
Update on Prognostic and Predictive Markers in Mucinous Ovarian Cancer
 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
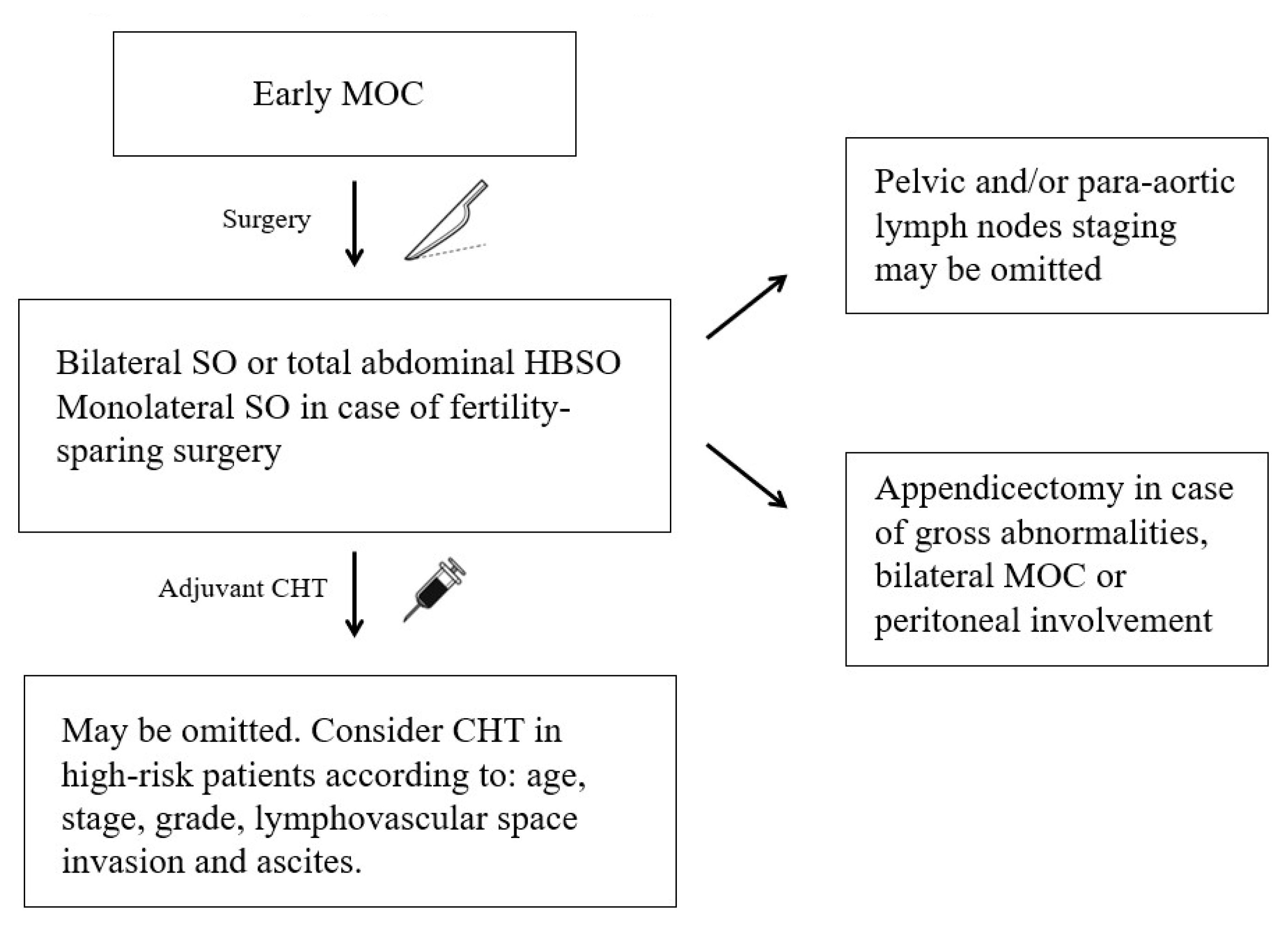
2. Early MOC
2.1. Histopathological Prognostic Factors
2.2. Surgical Prognostic Factors
2.3. Adjuvant Chemotherapy
2.4. Molecular Prognostic Factors
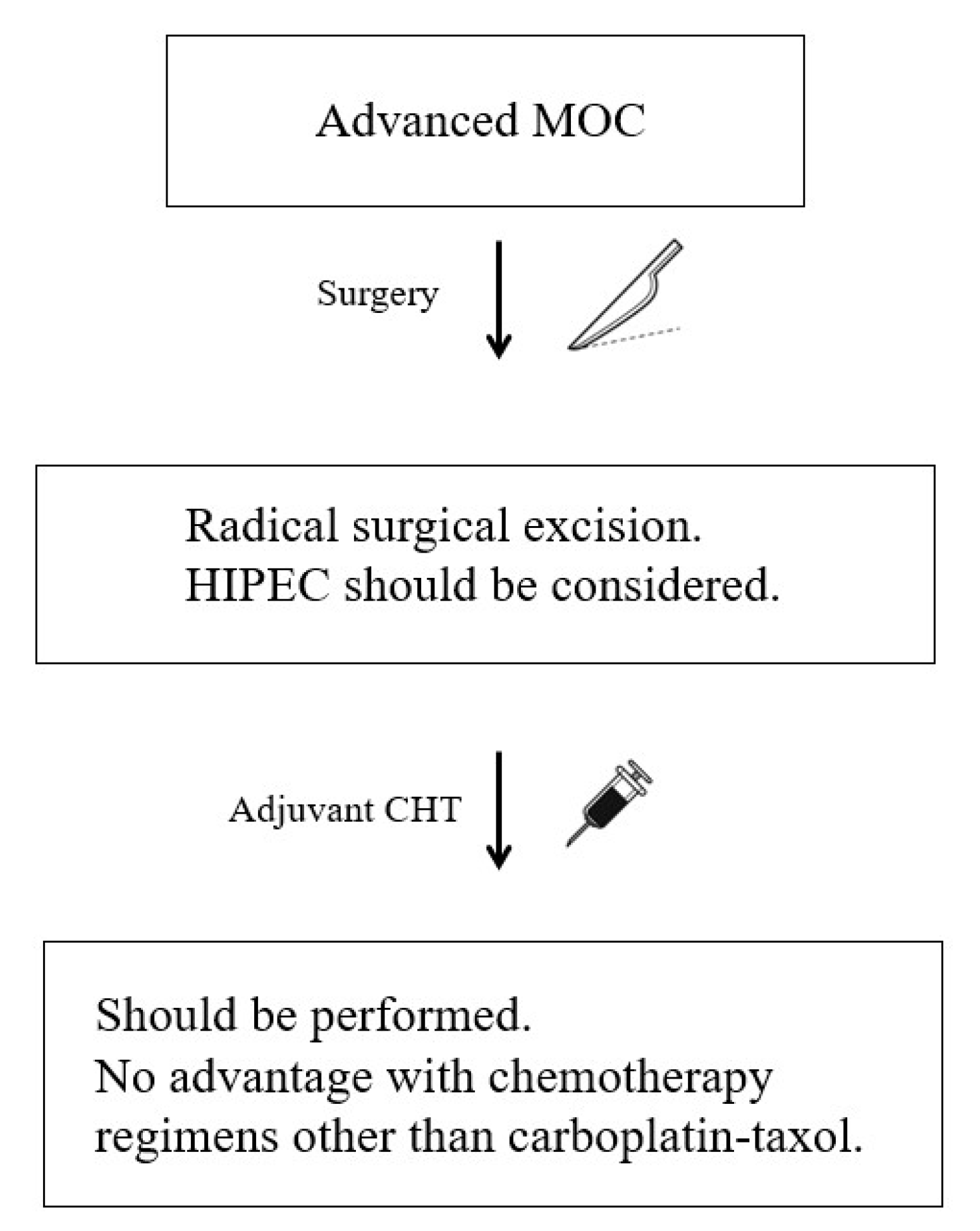
3. Advanced MOC
3.1. Histopathological Prognostic Factors
3.2. Surgical Prognostic Factors
3.3. Adjuvant Chemotherapy
3.4. Molecular Prognostic Factors
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Jelovac, D.; Armstrong, D.K. Recent progress in the diagnosis and treatment of ovarian cancer. CA Cancer J. Clin. 2011, 61, 183–203. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Lheureux, S.; Braunstein, M.; Oza, A.M. Epithelial ovarian cancer: Evolution of management in the era of precision medicine. CA Cancer J. Clin. 2019, 69, 280–304. [Google Scholar] [CrossRef] [PubMed]
- Kurman, R.J.; Shih, I.-M. The Dualistic Model of Ovarian Carcinogenesis. Am. J. Pathol. 2016, 186, 733–747. [Google Scholar] [CrossRef]
- Seidman, J.D.; Kurman, R.J.; Ronnett, B.M. Primary and Metastatic Mucinous Adenocarcinomas in the Ovaries: Incidence in Routine Practice with a New Approach to Improve Intraoperative Diagnosis. Am. J. Surg. Pathol. 2003, 27, 985–993. [Google Scholar] [CrossRef]
- Schiavone, M.B.; Herzog, T.J.; Lewin, S.N.; Deutsch, I.; Sun, X.; Burke, W.M.; Wright, J.D. Natural history and outcome of mucinous carcinoma of the ovary. Am. J. Obstet. Gynecol. 2011, 205, 480.e1–480.e8. [Google Scholar] [CrossRef]
- Yemelyanova, A.V.; Vang, R.; Judson, K.; Wu, L.-S.; Ronnett, B.M. Distinction of Primary and Metastatic Mucinous Tumors Involving the Ovary: Analysis of Size and Laterality Data by Primary Site with Reevaluation of an Algorithm for Tumor Classification. Am. J. Surg. Pathol. 2008, 32, 128–138. [Google Scholar] [CrossRef]
- McCluggage, W.G.; Rakha, E.A.; Morgan, D.; Macmillan, D. Immunohistochemistry in the distinction between primary and metastatic ovarian mucinous neoplasms. J. Clin. Pathol. 2012, 65, 596–600. [Google Scholar] [CrossRef]
- Vang, R.; Gown, A.M.; Barry, T.S.; Wheeler, D.T.; Yemelyanova, A.; Seidman, J.D.; Ronnett, B.M. Cytokeratins 7 and 20 in Primary and Secondary Mucinous Tumors of the Ovary: Analysis of Coordinate Immunohistochemical Expression Profiles and Staining Distribution in 179 Cases. Am. J. Surg. Pathol. 2006, 30, 1130–1139. [Google Scholar] [CrossRef]
