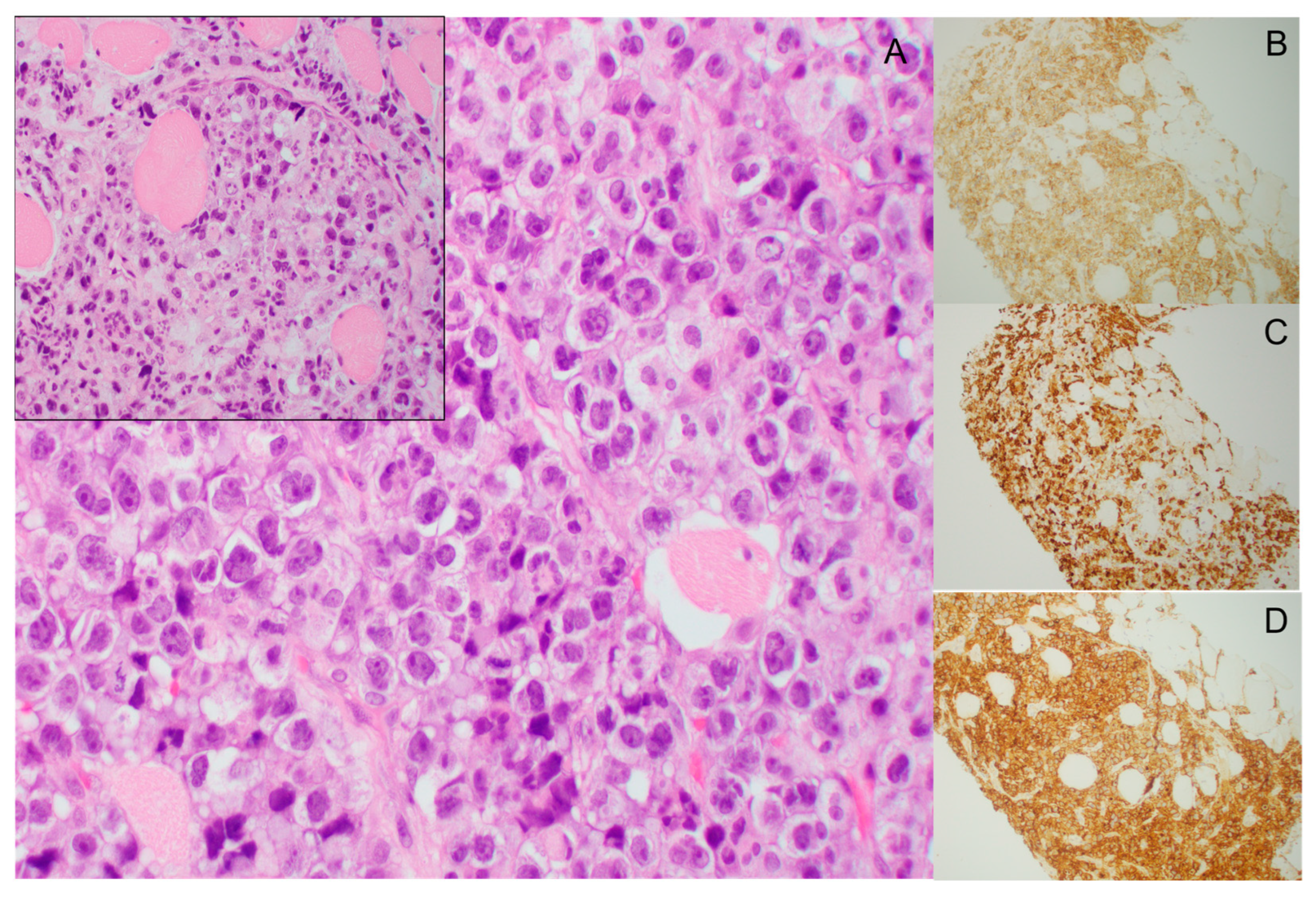
5. Pathology of Myeloid Sarcomas
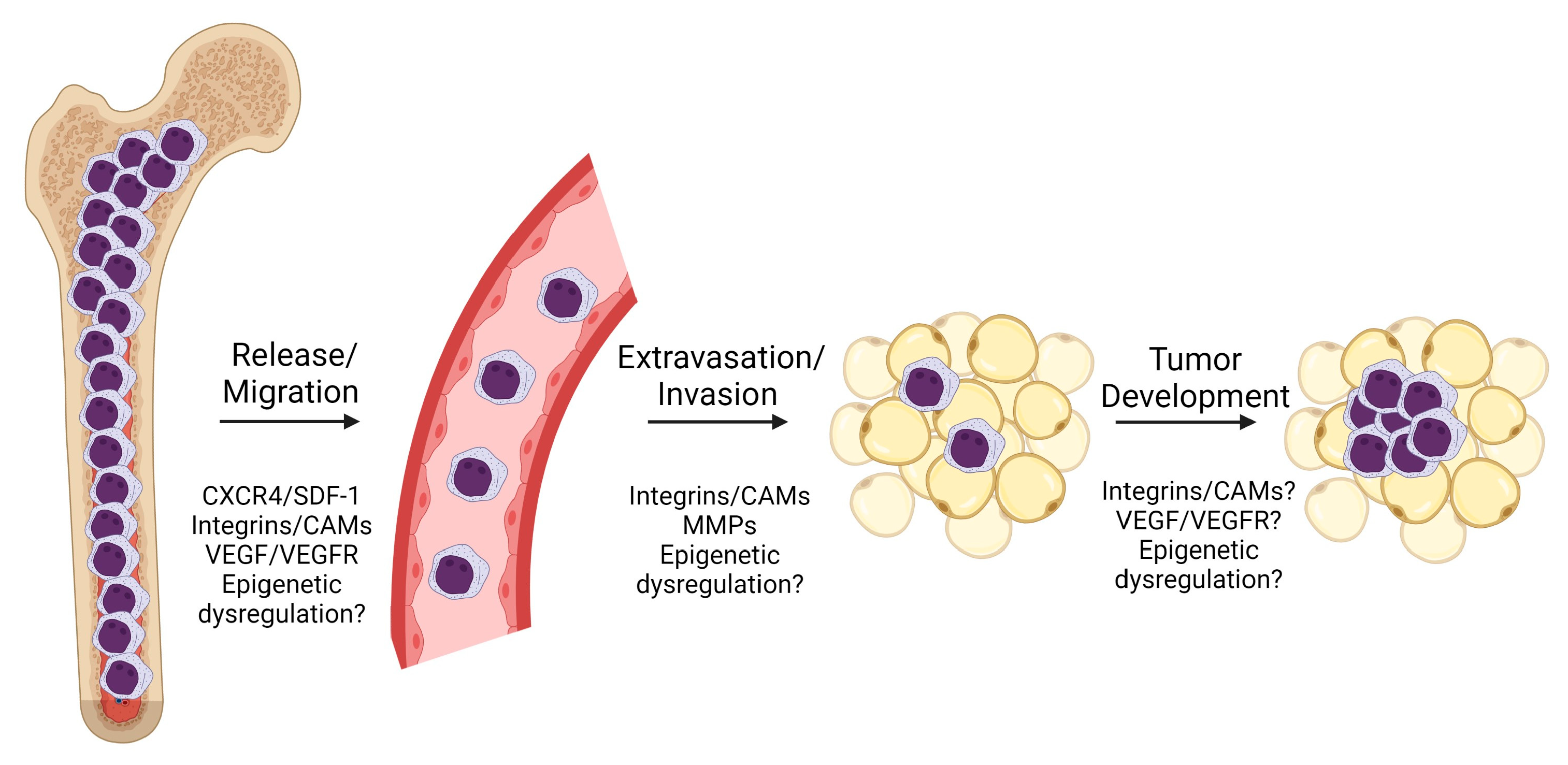
6. Biological Understandings of Pathogenesis
6.1. CXCR4
6.2. CD56
6.3. Integrins and Cell Adhesion Molecules (CAMs)
6.4. Vascular Endothelial Growth Factor (VEGF) and Receptor (VEGFR)
6.5. Matrix Metalloproteinases (MMP)
6.6. Epigenetic Dysregulation
6.7. Other Biological Associations
7. Treatment Considerations
8. Conclusions: Knowledge Gaps and Areas for Improvement
Author Contributions
Funding
Conflicts of Interest
References
- Wilson, C.S.; Medeiros, L.J. Extramedullary Manifestations of Myeloid Neoplasms. Am. J. Clin. Pathol. 2015, 144, 219–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campidelli, C.; Agostinelli, C.; Stitson, R.; Pileri, S.A. Myeloid sarcoma: Extramedullary manifestation of myeloid disorders. Am. J. Clin. Pathol. 2009, 132, 426–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef]
- Pileri, S.A.; Ascani, S.; Cox, M.C.; Campidelli, C.; Bacci, F.; Piccioli, M.; Piccaluga, P.P.; Agostinelli, C.; Asioli, S.; Novero, D.; et al. Myeloid sarcoma: Clinico-pathologic, phenotypic and cytogenetic analysis of 92 adult patients. Leukemia 2007, 21, 340–350. [Google Scholar] [CrossRef] [PubMed]
- De Rooij, J.D.; Zwaan, C.M.; van den Heuvel-Eibrink, M. Pediatric AML: From Biology to Clinical Management. J. Clin. Med. 2015, 4, 127–149. [Google Scholar] [CrossRef] [Green Version]
- Shallis, R.M.; Wang, R.; Davidoff, A.; Ma, X.; Zeidan, A.M. Epidemiology of acute myeloid leukemia: Recent progress and enduring challenges. Blood Rev. 2019, 36, 70–87. [Google Scholar] [CrossRef]
- Bolouri, H.; Farrar, J.E.; Triche, T., Jr.; Ries, R.E.; Lim, E.L.; Alonzo, T.A.; Ma, Y.; Moore, R.; Mungall, A.J.; Marra, M.A.; et al. The molecular landscape of pediatric acute myeloid leukemia reveals recurrent structural alterations and age-specific mutational interactions. Nat. Med. 2018, 24, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Papaemmanuil, E.; Gerstung, M.; Bullinger, L.; Gaidzik, V.I.; Paschka, P.; Roberts, N.D.; Potter, N.E.; Heuser, M.; Thol, F.; Bolli, N.; et al. Genomic Classification and Prognosis in Acute Myeloid Leukemia. N. Engl. J. Med. 2016, 374, 2209–2221. [Google Scholar] [CrossRef]
- Ley, T.J.; Miller, C.; Ding, L.; Raphael, B.J.; Mungall, A.J.; Robertson, A.; Hoadley, K.; Triche, T.J., Jr.; Laird, P.W.; Baty, J.D.; et al. Genomic and epigenomic landscapes of adult de novo acute myeloid leukemia. N. Engl. J. Med. 2013, 368, 2059–2074. [Google Scholar] [CrossRef] [Green Version]
- Chang, M.; Raimondi, S.C.; Ravindranath, Y.; Carroll, A.J.; Camitta, B.; Gresik, M.V.; Steuber, C.P.; Weinstein, H. Prognostic factors in children and adolescents with acute myeloid leukemia (excluding children with Down syndrome and acute promyelocytic leukemia): Univariate and recursive partitioning analysis of patients treated on Pediatric Oncology Group (POG) Study 8821. Leukemia 2000, 14, 1201–1207. [Google Scholar] [CrossRef] [Green Version]
- Bisschop, M.M.; Révész, T.; Bierings, M.; van Weerden, J.F.; van Wering, E.R.; Hählen, K.; van der Does-van den Berg, A. Extramedullary infiltrates at diagnosis have no prognostic significance in children with acute myeloid leukaemia. Leukemia 2001, 15, 46–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dusenbery, K.E.; Howells, W.B.; Arthur, D.C.; Alonzo, T.; Lee, J.W.; Kobrinsky, N.; Barnard, D.R.; Wells, R.J.; Buckley, J.D.; Lange, B.J.; et al. Extramedullary leukemia in children with newly diagnosed acute myeloid leukemia: A report from the Children’s Cancer Group. J. Pediatr. Hematol. Oncol. 2003, 25, 760–768. [Google Scholar] [CrossRef] [PubMed]
- Hiçsönmez, G.; Cetin, M.; Tuncer, A.M.; Yenicesu, I.; Aslan, D.; Ozyürek, E.; Unal, S. Children with acute myeloblastic leukemia presenting with extramedullary infiltration: The effects of high-dose steroid treatment. Leuk. Res. 2004, 28, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, R.; Tawa, A.; Hanada, R.; Horibe, K.; Tsuchida, M.; Tsukimoto, I. Extramedullary infiltration at diagnosis and prognosis in children with acute myelogenous leukemia. Pediatr. Blood Cancer 2007, 48, 393–398. [Google Scholar] [CrossRef]
- Johnston, D.L.; Alonzo, T.A.; Gerbing, R.B.; Lange, B.J.; Woods, W.G. Superior outcome of pediatric acute myeloid leukemia patients with orbital and CNS myeloid sarcoma: A report from the Children’s Oncology Group. Pediatr. Blood Cancer 2012, 58, 519–524. [Google Scholar] [CrossRef] [Green Version]
- Creutzig, U.; Dworzak, M.N.; Zimmermann, M.; Reinhardt, D.; Sramkova, L.; Bourquin, J.P.; Hasle, H.; Abrahamsson, J.; Kaspers, G.; van den Heuvel, M.M.; et al. Characteristics and outcome in patients with central nervous system involvement treated in European pediatric acute myeloid leukemia study groups. Pediatr. Blood Cancer 2017, 64, e26664. [Google Scholar] [CrossRef] [Green Version]
