
Sniffer Dogs Diagnose Lung Cancer by Recognition of Exhaled Gases: Using Breathing Target Samples to Train Dogs Has a Higher Diagnostic Rate Than Using Lung Cancer Tissue Samples or Urine Samples


Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Study Participants
2.3. Target and Non-Target Samples
2.4. Preparation of Lung Cancer and Non-Lung Cancer Tissue Samples
2.5. Preparation of Exhaled Breath and Urine Samples
2.6. Dog Training
2.7. Training Method
2.8. First Stage of Training
2.9. Second Stage of Training
2.10. Third Stage of Training
2.11. Ethical Issue
2.12. Statistical Analysis
3. Results
3.1. The Characteristics of Participants
3.2. Results of the Second Stage Training
3.3. Results of the Third Stage of Training
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Spiro, S.G.; Navani, N. Screening for lung cancer: Is this the way forward? Respirology 2012, 17, 237–246. [Google Scholar] [CrossRef] [Green Version]
- Mountain, C.F. Revisions in the international system for staging lung cancer. Chest 1997, 111, 1710–1717. [Google Scholar] [CrossRef] [Green Version]
- National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef] [Green Version]
- Pauling, L.; Robinson, A.B.; Teranishi, R.; Cary, P. Quantitative analysis of urine vapor and breath by gas-liquid partition chromatography. Proc. Natl. Acad. Sci. USA 1971, 68, 2374–2376. [Google Scholar] [CrossRef] [Green Version]
- Horvath, I.; Lazar, Z.; Gyulai, N.; Kollai, M.; Losonczy, G. Exhaled biomarkers in lung cancer. Eur. Respir. J. 2009, 34, 261–275. [Google Scholar] [CrossRef]