- Bassiouny, D.; Ismiil, N.; Dubé, V.; Han, G.; Cesari, M.; Lu, F.-I.; Slodkowska, E.; Parra-Herran, C.; Chiu, H.F.; Naeim, M.; et al. Comprehensive Clinicopathologic and Updated Immunohistochemical Characterization of Primary Ovarian Mucinous Carcinoma. Int. J. Surg. Pathol. 2018, 26, 306–317. [Google Scholar] [CrossRef]
- Shimada, M.; Kigawa, J.; Ohishi, Y.; Yasuda, M.; Suzuki, M.; Hiura, M.; Nishimura, R.; Tabata, T.; Sugiyama, T.; Kaku, T. Clinicopathological characteristics of mucinous adenocarcinoma of the ovary. Gynecol. Oncol. 2009, 113, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Ledermann, J.A.; Luvero, D.; Shafer, A.; O’Connor, D.; Mangili, G.; Friedlander, M.; Pfisterer, J.; Mirza, M.R.; Kim, J.-W.; Alexandre, J.; et al. Gynecologic Cancer InterGroup (GCIG) Consensus Review for Mucinous Ovarian Carcinoma. Int. J. Gynecol. Cancer 2014, 24, S14–S19. [Google Scholar] [CrossRef]
- Cheasley, D.; Wakefield, M.J.; Ryland, G.L.; Allan, P.E.; Alsop, K.; Amarasinghe, K.C.; Ananda, S.; Anglesio, M.S.; Au-Yeung, G.; Böhm, M.; et al. The molecular origin and taxonomy of mucinous ovarian carcinoma. Nat. Commun. 2019, 10, 3935. [Google Scholar] [CrossRef] [PubMed]
- Seidman, J.D.; Horkayne-Szakaly, I.; Haiba, M.; Boice, C.R.; Kurman, R.J.; Ronnett, B.M. The Histologic Type and Stage Distribution of Ovarian Carcinomas of Surface Epithelial Origin. Int. J. Gynecol. Pathol. 2004, 23, 41–44. [Google Scholar] [CrossRef]
- Hess, V.; A’Hern, R.; Nasiri, N.; King, D.M.; Blake, P.R.; Barton, D.P.; Shepherd, J.H.; Ind, T.; Bridges, J.; Harrington, K.; et al. Mucinous Epithelial Ovarian Cancer: A Separate Entity Requiring Specific Treatment. J. Clin. Oncol. 2004, 22, 1040–1044. [Google Scholar] [CrossRef]
- Morice, P.; Gouy, S.; Leary, A. Mucinous Ovarian Carcinoma. N. Engl. J. Med. 2019, 380, 1256–1266. [Google Scholar] [CrossRef]
- Mackay, H.J.; Brady, M.F.; Oza, A.; Reuss, A.; Pujade-Lauraine, E.; Swart, A.M.; Siddiqui, N.; Colombo, N.; Bookman, M.A.; Pfisterer, J.; et al. Prognostic Relevance of Uncommon Ovarian Histology in Women with Stage III/IV Epithelial Ovarian Cancer. Int. J. Gynecol. Cancer 2010, 20, 945–952. [Google Scholar] [CrossRef] [PubMed]