- Støve, H.K.; Sandahl, J.D.; Abrahamsson, J.; Asdahl, P.H.; Forestier, E.; Ha, S.Y.; Jahnukainen, K.; Jónsson, Ó.G.; Lausen, B.; Palle, J.; et al. Extramedullary leukemia in children with acute myeloid leukemia: A population-based cohort study from the Nordic Society of Pediatric Hematology and Oncology (NOPHO). Pediatr. Blood Cancer 2017, 64, e26520. [Google Scholar] [CrossRef] [Green Version]
- Pramanik, R.; Tyagi, A.; Chopra, A.; Kumar, A.; Vishnubhatla, S.; Bakhshi, S. Myeloid Sarcoma Predicts Superior Outcome in Pediatric AML; Can Cytogenetics Solve the Puzzle? Clin. Lymphoma Myeloma Leuk. 2018, 18, e249–e254. [Google Scholar] [CrossRef]
- Xu, L.H.; Wang, Y.; Chen, Z.Y.; Fang, J.P. Myeloid sarcoma is associated with poor clinical outcome in pediatric patients with acute myeloid leukemia. J. Cancer Res. Clin. Oncol. 2020, 146, 1011–1020. [Google Scholar] [CrossRef]
- Lee, J.W.; Kim, S.; Jang, P.S.; Chung, N.G.; Cho, B.; Im, S.A.; Kim, M. Prognostic Role of Postinduction Minimal Residual Disease and Myeloid Sarcoma Type Extramedullary Involvement in Pediatric RUNX1-RUNX1T1 (+) Acute Myeloid Leukemia. J. Pediatr. Hematol. Oncol. 2020, 42, e132–e139. [Google Scholar] [CrossRef]
- Hu, G.H.; Lu, A.D.; Jia, Y.P.; Zuo, Y.X.; Wu, J.; Zhang, L.P. Prognostic Impact of Extramedullary Infiltration in Pediatric Low-risk Acute Myeloid Leukemia: A Retrospective Single-center Study Over 10 Years. Clin. Lymphoma Myeloma Leuk. 2020, 20, e813–e820. [Google Scholar] [CrossRef] [PubMed]
- Hu, G.; Lu, A.; Wu, J.; Jia, Y.; Zuo, Y.; Ding, M.; Zhang, L. Characteristics and prognosis of pediatric myeloid sarcoma in the cytogenetic context of t(8;21). Pediatr. Hematol. Oncol. 2021, 38, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Samborska, M.; Barańska, M.; Wachowiak, J.; Skalska-Sadowska, J.; Thambyrajah, S.; Czogała, M.; Balwierz, W.; Kołtan, S.; Peszyńska-Żelazny, K.; Wysocki, M.; et al. Clinical Characteristics and Treatment Outcomes of Myeloid Sarcoma in Children: The Experience of the Polish Pediatric Leukemia and Lymphoma Study Group. Front. Oncol. 2022, 12, 935373. [Google Scholar] [CrossRef] [PubMed]
- Stölzel, F.; Lüer, T.; Löck, S.; Parmentier, S.; Kuithan, F.; Kramer, M.; Alakel, N.S.; Sockel, K.; Taube, F.; Middeke, J.M.; et al. The prevalence of extramedullary acute myeloid leukemia detected by 18FDG-PET/CT: Final results from the prospective PETAML trial. Haematologica 2020, 105, 1552–1558. [Google Scholar] [CrossRef] [Green Version]
- Xin, X.; Zhu, H.; Chang, Z.; Feng, M.; Gao, S.; Hou, L.; Su, X. Risk factors and prognosis analysis of acute myeloid leukemia in children. J. Balk. Union Oncol. 2021, 26, 166–172. [Google Scholar]
- Zhou, T.; Bloomquist, M.S.; Ferguson, L.S.; Reuther, J.; Marcogliese, A.N.; Elghetany, M.T.; Roy, A.; Rao, P.H.; Lopez-Terrada, D.H.; Redell, M.S.; et al. Pediatric myeloid sarcoma: A single institution clinicopathologic and molecular analysis. Pediatr. Hematol. Oncol. 2020, 37, 76–89. [Google Scholar] [CrossRef]
- Eckardt, J.N.; Stölzel, F.; Kunadt, D.; Röllig, C.; Stasik, S.; Wagenführ, L.; Jöhrens, K.; Kuithan, F.; Krämer, A.; Scholl, S.; et al. Molecular profiling and clinical implications of patients with acute myeloid leukemia and extramedullary manifestations. J. Hematol. Oncol. 2022, 15, 60. [Google Scholar] [CrossRef]
- Sakaguchi, H.; Miyamura, T.; Tomizawa, D.; Taga, T.; Ishida, H.; Okamoto, Y.; Koh, K.; Yokosuka, T.; Yoshida, N.; Sato, M.; et al. Effect of extramedullary disease on allogeneic hematopoietic cell transplantation for pediatric acute myeloid leukemia: A nationwide retrospective study. Bone Marrow Transplant. 2021, 56, 1859–1865. [Google Scholar] [CrossRef]
- Hazar, V.; Öztürk, G.; Yalçın, K.; Uygun, V.; Aksoylar, S.; Küpesiz, A.; Ok Bozkaya, İ.; Karagün, B.; Bozkurt, C.; İleri, T.; et al. Different Kinetics and Risk Factors for Isolated Extramedullary Relapse after Allogeneic Hematopoietic Stem Cell Transplantation in Children with Acute Leukemia. Transplant Cell Ther 2021, 27, 859.e1–859.e10. [Google Scholar] [CrossRef]
- Harris, A.C.; Kitko, C.L.; Couriel, D.R.; Braun, T.M.; Choi, S.W.; Magenau, J.; Mineishi, S.; Pawarode, A.; Yanik, G.; Levine, J.E. Extramedullary relapse of acute myeloid leukemia following allogeneic hematopoietic stem cell transplantation: Incidence, risk factors and outcomes. Haematologica 2013, 98, 179–184. [Google Scholar] [CrossRef]
