
Relationship of Post-Transplant Lymphoproliferative Disorders (PTLD) Subtypes and Clinical Outcome in Pediatric Heart Transplant Recipients: A Retrospective Single Institutional Analysis/Experience of 558 Patients
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
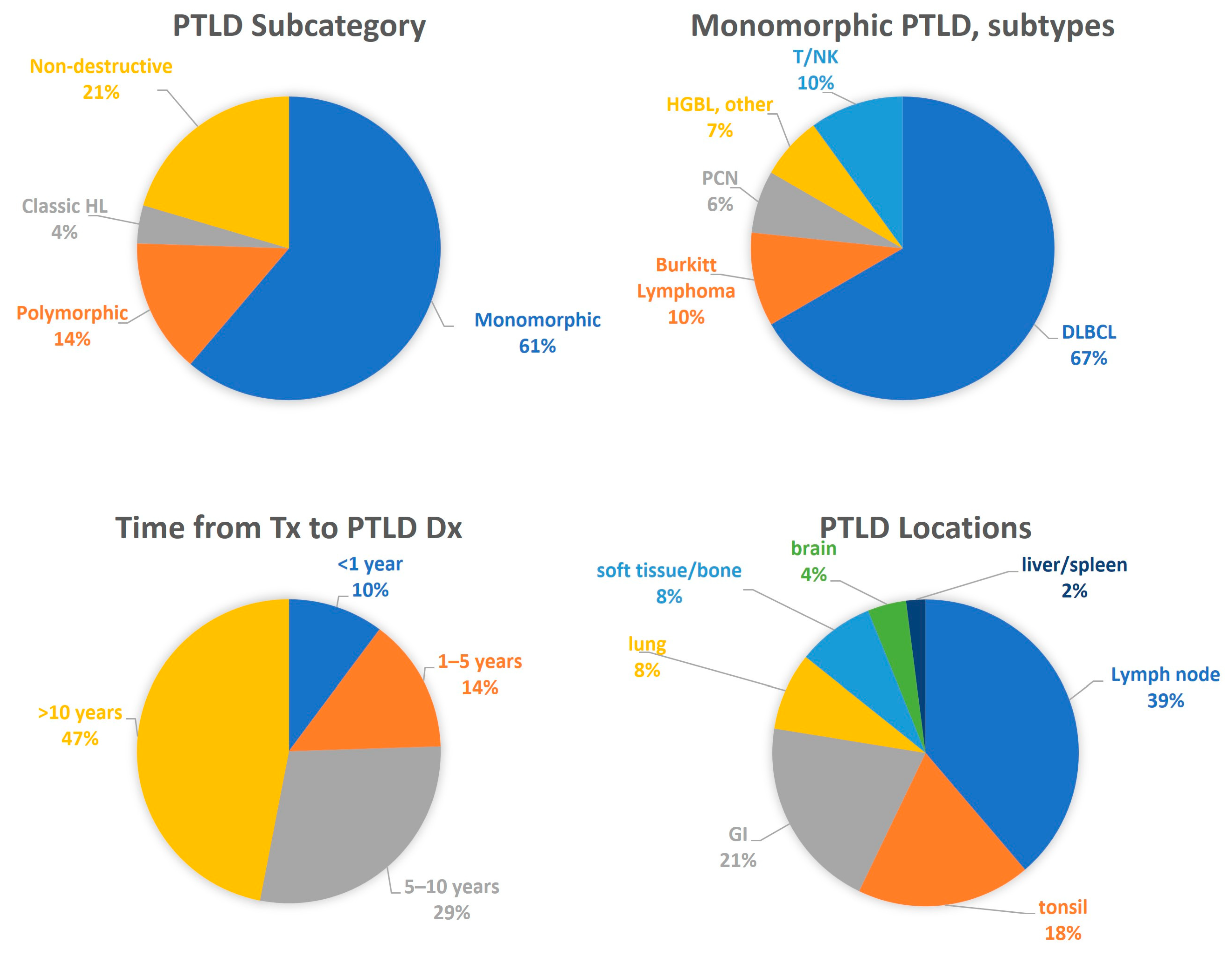
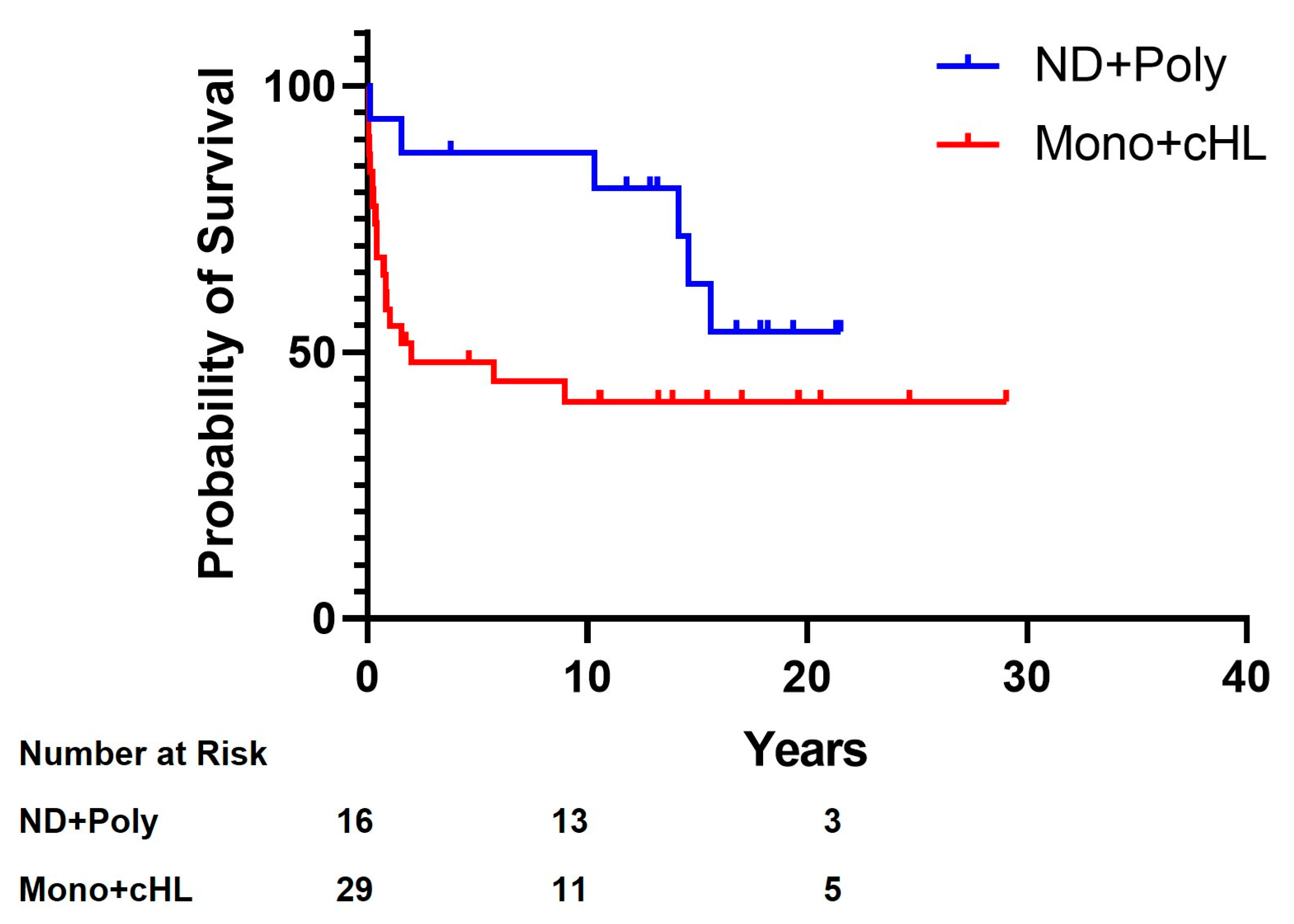
3.1. General Clinical Features
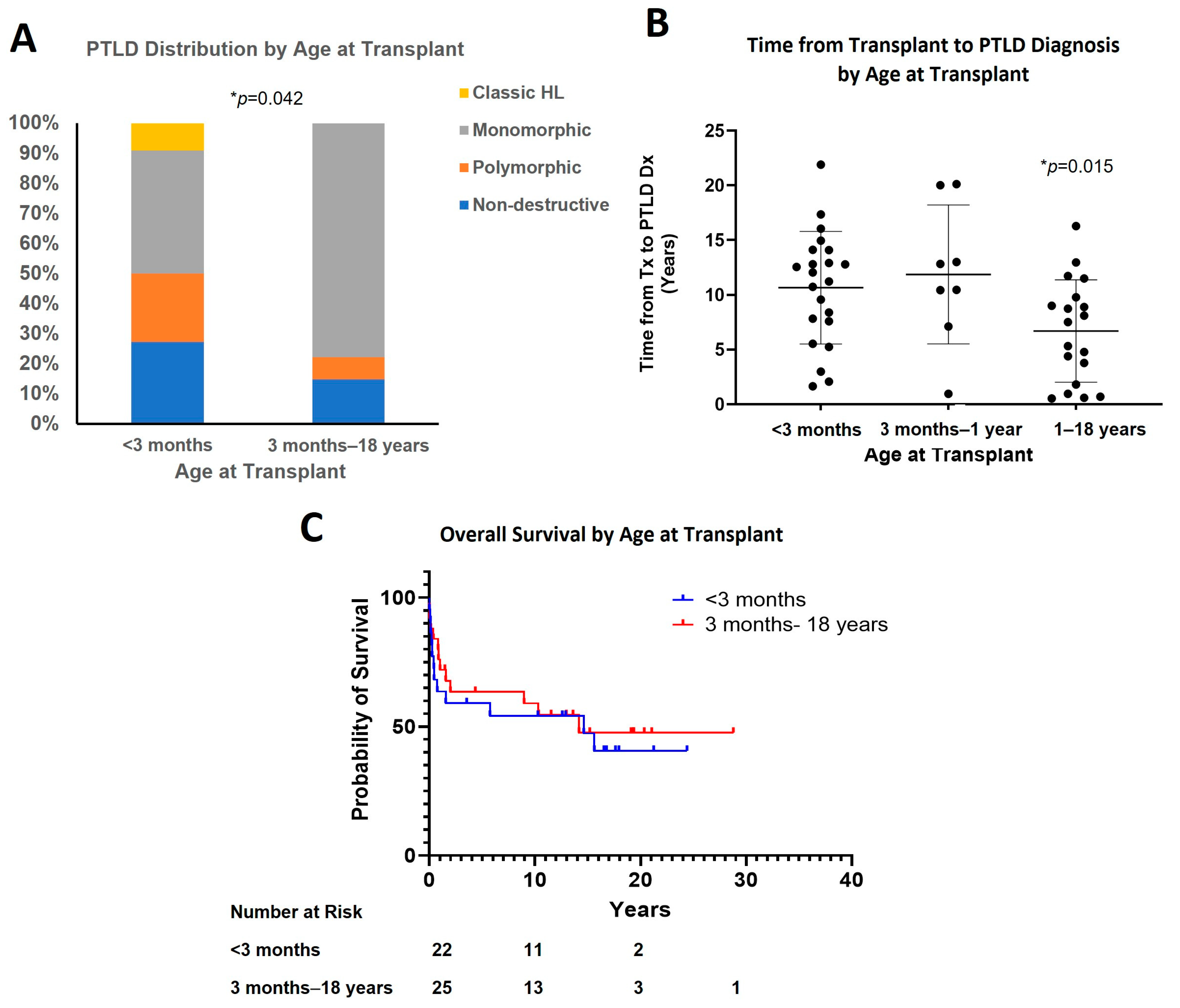
3.2. Effect of Age at Transplant
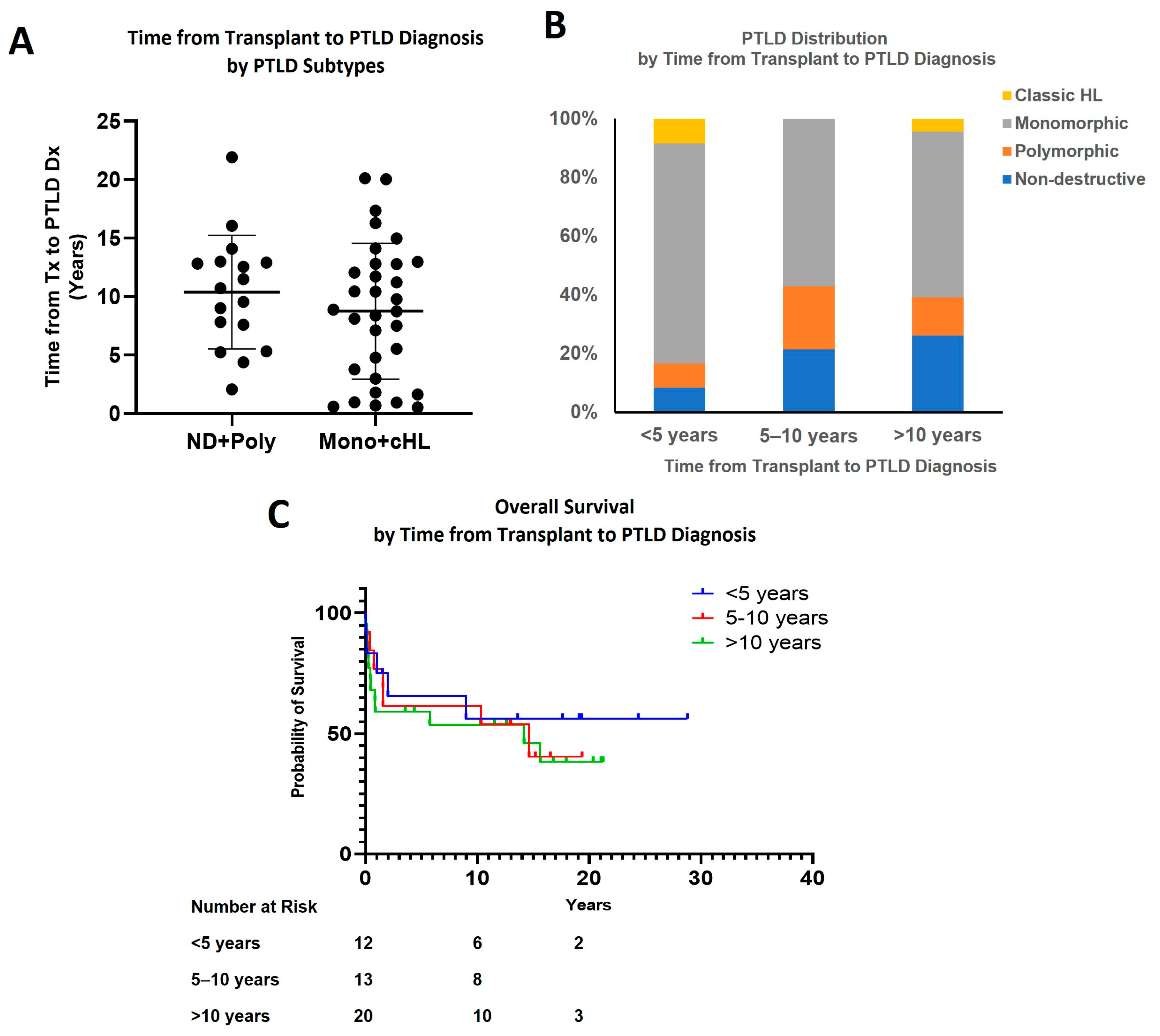
3.3. Effect of Time Interval from Transplant to PTLD Diagnosis
3.4. EBER and EBV Infection Status
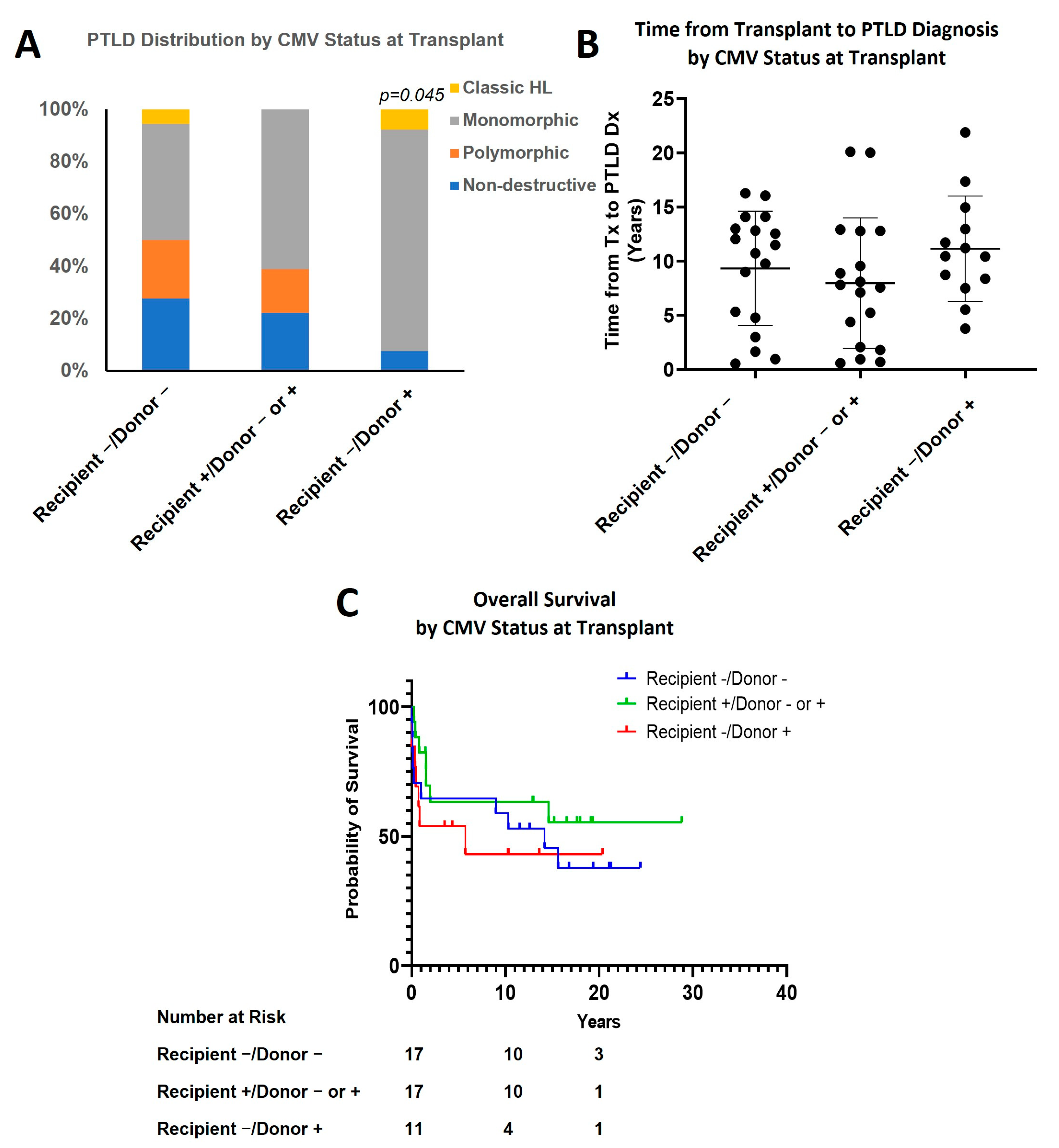
3.5. Effect of CMV Status
3.6. Effect of Recipient and Donor Blood Type
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hanto, D.W. Classification of Epstein-Barr Virus-Associated Posttransplant Lymphoproliferative Diseases: Implications for Understanding Their Pathogenesis and Developing Rational Treatment Strategies. Annu. Rev. Med. 1995, 46, 381–394. [Google Scholar] [CrossRef] [PubMed]
- Campo, E.; Jaffe, E.S.; Cook, J.R.; Quintanilla-Martinez, L.; Swerdlow, S.H.; Anderson, K.C.; Brousset, P.; Cerroni, L.; de Leval, L.; Dirnhofer, S.; et al. The International Consensus Classification of Mature Lymphoid Neoplasms: A Report from the Clinical Advisory Committee. Blood 2022, 140, 1229–1253. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 Revision of the World Health Organization Classification of Lymphoid Neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef] [PubMed]
