
Successful Lifetime/Long-Term Medical Treatment of Acid Hypersecretion in Zollinger-Ellison Syndrome (ZES): Myth or Fact? Insights from an Analysis of Results of NIH Long-Term Prospective Studies of ZES

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Initial Investigations
2.2. Determination of the Antisecretory Drug-Dose
2.3. Statistics
3. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Number (%) |
|---|---|
| Patient number | |
| Total treated | 303 (100%) |
| Number followed long-term (≥5 yrs) (a) | 260 (86%) |
| Number not followed long-term (<5 yrs) (a) | 43 (14%) |
| Age at ZES onset (yrs) (b) | |
| Mean ± SEM | 40.0 ± 0.7 |
| (Range) | (11.0–65.8) |
| Age at ZES Diagnosis (yrs) (c) | |
| Mean ± SEM | 45.8 0.7 |
| (Range) | (11.0–65.8) |
| Gender | |
| Male | 170 (56%) |
| Female | 133(44%) |
| MEN1 present | 89 (29%) |
| Presenting clinical symptoms/features (d) | |
| Pain | 233 (77%) |
| Diarrhea | 220 (72%) |
| GERD (moderate/severe) | 133 (44%) |
| Ulcer history | 205 (67%) |
| Bleeding | 70 (23%) |
| Other GERD/PUD Complication (e) | 39 (13%) |
| Prior gastric acid reduction surgery | 37 (12%) |
| Vagotomy-pyloroplasty/Selective vagotomy | 14 (4.6%) |
| Billroth I resection | 6 (2.0%) |
| Billroth 2 resection | 17 (5.6%) |
| Duration of medical acid treatment started (yrs) (f) | |
| From disease onset | |
| Mean ± SEM | 3.7 ± 0.3 |
| (Range) | (0–26.1) |
| Prior to ZES diagnosis (yrs) (g) | |
| Mean ± SEM | 3.5 ± 0.3 |
| (Range) | (0.01–26.0) |
| From time of diagnosis (yrs) | |
| Mean ± SEM | 1.2 ± 0.3 |
| (Range) | (0–18) |
| Characteristic | Number (%) |
|---|---|
| Fasting serum gastrin (FSG) (pg/mL) | |
| Mean ± SEM | 4932 ± 1272 |
| (Range) | (72–286,800) |
| Median | 644 |
| Hi FSG (≥644 pg/mL) (≥median) | 149 (49%) |
| BAO (mEq/h) (no gastric surgery) (a) | |
| Mean ± SEM | 43.0 ± 1.5 |
| (Range) | (1.8–159) |
| BAO (mEq/h) (previous gastric surgery) (b) | |
| Mean ± SEM | 26.3 ± 3.0 |
| (Range) | (2–94) |
| Hi BAO (≥36.8 mEq/h) (median output of 276 with BAO) | 127 (46%) |
| MAO (mEq/h) (no gastric surgery) (b) | |
| Mean ± SEM | 65.0 ± 2.0 |
| (Range) | (13–159) |
| MAO (mEq/h) (previous gastric surgery) (b) | |
| Mean ± SEM | 36.9 ± 4.3 |
| (Range) | (9.0–113) |
| Hi MAO (≥59.7 mEq/h) (median output of 227 with MAO) (b) | 112 (49%) |
| Primary tumor location (c) | |
| Pancreas | 78 (26%) |
| Duodenum | 114 (38%) |
| Other (d) | 36 (12%) |
| Unknown (d) | 86 (28%) |
| Tumor extent (e,f) | |
| Primary only | 113 (37%) |
| Primary and lymph node metastases | 82 (27%) |
| Primary and liver metastases | 84 (28%) |
| Characteristic | Number (% Total) |
|---|---|
| I. Treatment schedule | |
| Total acid treatment drugs (n = 303) (a) | |
| H2R (cimetidine, ranitidine, famotidine, nizatidine) at any time | 245 (81%) |
| Only H2R without any PPI treatment at any time | 41 (13.5%) |
| H2R with anticholinergeric agent at any time | 50 (16.5%) |
| H2R without anticholinergeric agent at any time | 195 (64.4%) |
| H2R then PPI (b) | 204 (67%) |
| PPI (omeprazole, lansoprazole, pantoprazole) at any time | 262 (86%) |
| PPI only | 58 (19.1%) |
| PPI then H2R (c) | 0 (0%) |
| First medical acid treatment drug (n = 303) (a) | |
| H2R | 245 (81%) |
| PPI | 58 (19%) |
| Pts with only short-term acid medical treatment <5 yrs (n = 42) (d) | |
| H2R only without any PPI treatment at any time | 18 (6.6%) |
| H2R with anticholinergic agent at any time | 7(2.3%) |
| H2R without anticholinergic agent at any time | 35(11.6%) |
| PPI only | 7 (2.3%) |
| H2-R then PPI | 17 (6.9%) |
| Pts with any long-term acid treatment (≥5 yrs) (n = 261) (d) | |
| H2R only without any PPI treatment at any time | 22 (7.3%) |
| H2R with anticholinergic agent at any time | 19 (6.2%) |
| H2R without anticholinergic agent at any time | 93 (30.7%) |
| PPI only | 149 (49%) |
| H2R, then PPI | 90(30%) |
| II. Treatment duration (yrs) | |
| All acid treatment (n = 303) | |
| Mean ± SEM | 13.7 ± 0.5 |
| Range | (0.08–48.1) |
| Only Short-term acid medical treatment <5 yrs (n = 42) | |
| Mean ± SEM | 2.8 ± 0.2 |
| Range | (0.08–4.9) |
| Any Long-term acid treatment ≥5 yrs (n = 261) | 15.5 ± 0.5 |
| Mean ± SEM | (5.1–48.1) |
| Range | |
| Any treatment with H2R (n = 245) | |
| Mean ± SEM | 6.4 ± 0.45 |
| Range | (0.07–29.2) |
| Any treatment with PPI (n = 262) | |
| Mean ± SEM | 9.8 ± 0.4 |
| Range | (0.1–48.1) |
| Variable | Number (Percent) | ||
|---|---|---|---|
| Change Daily PPI Dose (n = 123) | Same PPI Dose (n = 139) | p-Value | |
| Clinical | |||
| GERD | |||
| Any (b) | 77/156 (49%) | 53/106 (50%) | 0.99 |
| Severe (b) | 24/50 (48%) | 11/212 (5.2%) | <0.0001 |
| Diarrhea at onset (c) | 121/156 (78%) | 78/106 (73%) | 0.47 |
| PUD/GERD complication (d) | 31/156 (65%) | 17/106 (19.8%) | 0.52 |
| >6.4 yrs from ZES onset to treatment (c) | 76/156 (49%) | 53/106 (50%) | 0.90 |
| Age > 40 yrs at ZES onset (c) | 74/156 (47%) | 51/106 (48%) | 0.99 |
| Male gender | 91/156 (58%) | 60/106 (57%) | 0.80 |
| MEN1 present (c) | 43/156 (27.6%) | 35/106 (33%) | 0.41 |
| Prior gastric acid reduction surgery (d) | |||
| Any acid reduction surgery | 18/156 (11.5%) | 7/106 (6.6%) | 0.21 |
| Prior Billroth2 | 10/148 (6.3%) | 0/104 (0%) | 0.007 |
| Lab | |||
| High BAO > 36.8 mEq/h (e) | 78/156 (50%) | 39/106 (37%) | 0.043 |
| High MAO > 62 mEq/h (e) | 99/216 (89%) | 12/12 (100%) | <0.0001 |
| High FSG > 644 pg/mL (e) | 78/156 (50%) | 48/106 (45%) | 0.53 |
| Tumor features | |||
| Primary tumor size (f) | |||
| ≥3 cm | 42/156 (26.9%) | 34/105 (32.3%) | 0.41 |
| <1 cm | 98/156 (63%) | 60/105 (57%) | 0.37 |
| Localized Disease (g) | 110/156 (70%) | 80/206 (75%) | 0.40 |
| Liver Metastases | 46/156 (29.5%) | 26/106 (24.5%) | 0.40 |
| Pancreatic primary | 24/108 (53%) | 21/67 (31.3%) | 0.21 |
| Duodenal primary | 64/109 (59%) | 33/67 (49%) | 0.27 |
| Acid treatment | |||
| Length PPI Tx ≥ 9.5 yrs | 84/156 (54%) | 46/106 (43%) | 0.10 |
| Acid control 1st PPI dose (h) | |||
| 0 mEq/h | 7/91 (7.5%) | 29/144 (32%) | 0.0095 |
| ≥5–9.9 mEq/h | 23/143 (16%) | 10/92 (10.9%) | 0.34 |
| PPI daily dose (1st PPI dose) | |||
| QD: Daily PPI dose > 55 mg/day (i) | 54/80 (68%) | 26/80 (32%) | 0.0267 |
| BID: Daily PPI dose ≥ 80 mg/day (i) | 60/71 (84%) | 31/47 (15%) | 0.0252 |
| Frequency 1st PPI dose: >1×/day | 71/156 (46%) | 47/76 (62%) | 0.90 |
| H2R dose day > 600 mg prior to PPI | 59/124 (48%) | 35/83 (42%) | 0.48 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zollinger, R.M.; Ellison, E.H. Primary peptic ulcerations of the jejunum associated with islet cell tumors of the pancreas. Ann. Surg. 1955, 142, 709–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellison, E.H.; Wilson, S.D. The Zollinger-Ellison syndrome: Re-appraisal and evaluation of 260 registered cases. Ann. Surg. 1964, 160, 512–530. [Google Scholar] [CrossRef] [PubMed]
- Zollinger, R.M.; Ellison, E.C.; O’Dorisio, T.M.; Sparks, J. Thirty years’ experience with gastrinoma. World J. Surg. 1984, 8, 427–435. [Google Scholar] [CrossRef]
- Ellison, E.C.; Johnson, J.A. The Zollinger-Ellison syndrome: A comprehensive review of historical, scientific, and clinical considerations. Curr Probl. Surg. 2009, 46, 13–106. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.T. Gastrointestinal endocrine tumors. Gastrinoma. Bailliere’s Clin. Gastroenterol. 1996, 10, 555–766. [Google Scholar]
- Gregory, R.A.; Grossman, M.I.; Tracy, H.J.; Bentley, P.H. Nature of the gastric secretagogue in Zollinger-Ellison tumors. Lancet 1967, 2, 543–544. [Google Scholar] [CrossRef] [PubMed]
- Gregory, R.A.; Tracy, H.J.; Agarwal, K.L.; Grossman, M.I. Aminoacid constitution of two gastrins isolated from Zollinger-Ellison tumor tissue. Gut 1969, 10, 603–608. [Google Scholar] [CrossRef] [Green Version]
- McGuigan, J.E.; Trudeau, W.L. Immunochemical measurement of elevated levels of gastrin in the serum of patients with pancreatic tumors of the Zollinger-Ellison variety. N. Engl. J. Med. 1968, 278, 1308–1313. [Google Scholar] [CrossRef]
- Norton, J.A.; Foster, D.S.; Ito, T.; Jensen, R.T. Gastrinomas: Medical and SurgicalTreatment. Endocrinol. Metab. Clin. N. Am. 2018, 47, 577–601. [Google Scholar] [CrossRef]
- Howard, T.J.; Zinner, M.J.; Stabile, B.E.; Passaro, E., Jr. Gastrinoma excision for cure. A prospective analysis. Ann. Surg. 1990, 211, 9–14. [Google Scholar] [CrossRef]
- Thompson, N.W.; Pasieka, J.; Fukuuchi, A. Duodenal gastrinomas, duodenotomy, and duodenal exploration in the surgical management of Zollinger-Ellison syndrome. World J. Surg. 1993, 17, 455–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cingam, S.R.; Botejue, M.; Hoilat, G.J.; Karanchi, H. Gastrinoma. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Cho, M.S.; Kasi, A. Zollinger Ellison Syndrome. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Jensen, R.T.; Niederle, B.; Mitry, E.; Ramage, J.K.; Steinmuller, T.; Lewington, V.; Scarpa, A.; Sundin, A.; Perren, A.; Gross, D.; et al. Gastrinoma (duodenal and pancreatic). Neuroendocrinology 2006, 84, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.T.; Berna, M.J.; Bingham, M.D.; Norton, J.A. Inherited pancreatic endocrine tumor syndromes: Advances in molecular pathogenesis, diagnosis, management and controversies. Cancer 2008, 113, 1807–1843. [Google Scholar] [CrossRef] [Green Version]
- Gibril, F.; Venzon, D.J.; Ojeaburu, J.V.; Bashir, S.; Jensen, R.T. Prospective study of the natural history of gastrinoma in patients with MEN1: Definition of an aggressive and a nonaggressive form. J. Clin. Endocrinol. Metab. 2001, 86, 5282–5293. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Igarashi, H.; Jensen, R.T. Pancreatic neuroendocrine tumors: Clinical features, diagnosis and medical treatment: Advances. Best Pract. Res. Clin. Gastroenterol. 2012, 26, 737–753. [Google Scholar] [CrossRef] [Green Version]
