
Detection Efficacy of 68Ga-PSMA-11 PET/CT in Biochemical Recurrence of Prostate Cancer with Very Low PSA Levels: A 7-Year, Two-Center “Real-World” Experience
 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Design, Patients, and Endpoints
2.2. 68Ga–PSMA-11 PET/CT
2.3. Statistics
3. Results




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Overall scan classification, % (n) | |
| Positive | 25.2% (29) |
| Negative | 74.8% (86) |
| Suspicious lesions on positive scans | |
| Total | 44 |
| Median (minimum–maximum) | 1 (1–4) |
| Number of lesions/positive scan, % (n) | |
| 1 | 69% (20/29) |
| 2 | 14% (4/29) |
| 3 | 14% (4/29) |
| 4 | 3% (1/29) |
| Type of lesions, % (n) | |
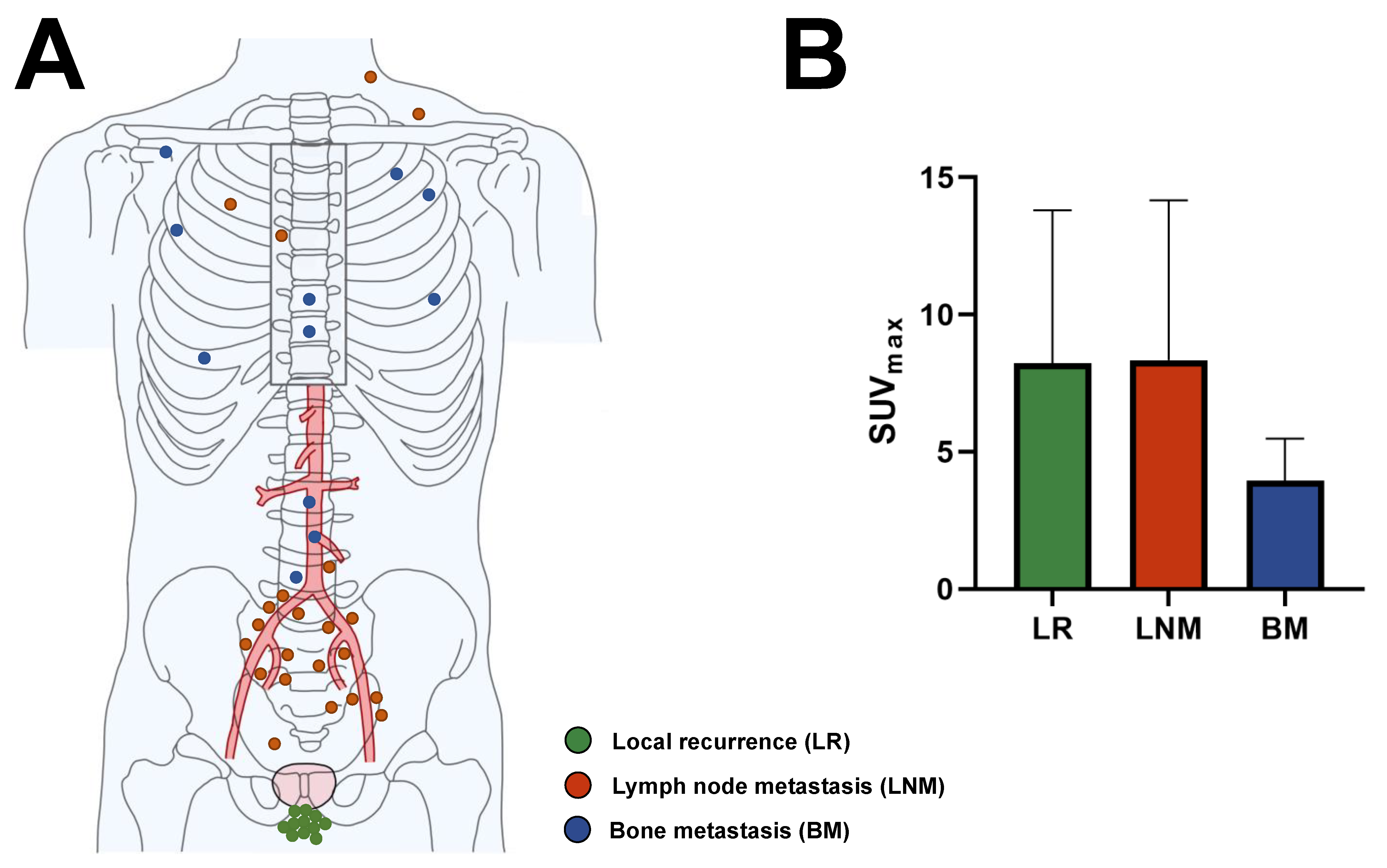
| Local recurrence | 25% (11/44) |
| Lymph node metastasis | 50% (22/44) |
| Bone metastasis | 25% (11/44) |
| Types of lesions on a positive scan, % (n) | |
| Local recurrence only | 24% (7/29) |
| Lymph node metastasis only | 34% (10/29) |
| Bone metastasis only | 24% (7/29) |
| Local recurrence + lymph node | |
| metastasis | 10% (3/29) |
| Local recurrence + bone metastasis | 3% (1/29) |
| Lymph node metastasis + bone | |
| metastasis | 3% (1/29) |
| SUVmax of suspicious lesions | |
| All suspicious lesions | |
| Median (minimum–maximum) | 5.3 (2.1–26.3) |
| Mean ± SD | 7.2 ± 5.3 |
| Local recurrence | |
| Median (minimum–maximum) | 5.7 (2.5–19.4) |
| Mean ± SD | 8.2 ± 5.6 |
| Lymph node metastasis | |
| Median (minimum–maximum) | 6.6 (2.1–26.3) |
| Mean ± SD | 8.3 ± 5.8 |
| Bone metastasis | |
| Median (minimum–maximum) | 3.3 (2.3–7.7) |
| Mean ± SD | 3.9 ± 1.5 |

4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 18F | Fluorine-18 |
| 68Ga | Gallium-68 |
| BCR | Biochemical recurrence of prostate cancer |
| BM | Bone metastasis |
| LR | Local recurrence |
| LN | Lymph node metastasis |
| MIP | Maximum intensity projection |
| NA | Not available |
| PET/CT | Positron emission tomography/computed tomography |
| p.i. | Post-injection |
| PSA | Prostate-specific antigen |
| PSMA | Prostate-specific membrane antigen |
| SD | Standard deviation |
References
- Wright, G.L., Jr.; Haley, C.; Beckett, M.L.; Schellhammer, P.F. Expression of prostate-specific membrane antigen in normal, benign, and malignant prostate tissues. Urol. Oncol. 1995, 1, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Silver, D.A.; Pellicer, I.; Fair, W.R.; Heston, W.D.; Cordon-Cardo, C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin. Cancer Res. 1997, 3, 81–85. [Google Scholar] [PubMed]
- Sweat, S.D.; Pacelli, A.; Murphy, G.P.; Bostwick, D.G. Prostate-specific membrane antigen expression is greatest in prostate adenocarcinoma and lymph node metastases. Urology 1998, 52, 637–640. [Google Scholar] [CrossRef] [PubMed]