- Nijland, M.L.; Kersten, M.J.; Pals, S.T.; Bemelman, F.J.; Ten Berge, I.J.M. Epstein-Barr Virus-Positive Posttransplant Lymphoproliferative Disease After Solid Organ Transplantation: Pathogenesis, Clinical Manifestations, Diagnosis, and Management. Transplant. Direct 2016, 2, e48. [Google Scholar] [CrossRef]
- Al Hamed, R.; Bazarbachi, A.H.; Mohty, M. Epstein-Barr Virus-Related Post-Transplant Lymphoproliferative Disease (EBV-PTLD) in the Setting of Allogeneic Stem Cell Transplantation: A Comprehensive Review from Pathogenesis to Forthcoming Treatment Modalities. Bone Marrow Transplant. 2020, 55, 25–39. [Google Scholar] [CrossRef]
- Abbas, F.; El Kossi, M.; Shaheen, I.S.; Sharma, A.; Halawa, A. Post-Transplantation Lymphoproliferative Disorders: Current Concepts and Future Therapeutic Approaches. World J. Transplant. 2020, 10, 29–46. [Google Scholar] [CrossRef]
- Schober, T.; Framke, T.; Kreipe, H.; Schulz, T.F.; Großhennig, A.; Hussein, K.; Baumann, U.; Pape, L.; Schubert, S.; Wingen, A.-M.; et al. Characteristics of Early and Late PTLD Development in Pediatric Solid Organ Transplant Recipients. Transplantation 2013, 95, 240–246. [Google Scholar] [CrossRef]
- Bishnoi, R.; Bajwa, R.; Franke, A.J.; Skelton, W.P.; Wang, Y.; Patel, N.M.; Slayton, W.B.; Zou, F.; Dang, N.H. Post-Transplant Lymphoproliferative Disorder (PTLD): Single Institutional Experience of 141 Patients. Exp. Hematol. Oncol. 2017, 6, 26. [Google Scholar] [CrossRef]
- Pierce, B.J.; Allen, E.; Pham, C.; Nguyen, D.T.; Graviss, E.A.; Goodarzi, A.; Yau, S.W.; Youssef, J.G.; Huang, H.J. Identification of Epstein-Barr Virus Related Risk Factors for the Occurrence of Post-Transplant Lymphoproliferative Disorder in Lung Transplant Recipients. J. Heart Lung Transplant. 2021, 40, S67. [Google Scholar] [CrossRef]