- Whittle, C.L.; Fakharzadeh, S.; Eades, J.; Preti, G. Human breath odors and their use in diagnosis. Ann. N. Y. Acad. Sci. 2007, 1098, 252–266. [Google Scholar] [CrossRef]
- Browne, C.; Stafford, K.; Fordham, R. The use of scent-detection dogs. Ir. Vet. J. 2006, 59, 97. [Google Scholar]
- Dalziel, D.J.; Uthman, B.M.; Mcgorray, S.P.; Reep, R.L. Seizure-alert dogs: A review and preliminary study. Seizure 2003, 12, 115–120. [Google Scholar] [CrossRef] [Green Version]
- Brown, S.W.; Strong, V. The use of seizure-alert dogs. Seizure 2001, 10, 39–41. [Google Scholar] [CrossRef] [Green Version]
- Gordon, R.T.; Schatz, C.B.; Myers, L.J.; Kosty, M.; Gonczy, C.; Kroener, J.; Tran, M.; Kurtzhals, P.; Heath, S.; Koziol, J.A.; et al. The use of canines in the detection of human cancers. J. Altern. Complement. Med. 2008, 14, 61–67. [Google Scholar] [CrossRef]
- Williams, H.; Pembroke, A. Sniffer dogs in the melanoma clinic? Lancet 1989, 333, 734. [Google Scholar] [CrossRef]
- Church, J.; Williams, H. Another sniffer dog for the clinic? Lancet 2001, 358, 930. [Google Scholar] [CrossRef]
- Willis, C.M.; Church, S.M.; Guest, C.M.; Cook, W.A.; McCarthy, N.; Bransbury, A.J.; Church, M.R.T.; Church, J.C.T. Olfactory detection of human bladder cancer by dogs: Proof of principle study. BMJ 2004, 329, 712. [Google Scholar] [CrossRef] [Green Version]
- McCulloch, M.; Jezierski, T.; Broffman, M.; Hubbard, A.; Turner, K.; Janecki, T. Diagnostic accuracy of canine scent detection in early-and late-stage lung and breast cancers. Integr. Cancer Ther. 2006, 5, 30–39. [Google Scholar] [CrossRef]