- Farolfi, A.; Calderoni, L.; Mattana, F.; Mei, R.; Telo, S.; Fanti, S.; Castellucci, P. Current and Emerging Clinical Applications of PSMA PET Diagnostic Imaging for Prostate Cancer. J. Nucl. Med. 2021, 62, 596–604. [Google Scholar] [CrossRef] [PubMed]
- de Feria Cardet, R.E.; Hofman, M.S.; Segard, T.; Yim, J.; Williams, S.; Francis, R.J.; Frydenberg, M.; Lawrentschuk, N.; Murphy, D.G.; De Abreu Lourenco, R. Is Prostate-specific Membrane Antigen Positron Emission Tomography/Computed Tomography Imaging Cost-effective in Prostate Cancer: An Analysis Informed by the proPSMA Trial. Eur. Urol. 2021, 79, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.A.; Wieler, H.J.; Baues, C.; Kuntz, N.J.; Richardsen, I.; Schreckenberger, M. The Impact of 68Ga-PSMA PET/CT and PET/MRI on the Management of Prostate Cancer. Urology 2019, 130, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; Ng, S.; et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomised, open-label, phase 2 trial. Lancet 2021, 397, 797–804. [Google Scholar] [CrossRef]
- Khreish, F.; Ghazal, Z.; Marlowe, R.J.; Rosar, F.; Sabet, A.; Maus, S.; Linxweiler, J.; Bartholoma, M.; Ezziddin, S. 177 Lu-PSMA-617 radioligand therapy of metastatic castration-resistant prostate cancer: Initial 254-patient results from a prospective registry (REALITY Study). Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 1075–1085. [Google Scholar] [CrossRef]
- Eiber, M.; Kroenke, M.; Wurzer, A.; Ulbrich, L.; Jooss, L.; Maurer, T.; Horn, T.; Schiller, K.; Langbein, T.; Buschner, G.; et al. (18)F-rhPSMA-7 PET for the Detection of Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy. J. Nucl. Med. 2020, 61, 696–701. [Google Scholar] [CrossRef]
- Giesel, F.L.; Knorr, K.; Spohn, F.; Will, L.; Maurer, T.; Flechsig, P.; Neels, O.; Schiller, K.; Amaral, H.; Weber, W.A.; et al. Detection Efficacy of (18)F-PSMA-1007 PET/CT in 251 Patients with Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy. J. Nucl. Med. 2019, 60, 362–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, M.J.; Rowe, S.P.; Gorin, M.A.; Saperstein, L.; Pouliot, F.; Josephson, D.; Wong, J.Y.C.; Pantel, A.R.; Cho, S.Y.; Gage, K.L.; et al. Diagnostic Performance of (18)F-DCFPyL-PET/CT in Men with Biochemically Recurrent Prostate Cancer: Results from the CONDOR Phase III, Multicenter Study. Clin. Cancer Res. 2021, 27, 3674–3682. [Google Scholar] [CrossRef] [PubMed]
- Perera, M.; Papa, N.; Roberts, M.; Williams, M.; Udovicich, C.; Vela, I.; Christidis, D.; Bolton, D.; Hofman, M.S.; Lawrentschuk, N.; et al. Gallium-68 Prostate-specific Membrane Antigen Positron Emission Tomography in Advanced Prostate Cancer-Updated Diagnostic Utility, Sensitivity, Specificity, and Distribution of Prostate-specific Membrane Antigen-avid Lesions: A Systematic Review and Meta-analysis. Eur. Urol. 2020, 77, 403–417. [Google Scholar] [CrossRef] [PubMed]