- Kinzel, M.; Dowhan, M.; Kalra, A.; Williamson, T.S.; Dabas, R.; Jamani, K.; Chaudhry, A.; Shafey, M.; Jimenez-Zepeda, V.; Duggan, P.; et al. Risk Factors for the Incidence of and the Mortality Due to Post-Transplant Lymphoproliferative Disorder after Hematopoietic Cell Transplantation. Transplant. Cell. Ther. 2022, 28, 53.e1–53.e10. [Google Scholar] [CrossRef]
- Uhlin, M.; Wikell, H.; Sundin, M.; Blennow, O.; Maeurer, M.; Ringden, O.; Winiarski, J.; Ljungman, P.; Remberger, M.; Mattsson, J. Risk Factors for Epstein-Barr Virus-Related Post-Transplant Lymphoproliferative Disease after Allogeneic Hematopoietic Stem Cell Transplantation. Haematologica 2014, 99, 346–352. [Google Scholar] [CrossRef]
- Bailey, L.L. Origins of Neonatal Heart Transplantation: An Historical Perspective. Semin. Thorac. Cardiovasc. Surg. Pediatr. Card. Surg. Annu. 2011, 14, 98–100. [Google Scholar] [CrossRef]
- Kawauchi, M.; Gundry, S.R.; Bailey, L.L. Infant and pediatric heart transplantation: Loma Linda experience. Kyobu Geka. 1991, 44, 748–752. [Google Scholar]
- Bouchart, F.; Gundry, S.R.; Bailey, L.L. Infant Heart Transplantation 1991. Clin. Transpl. 1991, 97–104. [Google Scholar]
- Dotti, G.; Fiocchi, R.; Motta, T.; Mammana, C.; Gotti, E.; Riva, S.; Cornelli, P.; Gridelli, B.; Viero, P.; Oldani, E.; et al. Lymphomas Occurring Late after Solid-Organ Transplantation: Influence of Treatment on the Clinical Outcome. Transplantation 2002, 74, 1095–1102. [Google Scholar] [CrossRef]