- Cornu, J.-N.; Cancel-Tassin, G.; Ondet, V.; Girardet, C.; Cussenot, O. Olfactory detection of prostate cancer by dogs sniffing urine: A step forward in early diagnosis. Eur. Urol. 2011, 59, 197–201. [Google Scholar] [CrossRef]
- Sonoda, H.; Kohnoe, S.; Yamazato, T.; Satoh, Y.; Morizono, G.; Shikata, K.; Morita, M.; Watanabe, A.; Kakeji, Y.; Inoue, F.; et al. Colorectal cancer screening with odour material by canine scent detection. Gut 2011, 60, 814–819. [Google Scholar] [CrossRef]
- Ehmann, R.; Boedeker, E.; Friedrich, U.; Sagert, J.; Dippon, J.; Friedel, G.; Walles, T. Canine scent detection in the diagnosis of lung cancer: Revisiting a puzzling phenomenon. Eur. Respir. J. 2012, 39, 669–676. [Google Scholar] [CrossRef] [Green Version]
- Amundsen, T.; Sundstrøm, S.; Buvik, T.; Gederaas, O.A.; Haaverstad, R. Can dogs smell lung cancer? First study using exhaled breath and urine screening in unselected patients with suspected lung cancer. Acta Oncol. 2014, 53, 307–315. [Google Scholar] [CrossRef]
- Guirao Montes, Á.; Molins López-Rodó, L.; Ramón Rodríguez, I.; Sunyer Dequigiovanni, G.; Viñolas Segarra, N.; Marrades Sicart, R.M.; Hernández Ferrández, J.; Fibla Alfara, J.J.; Agustí García-Navarro, Á. Lung cancer diagnosis by trained dogs. Eur. J. Cardio-Thorac. Surg. 2017, 52, 1206–1210. [Google Scholar] [CrossRef] [Green Version]
- Boedeker, E.; Friedel, G.; Walles, T. Sniffer dogs as part of a bimodal bionic research approach to develop a lung cancer screening. Interact. Cardiovasc. Thorac. Surg. 2012, 14, 511–515. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Xu, F.; Wang, Y.; Pan, Y.; Lu, D.; Wang, P.; Ying, K.; Chen, E.; Zhang, W. A study of the volatile organic compounds exhaled by lung cancer cells in vitro for breath diagnosis. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2007, 11, 835–844. [Google Scholar] [CrossRef]