- Hope, T.A.; Goodman, J.Z.; Allen, I.E.; Calais, J.; Fendler, W.P.; Carroll, P.R. Metaanalysis of (68)Ga-PSMA-11 PET Accuracy for the Detection of Prostate Cancer Validated by Histopathology. J. Nucl. Med. 2019, 60, 786–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afshar-Oromieh, A.; da Cunha, M.L.; Wagner, J.; Haberkorn, U.; Debus, N.; Weber, W.; Eiber, M.; Holland-Letz, T.; Rauscher, I. Performance of [(68)Ga]Ga-PSMA-11 PET/CT in patients with recurrent prostate cancer after prostatectomy-a multi-centre evaluation of 2533 patients. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2925–2934. [Google Scholar] [CrossRef] [PubMed]
- Meredith, G.; Wong, D.; Yaxley, J.; Coughlin, G.; Thompson, L.; Kua, B.; Gianduzzo, T. The use of (68) Ga-PSMA PET CT in men with biochemical recurrence after definitive treatment of acinar prostate cancer. BJU Int. 2016, 118 (Suppl. 3), 49–55. [Google Scholar] [CrossRef]
- van Leeuwen, P.J.; Stricker, P.; Hruby, G.; Kneebone, A.; Ting, F.; Thompson, B.; Nguyen, Q.; Ho, B.; Emmett, L. (68) Ga-PSMA has a high detection rate of prostate cancer recurrence outside the prostatic fossa in patients being considered for salvage radiation treatment. BJU Int. 2016, 117, 732–739. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.K.; Watson, T.; Denham, J.; Shakespeare, T.P.; Rutherford, N.; McLeod, N.; Picton, K.; Ainsworth, P.; Bonaventura, T.; Martin, J.M. Prostate-Specific Membrane Antigen Positron Emission Tomography-Computed Tomography for Prostate Cancer: Distribution of Disease and Implications for Radiation Therapy Planning. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 701–709. [Google Scholar] [CrossRef]
- Eiber, M.; Maurer, T.; Souvatzoglou, M.; Beer, A.J.; Ruffani, A.; Haller, B.; Graner, F.P.; Kubler, H.; Haberkorn, U.; Eisenhut, M.; et al. Evaluation of Hybrid (6)(8)Ga-PSMA Ligand PET/CT in 248 Patients with Biochemical Recurrence After Radical Prostatectomy. J. Nucl. Med. 2015, 56, 668–674. [Google Scholar] [CrossRef] [Green Version]
- Habl, G.; Sauter, K.; Schiller, K.; Dewes, S.; Maurer, T.; Eiber, M.; Combs, S.E. (68) Ga-PSMA-PET for radiation treatment planning in prostate cancer recurrences after surgery: Individualized medicine or new standard in salvage treatment. Prostate 2017, 77, 920–927. [Google Scholar] [CrossRef]