- Simons, M.; Massuger, L.; Bruls, J.; Bulten, J.; Teerenstra, S.; Nagtegaal, I. Relatively Poor Survival of Mucinous Ovarian Carcinoma in Advanced Stage: A Systematic Review and Meta-analysis. Int. J. Gynecol. Cancer 2017, 27, 651–658. [Google Scholar] [CrossRef]
- Lee, K.R.; Scully, R.E. Mucinous Tumors of the Ovary: A Clinicopathologic Study of 196 Borderline Tumors (of Intestinal Type) and Carcinomas, Including an Evaluation of 11 Cases with Pseudomyxoma Peritonei’. Am. J. Surg. Pathol. 2000, 24, 1447–1464. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Leitao, M.M.; Tornos, C.; Soslow, R.A. Invasion patterns in stage I endometrioid and mucinous ovarian carcinomas: A clinicopathologic analysis emphasizing favorable outcomes in carcinomas without destructive stromal invasion and the occasional malignant course of carcinomas with limited destructive stromal invasion. Mod. Pathol. 2005, 18, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, A.D.; Kalloger, S.E.; Köbel, M.; Cipollone, J.; Roskelley, C.D.; Mehl, E.; Gilks, C.B. Primary Ovarian Mucinous Carcinoma of Intestinal Type: Significance of Pattern of Invasion and Immunohistochemical Expression Profile in a Series of 31 Cases. Int. J. Gynecol. Pathol. 2010, 29, 99–107. [Google Scholar] [CrossRef]
- Muyldermans, K.; Moerman, P.; Amant, F.; Leunen, K.; Neven, P.; Vergote, I. Primary invasive mucinous ovarian carcinoma of the intestinal type: Importance of the expansile versus infiltrative type in predicting recurrence and lymph node metastases. Eur. J. Cancer 2013, 49, 1600–1608. [Google Scholar] [CrossRef]
- Gouy, S.; Saidani, M.; Maulard, A.; Bach-Hamba, S.; Bentivegna, E.; Leary, A.; Pautier, P.; Devouassoux-Shisheboran, M.; Genestie, C.; Morice, P. Results of Fertility-Sparing Surgery for Expansile and Infiltrative Mucinous Ovarian Cancers. Oncologist 2017, 23, 324–327. [Google Scholar] [CrossRef]
- Kajiyama, H.; Suzuki, S.; Yoshikawa, N.; Kawai, M.; Nagasaka, T.; Kikkawa, F. Survival impact of capsule status in stage I ovarian mucinous carcinoma—A mulicentric retrospective study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 234, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Kurman, R.J.; Carcangiu, M.L.; Herrington, C.S. World Health Organisation Classification of Tumours of Female Reproductive Organs; World Health Organisation: Geneva, Switzerland, 2014.