- Pezzuto, A.; Terzo, F.; Graziani, M.L.; Ricci, A.; Bruno, P.; Mariotta, S. Lung cancer requires multidisciplinary treatment to improve patient survival: A case report. Oncol. Lett. 2017, 14, 3035–3038. [Google Scholar] [CrossRef] [Green Version]
- Feil, C.; Staib, F.; Berger, M.R.; Stein, T.; Schmidtmann, I.; Forster, A.; Schimanski, C.C. Sniffer dogs can identify lung cancer patients from breath and urine samples. BMC Cancer 2021, 21, 917. [Google Scholar] [CrossRef]
- Hackner, K.; Errhalt, P.; Mueller, M.R.; Speiser, M.; Marzluf, B.A.; Schulheim, A.; Schenk, P.; Bilek, J.; Doll, T. Canine scent detection for the diagnosis of lung cancer in a screening-like situation. J. Breath Res. 2016, 10, 046003. [Google Scholar] [CrossRef]
- Staymates, M.E.; MacCrehan, W.A.; Staymates, J.L.; Kunz, R.R.; Mendum, T.; Ong, T.H.; Geurtsen, G.; Gillen, G.J.; Craven, B.A. Biomimetic Sniffing Improves the Detection Performance of a 3D Printed Nose of a Dog and a Commercial Trace Vapor Detector. Sci. Rep. 2016, 6, 36876. [Google Scholar] [CrossRef] [Green Version]
- Kort, S.; Brusse-Keizer, M.; Schouwink, H.; Citgez, E.; de Jongh, F.; van Putten, J.; van den Borne, B.; Kastelijn, L.; Stolz, D.; Schuurbiers, M.; et al. Diagnosing Non-Small Cell Lung Cancer by Exhaled-Breath Profiling Using an Electronic Nose: A Multicenter Validation Study. Chest 2022, S0012-3692(22)03914-9. [Google Scholar] [CrossRef]
- Pitkänen, O.; Hallman, M.; Andersson, S. Determination of ethane and pentane in free oxygen radical-induced lipid peroxidation. Lipids 1989, 24, 157–159. [Google Scholar] [CrossRef]