- Sanli, Y.; Kuyumcu, S.; Sanli, O.; Buyukkaya, F.; Iribas, A.; Alcin, G.; Darendeliler, E.; Ozluk, Y.; Yildiz, S.O.; Turkmen, C. Relationships between serum PSA levels, Gleason scores and results of 68Ga-PSMAPET/CT in patients with recurrent prostate cancer. Ann. Nucl. Med. 2017, 31, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Calais, J.; Kishan, A.U.; Cao, M.; Fendler, W.P.; Eiber, M.; Herrmann, K.; Ceci, F.; Reiter, R.E.; Rettig, M.B.; Hegde, J.V.; et al. Potential Impact of (68)Ga-PSMA-11 PET/CT on the Planning of Definitive Radiation Therapy for Prostate Cancer. J. Nucl. Med. 2018, 59, 1714–1721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beheshti, M.; Manafi-Farid, R.; Geinitz, H.; Vali, R.; Loidl, W.; Mottaghy, F.M.; Langsteger, W. Multiphasic (68)Ga-PSMA PET/CT in the Detection of Early Recurrence in Prostate Cancer Patients with a PSA Level of Less Than 1 ng/mL: A Prospective Study of 135 Patients. J. Nucl. Med. 2020, 61, 1484–1490. [Google Scholar] [CrossRef] [PubMed]
- Miksch, J.; Bottke, D.; Krohn, T.; Thamm, R.; Bartkowiak, D.; Solbach, C.; Bolenz, C.; Beer, M.; Wiegel, T.; Beer, A.J.; et al. Interobserver variability, detection rate, and lesion patterns of (68)Ga-PSMA-11-PET/CT in early-stage biochemical recurrence of prostate cancer after radical prostatectomy. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2339–2347. [Google Scholar] [CrossRef] [Green Version]
- Farolfi, A.; Ceci, F.; Castellucci, P.; Graziani, T.; Siepe, G.; Lambertini, A.; Schiavina, R.; Lodi, F.; Morganti, A.G.; Fanti, S. (68)Ga-PSMA-11 PET/CT in prostate cancer patients with biochemical recurrence after radical prostatectomy and PSA < 0.5 ng/mL. Efficacy and impact on treatment strategy. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 11–19. [Google Scholar] [CrossRef]
- Perry, E.; Talwar, A.; Taubman, K.; Ng, M.; Wong, L.M.; Booth, R.; Sutherland, T.R. [(18)F]DCFPyL PET/CT in detection and localization of recurrent prostate cancer following prostatectomy including low PSA < 0.5 ng/mL. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2038–2046. [Google Scholar] [CrossRef]
- Kranzbuhler, B.; Muller, J.; Becker, A.S.; Garcia Schuler, H.I.; Muehlematter, U.; Fankhauser, C.D.; Kedzia, S.; Guckenberger, M.; Kaufmann, P.A.; Eberli, D.; et al. Detection Rate and Localization of Prostate Cancer Recurrence Using (68)Ga-PSMA-11 PET/MRI in Patients with Low PSA Values ≤ 0.5 ng/mL. J. Nucl. Med. 2020, 61, 194–201. [Google Scholar] [CrossRef] [Green Version]
- Szydlo, M.; Pogoda, D.; Kowalski, T.; Pociegiel, M.; Jadwinski, M.; Amico, A. Synthesis and Quality Control of 68Ga-PSMA PET/CT Tracer Used in Prostate Cancer Imaging and Comparison with 18F-Fluorocholine as a Reference Point. J. Pharm. Sci. Emerg. Drugs 2018, 6, 1–8. [Google Scholar] [CrossRef]
- Van den Broeck, T.; van den Bergh, R.C.N.; Briers, E.; Cornford, P.; Cumberbatch, M.; Tilki, D.; De Santis, M.; Fanti, S.; Fossati, N.; Gillessen, S.; et al. Biochemical Recurrence in Prostate Cancer: The European Association of Urology Prostate Cancer Guidelines Panel Recommendations. Eur. Urol. Focus 2020, 6, 231–234. [Google Scholar] [CrossRef]