- Quinlan, S.C.; Pfeiffer, R.M.; Morton, L.M.; Engels, E.A. Risk Factors for Early-Onset and Late-Onset Post-Transplant Lymphoproliferative Disorder in Kidney Recipients in the United States. Am. J. Hematol. 2011, 86, 206–209. [Google Scholar] [CrossRef]
- Opelz, G.; Döhler, B. Lymphomas after Solid Organ Transplantation: A Collaborative Transplant Study Report. Am. J. Transplant. 2004, 4, 222–230. [Google Scholar] [CrossRef]
- Al-Mansour, Z.; Nelson, B.P.; Evens, A.M. Post-Transplant Lymphoproliferative Disease (PTLD): Risk Factors, Diagnosis, and Current Treatment Strategies. Curr. Hematol. Malig. Rep. 2013, 8, 173–183. [Google Scholar] [CrossRef]
- Fujimoto, A.; Hiramoto, N.; Yamasaki, S.; Inamoto, Y.; Uchida, N.; Maeda, T.; Mori, T.; Kanda, Y.; Kondo, T.; Tanaka, J.; et al. Risk Factors and Predictive Scoring System for Post-Transplant Lymphoproliferative Disorder after Hematopoietic Stem Cell Transplantation. Blood 2018, 132, 250. [Google Scholar] [CrossRef]
- Malyszko, J. Post-Transplant Lymphoproliferative Disorder: Risk Factors and Management. Nephrol. Dial. Transplant. 2021, 36, 1177–1179. [Google Scholar] [CrossRef]
- Jagadeesh, D.; Woda, B.A.; Draper, J.; Evens, A.M. Post Transplant Lymphoproliferative Disorders: Risk, Classification, and Therapeutic Recommendations. Curr. Treat. Options Oncol. 2012, 13, 122–136. [Google Scholar] [CrossRef]
- Pearse, W.B.; Vakkalagadda, C.V.; Helenowski, I.; Winter, J.N.; Gordon, L.I.; Karmali, R.; Ma, S.; Leventhal, J.R.; Friedewald, J.; Ganger, D.; et al. Prognosis and Outcomes of Patients with Post-Transplant Lymphoproliferative Disorder: A Single Center Retrospective Review. Blood 2020, 136, 9–10. [Google Scholar] [CrossRef]