- Shem-Tov, N.; Saraceni, F.; Danylesko, I.; Shouval, R.; Yerushalmi, R.; Nagler, A.; Shimoni, A. Isolated Extramedullary Relapse of Acute Leukemia after Allogeneic Stem Cell Transplantation: Different Kinetics and Better Prognosis than Systemic Relapse. Biol. Blood Marrow Transplant. 2017, 23, 1087–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyal, S.D.; Zhang, M.J.; Wang, H.L.; Akpek, G.; Copelan, E.A.; Freytes, C.; Gale, R.P.; Hamadani, M.; Inamoto, Y.; Kamble, R.T.; et al. Allogeneic hematopoietic cell transplant for AML: No impact of pre-transplant extramedullary disease on outcome. Bone Marrow Transplant. 2015, 50, 1057–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourlon, C.; Lipton, J.H.; Deotare, U.; Gupta, V.; Kim, D.D.; Kuruvilla, J.; Viswabandya, A.; Thyagu, S.; Messner, H.A.; Michelis, F.V. Extramedullary disease at diagnosis of AML does not influence outcome of patients undergoing allogeneic hematopoietic cell transplant in CR1. Eur. J. Haematol. 2017, 99, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Frietsch, J.J.; Hunstig, F.; Wittke, C.; Junghanss, C.; Franiel, T.; Scholl, S.; Hochhaus, A.; Hilgendorf, I. Extra-medullary recurrence of myeloid leukemia as myeloid sarcoma after allogeneic stem cell transplantation: Impact of conditioning intensity. Bone Marrow Transplant. 2021, 56, 101–109. [Google Scholar] [CrossRef]
- Huang, Q.; Reddi, D.; Chu, P.; Snyder, D.S.; Weisenburger, D.D. Clinical and pathologic analysis of extramedullary tumors after hematopoietic stem cell transplantation. Hum. Pathol. 2014, 45, 2404–2410. [Google Scholar] [CrossRef]
- Shimizu, H.; Saitoh, T.; Hatsumi, N.; Takada, S.; Handa, H.; Jimbo, T.; Sakura, T.; Miyawaki, S.; Nojima, Y. Prevalence of extramedullary relapses is higher after allogeneic stem cell transplantation than after chemotherapy in adult patients with acute myeloid leukemia. Leuk. Res. 2013, 37, 1477–1481. [Google Scholar] [CrossRef]
- Solh, M.; DeFor, T.E.; Weisdorf, D.J.; Kaufman, D.S. Extramedullary relapse of acute myelogenous leukemia after allogeneic hematopoietic stem cell transplantation: Better prognosis than systemic relapse. Biol. Blood Marrow Transplant. 2012, 18, 106–112. [Google Scholar] [CrossRef] [Green Version]
- Kikushige, Y.; Takase, K.; Sata, K.; Aoki, K.; Numata, A.; Miyamoto, T.; Fukuda, T.; Gondo, H.; Harada, M.; Nagafuji, K. Repeated relapses of acute myelogenous leukemia in the isolated extramedullary sites following allogeneic bone marrow transplantations. Intern. Med. 2007, 46, 1011–1014. [Google Scholar] [CrossRef] [Green Version]
- Ando, T.; Mitani, N.; Matsui, K.; Yamashita, K.; Nomiyama, J.; Tsuru, M.; Yujiri, T.; Tanizawa, Y. Recurrent extramedullary relapse of acute myelogenous leukemia after allogeneic hematopoietic stem cell transplantation in a patient with the chromosomal abnormality t(8;21) and CD56-positivity. Int. J. Hematol. 2009, 90, 374–377. [Google Scholar] [CrossRef]
- Ando, T.; Mitani, N.; Matsunaga, K.; Nakazora, T.; Gondo, T.; Yujiri, T.; Tanizawa, Y. Gemtuzumab ozogamicin therapy for isolated extramedullary AML relapse after allogeneic hematopoietic stem-cell transplantation. Tohoku J. Exp. Med. 2010, 220, 121–126. [Google Scholar] [CrossRef] [Green Version]
- Shan, M.; Lu, Y.; Yang, M.; Wang, P.; Lu, S.; Zhang, L.; Qiu, H.; Chen, S.; Xu, Y.; Zhang, X.; et al. Characteristics and transplant outcome of myeloid sarcoma: A single-institute study. Int. J. Hematol. 2021, 113, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Im, S.A.; Lee, J.H.; Lee, J.W.; Chung, N.G.; Cho, B. Extramedullary Relapse of Acute Myeloid and Lymphoid Leukemia in Children: A Retrospective Analysis. Iran. J. Pediatr. 2016, 26, e1711. [Google Scholar] [CrossRef] [PubMed]
- Meyer, H.J.; Beimler, M.; Borte, G.; Pönisch, W.; Surov, A. Radiological and clinical patterns of myeloid sarcoma. Radiol. Oncol. 2019, 53, 213–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, E.Y.; Anthony, M.P.; Leung, A.Y.; Loong, F.; Khong, P.L. Utility of FDG PET/CT in the assessment of myeloid sarcoma. Am. J. Roentgenol. 2012, 198, 1175–1179. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.L.; Wu, H.B.; Wang, L.J.; Tian, Y.; Dong, Y.; Wang, Q.S. Usefulness and pitfalls of F-18-FDG PET/CT for diagnosing extramedullary acute leukemia. Eur. J. Radiol. 2016, 85, 205–210. [Google Scholar] [CrossRef]
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues; IARC: Lyon, France, 2017; Volume 2. [Google Scholar]
- Greenland, N.Y.; Van Ziffle, J.A.; Liu, Y.C.; Qi, Z.; Prakash, S.; Wang, L. Genomic analysis in myeloid sarcoma and comparison with paired acute myeloid leukemia. Hum. Pathol. 2021, 108, 76–83. [Google Scholar] [CrossRef]
- Li, Z.; Stölzel, F.; Onel, K.; Sukhanova, M.; Mirza, M.K.; Yap, K.L.; Borinets, O.; Larson, R.A.; Stock, W.; Sasaki, M.M.; et al. Next-generation sequencing reveals clinically actionable molecular markers in myeloid sarcoma. Leukemia 2015, 29, 2113–2116. [Google Scholar] [CrossRef] [Green Version]
- Du, W.; Lu, C.; Zhu, X.; Hu, D.; Chen, X.; Li, J.; Liu, W.; Zhu, J.; He, Y.; Yao, J. Prognostic significance of CXCR4 expression in acute myeloid leukemia. Cancer Med. 2019, 8, 6595–6603. [Google Scholar] [CrossRef] [Green Version]