- McCluggage, W.G.; Judge, M.J.; Clarke, B.A.; Davidson, B.; Gilks, C.B.; Hollema, H.; Ledermann, J.A.; Matias-Guiu, X.; Mikami, Y.; Stewart, C.J.; et al. Data set for reporting of ovary, fallopian tube and primary peritoneal carcinoma: Recommendations from the International Collaboration on Cancer Reporting (ICCR). Mod. Pathol. 2015, 28, 1101–1122. [Google Scholar] [CrossRef]
- Ishioka, S.-I.; Sagae, S.; Terasawa, K.; Sugimura, M.; Nishioka, Y.; Tsukada, K.; Kudo, R. Comparison of the usefulness between a new universal grading system for epithelial ovarian cancer and the FIGO grading system. Gynecol. Oncol. 2003, 89, 447–452. [Google Scholar] [CrossRef]
- Gilks, C.B.; Ionescu, D.N.; Kalloger, S.E.; Köbel, M.; Irving, J.; Clarke, B.; Santos, J.; Le, N.; Moravan, V.; Swenerton, K. Tumor cell type can be reproducibly diagnosed and is of independent prognostic significance in patients with maximally debulked ovarian carcinoma. Hum. Pathol. 2008, 39, 1239–1251. [Google Scholar] [CrossRef]
- Busca, A.; Nofech-Mozes, S.; Olkhov-Mitsel, E.; Gien, L.T.; Bassiouny, D.; Mirkovic, J.; Djordjevic, B.; Parra-Herran, C. Histological grading of ovarian mucinous carcinoma—An outcome-based analysis of traditional and novel systems. Histopathology 2020, 77, 26–34. [Google Scholar] [CrossRef]
- Rodríguez, I.M.; Prat, J. Mucinous Tumors of the Ovary: A Clinicopathologic Analysis of 75 Borderline Tumors (of Intestinal Type) and Carcinomas. Am. J. Surg. Pathol. 2002, 26, 139–152. [Google Scholar] [CrossRef]
- Shappell, H.W.; Riopel, M.A.; Sehdev, A.E.S.; Ronnett, B.M.; Kurman, R.J. Diagnostic Criteria and Behavior of Ovarian Seromucinous (Endocervical-Type Mucinous and Mixed Cell-Type) Tumors: Atypical Proliferative (Borderline) Tumors, Intraepithelial, Microinvasive, and Invasive Carcinomas. Am. J. Surg. Pathol. 2002, 26, 1529–1541. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-Y.; Jo, Y.R.; Kim, T.H.; Kim, H.S.; Kim, M.A.; Kim, J.W.; Park, N.H.; Song, Y.-S. Safety of Fertility-Sparing Surgery in Primary Mucinous Carcinoma of the Ovary. Cancer Res. Treat. 2015, 47, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Ludwick, C.; Gilks, C.B.; Miller, D.; Yaziji, H.; Clement, P.B. Aggressive Behavior of Stage I Ovarian Mucinous Tumors Lacking Extensive Infiltrative Invasion: A Report of Four Cases and Review of the Literature. Int. J. Gynecol. Pathol. 2005, 24, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Alexandre, J.; Ray-Coquard, I.; Selle, F.; Floquet, A.; Cottu, P.; Weber, B.; Falandry, C.; Lebrun, D.; Pujade-Lauraine, E. Mucinous advanced epithelial ovarian carcinoma: Clinical presentation and sensitivity to platinum–paclitaxel-based chemotherapy, the GINECO experience. Ann. Oncol. 2010, 21, 2377–2381. [Google Scholar] [CrossRef]
- Naik, J.D.; Seligmann, J.; Perren, T. Mucinous tumours of the ovary. J. Clin. Pathol. 2012, 65, 580–584. [Google Scholar] [CrossRef]
- Craig, O.; Salazar, C.; Gorringe, K.L. Options for the Treatment of Mucinous Ovarian Carcinoma. Curr. Treat. Options Oncol. 2021, 22, 114. [Google Scholar] [CrossRef] [PubMed]
- Vergote, I.; De Brabanter, J.; Fyles, A.; Bertelsen, K.; Einhorn, N.; Sevelda, P.; Gore, M.E.; Kærn, J.; Verrelst, H.; Sjövall, K.; et al. Prognostic importance of degree of differentiation and cyst rupture in stage I invasive epithelial ovarian carcinoma. Lancet 2001, 357, 176–182. [Google Scholar] [CrossRef]
- Kim, H.S.; Ahn, J.H.; Chung, H.H.; Kim, J.W.; Park, N.H.; Song, Y.S.; Lee, H.P.; Kim, Y.B. Impact of intraoperative rupture of the ovarian capsule on prognosis in patients with early-stage epithelial ovarian cancer: A meta-analysis. Eur. J. Surg. Oncol. 2013, 39, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Machida, H.; Mariani, A.; Mandelbaum, R.S.; Glaser, G.E.; Gostout, B.S.; Roman, L.D.; Wright, J.D. Adequate pelvic lymphadenectomy and survival of women with early-stage epithelial ovarian cancer. J. Gynecol. Oncol. 2018, 29, e69. [Google Scholar] [CrossRef]
- Yoshihara, M.; Kajiyama, H.; Tamauchi, S.; Iyoshi, S.; Yokoi, A.; Suzuki, S.; Kawai, M.; Nagasaka, T.; Takahashi, K.; Matsui, S.; et al. Prognostic impact of pelvic and para-aortic lymphadenectomy on clinically-apparent stage I primary mucinous epithelial ovarian carcinoma: A multi-institutional study with propensity score-weighted analysis. Jpn. J. Clin. Oncol. 2020, 50, 145–151. [Google Scholar] [CrossRef]
- Cho, Y.-H.; Kim, D.-Y.; Kim, J.-H.; Kim, Y.-M.; Kim, K.-R.; Kim, Y.-T.; Nam, J.-H. Is complete surgical staging necessary in patients with stage I mucinous epithelial ovarian tumors? Gynecol. Oncol. 2006, 103, 878–882. [Google Scholar] [CrossRef] [PubMed]