- Schubert, S.; Abdul-Khaliq, H.; Lehmkuhl, H.B.; Yegitbasi, M.; Reinke, P.; Kebelmann-Betzig, C.; Hauptmann, K.; Gross-Wieltsch, U.; Hetzer, R.; Berger, F. Diagnosis and Treatment of Post-Transplantation Lymphoproliferative Disorder in Pediatric Heart Transplant Patients. Pediatr. Transplant. 2009, 13, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Manlhiot, C.; Pollock-Barziv, S.M.; Holmes, C.; Weitzman, S.; Allen, U.; Clarizia, N.A.; Ngan, B.-Y.; McCrindle, B.W.; Dipchand, A.I. Post-Transplant Lymphoproliferative Disorder in Pediatric Heart Transplant Recipients. J. Heart lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2010, 29, 648–657. [Google Scholar] [CrossRef]
- Lau, E.; Moyers, J.T.; Wang, B.C.; Jeong, I.S.D.; Lee, J.; Liu, L.; Kim, M.; Villicana, R.; Kim, B.; Mitchell, J.; et al. Analysis of Post-Transplant Lymphoproliferative Disorder (PTLD) Outcomes with Epstein-Barr Virus (EBV) Assessments-A Single Tertiary Referral Center Experience and Review of Literature. Cancers 2021, 13, 899. [Google Scholar] [CrossRef] [PubMed]
- Zangwill, S.D.; Hsu, D.T.; Kichuk, M.R.; Garvin, J.H.; Stolar, C.J.; Haddad, J.J.; Stylianos, S.; Michler, R.E.; Chadburn, A.; Knowles, D.M.; et al. Incidence and Outcome of Primary Epstein-Barr Virus Infection and Lymphoproliferative Disease in Pediatric Heart Transplant Recipients. J. Heart Lung Transplant. 1998, 17, 1161–1166. [Google Scholar]