- Chou, S.H.; Ko, B.S.; Chiou, J.S.; Hsu, Y.C.; Tsai, M.H.; Chiu, Y.C.; Yu, I.S.; Lin, S.W.; Hou, H.A.; Kuo, Y.Y.; et al. A knock-in Npm1 mutation in mice results in myeloproliferation and implies a perturbation in hematopoietic microenvironment. PLoS ONE 2012, 7, e49769. [Google Scholar] [CrossRef]
- Peled, A.; Klein, S.; Beider, K.; Burger, J.A.; Abraham, M. Role of CXCL12 and CXCR4 in the pathogenesis of hematological malignancies. Cytokine 2018, 109, 11–16. [Google Scholar] [CrossRef]
- Crazzolara, R.; Kreczy, A.; Mann, G.; Heitger, A.; Eibl, G.; Fink, F.M.; Möhle, R.; Meister, B. High expression of the chemokine receptor CXCR4 predicts extramedullary organ infiltration in childhood acute lymphoblastic leukaemia. Br. J. Haematol. 2001, 115, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Shuai, X.; Ye, Y.; Jin, Y.; Jiang, N.; Chen, X.; Su, J. The role of polymorphisms of stromal-derived factor-1 and CXC receptor 4 in acute myeloid leukemia and leukemia cell dissemination. Gene 2016, 588, 103–108. [Google Scholar] [CrossRef]
- Faaij, C.M.; Willemze, A.J.; Révész, T.; Balzarolo, M.; Tensen, C.P.; Hoogeboom, M.; Vermeer, M.H.; van Wering, E.; Zwaan, C.M.; Kaspers, G.J.; et al. Chemokine/chemokine receptor interactions in extramedullary leukaemia of the skin in childhood AML: Differential roles for CCR2, CCR5, CXCR4 and CXCR7. Pediatr. Blood Cancer 2010, 55, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Ponziani, V.; Mannelli, F.; Bartalucci, N.; Gianfaldoni, G.; Leoni, F.; Antonioli, E.; Guglielmelli, P.; Ciolli, S.; Bosi, A.; Vannucchi, A.M. No role for CXCL12-G801A polymorphism in the development of extramedullary disease in acute myeloid leukemia. Leukemia 2008, 22, 669–671. [Google Scholar] [CrossRef]
- Chang, H.; Brandwein, J.; Yi, Q.L.; Chun, K.; Patterson, B.; Brien, B. Extramedullary infiltrates of AML are associated with CD56 expression, 11q23 abnormalities and inferior clinical outcome. Leuk. Res. 2004, 28, 1007–1011. [Google Scholar] [CrossRef] [PubMed]
- Deeb, G.; Baer, M.R.; Gaile, D.P.; Sait, S.N.; Barcos, M.; Wetzler, M.; Conroy, J.M.; Nowak, N.J.; Cowell, J.K.; Cheney, R.T. Genomic profiling of myeloid sarcoma by array comparative genomic hybridization. Genes Chromosomes Cancer 2005, 44, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Park, S.S.; Yoon, J.H.; Kim, H.J.; Jeon, Y.W.; Lee, S.E.; Cho, B.S.; Eom, K.S.; Kim, Y.J.; Lee, S.; Min, C.K.; et al. Characteristics and Survival Outcome Analysis of Extramedullary Involvement in Adult Patients with t(8;21) Acute Myeloid Leukemia. Clin. Lymphoma Myeloma Leuk. 2017, 17, 38–45.e32. [Google Scholar] [CrossRef]
- Alegretti, A.P.; Bittar, C.M.; Bittencourt, R.; Piccoli, A.K.; Schneider, L.; Silla, L.M.; Bó, S.D.; Xavier, R.M. The expression of CD56 antigen is associated with poor prognosis in patients with acute myeloid leukemia. Rev. Bras. Hematol. Hemoter. 2011, 33, 202–206. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, N.; Oda, T.; Takizawa, M.; Ishizaki, T.; Tsukamoto, N.; Yokohama, A.; Takei, H.; Saitoh, T.; Shimizu, H.; Honma, K.; et al. Integrin α7 and Extracellular Matrix Laminin 211 Interaction Promotes Proliferation of Acute Myeloid Leukemia Cells and Is Associated with Granulocytic Sarcoma. Cancers 2020, 12, 363. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.N.; Ruan, Y.; Ogana, H.; Kim, Y.M. Cadherins, Selectins, and Integrins in CAM-DR in Leukemia. Front. Oncol. 2020, 10, 592733. [Google Scholar] [CrossRef]
- Valent, P.; Sadovnik, I.; Eisenwort, G.; Herrmann, H.; Bauer, K.; Mueller, N.; Sperr, W.R.; Wicklein, D.; Schumacher, U. Redistribution, homing and organ-invasion of neoplastic stem cells in myeloid neoplasms. Semin. Cancer Biol. 2020, 60, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Piccaluga, P.P.; Paolini, S.; Navari, M.; Etebari, M.; Visani, G.; Ascani, S. Increased angiogenesis seems to correlate with inferior overall survival in myeloid sarcoma patients. Pol. J. Pathol. 2018, 69, 254–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuch, G.; Machluf, M.; Bartsch, G., Jr.; Nomi, M.; Richard, H.; Atala, A.; Soker, S. In vivo administration of vascular endothelial growth factor (VEGF) and its antagonist, soluble neuropilin-1, predicts a role of VEGF in the progression of acute myeloid leukemia in vivo. Blood 2002, 100, 4622–4628. [Google Scholar] [CrossRef] [Green Version]
- Pillozzi, S.; Brizzi, M.F.; Bernabei, P.A.; Bartolozzi, B.; Caporale, R.; Basile, V.; Boddi, V.; Pegoraro, L.; Becchetti, A.; Arcangeli, A. VEGFR-1 (FLT-1), beta1 integrin, and hERG K+ channel for a macromolecular signaling complex in acute myeloid leukemia: Role in cell migration and clinical outcome. Blood 2007, 110, 1238–1250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, M.; Zha, J.; Zhao, H.; Jia, X.; Shi, Y.; Li, Z.; Fu, G.; Yu, L.; Fang, Z.; Xu, B. Apatinib exhibits cytotoxicity toward leukemia cells by targeting VEGFR2-mediated prosurvival signaling and angiogenesis. Exp. Cell Res. 2020, 390, 111934. [Google Scholar] [CrossRef]