- Friesen, S.R.; Schimke, R.N.; Pearse, A.G. Genetic aspects of the Z-E syndrome: Prospective studies in two kindreds: Antral gastrin cell hyperplasia. Ann. Surg. 1972, 176, 370–383. [Google Scholar] [CrossRef]
- Cadiot, G.; Vuagnat, A.; Doukhan, I.; Murat, A.; Bonnaud, G.; Delemer, B.; Thiefin, G.; Beckers, A.; Veyrac, M.; Proye, C.; et al. Prognostic factors in patients with Zollinger-Ellison syndrome and multiple endocrine neoplasia type 1. Gastroenterology 1999, 116, 286–293. [Google Scholar] [CrossRef]
- Jensen, R.T.; Gardner, J.D. Gastrinoma. In The Pancreas: Biology, Pathobiology and Disease, 2nd ed.; Go, V.L.W., DiMagno, E.P., Gardner, J.D., Lebenthal, E., Reber, H.A., Scheele, G.A., Eds.; Raven Press Publishing Co.: New York, NY, USA, 1993; pp. 931–978. [Google Scholar]
- Creutzfeldt, W.; Arnold, R.; Creutzfeldt, C.; Track, N.S. Pathomorphologic, biochemical and diagnostic aspects of gastrinomas (Zollinger-Ellison syndrome). Hum. Pathol. 1975, 6, 47–76. [Google Scholar] [CrossRef]
- Jensen, R.T. Natural history of digestive endocrine tumors. In Recent Advances in Pathophysiology and Management of Inflammatory Bowel Diseases and Digestive Endocrine Tumors; Mignon, M., Colombel, J.F., Eds.; John Libbey Eurotext Publishing Co.: Paris, France, 1999; pp. 192–219. [Google Scholar]
- Zollinger, R.M.; Ellison, E.C.; Fabri, P.J.; Johnson, J.; Sparks, J.; Carey, L.C. Primary peptic ulcerations of the jejunum associated with islet cell tumors. Twenty-five-year appraisal. Ann. Surg. 1980, 192, 422–430. [Google Scholar] [CrossRef]
- Thompson, J.C.; Reeder, D.D.; Villar, H.V.; Fender, H.R. Natural history and experience with diagnosis and treatment of the Zollinger-Ellison syndrome. Surg. Gynecol. Obstet. 1975, 140, 721–739. [Google Scholar]
- Ito, T.; Jensen, R.T. Perspectives on the Current Pharmacotherapeutic Strategies for Management of Functional Neuroendocrine Tumor Syndromes. Expert Opin. Pharmacother. 2021, 22, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Zollinger, R.M. Gastrinoma: Factors influencing prognosis. Surgery 1985, 97, 49–54. [Google Scholar] [PubMed]
- Zollinger, R.M.; Martin, E.W., Jr.; Carey, L.C.; Sparks, J.; Minton, J.P. Observations on the postoperative tumor growth behavior of certain islet cell tumors. Ann. Surg. 1976, 184, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Poitras, P.; Gingras, M.H.; Rehfeld, J.F. The Zollinger-Ellison syndrome: Dangers and consequences of interrupting antisecretory treatment. Clin Gastroenterol. Hepatol. 2012, 10, 199–202. [Google Scholar] [CrossRef]
- Weber, H.C.; Venzon, D.J.; Lin, J.T.; Fishbein, V.A.; Orbuch, M.; Strader, D.B.; Gibril, F.; Metz, D.C.; Fraker, D.L.; Norton, J.A.; et al. Determinants of metastatic rate and survival in patients with Zollinger-Ellison syndrome: A prospective long-term study. Gastroenterology 1995, 108, 1637–1649. [Google Scholar] [CrossRef]
- Lee, L.; Ramos-Alvarez, I.; Ito, T.; Jensen, R.T. Insights into Effects/Risks of Chronic Hypergastrinemia and Lifelong PPI Treatment in Man Based on Studies of Patients with Zollinger-Ellison Syndrome. Int. J. Mol. Sci. 2019, 20, 5128. [Google Scholar] [CrossRef] [Green Version]
- Berna, M.J.; Annibale, B.; Marignani, M.; Luong, T.V.; Corleto, V.; Pace, A.; Ito, T.; Liewehr, D.J.; Venzon, D.J.; Delle Fave, G.; et al. A prospective study of gastric carcinoids and enterochromaffin-like cells changes in Multple Endocrine Neoplaisa Type 1 and Zollinger-Ellison syndrome: Identification of risk factors. J. Clin. Endocrinol. Metab. 2008, 93, 1582–1591. [Google Scholar] [CrossRef] [Green Version]
- Peghini, P.L.; Annibale, B.; Azzoni, C.; Milione, M.; Corleto, V.D.; Gibril, F.; Venzon, D.J.; Delle Fave, G.; Bordi, C.; Jensen, R.T. Effect of chronic hypergastrinemia on human enterochromaffin-like cells: Insights from patients with sporadic gastrinomas. Gastroenterology 2002, 123, 68–85. [Google Scholar] [CrossRef]
- Jensen, R.T. Gastrinoma as a model for prolonged hypergastrinemia in man. In Gastrin; Walsh, J.H., Ed.; Raven Press Publishing Co.: New York, NY, USA, 1993; pp. 373–393. [Google Scholar]
- Jensen, R.T. Consequences of Long-Term Proton Pump Blockade: Insights from Studies of Patients with Gastrinomas. Basic Clin. Pharmacol. Toxicol. 2006, 98, 4–19. [Google Scholar] [CrossRef]
- Neuburger, P.; Lewin, M.; Recherche, C.d.; Bonfils, S. Parietal and chief cell population in four cases of the Zollinger-Ellison syndrome. Gastroenterology 1972, 63, 937–942. [Google Scholar] [CrossRef]
- Polacek, M.A.; Ellison, E.H. Parietal cell mass and gastric acid secretion in the Zollinger-Ellison syndrome. Surgery 1966, 60, 606–614. [Google Scholar] [PubMed]
- Roy, P.K.; Venzon, D.J.; Feigenbaum, K.M.; Koviack, P.D.; Bashir, S.; Ojeaburu, J.V.; Gibril, F.; Jensen, R.T. Gastric secretion in Zollinger-Ellison syndrome: Correlation with clinical expression, tumor extent and role in diagnosis-A prospective NIH study of 235 patients and review of the literature in 984 cases. Medicine 2001, 80, 189–222. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, D.M.; Olinger, E.J.; May, R.J.; Long, B.W.; Gardner, J.D. H2-histamine receptor blocking agents in the Zollinger-Ellison syndrome. Experience in seven cases and implications for long-term therapy. Ann. Intern. Med. 1977, 87, 668–675. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, D.M. Report on the United States experience with cimetidine in Zollinger-Ellison syndrome and other hypersecretory states. Gastroenterology 1978, 74, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.T.; Gardner, J.D.; Raufman, J.P.; Pandol, S.J.; Doppman, J.L.; Collen, M.J. Zollinger-Ellison syndrome: Current concepts and management. Ann. Intern. Med. 1983, 98, 59–75. [Google Scholar] [CrossRef]
- Jensen, R.T. Use of omeprazole and other proton pump inhibitors in the Zollinger-Ellison syndrome. In Milestones in Drug Therapy; Olbe, L., Ed.; Birkhauser Verlag AG Publish. Co.: Basel, Switzerland, 1999; pp. 205–221. [Google Scholar]
- Vallot, T.; Mignon, M.; Mazure, R.; Bonfils, S. Evaluation of antisecretory drug therapy of Zollinger-Ellison syndrome (ZES) using 24-hour pH monitoring. Dig. Dis. Sci. 1983, 28, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.T.; Ito, T. Gastrinoma. In Endotext [Internet]; MDText.com, Inc.: South Dartmouth, MA, USA, 2020; Available online: www.endotext.org (accessed on 10 January 2023).
- Bonfils, S.; Mignon, M.; Vallot, T.; Haffar, S. Place of ranitidine in the management of the Zollinger-Ellison syndrome. Dig. Dis. Sci. 1984, 29, 12S. [Google Scholar]
- Bonfils, S.; Mignon, M.; Vallot, T.; Mayeur, S. Use of ranitidine in the medical treatment of Zollinger-Ellison syndrome. Scand. J. Gastroenterol. Suppl. 1981, 69, 119–122. [Google Scholar]
- Bonfils, S.; Mignon, M.; Gratton, J. Cimetidine treatment of acute and chronic Zollinger-Ellison syndrome. World J. Surg. 1979, 3, 597–604. [Google Scholar] [CrossRef]
- Bonfils, S.; Mignon, M.; Kloeti, G. Antagonistes des recepteurs H2 a l’histamine et traitement medical du syndrome de Zollinger-Ellison. Sem. Hop. Paris 1978, 54, 309–312. [Google Scholar]
- Vogel, S.B.; Wolfe, M.M.; McGuigan, J.E.; Hawkins, I.F., Jr.; Howard, R.J.; Woodward, E. Localization and resection of gastrinomas in Zollinger-Ellison syndrome. Ann. Surg. 1987, 205, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Vezzadini, P.; Bonora, G.; Tomassetti, P.; Pazzaglia, M.; Labo, G. Medical treatment of Zollinger-Ellison syndrome with ranitidine. Int. J. Tiss. Reac. 1983, 4, 339–343. [Google Scholar]
- Vellar, D.; Henderson, M.; Vellar, I.D.; Desmond, P. The Zollinger-Ellison syndrome: A review of the St. Vincent’s hospital, Melbourne experience. Aust. N. Z. J. Surg. 1985, 55, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Ziemniak, J.A.; Madura, M.; Adamonis, A.J.; Olinger, E.J.; Dreyer, M.; Schentag, J.J. Failure of cimetidine in Zollinger-Ellison syndrome. Dig. Dis. Sci. 1983, 28, 976–980. [Google Scholar] [CrossRef] [PubMed]
- Habal, F.M.; Soldin, S.J.; Greenberg, G.R. Cimetidine-resistant Zollinger-Ellison syndrome: Successful management with ranitidine. Can. Med. Assoc. J. 1983, 129, 256–258. [Google Scholar] [PubMed]
- Malagelada, J.R.; Edis, A.J.; Adson, M.A.; Van Heerden, J.A.; Go, V.L.W. Medical and surgical options in the management of patients with gastrinoma. Gastroenterology 1983, 84, 1524–1532. [Google Scholar] [CrossRef]
- Stage, J.G.; Rune, S.J.; Stadil, F.; Worning, H. Treatment of Zollinger-Ellison patients with cimetidine. In Cimetidine; Burland, W.L., Simkins, M.A., Eds.; Excerpta Medica: Amsterdam, The Netherlands, 1977; pp. 306–310. [Google Scholar]
- Stadil, F.; Stage, J.G. Cimetidine and the Zollinger-Ellison (Z-E) syndrome. In Cimetidine: The Westminster Hospital Symposium; Churchill Livingstone: London, UK, 1978; pp. 91–104. [Google Scholar]
- Bonfils, S.; Mignon, M.; Jian, R.; Kloeti, G. Biological studies during long-term cimetidine administration in Zollinger-Ellison syndrome. In Cimetidine; Burland, W.L., Simkins, M.A., Eds.; Excerpta Medica: Amsterdam, The Netherlands, 1977; pp. 311–321. [Google Scholar]
- Bonfils, S.; Mignon, M.; Kloeti, G. Cimetidine treatment in Zollinger-Ellison syndrome. In Gastrointestinal Hormones and Pathology of the Digestive System; Grossman, M., Speranza, V., Basso, N., LeZoche, E., Eds.; Plenum Press: New York, NY, USA, 1977; pp. 111–116. [Google Scholar]
- Kulke, M.H.; Anthony, L.B.; Bushnell, D.L.; de Herder, W.W.; Goldsmith, S.J.; Klimstra, D.S.; Marx, S.J.; Pasieka, J.L.; Pommier, R.F.; Yao, J.C.; et al. NANETS Treatment Guidelines: Well-Differentiated Neuroendocrine Tumors of the Stomach and Pancreas. Pancreas 2010, 39, 735–752. [Google Scholar] [CrossRef] [Green Version]