- Nelson, B.P.; Wolniak, K.L.; Evens, A.; Chenn, A.; Maddalozzo, J.; Proytcheva, M. Early Posttransplant Lymphoproliferative Disease: Clinicopathologic Features and Correlation with MTOR Signaling Pathway Activation. Am. J. Clin. Pathol. 2012, 138, 568–578. [Google Scholar] [CrossRef]
- Webber, S.A.; Naftel, D.C.; Fricker, F.J.; Olesnevich, P.; Blume, E.D.; Addonizio, L.; Kirklin, J.K.; Canter, C.E. Lymphoproliferative Disorders after Paediatric Heart Transplantation: A Multi-Institutional Study. Lancet 2006, 367, 233–239. [Google Scholar] [CrossRef]
- Reshef, R.; Vardhanabhuti, S.; Luskin, M.R.; Heitjan, D.F.; Hadjiliadis, D.; Goral, S.; Krok, K.L.; Goldberg, L.R.; Porter, D.L.; Stadtmauer, E.A.; et al. Reduction of Immunosuppression as Initial Therapy for Posttransplantation Lymphoproliferative Disorder. Am. J. Transplant. 2011, 11, 336–347. [Google Scholar] [CrossRef]
- Luong, M.-L.; Kim, J.; Rotstein, C.; Husain, S. Does CMV Mismatch Status Modify the Risk of PTLD Due to EBV Mismatch Status in Lung and Heart Transplant Recipients? J. Heart Lung Transplant. 2013, 32, S130. [Google Scholar] [CrossRef]
- Kim, J.M.; Lee, S.-K.; Kim, S.J.; Joh, J.-W.; Kwon, C.H.D.; Choe, Y.H.; Shin, M.; Kim, E.Y.; Moon, J.I.; Jung, G.O.; et al. Risk Factors for Posttransplant Lymphoproliferative Disorder in Pediatric Liver Transplant Recipients with Cytomegalovirus Antigenemia. Transplant. Proc. 2010, 42, 895–899. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | ND-PTLD | P-PTLD | M-PTLD | cHL-PTLD | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| PH | IM-Like | FFH | DLBCL | Burkitt | HGBL, Other | PCN | T/NK | ||||