- Xian, J.; Shao, H.; Chen, X.; Zhang, S.; Quan, J.; Zou, Q.; Jin, H.; Zhang, L. Nucleophosmin Mutants Promote Adhesion, Migration and Invasion of Human Leukemia THP-1 Cells through MMPs Up-regulation via Ras/ERK MAPK Signaling. Int. J. Biol. Sci. 2016, 12, 144–155. [Google Scholar] [CrossRef] [Green Version]
- Song, J.H.; Kim, S.H.; Cho, D.; Lee, I.K.; Kim, H.J.; Kim, T.S. Enhanced invasiveness of drug-resistant acute myeloid leukemia cells through increased expression of matrix metalloproteinase-2. Int. J. Cancer 2009, 125, 1074–1081. [Google Scholar] [CrossRef]
- Wang, C.; Cai, X.; Chen, B.; He, Z.; Chen, Z.; Cen, J.; Li, Z. Up-regulation of tissue inhibitor of metalloproteinase-2 promotes SHI-1 cell invasion in nude mice. Leuk. Lymphoma 2013, 54, 2707–2711. [Google Scholar] [CrossRef]
- Wang, C.; Chen, Z.; Li, Z.; Cen, J. The essential roles of matrix metalloproteinase-2, membrane type 1 metalloproteinase and tissue inhibitor of metalloproteinase-2 in the invasive capacity of acute monocytic leukemia SHI-1 cells. Leuk. Res. 2010, 34, 1083–1090. [Google Scholar] [CrossRef]
- Stefanidakis, M.; Karjalainen, K.; Jaalouk, D.E.; Gahmberg, C.G.; O’Brien, S.; Pasqualini, R.; Arap, W.; Koivunen, E. Role of leukemia cell invadosome in extramedullary infiltration. Blood 2009, 114, 3008–3017. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, M.; Hamada, J.; Li, Y.Q.; Shinobu, N.; Imamura, M.; Okada, F.; Takeichi, N.; Hosokawa, M. A possible role of 92 kDa type IV collagenase in the extramedullary tumor formation in leukemia. Jpn. J. Cancer Res. 1995, 86, 298–303. [Google Scholar] [CrossRef]
- Zhu, Q.; Zhang, L.; Li, X.; Chen, F.; Jiang, L.; Yu, G.; Wang, Z.; Yin, C.; Jiang, X.; Zhong, Q.; et al. Higher EZH2 expression is associated with extramedullary infiltration in acute myeloid leukemia. Tumour Biol. 2016, 37, 11409–11420. [Google Scholar] [CrossRef]
- Guryanova, O.A.; Lieu, Y.K.; Garrett-Bakelman, F.E.; Spitzer, B.; Glass, J.L.; Shank, K.; Martinez, A.B.; Rivera, S.A.; Durham, B.H.; Rapaport, F.; et al. Dnmt3a regulates myeloproliferation and liver-specific expansion of hematopoietic stem and progenitor cells. Leukemia 2016, 30, 1133–1142. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Zhang, W.; Yan, X.J.; Lin, X.Q.; Li, W.; Mi, J.Q.; Li, J.M.; Zhu, J.; Chen, Z.; Chen, S.J. DNMT3A mutation leads to leukemic extramedullary infiltration mediated by TWIST1. J. Hematol. Oncol. 2016, 9, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Miao, Z.; Jiang, Y.; Zou, P.; Li, W.; Tang, X.; Lv, Y.; Xing, D.; Chen, S.; Yang, F.; et al. Characteristics of myeloid sarcoma in mice and patients with TET2 deficiency. Oncol. Lett. 2020, 19, 3789–3798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, D.; Shi, Y.; Fu, C.; Jia, J.; Pan, Y.; Jiang, Y.; Chen, L.; Liu, S.; Zhou, W.; Zhou, J.; et al. Decrease of TET2 expression and increase of 5-hmC levels in myeloid sarcomas. Leuk. Res. 2016, 42, 75–79. [Google Scholar] [CrossRef]
- Kaeding, A.J.; Barwe, S.P.; Gopalakrishnapillai, A.; Ries, R.E.; Alonzo, T.A.; Gerbing, R.B.; Correnti, C.; Loken, M.R.; Broderson, L.E.; Pardo, L.; et al. Mesothelin is a novel cell surface disease marker and potential therapeutic target in acute myeloid leukemia. Blood Adv. 2021, 5, 2350–2361. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Wang, L.; Yang, Z.; Jin, H.; Zou, Q.; Zhan, Q.; Tang, Y.; Tao, Y.; Lei, L.; Jing, Y.; et al. Up-regulation of EMT-related gene VCAN by NPM1 mutant-driven TGF-β/cPML signalling promotes leukemia cell invasion. J. Cancer 2019, 10, 6570–6583. [Google Scholar] [CrossRef]
- Kunadt, D.; Kramer, M.; Dill, C.; Altmann, H.; Wagenführ, L.; Mohr, B.; Thiede, C.; Röllig, C.; Schetelig, J.; Bornhäuser, M.; et al. Lysyl oxidase expression is associated with inferior outcome and Extramedullary disease of acute myeloid leukemia. Biomark. Res. 2020, 8, 20. [Google Scholar] [CrossRef]
- Kwon, M.; Martínez-Laperche, C.; Infante, M.; Carretero, F.; Balsalobre, P.; Serrano, D.; Gayoso, J.; Pérez-Corral, A.; Anguita, J.; Díez-Martín, J.L.; et al. Evaluation of minimal residual disease by real-time quantitative PCR of Wilms’ tumor 1 expression in patients with acute myelogenous leukemia after allogeneic stem cell transplantation: Correlation with flow cytometry and chimerism. Biol. Blood Marrow Transplant. 2012, 18, 1235–1242. [Google Scholar] [CrossRef] [Green Version]