- Rudnicka, J.; Kowalkowski, T.; Ligor, T.; Buszewski, B. Determination of volatile organic compounds as biomarkers of lung cancer by SPME-GC-TOF/MS and chemometrics. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2011, 879, 3360–3366. [Google Scholar] [CrossRef]
- Hackner, K.; Pleil, J. Canine olfaction as an alternative to analytical instruments for disease diagnosis: Understanding ‘dog personality’ to achieve reproducible results. J. Breath Res. 2017, 11, 012001. [Google Scholar] [CrossRef]
- Jezierski, T.; Walczak, M.; Ligor, T.; Rudnicka, J.; Buszewski, B. Study of the art: Canine olfaction used for cancer detection on the basis of breath odour. Perspectives and limitations. J. Breath Res. 2015, 9, 027001. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lung Cancer N (53) | Non-Lung Cancer N (6) | Healthy Controls N (20) | |
|---|---|---|---|
| Total subjects (N = 79) | 53 (67.1%) | 6 (7.6%) | 20 (25.3%) |
| Age (years ± SD) | 63.3 ± 9.5 | 56.6 ± 6.3 | 29.2 ± 2.5 |
| Gender | |||
| Male | 31 (55.4%) | 1 (16.7%) | 8 (40%) |
| Female | 24 (44.6%) | 5 (83.3%) | 12 (60%) |
| Lung cancer (N = 53) | |||
| Adenocarcinoma | 46 (58.2%) | ||
| Squamous cell carcinoma | 5 (6.3%) | ||
| Small cell lung cancer | 1 (1.3%) | ||
| Spindle cell carcinoma | 1 (1.3%) | ||
| Staging of lung cancer | |||
| Stage I | 28 (35.4%) | ||
| Stage II | 10 (12.7%) | ||
| Stage III | 10 (12.7%) | ||
| Stage IV | 5 (6.3%) | ||
| Location of tumor | |||
| RUL | 16 (30.2%) | 2 (33.2%) | |
| RML | 1 (1.9%) | 1 (16.7%) | |
| RLL | 8 (15.1%) | 1 (16.7%) | |