- Metz, D.C.; Pisegna, J.R.; Fishbeyn, V.A.; Benya, R.V.; Jensen, R.T. Control of gastric acid hypersecretion in the management of patients with Zollinger-Ellison syndrome. World J. Surg. 1993, 17, 468–480. [Google Scholar] [CrossRef]
- Metz, D.C.; Cadiot, G.; Poitras, P.; Ito, T.; Jensen, R.T. Diagnosis of Zollinger-Ellison syndrome in the era of PPIs, faulty gastrin assays, sensitive imaging and limited access to acid secretory testing. Int. J. Endocr. Oncol. 2017, 4, 167–185. [Google Scholar] [CrossRef] [Green Version]
- Bardram, L.; Stadil, F. Omeprazole in the Zollinger-Ellison syndrome. Scand. J. Gastroenterol. 1986, 21, 374–378. [Google Scholar] [CrossRef]
- Delchier, J.C.; Soule, J.C.; Mignon, M.; Goldfain, D.; Cortot, A.; Travers, B.; Isal, J.P.; Bader, J.P. Effectiveness of omeprazole in seven patients with Zollinger- Ellison syndrome resistant to histamine H2-receptor antagonists. Dig. Dis. Sci. 1986, 31, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Hirschowitz, B.I.; Mohnen, J.; Shaw, S. Long-term treatment with lansoprazole for patients with Zollinger-Ellison syndrome. Aliment. Pharmacol. Ther. 1996, 10, 507–522. [Google Scholar] [CrossRef] [PubMed]
- Hirschowitz, B.I.; Simmons, J.L.; Johnson, L.F.; Mohnen, J. Risk factors for esophagitis in extreme acid hypersecretors with and without Zollinger-Ellison syndrome. Clin. Gastroenterol. Hepatol. 2004, 2, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Bordi, C.; Ravazzola, M.; DeVita, O. Pathology of endocrine cells in gastric mucosa. Ann. Pathol. 1983, 3, 19–28. [Google Scholar] [PubMed]
- Hage, E.; Hendel, L.; Gustafsen, J.; Hendel, J. Histopathology of the gastric oxyntic mucosa in two different patient groups during long-term treatment with omeprazole. Eur. J. Gastroenterol. Hepatol. 2003, 15, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Hirschowitz, B.I.; Simmons, J.; Mohnen, J. Minor effects of Helicobacter pylori on gastric secretion and dose of lansoprazole during long-term treatment in ZE and non-ZE acid hypersecretors. Aliment. Pharmacol. Ther. 2002, 16, 303–313. [Google Scholar] [CrossRef]
- Raddatz, D.; Horstmann, O.; Basenau, D.; Becker, H.; Ramadori, G. Cushing’s syndrome due to ectopic adrenocorticotropic hormone production by a non-metastatic gastrinoma after lonterm conservative treatment of Zollinger-Ellison syndrome. Ital. J. Gastroenterol. Hepatol. 1998, 30, 636–640. [Google Scholar]
- Imamura, M.; Komoto, I.; Wada, M.; Doi, R.; Adachi, Y.; Yabana, T.; Kabumoto, T.; Miyamoto, S.; Hirota, T.; Miyoshi, A.; et al. Clinical evaluation of rabeprazole in patients with Zollinger-Ellison syndrome. Therpeutic Res. 2005, 26, 1287–1308. [Google Scholar]
- Mignon, M.; Hochlaf, S.; Forestier, S.; Ruszniewski, P.; Vatier, J.; Joubert-Collin, M. Dose-response effect of lansoprazole in patients with Zollinger-Ellison syndrome. Gastroenterol. Clin. Biol. 1994, 18, 13–16. [Google Scholar]
- Paul, G.; Ramdani, A.; Mignon, M.; Vallot, T.; Forestier, S.; Cadiot, G.; Ruszniewski, P.; Joubert-Collin, M. Comparative efficacy of lansoprazole and omeprazole on the intragastric pH measured over a period of 24 hours and on the basal. Gastroenterol. Clin. Biol. 1994, 18, 695–701. [Google Scholar]
- Ramdani, A.; Mignon, M.; Samoyeau, R. Effect of pantoprazole versus other proton pump inhibitors on 24-hour intragastric pH and basal acid output in Zollinger-Ellison syndrome. Gastroenterol. Clin. Biol. 2002, 26, 355–359. [Google Scholar] [PubMed]
- Modlin, I.M. Efficacy and safety of intravenously administered pantoprazole in the treatment of gastrinoma. Recenti Prog. Med. 2001, 92, 456–461. [Google Scholar] [PubMed]
- Norton, J.A.; Fraker, D.L.; Alexander, H.R.; Venzon, D.J.; Doppman, J.L.; Serrano, J.; Goebel, S.U.; Peghini, P.; Roy, P.K.; Gibril, F.; et al. Surgery to cure the Zollinger-Ellison syndrome. N. Engl. J. Med. 1999, 341, 635–644. [Google Scholar] [CrossRef] [PubMed]
- Norton, J.A.; Doppman, J.L.; Jensen, R.T. Curative resection in Zollinger-Ellison syndrome: Results of a 10-year prospective study. Ann. Surg. 1992, 215, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Norton, J.A.; Fraker, D.L.; Alexander, H.R.; Gibril, F.; Liewehr, D.J.; Venzon, D.J.; Jensen, R.T. Surgery increases survival in patients with gastrinoma. Ann. Surg. 2006, 244, 410–419. [Google Scholar] [CrossRef]
- MacFarlane, M.P.; Fraker, D.L.; Alexander, H.R.; Norton, J.A.; Jensen, R.T. A prospective study of surgical resection of duodenal and pancreatic gastrinomas in multiple endocrine neoplasia-Type 1. Surgery 1995, 118, 973–980. [Google Scholar] [CrossRef]
- Pipeleers-Marichal, M.; Somers, G.; Willems, G.; Foulis, A.; Imrie, C.; Bishop, A.E.; Polak, J.M.; Hacki, W.H.; Stamm, B.; Heitz, P.U.; et al. Gastrinomas in the duodenums of patients with multiple endocrine neoplasia type 1 and the Zollinger-Ellison syndrome. N. Engl. J. Med. 1990, 322, 723–727. [Google Scholar] [CrossRef]
- Pipeleers-Marichal, M.; Donow, C.; Heitz, P.U.; Kloppel, G. Pathologic aspects of gastrinomas in patients with Zollinger-Ellison syndrome with and without multiple endocrine neoplasia type I. World J. Surg. 1993, 17, 481–488. [Google Scholar] [CrossRef]
- Norton, J.A.; Krampitz, G.; Jensen, R.T. Multiple Endocrine Neoplasia: Genetics and Clinical Management. Surg. Oncol. Clin. N. Am. 2015, 24, 795–832. [Google Scholar] [CrossRef] [Green Version]
- Kong, W.; Albers, M.B.; Manoharan, J.; Goebel, J.N.; Kann, P.H.; Jesinghaus, M.; Bartsch, D.K. Pancreaticoduodenectomy Is the Best Surgical Procedure for Zollinger-Ellison Syndrome Associated with Multiple Endocrine Neoplasia Type 1. Cancers 2022, 14, 1928. [Google Scholar] [CrossRef]
- Cadiot, G.; Laurent-Puig, P.; Thuille, B.; Lehy, T.; Mignon, M.; Olschwang, S. Is the multiple endocrine neoplasia type 1 gene a suppressor for fundic argyrophil tumors in the Zollinger-Ellison syndrome? Gastroenterology 1993, 105, 579–582. [Google Scholar] [CrossRef] [PubMed]
- Prichard, P.J.; Yeomans, N.D.; Mihaly, G.W.; Jones, D.B.; Buckle, P.J.; Smallwood, R.A.; Louis, W.J. Omeprazole: A study of its inhibition of gastric pH and oral pharmacokinetics after morning or evening dosage. Gastroenterology 1985, 88, 64–69. [Google Scholar] [CrossRef]
- Imamura, M.; Komoto, I.; Taki, Y. How to treat gastrinomas in patients with multiple endocrine neoplasia type1: Surgery or long-term proton pump inhibitors? Surg. Today 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Maton, P.N.; Gardner, J.D.; Jensen, R.T. Cushing’s syndrome in patients with Zollinger-Ellison syndrome. N. Engl. J. Med. 1986, 315, 1–5. [Google Scholar] [CrossRef]
- Ito, T.; Igarashi, H.; Uehara, H.; Berna, M.J.; Jensen, R.T. Causes of Death and Prognostic Factors in Multiple Endocrine Neoplasia Type 1: A Prospective Study: Comparison of 106 MEN1/Zollinger-Ellison Syndrome Patients with 1613 Literature MEN1 Patients with or Without Pancreatic Endocrine Tumors. Medicine 2013, 92, 135–181. [Google Scholar] [CrossRef] [PubMed]
- Tomassetti, P.; Migliori, M.; Lalli, S.; Campana, D.; Tomassetti, V.; Corinaldesi, R. Epidemiology, clinical features and diagnosis of gastroenteropancreatic endocrine tumours. Ann. Oncol. 2001, 12, S95–S99. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.T. Basis for failure of cimetidine in patients with Zollinger- Ellison syndrome. Dig. Dis. Sci. 1984, 29, 363–366. [Google Scholar] [CrossRef]
- Metz, D.C.; Jensen, R.T. Advances in gastric antisecretory therapy in Zollinger-Ellison syndrome. In Endocrine Tumors of the Pancreas: Recent Advances in Research and Management. Series: Frontiers of Gastrointestinal Research; Mignon, M., Jensen, R.T., Eds.; S. Karger: Basel, Switzerland, 1995; Volume 23, pp. 240–257. [Google Scholar]
- Deveney, C.W.; Stein, S.; Way, L.W. Cimetidine in the treatment of Zollinger-Ellison syndrome. Am. J. Surg. 1983, 146, 116–123. [Google Scholar] [CrossRef]
- Martino, B.R.; Manibusan, P. Zollinger Ellison Syndrome Refractory to Medical Therapy in the Setting of Multiple Endocrine Neoplasia Type I. Cureus 2022, 14, e26468. [Google Scholar] [CrossRef]
- Pratap, T.; Jalal, M.J.A.; Jacob, D.; Mahadevan, P.; Nair, S.S.; Raja, S. Radiological Features of Zollinger-Ellison Syndrome: A Report of Two Cases. Indian J. Radiol. Imaging 2022, 32, 395–402. [Google Scholar] [CrossRef]
- Lui, J.; Terra, S.B.S.P.; de la Fuente, J. Metastatic Gastrinoma Localized on Gallium-68 DOTATATE Imaging. Mayo Clin. Proc. 2021, 96, 285–286. [Google Scholar] [CrossRef] [PubMed]
- Perrier, M.; Delemer, B.; Deguelte, S.; Legros, V.; Brixi, H.; Kianmanesh, R.; Cadiot, G. Total gastrectomy for severe proton pump inhibitor-induced hypomagnesemia in a MEN1/Zollinger Ellison syndrome patient. Pancreatology 2021, 21, 236–239. [Google Scholar] [CrossRef] [PubMed]
- Venkat, P.G.; Longstreth, G.F. Gastroesophageal Reflux Disease and the Zollinger-Ellison Syndrome. Am. J. Gastroenterol. 2022, 117, 1012–1013. [Google Scholar] [CrossRef] [PubMed]
- Daniels, L.M.; Khalili, M.; Morano, W.F.; Simoncini, M.; Mapow, B.C.; Leaf, A.; Bowne, W.B. Case report: Optimal tumor cytoreduction and octreotide with durable disease control in a patient with MEN-1 and Zollinger-Ellison syndrome-over a decade of follow-up. World J. Surg. Oncol. 2019, 17, 213. [Google Scholar] [CrossRef] [Green Version]
- Eyal, A.; Sueissa, A.; Braun, E.; Naffaa, M.E. From hypomagnesaemia to Zollinger-Ellison syndrome: An adverse effect of a proton pump inhibitor. BMJ Case. Rep. 2014, 2014, bcr2014205165. [Google Scholar] [CrossRef] [Green Version]
- Simmons, L.H.; Guimaraes, A.R.; Zukerberg, L.R. Case records of the Massachusetts General Hospital. Case 6-2013. A 54-year-old man with recurrent diarrhea. N. Engl. J. Med. 2013, 368, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, S.; Blau, J.E.; Koh, C. Acute oesophageal necrosis in multiple endocrine neoplasia type 1: An undescribed complication. BMJ Case. Rep. 2021, 14, e238214. [Google Scholar] [CrossRef]