- Al-Adnani, M.; Williams, S.; Anderson, J.; Ashworth, M.; Malone, M.; Sebire, N.J. Immunohistochemical nuclear positivity for WT1 in childhood acute myeloid leukemia. Fetal Pediatr. Pathol. 2007, 26, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Vargas, A.C.; Turner, J.; Burchett, I.; Ho, L.L.; Zumbo, R.; Gill, A.J.; Maclean, F.M. Myeloid sarcoma and extramedullary hematopoiesis expand the spectrum of ERG-positive proliferations: An ancillary tool in the diagnosis. Hum. Pathol. 2022, 124, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.L.; Ding, B.J.; Jiang, L.; Yin, C.X.; Zhong, Q.X.; Yu, G.P.; Li, X.D.; Meng, F.Y. Increased expression of amyloid precursor protein promotes proliferation and migration of AML1/ETO-positive leukemia cells and be inhibited by panobinostat. Neoplasma 2015, 62, 864–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, Y.; Lu, W.; Yu, Y.; Zhai, Y.; Guo, H.; Yang, S.; Zhao, C.; Zhang, Y.; Liu, J.; Liu, Y.; et al. miR-29c&b2 encourage extramedullary infiltration resulting in the poor prognosis of acute myeloid leukemia. Oncogene 2021, 40, 3434–3448. [Google Scholar] [CrossRef]
- Lv, C.; Sun, L.; Guo, Z.; Li, H.; Kong, D.; Xu, B.; Lin, L.; Liu, T.; Guo, D.; Zhou, J.; et al. Circular RNA regulatory network reveals cell-cell crosstalk in acute myeloid leukemia extramedullary infiltration. J. Transl. Med. 2018, 16, 361. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.; Wang, Y.; Bian, S.; Sun, L.; Guo, Z.; Kong, D.; Zhao, L.; Guo, D.; Li, Q.; Wu, M.; et al. A circular RNA derived from PLXNB2 as a valuable predictor of the prognosis of patients with acute myeloid leukaemia. J. Transl. Med. 2021, 19, 123. [Google Scholar] [CrossRef]
- Chen, J.; Yanuck, R.R., 3rd; Abbondanzo, S.L.; Chu, W.S.; Aguilera, N.S. c-Kit (CD117) reactivity in extramedullary myeloid tumor/granulocytic sarcoma. Arch. Pathol. Lab. Med. 2001, 125, 1448–1452. [Google Scholar] [CrossRef]
- Jiang, L.; Meng, W.; Yu, G.; Yin, C.; Wang, Z.; Liao, L.; Meng, F. MicroRNA-144 targets APP to regulate AML1/ETO+ leukemia cell migration via the p-ERK/c-Myc/MMP-2 pathway. Oncol. Lett. 2019, 18, 2034–2042. [Google Scholar] [CrossRef] [Green Version]
- Isshiki, Y.; Ohwada, C.; Togasaki, E.; Shimizu, R.; Hasegawa, N.; Yamazaki, A.; Sugita, Y.; Kawaguchi, T.; Tsukamoto, S.; Sakai, S.; et al. Acute myeloid leukemia concurrent with spinal epidural extramedullary myeloid sarcoma accompanied by a high CD25 expression and the FLT3-ITD mutation. Intern. Med. 2014, 53, 1159–1164. [Google Scholar] [CrossRef] [Green Version]
- Casolaro, A.; Golay, J.; Albanese, C.; Ceruti, R.; Patton, V.; Cribioli, S.; Pezzoni, A.; Losa, M.; Texido, G.; Giussani, U.; et al. The Polo-Like Kinase 1 (PLK1) inhibitor NMS-P937 is effective in a new model of disseminated primary CD56+ acute monoblastic leukaemia. PLoS ONE 2013, 8, e58424. [Google Scholar] [CrossRef]
- Meleveedu, K.S.; Chen, D.; Nadiminti, K.; Sidiqi, H.; Khan, S.; Alkhateeb, H.; Shah, M.V.; Patnaik, M.; Hogan, W.J.; Begna, K.; et al. PD-1/PD-L1 expression in extramedullary lesions of acute myeloid leukemia. Leuk. Lymphoma 2021, 62, 764–767. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, K.; Miyoshi, H.; Suzuki, T.; Kiyasu, J.; Yokoyama, S.; Sasaki, Y.; Sone, H.; Seto, M.; Takizawa, J.; Ohshima, K. Expression of programmed death ligand 1 is associated with poor prognosis in myeloid sarcoma patients. Hematol. Oncol. 2018, 36, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Ngo, S.; Oxley, E.P.; Ghisi, M.; Garwood, M.M.; McKenzie, M.D.; Mitchell, H.L.; Kanellakis, P.; Susanto, O.; Hickey, M.J.; Perkins, A.C.; et al. Acute myeloid leukemia maturation lineage influences residual disease and relapse following differentiation therapy. Nat. Commun. 2021, 12, 6546. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Chung, H.Y. MYC and PIM2 co-expression in mouse bone marrow cells readily establishes permanent myeloid cell lines that can induce lethal myeloid sarcoma in vivo. Mol. Cells 2012, 34, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.F.; Yen, T.H.; Chen, Y.; Huang, Y.J.; Hsu, C.L.; Liang, D.C.; Shih, L.Y. Involvement of Gpr125 in the myeloid sarcoma formation induced by cooperating MLL/AF10(OM-LZ) and oncogenic KRAS in a mouse bone marrow transplantation model. Int. J. Cancer 2013, 133, 1792–1802. [Google Scholar] [CrossRef]
- Fu, J.F.; Wen, C.J.; Yen, T.H.; Shih, L.Y. Hoxa11-mediated reduction of cell migration contributes to myeloid sarcoma formation induced by cooperation of MLL/AF10 with activating KRAS mutation in a mouse transplantation model: Hoxa11 in myeloid sarcoma formation. Neoplasia 2022, 29, 100802. [Google Scholar] [CrossRef] [PubMed]
- Halahleh, K.; Alhalaseh, Y.; Al-Rimawi, D.; Da’na, W.; Alrabi, K.; Kamal, N.; Muradi, I.; Abdel-Razeq, H. Extramedullary acute myeloid leukemia (eAML): Retrospective single center cohort study on clinico-pathological, molecular analysis and survival outcomes. Ann. Med. Surg. 2021, 72, 102894. [Google Scholar] [CrossRef]
- Choi, K.H.; Song, J.H.; Kwak, Y.K.; Lee, J.H.; Jang, H.S. Analysis of PET parameters predicting response to radiotherapy for myeloid sarcoma. PLoS ONE 2021, 16, e0261550. [Google Scholar] [CrossRef]