- Schmeler, K.M.; Tao, X.; Frumovitz, M.; Deavers, M.T.; Sun, C.C.; Sood, A.K.; Brown, J.; Gershenson, D.M.; Ramirez, P.T. Prevalence of Lymph Node Metastasis in Primary Mucinous Carcinoma of the Ovary. Obstet. Gynecol. 2010, 116, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Salgado-Ceballos, I.; Ríos, J.; Pérez-Montiel, D.; Gallardo, L.; Barquet-Muñoz, S.; Salcedo-Hernández, R.; Pérez-Plasencia, C.; Herrera, L.A.; de León, D.F.C. Is lymphadenectomy necessary in mucinous ovarian cancer? A single institution experience. Int. J. Surg. 2017, 41, 1–5. [Google Scholar] [CrossRef]
- Hoogendam, J.; Vlek, C.; Witteveen, P.; Verheijen, R.; Zweemer, R. Surgical lymph node assessment in mucinous ovarian carcinoma staging: A systematic review and meta-analysis. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 370–378. [Google Scholar] [CrossRef]
- Gouy, S.; Saidani, M.; Maulard, A.; Faron, M.; Bach-Hamba, S.; Bentivegna, E.; Leary, A.; Pautier, P.; Devouassoux-Shisheboran, M.; Genestie, C.; et al. Staging surgery in early-stage ovarian mucinous tumors according to expansile and infiltrative types. Gynecol. Oncol. Rep. 2017, 22, 21–25. [Google Scholar] [CrossRef]
- Heyward, Q.D.; Nasioudis, D.; Cory, L.; Haggerty, A.F.; Ko, E.M.; Latif, N. Lymphadenectomy for early-stage mucinous ovarian carcinoma. Int. J. Gynecol. Cancer 2021, 31, 104–109. [Google Scholar] [CrossRef]
- Cheng, A.; Li, M.; Kanis, M.J.; Xu, Y.; Zhang, Q.; Cui, B.; Jiang, J.; Zhang, Y.; Yang, X.; Kong, B. Is it necessary to perform routine appendectomy for mucinous ovarian neoplasms? A retrospective study and meta-analysis. Gynecol. Oncol. 2017, 144, 215–222. [Google Scholar] [CrossRef]
- Albloshi, A.; Fadare, O. Revisiting the necessity for routine appendectomies in mucinous neoplasms of the ovary: An evaluation of 460 mucinous ovarian tumors. Ann. Diagn. Pathol. 2022, 59, 151950. [Google Scholar] [CrossRef]
- Peres, L.C.; Cushing-Haugen, K.L.; Köbel, M.; Harris, H.R.; Berchuck, A.; Rossing, M.A.; Schildkraut, J.M.; Doherty, J.A. Invasive Epithelial Ovarian Cancer Survival by Histotype and Disease Stage. J. Natl. Cancer Inst. 2019, 111, 60–68. [Google Scholar] [CrossRef]
- Bentivegna, E.; Fruscio, R.; Roussin, S.; Ceppi, L.; Satoh, T.; Kajiyama, H.; Uzan, C.; Colombo, N.; Gouy, S.; Morice, P. Long-term follow-up of patients with an isolated ovarian recurrence after conservative treatment of epithelial ovarian cancer: Review of the results of an international multicenter study comprising 545 patients. Fertil. Steril. 2015, 104, 1319–1324. [Google Scholar] [CrossRef] [Green Version]
- Mueller, J.J.; Lajer, H.; Mosgaard, B.J.; Hamba, S.B.; Morice, P.; Gouy, S.; Hussein, Y.; Soslow, R.A.; Schlappe, B.A.; Zhou, Q.C.; et al. International Study of Primary Mucinous Ovarian Carcinomas Managed at Tertiary Medical Centers. Int. J. Gynecol. Cancer 2018, 28, 915–924. [Google Scholar] [CrossRef]
- Nasioudis, D.; Haggerty, A.F.; Giuntoli, R.L.; Burger, R.A.; Morgan, M.A.; Ko, E.M.; Latif, N.A. Adjuvant chemotherapy is not associated with a survival benefit for patients with early stage mucinous ovarian carcinoma. Gynecol. Oncol. 2019, 154, 302–307. [Google Scholar] [CrossRef]
- Matsuo, K.; Huang, Y.; Zivanovic, O.; Shimada, M.; Machida, H.; Grubbs, B.H.; Roman, L.D.; Wright, J.D. Effectiveness of postoperative chemotherapy for stage IC mucinous ovarian cancer. Gynecol. Oncol. 2019, 154, 505–515. [Google Scholar] [CrossRef]
- Ikeda, Y.; Yoshihara, M.; Yoshikawa, N.; Yokoi, A.; Tamauchi, S.; Nishino, K.; Niimi, K.; Kajiyama, H. Is adjuvant chemotherapy necessary for young women with early-stage epithelial ovarian cancer who have undergone fertility-sparing surgery?: A multicenter retrospective analysis. BMC Women’s Health 2022, 22, 80. [Google Scholar] [CrossRef]
- Long, X.; Li, R.; Tang, Y.; Yang, L.; Zou, D. The effect of chemotherapy in patients with stage I mucinous ovarian cancer undergoing fertility-sparing surgery. Front. Oncol. 2022, 12, 1028842. [Google Scholar] [CrossRef]
- Richardson, M.T.; Mysona, D.P.; Klein, D.A.; Mann, A.; Liao, C.-I.; Diver, E.J.; Darcy, K.M.; Tian, C.; She, J.-X.; Ghamande, S.; et al. Long term survival outcomes of stage I mucinous ovarian cancer—A clinical calculator predictive of chemotherapy benefit. Gynecol. Oncol. 2020, 159, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Engqvist, H.; Parris, T.Z.; Kovács, A.; Nemes, S.; Rönnerman, E.W.; De Lara, S.; Biermann, J.; Sundfeldt, K.; Karlsson, P.; Helou, K. Immunohistochemical validation of COL3A1, GPR158 and PITHD1 as prognostic biomarkers in early-stage ovarian carcinomas. BMC Cancer 2019, 19, 928. [Google Scholar] [CrossRef] [PubMed]