- Hoffmann, K.M.; Gibril, F.; Entsuah, L.K.; Serrano, J.; Jensen, R.T. Patients with multiple endocrine neoplasia type 1 with gastrinomas have an increased risk of severe esophageal disease including stricture and the premalignant condition, Barrett’s esophagus. J. Clin. Endocrinol. Metab. 2006, 91, 204–212. [Google Scholar] [CrossRef] [Green Version]
- Matsubayashi, H.; Kawata, N.; Kakushima, N.; Tanaka, M.; Takizawa, K.; Kiyozumi, Y.; Horiuchi, Y.; Sasaki, K.; Sugiura, T.; Uesaka, K.; et al. A case of type 1 multiple endocrine neoplasia with esophageal stricture successfully treated with endoscopic balloon dilation and local steroid injection combined with surgical resection of gastrinomas. BMC. Gastroenterol. 2017, 17, 37. [Google Scholar] [CrossRef] [Green Version]
- Gaztambide, S.; Vazquez, J.A. Short- and long-term effect of a long-acting somatostatin analogue, lanreotide (SR-L) on metastatic gastrinoma. J. Endocrinol. Investig. 1999, 22, 144–146. [Google Scholar] [CrossRef]
- Wilson, S.D.; Doffek, K.M.; Krzywda, E.A.; Quebbeman, E.J.; Christians, K.K.; Pappas, S.G. Zollinger-Ellison syndrome associated with a history of alcohol abuse: Coincidence or consequence? Surgery 2011, 150, 1129–1135. [Google Scholar] [CrossRef]
- Thodiyil, P.A.; El-Masry, N.S.; Williamson, R.C. Supergastrinoma: Simultaneous peptic ulceration of esophagus, stomach, and small intestine. Int. Surg. 2003, 88, 155–158. [Google Scholar]
- Franz, R.C.; Penzhorn, H.O. Is total gastrectomy still a viable option in the management of patients with the Zollinger-Ellison syndrome? S. Afr. J. Surg. 2007, 45, 58–60. [Google Scholar]
- Aamar, A.; Madhani, K.; Virk, H.; Butt, Z. Zollinger-Ellison Syndrome: A Rare Case of Chronic Diarrhea. Gastroenterol. Res. 2016, 9, 103–104. [Google Scholar] [CrossRef] [Green Version]
- Stroker, E.; Leone, L.; Vandeput, Y.; Borbath, I.; Lefebvre, C. Severe symptomatic hypomagnesaemia induced by the chronic use of proton pump inhibitors: A case report of a patient with Zollinger-Ellison syndrome. Acta Clin. Belg. 2014, 69, 62–65. [Google Scholar] [CrossRef]
- Metz, D.C.; Pisegna, J.R.; Fishbeyn, V.A.; Benya, R.V.; Feigenbaum, K.M.; Koviack, P.D.; Jensen, R.T. Currently used doses of omeprazole in Zollinger-Ellison syndrome are too high. Gastroenterology 1992, 103, 1498–1508. [Google Scholar] [CrossRef]
- Metz, D.C.; Strader, D.B.; Orbuch, M.; Koviack, P.D.; Feigenbaum, K.M.; Jensen, R.T. Use of omeprazole in Zollinger-Ellison: A prospective nine-year study of efficacy and safety. Aliment. Pharmacol. Ther. 1993, 7, 597–610. [Google Scholar] [CrossRef]
- McArthur, K.E.; Collen, M.J.; Maton, P.N.; Cherner, J.A.; Howard, J.M.; Ciarleglio, C.A.; Cornelius, M.J.; Jensen, R.T.; Gardner, J.D. Omeprazole: Effective, convenient therapy for Zollinger-Ellison syndrome. Gastroenterology 1985, 88, 939–944. [Google Scholar] [CrossRef]
- Lloyd-Davies, K.A.; Rutgersson, K.; Solvell, L. Omeprazole in the treatment of Zollinger-Ellison syndrome: A 4-year international study. Aliment. Pharmacol. Ther. 1988, 2, 13–32. [Google Scholar] [CrossRef]
- Howard, J.M.; Chremos, A.N.; Collen, M.J.; McArthur, K.E.; Cherner, J.A.; Maton, P.N.; Ciarleglio, C.A.; Cornelius, M.J.; Gardner, J.D.; Jensen, R.T. Famotidine, a new, potent, long-acting histamine H2-receptor antagonist: Comparison with cimetidine and ranitidine in the treatment of Zollinger-Ellison syndrome. Gastroenterology 1985, 88, 1026–1033. [Google Scholar] [CrossRef]
- Hirschowitz, B.I.; Simmons, J.; Mohnen, J. Long-term lansoprazole control of gastric acid and pepsin secretion in ZE and non-ZE hypersecretors: A prospective 10-year study. Aliment. Pharmacol. Ther. 2001, 15, 1795–1806. [Google Scholar] [CrossRef] [PubMed]
- Hirschowitz, B.I.; Simmons, J.; Mohnen, J. Clinical outcome using lansoprazole in acid hypersecretors with and without Zollinger-Ellison syndrome: A 13-year prospective study. Clin. Gastroenterol. Hepatol. 2005, 3, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Morocutti, A.; Merrouche, M.; Bjaaland, T.; Humphries, T.; Mignon, M. An open-label study of rabeprazole in patients with Zollinger-Ellison syndrome or idiopathic gastric acid hypersecretion. Aliment. Pharmacol. Ther. 2006, 24, 1439–1444. [Google Scholar] [CrossRef]
- Metz, D.C.; Comer, G.M.; Soffer, E.; Forsmark, C.E.; Cryer, B.; Chey, W.; Pisegna, J.R. Three-year oral pantoprazole administration is effective for patients with Zollinger-Ellison syndrome and other hypersecretory conditions. Aliment. Pharmacol. Ther. 2006, 23, 437–444. [Google Scholar] [CrossRef]
- Lehy, T.; Mignon, M.; Cadiot, G.; Elouaer-Blanc, L.; Ruszniewski, P.; Lewin, M.J.; Bonfils, S. Gastric endocrine cell behavior in Zollinger-Ellison patients upon long-term potent antisecretory treatment. Gastroenterology 1989, 96, 1029–1040. [Google Scholar] [CrossRef]
- Metz, D.C.; Sostek, M.B.; Ruszniewski, P.; Forsmark, C.E.; Monyak, J.; Pisegna, J.R. Effects of esomeprazole on Acid output in patients with zollinger-ellison syndrome or idiopathic gastric Acid hypersecretion. Am. J. Gastroenterol. 2007, 102, 2648–2654. [Google Scholar] [CrossRef]
- Riff, B.P.; Leiman, D.A.; Bennett, B.; Fraker, D.L.; Metz, D.C. Weight Gain in Zollinger-Ellison Syndrome After Acid Suppression. Pancreas 2016, 45, 193–197. [Google Scholar] [CrossRef] [Green Version]
- Strand, D.S.; Kim, D.; Peura, D.A. 25 Years of Proton Pump Inhibitors: A Comprehensive Review. Gut Liver 2017, 11, 27–37. [Google Scholar] [CrossRef]
- Katz, P.O.; Dunbar, K.B.; Schnoll-Sussman, F.H.; Greer, K.B.; Yadlapati, R.; Spechler, S.J. ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease. Am. J. Gastroenterol. 2022, 117, 27–56. [Google Scholar] [CrossRef]
- Chinzon, D.; Domingues, G.; Tosetto, N.; Perrotti, M. Safety of long-term proton pump inhibitors: Facts and myths. Arq. Gastroenterol. 2022, 59, 219–225. [Google Scholar] [CrossRef]
- Ito, T.; Jensen, R.T. Association of long-term proton pump inhibitor therapy with bone fractures and effects on absorption of calcium, vitamin b(12), iron, and magnesium. Curr. Gastroenterol. Rep. 2010, 12, 448–457. [Google Scholar] [CrossRef] [Green Version]
- Richter, J.E.; Pandol, S.J.; Castell, D.O.; McCarthy, D.M. Gastroesophageal reflux disease in the Zollinger-Ellison syndrome. Ann. Intern. Med. 1981, 95, 37–43. [Google Scholar] [CrossRef]
- Roy, P.K.; Venzon, D.J.; Shojamanesh, H.; Abou-Saif, A.; Peghini, P.; Doppman, J.L.; Gibril, F.; Jensen, R.T. Zollinger-Ellison syndrome: Clinical presentation in 261 patients. Medicine 2000, 79, 379–411. [Google Scholar] [CrossRef]
- Gibril, F.; Schumann, M.; Pace, A.; Jensen, R.T. Multiple endocrine neoplasia type 1 and Zollinger-Ellison syndrome. A prospective study of 107 cases and comparison with 1009 patients from the literature. Medicine 2004, 83, 43–83. [Google Scholar] [CrossRef]
- Norton, J.A.; Alexander, H.R.; Fraker, D.L.; Venzon, D.J.; Jensen, R.T. Does the use of routine duodenotomy (DUODX) affect rate of cure, development of liver metastases or survival in patients with Zollinger-Ellison syndrome (ZES)? Ann. Surg. 2004, 239, 617–626. [Google Scholar] [CrossRef]
- Berna, M.J.; Hoffmann, K.M.; Serrano, J.; Gibril, F.; Jensen, R.T. Serum gastrin in Zollinger-Ellison syndrome: I. Prospective study of fasting serum gastrin in 309 patients from the National Institutes of Health and comparison with 2229 cases from the literature. Medicine 2006, 85, 295–330. [Google Scholar] [CrossRef]
- Berna, M.J.; Hoffmann, K.M.; Long, S.H.; Serrano, J.; Gibril, F.; Jensen, R.T. Serum gastrin in Zollinger-Ellison syndrome: II. Prospective study of gastrin provocative testing in 293 patients from the National Institutes of Health and comparison with 537 cases from the literature. evaluation of diagnostic criteria, proposal of new criteria, and correlations with clinical and tumoral features. Medicine 2006, 85, 331–364. [Google Scholar]
- Miller, L.S.; Vinayek, R.; Frucht, H.; Gardner, J.D.; Jensen, R.T.; Maton, P.N. Reflux esophagitis in patients with Zollinger-Ellison syndrome. Gastroenterology 1990, 98, 341–346. [Google Scholar] [CrossRef]
- Metz, D.C.; Pisegna, J.R.; Ringham, G.L.; Feigenbaum, K.M.; Koviack, P.D.; Maton, P.N.; Gardner, J.D.; Jensen, R.T. Prospective study of efficacy and safety of lansoprazole in Zollinger-Ellison syndrome. Dig. Dis. Sci. 1993, 38, 245–256. [Google Scholar] [CrossRef]
- Ito, T.; Cadiot, G.; Jensen, R.T. Diagnosis of Zollinger-Ellison syndrome: Increasingly difficult. World J. Gastroenterol. 2012, 18, 5495–5503. [Google Scholar] [CrossRef]
- Ito, T.; Igarashi, H.; Jensen, R.T. Therapy of metastatic pancreatic neuroendocrine tumors (pNETs): Recent insights and advances. J. Gastroenterol. 2012, 47, 941–960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mignon, M.; Jais, P.; Cadiot, G.; Yedder, D.; Vatier, J. Clinical features and advances in biological diagnostic criteria for Zollinger-Ellison syndrome. In Endocrine Tumors of the Pancreas: Recent Advances in Research and Management. Series: Frontiers of Gastrointestinal Research; Mignon, M., Jensen, R.T., Eds.; S. Karger: Basel, Switzerland, 1995; Volume 23, pp. 223–239. [Google Scholar]
- Mignon, M.; Cadiot, G. Diagnostic and therapeutic criteria in patients with Zollinger-Ellison syndrome and multiple endocrine neoplasia type 1. J. Intern. Med. 1998, 243, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Malagelada, J.R.; Davis, C.S.; O’Fallon, W.M.; Go, V.L. Laboratory diagnosis of gastrinoma. I. A prospective evaluation of gastric analysis and fasting serum gastrin levels. Mayo Clin. Proc. 1982, 57, 211–218. [Google Scholar] [PubMed]