| All | 49 | 2 | 7 | 1 | 7 | 20 | 3 | 2 | 2 | 3 | 2 |
| Genders | |||||||||||
| Male | 31 | 1 | 4 | 0 | 4 | 13 | 2 | 0 | 2 | 3 | 2 |
| Female | 18 | 1 | 3 | 1 | 3 | 7 | 1 | 2 | 0 | 0 | 0 |
| Race | |||||||||||
| Caucasian | 22 | 0 | 5 | 1 | 4 | 8 | 0 | 1 | 0 | 2 | 1 |
| Hispanic/Latino | 21 | 2 | 2 | 0 | 2 | 9 | 2 | 1 | 2 | 1 | 0 |
| Others | 6 | 0 | 0 | 0 | 1 | 3 | 1 | 0 | 0 | 0 | 1 |
| Tumor EBER status | |||||||||||
| Positive | 33 | 1 | 6 | 1 | 5 | 13 | 1 | 1 | 1 | 2 | 2 |
| Negative | 9 | 0 | 0 | 0 | 1 | 4 | 2 | 0 | 1 | 1 | 0 |
| Not available | 7 | 1 | 1 | 0 | 1 | 3 | 0 | 1 | 0 | 0 | 0 |
| EBV infection | |||||||||||
| Positive | 35 | 1 | 7 | 0 | 6 | 15 | 3 | 1 | 1 | 1 | 0 |
| Negative | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| Not avaible | 13 | 1 | 0 | 1 | 1 | 4 | 0 | 1 | 1 | 2 | 2 |
| Tumor EBER status/EBV infection | |||||||||||
| Pos/Pos | 28 | 1 | 6 | 0 | 5 | 12 | 1 | 1 | 1 | 1 | 0 |
| Neg/Neg | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| Neg/Pos | 3 | 0 | 0 | 0 | 0 | 1 | 2 | 0 | 0 | 0 | 0 |
| Age at Tx | |||||||||||
| <3 months | 22 | 0 | 6 | 0 | 5 | 5 | 1 | 0 | 1 | 2 | 2 |
| 3 months–18 years | 27 | 2 | 1 | 1 | 2 | 15 | 2 | 2 | 1 | 1 | 0 |
| Time from Tx to PTLD Dx | |||||||||||
| <1 year | 5 | 0 | 0 | 0 | 0 | 3 | 0 | 1 | 1 | 0 | 0 |
| 1–5 years | 7 | 1 | 0 | 0 | 1 | 3 | 1 | 0 | 0 | 0 | 1 |
| 5–10 years | 14 | 1 | 2 | 0 | 3 | 6 | 2 | 0 | 0 | 0 | 0 |
| >10 years | 23 | 0 | 5 | 1 | 3 | 8 | 0 | 1 | 1 | 3 | 1 |
| CMV status at Tx | |||||||||||
| Recipient−/Donor− | 18 | 1 | 3 | 1 | 4 | 3 | 2 | 0 | 2 | 1 | 1 |
| Recipient−/Donor+ | 13 | 0 | 1 | 0 | 0 | 9 | 1 | 0 | 0 | 1 | 1 |