| LUL | 21 (39.6%) | 1 (16.7%) | |
| LLL | 7 (13.2%) | 1 (16.7%) |
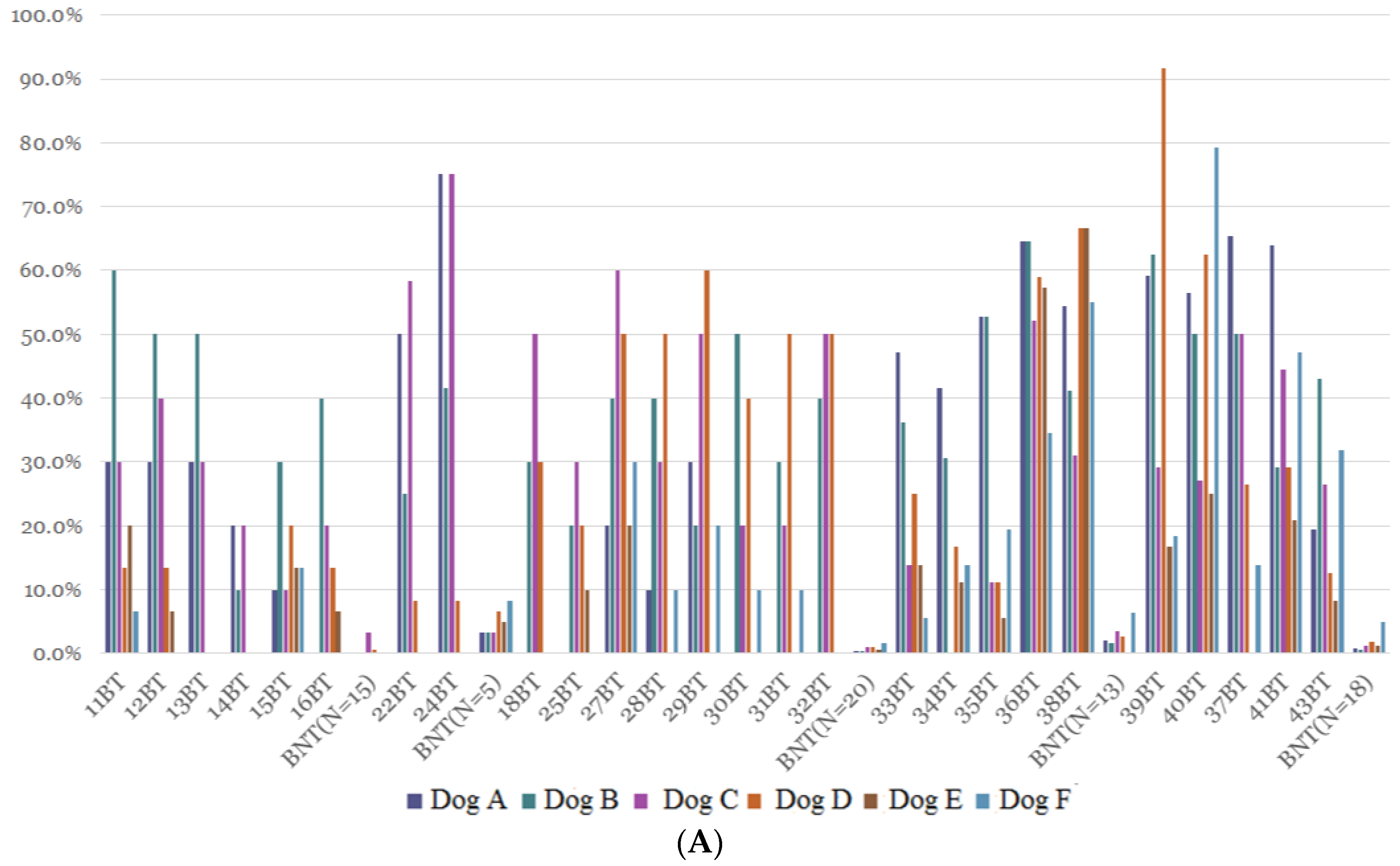
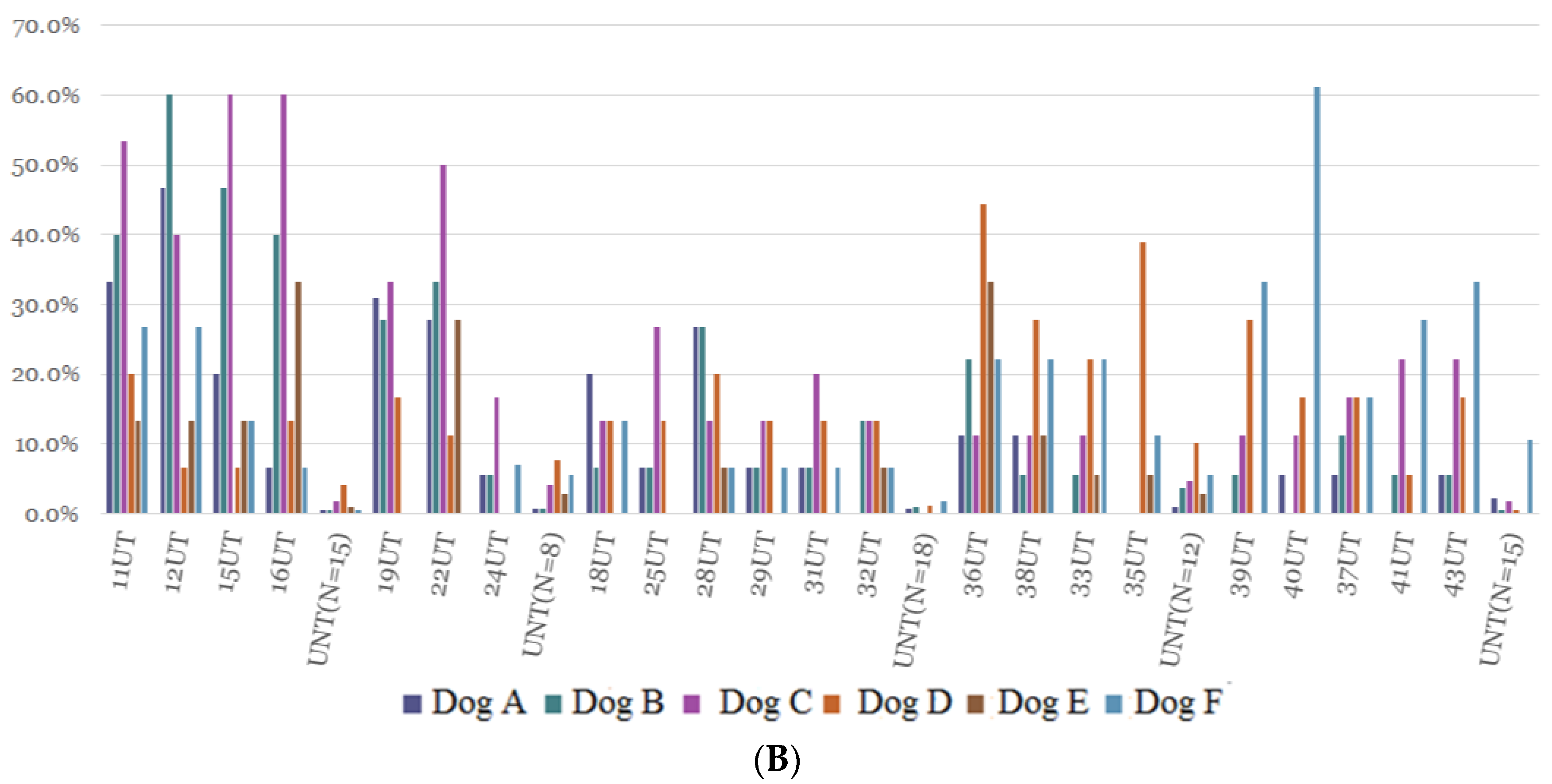
| Dog A | Dog B | Dog C | Dog D | Dog E | Dog F | Average | |
|---|---|---|---|---|---|---|---|
| BT (N = 14) (%) | 28.9 | 40.9 | 32.0 | 33.4 | 15.9 | 15.5 | 27.7 |
| BTN (N = 12) (%) | 35.4 | 38.6 | 35.9 | 29.9 | 6.6 | 16.8 | 27.2 |
| BNT (N = 71) (%) | 0.9 | 0.8 | 2.1 | 1.9 | 0.9 | 3.5 | 1.7 |
| UT (N = 13) (%) | 15.9 | 23.7 | 30.9 | 17.8 | 11.7 | 17.4 | 19.5 |
| UTN (N = 9) (%) | 7.8 | 8.2 | 14.3 | 16.3 | 2.0 | 16.1 | 10.8 |
| UNT (N = 68) (%) | 1 | 1.2 | 2.16 | 4.06 | 1.06 | 4.6 | 2.3 |
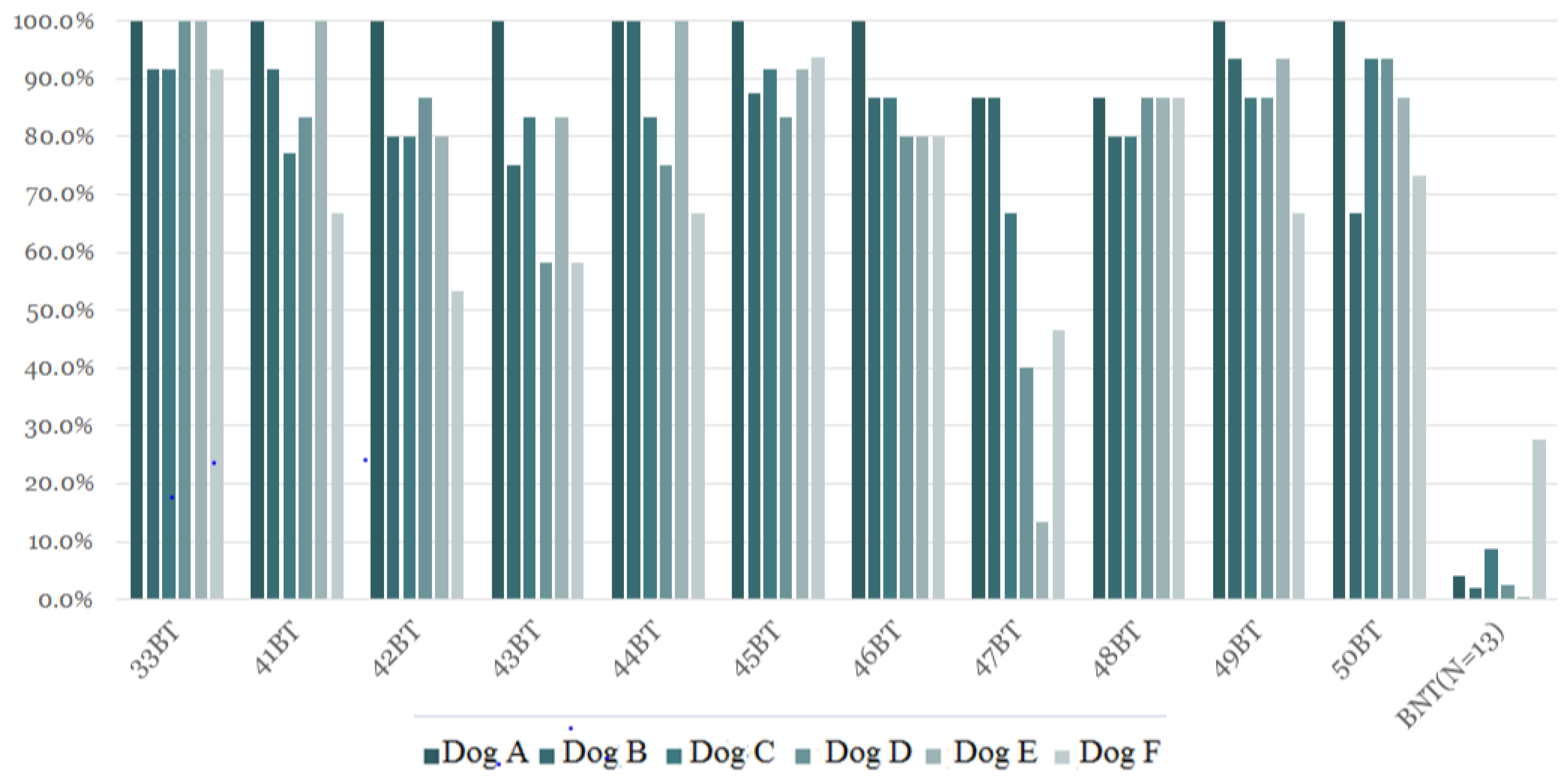
| Dog A | Dog B | Dog C | Dog D | Dog E | Dog F | Average | |
|---|---|---|---|---|---|---|---|
| BT (N = 11) (%) | 97.6 * | 85.4 * | 86.7 * | 79.4 * | 83.2 * | 71.3 * | 83.9 * |
| BNT (N = 13) (%) | 4.1 | 2.1 | 8.7 | 2.6 | 0.5 | 27.7 | 7.6 |
| A | B | C | D | E | F | Average | |
|---|---|---|---|---|---|---|---|
| BT 1 (N = 11) (%) | 97.6 * | 85.4 * | 86.7 * | 79.4 * | 83.2 * | 71.3 * | 83.9 * |
| BT 2 (N = 14) (%) | 28.9 | 40.9 | 32.0 | 33.4 | 15.9 | 15.5 | 27.7 |
| Sample | Lung Cancer Stage | Location | Dog A | Dog B | Dog C | Dog D | Dog E | Dog F |
|---|---|---|---|---|---|---|---|---|
| 33 BT | Adenocarcinoma (IIIB) | RUL | 100% | 91.7% | 91.7% | 100% | 100% | 91.7% |
| 41 BT | Adenocarcinoma (IA) | LUL | 100% | 91.7% | 77.1% | 83.3% | 100% | 66.7% |
| 42 BT | Squamous cell carcinoma (IA) | LUL | 100% | 80.0% | 80.0% | 86.7% | 80.0% | 53.3% |
| 43 BT | Adenocarcinoma (IIIA) | RUL | 100% | 75.0% | 83.3% | 58.3% | 83.3 | 58.3% |