- Creutzig, U.; van den Heuvel-Eibrink, M.M.; Gibson, B.; Dworzak, M.N.; Adachi, S.; de Bont, E.; Harbott, J.; Hasle, H.; Johnston, D.; Kinoshita, A.; et al. Diagnosis and management of acute myeloid leukemia in children and adolescents: Recommendations from an international expert panel. Blood 2012, 120, 3187–3205. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, S. Current Understandings of Myeloid Differentiation Inducers in Leukemia Therapy. Acta Haematol. 2021, 144, 380–388. [Google Scholar] [CrossRef]
- Melnick, A.M. Epigenetics in AML. Best Pract. Res. Clin. Haematol. 2010, 23, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Shabanova, I.; Cada, M.; Johnston, D.L.; Abbott, L.S.; Leung, E.W.; Schechter, T.; Dror, Y.; Klaassen, R.J. Reduction of Extramedullary Complications in Patients with Acute Myeloid Leukemia/Myelodysplastic Syndrome Treated with Azacitidine. J. Pediatr. Hematol. Oncol. 2020, 42, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Antar, A.; Otrock, Z.K.; Kharfan-Dabaja, M.; Salem, Z.; Aractingi, S.; Mohty, M.; Bazarbachi, A. Azacitidine in the treatment of extramedullary relapse of AML after allogeneic hematopoietic cell transplantation. Bone Marrow Transplant. 2013, 48, 994–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okamoto, H.; Kamitsuji, Y.; Komori, Y.; Sasaki, N.; Tsutsumi, Y.; Miyashita, A.; Tsukamoto, T.; Mizutani, S.; Shimura, Y.; Kobayashi, T.; et al. Durable Remission of Chemotherapy-Refractory Myeloid Sarcoma by Azacitidine. Tohoku J. Exp. Med. 2021, 254, 101–105. [Google Scholar] [CrossRef]
- Gornicec, M.; Wölfler, A.; Stanzel, S.; Sill, H.; Zebisch, A. Evidence for a role of decitabine in the treatment of myeloid sarcoma. Ann. Hematol. 2017, 96, 505–506. [Google Scholar] [CrossRef]
- Singh, S.N.; Cao, Q.; Gojo, I.; Rapoport, A.P.; Akpek, G. Durable complete remission after single agent decitabine in AML relapsing in extramedullary sites after allo-SCT. Bone Marrow Transplant. 2012, 47, 1008–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niscola, P.; Abruzzese, E.; Trawinska, M.M.; Palombi, M.; Tendas, A.; Giovannini, M.; Scaramucci, L.; Cupelli, L.; Fratoni, S.; Noguera, N.I.; et al. Decitabine treatment of multiple extramedullary acute myeloid leukemia involvements after essential thrombocytemia transformation. Acta Oncol. 2017, 56, 1331–1333. [Google Scholar] [CrossRef]
- Shatilova, A.; Girshova, L.; Zaytsev, D.; Budaeva, I.; Mirolyubova, Y.; Ryzhkova, D.; Grozov, R.; Bogdanov, K.; Nikulina, T.; Motorin, D.; et al. The myeloid sarcoma treated by Venetoclax with hypomethylating agent followed by stem cell transplantation: Rare case report. BMC Womens Health 2021, 21, 184. [Google Scholar] [CrossRef]
- Otoukesh, S.; Zhang, J.; Nakamura, R.; Stein, A.S.; Forman, S.J.; Marcucci, G.; Pullarkat, V.; Aldoss, I. The efficacy of venetoclax and hypomethylating agents in acute myeloid leukemia with extramedullary involvement. Leuk. Lymphoma 2020, 61, 2020–2023. [Google Scholar] [CrossRef]
- Pan, W.; Zhao, X.; Shi, W.; Jiang, Z.; Xiao, H. Venetoclax induced complete remission in extramedullary relapse of AML co-harboring NPM1, TET2, and NRAS mutations after haploidentical hematopoietic stem cell transplantation. Leuk. Lymphoma 2020, 61, 2756–2759. [Google Scholar] [CrossRef]
- Farrar, J.E.; Bolouri, H.; Ries, R.E.; Triche, T.J.; Lim, E.L.; Alonzo, T.A.; Ma, Y.; Moore, R.; Mungall, A.J.; Marra, M.A.; et al. Marked Differences in the Genomic Landscape of Pediatric Compared to Adult Acute Myeloid Leukemia: A Report from the Children’s Oncology Group and NCI/COG Therapeutically Applicable Research to Generate Effective Treatments (TARGET) Initiative. Blood 2016, 128, 595. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study/Publication | Age | Extramedullary Disease Involvement Study Definitions | Population | Incidence | 5-Year Estimated EFS (±SE) or (95% CI) | 5-Year Estimated OS (±SE) or (95% CI) | ||
|---|---|---|---|---|---|---|---|---|
| POG8821 (Chang, et. al., 2000) [10] | <21 yo | EMD: including CSF disease, not defined | n = 492 | Any EMD 10.4% | 4-year EFS | Not available | ||
| CSF only 4.7% | CSF only: 34.8 ± 9.9% | p = 0.91 | ||||||
| Non-CSF EMD 5.7% | Non-CSF EMD: 21.6 ± 8.6% | p = 0.043 | ||||||
| No EMD: 34.4 ± 2.5% | p = 0.18 | |||||||
| DCLSG (Bisschop et. al., 2001) [11] | 0–16 yo | EML: Clinically obvious infiltrate in soft tissues, skin, muscles or bone, gingiva, CSF or brain | n = 477 | EML in 25.1% | No EML 38% ± 3% | p = 0.85 | Not available | |
| Myeloblastoma (MS) 43 ± 13% | ||||||||
| Skin infiltrates 45 ± 21% | ||||||||
| Children’s Cancer Group, CCG AML 213 and 213P, 2861 and 2891 (Dusenbery et. al., 2003) [12] | 0–21 yo | “Chloroma” on data entry form yes or no, gum only not included | n = 1832 | Skin EML ± other 5.9% | Skin ± other: 26% (17–35%) | p = 0.005 | Not available | |
| “Skin involvement” yes or no | Non skin EML 4.9% | Non skin EML: 46% (34–58%) | ||||||