| Recipient+/Donor− or + | 18 | 1 | 3 | 0 | 3 | 8 | 0 | 2 | 0 | 1 | 0 |
| Blood type and Rh status | |||||||||||
| Recipient O+/Donor O+ or O− or Recipient B+/Donor B+ or B− or Recipient A+/Donor A+ or A− | 37 | 2 | 7 | 1 | 5 | 16 | 2 | 1 | 1 | 1 | 1 |
| Recipient A+ or B+/Donor O+ | 7 | 0 | 0 | 0 | 1 | 2 | 0 | 1 | 1 | 2 | 0 |
| Recipient A−/Donor A+ or Recipient O−/Donor O+ | 5 | 0 | 0 | 0 | 1 | 2 | 1 | 0 | 0 | 0 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.; Wang, B.C.; Zuppan, C.W.; Chau, P.; Fitts, J.; Chinnock, R.; Wang, J. Relationship of Post-Transplant Lymphoproliferative Disorders (PTLD) Subtypes and Clinical Outcome in Pediatric Heart Transplant Recipients: A Retrospective Single Institutional Analysis/Experience of 558 Patients. Cancers 2023, 15, 976. https://doi.org/10.3390/cancers15030976
Liu Y, Wang BC, Zuppan CW, Chau P, Fitts J, Chinnock R, Wang J. Relationship of Post-Transplant Lymphoproliferative Disorders (PTLD) Subtypes and Clinical Outcome in Pediatric Heart Transplant Recipients: A Retrospective Single Institutional Analysis/Experience of 558 Patients. Cancers. 2023; 15(3):976. https://doi.org/10.3390/cancers15030976
Chicago/Turabian StyleLiu, Yan, Billy C. Wang, Craig W. Zuppan, Peter Chau, James Fitts, Richard Chinnock, and Jun Wang. 2023. "Relationship of Post-Transplant Lymphoproliferative Disorders (PTLD) Subtypes and Clinical Outcome in Pediatric Heart Transplant Recipients: A Retrospective Single Institutional Analysis/Experience of 558 Patients" Cancers 15, no. 3: 976. https://doi.org/10.3390/cancers15030976