- Engqvist, H.; Parris, T.Z.; Kovács, A.; Rönnerman, E.W.; Sundfeldt, K.; Karlsson, P.; Helou, K. Validation of Novel Prognostic Biomarkers for Early-Stage Clear-Cell, Endometrioid and Mucinous Ovarian Carcinomas Using Immunohistochemistry. Front. Oncol. 2020, 10, 162. [Google Scholar] [CrossRef] [PubMed]
- Calura, E.; Fruscio, R.; Paracchini, L.; Bignotti, E.; Ravaggi, A.; Martini, P.; Sales, G.; Beltrame, L.; Clivio, L.; Ceppi, L.; et al. miRNA Landscape in Stage I Epithelial Ovarian Cancer Defines the Histotype Specificities. Clin. Cancer Res. 2013, 19, 4114–4123. [Google Scholar] [CrossRef]
- Stehling, O.; Vashisht, A.A.; Mascarenhas, J.; Jonsson, Z.O.; Sharma, T.; Netz, D.J.A.; Pierik, A.J.; Wohlschlegel, J.A.; Lill, R. MMS19 Assembles Iron-Sulfur Proteins Required for DNA Metabolism and Genomic Integrity. Science 2012, 337, 195–199. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Xiong, Y.; Yarbrough, W.G. ARF Promotes MDM2 Degradation and Stabilizes p53: ARF-INK4a Locus Deletion Impairs Both the Rb and p53 Tumor Suppression Pathways. Cell 1998, 92, 725–734. [Google Scholar] [CrossRef]
- Kim, J.H.; Yoon, S.Y.; Kim, C.-N.; Joo, J.H.; Moon, S.K.; Choe, I.S.; Choe, Y.-K.; Kim, J.W. The Bmi-1 oncoprotein is overexpressed in human colorectal cancer and correlates with the reduced p16INK4a/p14ARF proteins. Cancer Lett. 2004, 203, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Calura, E.; Paracchini, L.; Fruscio, R.; DiFeo, A.; Ravaggi, A.; Peronne, J.; Martini, P.; Sales, G.; Beltrame, L.; Bignotti, E.; et al. A prognostic regulatory pathway in stage I epithelial ovarian cancer: New hints for the poor prognosis assessment. Ann. Oncol. 2016, 27, 1511–1519. [Google Scholar] [CrossRef]
- Calura, E.; Ciciani, M.; Sambugaro, A.; Paracchini, L.; Benvenuto, G.; Milite, S.; Martini, P.; Beltrame, L.; Zane, F.; Fruscio, R.; et al. Transcriptional Characterization of Stage I Epithelial Ovarian Cancer: A Multicentric Study. Cells 2019, 8, 1554. [Google Scholar] [CrossRef]
- Velle, A.; Pesenti, C.; Grassi, T.; Beltrame, L.; Martini, P.; Jaconi, M.; Agostinis, F.; Calura, E.; Katsaros, D.; Borella, F.; et al. A comprehensive investigation of histotype-specific microRNA and their variants in stage I epithelial ovarian cancers. Int. J. Cancer 2022, ijc.34408, early view. [Google Scholar] [CrossRef]
- Pesenti, C.; Beltrame, L.; Velle, A.; Fruscio, R.; Jaconi, M.; Borella, F.; Cribiù, F.M.; Calura, E.; Venturini, L.V.; Lenoci, D.; et al. Copy number alterations in stage I epithelial ovarian cancer highlight three genomic patterns associated with prognosis. Eur. J. Cancer 2022, 171, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.; Frumovitz, M. Mucinous Tumors of the Ovary: Current Thoughts on Diagnosis and Management. Curr. Oncol. Rep. 2014, 16, 389. [Google Scholar] [CrossRef] [PubMed]
- Hollis, R.L.; Stillie, L.J.; Hopkins, S.; Bartos, C.; Churchman, M.; Rye, T.; Nussey, F.; Fegan, S.; Nirsimloo, R.; Inman, G.J.; et al. Clinicopathological Determinants of Recurrence Risk and Survival in Mucinous Ovarian Carcinoma. Cancers 2021, 13, 5839. [Google Scholar] [CrossRef]
- Lee, S.W.; Sung, J.-A.; Jung, M.; Kim, H.; Lee, C. Prognosis in primary mucinous ovarian carcinoma: Focusing on the five pathological findings indicating metastatic mucinous carcinoma to the ovary. J. Gynecol. Oncol. 2022, 33, e18. [Google Scholar] [CrossRef]
- Qi, X.; Xu, L.; Wang, J.; Yu, J.; Wang, Y. Nomograms for primary mucinous ovarian cancer: A SEER population-based study. J. Gynecol. Obstet. Hum. Reprod. 2022, 51, 102424. [Google Scholar] [CrossRef]
- Du Bois, A.; Reuss, A.; Pujade-Lauraine, E.; Harter, P.; Ray-Coquard, I.; Pfisterer, J. Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: A combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials: By the Arbeitsgemeinschaft Gynaekologische Onkologie Studiengruppe Ovarialkarzinom (AGO-OVAR) and the Groupe d’Investigateurs Nationaux Pour les Etudes des Cancers de l’Ovaire (GINECO. Cancer 2009, 115, 1234–1244. [Google Scholar] [CrossRef]
- Karabuk, E.; Kose, M.F.; Hizli, D.; Taşkin, S.; Karadağ, B.; Turan, T.; Boran, N.; Ozfuttu, A.; Ortaç, U.F. Comparison of advanced stage mucinous epithelial ovarian cancer and serous epithelial ovarian cancer with regard to chemosensitivity and survival outcome: A matched case-control study. J. Gynecol. Oncol. 2013, 24, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Zhu, Y.; Liu, C.; Chao, G.; Cui, R.; Zhang, Z. The prognosis impact of hyperthermic intraperitoneal chemotherapy (HIPEC) plus cytoreductive surgery (CRS) in advanced ovarian cancer: The meta-analysis. J. Ovarian Res. 2019, 12, 33. [Google Scholar] [CrossRef] [PubMed]