| EML 10.9% | Non EML: 29% (27–32%) | |||||||
| Single Center—Turkey (AML-90 and AML-94 protocols) (Hiçsönmez et. al., 2004) [13] | <17 yo | EMI: involvement of gingiva, CNS, orbit, soft tissue, bone, pleura | n = 127 | EMI total in 40% | 4-year EFS: | Not available | ||
| Gingiva only in 11% | AML-90 therapy: MS = 0% | p < 0.05 | ||||||
| Orbital in 10% | Without EMI = 37 ± 11% | |||||||
| MS in 21% | AML-94 therapy: MS = 56 ± 17% | p > 0.05 | ||||||
| Without EMI = 31 ± 1% | ||||||||
| Japanese childhood AML cooperative study group (Kobayashi et. al., 2007) [14] | <16 yo | CNS disease (>5 WBC/μL with blasts) | n = 240 | EMI in 23.3% | 3-year estimate EFS | 3-year OS | ||
| EMI: leukemic infiltration in organs other than liver, spleen, lymph nodes (including CNS disease) | (Excluding CSF only: 20.4%) | EMI: 53.3 ± 6.7% | p = 0.11 | EMI: 77.3% | ||||
| No EMI: 62.5 ± 3.6% | No EMI: 77.6% | |||||||
| EMI + WBC > 100 × 109/L: 23.8 ± 12.9% | p = 0.0052 | |||||||
| No EMI or EMI + WBC < 100 × 109/L: 60 ± 3.5% | ||||||||
| Children’s Oncology Group (CCG 2861, 2891, 2941, 2961) (Johnston et. al., 2012) [15] | 0–21 yo | CNS3 (≥5 WBC/μL with blasts) | n = 1459 | CNS3 11% | No MS 40 ± 3% | p = 0.005 | No MS 50 ± 3% | p < 0.001 |
| CNS MS (brain or spinal cord tumor) | CNS MS 1% | CNS MS 52 ± 21% | CNS MS 73 ± 19% | |||||
| Orbital MS 2% | Orbital MS 76 ± 17% | Orbital MS 92 ± 11% | ||||||
| Non CNS MS 4% | Non CNS MS 34 ± 13% | Non CNS MS 38 ± 13% | ||||||
| European AML Study Groups (Creutzig et. al., 2017) [16] | 0–17 yo | CNS involvement | n = 2365 | CNS 11.0% | CNS + 48 ± 3% | p = 0.11 | CNS + 64 ± 3% | p = 0.23 |
| (CSF with >5 WBC/μL with blasts or intracranial infiltrates on imaging or neurologic symptoms) | CNS—52 ± 2% | CNS—67 ± 1% | ||||||
| NOPHO AML 2004 (Støve et. al., 2017) [17] | 0–17 yo | MS: myeloblast tumor | n = 322 | MS (± CNS disease) 15.8% | EML: 54% (42–65%) | p = 0.57 | p = 0.008 | |
| CNS disease (≥ 5 WBC/μL with blasts or new neurologic symptoms) | CNS only an additional 7% | No EML: 45% (37–51%) | EML: 64% (51–74%) | |||||
| EML: MS or CNS disease | No EML: 73% (66–78%) | |||||||
| Single Center—India (Pramanik et. al., 2018) [18] | 0–18 yo | MS (did not include CSF only disease) | n = 570 | MS in 21.2% | Median EFS: | p = 0.002 | Median OS: | p = 0.002 |
| AML with MS: 21.6 months | With MS: 26.3 months | |||||||
| AML without MS: 11.1 months | Without MS: 12.7 months | |||||||
| TARGET dataset (COG-NCI) (COG AAML03P1, AAML0531, CCG-2961) (Xu et. al., 2020) [19] | <18 yo | MS on biopsy diagnosis, excluding CSF disease | n = 884 | MS in 12.3% | MS: 35.4 ± 4.6% | p = 0.001 | MS: 53.4 ± 4.8% | p = 0.008 |
| Non-MS: 48.5 ± 1.8% | Non-MS: 64.0 ± 1.8% | |||||||
| Single Center—Korea (Lee et. al., 2020) [20] | <18 yo | EMI: excluded CSF only | n = 40 | EMI in 30% | EMI: 50.0 ± 14.4% | p = 0.022 | Not available | |
| Only RUNX1-RUNX1T1 AML | No EMI: 78.6 ± 7.8% | |||||||
| Single Center—China (Hu et. al., 2020) [21] | ≤18 yo | MS: including lymph nodes >2cm, excluded CNSL | n = 214 | MS in 20.6% | 3-year RFS | p = 0.000 | 3-year OS | p = 0.01 |
| Only Low Risk AML (includes Hu et. al., 2021 study) | With MS: 62.6 ± 7.5% | With MS 73.5 ± 7.1% | ||||||
| Without MS: 87.0 ± 2.8% | Without MS 88.8 ± 2.6% | |||||||
| Single Center—China (Hu et. al., 2021) [22] | 1–18 y | MS: clinical, biopsy, radiology findings | n = 127 | MS in 23.6% | 3-year RFS | p = 0.004 | 3-year OS | p = 0.249 |
| Only t(8;21) AML | CNS MS: dura deposits or paraspinal tumor | With MS: 68.8 ± 8.8% | With MS: 78.1 ± 8.1% | |||||
| o | Without MS: 88.0 ± 3.4% | Without MS: 86.4 ± 3.7% | ||||||
| Polish Pediatric Leukemia and Lymphoma Study Group (Samborska et. al., 2022) [23] | 0–18 yo | MS: pathology diagnosis or extramedullary tumor and concurrent bone marrow disease (AML, MDS) | n = 43 | MS in 100% | De novo: 0.56 ± 0.12 | p = 0.0247 | pOS | p = 0.0251 |
| De novo/isolated in 37.2% | Concurrent: 0.82 ± 0.08 | De novo: 0.56 ± 0.12 | ||||||
| Concurrent in 55.8% | Concurrent: 0.84 ± 0.09 | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zorn, K.E.; Cunningham, A.M.; Meyer, A.E.; Carlson, K.S.; Rao, S. Pediatric Myeloid Sarcoma, More than Just a Chloroma: A Review of Clinical Presentations, Significance, and Biology. Cancers 2023, 15, 1443. https://doi.org/10.3390/cancers15051443
Zorn KE, Cunningham AM, Meyer AE, Carlson KS, Rao S. Pediatric Myeloid Sarcoma, More than Just a Chloroma: A Review of Clinical Presentations, Significance, and Biology. Cancers. 2023; 15(5):1443. https://doi.org/10.3390/cancers15051443
Chicago/Turabian StyleZorn, Kristin E., Ashley M. Cunningham, Alison E. Meyer, Karen Sue Carlson, and Sridhar Rao. 2023. "Pediatric Myeloid Sarcoma, More than Just a Chloroma: A Review of Clinical Presentations, Significance, and Biology" Cancers 15, no. 5: 1443. https://doi.org/10.3390/cancers15051443