| 44 BT | Adenocarcinoma (IA) | LUL | 100% | 100% | 83.3% | 75.0% | 100% | 66.7% |
| 45 BT | Adenocarcinoma (IA) | LLL | 100% | 87.5% | 91.7% | 83.3% | 92.7% | 93.8% |
| 46 BT | Adenocarcinoma (IIA) | LUL | 100% | 86.7% | 86.7% | 80.0% | 80.0% | 80.0% |
| 47 BT | Adenocarcinoma (IA) | RLL | 86.7% | 86.7% | 66.7% | 40.0% | 13.3% | 46.7% |
| 48 BT | Adenocarcinoma (IA) | LLL | 86.7% | 80% | 80.0% | 86.7% | 86.7% | 86.7% |
| 49 BT | Adenocarcinoma (IA) | RUL | 100% | 93.3% | 86.7% | 86.7% | 93.3% | 66.7% |
| 50 BT | Adenocarcinoma (IIIB) | LUL | 100% | 66.7% | 93.3% | 93.3% | 86.7% | 73.3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, S.-F.; Lu, H.-I.; Chi, W.-L.; Liu, G.-H.; Kuo, H.-C. Sniffer Dogs Diagnose Lung Cancer by Recognition of Exhaled Gases: Using Breathing Target Samples to Train Dogs Has a Higher Diagnostic Rate Than Using Lung Cancer Tissue Samples or Urine Samples. Cancers 2023, 15, 1234. https://doi.org/10.3390/cancers15041234
Liu S-F, Lu H-I, Chi W-L, Liu G-H, Kuo H-C. Sniffer Dogs Diagnose Lung Cancer by Recognition of Exhaled Gases: Using Breathing Target Samples to Train Dogs Has a Higher Diagnostic Rate Than Using Lung Cancer Tissue Samples or Urine Samples. Cancers. 2023; 15(4):1234. https://doi.org/10.3390/cancers15041234
Chicago/Turabian StyleLiu, Shih-Feng, Hung-I Lu, Wei-Lien Chi, Guan-Heng Liu, and Ho-Chang Kuo. 2023. "Sniffer Dogs Diagnose Lung Cancer by Recognition of Exhaled Gases: Using Breathing Target Samples to Train Dogs Has a Higher Diagnostic Rate Than Using Lung Cancer Tissue Samples or Urine Samples" Cancers 15, no. 4: 1234. https://doi.org/10.3390/cancers15041234