- Iavazzo, C.; Spiliotis, J. Is there a promising role of HIPEC in patients with advanced mucinous ovarian cancer? Arch. Gynecol. Obstet. 2021, 303, 597–598. [Google Scholar] [CrossRef] [PubMed]
- Van Driel, W.J.; Koole, S.N.; Sikorska, K.; Schagen van Leeuwen, J.H.; Schreuder, H.W.R.; Hermans, R.H.M.; De Hingh, I.H.; Van Der Velden, J.; Arts, H.J.; Massuger, L.F.; et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. N. Engl. J. Med. 2018, 378, 230–240. [Google Scholar] [CrossRef]
- The PSOGI Working Group; The BIG-RENAPE Working Group; Mercier, F.; Bakrin, N.; Bartlett, D.L.; Goere, D.; Quenet, F.; Dumont, F.; Heyd, B.; Abboud, K.; et al. Peritoneal Carcinomatosis of Rare Ovarian Origin Treated by Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy: A Multi-Institutional Cohort from PSOGI and BIG-RENAPE. Ann. Surg. Oncol. 2018, 25, 1668–1675. [Google Scholar] [CrossRef]
- Gore, M.; Hackshaw, A.; Brady, W.E.; Penson, R.T.; Zaino, R.; McCluggage, W.G.; Ganesan, R.; Wilkinson, N.; Perren, T.; Montes, A.; et al. An international, phase III randomized trial in patients with mucinous epithelial ovarian cancer (mEOC/GOG 0241) with long-term follow-up: And experience of conducting a clinical trial in a rare gynecological tumor. Gynecol. Oncol. 2019, 153, 541–548. [Google Scholar] [CrossRef]
- Li, X.; Sun, J.; He, X. Expression of c-myc and mutation of the KRAS gene in patients with ovarian mucinous tumors. Genet. Mol. Res. 2015, 14, 10752–10759. [Google Scholar] [CrossRef]
- Mackenzie, R.; Kommoss, S.; Winterhoff, B.J.; Kipp, B.R.; Garcia, J.J.; Voss, J.; Halling, K.; Karnezis, A.; Senz, J.; Yang, W.; et al. Targeted deep sequencing of mucinous ovarian tumors reveals multiple overlapping RAS-pathway activating mutations in borderline and cancerous neoplasms. BMC Cancer 2015, 15, 415. [Google Scholar] [CrossRef]
- Lin, W.-L.; Kuo, W.-H.; Chen, F.-L.; Lee, M.-Y.; Ruan, A.; Tyan, Y.-S.; Hsu, J.-D.; Chiang, H.; Han, C.-P. Identification of the Coexisting HER2 Gene Amplification and Novel Mutations in the HER2 Protein-Overexpressed Mucinous Epithelial Ovarian Cancer. Ann. Surg. Oncol. 2011, 18, 2388–2394. [Google Scholar] [CrossRef]
- Rechsteiner, M.; Zimmermann, A.-K.; Wild, P.J.; Caduff, R.; von Teichman, A.; Fink, D.; Moch, H.; Noske, A. TP53 mutations are common in all subtypes of epithelial ovarian cancer and occur concomitantly with KRAS mutations in the mucinous type. Exp. Mol. Pathol. 2013, 95, 235–241. [Google Scholar] [CrossRef]
- Meagher, N.S.; Gorringe, K.L.; Wakefield, M.J.; Bolithon, A.; Pang, C.N.I.; Chiu, D.S.; Anglesio, M.S.; Mallitt, K.-A.; Doherty, J.A.; Harris, H.R.; et al. Gene-Expression Profiling of Mucinous Ovarian Tumors and Comparison with Upper and Lower Gastrointestinal Tumors Identifies Markers Associated with Adverse Outcomes. Clin. Cancer Res. 2022, 28, 5383–5395. [Google Scholar] [CrossRef]
- Richardson, M.T.; Recouvreux, M.S.; Karlan, B.Y.; Walts, A.E.; Orsulic, S. Ciliated Cells in Ovarian Cancer Decrease with Increasing Tumor Grade and Disease Progression. Cells 2022, 11, 4009. [Google Scholar] [CrossRef] [PubMed]
- Affatato, R.; Carrassa, L.; Chilà, R.; Lupi, M.; Restelli, V.; Damia, G. Identification of PLK1 as a New Therapeutic Target in Mucinous Ovarian Carcinoma. Cancers 2020, 12, 672. [Google Scholar] [CrossRef] [PubMed]
- The Cancer Genome Atlas Research Network. Integrated genomic analyses of ovarian carcinoma. Nature 2011, 474, 609–615. [Google Scholar] [CrossRef]
- D’Ambrosio, C.; Erriquez, J.; Arigoni, M.; Capellero, S.; Mittica, G.; Ghisoni, E.; Borella, F.; Katsaros, D.; Privitera, S.; Ribotta, M.; et al. PIK3R1W624R Is an Actionable Mutation in High Grade Serous Ovarian Carcinoma. Cells 2020, 9, 442. [Google Scholar] [CrossRef] [PubMed]
- Inaba, K.; Oda, K.; Aoki, K.; Sone, K.; Ikeda, Y.; Miyasaka, A.; Kashiyama, T.; Fukuda, T.; Makii, C.; Arimoto, T.; et al. Synergistic antitumor effects of combination PI3K/mTOR and MEK inhibition (SAR245409 and pimasertib) in mucinous ovarian carcinoma cells by fluorescence resonance energy transfer imaging. Oncotarget 2016, 7, 29577–29591. [Google Scholar] [CrossRef]
- Spreafico, A.; Oza, A.M.; Clarke, B.A.; Mackay, H.J.; Shaw, P.; Butler, M.; Dhani, N.C.; Lheureux, S.; Wilson, M.K.; Welch, S.; et al. Genotype-matched treatment for patients with advanced type I epithelial ovarian cancer (EOC). Gynecol. Oncol. 2017, 144, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Liew, P.-L.; Huang, R.-L.; Weng, Y.-C.; Fang, C.-L.; Huang, T.H.-M.; Lai, H.-C. Distinct methylation profile of mucinous ovarian carcinoma reveals susceptibility to proteasome inhibitors: Methylation Profile of MuOC and PSMB8. Int. J. Cancer 2018, 143, 355–367. [Google Scholar] [CrossRef]