- Fendler, W.P.; Eiber, M.; Beheshti, M.; Bomanji, J.; Ceci, F.; Cho, S.; Giesel, F.; Haberkorn, U.; Hope, T.A.; Kopka, K.; et al. 68Ga-PSMA PET/CT: Joint EANM and SNMMI Procedure Guideline for Prostate Cancer Imaging: Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1014–1024. [Google Scholar] [CrossRef]
- Hoffmann, M.A.; Buchholz, H.G.; Wieler, H.J.; Hofner, T.; Muller-Hubenthal, J.; Trampert, L.; Schreckenberger, M. The positivity rate of 68Gallium-PSMA-11 ligand PET/CT depends on the serum PSA-value in patients with biochemical recurrence of prostate cancer. Oncotarget 2019, 10, 6124–6137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deek, M.P.; Van der Eecken, K.; Sutera, P.; Deek, R.A.; Fonteyne, V.; Mendes, A.A.; Decaestecker, K.; Kiess, A.P.; Lumen, N.; Phillips, R.; et al. Long-Term Outcomes and Genetic Predictors of Response to Metastasis-Directed Therapy Versus Observation in Oligometastatic Prostate Cancer: Analysis of STOMP and ORIOLE Trials. J. Clin. Oncol. 2022, 40, 3377–3382. [Google Scholar] [CrossRef] [PubMed]
- Jadvar, H.; Abreu, A.L.; Ballas, L.K.; Quinn, D.I. Oligometastatic Prostate Cancer: Current Status and Future Challenges. J. Nucl. Med. 2022, 63, 1628–1635. [Google Scholar] [CrossRef] [PubMed]
- von Deimling, M.; Rajwa, P.; Tilki, D.; Heidenreich, A.; Pallauf, M.; Bianchi, A.; Yanagisawa, T.; Kawada, T.; Karakiewicz, P.I.; Gontero, P.; et al. The current role of precision surgery in oligometastatic prostate cancer. ESMO Open 2022, 7, 100597. [Google Scholar] [CrossRef]
- Combes, A.D.; Palma, C.A.; Calopedos, R.; Wen, L.; Woo, H.; Fulham, M.; Leslie, S. PSMA PET-CT in the Diagnosis and Staging of Prostate Cancer. Diagnostics 2022, 12, 2594. [Google Scholar] [CrossRef]
- Vazquez, S.M.; Endepols, H.; Fischer, T.; Tawadros, S.G.; Hohberg, M.; Zimmermanns, B.; Dietlein, F.; Neumaier, B.; Drzezga, A.; Dietlein, M.; et al. Translational Development of a Zr-89-Labeled Inhibitor of Prostate-specific Membrane Antigen for PET Imaging in Prostate Cancer. Mol. Imaging Biol. 2022, 24, 115–125. [Google Scholar] [CrossRef]
- Prive, B.M.; Derks, Y.H.W.; Rosar, F.; Franssen, G.M.; Peters, S.M.B.; Khreish, F.; Bartholoma, M.; Maus, S.; Gotthardt, M.; Laverman, P.; et al. (89)Zr-labeled PSMA ligands for pharmacokinetic PET imaging and dosimetry of PSMA-617 and PSMA-I&T: A preclinical evaluation and first in man. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 2064–2076. [Google Scholar] [CrossRef]
- Rosar, F.; Bartholoma, M.; Maus, S.; Prive, B.M.; Khreish, F.; Franssen, G.M.; Derks, Y.H.W.; Nagarajah, J.; Ezziddin, S. 89Zr-PSMA-617 PET/CT May Reveal Local Recurrence of Prostate Cancer Unidentified by 68Ga-PSMA-11 PET/CT. Clin. Nucl. Med. 2022, 47, 435–436. [Google Scholar] [CrossRef]