- Passaro, E., Jr.; Basso, N.; Walsh, J.H. Calcium challenge in the Zollinger-Ellison syndrome. Surgery 1972, 72, 60–67. [Google Scholar]
- Frucht, H.; Howard, J.M.; Slaff, J.I.; Wank, S.A.; McCarthy, D.M.; Maton, P.N.; Vinayek, R.; Gardner, J.D.; Jensen, R.T. Secretin and calcium provocative tests in the Zollinger-Ellison syndrome: A prospective study. Ann. Intern. Med. 1989, 111, 713–722. [Google Scholar] [CrossRef]
- Isenberg, J.I.; Walsh, J.H.; Passaro, E., Jr.; Moore, E.W.; Grossman, M.E. Unusual effect of secretin on serum gastrin, serum calcium and gastric acid secretion in a patient with suspected Zollinger- Ellison syndrome. Gastroenterology 1972, 62, 626–631. [Google Scholar] [CrossRef]
- Deveney, C.W.; Deveney, K.S.; Jaffe, B.M.; Jones, R.S.; Way, L.W. Use of calcium and secretin in the diagnosis of gastrinoma (Zollinger-Ellison syndrome). Ann. Intern. Med. 1977, 87, 680–686. [Google Scholar] [CrossRef]
- Gibril, F.; Reynolds, J.C.; Roy, P.K.; Peghini, P.L.; Doppman, J.L.; Jensen, R.T. Ability of somatostatin receptor scintigraphy to identify patients with localized gastric carcinoids: A prospective study. J. Nucl. Med. 2000, 41, 1646–1656. [Google Scholar]
- Maton, P.N.; Miller, D.L.; Doppman, J.L.; Collen, M.J.; Norton, J.A.; Vinayek, R.; Slaff, J.I.; Wank, S.A.; Gardner, J.D.; Jensen, R.T. Role of selective angiography in the management of Zollinger- Ellison syndrome. Gastroenterology 1987, 92, 913–918. [Google Scholar] [CrossRef]
- Doppman, J.L.; Miller, D.L.; Chang, R.; Maton, P.N.; London, J.F.; Gardner, J.D.; Jensen, R.T.; Norton, J.A. Gastrinomas: Localization by means of selective intraarterial injection of secretin. Radiology 1990, 174, 25–29. [Google Scholar] [CrossRef]
- Wank, S.A.; Doppman, J.L.; Miller, D.L.; Collen, M.J.; Maton, P.N.; Vinayek, R.; Slaff, J.I.; Norton, J.A.; Gardner, J.D.; Jensen, R.T. Prospective study of the ability of computerized axial tomography to localize gastrinomas in patients with Zollinger-Ellison syndrome. Gastroenterology 1987, 92, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Krudy, A.G.; Doppman, J.L.; Jensen, R.T.; Norton, J.A.; Collen, M.J.; Shawker, T.H.; Gardner, J.D.; McArthur, K.K.; Gorden, P. Localization of islet cell tumors by dynamic CT: Comparison with plain CT, arteriography, sonography and venous sampling. Am. J. Roentgenol. 1984, 143, 585–589. [Google Scholar] [CrossRef] [PubMed]
- London, J.F.; Shawker, T.H.; Doppman, J.L.; Frucht, H.H.; Vinayek, R.; Stark, H.A.; Miller, L.S.; Miller, D.L.; Norton, J.A.; Gardner, J.D.; et al. Zollinger-Ellison syndrome: Prospective assessment of abdominal US in the localization of gastrinomas. Radiology 1991, 178, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Frucht, H.; Doppman, J.L.; Norton, J.A.; Miller, D.L.; Dwyer, A.J.; Frank, J.A.; Vinayek, R.; Maton, P.N.; Jensen, R.T. Gastrinomas: Comparison of MR Imaging with CT, angiography and US. Radiology 1989, 171, 713–717. [Google Scholar] [CrossRef] [PubMed]
- Pisegna, J.R.; Doppman, J.L.; Norton, J.A.; Metz, D.C.; Jensen, R.T. Prospective comparative study of ability of MR imaging and other imaging modalities to localize tumors in patients with Zollinger-Ellison syndrome. Dig. Dis. Sci. 1993, 38, 1318–1328. [Google Scholar] [CrossRef] [PubMed]
- Gibril, F.; Reynolds, J.C.; Doppman, J.L.; Chen, C.C.; Venzon, D.J.; Termanini, B.; Weber, H.C.; Stewart, C.A.; Jensen, R.T. Somatostatin receptor scintigraphy: Its sensitivity compared with that of other imaging methods in detecting primary and metastatic gastrinomas: A prospective study. Ann. Intern. Med. 1996, 125, 26–34. [Google Scholar] [CrossRef]
- Norton, J.A.; Foster, D.S.; Blumgart, L.H.; Poultsides, G.A.; Visser, B.C.; Fraker, D.L.; Alexander, H.R.; Jensen, R.T. Incidence and Prognosis of Primary Gastrinomas in the Hepatobiliary Tract. JAMA Surg. 2018, 153, e175083. [Google Scholar] [CrossRef] [Green Version]
- Gibril, F.; Doppman, J.L.; Reynolds, J.C.; Chen, C.C.; Sutliff, V.E.; Yu, F.; Serrano, J.; Venzon, D.J.; Jensen, R.T. Bone metastases in patients with gastrinomas: A prospective study of bone scanning, somatostatin receptor scanning, and MRI in their detection, their frequency, location and effect of their detection on management. J. Clin. Oncol. 1998, 16, 1040–1053. [Google Scholar] [CrossRef]
- Gibril, F.; Reynolds, J.C.; Chen, C.C.; Yu, F.; Goebel, S.U.; Serrano, J.; Doppman, J.L.; Jensen, R.T. Specificity of somatostatin receptor scintigraphy: A prospective study and the effects of false positive localizations on management in patients with gastrinomas. J. Nucl. Med. 1999, 40, 539–553. [Google Scholar]
- Cherner, J.A.; Doppman, J.L.; Norton, J.A.; Miller, D.L.; Krudy, A.G.; Raufman, J.P.; Collen, M.J.; Maton, P.N.; Gardner, J.D.; Jensen, R.T. Selective venous sampling for gastrin to localize gastrinomas. A prospective study. Ann. Intern. Med. 1986, 105, 841–847. [Google Scholar] [CrossRef]
- Carty, S.E.; Jensen, R.T.; Norton, J.A. Prospective study of aggressive resection of metastatic pancreatic endocrine tumors. Surgery 1992, 112, 1024–1031. [Google Scholar] [PubMed]
- Thom, A.K.; Norton, J.A.; Axiotis, C.A.; Jensen, R.T. Location, incidence and malignant potential of duodenal gastrinomas. Surgery 1991, 110, 1086–1093. [Google Scholar] [PubMed]
- Sugg, S.L.; Norton, J.A.; Fraker, D.L.; Metz, D.C.; Pisegna, J.R.; Fishbeyn, V.; Benya, R.V.; Shawker, T.H.; Doppman, J.L.; Jensen, R.T. A prospective study of intraoperative methods to diagnose and resect duodenal gastrinomas. Ann. Surg. 1993, 218, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Norton, J.A.; Cromack, D.T.; Shawker, T.H.; Doppman, J.L.; Comi, R.; Gorden, P.; Maton, P.N.; Gardner, J.D.; Jensen, R.T. Intraoperative ultrasonographic localization of islet cell tumors. A prospective comparison to palpation. Ann. Surg. 1988, 207, 160–168. [Google Scholar] [CrossRef]
- Frucht, H.; Norton, J.A.; London, J.F.; Vinayek, R.; Doppman, J.L.; Gardner, J.D.; Jensen, R.T.; Maton, P.N. Detection of duodenal gastrinomas by operative endoscopic transillumination: A prospective study. Gastroenterology 1990, 99, 1622–1627. [Google Scholar] [CrossRef]
- von Schrenck, T.; Howard, J.M.; Doppman, J.L.; Norton, J.A.; Maton, P.N.; Smith, F.P.; Vinayek, R.; Frucht, H.; Wank, S.A.; Gardner, J.D.; et al. Prospective study of chemotherapy in patients with metastatic gastrinoma. Gastroenterology 1988, 94, 1326–1334. [Google Scholar] [CrossRef]
- Fishbeyn, V.A.; Norton, J.A.; Benya, R.V.; Pisegna, J.R.; Venzon, D.J.; Metz, D.C.; Jensen, R.T. Assessment and prediction of long-term cure in patients with Zollinger-Ellison syndrome: The best approach. Ann. Intern. Med. 1993, 119, 199–206. [Google Scholar] [CrossRef]
- Pisegna, J.R.; Norton, J.A.; Slimak, G.G.; Metz, D.C.; Maton, P.N.; Jensen, R.T. Effects of curative resection on gastric secretory function and antisecretory drug requirement in the Zollinger-Ellison syndrome. Gastroenterology 1992, 102, 767–778. [Google Scholar] [CrossRef]
- Benya, R.V.; Metz, D.C.; Venzon, D.J.; Fishbeyn, V.A.; Strader, D.B.; Orbuch, M.; Jensen, R.T. Zollinger-Ellison syndrome can be the initial endocrine manifestation in patients with multiple endocrine neoplasia-type 1. Am. J. Med. 1994, 97, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Norton, J.A.; Cornelius, M.J.; Doppman, J.L.; Maton, P.N.; Gardner, J.D.; Jensen, R.T. Effect of parathyroidectomy in patients with hyperparathyroidism, Zollinger-Ellison syndrome and multiple endocrine neoplasia Type I: A prospective study. Surgery 1987, 102, 958–966. [Google Scholar]
- Norton, J.A.; Venzon, D.J.; Berna, M.J.; Alexander, H.R.; Fraker, D.L.; Libutti, S.K.; Marx, S.J.; Gibril, F.; Jensen, R.T. Prospective study of surgery for primary hyperaparathyroidism (HPT) in Multiple Endocrine Neoplasia type 1 (MEN1), and Zollinger-Ellison syndrome (ZES): Longterm outcome of a more virulent form of HPT. Ann. Surg. 2008, 247, 501–510. [Google Scholar] [CrossRef] [Green Version]
- Jensen, R.T. Management of the Zollinger-Ellison syndrome in patients with multiple endocrine neoplasia type 1. J. Intern. Med. 1998, 243, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.T.; Norton, J.A. Treatment of Pancreatic Neuroendocrine Tumors in Multiple Endocrine Neoplasia Type 1: Some Clarity but Continued Controversy. Pancreas 2017, 46, 589–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norton, J.A.; Jensen, R.T. Current surgical management of Zollinger-Ellison syndrome (ZES) in patients without multiple endocrine neoplasia-type 1 (MEN1). Surg. Oncol. 2003, 12, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Igarashi, H.; Uehara, H.; Jensen, R.T. Pharmacotherapy of Zollinger-Ellison syndrome. Expert Opin. Pharmacotherapy 2013, 14, 307–321. [Google Scholar]
- Collen, M.J.; Howard, J.M.; McArthur, K.E.; Raufman, J.P.; Cornelius, M.J.; Ciarleglio, C.A.; Gardner, J.D.; Jensen, R.T. Comparison of ranitidine and cimetidine in the treatment of gastric hypersecretion. Ann. Intern. Med. 1984, 100, 52–58. [Google Scholar] [CrossRef]
- Jensen, R.T.; Collen, M.J.; McArthur, K.E.; Howard, J.M.; Maton, P.N.; Cherner, J.A.; Gardner, J.D. Comparison of the effectiveness of ranitidine and cimetidine in inhibiting acid secretion in patients with gastric acid hypersecretory states. Am. J. Med. 1984, 77, 90–105. [Google Scholar]
- Jensen, R.T.; Collen, M.J.; Allende, H.D.; Pandol, S.J.; Raufman, J.P.; Bissonnette, B.M.; Duncan, W.C.; Durgin, P.L.; Gillin, J.C.; Gardner, J.D. Cimetidine-induced impotence and breast changes in patients with gastric hypersecretory states. N. Engl. J. Med. 1983, 308, 883–887. [Google Scholar] [CrossRef]