- Sato, E.; Olson, S.H.; Ahn, J.; Bundy, B.; Nishikawa, H.; Qian, F.; Jungbluth, A.A.; Frosina, D.; Gnjatic, S.; Ambrosone, C.; et al. Intraepithelial CD8+ tumor-infiltrating lymphocytes and a high CD8+/regulatory T cell ratio are associated with favorable prognosis in ovarian cancer. Proc. Natl. Acad. Sci. USA 2005, 102, 18538–18543. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Conejo-Garcia, J.R.; Katsaros, D.; Gimotty, P.A.; Massobrio, M.; Regnani, G.; Makrigiannakis, A.; Gray, H.; Schlienger, K.; Liebman, M.N.; et al. Intratumoral T Cells, Recurrence, and Survival in Epithelial Ovarian Cancer. N. Engl. J. Med. 2003, 348, 203–213. [Google Scholar] [CrossRef]
- Hwang, W.-T.; Adams, S.F.; Tahirovic, E.; Hagemann, I.S.; Coukos, G. Prognostic significance of tumor-infiltrating T cells in ovarian cancer: A meta-analysis. Gynecol. Oncol. 2012, 124, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Borella, F.; Ghisoni, E.; Giannone, G.; Cosma, S.; Benedetto, C.; Valabrega, G.; Katsaros, D. Immune Checkpoint Inhibitors in Epithelial Ovarian Cancer: An Overview on Efficacy and Future Perspectives. Diagnostics 2020, 10, 146. [Google Scholar] [CrossRef]
- Martín, A.G.; Sánchez-Lorenzo, L. Immunotherapy with checkpoint inhibitors in patients with ovarian cancer: Still promising? Cancer 2019, 125 (Suppl. S24), 4616–4622. [Google Scholar] [CrossRef] [PubMed]
- Meagher, N.S.; Hamilton, P.; Milne, K.; Thornton, S.; Harris, B.; Weir, A.; Alsop, J.; Bisinoto, C.; Brenton, J.D.; Brooks-Wilson, A.; et al. Profiling the immune landscape in mucinous ovarian carcinoma. Gynecol. Oncol. 2022, 168, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Pal, T.; Permuth-Wey, J.; Kumar, A.; Sellers, T.A. Systematic Review and Meta-analysis of Ovarian Cancers: Estimation of Microsatellite-High Frequency and Characterization of Mismatch Repair Deficient Tumor Histology. Clin. Cancer Res. 2008, 14, 6847–6854. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.A.; Wentzensen, N. Frequency of mismatch repair deficiency in ovarian cancer: A systematic review This article is a US Government work and, as such, is in the public domain of the United States of America. Int. J. Cancer 2011, 129, 1914–1922. [Google Scholar] [CrossRef] [PubMed]
- Segev, Y.; Pal, T.; Rosen, B.; McLaughlin, J.R.; Sellers, T.A.; Risch, H.A.; Zhang, S.; Sun, P.; Narod, S.A.; Schildkraut, J. Risk Factors for Ovarian Cancers with and without Microsatellite Instability. Int. J. Gynecol. Cancer 2014, 24, 664–669. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Study | Growth Pattern | Number of Early MOC Patients | FIGO Staging, Number | Tumor Grading, Number | Rupture Capsule | Recurrence Rate | FU (Months) |
|---|---|---|---|---|---|---|---|
| Lee and Scully 2000 [20] | ESI ISI | 12 6 | Ia Ia | G1: 8, G2: 4 NA | IO: 3/25 * | 0/12 1/6(16.7%) | 33–135 36–135 |
| Chen et al. [21] | ISI | 4/6 | Ia, 2 Ic, 2 | G1:1 G2: 3 | PO:1 IO: 1 | 1/2 1/2 | 9–161 |
| Tabrizi et al. [22] | ESI ISI | 26 4 | NA NA | NA G3: 4 | PO: 5 IO: 12 | 6/26 1/4 | 6–176 |
| Muyldermans et al. [23] | ESI ISI | 21 12 | Ia, 11 Ic, 10 Ia, 9 Ic, 3 | G1: 20 G2: 20 G3: 4 | NA NA | 0 1/9 1/3 | 64 |
| Gouy S et al. [24] | ESI ISI | 29 39 | Ia, 13 Ic1, 9 Ic2, 5 Ic3, 2 Ia, 22 Ic1, 9 Ic2, 7 Ic3, 1 | G1: 11 G2: 10 G3: 0 Gx: 8 NA | PO:6 IO: 8 PO:6 IO: 6 | 3/29 6/39 | NA |
| Kajiyama et al. [25] | NA | 194 | Ia, 85 Ib, 2 Ic1, 58 Ic2, 18 Ic3, 31 | NA | IO: 58 PO: 49 | 36/194 | 2–248 |
| Rodriguez and Prat [31] | ESI ISI | 15 11 | Ia, 10 Ic, 5 Ia, 8 Ic, 3 | G1:4, G2:11 G3: 11 | PO: 4/15 IO: 1/15 PO: 1/11 IO: 2/11 | 0/15 0/8 3/3(100) | 40–194 12–180 |
| Ludwick et al. [34] | ESI | 3 | Ia:3 | NA | NA | 3/3 | 7–32 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borella, F.; Mitidieri, M.; Cosma, S.; Benedetto, C.; Bertero, L.; Fucina, S.; Ray-Coquard, I.; Carapezzi, A.; Ferraioli, D. Update on Prognostic and Predictive Markers in Mucinous Ovarian Cancer. Cancers 2023, 15, 1172. https://doi.org/10.3390/cancers15041172
Borella F, Mitidieri M, Cosma S, Benedetto C, Bertero L, Fucina S, Ray-Coquard I, Carapezzi A, Ferraioli D. Update on Prognostic and Predictive Markers in Mucinous Ovarian Cancer. Cancers. 2023; 15(4):1172. https://doi.org/10.3390/cancers15041172
Chicago/Turabian StyleBorella, Fulvio, Marco Mitidieri, Stefano Cosma, Chiara Benedetto, Luca Bertero, Stefano Fucina, Isabelle Ray-Coquard, Annalisa Carapezzi, and Domenico Ferraioli. 2023. "Update on Prognostic and Predictive Markers in Mucinous Ovarian Cancer" Cancers 15, no. 4: 1172. https://doi.org/10.3390/cancers15041172