- Rosar, F.; Schaefer-Schuler, A.; Bartholoma, M.; Maus, S.; Petto, S.; Burgard, C.; Prive, B.M.; Franssen, G.M.; Derks, Y.H.W.; Nagarajah, J.; et al. [(89)Zr]Zr-PSMA-617 PET/CT in biochemical recurrence of prostate cancer: First clinical experience from a pilot study including biodistribution and dose estimates. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 4736–4747. [Google Scholar] [CrossRef]
- Dietlein, F.; Kobe, C.; Vazquez, S.M.; Fischer, T.; Endepols, H.; Hohberg, M.; Reifegerst, M.; Neumaier, B.; Schomacker, K.; Drzezga, A.E.; et al. An (89)Zr-Labeled PSMA Tracer for PET/CT Imaging of Prostate Cancer Patients. J. Nucl. Med. 2022, 63, 573–583. [Google Scholar] [CrossRef]
| Characteristic | Value |
|---|---|
| Age, yr | |
| Median (minimum–maximum) | 67.6 (48.4–85.7) |
| Mean ± SD | 66.9 ± 8.0 |
| PSA, ng/mL | |
| Median (minimum–maximum) | 0.13 (0.01–0.2) |
| Mean ± SD | 0.13 ± 0.06 |
| Category, ng/mL, % (n) | |
| ≤0.1 | 33.0% (38) |
| >0.1–0.15 | 32.2% (37) |
| >0.15–0.2 | 34.8% (40) |
| PSA doubling time, months | n = 83 |
| Median (minimum–maximum) | 4.9 (0.75–24) |
| Category, % (n) | |
| <3 | 23% (19) |
| 3–6 | 29% (24) |
| >6–12 | 29% (24) |
| >12 | 19% (16) |
| Gleason score, % (n) unless otherwise noted | n = 107 |
| Minimum–maximum | 6–10 |
| 6 | 8.4% (9) |
| 7a | 33.6% (36) |
| 7b | 24.3% (26) |
| 8 | 15.0% (16) |
| 9 | 15.9% (17) |
| 10 | 2.8% (3) |
| Additional treatment besides radical prostatectomy, % (n) | |
| Radiation therapy | 8.7% (10) |
| Androgen deprivation therapy | 8.7% (10) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burgard, C.; Hoffmann, M.A.; Frei, M.; Buchholz, H.-G.; Khreish, F.; Marlowe, R.J.; Schreckenberger, M.; Ezziddin, S.; Rosar, F. Detection Efficacy of 68Ga-PSMA-11 PET/CT in Biochemical Recurrence of Prostate Cancer with Very Low PSA Levels: A 7-Year, Two-Center “Real-World” Experience. Cancers 2023, 15, 1376. https://doi.org/10.3390/cancers15051376
Burgard C, Hoffmann MA, Frei M, Buchholz H-G, Khreish F, Marlowe RJ, Schreckenberger M, Ezziddin S, Rosar F. Detection Efficacy of 68Ga-PSMA-11 PET/CT in Biochemical Recurrence of Prostate Cancer with Very Low PSA Levels: A 7-Year, Two-Center “Real-World” Experience. Cancers. 2023; 15(5):1376. https://doi.org/10.3390/cancers15051376
Chicago/Turabian StyleBurgard, Caroline, Manuela A. Hoffmann, Madita Frei, Hans-Georg Buchholz, Fadi Khreish, Robert J. Marlowe, Mathias Schreckenberger, Samer Ezziddin, and Florian Rosar. 2023. "Detection Efficacy of 68Ga-PSMA-11 PET/CT in Biochemical Recurrence of Prostate Cancer with Very Low PSA Levels: A 7-Year, Two-Center “Real-World” Experience" Cancers 15, no. 5: 1376. https://doi.org/10.3390/cancers15051376