- Metz, D.C.; Benya, R.V.; Fishbeyn, V.A.; Pisegna, J.R.; Orbuch, M.; Strader, D.B.; Norton, J.A.; Jensen, R.T. Prospective study of the need for long-term antisecretory therapy in patients with Zollinger-Ellison syndrome following successful curative gastrinoma resection. Aliment. Pharmacol. Ther. 1993, 7, 247–257. [Google Scholar] [CrossRef]
- Maton, P.N.; Vinayek, R.; Frucht, H.; McArthur, K.A.; Miller, L.S.; Saeed, Z.A.; Gardner, J.D.; Jensen, R.T. Long-term efficacy and safety of omeprazole in patients with Zollinger-Ellison syndrome: A prospective study. Gastroenterology 1989, 97, 827–836. [Google Scholar] [CrossRef]
- Raufman, J.P.; Collins, S.M.; Pandol, S.J.; Korman, L.Y.; Collen, M.J.; Cornelius, M.J.; Feld, M.K.; McCarthy, D.M.; Gardner, J.D.; Jensen, R.T. Reliability of symptoms in assessing control of gastric acid secretion in patients with Zollinger-Ellison syndrome. Gastroenterology 1983, 84, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Maton, P.N.; Frucht, H.; Vinayek, R.; Wank, S.A.; Gardner, J.D.; Jensen, R.T. Medical management of patients with Zollinger-Ellison syndrome who have had previous gastric surgery: A prospective study. Gastroenterology 1988, 94, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Termanini, B.; Gibril, F.; Sutliff, V.E., III; Yu, F.; Venzon, D.J.; Jensen, R.T. Effect of long-term gastric acid suppressive therapy on serum vitamin B12 levels in patients with Zollinger-Ellison syndrome. Am. J. Med. 1998, 104, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Mignon, M.; Pospai, D.; Forestier, S.; Vatier, J.; Vallot, T. Treatment of patients with Zollinger-Ellison syndrome. Clin. Ther. 1993, 15, 22–31. [Google Scholar] [PubMed]
- Graham, D.Y.; Tansel, A. Interchangeable Use of Proton Pump Inhibitors Based on Relative Potency. Clin. Gastroenterol. Hepatol. 2018, 16, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Farley, D.R.; Van Heerden, J.A.; Grant, C.S.; Miller, L.J.; Ilstrup, D.M. The Zollinger-Ellison syndrome. A collective surgical experience. Ann. Surg. 1992, 215, 561–569. [Google Scholar] [CrossRef]
- Soga, J.; Yakuwa, Y. The gastrinoma/Zollinger-Ellison syndrome: Statistical evaluation of a Japanese series of 359 cases. J. Hep. Bil. Pancr. Surg. 1998, 5, 77–85. [Google Scholar] [CrossRef]
- Mignon, M.; Ruszniewski, P.; Podevin, P.; Sabbagh, L.; Cadiot, G.; Rigaud, D.; Bonfils, S. Current approach to the management of gastrinoma and insulinoma in adults with multiple endocrine neoplasia type 1. World J. Surg. 1993, 17, 489–497. [Google Scholar] [CrossRef]
- Goudet, P.; Peschaud, F.; Mignon, M.; Nicoli-Sire, P.; Cadiot, G.; Ruszniewski, P.; Calender, A.; Murat, A.; Sarfati, E.; Peix, J.L.; et al. Les gastrinomes dans les neoplasies endocriniennes multiples de type 1. Une etude de cohorte de 127 cas du groupe des tumeurs endocrines (GTE). Ann. Chir. 2004, 129, 149–155. [Google Scholar] [CrossRef]
- Stage, J.G.; Stadil, F. The clinical diagnosis of the Zollinger-Ellison syndrome. Scand. J. Gastroenterol. Suppl. 1979, 53, 79–91. [Google Scholar]
- Eberle, F.; Grun, R. Multiple endocrine neoplasia, type I (MEN I). Ergeb. Inn. Med. Kinderheilkd 1981, 46, 76–149. [Google Scholar] [PubMed]
- Mignon, M.; Ruszniewski, P.; Haffar, S.; Rignaud, D.; Rene, E.; Bonfils, S. Current approach to the management of tumoral process in patients with gastrinoma. World J. Surg. 1986, 10, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Richardson, C.T.; Peters, M.N.; Feldman, M.; McClelland, R.N.; Walsh, J.H.; Cooper, K.A.; Willeford, G.; Dickerman, R.M.; Fordtran, J.S. Treatment of Zollinger-Ellison syndrome with exploratory laparotomy, proximal gastric vagotomy, and H2-receptor antagonists. A prospective study. Gastroenterology 1985, 89, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Norton, J.A.; Jensen, R.T. Resolved and unresolved controversies in the surgical management of patients with Zollinger-Ellison syndrome. Ann. Surg. 2004, 240, 757–773. [Google Scholar] [CrossRef]
- Norton, J.A.; Alexander, H.R.; Fraker, D.L.; Venzon, D.J.; Gibril, F.; Jensen, R.T. Comparison of surgical results in patients with advanced and limited disease with multiple endocrine neoplasia type 1 and Zollinger-Ellison syndrome. Ann. Surg. 2001, 234, 495–506. [Google Scholar] [CrossRef]
- Strader, D.B.; Benjamin, S.; Orbuch, M.; Lubensky, I.A.; Weber, C.; Gibril, F.; Jensen, R.T.; Metz, D.M. Esophageal function and occurrence of Barrett’s esophagus in Zollinger-Ellison syndrome. Digestion 1995, 56, 347–356. [Google Scholar] [CrossRef]
- Norton, J.A.; Alexander, H.A.; Fraker, D.L.; Venzon, D.J.; Gibril, F.; Jensen, R.T. Possible primary lymph node gastrinomas: Occurrence, natural history and predictive factors: A prospective study. Ann. Surg. 2003, 237, 650–659. [Google Scholar] [CrossRef]
- Arnold, W.S.; Fraker, D.L.; Alexander, H.R.; Weber, H.C.; Jensen, R.T. Apparent lymph node primary gastrinoma. Surgery 1994, 116, 1123–1130. [Google Scholar]
- Martignoni, M.E.; Friess, H.; Lubke, D.; Uhl, W.; Maurer, C.; Muller, M.; Richard, H.P.; Reubi, J.C.; Buchler, M.W. Study of a primary gastrinoma in the common hepatic duct—A case report. Digestion 1998, 60, 187–190. [Google Scholar] [CrossRef]
- Hoffmann, K.M.; Furukawa, M.; Jensen, R.T. Duodenal neuroendocrine tumors: Classification, functional syndromes, diagnosis and medical treatment. Best Pract. Res. Clin. Gastroenterol. 2005, 19, 675–697. [Google Scholar] [CrossRef]
- Bollen, E.C.M.; Lamers, C.B.; Jansen, J.B.; Larsson, L.I.; Joosten, H.J. Zollinger-Ellison syndrome due to a gastrin-producing ovarian cystadenocarcinoma. Br. J. Surg. 1981, 68, 776–777. [Google Scholar] [CrossRef] [PubMed]
- Maton, P.N.; Mackem, S.M.; Norton, J.A.; Gardner, J.D.; O’Dorisio, T.M.; Jensen, R.T. Ovarian carcinoma as a cause of Zollinger-Ellison syndrome. Natural history, secretory products and response to provocative tests. Gastroenterology 1989, 97, 468–471. [Google Scholar] [CrossRef]
- Rafieian, S.; Vahedi, M.; Jahanbin, B.; Ghasemloee, A. Primary thoracic gastrinoma causing Zollinger-Ellison syndrome. Indian J. Thorac. Cardiovasc. Surg. 2021, 37, 706–709. [Google Scholar] [CrossRef] [PubMed]
- Pipek, L.Z.; Jardim, Y.J.; de Mesquita, G.H.A.; Nii, F.; Medeiros, K.A.A.; Carvalho, B.J.; Martines, D.R.; Iuamoto, L.R.; Waisberg, D.R.; D’Albuquerque, L.A.C.; et al. Large primary hepatic gastrinoma in young patient treated with trisegmentectomy: A case report and review of the literature. World J. Hepatol. 2018, 10, 517–522. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, D.M.; Hyman, P.E. Effect of isopropamide on response to oral cimetidine in patients with Zollinger-Ellison syndrome. Dig. Dis. Sci. 1982, 27, 353–359. [Google Scholar] [CrossRef]
- Lamers, C.B.H.W.; Lind, T.; Moberg, S.; Jansen, J.B.M.J.; Olbe, L. Omeprazole in Zollinger-Ellison syndrome: Effects of a single dose and of long term treatment in patients resistant to histamine H2-receptor antagonists. N. Engl. J. Med. 1984, 310, 758–761. [Google Scholar] [CrossRef]
- Vinayek, R.; Howard, J.M.; Maton, P.N.; Wank, S.A.; Slaff, J.I.; Gardner, J.D.; Jensen, R.T. Famotidine in the therapy of gastric hypersecretory states. Am. J. Med. 1986, 81, 49–59. [Google Scholar] [CrossRef]
- Jensen, R.T.; Metz, D.C.; Koviack, P.D.; Feigenbaum, K.M. Prospective study of the long-term efficacy and safety of lansoprazole in patients with Zollinger-Ellison syndrome. Aliment. Pharmacol. Ther. 1993, 7, 41–50. [Google Scholar] [CrossRef]
- Maton, P.N.; Lack, E.E.; Collen, M.J.; Cornelius, M.J.; David, E.; Gardner, J.D.; Jensen, R.T. The effect of Zollinger-Ellison syndrome and omeprazole therapy on gastric oxyntic endocrine cells. Gastroenterology 1990, 99, 943–950. [Google Scholar] [CrossRef]
- Termanini, B.; Gibril, F.; Stewart, C.A.; Weber, H.C.; Jensen, R.T. A prospective study of the effectiveness of low dose omeprazole as initial therapy in Zollinger-Ellison syndrome. Aliment. Pharmacol. Ther. 1996, 10, 61–71. [Google Scholar] [CrossRef]
- Mignon, M.; Vallot, T.; Galmiche, J.P.; Dupas, J.L.; Bonfils, S. Interest of a combined anti-secretory treatment, cimetidine and pirenzepin, in the management of severe forms of Zollinger- Ellison syndrome. Digestion 1981, 20, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Frucht, H.; Maton, P.N.; Jensen, R.T. Use of omeprazole in patients with the Zollinger-Ellison syndrome. Dig. Dis. Sci. 1991, 36, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Meijer, J.L.; Jansen, J.B.; Lamers, C.B. Omeprazole in the treatment of Zollinger-Ellison syndrome and histamine H2-antagonist refractory ulcers. Digestion 1989, 44 (Suppl. S1), 31–39. [Google Scholar] [CrossRef] [PubMed]
- Bardram, L.; Stadil, F. Effects of omeprazole on acid secretion and acid related symptoms in patients with Zollinger-Ellison syndrome. Scand. J. Gastroenterol. 1989, 24, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.T. Overview of chronic diarrhea caused by functional neuroendocrine neoplasms. Semin. Gastrointest. Dis. 1999, 10, 156–172. [Google Scholar]
- Modlin, I.M.; Jaffe, B.M.; Sank, A.; Albert, D. The early diagnosis of gastrinoma. Ann. Surg. 1982, 196, 512–517. [Google Scholar] [CrossRef]
- Jensen, R.T.; Doppman, J.L.; Gardner, J.D. Gastrinoma. In The Exocrine Pancreas: Biology, Pathobiology and Disease, 1st ed.; Go, V.L.W., Brooks, F.A., DiMagno, E.P., Gardner, J.D., Lebenthal, E., Scheele, G.A., Eds.; Raven Press: New York, NY, USA, 1986; pp. 727–744. [Google Scholar]
- Yu, F.; Venzon, D.J.; Serrano, J.; Goebel, S.U.; Doppman, J.L.; Gibril, F.; Jensen, R.T. Prospective study of the clinical course, prognostic factors and survival in patients with longstanding Zollinger-Ellison syndrome. J. Clin. Oncol. 1999, 17, 615–630. [Google Scholar] [CrossRef]
- Cadranel, J.F.; Ruszniewski, P.; Elouaer-Blanc, L.; Lehy, T.; Delchier, J.C.; Cadiot, G.; Florent, C.; Vatier, J.; Mignon, M. Long term efficacy and tolerability of omeprazole in 20 patients with severe Zollinger-Ellison syndrome. Gastroenterol. Clin. Biol. 1989, 13, 654–662. [Google Scholar]
- Desir, B.; Poitras, P. Oral pantoprazole for acid suppression in the treatment of patients with Zollinger-Ellison syndrome. Can. J. Gastroenterol. 2001, 15, 795–798. [Google Scholar] [CrossRef] [Green Version]
- Collins, J.S.A.; Buchanan, K.D.; Kennedy, T.L.; Johnston, C.F.; Ardill, J.E.S.; Sloan, J.M.; McIlrath, E.M.; Russell, C. Changing patterns in presentation and management of the Zollinger-Ellison syndrome in Northern Ireland, 1970–1988. Q. J. Med. 1991, 78, 215–225. [Google Scholar]
- Lind, T.; Olbe, L. Long term follow up of patients with Zollinger-Ellison syndrome (ZES). Acta Chir. Scand. 1989, 155, 383–388. [Google Scholar] [PubMed]
- Mortellaro, V.E.; Hochwald, S.N.; McGuigan, J.E.; Copeland, E.M.; Vogel, S.B.; Grobmyer, S.R. Long-term results of a selective surgical approach to management of Zollinger-Ellison syndrome in patients with MEN-1. Am Surg. 2009, 75, 730–733. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.T. Zollinger-Ellison syndrome. In Yamada’s Textbook of Gastroenterology, 6th ed.; Podolsky, D.K., Camilleri, M., Fitz, J.G.K.A.N., Shanahan, F., Wang, T.C., Eds.; John Wiley and Sons, Ltd.: West Sussex, UK, 2016; pp. 1078–1102. [Google Scholar]
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D.K.; Capdevila, J.; Caplin, M.; Kos-Kudla, B.; Kwekkeboom, D.; Rindi, G.; Kloppel, G.; et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016, 103, 153–171. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Lee, L.; Jensen, R.T. Treatment of symptomatic neuroendocrine tumor syndromes: Recent advances and controversies. Expert Opin. Pharmacother. 2016, 17, 2191–2205. [Google Scholar] [CrossRef] [Green Version]
- Massironi, S.; Cavalcoli, F.; Elvevi, A.; Quatrini, M.; Invernizzi, P. Somatostatin analogs in patients with Zollinger Ellison syndrome (ZES): An observational study. Endocrine 2022, 75, 942–948. [Google Scholar] [CrossRef]
- Hirschowitz, B.I.; Denen, J.; Raufman, J.-P.; LaMont, B.; Berman, R.; Humphries, T. A multicenter US study of omeprazole treatment of Zollinger- Ellison syndrome. In Gastroenterology; Wb Saunders Co-Elsevier Inc.: Philadelphia, PA, USA, 1988; Volume 94, p. A188. [Google Scholar]
- Andersen, B.N.; Larsen, N.E.; Rune, S.J.; Worning, H. Development of cimetidine resistance in Zollinger-Ellison syndrome. Gut 1985, 26, 1263–1265. [Google Scholar] [CrossRef]
- Benya, R.V.; Fathi, Z.; Battey, J.F.; Jensen, R.T. Serines and threonines in the gastrin-releasing peptide receptor carboxyl terminus mediate internalization. J. Biol. Chem. 1993, 268, 20285–20290. [Google Scholar] [CrossRef]
- McRorie, J.W.; Kirby, J.A.; Miner, P.B. Histamine2-receptor antagonists: Rapid development of tachyphylaxis with repeat dosing. World J. Gastrointest. Pharmacol. Ther. 2014, 5, 57–62. [Google Scholar] [CrossRef] [Green Version]
- Ley, L.M.; Becker, A.; Lühmann, R.; Sander, P.; Lücker, P.W. Pharmacodynamic effects of 3-day intravenous treatment with pantoprazole or ranitidine after 10 days of oral ranitidine. Methods Find. Exp. Clin. Pharmacol. 2005, 27, 25–29. [Google Scholar] [CrossRef]
- Scarpignato, C.; Gatta, L.; Zullo, A.; Blandizzi, C. Effective and safe proton pump inhibitor therapy in acid-related diseases-A position paper addressing benefits and potential harms of acid suppression. BMC. Med. 2016, 14, 179. [Google Scholar] [CrossRef]
- Lundell, L.; Miettinen, P.; Myrvold, H.E.; Hatlebakk, J.G.; Wallin, L.; Malm, A.; Sutherland, I.; Walan, A. Seven-year follow-up of a randomized clinical trial comparing proton-pump inhibition with surgical therapy for reflux oesophagitis. Br. J. Surg. 2007, 94, 198–203. [Google Scholar] [CrossRef]
- Nehra, A.K.; Alexander, J.A.; Loftus, C.G.; Nehra, V. Proton Pump Inhibitors: Review of Emerging Concerns. Mayo Clin. Proc. 2018, 93, 240–246. [Google Scholar] [CrossRef] [Green Version]
- Stewart, C.A.; Termanini, B.; Sutliff, V.E.; Serrano, J.; Yu, F.; Gibril, F.; Jensen, R.T. Assessment of the risk of iron malabsorption in patients with Zollinger-Ellison syndrome treated with long-term gastric acid antisecretory therapy. Aliment. Pharmacol. Ther. 1998, 12, 83–98. [Google Scholar] [CrossRef]
- Yibirin, M.; De Oliveira, D.; Valera, R.; Plitt, A.E.; Lutgen, S. Adverse Effects Associated with Proton Pump Inhibitor Use. Cureus 2021, 13, e12759. [Google Scholar] [CrossRef]
- Heidelbaugh, J.J.; Kim, A.H.; Chang, R.; Walker, P.C. Overutilization of proton-pump inhibitors: What the clinician needs to know. Therap. Adv. Gastroenterol. 2012, 5, 219–232. [Google Scholar] [CrossRef] [Green Version]
- Farrell, B.; Pottie, K.; Thompson, W.; Boghossian, T.; Pizzola, L.; Rashid, F.J.; Rojas-Fernandez, C.; Walsh, K.; Welch, V.; Moayyedi, P. Deprescribing proton pump inhibitors: Evidence-based clinical practice guideline. Can. Fam. Physician 2017, 63, 354–364. [Google Scholar]
- Jensen, R.T.; Cadiot, G.; Brandi, M.L.; de Herder, W.W.; Kaltsas, G.; Komminoth, P.; Scoazec, J.Y.; Salazar, R.; Sauvanet, A.; Kianmanesh, R. ENETS Consensus Guidelines for the Management of Patients with Digestive Neuroendocrine Neoplasms: Functional Pancreatic Endocrine Tumor Syndromes. Neuroendocrinology 2012, 95, 98–119. [Google Scholar] [CrossRef] [Green Version]
- Sachs, G.; Shin, J.M.; Briving, C.; Wallmark, B.; Hersey, S. The pharmacology of the gastric acid pump: The H+, K+ ATPase. Annu. Rev. Pharmacol Toxicol. 1995, 35, 277–305. [Google Scholar] [CrossRef]
- Kuo, B.; Castell, D.O. Optimal dosing of omeprazole 40 mg daily: Effects on gastric and esophageal pH and serum gastrin in healthy controls. Am. J. Gastroenterol. 1996, 91, 1532–1538. [Google Scholar]
- Hammer, J.; Schmidt, B. Effect of splitting the dose of esomeprazole on gastric acidity and nocturnal acid breakthrough. Aliment. Pharmacol Ther. 2004, 19, 1105–1110. [Google Scholar] [CrossRef]
- Carty-Dawson, D.; Sue, S.O.; Morrill, B.; Murdock, R.H., Jr. Ranitidine versus cimetidine in the healing of erosive esophagitis. Clin. Ther. 1996, 18, 1150–1160. [Google Scholar] [CrossRef] [PubMed]
- De Giorgi, F.; Savarese, M.F.; Atteo, E.; Leone, C.A.; Cuomo, R. Medical treatment of gastro-oesophageal reflux disease. Acta Otorhinolaryngol. Ital. 2006, 26, 276–280. [Google Scholar] [PubMed]
- Cloud, M.L.; Offen, W.W.; Robinson, M. Nizatidine versus placebo in gastro-oesophageal reflux disease: A 12-week, multicentre, randomised, double-blind study. Br. J. Clin. Pract. Suppl. 1994, 76, 3–10. [Google Scholar]
- Sabesin, S.M.; Berlin, R.G.; Humphries, T.J.; Bradstreet, D.C.; Walton-Bowen, K.L.; Zaidi, S. Famotidine relieves symptoms of gastroesophageal reflux disease and heals erosions and ulcerations. Results of a multicenter, placebo-controlled, dose-ranging study. USA Merck Gastroesophageal Reflux Disease Study Group. Arch. Intern. Med. 1991, 151, 2394–2400. [Google Scholar] [CrossRef] [PubMed]
- Vezzadini, P.; Tomassetti, P.; Toni, R.; Bonora, G.; Labo, G. Omeprazole in the medical treatment of Zollinger-Ellison syndrome. Curr. Ther. Res. 1984, 35, 772–776. [Google Scholar]
- Tomassetti, P.; Salomone, T.; Migliori, M.; Campana, D.; Corinaldesi, R. Optimal treatment of Zollinger-Ellison syndrome and related conditions in elderly patients. Drugs Aging 2003, 20, 1019–1034. [Google Scholar] [CrossRef]
- Pospai, D.; Cadiot, G.; Forestier, S.; Ruszniewski, P.; Coste, T.; Escourrou, J.; Mignon, M. Efficacite et tolerance due lansoprazole dans le traitement du syndrome de Zollinger-Ellison. Gastroenterol. Clin. Biol. 1998, 22, 801–808. [Google Scholar]
- Corleto, V.; Annibale, B.; D’Ambra, G.; Saggioro, A.; Ferrua, B.; Cassetta, M.R.; Della Fave, G. Efficacy of long-term therapy with low doses of omeprazole in the control of gastric acid secretion in Zollinger-Ellison syndrome patients. Aliment. Pharmacol. Ther. 1993, 7, 167–173. [Google Scholar] [CrossRef]
- Kunz, P.L.; Reidy-Lagunes, D.; Anthony, L.B.; Bertino, E.M.; Brendtro, K.; Chan, J.A.; Chen, H.; Jensen, R.T.; Kim, M.K.; Klimstra, D.S.; et al. Consensus Guidelines for the Management and Treatment of Neuroendocrine Tumors. Pancreas 2013, 42, 557–577. [Google Scholar] [CrossRef] [Green Version]
- Fraker, D.L.; Norton, J.A.; Saeed, Z.A.; Maton, P.N.; Gardner, J.D.; Jensen, R.T. A prospective study of perioperative and postoperative control of acid hypersecretion in patients with Zollinger-Ellison syndrome. Surgery 1988, 104, 1054–1063. [Google Scholar]
- Gogel, H.K.; Buckman, M.T.; Cadieux, D.; McCarthy, D.M. Gastric secretion and hormonal interactions in multiple endocrine neoplasia type 1. Arch. Intern. Med. 1985, 145, 855–859. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, D.M.; Peikin, S.R.; Lopatin, R.N.; Long, B.W.; Spiegel, A.; Marx, S.; Brennan, A. Hyperparathyroidism a reversible cause of cimetidine-resistant gastric hypersecretion. Br. Med. J. 1979, 1, 1765–1766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKeage, K.; Blick, S.K.; Croxtall, J.D.; Lyseng-Williamson, K.A.; Keating, G.M. Esomeprazole: A review of its use in the management of gastric acid-related diseases in adults. Drugs 2008, 68, 1571–1607. [Google Scholar] [CrossRef] [PubMed]
- Hirschowitz, B.I.; Worthington, J.; Mohnen, J. Vitamin B12 deficiency in hypersecretors during long-term acid suppression with proton pump inhibitors. Aliment. Pharmacol Ther. 2008, 27, 1110–1121. [Google Scholar] [CrossRef]
- Wilcox, C.M.; Seay, T.; Arcury, J.T.; Mohnen, J.; Hirschowitz, B.I. Zollinger-Ellison syndrome: Presentation, response to therapy, and outcome. Dig. Liver Dis. 2011, 43, 439–443. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Gonzalez, L.; Calvet, X.; Roque, M.; Gabriel, R.; Pajares, J.M. Proton pump inhibitors versus H2-antagonists: A meta-analysis of their efficacy in treating bleeding peptic ulcer. Aliment. Pharmacol. Ther. 2001, 15, 917–926. [Google Scholar] [CrossRef]
- Lew, E.A.; Pisegna, J.R.; Starr, J.A.; Soffer, E.F.; Forsmark, C.; Modlin, I.M.; Walsh, J.H.; Beg, M.; Bochenek, W.; Metz, D.C. Intravenous pantoprazole rapidly controls gastric acid hypersecretion in patients with Zollinger-Ellison syndrome. Gastroenterology 2000, 118, 696–704. [Google Scholar] [CrossRef]
- Metz, D.C.; Forsmark, C.; Lew, E.A.; Starr, J.A.; Soffer, E.F.; Bochenek, W.; Pisegna, J.R. Replacement of oral proton pump inhibitors with intravenous pantoprazole to effectively control gastric acid hypersecretion in patients with Zollinger-Ellison syndrome. Am. J. Gastroenterol. 2001, 96, 3274–3280. [Google Scholar] [CrossRef]
- Shah, P.; Singh, M.H.; Yang, Y.X.; Metz, D.C. Hypochlorhydria and achlorhydria are associated with false-positive secretin stimulation testing for zollinger-ellison syndrome. Pancreas 2013, 42, 932–936. [Google Scholar] [CrossRef] [Green Version]
- Cadiot, G.; Lehy, T.; Ruszniewski, P.; Bonfils, S.; Mignon, M. Gastric endocrine cell evolution in patients with Zollinger-Ellison syndrome. Influence of gastrinoma growth and long-term omeprazole treatment. Dig. Dis. Sci. 1993, 38, 1307–1317. [Google Scholar] [CrossRef]
- Lehy, T.; Roucayrol, A.M.; Mignon, M. Histomorphological characteristics of gastric mucosa in patients with Zollinger-Ellison syndrome or autoimmune gastric atrophy: Role of gastrin and atrophying gastritis. Microsc. Res. Tech. 2000, 48, 327–338. [Google Scholar] [CrossRef]





| Characteristic | Number (%) | ||
|---|---|---|---|
| H2R (a,b) | PPI (a,c) | p-Value | |
| I. Dosing (a) | |||
| Overall (n = 303) | |||
| Initial daily dose (mg/day) | |||
| # of patients | 241 | 262 | |
| Mean ± SEM | 968 ± 62 | 71.7 ± 2.3 | |
| (Range) | (80–4800) | (20–240) | |
| Final daily dose (mg/day) | |||
| Mean ± SEM | 2440 ± 141 | 58.5 ± 2.4 | |
| (Range) | (233–14400) | (20–240) | |
| % Patients with change in daily dose | |||
| Increase | 70.0% | 12.6% | <0.0001 |
| Decrease | 2.1% | 46.9% | <0.0001 |
| No change | 27.9% | 40.5% | 0.0037 |
| % of patients with different daily doses | |||
| Lowest initial dose (i.e., H2-R ≤ 900 mg/day/PPI 20 QD/20 BID) | 154/229 (67%) | 143/261 (22%) | <0.0001 |
| Lowest final dose (i.e., H2-R ≤ 900 mg/day/PPI 20 QD/20 BID) | 61/229 (27%) | 128/261 (49%) | <0.0001 |
| Higher initial doses (i.e., ≥2300 mg/day/PPI-80 mg/day) | 31/229 (13%) | 125/261 (49%) | <0.0001 |
| Higher final doses (i.e., ≥2300 mg/day/PPI-80 mg/day) | 138/229 (60%) | 99/261 (38%) | <0.0001 |
| Short-term acid treatment (<5 yrs) with any drug (c) | |||
| Initial daily dose (mg/day) | |||
| # of patients | 124 | 60 | |
| Mean ± SEM | 1112 ± 96 | 63.3 ± 3.8 | |
| (Range) | (80–4800) | (20–120) | |
| Final daily dose (mg/day) | |||
| Mean ± SEM | 2534 ± 204 | 62.7 ± 5.0 | |
| (Range) | (90–4800) | (20–200) | |
| Long-term acid treatment (≥5 yrs) with any drug (d) | |||
| Initial daily dose (mg/day) | |||
| # of patients | 114 | 202 | |
| Mean ± SEM | 812 ± 75 | 74.2 ± 2.7 | |
| (Range) | (100–4800) | (20–240) | |
| Final daily dose (mg/day) | |||
| Mean ± SEM | 2341 ± 196 | 57.3 ± 2.7 | |
| (Range) | (200–12000) | (20–240) | |
| Characteristic | Number (%) | ||
|---|---|---|---|
| H2-R (a,b) | PPI (a,c) | p-Value | |
| I. Dosing (a) | |||
| Overall (n = 303) | |||
| Initial daily dosing frequency | |||
| # of patients | 241 | 262 | |
| Mean ± SEM | 2.85 ± 0.07 | 1.47 ± 02.3 | <0.0001 |
| (Range) | (1–6) | (1–3) | |
| Final daily dosing frequency | |||
| Mean ± SEM | 3.53 ± 0.07 | 1.48 ± 0.3 | <0.0001 |
| (Range) | (1–6) | (0–3) | |
| % Patients with change in daily dosing frequency | |||
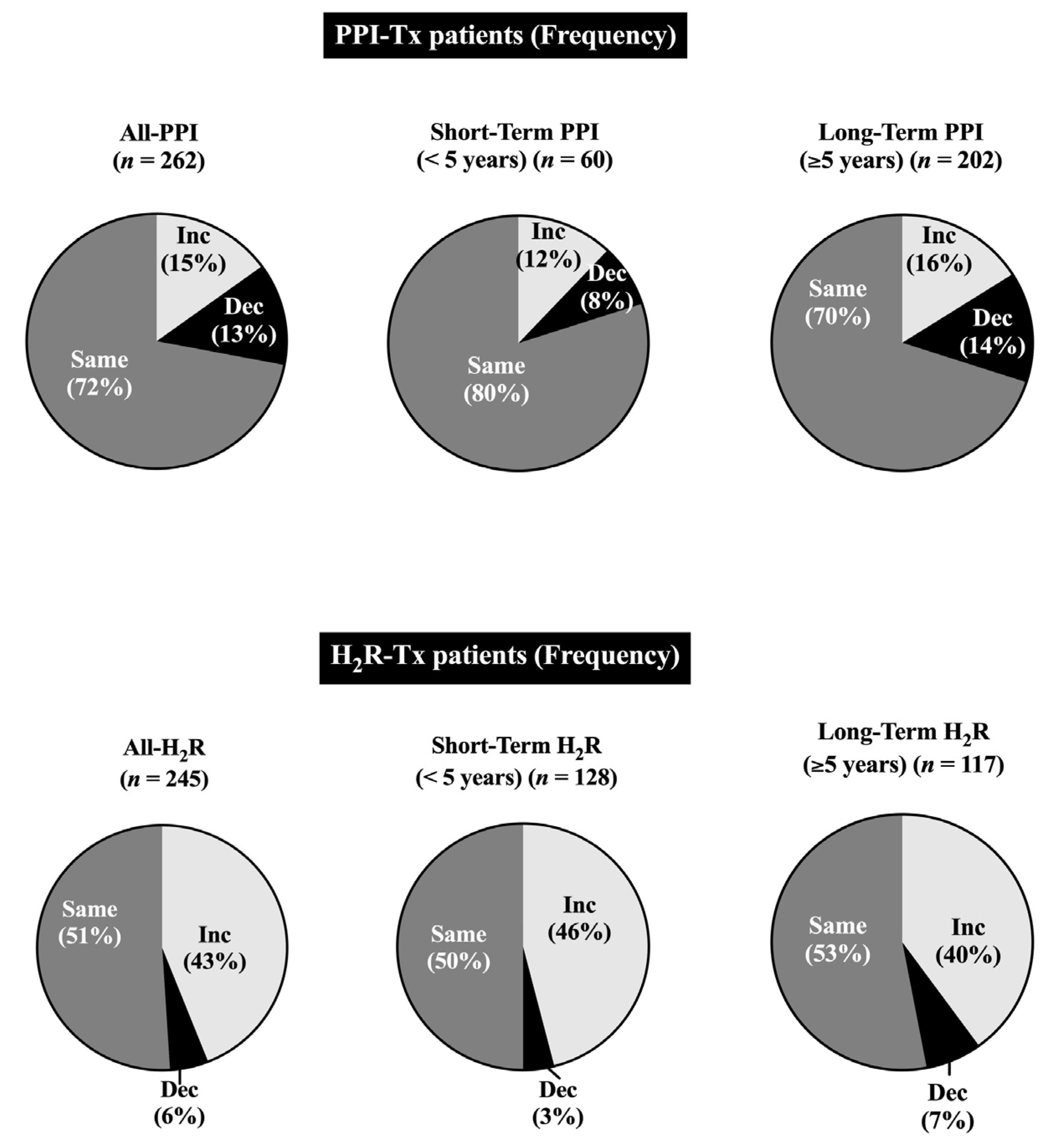
| Increase | 99/229 (43%) | 39/262 (15%) | <0.0001 |
| Decrease | 13/229 (5.6%) | 33/262 (13%) | <0.0001 |
| No change | 117/229 (51%) | 190/262 (72%) | 0.0037 |
| % of patients with different daily doses | |||
| Lower initial frequency (i.e., H2-R ≤ 3×/day/PPI ≤ 1×/day) | 104/241 (43%) | 142/262 (54%) | <0.0001 |
| Lower final frequency (i.e., H2-R ≤ 3×/day/PPI ≤ 1×/day) | 44/229 (19%) | 134/262 (51%) | <0.0001 |
| Highest initial frequency (i.e., ≥4×/DAY-H2-R/ day/ > 2/day PPI) | 86/241 (36%) | 2/262 (0.76%) | <0.0001 |
| Higher final frequency (i.e., ≥4×/H2-R/ day/ > 2/day PPI) | 150/229(66%) | 2/262 (0.76%) | <0.0001 |
| Short-term acid treatment (<5 yrs) with either H2R or PPI (c) | |||
| Initial daily dosing frequency | |||
| # of patients | 126 | 60 | |
| Mean ± SEM | 2.76 ± 0.10 | 1.28 ± 0.6 | |
| (Range) | (1–6) | (1–2) | |
| Final daily dosing frequency | |||
| Mean ± SEM | 3.54 ± 010 | 1.32 ± 0.07 | |
| (Range) | (1–6) | (1–2) | |
| Long-term acid treatment (≥5 yrs) with either H2R or PPI (c), (d) | |||
| Initial daily dosing frequency | |||
| # of patients | 117 | 202 | |
| Mean ± SEM | 2.93 ± 0.09 | 1.52 ± 0.4 | |
| (Range) | (1–5) | (1–3) | |
| Final daily dosing frequency | |||
| Mean ± SEM | 3.52 ± 0.10 | 1.52 ± 0.4 | |
| (Range) | (1–6) | (1–2) | |
| Characteristic | Number (%) | ||
|---|---|---|---|
| H2R (a,b) (n = 245) | PPI (a,b) (n = 262) | p-Value | |
| I. Acid control on treatment (a) | |||
| A. All patients- BAO -no drug (mEq/h) | |||
| Mean ± SEM | 40.1 ± 1.54 | 42.2 ± 1.6 | |
| (Range) | (1.8–159) | (6–159) | |
| B. All patients- H2R/PPI control (a) (mEq/h) | |||
| Mean ± SEM | 4.16 ± 0.46 | 2.16 ± 0.16 | <0.0001 |
| (Range) | (01–10.5) | (0–9.8) | |
| Final acid control (mEq/h) (a,b) | |||
| Mean ± SEM | 3.31 ± 0.40 | 0.97 ± 0.12 | <0.0001 |
| (Range) | (0–10.4) | (0–7) | |
| C. Level of acid control in all patients- H2R/PPI (a) (% total at initial/final treatment) | |||
| <1 mEq/h (c) | 39/130 (30%) | 207/377 (55%) | <0.0001 |
| 1–5 mEq/h (c) | 53/130 (22%) | 138/377 (37% | 0.40 |
| ≥8–10 mEq/h (c) | 23/130 (14%) | 11/377 (2.9%) | <0.0001 |
| D. Outcome of acid control-all patients | |||
| Control symptoms/acid-peptic mucosal disease | 100% | 100% | |
| Not control symptoms/acid acid-peptic mucosal disease | 0% | 0% | |
| Nr. | Summary of Key Findings |
|---|---|
| 1. | Long-term control (mean 14 yrs)/lifelong control (30%) as well as acute control of gastric acid hypersecretion by antisecretory medications was successful in all in 303 ZES patients. |
| 2. | This was only possible by individually regulating antisecretory drug doses using proven acid inhibitory secretory criteria and adjusting doses accordingly, combined with assessments of acid-peptic/GERD symptoms and UGI endoscopic findings. |
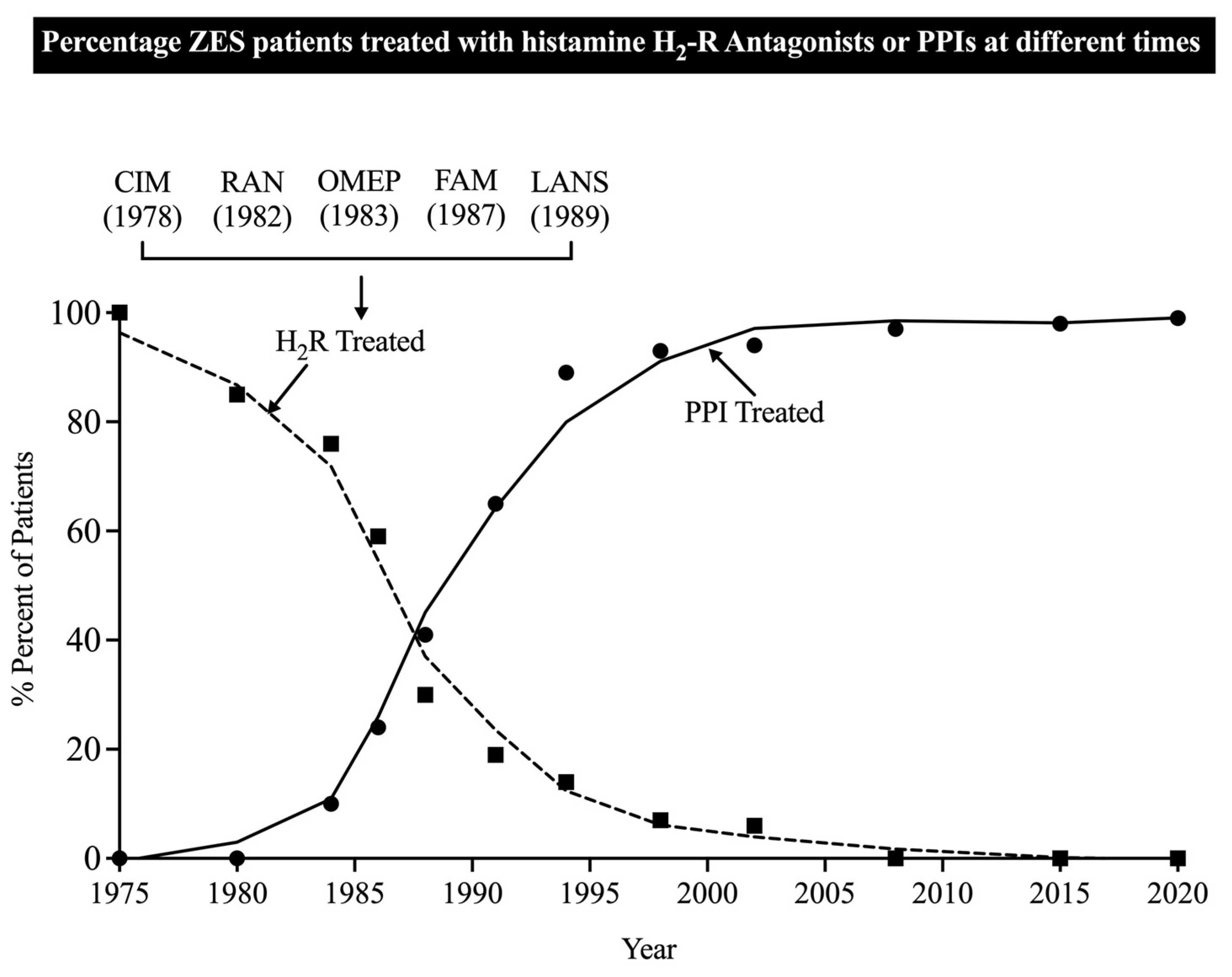
| 3. | Both H2Rs and PPIs were successfully used for both acute and maintenance control of acid hypersecretion; however, because of their greater potency and longer duration of action, PPIs are now routinely used in almost all patients. |
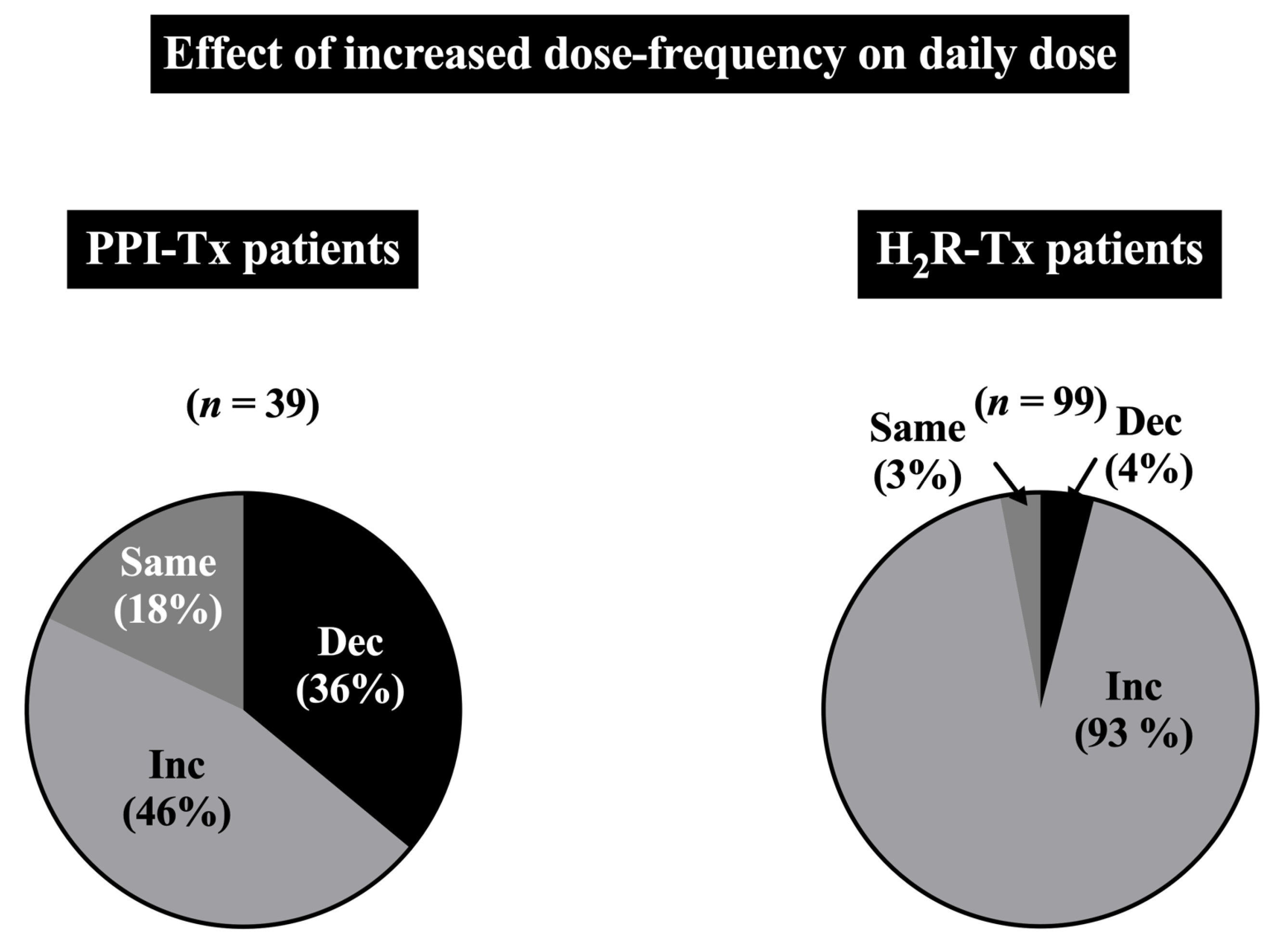
| 4. | During the initial drug dosing, the mean PPI dose was 72 mg/day, whereas with long-term treatment, half of ZES patients could have their daily PPI total dose reduced and 13% required an increase in their daily PPI dose. In contrast, with H2Rs, the mean initial dose was 969 mg/day of a ranitidine-equivalent dose (RED), with 70% of patients requiring increased daily doses and only 2% tolerating a total H2R daily dose decrease, resulting in an almost 3-fold increase in final mean final H2R daily dose (i.e., 2440 mg RED/day). |
| 5. | During long-term control of acid hypersecretion, total PPI daily use could be reduced to the lowest dose level of 20 mg QD/20 mg BID, with a 2-fold higher percentage of patients than during initial treatment, whereas the opposite occurred with H2Rs, with a 2.6-fold lower percentage of patients requiring the lowest dose. |
| 6. | H2Rs also differed from PPIs in dosing frequency. At the initial acid control, the mean frequency of H2Rs was almost 3 times/day, whereas it was 1.5 times/day for PPIs. On the final dose, the frequency of H2Rs had increased further to 3.5/day and the PPI mean frequency remained unchanged. These changes were amplified by individual patient drug frequency changes, which showed an average 3-fold greater increased dose frequency required for H2Rs compared to no change with PPIs. |
| 7. | The use of PPIs at both the initial and final drug dosing demonstrated markedly better (p < 0.001) acid control than with H2Rs. |
| 8. | Some clinical (i.e., severe GERD), laboratory (BAO, MAO), and initial acid treatment variables (presence of achlorhydria, PPI dosing frequency) correlated with the need for subsequent PPI dose changes, raising the possibility of selectively identifying patients needing dose changes and tailoring acid testing based on these variables. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ito, T.; Ramos-Alvarez, I.; Jensen, R.T. Successful Lifetime/Long-Term Medical Treatment of Acid Hypersecretion in Zollinger-Ellison Syndrome (ZES): Myth or Fact? Insights from an Analysis of Results of NIH Long-Term Prospective Studies of ZES. Cancers 2023, 15, 1377. https://doi.org/10.3390/cancers15051377
Ito T, Ramos-Alvarez I, Jensen RT. Successful Lifetime/Long-Term Medical Treatment of Acid Hypersecretion in Zollinger-Ellison Syndrome (ZES): Myth or Fact? Insights from an Analysis of Results of NIH Long-Term Prospective Studies of ZES. Cancers. 2023; 15(5):1377. https://doi.org/10.3390/cancers15051377
Chicago/Turabian StyleIto, Tetsuhide, Irene Ramos-Alvarez, and Robert T. Jensen. 2023. "Successful Lifetime/Long-Term Medical Treatment of Acid Hypersecretion in Zollinger-Ellison Syndrome (ZES): Myth or Fact? Insights from an Analysis of Results of NIH Long-Term Prospective Studies of ZES" Cancers 15, no. 5: 1377. https://doi.org/10.3390/cancers15051377